Embed Size (px)
Citation preview

INTERNATIONAL JOURNAL OF LEPROSY Volume 63, Number IPrinted in the U.S.A.
Minocycline in Lepromatous Leprosy'Tranquilino T. Fajardo, Jr., Laarni G. Villahermosa,
Eduardo C. dela Cruz, Rodolfo M. Abalos,Scott G. Franzblau, and Gerald P. Walsh 2
Multidrug therapy (MDT) is the recom-mended treatment for leprosy to minimizeemergence of drug resistant strains of My-cobacterium leprac (14• 22 ) . The developmentof MDT was prompted by the marked in-crease in dapsone resistance in patients re-ceiving dapsone monotherapy. CurrentWorld Health Organization (WHO)/MDTfor multibacillary (MB) leprosy utilizes acombination of rifampin, dapsone and clo-fazimine (22). Of the three drugs, only rif-ampin is rapidly bactericidal. However, M.leprac strains resistant to rifampin ( 13 ), andpossibly to clofazimine (21 ), have been re-ported. Lapses in compliance, which arc es-pecially a problem with the treatment du-rations required for leprosy, certainly con-tribute to treatment failure and relapse and,more importantly, to the development ofbacterial resistance. The use of two or morerapidly bactericidal drugs in combinationshould shorten the duration of treatmentand minimize compliance problems. Thus,there is a need for new, rapidly bactericidaldrugs for the treatment of leprosy.
Recently, minocycline, an alkylated ami-no-tetracycline, widely used for bacterial in-fections and safely used for the long-termtherapy of acne vulgaris, has been shown tohave bactericidal activity against M. lepraein mice at dietary doses of 0.02%-0.04%.These doses give a minimum inhibitoryconcentration (MIC) for M. leprac of < 0.2mom' (9. 10. 16) which is very much lower than
' Received for publication on 25 May 1994; acceptedfor publication in revised form on 30 August 1994.
2 T. T. Fajardo, Jr., M.D., M.P.H., Senior ClinicalConsultant; L. G. Villahermosa, M.D., Acting Chief,Clinical Research Branch; E. C. dela Cruz, D.V.M.,Chief, Vivarium; R. M. Abalos, M.D., Pathologist; G.P. Walsh, Ph.D., Scientific Director, Leonard WoodMemorial Center, P. O. Box 727, Cebu City, The Phil-ippines. S. G. Franzblau, Ph.D., Chief, PharmacologyResearch Department, Laboratory Research Branch,GWL Long Hansen's Disease Center at Louisiana StateUniversity, P. O. Box 25072, Baton Rouge, Louisiana,U.S.A.
plasma levels of 2-4 /./g/m1 easily achieva-ble in humans with doses of 100 mg 2 xdaily (''). Furthermore, in vitro studies( 5, 8 ' 18 ) also have shown that minocyclineinhibited the metabolic activity of Al. lep-rac. In human leprosy, minocycline at 100mg/day for 3 months showed remarkableresults (I I. 15 ).
We evaluated minocycline therapy for 6months with three different dose levels dur-ing the first month. Drug efficacy was mea-sured by clinical changes as well as changesin the bacterial index (BI) and histopathol-ogy. Antibacterial effects were evaluated bydetermination of the viability of M. lepracin the mouse foot pad and palmitic acidoxidation assays, both being performed onthe same biopsy suspensions to permit acomparison of these assays. In some pa-tients, determination of serum phenolic gly-colipid I (PGL-I) antigen also was per-formed at the time of the biopsies. Mostviability assays were done during the firstmonth of therapy to determine how quicklyand which dosage levels would be most ef-fective. Palmitic acid oxidation studies weredone at the Leonard Wood Memorial Lep-rosy Research Center, Cebu, The Philip-pines, and at the G.W. Long Hansen's Dis-ease Center, Louisiana, U.S.A. Adverse drugeffects, intolerance, and the occurrence oflepra reactions were monitored.
METHODOLOGYA total of 14 lepromatous or near lep-
romatous (13 LL and 1 BL) patients, 8 males(average age 27.4 years) and 6 females (av-erage age 22.2 years), were sequentially ad-mitted to the study. Of these, 10 were new,previously untreated patients and 4 werepreviously treated, relapsed patients. In thelatter group, no active antileprosy treatmenthad been taken for at least 2 years beforeadmission to the study.
Minocycline was administered in the fol-lowing regimens: (A) 200 mg daily for 30
8

63, 1^Fajardo, et al.: Minocycline Clinical Trial^ 9
days, followed by 100 mg daily for another5 months in 4 patients; (B) 100 mg daily for30 days, followed by 100 mg daily for 5months in 8 patients; (C) 100 mg daily ondays 1, 2, 3 during the first 2 weeks, andanother dosaging with 100 mg daily on days15, 16 and 17 during the second 2 weeks,followed by 100 mg/day for 5 months in 2patients.
All the patients would be treated withstandard WHO/MDT for MB leprosy ( 10 )after completing 6 months of minocyclinemonotherapy.
Informed consent was obtained and med-ical and laboratory clearances were per-formed before admission to the trial. Lab-oratory examinations included a completehematologic examination, routine urinaly-sis and stool examinations; liver and kidneyprofile studies also were performed. All ex-aminations were repeated at the end of thestudy, and during the study period whenindicated.
Treatment was fully supervised for 10 pa-tients admitted to the Eversley Childs San-itarium. For the 4 who were outpatients, thedrug was given as a weekly supply.
Clinical, bacteriological and histologicalexaminations were performed followingstandard procedures established at the Cen-ter (Standard protocol for trials of combineddrug regimens among lepromatous patients.Report of the first meeting of the THELEPScientific Working Group, Geneva, 25-29April 1977. TDR/SWG-THELEP (1)/77.3).Detailed clinical dermatologic/neurologicexaminations were performed at prethera-py, day 28, and at the end of 6 months.Inpatients were seen daily during super-vised drug administration; outpatients wereseen weekly when they came for their med-icines. Clinical changes and the occurrenceof lepra reactions or adverse drug effectsalso were monitored at this time.
Bacteriologic skin smears were taken fromsix skin sites before treatment and at theend of 6 months. Skin biopsies for histo-pathology, mouse foot pad inoculation, andpalmitic acid oxidation studies were takenat pretherapy from skin sites having thegreatest number of acid-fast bacilli (AFB).Subsequent biopsies were taken adjacent tothe original biopsy sites or from lesions withsimilar characteristics as those of the biop-sied pretherapy lesions. Suspensions pre-
pared from the same biopsy were used forthe mouse foot pad inoculation and pal-mitic acid oxidation assay to permit com-parative studies of the two procedures. His-tologic evaluation for changes in the gran-uloma and the logarithmic index of acid-fast bacilli in biopsies (LIB) ( 19) were per-formed by comparing pretreatment histol-ogy and histology at 6 months.
Mouse foot pad viability studies weredone as previously described using theShepard technique (20s.) M. leprae suspen-sions from biopsies taken at pretherapy andat various intervals during the treatment pe-riod were inoculated into both hind footpads of inbred CBA mice. Five thousandAFB were inoculated per foot pad. Mostinoculations were done during the firstmonth of treatment (days 3, 7, 10, 14, 21,30) and then at day 180 (at 6 months). Foreach patient, 15 mice were used for pre-treatment biopsy specimens (control), while20 were used for isolates taken during treat-ment and at the end of 6 months. Harvestswere performed 8-12 months after inocu-lation. AFB in the foot pads of individualmice were counted, and a 20-fold increasein the AFB count was considered positivegrowth.
Radiorespirometric studies were con-ducted by a slight modification of a previ-ously described procedure ('). From eachbiopsy, for mouse foot pad inoculation, partof the remaining bacillary suspension wastransferred to a sterile microfuge tube andcentrifuged at 9430 x g x 10 min at 10°C.The supernatant was discarded and the ba-cilli suspended in 1 ml Middlebrook 7H12medium adjusted to pH 5.8 (with citric acid).The number of bacilli was determined mi-croscopically. Part of the suspension waskilled by immersion in a boiling-water bathfor 10 min. Aliquots of 1 x 10 6 AFB wereadded to 6-ml screw-cap vials ("shorty vi-als;" Wheaton Scientific, Milleville, NewJersey, U.S.A.) containing 1 ml 7H12 me-dium, pH 5.8, containing 50 pg/m1 ampi-cillin and 5 pg/mlamphotericin B. One mi-crocurie of [1-14]C-palmitic acid (57 mCi/mmole; New England Nuclear Corp., Bos-ton, Massachusetts, U.S.A.) was added toeach vial in a volume of 10 pl. Vials wereplaced with loose caps within wide-mouthscintillation vials (Poly-Q; Beckman Instru-ments, Fullerton, California. U.S.A.) con-

10^ International Journal of Leprosy^ 1995
TABLE 1. Pretherapy characteristics of patient population and minocycline dose.
Name Age/sexDis.dur.(Yr.)
Clin.diagnosis
Histo.diagnosis
Avg.BI Minocycline dose
New untreatedLN 15/F 8 LL LLp 4.8 Intermittent'QE 23/M 1.5 LL LLp 4.3 100 mg/day x 6 mos.CL I3/F LL LLs 5.0 Intermittent'IC" 19/F 3 LL LLs 5.0 200 mg/day x 1 mo.
100 mg/day x 5 mos.EL 27/F 1 LL LLs 5.5 100 mg/day x 6 mos.BJ 27/M 3 LL LLp 4.8 100 mg/day x 6 mos.TP 15/M LL LLs 5.0 100 mg/day x 6 mos.CF I4/M 3 LL LLs 5.0 100 mg/day x 6 mos.FS 19/M 5 LL LLs 5.0 200 mg/day x 1 mo.
100 mg/day x 5 mos.FM 21/F LL BL 4.5 200 mg/day x I mo.
100 mg/day x 5 mos.
RelapsedJM' 59/M 50 LL LLs 3.5 100 mg/day x 6 mos.SU 3I/M 5 LL LLs 5.0 100 mg/day x 6 mos.PI) 3I/M 23 LL Hist. nod. 3.3 100 mg/day x 6 mos.RE 38/F 28 LL LLs 4.7 200 mg/day x 1 mo.
100 mg/day x 5 mos.
100 mg daily, 3 days (1, 2, 3), no treatment days 4-14; 100 mg daily, 3 days (15, 16, 17), no treatment days18-30 (CL); no treatment days 18-42 (LN), then 100 mg daily for 5 months.
No pretherapy mouse foot pad inoculation.Absconded, treatment only for 72 days.
taming a 2 x 4-cm strip of filter paper towhich 100 pl of 2 N NaOH had been added.The scintillation vial caps were tightenedand the entire assembly was incubated at33°C for 1 week. The inner vials containingthe bacilli were then removed, and the scin-tillation vials with enclosed filter strips wereshipped by air to Louisiana, U.S.A., wherethe evolved ' 4CO, was measured by adding5 ml liquid scintillation fluid and determin-ing the counts per minute (cpm) in a Beck-man LS-5801 liquid scintillation counter.Data are presented as mean cpm of replicatesamples (N = 2-10) corrected for back-ground activity by subtraction of the meancpm from replicate heat-killed samples (N= 1-5).
In some patients, serum PGL-I antigendeterminations as described by Cho, et al.( 1 ' 4 ) also were performed at the time of bi-opsies.
RESULTS AND DISCUSSIONOur study is an open trial to determine
the efficacy of minocycline in lepromatousleprosy. The characteristics of the patientssequentially admitted and the dose of min-
ocycline are summarized in Table 1. Onepatient (JM) with relapsed leprosy abscond-ed after receiving minocycline 100 mg dailyfor 21/2 months and was not included in theevaluation. Also, a new untreated patient(IC) with no pretherapy mouse foot pad in-oculation result was not included in theevaluation of the results.
The clinical and bacteriologic results after6 months of therapy are presented in Table2. Since the numbers of patients are limitedand because no appreciable differences wereobserved in the clinical and bacteriologicresponses for new, untreated patients andpreviously treated, relapsed patients, the re-sults for both groups were combined.
Clinical improvement was observed in all12 patients completing 6 months of therapy;slight improvement in 6 and moderate-to-marked improvement in the other 6 pa-tients. All papular and nodular lesions sub-sided completely. The effects of differentdoses during the first month is not demon-strable.
Early clinical improvement was notedduring the first 30 days, subsequently be-coming less dramatic. Papular, nodular and

63, 1^Fajardo, et al.: Alinocycline Clinical Trial^ 1 1
TABLE 2. Clinical and bacteriologic (average BI and LIB) results for patients completing6 months of therapy.
Dose/duration No. ClinicalBacteriology
status'Avg. 131 Avg. LIBpatients Isl [mod
Prel. Final Prel. Final
Regimen A200 mg/day 1 mo. 3h I 2 4.73 4.33 4.13 4.35100 mg/day 5 mo.
Regimen B100 mg/day 6 mo. 7, 4 3 4.70 4.60 5.75 5.18
Regimen CIntermittent 1 mo. 2 I 4.90 4.65 5.90 5.72100 mg/day 5 mo.
Total 12 6 6 4.78 4.54 5.37 5.06
" Isl = Slight improvement; !mod = moderate improvement.h One patient (IC), no pretherapy MEP inoculation result, not included in the above tabulation.One patient (JM) absconded and is not included in the above tabulation.
small plaque-type lesions were noted to showthe earliest clinical changes. One relapsedpatient receiving 200 nig daily showed fad-ing of erythema, slight softening and slightwrinkling of the surface of the papulono-dules after 3 days of treatment. In anothertwo patients, also receiving 200 mg daily,fading of erythema and softening of the pa-pulonodules with wrinkling of the overlyingskin became noticeable after 7 days of treat-ment. Similar changes were noted after 14days of treatment in three patients receiving100 mg daily and in another patient, alsoon 100 mg daily, after 30 days of treatment.In one patient, who received only 100 mgdaily for 3 consecutive days, fading of er-ythema, and softening and fine surface wrin-kling of the papulonodules were noted at 14days (11 days after the last dose of mino-cycline). These early changes and the morerapid responses among those receiving 200mg daily strongly suggests an antiinflam-matory effect of minocycline. Some depoteffect is suggested in one patient who showedimprovement 11 days after the last dose ofminocycline 100 mg/day for 3 days. Theserecognizable changes were very encouragingto the patients, and would be an advantageof minocycline in leprosy chemotherapy.
Results of the skin smears for bacterialload (BI) (Table 2) show an overall reduc-tion of 0.24 units after 6 months of treat-ment. One month of minocycline 200 mgdaily or 100 mg daily or a total dosage of600 mg (for patients treated intermittently)
did not show any effect on the BI at 6months. As can be seen, a decrease in theaverage BI was 0.40 units for patients onregimen A; for regimen B, 0.10 units, forregimen C, 0.25 units. None of these de-creases is significant.
In an attempt to evaluate the histologiceffects of treatment, the granuloma fractionand biopsy index were compared at pre-therapy and after 6 months of treatment(Table 2). For the 12 patients completingthe study, there was an average reductionof the granuloma fraction from 54.9% to31.7% and an average reduction of the LIBfrom 5.37 to 5.06 at the end of 6 months.
No reactional episode occurred during the6 months of minocycline therapy, againstrongly suggesting an antiinflammatory ef-fect of minocycline. This was further con-firmed by our observation of the occurrenceof erythema nodosum leprosum (ENL) in 6of the 12 patients after the institution of thestandard WHO/MDT chemotherapy. MildENL (+/+ +) developed in 4 patients (3weeks, 5 months, 6 months and 8 monthsafter MDT was started), and moderate-to-severe ENL (+ +/+ + +) occurred in 2 pa-tients after only 2 weeks on standard WHO/MDT chemotherapy (20).
Tolerable side effects were experiencedonly during the first week of treatment in 2of 8 patients who were receiving minocyc-line 100 mg/day. One male patient experi-enced dizziness and nausea during the firstweek of treatment. This was remedied by

12^ International Journal of Leprosy^ 1995
TABLE 3. Clinical and bacteriologic effects of various minocycline dosages.
Day 0 Day 3 Day 7 Day 10Patient MFP'
+/totalcpm''(S.D.) PGL-I MFI'
+/totalcpm PGL-I(S.D.)
MFP+/total
cpm(S.D.) PGL-I MFP
+/totalcpm
(S.D.) PGL-I
200 mg/day x 1 mo., 100 mg/day x 5 mos.FS 7/7 4533 2+ 9/9 4424^3+ 9/9 5545 2+ 9/9 4314 2+
(929) (1147) (1090) (1249)FM 9/9 3019 3+ 9/10 3182^3+ 9/9 2883 2+ 9/10 3029 2+
(336) (932) (607) (454)RE 8/9 3257 2+ 10/10 —^— 9/10 5718 1+ 7/10 I+
(1242)
100 mg/day x 6 mos.(2396)
EL 2/9 750 1+ 1/10 67 6/7 77 —(230) (40) (56)
TP 7/8 5296 2+ 10/10 1869 2+ 8/10 610 2+(1746) (349) (171)
CF 6/7 2024 2+ 5/10 523 2+ 5/10 230 2+(214) (241) (54)
BJ 9/9 521 7/9 492 1/9 388 —(86) (49) (72)
QE 7/8 6787 8/10 9279^— 7/8 3446(356) (476) (1318)
Pit 11/11 4209 — —(1411)
SU 8/9 723(56)
IntermittentLN' 8/9 5026 9/10 769^— 9/9 2540 —
(1455) (36) (777)CU 8/9 2279 9/9 4463 9/9
(1191) (1832)
a MFP = Mouse foot pad.CPM = Mean counts per minute/10E6 AFB (standard deviation).ISL = Slight improvement; Imod = moderate improvement.Day 42.LN = 100 mg/day on days 1, 2, 3, 15, 16, 17, 43-180.
'CL + 100 mg/day on days 1, 2, 3, 15, 16, 17, 31-180.— = Not done.
taking the dose at night. The other patientwas a female who experienced abdominalpain and nausea during the first 3 days oftreatment, and the drug was temporarilydiscontinued. In this instance, the dose ofminocycline was taken 3 to 4 hours afterbreakfast and may have caused some formof gastritis. The patient was relieved by ant-acid therapy. When treatment was resumedand the dose was given much closer afterbreakfast, no similar side effects were ex-perienced. None of the 3 patients who re-ceived 200 mg/day, taken by 2 patients (1female and 1 male) as a single dose in themorning, and by the other patient (female)as 100 mg in the morning and 100 mg atnight during the first 30 days of the study,
experienced any intolerance. All patients hada slight but definite dark brownish discol-oration of the skin at 6 months which wasmore apparent among those with fair skin.The pigmentation was more pronounced andwas bluish-gray over sites of subsided lo-calized skin lesions. The pigmentation,however, was much less than that observedamong patients receiving the standard MBWHO/MDT chemotherapy at 6 months.
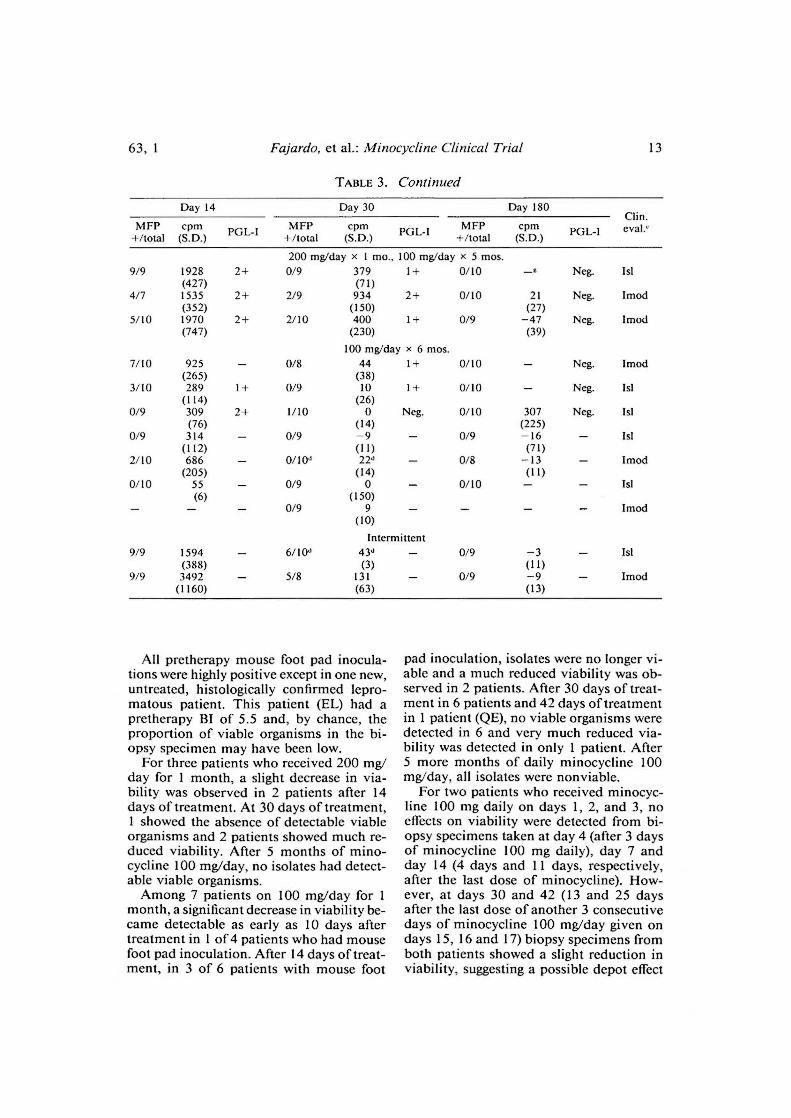
Table 3 gives the results of the viabilitytests with the mouse foot pad inoculationsand palmitic acid oxidation assays and se-rum PGL-I antigen determinations at var-ious intervals during the treatment periodas well as clinical evaluations for the 12patients completing the study.
63, 1^Fajardo, et al.: Minocycline Clinical Trial^13
TABLE 3. Continued
Day 14 Day 30 Day 180Clin.
MFP+/total
cpm(S.D.) PGL-I MFP
+/totalcpm PGL-I(S.D.)
MFP+/total
cpm(S.D.) PGL-I eyal.'
200 mg/day x 1 mo., 100 mg/day x 5 mos.9/9 1928 2+ 0/9 379^1+ 0/10 Neg. Isl
(427) (71)4/7 1535 2+ 2/9 934^2+ 0/10 21 Neg. Imod
(352) (150) (27)5/10 1970 2+ 2/10 400^1+ 0/9 —47 Neg. Imod
(747) (230) (39)100 mg/day x 6 mos.
7/10 925 0/8 44^1+ 0/10 Neg. Imod(265) (38)
3/10 289 1+ 0/9 10^1+ 0/10 Neg. Isl(114) (26)
0/9 309 2+ 1/10 0^Neg. 0/10 307 Neg. Isl(76) (I 4) (225)
0/9 314 0/9 —9^— 0/9 —16(112) (11) (71)
2/10 686 0/10d 22d^— 0/8 —13 Imod(205) (14) (11)
0/10 55 0/9 0^— 0/10 — Isl(6) (150)
0/9 9^— Imod(10)
Intermittent9/9 1594 6/10d 43d^— 0/9 —3 — 1st
(388) (3) (11)9/9 3492 5/8 131^— 0/9 —9 — Imod
(1160) (63) (13)
All pretherapy mouse foot pad inocula-tions were highly positive except in one new,untreated, histologically confirmed lepro-matous patient. This patient (EL) had apretherapy BI of 5.5 and, by chance, theproportion of viable organisms in the bi-opsy specimen may have been low.
For three patients who received 200 mg/day for 1 month, a slight decrease in via-bility was observed in 2 patients after 14days of treatment. At 30 days of treatment,1 showed the absence of detectable viableorganisms and 2 patients showed much re-duced viability. After 5 months of mino-cycline 100 mg/day, no isolates had detect-able viable organisms.
Among 7 patients on 100 mg/day for 1month, a significant decrease in viability be-came detectable as early as 10 days aftertreatment in 1 of 4 patients who had mousefoot pad inoculation. After 14 days of treat-ment, in 3 of 6 patients with mouse foot
pad inoculation, isolates were no longer vi-able and a much reduced viability was ob-served in 2 patients. After 30 days of treat-ment in 6 patients and 42 days of treatmentin 1 patient (QE), no viable organisms weredetected in 6 and very much reduced via-bility was detected in only 1 patient. After5 more months of daily minocycline 100mg/day, all isolates were nonviable.
For two patients who received minocyc-line 100 mg daily on days 1, 2, and 3, noeffects on viability were detected from bi-opsy specimens taken at day 4 (after 3 daysof minocycline 100 mg daily), day 7 andday 14 (4 days and 11 days, respectively,after the last dose of minocycline). How-ever, at days 30 and 42 (13 and 25 daysafter the last dose of another 3 consecutivedays of minocycline 100 mg/day given ondays 15, 16 and 17) biopsy specimens fromboth patients showed a slight reduction inviability, suggesting a possible depot effect

14^ International Journal of Leprosy^ 1995
of minocycline. After daily dosages of min-ocycline 100 mg/day from day 31 to day180 in one patient and from day 43 to day180 in the other patient, no viable M. lepraecould be detected in the biopsy specimens.
The results of radiorespirometric moni-toring done on organisms for mouse footpad inoculation at various intervals duringtreatment are also presented in Table 3. Anarbitrary designation of a "negative" resultin radiorespiromctry was taken to be a meancpm of zero or less than zero (occurs whenheat-killed controls give a slightly higherreading than test samples) or when the stan-dard deviation of the mean overlapped zero.
In all cases radiorespirometric values de-clined with treatment, although there wasnot always an absolute correlation with themouse foot pad data. In most cases a sharpdecline in mouse foot pad infectivity be-tween two time points also was reflected inthe radiorespirometric values. This rela-tionship was also observed in clinical trialsof sparfloxacin ( 1 ) and clarithromycin ( 2 ) butwas not evident with a trial of fusidic acid( 7 )•
Radiorespirometric measurement of theoxidation of palmitic acid to carbon dioxideis currently the only metabolic viability as-say which has withstood the scrutiny of dou-ble-blind evaluation as a primary drug-screening assay for leprosy ( 6). The Bud-clemeyer-type assay was employed for thesestudies due to its greater sensitivity (com-pared to the BACTEC system) in terms ofthe minimum AFB requirement. A few pa-tients with very high bacillary yields wereevaluated by both the BACTEC and Bud-demeyer assays with essentially identical re-sults (data not shown).
An obvious advantage of radiorespiro-metry is the generation of quantitative datawithin 1 week of biopsy in contrast to the6 to 8 months' incubation typically used todetect growth of M. leprae in the mouse footpad. As demonstrated in this study, a liquidscintillation counter need not be present onsite since the filters can easily be mailed toa distant laboratory for determination of thecpm. One limitation is that biopsies musthave a minimum BI of 4 to 5 in order toobtain sufficient bacilli. Another disadvan-tage is the possibility of contamination withother microorganisms. This problem wasrarely encountered (1 of 61 biopsies pro-
cessed on site at LWM) and it appears thatthe addition of only ampicillin and ampho-tericin B is highly satisfactory for contam-ination control.
In 6 patients (3 on minocycline 200 mg/day and another 3 on minocycline 100 mg/day), serum PGL-I antigen determinationswere performed at prctherapy, at 30 days,and at 6 months, and in some patients dur-ing the first month (Table 3). All prethcrapydeterminations were positive. At 30 daysonly one patient had become PGL-I nega-tive and at 6 months all samples were neg-ative. Positivity to PGL-I antigen during thefirst month showed poor correlation withthe mouse foot pad inoculation and pal-mitic acid oxidation results. Apparently,PGL-I antigen determination is not sensi-tive enough to show reductions in viabilityas observed in the mouse foot pad and pal-mitic acid oxidation assays. At day 14, inone patient (CF) PGL-I antigen was stillpositive, while results of palmitic acid ox-idation was much reduced and the mousefoot pad harvest was negative. At day 30,three patients with negative mouse foot padharvests and much reduced radiorespiro-metric results were still positive to PGL-Iantigen. Also, in another two patients PGL-Iantigen was still positive while the mousefoot pad inoculation and palmitic acid ox-idation assays were much reduced. Thus,PGL-I antigen is still measurable for someperiod of time after viability can no longerbe detected by the mouse foot pad inocu-lation technique and the palmitic acid ox-idation assay.
From the above results, a daily dose of200 mg is no more effective than a dailydose of 100 mg as observed in viabilitystudies, using mouse foot pad inoculationand the palmitic acid oxidation assay, dur-ing the first 30 days of treatment. In fact,more significant reductions in viability wereobserved among those on minocycline 100mg/day. However, this observation is basedon only 3 versus 7 patients, and may be achance occurrence. A larger patient popu-lation is obviously needed to investigate thisobservation further.
In our attempt to study possible depoteffects using intermittent dosaging, some re-duction in the viability of M. leprae wasobserved in both the mouse foot pad systemand by the palmitic acid oxidation assay in

63, 1^Fajardo, et al.: Minocycline Clinical Trial^ 15
the two patients under this regimen withonly two pulsed doses. However, we wereable to observe some reduction in viabilityafter pulsed dosaging, confirming favorableresults obtained in mouse studies using in-termittent dosaging ( 12 ). More intermittentdosages in a larger patient population wouldpermit a better evaluation of intermittentdosaging.
SUMMARYTwelve patients were treated with three
dose levels of minocycline for 30 days, pri-marily to detect the dose-related effects onMycobacterium leprae viability, followed byanother 5 months of daily minocycline foroverall efficacy and persistence of clinicaland antibacterial effects. Subsequently, thepatients were given standard WHO/MDTchemotherapy for multibacillary leprosy.
Clinical improvement was recognizableduring the first month, occurring much ear-lier among those on minocycline 200 mgdaily than those who received minocycline100 mg daily. A similar change also wasobserved in one patient 11 days after threedaily doses of 100 mg of minocycline. Atthe end of 6 months, all patients were clin-ically improved with a slight reduction inthe average bacterial index (BI) and loga-rithmic index of bacilli in biopsy (LIB).
The effects of minocycline on viability bymouse foot pad inoculation and palmiticacid oxidation assays were noted beginningat 10 to 14 days of daily dosing and becom-ing more definite after 30 days of treatment.Both tests correlated fairly well. Doses of200 mg daily did not appear to be moreefficient than minocycline 100 daily. Phe-nolic glycolipid-I (PGL-I) antigen deter-minations done on some patients during thefirst month remained positive and did notcorrelate with changes in viability results.
At the end of 6 months, after 5 monthsof 100 mg of minocycline monotherapy, noviable organisms could be demonstrated bymouse foot pad inoculation and palmiticacid oxidation assays; assays for PGL-I an-tigen were all negative.
No lepra reactions were observed duringthe 6 months of therapy. Tolerable side ef-fects, dizziness and abdominal discomfortwere noted only during the first week oftreatment in 2 of 12 patients. A generalizedlight-brown pigmentation was observed,
which was more intense and blue-gray overthe sites of subsided localized lesions.
The results of this study further confirmthe early effects of minocycline on clinicallesions and the viability of M. leprae withantibacterial and clinical effects becomingdefinitely more demonstrable after 6 monthsof treatment. Thus, minocycline is a valu-able drug in the treatment of leprosy, andstudies to determine its efficacy in combi-nation with other antileprosy drugs, dosagelevels and pulsed dosaging, as well as theeffects of lepra reaction, should be pursued.
RESUMENSe trataron 12 pacientes con tres dosificaciones de
minociclina por 30 dias, primariamente para detectarlos efectos de las diferentes dosis sobre la viabilidadde Mycobacterium leprae, seguido por otros 5 mesesde minociclina diaria para establecer la eficiencia gen-eral de la droga y la persistencia de sus efectos clinicosy antibacterianos. Posteriormente los pacientes reci-bieron la poliquimioterapia estandar de Ia WHO parala lepra multibacilar.
La mejoria clinica fue notada durante el primer mes,ocurriendo mucho mas temprano entre aquellos en tra-tamiento con 200 mg diarios de minociclina que entreaquellos tratados con 100 mg diarios de minociclina.TambiOn se observe) un cambio similar en un pacientea los 11 dias de haber recibido 3 dosis diarias de 100mg de minociclina. Al final de los 6 meses, todos lospacientes mostraron mejoria clinica con una ligera re-ducciOn en el indice bacteriano (BI) y en el indice lo-garitmico de bacilos en las biopsias (LIB).
Los efectos de Ia minociclina sobre la viabilidad, porla têcnica de inoculaciOn en la almohadilla plantar delratOn y por los ensayos de oxidaciOn del acid() pal-mitico, fueron notados entre los dias 10 a 14 de tra-tamiento diario y Ilegaron a ser mas aparentes despuOsde 30 dias de tratamiento. Ambas pruebas mostraronuna buena correlaciOn. Las dosis de 200 mg diarios deminociclina no parecieron ser mas eficientes que ladosis de 100 mg diarios de la misma. Las determina-ciones de glicolipido fenOlico-I (PGL-I) practicadas enalgunos pacientes durante el primer mes de tratamien-to, permanecieron positivas y no correlacionaron conlos cambios en los resultados de viabilidad.
Al final de 6 meses, despuês de 5 meses de mono-terapia con 100 mg de minociclina, no se pudierondemostrar bacilos viables por la têcnica de la almo-hadilla plantar del ratOn y por Ia oxidaciOn del acid°palmitico; los ensayos para PGL-I fueron todos ne-gati vos.
No se observaron reacciones leprosas durante los 6meses de terapia. Algunos efectos colaterales tolera-bles, mareo y malestar abdominal, ocurrieron solo du-rante la primera semana de tratamiento en 2 de 12pacientes. Se observe) una pigmentaciOn generalizada

1 6^ International Journal of Leprosy^ 1995
de color care que fue mds intensa y de color azulgris
sobre los sitios de las lesiones curadas.
Los resultados de este estudio confirman los efectostempranos de la minociclina sobre las lesiones clinicas
y sobre Ia viabilidad de M. leprae, con sus efectos anti-bacterianos y clinicos definitivos despues de 6 meses
de tratamiento. Asi, la minociclina es una droga valiosaen el tratamiento de la lepra pero dcbc investigarse aim
mds, su eficacia en combinaciOn con otras drogas anti-leprosas, los niveles y frecuencia de la dosis, y sus
efectos sobre Ia reacciim leprosa.
RÉSUMÉ
Douze patients ont etc traites avec trois dosages de
minocycline pendant 30 jours, tout d'abord pour de-teeter les diets lies au dosage sur la viabilite du My-
cobacterium leprae; cette periode a etc suivic de 5 mois
de minocycline quotidienne pour etudier l'efficacite
globale et la persistance d'effets cliniques et antibac-
tin-lens. Par Ia suite, les patients ont recu une chimio-therapie PCT/OMS standard pour la lepre multibacil-
laire.line amelioration clinique a etc": reconnue durant le
premier mois, survenant beaucoup plus U.-ft parmi ceux
qui recevaient 200 mg de minocycline par jour que
chez ceux qui recevaient 100 mg de minocycline parjour. Un changement semblable etait egalement ob-
serve chez un patient I I jours apres trois doses quo-tidiennes de 100 mg de minocycline. A la fin des 6
mois, tous les patients etaient ameliores cliniquement,avec une legere reduction de l'indice bacterien (113)
moyen et de l'indice logarithmique de bacilles (ILB)
dans la biopsie.On a note que les effets de Ia minocycline sur la
viabilitc mesuree par inoculation dans le coussinet
plantaire de souris et des tests bases sur l'oxydation de
l'acide palmitique commencaient du 1 °erne au 14emejours du traitement quotidien, et devenaient plus netsapres 30 jours de traitement. II y avait une assez bonne
correlation entre ces deux tests. Des doses de 200 mg
par jour n'apparaissaient pas plus efficaces que 100 mg
de minocycline par jour. Les determinations d'antigenedu glycolipide phenolique I (PGL-I) realisee chez cer-
tains patients durant Ic premier mois sont restees pos-
itives et ne montraient pas de correlation avec deschangements dans les resultats de viabilite.
A la fin des 6 mois, apres 5 mois de monotherapie
par 100 mg de minocycline, aucun organisme viable
ne pouvait 'etre mis en evidence par inoculation dans
le coussinet plantaire de la souris et des tests d'oxy-
dation de I'acide palmitique; les tests pour Eantigene
PGL-1 etaient tous negatifs. Aucune reaction lepreuse
n'a ("me observee durant les 6 mois de traitement. Des
effets secondaires supportables, des vertiges et une geneabdominale n'ont Ole notes que durant la premieresemaine de traitement chez 2 des 12 patients. On aobserve une pigmentation generalisee brun-clair, qui
etait plus intense et bleu-gris aux endroits des an-
ciennes lesions localisees.
Les resultats de cette etude confirment les effets pre-coces de Ia minocycline sur les lesions cliniques et la
viabilite de Af. leprae, avec des effets anti-bacteriens
et cliniques devenant nettement plus dêmontrablesapres
6 mois de traitement. En consequence, la minocyclineest un medicament utile dans Ic traitement de la lepre,
et des etudes pour determiner son efficacité en combi-naison avec d'autres medicaments anti-lepreux, difre-
rents dosages et des administrations espacees, ainsi que
ses effets sur Ia reaction lepreuse, devraient 'etre pour-
suivies.
Acknowledgment. We wish to acknowledge the ex-
cellent technical assistance given by the staff of theclinical and laboratory branches of the Leonard Wood
Memorial with special mention to Mrs. Cecilia Alerta,nurse of the clinical branch, Mrs. Rhea Fajardo, of the
vivarium section; Mrs. Manuela Luisa P. Franzblau,Mrs. Elna Nunez and Mrs. Paulina Munalem of the
laboratory branch, and Mrs. Loida Gabiana for com-
puter and clerical help. Also, we thank the EversleyChilds Sanitarium, the medical and technical staff for
their support. Lastly, we wish to thank the LederleLaboratories Division Cyanamid Philippines, Inc., for
some supply of minocycline capsules.This research was supported under Grant #5600 G
00 010100, program in Science and Technology Co-operation, Office of the Science Advisor, USAIR and
the Leonard Wood Memorial, American LeprosyFoundation.
REFERENCES1. CHAN, G. P., GARCIA-IGNACIO, B. Y., CHAVEZ, V.
E., LIVELO, J. B., JIMENEZ, C. L., PARRILLA, M. L.
R. and FRANZBLAU, S. G. Clinical trial of spar-
floxacin for lepromatous leprosy. Antimicrob.Agents Chemother. 38 (1994) 61-65.
2. CHAN, G. P., GARCIA-IGNACIO, 13. Y., CHAVEZ, V.
E., LIVELO, J. B., JIMENEZ, C. L., PARRILLA, M. L.
R. and FRANZBLAU, S. G. Clinical trial of clarith-
romycin for lepromatous leprosy. Antimicrob.Agents Chemother. 38 (1994) 515-517.
3. CHO, S.-N., HUNTER, S. W., GELBER, R. H., REA,T. H. and BRENNAN, P. J. Quantitation of the
phenolic glycolipid of Mycobacterium leprae and
relevance to glycolipid antigenemia in leprosy. J.Infect. Dis. 153 (1986) 560-569.
4. CHO, S.-N., SHIN, J. S., CHOI, I. H., KUN, S. H.,
KIM, D. I. and KUN, J. D. Detection of phenolic
glycolipid-I of Mycobacterium leprae and anti-
bodies to the antigen in sera from leprosy patients
and their contacts. Yonsei Med. J. 29 (1988) 219-
224.
5. FRANZBLAU, S. G. Drug susceptibility testing of
Mycobacterium leprae in the BACTEC 460 sys-
tem. Antimicrob. Agents Chemother. 32 (1989)
2115-2117.
6. FRANZBLAU, S. G., BISWAS, A. N., JENNER, P. and
COLSTON, M. J. Double-blind evaluation of BAC-

63, 1^Fajardo, et al.: Minocycline Clinical Trial^ 17
TEC and Buddemeyer-type radiorespirometric as-says for in vitro screening of anti leprosy agents.Lepr. Rev. 63 (1992) 125-133.
7. FRANZBLAU, S. G., CHAN, G. P., GARCIA-IGNACIO,
B. Y., CHAVEZ, V. E., LIVELO, J. B., JIMENEZ, C.L., PARRILLA, M. L. R., CALVO, R. F., WILLIAMS,
D. L. and Gitus, T. P. Clinical trial of fusidicacid for lepromatous leprosy. Antimicrob. AgentsChemother. 38 (1994) 1651-1654.
8. FRANZBLAU, S. G. and HASTINGS, R. C. Rapid invitro metabolic screen for anti leprosy compounds.Antimicrob. Agents Chemother. 31 (1987) 780-783.
9. GELBER, R. H. Minocycline studies in mice of apromising agent for the treatment of Leprosy. Int.J. Lepr. 54 (1986) 722-723.
10. GELBER, R. 11. Activity of minocycline in My-cobacterium leprae-infected mice. J. Infect. Dis.156 (1987) 236-239.
11. GELBER, R. H., FUKUDA, K., I3YRD, S., MURRAY,
L. P., SIN, P., TSANG, M. and REA, T. H. A clinicaltrial of minocycline in lepromatous leprosy. Br.Med. J. 304 (1992) 91-92.
12. GELBER, R. H., SIN, P., TSANG, M., ALLEY, E. andMURRAY, L. P. Effect of low-level and intermit-tent minocycline therapy on growth of Al. lepraein mice. Antimicrob. Agents Chemother. 35 (1991)992-994.
13. JACOBSON, R. R. and HASTINGS, R. C. Rifampinresistant leprosy. Lancet 2 (1976) 1304-1305.
14. JI, 13. and GROSSET, J-H. Recent advances in thechemotherapy of leprosy. (Editorial) Lcpr. Rev.61 (1990) 313-329.
15. Ji, 13., JAMET, P., PERANI, E. G., BOBIN, P. andGROSSET, J. N. Powerful bactericidal activities ofclarithromycin and minocycline against Alycobac-terium leprae in the treatment of lepromatous lep-rosy. J. Infect. Dis. 168 (1993) 188-190.
16. J1, 13., PERRANI, E. G. and GROSSET, J. H. Effec-tiveness of clarithromycin and minocycline aloneand in combination against Mycobacterium lepraeinfection in mice. Antimicrob. Agents Chemother.35 (1991) 579-581.
17. MACDONALD, H., KELLY, R. G., ALLEN, E. S., NOBE,
J. F. and KANEGIS, L. A. Pharmacokinetic studieson minocycline in man. Clin. Pharmacol. Ther.14 (1973) 852-861.
18. RAMASESH, N., KRAIIENBUHL, J. L. and HASTINGS,R. C. In vitro effects of antimicrobial agents onMycobacterium leprae in mouse peritoneal mac-rophages. Antimicrob. Agents Chemother. 33(1989) 657-662.
19. RIDLEY, D. S. and HILSON, G. R. F. A logarithmicindex of bacilli in biopsies. Int. J. Lcpr. 35 (1967)184-186.
20. Shepard, C. C. Multiplication of M. leprae in thefoot pad of the mouse. Int. J. Lepr. 30 (1962) 291-306.
21. WARNDORFF-VAN DIEPEN, T. Clofazimine-resis-tant leprosy, a case report. Int. J. Lcpr. 50 (1982)139-142.
22. WHO STUDY GROUP. Chemotherapy of leprosyfor control programmes. Geneva: World HealthOrganization, 1982. Tech. Rep. Ser. 675.





























