Embed Size (px)
Citation preview
![Page 1: [IEEE 2014 Middle East Conference on Biomedical Engineering (MECBME) - Doha, Qatar (2014.02.17-2014.02.20)] 2nd Middle East Conference on Biomedical Engineering - Accurate automatic](https://reader043.pdfslide.us/reader043/viewer/2022030221/5750a4b01a28abcf0cac479f/html5/page/1.jpg)
Abstract Diagnosis and treatment of sleep disorders
require analysis of the sleep stages and patterns in the
polysomnographic (PSG) signals recorded over several hours.
Traditionally, sleep is monitored based on PSG signals that
require several measurements collected from different locations
on the head and the body. These signals are used to evaluate the
sleep quantity and quality. However, the need for unobtrusive
monitoring and convenience motivates a variety of alternative
approaches focused on the minimization of a number of
monitored physiological signals. Previous studies have shown
that the quantity and length of slow wave sleep (SWS) periods
during sleep are the major indicators of the sleep quality. The
aim of this paper is to present a new automatic method to
detect SWS epochs using a single-channel electro-oculography
(EOG). This method is based on a simple rule based algorithm
with an adaptive method to adjust thresholds. The new method
is evaluated through 9 healthy subjects and the results are
compared to the clinical visual scoring. The agreement of our
detection method for the validation data was 90.0%, the
sensitivity was 90.5% and the specificity was 89.9% and the
kappa value was 0.74.
I. INTRODUCTION
Sleep staging, also known as sleep scoring, consists of collecting overnight polysomnographic (PSG) measurements sleep. These signals are acquired from the patient by the placement of a large number of skin electrodes on various locations on the head and body [1]. Traditionally, these include recording of electroencephalogram (EEG), electromyogram (EMG), electrocardiogram (ECG) and electrooculogram (EOG). The frequency and amplitude of these measures depend on the state of the brain and the body activity among the wakefulness and sleep states. During analysis, the PSG data is usually divided into epochs of 20s or 30s. Then, a well-trained expert visually classifies the different epochs into sleep stages according to the new sleep clinical standard proposed by the American Academy of Sleep Medicine (AASM) [2]. The AASM rules categorize the normal healthy sleep into four states: Movement (MT), Wake (W), NREM (non-Rapid Eye Movements) sleep and REM (Rapid Eye Movements) sleep. The NREM sleep is then classified into three stages (referred to N1 through N3). The stage N3 in AASM is often known as deep sleep or Slow Wave Sleep (SWS). The quantity and length of SWS periods during sleep are the major indicators of sleep quality ( [3],
* Manuscript received October 26th, 2013.
+Mohamed ElMessidi, Sana Tmar-Ben Hamida and Beena Ahmed are
withElectrical and Computer Engineering Department, Texas A & M University, Doha, Qatar (email: {mohamed.elmessidi, sana.tmar,beena.ahmed}@qatar.tamu.edu).
++Thomas Penzel is with Interdisciplinary Center of Sleep Medicine,
Charite University Hospital Berlin, Germany (email: [email protected])
[4]). Previous research papers have demonstrated that SWS plays an important role in cerebral restoration and recovery in humans [5] and [6]. Moreover, low amounts of SWS sleep are highly associated to the risk of diabetes [7] and impaired memory consolidation [8].
Sleep studies in clinical environments are considered to be complicated and uncomfortable for patients and healthy subjects. There is a great interest in developing non-invasive ambulatory sleep monitoring devices for home use. There has been recent interest in reducing the number of skin electrodes and demonstrate that the use for example of only a single EEG channel or two EOG channels [9] can be sufficient to classify epochs into sleep stages or to detect particular events such as the SWS epochs. The paper [10] presents an automatic SWS detection algorithm using two EOG channels with substantial results compared to expert classification
An algorithm for the classification of separate several sleep stages using a single EOG channel has been presented in [11]system but a poor 69.3% sensitivity for SWS detection. The paper [12] discusses a classification method using a single EEG channel. It reports a 0.81, 0.75, and 0.72) for the separate stages (Wake/REM/S1-S2/SWS) respectively. It can be noticed that the poorest result was obtained at SWS classification (0.72).
In this paper we propose a new SWS automatic detection method based on only one electro-oculogram channel. Using only one EOG channel means that only two adhesive skin electrodes would need to be placed at specific locations on the subject's eye and forehead area as recommended by the AASM rules [2]. In addition, we propose an adaptive method to adjust the optimal thresholds used in our algorithm. Our solution explores a simple rule based method to accurately predict the occurrence of slow wave sleep. Several spectral features were analyzed at different spectral bands. The agreement of our detection method for the validation data was 90.0%, the sensitivity was 90.5% and the specificity was 89.9% and the kappa value was 0.74.
The remainder of the paper is organized as follow. In Section II the materials used to evaluate and validate our solution are described. Our SWS detection method is presented in section III. Results are reported in section IV. Lastly, a discussion of the results and conclusions are given in section V.
II. MATERIALS
In order to validate our method, PSG recordings were obtained from the Interdisciplinary Center of Sleep Medicine at Charité University. Nine healthy subjects were admitted in the sleep clinic for 8 hours night of sleep. Subjects were 18 to
-
Mohamed ElMessidi+, Sana Tmar-Ben Hamida+, Beena Ahmed+ and Thomas Penzel++
2014 Middle East Conference on Biomedical Engineering (MECBME)February 17-20, 2014, Hilton Hotel, Doha, Qatar
978-1-4799-4799-7/14/$31.00 ©2014 IEEE 232
![Page 2: [IEEE 2014 Middle East Conference on Biomedical Engineering (MECBME) - Doha, Qatar (2014.02.17-2014.02.20)] 2nd Middle East Conference on Biomedical Engineering - Accurate automatic](https://reader043.pdfslide.us/reader043/viewer/2022030221/5750a4b01a28abcf0cac479f/html5/page/2.jpg)
64 years old. A 24 channel PSG including EEG, EOG, EMG and ECG was collected. In our study we used only one EOG channel, sampled at 200Hz. The sleep scoring was done according to standard AASM [2] rules based on EEG, EOG (left and right) and EMG channels with 30s epoch segmentation. For our study we only used the left EOG channel to distinguish between the SWS epochs and Non-SWS (NSWS) epochs.
III. METHOD DESCRIPTION
Our method consists of four steps: preprocessing, features extraction, classification and smoothing. The aim of the first phase was to detect artifacts, eliminate noise and segment the whole signal into epochs. During the second step, features were extracted from individual epochs of recorded PSG signals. These were then used to identify possible SWS epochs before smoothing to ensure optimal results.
A. Preprocessing
A 50 Hz notch filter was applied to the left EOG, denoted by EOG-L to remove any noise due to the 50 Hz power signal. The signal was divided into 30 s epochs and epochs containing large amplitude levels ( 250 μV) were removed from the acquired data signal. The signal was normalized to eliminate any DC-shift that may have been occurred while recording the data. The EOG-L signal was filtered between 0.5-30Hz using a 7th order Butterworth filter.
B. Features extraction
Each 30-s epoch was segmented into two-second segments with one-second overlap resulting in a total of fifteen segments per epoch of data. At each segment the total power of each segment in the 0.5 30 Hz band was obtained from the power spectral density using the Burg's method [13]. The following characteristic sleep waves were then computed: alpha band (8 12 Hz), beta band (18 30 Hz) and delta band (0.5 4 Hz). The power of these bands for each data segment was obtained from the power spectral density function. A power percentage was then obtained for each of these frequency bands (alpha, beta and delta) relative to the total power of the segment.
Several different features were computed and evaluated prior to the selection of the above key features that are used in this method. These features include various band filtered time signal peak-to-peak features, several other spectral power and activity features and time domain features such as variance and skewness. Histograms of feature activity during SWS and NSWS were used to observe any data trends to aid in classification and thus were the basis for the selection and/or exclusion of the evaluated features.
C. Classification
For each epoch, the quantity of two-second segments with alpha power percentage below an adaptive alpha power threshold ( ), the quantity of two-second segments with beta power percentage below an adaptive beta power threshold ( ) and the quantity of two-second segments above a adaptive delta power threshold ( ) were calculated. These adaptive power percentage thresholds are calibrated automatically on a subject-to-subject basis after analyzing the first ten epochs of sleep. The mean power at
the characteristic frequency bands ( , , ) is compared to predetermined reference power percentages ( , , ) and then each of these three power percentage thresholds is adjusted by a small margin (m) based on the results of that comparison as in (1) X represents alpha, beta or delta power.
)(meanrefrefPwThr
xxmxx (1)
For an epoch to be considered as a potential SWS epoch the quantity of two-second segments contained in an epoch that satisfy the alpha power percentage threshold rule must be below a fixed alpha quantity threshold ( ), the quantity of two-second segments that satisfy the beta power percentage threshold rule must be below a fixed beta quantity threshold ( ) and the number of two-second segments that satisfy the delta power percentage threshold rule must be above a fixed delta power quantity threshold ( ).
D. Smoothing
Only those epochs marked as SWS with at least one adjacent epoch also marked as SWS, were classified as SWS epochs; this prevents any outliers or false positive detection and results in increased system accuracy.
IV. RESULTS
Data from the subjects was separated at random into a testing and a validation group with 5 subjects and 4 subjects respectively in our experiments.
A. Thresholding
All testing epochs that were classified as SWS by the expert analysis were collected together and labeled
to observe any trends in the data and set specific references and thresholds.
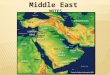
The boxplots in Fig. 1, Fig. 2 and Fig. 3 show the trends of the mean and standard deviation of the total quantity of 2s-segments per epoch at different power percentage intervals. The red line inside each box represents the mean, the box length shows the range of y-axis values and the crosses represent outliers.
The beta power boxplot (Fig. 1) shows only a minimal number of segments per epoch with the presence of beta power during SWS and high number of segments per epoch with beta power at 0-20% percent of the total power during NSWS.
The alpha power boxplot (Fig. 2) shows a high number of segments per epoch (>20) with 0-10% alpha power relative to the total power and smaller quantity of segments per epoch (<5) having 10-20% alpha power during SWS. The quantity of segments per epoch with alpha power varying between the 0%-40% range (relative to the total power) during NSWS on the other hand is less than 20 segments/epoch.
The delta power boxplot (Fig. 3) shows a trend of an increasing quantity of segments per epoch at higher delta power percentages starting at 50% delta power of total power during SWS. However during NSWS, a uniformly low
233
![Page 3: [IEEE 2014 Middle East Conference on Biomedical Engineering (MECBME) - Doha, Qatar (2014.02.17-2014.02.20)] 2nd Middle East Conference on Biomedical Engineering - Accurate automatic](https://reader043.pdfslide.us/reader043/viewer/2022030221/5750a4b01a28abcf0cac479f/html5/page/3.jpg)
number of segments per epoch at almost all delta power percent intervals are present.
Figure 1. Beta power boxplots of (a) SWS and (b) non-SWS epochs
Figure 2. Alpha power boxplots of (a) SWS and (b) NSWS epochs
Figure3. Delta power boxplots of (a) SWS and (b) NSWS epochs
The reference and threshold values for the rules described in section III were modified based on the trends of each feature as observed in the boxplots above to achieve the optimal results for the testing subjects.
B. SWS classification results
The developed algorithm was run on the testing and validation data separately. Sensitivity, specificity, relative observed agreement [15] and values [16] were computed and used to compare the output of
I shows the sensitivity, specificity, agreement and Cohen's kappa values that were obtained and proves the efficiency of the results.
kappa for the validation data subjects were 0.79 and 0.68 respectively. The
kappa result are shown in Fig. 4 and Fig. 5. The red segments show SWS periods correctly marked by the algorithm, the green segments show false positive epoch classification and the purple segments show false negative epoch classification. The algorithm was able to accurately identify continuous periods of SWS but struggled slightly when detecting odd SWS occurrences.
TABLE I. COMPARISON OF ALGORITHIM AND EXPERTS RESULTS
Feature Testing Data
(mean, [range] )
Validation Data
(mean, [range] )
Sensitivity (%) 87.7 , [59.4 - 98.1] 90.5 , [84.4 93.0]
Specificity (%) 91.1 , [86.1 96.8] 89.9 , [88.9 90.7]
Agreement (%) 90.0 , [87.5 95.3] 90.0 , [87.9 91.1]
0.70 , [0.57 - 0.85] 0.74 , [0.68 0.79]
V. DISCUSSION AND CONCLUSIONS
In this study only one electro-oculogram channel (EOG-L) was used to develop an algorithm for the automatic detection of slow wave sleep periods. The automatic classification method features a rule-based algorithm that relies on different adaptive thresholds to detect the occurrence of SWS. This method has the advantage of adapting to different subjects by modifying selection criteria of every individual subject based on his/her average spectral power activity, therefore, ensuring optimal results for every individual sleep subject.
Cohen's kappa was used as the primary measure to show agreement to the expert results as it takes into
account the agreement occurring due to chance [14]. The epoch-by-epoch agreement of our automatic classification method compared to the expert was 90% in
Kappa was 0.70 for the testing subjects and 0.74 for the validation subjects. As a general rule, a kappa coefficient over 0.75 indicates excellent agreement, 0.40 to 0.75 indicates fair to good agreement, and below 0.40 indicates that this agreement is poor [15].
The results obtained by this proposed method show relatively consistency between the testing and validation groups and also the individual subjects in each group; however, there was one subject in particular with expressed an atypical sensitivity value of only 59.4% casing a
results. The reason for this abnormally low sensitivity value was the fact that the subject did not experience any major SWS periods during the entirety his/her sleep hours and had
234
![Page 4: [IEEE 2014 Middle East Conference on Biomedical Engineering (MECBME) - Doha, Qatar (2014.02.17-2014.02.20)] 2nd Middle East Conference on Biomedical Engineering - Accurate automatic](https://reader043.pdfslide.us/reader043/viewer/2022030221/5750a4b01a28abcf0cac479f/html5/page/4.jpg)
only short occurrences of SWS were classified by the expert analysis.
The described system is a part of our project for an accurate ambulatory sleep monitoring for insomnia assessment. We are looking to reduce the number of electrodes required for sleep staging. Using multiple electrodes is inconvenient and uncomfortable for the user, resulting in modified sleep activity different from their normal night of sleep. This study aims to test new methods to simplify the process of sleep staging and reduce the complexity of the sleep monitoring experience.
ACKNOWLEDGMENT
The work was supported by NPRP grant #[5-1327-2-568] from the Qatar National Research Fund which is a member of Qatar Foundation. The statements made herein are solely the responsibility of the authors.
REFERENCES
[1] T. Penzel and R. Conradt, "Computer based sleep recording and analysis," Sleep medicine reviews , vol. 4, no. 2, pp. 131-148, 1 April 2000.
[2] H. Danker-Hopfe et al., "Interrater reliability for sleep scoring according to the Rechtschaffen & Kales and the new AASM standard," Journal of sleep research, vol. 18, no. 1, p. 74 84, 2009.
[3] J. Benington and H. Heller , " Restoration of brain energy metabolism as the function of sleep," Progress in neurobiology, vol. 45:47 60, 1995.
[4] J. Horne, "Human slow wave sleep: a review and appraisal of recent findings, with implications for sleep functions, and psychiatric illness," Experientia, vol. 48, no. 10, pp. 941 954.
[5] -wave sleep (SWS) deprivation and time of night on behavioral performance upon awakening," Physiology and Behavior, vol. 68, no.1-2, pp. 55 61, December 2009.
[6] T. ÅKERSTEDT, K. HUME, D. MINORS and J. WATERHOUS, "The meaning of good sleep: a longitudinal study of polysomnography and subjective sleep quality," Journal of Sleep Research, vol. 3, no. 3, pp. 152 158, 1994.
[7] E. Tasali, R. Leproult, D. Ehrmann and E. Van , "Slow-wave sleep and the risk of type 2 diabetes in humans," Proc. Natl. Acad. Sci. U.S.A.,
vol. 105, no. 3, pp. 1044 1049, Jan. 2008..
[8] D. Aeschbach, . A. J. Cutler and . J. M. Ronda, "A role for non-rapid-eye-movement sleep homeostasis in perceptual learning," The Journal
of Neuroscience, vol. 28(11), pp. 2766-2772, 2008.
[9] S. Tmar-Ben Hamida and B. Ahmed, "Computer based Sleep Staging: Challenges for the future," in 7th IEEE GCC Conference, Doha, Qatar, 2013.
[10] J. Virkkala, J. Hasan, A. Värri, . S. L. Himanen and K. Müller, "Automatic detection of slow wave sleep using two channel electrooculography," Journal of Neuroscience Methods, vol. 160, pp. 171-177, 2007.
[11] J. Virkkala, R. Velin, L. Himanen, A. Värri and K. Müller, "Automatic sleep stage classification using two facial electrodes," in Conference
Proceeding IEEE Eng Med Biol, 2008.
[12] C. e. a. Berthomier, "Automatic Analysis of Single-Channel Sleep EEG: Validation in Healthy Individuals," SLEEP, vol. 30, pp. 1587-1595, 2007.
[13] K. e. a. Roth, "Frequency warped Burg's method for AR-modeling.," in IEEE Workshop on Applications of Signal Processing to Audio and
Acoustics, 2003.
[14] J. Carletta, "Assessing Agreement on Classification Tasks: The Kappa Statistic," Journal Computational Linguistics, vol. 22, no. 2, pp. 249-254, 1996.
[15] L. J. Fleiss, B. Levin and M. Cho Paik, "The Measurement of Interrater Agreement," Statistical methods for rates and proportions,
vol. 3, pp. 212-236, 1981.
235