Embed Size (px)
Citation preview
![Page 1: [IEEE 2014 Middle East Conference on Biomedical Engineering (MECBME) - Doha, Qatar (2014.02.17-2014.02.20)] 2nd Middle East Conference on Biomedical Engineering - Tissue perfusion](https://reader031.pdfslide.us/reader031/viewer/2022020410/5750a7f71a28abcf0cc50749/html5/thumbnails/1.jpg)
Jamal Siam is a doctoral candidate at the Department of Biomedical
Engineering at Tel Aviv University, Israel, and a lecturer at Birzeit University, Palestine (email: [email protected]).
Ofer Barnea is a Professor of Biomedical Engineering at the Department of
Biomedical Engineering at Tel Aviv University, Ramat Aviv 69978, Israel (e-mail: [email protected]).
\ \
Abstract Fluid resuscitation affects blood flow and oxygen
concentration. Administered fluid increases blood flow and
oxygen delivery rate but also decreases blood oxygen
concentration. This study aims at analyzing these two effects on
oxygen supply to tissue to determine an optimal fluid regimen.
For this purpose a hemodynamic model of the cardiovascular
system and a model of oxygen transfer to tissue were developed
and combined. Simulation results showed that indeed fluid
administration increases oxygen delivery by the blood stream.
However, oxygen transfer to tissue deteriorates during the
course of the fluid therapy due to the high sensitivity of oxygen
diffusion to oxygen partial pressure in the blood.
I. INTRODUCTION
Hemorrhagic shock is one of the most frequent aspects of
injury that trauma care emergency units have to deal with.
Advanced Trauma Life Support (ATLS) and the British
National Institute for Clinical Excellence (NHS) consider
fluid resuscitation as one of the essential procedures that
must be followed in the treatment of the hemorrhage trauma
[1,2]. Fluid resuscitation aims at maintaining oxygen
delivery to tissue and restoring hemodynamic stability.
Effectiveness of fluid resuscitation and clinical endpoint are
determined using general clinical symptoms. These
symptoms are generally a cumulative effect of several
shock and fluid therapy. Several studies used animal
experiments and other used mathematical modeling to study
and better understand the effects of hemorrhage and fluid
resuscitation on oxygen delivery and tissue perfusion. Some
of these studies focused on the cardiovascular,
hemodynamic and oxygen related phenomena at the system
level [3-17], while others developed tissue and oxygen
diffusion models using specific parameters at the tissue side
[18-30].
Despite the results of studies that indicated that fluid
infusion should be limited, many issues regarding type of
fluid, infusion rate, and infusion volume remain
controversial. Fluid replacement with crystalloid and colloid
fluids is believed to improve the hemodynamic stability, but
it has the collateral effect of diluting blood and reducing the
concentration of oxygen carriers. Therefore, there is need to
better understand the effects fluid on the actual target
parameters, i.e. oxygen partial pressure in the tissue that is
directly related to oxygen supply to the mitochondria.
II. METHODS
Two models were developed and combined: a model of
cardiovascular hemodynamics and a model of a capillary
irrigating a tissue segment. The cardiovascular model was
developed to generate a hemodynamic response and predict
blood pressure and flow as well as oxygen content in the
blood in normal conditions, hemorrhage and fluid
resuscitation. The model is described in [3]. It considers a
human body of 75 kg with a total blood volume of 5600 and
initial hematocrit of 44%. The model assumes autoregulation
mechanisms have been exhausted. The model is composed
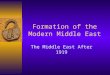
of four cardiac chambers, a nine-segment aorta, seven
systemic branches, a systemic vein, and a pulmonary
circulation (Fig. 1). Important effects such as blood dilution,
effects of hematocrit on blood viscosity, fluid exchange
between the intravascular space and the interstitium,
bleeding and fluid infusion are also included in this module.
The tissue model was structured as a cascade of identical
tissue sample volumes (Fig. 2). Each sample volume is
based on structure and is composed of a set of
parallel cylindrical fibers [25]. Oxygen is delivered to each
cylindrical tissue segment by a concentric cylindrical blood
capillary. The model represents a single tissue element; this
into hollow tubes of equal radial thickness and equal axial
length (Fig.2). The tissue element and the capillary are both
axially segmented. Blood oxygen is assumed to diffuse
Tissue Perfusion in Fluid Therapy
Jamal Siam, and Ofer Barnea, Senior Member, IEEE
Figure 1. Structure of the hemodynamic model
Figure 2. Structure of the capillary-tissue model.
2014 Middle East Conference on Biomedical Engineering (MECBME)February 17-20, 2014, Hilton Hotel, Doha, Qatar
978-1-4799-4799-7/14/$31.00 ©2014 IEEE 196
![Page 2: [IEEE 2014 Middle East Conference on Biomedical Engineering (MECBME) - Doha, Qatar (2014.02.17-2014.02.20)] 2nd Middle East Conference on Biomedical Engineering - Tissue perfusion](https://reader031.pdfslide.us/reader031/viewer/2022020410/5750a7f71a28abcf0cc50749/html5/thumbnails/2.jpg)
between the capillary and the tissue cylinder in the radial
direction. However, the diffusion in the tissue is not limited
to the radial direction as in other models. The model
-
symmetric structure and no-flux condition among the
parallel cylinders from the cylindrical surfaces but the
restrictions and boundary condition have been dramatically
relaxed. Moreover, we do not impose any conditions on the
oxygen partial pressure at the venous-end of the capillary.
To study the effects of fluid therapy in controlled
hemorrhagic shock, several hemorrhagic conditions were
simulated. The hemodynamic model provided pressure and
capillary flow, hematocrit (HCT) during blood loss, infusion
and stabilization period with no infusion. Oxygen delivery
rate ( ) was calculated as the product of blood flow and
blood oxygen content. Capillary blood flow and oxygen
content were used in the capillary-tissue model to calculate
the oxygen partial pressure field in the tissue and to
determine the mean in the tissue.
III. RESULTS
The total blood losses for the various hemorrhage
conditions (class II, III, and IV) were 1100 ml, 1540 ml, and
2420 ml, respectively. Infusion of fluid caused a significant
increase in blood pressure in parallel with marked reduction
in hematocrit. Higher infusion rates induced a more
substantial increase in blood volume and arterial pressures
resulting in greater capillary flow and decrease in HCT.
After the termination of fluid infusion, intravascular fluid
volume continued to filtrate into the interstitial compartment
resulting in decrease of blood volume and mean arterial
pressure (MAP) while HCT increased.
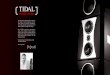
The time-dependent pattern of the oxygen delivery rate
was similar between all classes of hemorrhage and fluid
infusion rates as shown in (Fig. 3) for class II hemorrhage.
Fluid treatment caused a significant increase in oxygen
delivery rates up to a maximum that was lower for higher
bleeding volume (905 mlO2/min, 821 mlO2/min, and 650
mlO2/min for the classes II, III, and IV, respectively).
Interestingly, similar values of maximum delivery rates were
obtained for all three infusion rates, however, higher
infusion rates were associated with earlier appearance of that
maximum. The maximal oxygen delivery rate point was
followed by a continuous decrease which was faster for
higher infusion rates and continued to decrease as long as
fluid was administrated. Following discontinuation of fluid
infusion, there was a second increase in oxygen delivery
rate, which was caused by fluid shifts from the intravascular
into the interstitial compartment and the resulting hematocrit
increase that caused an increase in oxygen delivery.
Changes in oxygen delivery occurred due to changes in
blood flow and Hct. The relative effect of each was studied
to assess the contribution of each parameter in the capillary-
tissue model. Capillary blood flow (Qc) and hematocrit (Hct)
changes during infusion are shown in Fig. 4 for class II
hemorrhage with fluid infusion rate of 80 (ml/min).
Fig. 4 starts at the point in time when hemorrhage was
controlled, hematocrit and capillary flow were decreased to
41.8% and 5.24x10-9 ml/sec, from the original normal
values of 44% and 7.7x10-9 ml/sec, respectively. During
fluid infusion capillary flow was increased while hematocrit
decreased continuously. The final value of hematocrit at the
complete recovery of capillary flow (7.7x10-9 ml/sec) was
35.7% (Fig. 4).
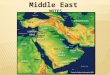
Using the capillary-tissue model, assuming 98%
saturation, a field in a tissue segment was generated for
different values of capillary flow and Hct. The mean value
of oxygen partial pressure in the tissue segment
was calculated for each combination of capillary flow and
blood oxygen content. Fig. 5 shows a contour map where
in a tissue segment is depicted as a function of
capillary flow and Hct.
Figure 4. Effects of infusion on HCT and capillary blood flow. Blood
volume represents the amount remaining after hemorrhage was
controlled plus infused fluid.
Figure 3. Oxygen delivery rate ( ) as a function of time during
bleeding, fluid infusion and following end of infusion for class II
hemorrhage.
197
![Page 3: [IEEE 2014 Middle East Conference on Biomedical Engineering (MECBME) - Doha, Qatar (2014.02.17-2014.02.20)] 2nd Middle East Conference on Biomedical Engineering - Tissue perfusion](https://reader031.pdfslide.us/reader031/viewer/2022020410/5750a7f71a28abcf0cc50749/html5/thumbnails/3.jpg)
Fig. 5 shows that is more sensitive to Hct than to
capillary flow, especially in the low capillary flow and low
Hct values. In the normal range, the line are approximately
at 45 degrees, indicating same sensitivity to the two
parameters.
Combinations of Capillary flow and Hct taken from Fig 4
were marked by black circles in Fig 5. The temporal
direction of this trajectory begins on the right at high values
of Hct and low values of capillary flow as occurs following
hemorrhage and hemorrhage control. The trajectory moves
up and to the left while crossing isobaric lines into lower
levels of oxygen partial pressure. Average partial pressure of
oxygen in the tissue segment decreased continuously from
22.8 mmHg to 21 mmHg during all the course of fluid
replacement as shown by Fig.5.
Fig 6 summarizes the effects of the two parameters on
mean tissue oxygen partial pressure . It shows that
indeed is more sensitive to Hct than it is to flow.
IV. DISCUSSION
Fluid infusion increases blood flow. It is perceived as
restoration of the circulation and that it improves oxygen
delivery to the tissue. According to our study, this is true to a
limited extent. According to our model predictions,
continuing fluid infusion beyond the point of maximum
oxygen delivery will be harmful due to the continuing drop
in . Therefore, based on oxygen delivery rate, restoring
hemodynamic stability should be practiced only during the
increasing phase. During this phase the effect of
increased cardiac output on oxygen delivery is higher than
the deterioration caused by blood dilution. Fluid infusion
should be terminated before this point to maintain the
advantages of fluid therapy on oxygen transport. Looking
deeper into the tissue allows better insight into the actual
oxygen supply t luid therapy indeed seems
to be useful in increasing before the maximum point.
However, analysis of tissue oxygenation during fluid
administration reveals that tissue perfusion is improved only
when blood oxygen concentration is preserved. This is true
with the autoregulation mechanisms that increase blood flow
and maintains hematocrit, and consequently improves tissue
perfusion to vital organs. When crystalloid and colloid fluids
are used they dilute blood and decrease hematocrit.
Consequently, capillary oxygen concentration decreases.
Simulation results showed that the hemodynamic pathway of
hematocrit-capillary flow generated by fluid therapy, causes
a continuous decrease of in tissue. This fact is due to the
sensitivity of oxygen diffusion between capillary and tissue
to oxygen concentration. Therefore, fluid therapy with
solutions that do not include oxygen carrier will restore the
circulation, but without maintaining oxygen partial pressure
in the blood, oxygen supply to the tissue will deteriorate.
V. CONCLUSIONS
Fluid therapy with crystalloid and colloid fluid is useful to
restore hemodynamic stability and increase oxygen delivery
in blood. However, fluid therapy with fluids that do not
include oxygen carriers dilute the blood. This results in
lower oxygen transport to the tissue despite the increase in
blood flow.
VI. REFERENCES
[1] American College of Surgeons, Advanced Trauma Life
Support for Doctors, 8thed, American College of
Surgeons, 2008..
[2] National Institute for Clinical Excellence Excellence
therapy in trauma, issue 2004, National Institute for
Clinical Excellence, 2007.
[3] J. Siam, et al., "Optimization of Oxygen Delivery in
Fluid Resuscitation for Hemorrhagic Shock: A
Figure 5. Mean values of oxygen partial pressure in a tissue segment
for different combinations of capillary flow and Hct. The black circles depict the specific combinations shown in Fig 4 during infusion
following class II hemorrhage.
Figure 6. Effects of Hct and capillary flow on mean oxygen partial pressure of a tissue segment.
198
![Page 4: [IEEE 2014 Middle East Conference on Biomedical Engineering (MECBME) - Doha, Qatar (2014.02.17-2014.02.20)] 2nd Middle East Conference on Biomedical Engineering - Tissue perfusion](https://reader031.pdfslide.us/reader031/viewer/2022020410/5750a7f71a28abcf0cc50749/html5/thumbnails/4.jpg)
Computer Simulation Study" Cardiovascular
Engineering and Technology , Vols.
DOI10.1007/s13239-013-0169-z, 2013.
[4] J. Boldt and C. Ince, "The impact of fluid therapy on
microcirculation and tissue oxygenation in
hypovolemic patients: a review," Intensive Care Med,
vol. 36, p. 1299 1308, 2010.
[5] A. Dubin, et al., "Systemic and microcirculatory
responses to progressive hemorrhage," Intensive Care
Med , vol. 35, p. 556 564, 2009 ..
[6] J. Elmer, et al. "Hemoglobin-based oxygen carriers for
hemorrhagic shock," Resuscitation, vol. 83, pp. 285-
292, 2012.
[7] T. Moschandreou,et al., "Influence of tissue metabolism
and capillary oxygen supply on arteriolar oxygen
transport: A computational model," Mathematical
Biosciences , vol. 232, p. 1 10, 2011.
[8] T. Tatara,et al., "Crystalloid infusion rate during fluid
resuscitation from acute haemorrhage," British Journal
of Anaesthesia , vol. 99, no. 2, p. 212 217, 2007.
[9] P. Perel, et al., "Colloids versus crystalloids for fluid
resuscitation in critically ill patients (Review)," The
Cochrane Collaboration. Published by JohnWiley &
Sons, Ltd., no. Issue 2, 2013.
[10] S. Gundersen, et al., "Mathematical model of NO and
O2 transport in an arteriole facilitated by hemoglobin
based O2 carriers," Biophys. Chem., vol. 143, no. 1,
2009.
[11] H. Santry and H. Alam, "Fluid resuscitation: past,
present, and the future," Shock, vol. 33, pp. 229-241,
2010..
[12] S. Simpson et al., "A computer model of major
haemorrhage and resuscitation," Med. Eng. Phys., vol.
18, no. 4, pp. 339-343, 1996.
[13] C. Gyenge et al., "Transport of fluid and solutes in the
body I.Formulation of a mathematical model," Am J
Physiol Heart Circ Physiol, vol. 277, pp. 215-227,
1999.
[14] C. Gyenge et al., "Transport of fluid and solutes in the
body II. validation and implications," Am J Physiol
Heart Circ Physiol, vol. 277, pp. 1228-1240, 1999.
[15] A. Hedlund et al., "Computer Methods and Programs in
Biomedicine," Elsevier, vol. 27, pp. 7-21, 1988.
[16] Barnea O. and Sheffer N., "A computer model for
analysis of fluid resuscitation," Computers in Biology
and Medicine, vol. 23, no. 6, 1993.
[17] M. Mazzoni et al., "Dynamic fluid redistribution in
hyperosmotic resuscitation of hypovolumic
hemorrhage," AM J Physiol, vol. 255, pp. 629-637,
1988.
[18] N. Safaeian and T. David, "A computational model of
oxygen transport in the cerebrocapillary levels for
normal and pathologic brain function," Journal of
Cerebral Blood Flow & Metabolism, vol. 33, p. 1633
1641, 2013.
[19] C. Beynon, et al., "Brain Tissue Oxygen Monitoring
and Hyperoxic Treatment in Patients with Traumatic
Brain Injury," JOURNAL OF NEUROTRAUMA , vol.
29, p. 2109 2123, 2012.
[20] J. Spires, et al., "Model analysis of the relationship
between intracellular PO2 and energy demand in
skeletal muscle," Am J Physiol Regul Integr Comp
Physiol, vol. 303, pp. 1110-1126, 2012.
[21] D. Goldman, " A mathematical model of oxygen
transport in intact muscle with imposed surface
oscillations," Math. Biosc, vol. 213, 2008..
[22] K. Masamoto and K. Tanishita, "Oxygen transport in
brain tissue," J Biomech Eng , vol. 131, no. 074002,
2009.
[23] D. Goldman, " Theoretical models of microvascular
oxygen transport to tissue," Microcirculation, pp. 15(8):
795-811, 2008.
[24] A. Popel, " Theory of oxygen transport to tissue," Crit
Rev Biomed Eng, pp. 17(3):257-321, 1989.
[25] A. Krogh, " The number and distribution of capillaries
in muscles with calculations of the oxygen pressure
head necessary for supplying the tissue," . J Physiol,,
pp. 52(6):409-15, 1991.
[26] B. McGuire and T. Secomb., " Estimation on capillary
density in human skeletal muscle based on maximal
oxygen consumption rates," Am J. Physiol. Heart Circ.
Physiol., p. 285:2382 2391, 2003.
[27] J. Blum, " Concentration profiles in and around
capillaries," Am J Physiol., pp. 198: 991-998, 1960.
[28] J. Whiteley et al., " Mathematical modelling of oxygen
transport to tissue," J Math Biol, pp. 44(6): 503-522 ,
2002.
[29] D. Reneau et al., "A mathematical simulation of
release, diffusion, and consumption in the capillaries
and tissue of the human brain," Chemical Engineering
in Medicine and Biology, p. 135, 1967.
[30] D. Reneau et al., "A digital simulation of transient
oxygen transport in capillary-tissue systems (cerebral
gray matter). Development of a numerical method for
solution of transport equations describing coupled
convection-diffusion systems," AIChE J, p. 15: 916,
1969.
199