-
INTERNATIONAL JOURNAL OF LEPROSY^ Volume 62, Number 4
Printed in the U.S.A.
Epidemiologic Characteristics of Leprosy Reactions'David M.
Scollard, Trevor Smith, Lertlakana Bhoopat,
Choti Theetranont, Samreung Rangdaeng, andDavid M. Morens 2
Leprosy reactions are acute emergenciesin the otherwise
generally indolent courseof human infection with
Mycobacteriumleprae, and account for substantial morbid-ity,
hospitalization, and difficulty in clinicalmanagement of leprosy (
2, 22, 24 ) . Two typesof reaction are clinically differentiated:
type1 reactions, often called "reversal reac-tions" (RR), appear as
exacerbations of pre-existing lesions, and arc accompanied
bysystemic symptoms; type 2 reactions, oth-erwise known as erythema
nodosum lepro-sum (ENL), are characterized by the suddenappearance
of crops of tender, erythema-tous nodules in areas of the body that
hadnot necessarily been involved previously(I I. 16) .
Although leprosy reactions have been thesubject of several
clinical and laboratory in-
9, 12 , 14 , 22 , ,vestigations ( 21 ) their etiologies
areunknown and their pathogenesis poorly un-derstood. Several
studies indicate that type1 reactions are associated with
activation ofthe cellular immune system (I. 27, 30, 343 ,) butthe
stimulus for this activation is not known.Type 2 reactions are
generally consideredto be immune complex phenomena ( 32 ),
al-though much evidence suggests that circu-lating complexes are
not responsible (Is. 29 )and available data are consistent with
butdo not convincingly implicate tissue-de-rived complexes ( 4 . 20
).
To learn more about the epidemiology ofleprosy reactions, we
therefore examined
' Received for publication on 30 December 1993;accepted for
publication in revised form on 10 August1994.
= D. M. Scollard, M.D., Ph.D., Laboratory ResearchBranch, GWL
Hansen's Disease Center at LouisianaState University, P. 0. Box
25072, Baton Rouge, LA70894, U.S.A. T. Smith, M.B.B.S., McKean
Rehabil-itation Institute, Chiang Mai, Thailand. L. Bhoopat,M.D.;
C. Theetranont, M.D.; S. Rangdaeng, M.D., De-partment of Pathology,
Faculty of Medicine, ChiangMai University, Chiang Mai, Thailand. D.
M. Morons,M.D., Schools of Medicine and Public Health, Uni-versity
of Hawaii at Manoa, Honolulu, Hawaii, U.S.A.
their occurrence in a longitudinal, prospec-tive study of newly
diagnosed leprosy pa-tients. We sought particularly to
determinewhether temporal variables in the earlycourse of the
disease (including age of onset,duration of illness prior to
reaction, age offirst reaction, etc.) were associated with arisk of
either reaction.
MATERIALS AND METHODSStudy subjects were enrolled from those
patients presenting for initial diagnosis atthe clinics of the
McKean RehabilitationInstitute, Chiang Mai, Thailand. Patientswho
had been previously diagnosed andtreated at other facilities were
excluded; allnewly diagnosed patients were consideredeligible for
study except those occasionalpatients from "hill tribes," for whom
nosuitable translators were available or wholived at great
distances and could not besuitably followed. Patients with
reactions atthe time of diagnosis were included in thestudy.
Otherwise, the outcome endpoint wasconsidered to be the first type
1 or type 2reaction experienced by each patient.
Enrollment began in the fall of 1984 andcontinued until the fall
of 1989. Follow-upcontinued through fall 1992, so that eachpatient
was followed a minimum of 3 years.
Initial histories by both the research teamand the attending
physicians documentedthe patient's year of birth and age at onsetof
first leprosy symptoms. A representativelesion was biopsied in each
patient; eachwas classified as to clinical category of lep-rosy,
according to the five-part scale of Rid-ley and Jopling ( 19),
based on clinical andhistologic criteria.
All patients were given standard multipledrug therapy (MDT): 100
mg dapsone daily,100 mg clofazimine every other day, and1.2 g of
rifampin monthly in two consecu-tive doses (if multibacillary), or
dapsone andrifampin (if paucibacillary). Treatment wasusually
continued until patients were skin-
559
-
• " A...SWAM a% 4
560^ International Journal of Leprosy^ 1994
Female^
Male
50^411^30^20^10^0^
10^20^
30^
40^
50
Number of PatientsChitong N1.11 Study Cohort, 1484-1502
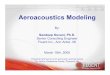
FiG. I . Distribution of reactions among leprosy pa-tients. The
distribution of incident, medically observedreactions is indicated
in the cohort of I7(1 new patientsaccording to sex and leprosy
classification I IN = inde-terminate). Ii = All patients of each
classification inthe cohort: 0 type I reaction: l -= type 2
reaction.
smear negative for multibacillary (MB) pa-tients, and for at
least 6 months for pauci-bacillary (P13) patients. Patients were
seenat regular intervals, usually every 1 or 2months, and were
encouraged to come tothe clinic or hospital if they
experiencedworsening of local or systemic symptoms.
All reactions documented in this studywere severe enough to
warrant hospital ad-mission. An attempt was made to biopsyall
reaction lesions. However, due to thedifferent durations of
reactions before di-agnostic presentation and the lack of uni-form
criteria for histologic diagnosis, diag-nosis of reactions was
ultimately based onthe clinical appearance of characteristic
le-sions of type 1 or type 2 reactions. Type 1reactions were
diagnosed when existing bor-derline lesions became inflamed, i.e.,
ery-thematous, swollen or raised, and tender,
combined with pain and/or tenderness ofinvolved peripheral
nerves. The degree ofsystematic involvement varied, but mosthad
low-grade fever with or without mal-aise. In patients who
originally presentedwithout type 1 reactions, these findings
rep-resented definite changes from the patient'sprevious status.
Type 2 reactions were di-agnosed when small, inflammatory,
red,swollen and highly tender nodules devel-oped suddenly in the
skin or subcutis, ac-companied by fever and malaise. Most ofthese
patients also had a mild leukocytosisand acute neuritis, with one
or more of thefollowing: arthritis, orchitis, iritis, myalgia,and
peripheral edema.
Patients with reactions were given stan-dard treatment with
corticosteroids and/orthalidomide as considered appropriate
inindividual cases by the attending physi-cians, and their MDT
regimen for leprosywas not interrupted. All medication, as wellas
the progression and regression of signsand symptoms, were charted
on flow sheetsespecially designed for the study. Immu-nologic
studies of reactions in the patientsreported here have been
published previ-ousl y (3, 17, 26, 27) .
Statistical comparisons of proportionswere made using the
two-tailed chi-squaredtest with Yates' correction for
continuity.
RESULTSA total of 176 patients were prospectively
enrolled in the study between 1984 and1989. The distribution of
patients by clas-sification of leprosy was as follows: 55 LL,64 BL,
16 BB, 31 BT, 9 TT, and 1 indeter-minate. When this distribution
was furthercategorized by sex (Fig. 1), the preponder-
BI,
BB
BT
TT
IN
TABLE 1. Frequency of occurrence of reactions in leprosy.a
Reaction typeLL 13L 1313 BT All
class.M F Total M F Total M F Total M F Total
Type I (RR) 0 0 0 16 I0 26 2 3 5 3 1 4 35At risk 46 18 64 I0 6
16 25 6 31 111Frequency (%) 35, 56 41 20 50 31 12 17 13 32%
Type 2 (ENL) 23 6 29 11 4 15 0 0 0 0 0 0 44At risk 42 12 54 46
18 64 118Frequency (%) 55 50 54 24 22 23 37%
Data regarding type 1 (RR) and type 2 (ENL) reactions are
presented according to clinical category of leprosyand sex of the
patients from a cohort of 174 new patients seen at McKean
Rehabilitation Institute, Chiang Mai,Thailand, from 1984-1989 and
followed for a minimum of 3 years. No reactions were seen in 1
indeterminateor 9 TT patients.
-
62, 4^ Scollard, et al.: Leprosy Reactions^ 561
TABLE 2. Occurrence of type I (RR) reactions in males and
females, by age at onset ofleprosy.
Decade ofonset ofleprosy
Totalmalesat risk
Totalmales
affected
% Malesaffected
Totalfemalesat risk
Total % Females Total no. Total no.females affected^at
risk^affectedaffectedTotal °/oaffected
1 4 2 50 1 0 — 5 2 402 15 3 20 6 2 33 21 5 243 23 4 17 6 4 67 29
8 284 17 5 29 4 I 25 21 6 295 7 3 43 6 3 50 13 6 466+ 15 4 27 7 4
57 22 8 36
Total 81 21 26 30 14 47 111 35 32
ance of males and of MB patients is evident,as previously
documented in this popula-tion. One patient in our cohort, a
28-year-old male with LL disease, died soon afterdiagnosis of an
apparent dapsonc reaction,and he is not included in the
calculations ofthe incidence of leprosy reactions since theduration
of follow up was only a few months.None of the remaining 175
patients was lostto follow up during the study.
The study cohort equalled 45% (176) ofthe 388 new, untreated
patients registeredat McKean during the study interval, in-cluding
79% of 171 MB (LL-BB) patientsand 32% of 97 BT patients.
Twenty-threeof the new patients at McKean were inde-terminate, of
whom one was enrolled in ourstudy. This sample thus may
underestimatereactions in BT patients, but approximatesthe total
population of new MB patients inthis population, whose greater
acceptanceof a brief hospital admission (for relatedimmunologic
studies) may have led to in-creased enrollment. Despite the
differentproportions of study volunteers in eachgroup, a review of
medical records of par-
TABLE 3. Frequency of occurrence of type2 (ENL) reactions by age
at onset of leprosy.
Decade of onsetof leprosy
No.affected
Totalat risk
Affectedper onsetdecade
1 0 3 012 17 71
3 12 36 334 12 24 505 5 16 316 3 13 23
>6 0 9 0Total 44 118 37
ticipating and non-participating patients ineach clinical group
revealed no differencesin age, gender, occupation, area of
resi-dence, or severity of leprosy, except for pa-tients excluded
because of inaccessibility tofollow up.
Of the 175 patients followed, 79 (45%)developed one or more
reaction; 35 devel-oped type 1 reactions and 44 developed type2
reactions. Two patients developed bothtype 1 and type 2 reactions.
Two additionalpatients who developed severe neuritis notassociated
with typical reaction skin lesionswere excluded from analysis
because the ba-sis for their neuritis could not be
clearlydetermined.
The incidence of reactions in this cohortof new patients,
unadjusted for duration offollow up, indicates the association of
type1 reactions with borderline patients, and of
20
S 15
toLri
:
09-14^15-19^20-29^30-39^40-49^50-59^>59
Age at Onset of Leprosy
FIG. 2. Mean duration of leprosy before diagnosisand treatment
(MDT). The duration of leprosy (in years)was determined by careful
history at the time of di-agnosis; MDT was initiated at diagnosis.
Dates areshown according to age at onset of leprosy. patients who
developed ENL; --- = patients who didnot develop ENL. The two
curves are not statisticallydifferent.
-
562^ International Journal of Leprosy^ 1994
TABLE 4. Incidence of type 2 (ENL) reactions, by age of leprosy
onset and duration ofleprosy before and after initiation of
treatment, per 100 person-years.
Age at leprosyonset No.
Person-^No.^Inci-^Person-^No.^Inci-years ENL dence years type 2
dence
leprosy cases of type 2 followed reaction type 2pre-Rx' pre-Rxh
pre-Rx post-Rxc post-Rx post-Rx
Totalperson- Totalyears type 2
followed
Totalinci-
dencetype
2/100person-years
9-14 8 103 0 41.1 1 2.4 144.1 1 0.715-19 12 51 4 7.8 58.7 7 11.9
109.7 11 10.0
Total, 9-19 20 154 4 2.6 98.8 8 8.1 253.8 12 4.7
20-29 36 160 3 1.9 165.0 9 5.5 325.0 12 3.730-39 24 97 7 7.2
132.1 5 3.8 229.1 12 5.240-49 16 37 0 78.3 5 6.4 110.3 5 4.550+ 22
43 0 119.8 3 2.5 162.8 3 1.8
Total, 20+ 98 337 10 3.0 490.2 22 4.5 827.2 32 3.9
Person-years of leprosy pretreatment is defined as the number of
individuals multiplied by the number ofyears during which they had
leprosy before treatment.
h Type 2 reaction pretreatment refers to observed reactions in
patients at the first presentation to the clinic,i.e., those who
had a reaction before they received treatment.
Post-Rx refers to the time after initiation of treatment."
Number of patients with at least one type 2 reaction.
type 2 reactions with LL and I3L patients(Table 1). Thirty-two
percent of patients atrisk for type 1 reactions (i.e., borderline
pa-tients, BL-BB-BT) developed this reaction,and 37% of patients at
risk for type 2 re-actions (i.e., MB patients, LL and BL)
de-veloped this reaction.
Also noteworthy is the greater risk fortype 1 reactions in
female patients, 47% vs26% overall, which appears independent
ofclinical category (Table 1). Analysis of thefrequency of type 1
reactions by age at onsetof leprosy shows that the increased
occur-rence is seen in women with onset ofleprosyat all ages (Table
2). These findings were notconfounded by duration of leprosy prior
todiagnosis (data not shown).
The development of type 2 reactions ap-pears to be predicted by
the age of onset ofleprosy rather than by patient age at the timeof
the reaction (Table 3). Unadjusted forduration of follow up,
patients whose firstsymptom occurred during adolescence hada much
greater frequency (71%) of experi-encing a type 2 reaction than
patients whoseonset of leprosy occurred after adolescence(p
-
62, 4^ Scollard, et al.: Leprosy Reactions^ 563
no evidence that treatment either protectsor precipitates type 2
reactions in patientsat risk.
Recurrence of type 1 and type 2 reactionsfollowed different
patterns. The majority ofpatients (34/44) with type 2 reactions
hadmultiple episodes of reaction, while only aminority of patients
(11/25) with type 1 re-actions had multiple episodes (Table 5).
Thisdifference was statistically significant (p
-
564^ International Journal of Leprosy^ 1994
mative if interpreted in the light of a pos-sible endocrine
influence on either systemicor dermal immune mechanisms ( 2 ').
An-other possibility is that the mechanisms in-volved in type 1
reactions may share somecommon determinants with other autoim-mune
phenomena to which women are pre-disposed ( 31 ).
The observation that type 1 reactions typ-ically occur only once
(or a very few times)suggests that in each individual only a
lim-ited degree of "adjustment" in the immuneresponse to M. leprae
can take place. If so,the permissible range of such change mightbe
determined or limited by genetic or im-munologic factors which can
be examinedin future studies.
The most interesting observation con-cerning type 2 reactions in
this study is theapparently increased frequency of these re-actions
in individuals whose onset of lep-rosy symptoms occur before
adulthood.Other studies have noted that type 2 reac-tions are more
often seen in patients be-tween 20 and 40 years old ( 6 ' 25 ), but
theassociation with onset of leprosy in adoles-cence previously has
not been noted. Anyhypothesis to explain this observation
mustaccount for the fact that type 2 reactionsoccur after a
variable duration of 4 monthsto 3 or more years after the onset of
leprosy.If the later occurrence of type 2 reactions isrelated to
onset during adolescence, the ini-tiating events must take a long
and variabletime to become manifest.
Davey and Schenk ( 7 ) long ago cited stud-ies noting that
puberty is associated withincreased risk of relapse of leprosy and
ofthe development of lepromin sensitivity.The association of
puberty with increasedsusceptibility to and mortality from
tuber-culosis is also well documented ("), as isthe increase in the
incidence of systemiclupus erythematosus in the decade follow-ing
puberty ( 3 '). These clinical and epide-miologic phenomena remain
unexplained.Neuroendocrine-immune interactions haverecently
attracted interest ( 8 . 2 '), as have theirpossible effects on
immunity to mycobac-teria (33 ), and the effects of
infection-in-duced cytokines on neuroendocrine func-tion (23, 28,
33 , .) The possible role(s) of thechanges at puberty have not
received asmuch attention, however, as the more ob-
vious mechanisms related to adrenal func-tion.
In addition to the major endocrinechanges that occur in both
sexes during pu-berty, this also may be an important phasein the
maturation of the immune system.This has not been the subject of
substantialresearch, however, and little is known aboutit beyond
the oft-repeated maxim that thefunction of the immune system
"peaks"around the time of puberty ( 1 "). Our datado not provide a
basis to select from anendocrine or an immune-maturation
hy-pothesis in explaining the pathogenesis ofENL, but suggest that
further studies of ENLshould consider both possibilities.
The characteristics of both type 1 and type2 reactions
identified in this study may as-sist in distinguishing between
them: type 1reactions occurred predominantly in wom-en who had
onset at all ages, and type 2reactions were more common in males
andfemales who had leprosy onset in adoles-cence. Future studies of
immunologic pa-rameters of these reactions may benefit fromthe
stratification of data by sex and age ofonset of leprosy in
addition to the routineclassification of results by leprosy
classifi-cation.
SUMMARYAn 8-year prospective study of a cohort
of 176 newly diagnosed leprosy patients wasconducted to examine
the possible influenceof age, sex, multidrug therapy (MDT),
andduration of illness on the risk of either type1 or type 2
reactions. Patients were enrolledover a 5-year period (1984-1989)
and fol-lowed for a minimum of 3 years. All reac-tions studied were
severe enough to warranthospital admission. Overall, 45% of this
co-hort developed a reaction; 32% of patientsconsidered at risk
developed type 1 reac-tions, and 37% of patients considered at
riskdeveloped type 2 reactions. Despite the pre-dominance of men
among the leprosy pa-tients, type 1 reactions occurred with
sig-nificantly greater frequency in women, anddid not appear to be
influenced by age ofonset of leprosy. Individuals experiencingone
type 1 reaction were not likely to ex-perience a recurrence,
suggesting that theimmunologic mechanisms of this reaction
-
62, 4^ Scollard, et al.: Leprosy Reactions^ 565
may be limited or regulated by genetic orimmunologic
factors.
Type 2 reactions, on the other hand, oc-curred with equal
frequency in both malesand females, but were highly associated
withonset of leprosy in the second decade of life.Individuals who
experienced type 2 reac-tions often had one or more recurrence
ofthe reaction. No increased risk was seen foreither reaction with
longer duration of lep-rosy or longer duration of treatment.
Themechanisms by which these differences re-late to the
pathogenesis of leprosy reactionsremains unclear, but future
studies of clin-ical and immunological parameters of lep-rosy
reactions may benefit from stratifica-tion of data by gender and
age of onset ofleprosy in addition to the routine groupingof
results by leprosy classification.
RESUMENSe hizo un estudio prospcctivo en un grupo de 176
pacientes con lepra rccien diagnosticada apra examinar
la influencia de la edad, el sex°, el tratamiento
conpoliquimioterapia (PQT) y la duraciOn de Ia enfer-
medad, en el desarrollo de reacciones leprosas de lostipos I 6
2. Los pacicntes se cnrolaron en el estudio alo largo de 5 atios
(1984-1989) y se estudiaron duranteun periodo minimo de 3 aims.
Todas las rcaccioncs
leprosas estudiadas fucron lo suficientemente severas
como para justificar la hospitalizaciOn de los pacientes.El 45%
de los pacientes desarrollaron algUn tipo de
reacciOn; 32% de los pacientcs considerados en riesgo
desarrollaron rcaccioncs del tipo I, y 37%, reaccionesdel tipo
2. No obstantc el predominio de hombres en
el grupo de pacientes, las rcaccioncs de tipo 1 fucron
mas frecuentes entre las mujeres. Las rcaccioncs noestuvieron
asociadas con la edad de apariciOn de Ia
cnfermedad. Los individuos con reacciOn de tipo I nofucron
propensos a experimentar rccaidas, sugiricndo
que los mecanismos inmunolOgicos de esta reacciOn
pueden estar sujetos a regulaciOn por factorcs geneticoso
inmunolOgicos.
Por otro lado, las reacciones de tipo 2 ocurricron
con igual frecuencia tanto en hombres como en mu-
jeres, pero fucron inns frecuentes en los casos dondcla
enfermedad apareciO en Ia scgunda decada de la vida.
Los individuos que desarrollaron reacciones de tipo 2,
frecuentemente presentaron una o mAs recurrenciasrcaccionales.
El riesgo de apariciOn de Ia reacciOn Ic-prosa no cstuvo asociado
ni con una mayor duraciOnde la enfermedad, ni con un mayor tiempo
de trata-
micnto de Ia misma.
Los mecanismos de relaciOn entre las rcaccioncs le-prosas y los
parAmetros analizados permanecen obs-
curos, pero los cstudios clinicos c inmunolOgicos de las
reacciones leprosas, podrian, en un futuro, bcneficiarse
si los datos se presentaran en forma estratificada en
funciOn del sexo del paciente y de Ia edad de apariciOnde la
enfermedad.
RÉSUMÉ
Une etude prospective d'une duree de 8 ans dune
cohorte de 176 malades de la lepre nouvellemcnt dia-
gnostiques a Le realisee pour etudier l'influence pos-sible de
Page, du sexc, de Ia polychimiotherapie (PCT)
et de Ia duree de Ia maladie sur lc risque de developperdes
reactions de type I ou de type 2. Les patients ont
etc enroles dans ('etude au cours d'une periode de 5ans
(1984-1989) et suivis pour un minimum de 3 ans.
Toutes les reactions etudiees &talent suffisamment se-vexes
pour meriter l'hospitalisation. Au total, 45% des
patients de cette cohorte ont developpe unc reaction;32°h des
patients consideres a risque ont devcloppe
unc reaction de type 1 et 37% des patients consideres
A risque une reaction de type 2. En &pit de la pre-
dominance masculine parmi les malades de la lepre,les reactions
de type 1 sont apparues avec une frê-
quence significativement plus elevec chez les femmes,
et nc paraissaicnt pas etre influencees par l'Age a
l'ac-quisition de Ia lepre. Les personnes chez qui survenait
une reaction de type I avaient pcu de risque de pre-senter une
recidive, ce qui suggere que les mecanismes
immunologiques de cette reaction pcuvent etre limites
ou controlês par des facteurs genetiques ou immuno-logiques.
Les rections de type 2 apparaissaient, quant A elks
avec unc frequence semblable chez les hommes et les
femmes, mais it y avait unc forte relation avec lc
de-veloppement de la lepre au cours do la deuxieme de-
cennie de vie. Les personnes qui avaient Cu une reac-tion de
type 2 avaient souvent unc ou plusieurs recidivesde la reaction. On
n'a pas observe d'augmentation du
risque d'aucun des types de reaction pour une lepre delongue
duree ou un traitement de longue duree. Les
mecanismes par lesquels ces differences sont reliCes
la pathogenese des reactions lepreuses reste peu Clair,mais des
etudes futures de parametres cliniques et im-
munologiques des reactions lépreuses pourraient be-neficier de
Ia stratification des donnOes par sexc et age
A ('acquisition de Ia lepre, en plus du groupement ha-
bitue' des resultats scion le type de lepre.
ACKNOWLEDGMENTWe arc indebted to the nursing and technical
staff
of McKean Rehabilitation Institute for their generous
cooperation and excellent patient care, and to the staffof the
Research Institute for Health Sciences, ChiangMai University,
Chiang Mai, Thailand, for providing
years of technical and administrative support. These
studies were supported by grants from USAID and by
a Research Strengthening Grant from the World Health
Organization.
-
566^ International Journal of Leprosy^ 1994
REFERENCES
1. BARNETSON, R. ST.C., 13JuNE, G., PEARSON, J. M.H.
and KRONVALL, G. Cell-mediated and humoral
immunity in "reversal reactions". Int. J. Lepr. 44(1976)
267-274.
2. BECX-BLEUMINK, M. and BERHE, D. Occurrence
of reactions, their diagnosis and management inleprosy patients
treated with multidrug therapy;
experience in the leprosy control program of theAll Africa
Leprosy and Rehabilitation Training
Center (ALERT) in Ethiopia. Int. J. Lepr. 60 (1992)173-184.
3. BH(X)PAT, L., SCOLLARD, D.M., THEETRANONT, C.,
CHIEWCHANVIT, S., NELSON, D.L. and UTAIPAT, U.
Studies of human leprosy lesions in situ using suc-tion-induced
blisters: cell changes with 1gM anti-
body to PGL-1 and interlcukin-2 receptor in clin-
ical subgroups of erythema nodosum leprosum.Asian Pacific J.
Allergy Immunol. 9 (1991) 107-
119.4. BJORVATN, B., BARNETSON, R.ST.C., KRONVALL,
G., ZUMER, R.H. and LAMBERT, P.H. Immune
complexes and complement hypercatabolism inpatients with
leprosy. Clin. Exp. Immunol. 26
(1976) 388-396.5. BROWN, D.11., SHERIDAN, J., PEARL, D. and
ZWIL-
LIG, B.S. Regulation of mycobactcrial growth by
the hypothalamus-pituitary-adrenal axis: differ-
ential responses of Al. bolls BCG-resistant and-
susceptible mice. Infect. Immun. 61 (1993) 4793-
4800.
6. CHOPRA, N.K., AGRAWAL, J.S. and PANDYA, P.G.
Reactions in leprosy; a study of 250 patients in amultidrug
therapy project, I3aroda District, Gu-
jarat, India. Int. J. Dermatol. 29 (1990) 490-493.
7. DAVEY, T.F. and SCHENCK, R.R. The endocrines
in leprosy." In: Leprosy in Theory and Practice.Cochrane, R.G.
and Davey, T.F. Bristol: John
Wright & Sons, 1964, pp. 190-204.8. EPSTEIN, F.H.
Neuroendocrine-immune interac-
tions. N. Engl. J. Med. 329 (1993) 1246-1253.
9. GROENEN, G., JANSSENS, L., KAYEMBE, T., NOLLET,E., COUSSENS,
L. and PATTYN, S. Prospective study
on the relationship between intensive bactericidaltherapy and
leprosy reactions. Int. J. Lcpr. 54 (1986)236-244.
10. HIROKAWA, K., UTSUYAMA, M., KASAI, M. andKURASHIMA, C. Aging
and immunity. Acta Path-ol. Jpn. 42 (1993) 537-548.
11. JOPLING, W.H. Leprosy reactions. In: handbookof Leprosy.
London: Heinemann Medical Books,1971, p. 42.
12. LOCKWOOD, D.N.J., VINAYAKUMAR, S., STANLEY,J.N.A., McADAm,
K.P.W.J. and COLSTON, M.J.
Clinical features and outcome of reversal (type 1)reactions in
Hyderabad, India. Int. J. Lepr. 61(1993) 8-15.
13. MODLIN, R.L., GERHARD, F., TAYLOR, C.R. and
REA, T. H. In situ characterization of T lympho-cyte subsets in
the reactional states of leprosy. Clin.Exp. Immunol. 53 (1983)
17-24.
14. NAAPS, B. and WHEATE, H.W. The time intervalbetween the
start of anti-leprosy treatment and the
development of reactions in borderline patients.Lepr. Rev. 49
(1978) 153-157.
15. NG, W.L., SCOLLARD, D.M. and Hun, A. Glom-erulonephritis in
leprosy: case report and reviewof the literature. Am. J. Clin.
Pathol. 76 (1981)67-75.
16. PFALTZGRAFF, R.E. and BRYCESON, A.B. ClinicalLeprosy. In:
Leprosy. Hastings, R. C., ed. NewYork: Churchill Livingstone, 1985,
pp. 134-176.
17. RANGDAENG, S., SCOLLARD, D.M., SURIYANON, V.,SMITH, T.,
THAMPRASERT, K. and THEETRANONT,C. Studies of human leprosy lesions
in situ usingsuction-induced blisters. I. Cellular componentsof
new, uncomplicated lesions. Int. J. Lepr. 57(1989) 492-498.
18. RICH , A.R. Tlu' Pathogenesis of Tuberculosis.Springfield,
Illinois: Charles C. Thomas, 1951, p.237 ff.
19. RIDLEY, D.S. and JOPLING, W.H. Classification ofleprosy
according to immunity; a five-group sys-
tem. Int. J. Lepr. 34 (1966) 255-273.20. RIDLEY, M. and RIDLEY,
D.S. The immunopath-
ology of erythema nodosum leprosum: the role ofextravascular
complexes. Lepr. Rev. 54 (1983) 95-107.
21. ROOK, G.A.W., HERNANDEZ-PANDO, R. and LI-GHTmAN, S.L.
Hormones, peripherally activatedprohormones, and regulation of the
Th I /1 -112 bal-ance. Immunol. Today 15 (1984) 301-303.
ROSE, P. and WATERS, M.F.R. Reversal reactionsin leprosy and
their management. Lepr. Rev. 62(1991) 113-121.
23. SAPOLSKY, R., RIVIER, C., YAMAMOTO, G., PLOTSKY,P. and VALE,
W. Interleukin-1 stimulates the se-cretion of hypothalamic
corticotropin-releasing
factor. Science 238 (1987) 522-524.24. SEHGAL, V.N. Reactions in
leprosy; clinical as-
pects. Int. J. Dermatol. 26 (1987) 278-285.
25. SEHGAL, V.N., and SHARMA, V. Reactions in lep-rosy-a
prospective study of clinical, bacteriolog-
ical, immunological, and histopathological pa-rameters in
thirty-five Indians. J. Dermatol. 15(1988) 412-419.
26. SCOLLARD, D.M., BHOOPAT, L., KESTENS, L.,VANHAM, G.,
DOUGLAS, J.T. and MOAD, J. Im-mune complexes and antibody levels in
blistersover human leprosy skin lesions with or without
erythema nodosum leprosum. Clin. Immunol. Im-munopathol. 63
(1992) 230-236.
27. SCOLLARD, D.M., SURIYANON, V., BHOOPAT, L.,WAGNER, D.K.,
SMITH, T., THAMPRASERT, K.,NELSON, D. and THEETRANONT, C. Studies
of hu-
-
62, 4^ Scollard, et al.: Leprosy Reactions^ 567
man leprosy lesions in situ using suction-inducedblisters. 2.
Cell changes and soluble interleukin-2receptor (tac peptide) in
reversal reactions. Int. J.Lcpr. 58 (1990) 469-479.
28. TRACY, K.J. and CERAMI, A. Metabolic responsesto
cachectin/TNF: a brief review. Ann. N.Y.Acad. Sci. 587 (1990)
325-331.
29. TUNG, K.S.K., KIM, B., BJORVATN, B., KRONVALL,G., MCLAREN,
L.C. and WILLIAMS, R.C. Discrep-ancy between Clq deviation and Raji
cell tests indetection of circulating immune complexes in pa-tients
with leprosy. J. Infect. Dis. 136 (1977) 216-221.
30. TUNG, K.S.K., UMLAND, E., MATZNER, P., NELSON,K., SCHAUF,
V., RUBIN, L., WAGNER, D., SCOLLARD,D., VITHAYASAI, P., VITHAYASAI,
V., WOROBEC, S.and SMITH, T. Soluble serum interleukin-2 recep-tor
levels in leprosy patients. Clin. Exp. Immunol.69 (1987) 10-15.
31. WALLACE, D.J., HAHN, B.H., QUISMORO, F.P., JR.,and
KLINENBERG, J. R., EDS. Dubois' Lupus Er-ytheinutosus. 4th edn.
Philadelphia: Lea & Febi-ger, 1993.
32. WEMAMBU, S.N.C., TURK, J.L., WATERS, M.F.R.and REES, R.J.W.
Erythema nodosum leprosum:a clinical manifestation of the Arthus
phenome-non. Lancet 2 (1969) 933-935.
33. WOLOSKI, B.M.R.N.J., SMITH, E.M., MEYER, W.J.,III, FULLER,
G.M. and BLALOCK, J.E. Corticotro-pin-releasing activity of
monokines. Science 230(1985) 1035-1037.
34. YAMAMURA, M., UYEMURA, K., DEANS, R.J., WE-INBERG, K., REA,
T.H., BLOOM, B.R. and MODLIN,R.L. Defining protective responses to
infectiouspathogens: cytokine profiles in leprosy lesions. Sci-ence
254 (1991) 277.
Page 1Page 2Page 3Page 4Page 5Page 6Page 7Page 8Page 9












![LNL Introduction Course v5[1].2](https://img.pdfslide.us/doc/110x75/577cc9f31a28aba711a50766/lnl-introduction-course-v512.jpg)