Embed Size (px)
Citation preview

Idioventricular Rhythm in Acute MyocardialInfarction
By EDWIN L. ROTHFELD, M.D., I. RICHARD ZUCKER, M.D.,
VICTOR PARSONNET, M.D., AND CEsAR A. ALINSONORIN, M.D.
SUMMARYAn ectopic ventricular rhythm (IVR) with a rate of 60 to 100/min was detected in
36 of 100 consecutive patients with acute myocardial infarction by constant monitoringof the electrocardiogram. This mechanism was not apparent clinically and was usuallytransient, lasting 4 to 30 beats. It was frequently associated with inferior myocardialinfarction and usually occurred during sinus bradycardia or the slow phase of sinusarrhythmia. Unlike true paroxysmal ventricular tachycardia (PVT), IVR did not progressto ventricular fibrillation and did not influence the prognosis adversely. Recognition ofIVR is important in order to avoid unnecessary and perhaps dangerous treatment withcardiosuppressive drugs and electrical cardioversion.
Additional Indexing Words:Arrhythmia Ventricular tachycardia
B EFORE THE ADVENT of constant mon-itoring of the electrocardiogram and in-
tensive coronary care, ventricular tachycardiawas thought to occur rarely in acute myo-cardial infarction and was invariably associ-ated with a grave prognosis.1-3 In a review ofarrhythmias in acute myocardial infarction,Master and associates3 mentioned "the rarityof ventricular tachycardia in coronary ar-tery thrombosis." But recent investigationshave shown that ventricular tachycardia oc-curs rather commonly and is perhaps themost frequently observed disturbance inrhythm in the immediate postinfarction peri-od.4-7 Most of these episodes were not de-tected previously because they were transientand usually not obvious clinically. The highincidence of ventricular tachycardia in thesepatients is in keeping with the frequency ofthis finding after experimental coronary ar-tery ligation.8
In general, two types of ectopic ventricular
From the Newark Beth Israel Hospital Institute,Newark, New Jersey.
This investigation was supported by Grant G-106-64,National Heart Institute, National Institutes of Health,U. S. Public Health Service.
Circulation, Volume XXXVII, February 1968
Intensive coronary care
rhythm have been reported in the course ofacute myocardial infarction. The first has agradual onset usually during sinus bradyear-dia or the slow phase of sinus arrhythmia; itsrate is relatively slow, 60 to 100/min, and itsduration is brief, 6 to 30 beats. The second ec-topic ventricular rhythm has a more rapidrate and is usually initiated abruptly by a pre-mature beat that interrupts the precedingT wave. The latter form, called "paroxysmalventricular tachycardia (PVT)," is often sus-tained and may progress to fatal ventricularfibrillation.The slower form of ectopic ventricular
rhythm has been observed in 36 of 100 con-secutive patients with acute myocardial in-farction monitored by a relay telemetric sys-tem.9' 10 At first this mechanism was called".nonparoxysmal ventricular tachycardia"l" be-cause it was similar to the nonparoxysmalA-V nodal tachycardia originally describedby Pick and Dominguez'2 with the exceptionthat the pacemaker was idioventricular. Wehave now abandoned this term in favor of themore descriptive designation, "idioventricularrhythm (IVR)" in acute myocardial infarc-tion. The purpose of this report is to define
203
by guest on July 2, 2018http://circ.ahajournals.org/
Dow
nloaded from

ROTHFELD ET AL.
this interesting ectopic rhythm and to describeits clinical setting, cause, prognosis, and man-agement.
MethodsPatients with acute myocardial infarction were
admitted to the study if they had an episode ofcharacteristic chest pain in addition to electro-cardiographic evidence of transmural infarctionand a typical rise in serum glutamic oxaloacetictransaminase (SGOT) concentration within 12hours of entering the hospital. Each patient wasexamined at least four times daily, and routineelectrocardiograms were obtained twice daily forthe first 72 hours. The electrocardiogram wasmonitored continuously by the telemetry systemfor the first 72 hours in the hospital.The telemetry unit has been described in detail
in previous publications.9' 10 EssentiaIly it con-sists of a RKG-100 transistorized, battery-pow-ered, frequency-modulated transmitter and a re-ceiving apparatus. The latter comprises a recordand playback console and an arrhythmia detectorthat provides for continuous recording on magnet-ic tape of electrocardiograms from one or twosubjects, the automatic detection of arrhythmiasfrom such subjects, the encoding of arrhythmiason tape, and the rapid playback of recorded sig-nals with automatic search for arrhythmias.
ResultsOne hundred consecutive patients with
acute transmural infarction were admitted tothe study between April 15 and December30, 1966. There were 64 males and 36 fe-males with an age range of 38 to 84 years.The electrocardiograms demonstrated anter-ior myocardial infarction in 52, inferior myo-cardial infarction in 41, and combined ante-rior and inferior infarction in seven patients.Known previous myocardial infarction wasdocumented in 14 patients. Twenty-one pa-tients died in the hospital, 13 within the first72 hours. Death was a result of cardiogenicshock or intractable failure in 12 instances,ventricular tachyeardia and fibrillation infour, and presumed thromboembolic com-plications in the remaining five.True PVT with a rate of 118 to 224/min
occurred in eight patients, four of whom hadanterior, three inferior, and one combinedanterior and inferior myocardial infarction.Four of these were terminated by quinidineor procainamide, while the remaining four
progressed to fatal ventricular fibrillation.Seven episodes occurred in the first 24 hours,and there was no diurnal variation. In onlyone case was the onset of the ventriculartachycardia clinically apparent. This arrhyth-mia was initiated by ventricular prematurebeats with an R on T phenomenon observedin all.13 The mean peak serum glutamic oxalo-acetic transaminase (SGOT) concentrationwas 224 units/ml in patients with PVT as op-posed to 96 units/ml in those without ven-tricular arrhythmias.One to 14 runs of IVR with a rate of 60 to
100/min were detected in 36 patients by themonitor but were recorded only twice byroutine electrocardiography. Most episodeslasted 4 to 30 beats and were usually re-corded during sleeping hours (figs. 1 and 2).In one instance, the arrhythmia persisted formore than 8 hours and was possibly relatedto digitalis overdosage. It occurred in thepresence of inferior myocardial infarction in22 cases and of anterior infarction in 14. Itsonset was invariably associated with sinusbradycardia or the slow phase of sinus ar-rhythmia. IVR usually terminated after slow-ing of its rate, allowing the sinus mechanismto regain dominance. The rate at the onsetwas slightly in excess of that of the sinus nodefrequently giving rise to varying degrees offusion, a manifestation of the interplay be-tween the two pacemakers (fig. 1). The meanpeak SGOT concentration in this group was84 units/ml, not significantly different fromthat of those patients without ventricular ar-rhythmias. This mechanism was not seen af-ter the first 48 hours and did not result inrapid ventricular tachycardia or fibrillationin any of the patients. All of these disap-peared spontaneously with no specific drugor electrical therapy. Only three patients diedin this group, two of cardiogenic shock andone of a cerebral embolus.
DiscussionEctopic ventricular rhythms occur com-
monly in acute myocardial infarction andmay be divided into two groups, PVT andIVR. True PVT is defined as a succession of
Csrcalation, Volame XXXVII, February 1968
204
by guest on July 2, 2018http://circ.ahajournals.org/
Dow
nloaded from

IDIOVENTRICULAR RHYTHM
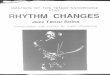
Figure 1
These strips demonstrate three runs of IVR in a 54-year-old man with acute inferior myocardialinfarction. They were recorded with a bipolar chest lead during the early morning hours of thefirst hospital day with the patient asleep. Note the marked sinus arrhythmia in strips A and Bwith IVR initiated by a ventricular fusion beat in A and a slightly premature ventricular beatin B. In strip C the rates of the sinus mechanism and the IVR are nearly identical giving riseto 11 successive fusion beats, QRS complexes five to 15.
I I
FHEI-V.lt7tthi 4 4h-a.tj tE .ot
t;--I
F4t I rI ;_ I
it
I+--- _I.#-
v
I 4a,:.
F^--r-^ 1 r
JAr.-t--~e_}w->0 # sa>Feo..A+
.f4L147itF-L~~~t~~~~tM2flThJ~~~~~TZFL~ 4±11.:j y M Nii..ip-" I VIIIII
W~~~~~~~~~~~~~~~~~~f tt.EtS gS gSFigure 2
The strips represent a conttinuous recording in a 48-year-old man with acute inferior infarction.Note the alternating dominance of the sinus arrhythmia and the IVR and the similarity of therates. The first run of IVR is introduced by a fusion beat and the second by a slightly prematureventricular beat. Alternating dominance of the heart by sinus arrhythmia and IVR is commonlyseen in the immediate postinfarction period.
Circulation, Volume XXXVII, February 1968
W-T l j
-hWVW I K
i- 7-715ft .IE ti -V4141--j ] 1-
..i4-t-.
t
-- .-... .Ft.
m
T
205
f'-
iA ._ sr,
A.=t.t
t->- w". isweo, t.. -> -x>w ** } w_-5 _ ~ '-
I
by guest on July 2, 2018http://circ.ahajournals.org/
Dow
nloaded from

ROTHFELD ET AL.
three or more ventricular premature beatswith a rate in excess of 100/min. Althoughusually related to important heart disease anddrug intoxication, PVT has been reported inat least 35 subjects with no known heartdisease.'4 IVR is a slower ventricular mech-anism with a rate of 60 to 100/min. The dis-tinction is important because of differencesregarding clinical background, mode of pro-duction, prognosis, and management (table1). IVR occurred more commonly than PVTin the present series and was more frequentlyassociated with inferior myocardial infarc-tion. Mean peak SGOT levels were muchhigher in patients with PVT than in thosewith IVR suggesting more extensive myo-cardial necrosis in the former. IVR was lessapt to be detected clinically because of itsbrief duration, its relatively slow rate simu-lating normal sinus rhythm, and its failure toinduce changes in vital signs. IVR lacked theabrupt onset and termination of PVT; it wasusually initiated during sinus bradycardia orthe slow phase of sinus arrhythmia by aventricular premature beat that occurred latein diastole giving rise to a fusion beat. Similar-ly, the sinus mechanism regained control ofthe heart when its rate exceeded that of the
IVR. Ventricular fusion beats were seen muchmore frequently in IVR than in PVT becauseof the close approximation of the sinus andidioventricular rates in the former. In ourexperience IVR has not given rise to ven-tricular fibrillation, and the prognosis wouldseem to be more favorable than for PVT.
Unfortunately, the literature regarding thismechanism is confusing because of an arrayof descriptive terms; it has been referred toas slower ectopic ventricular rhythm,4 ven-tricular tachycardia with Wenckebach-type exitblock,5 accelerated idioventricular rhytfhm(personal communication from H. J. L. Mar-riott), type 1 idioventricular rhythm,'5 ven-tricular tachycardia with slow rate,'6 slowventricular tachycardia,17 and atrioventriculardissociation with idioventricular rhythm.'8
In his description of ventricular arrhyth-mias following experimental coronary occlu-sion, Harris8 observed that a "ventricularfocus with a frequency of impulse formationalmost equal to that of the S-A node was al-ternately gaining and losing dominance ofthe cardiac rhythm." Subsequently the ectopicrhythm became sustained, followed by re-appearance of alternating dominance as the
Table 1Comparison of Idioventricular Rhythm (IVR) and Paroxysmal Ventricular Tachycardia(PVT)
Prevalence in this seriesSite of infarction inmyocardium
Rate per minuteOnset
Termination
Fusion beatsDurationVital signs
SGOT
Prognosis
IVR
36%Inferior in 22 of 36
60 to 100Idioventricular escape or
ventricular fusion beatGradual slowing
Very commonBrief; 4 to 30 beatsUnchanged
Same as in patientswithout ventriculararrhythmias
Favorable; spontaneousdisappearance
PVT
8%None specific
> 100Abrupt with R on T
Abrupt with compensa-tory pause
RareOften sustainedTachycardia; hypo-
tensionSignificantly higher
than in patientswithout ventriculararrhythmias
Grave; 50% fatal
Circulation, Volume XXXVII, February 1968
206
by guest on July 2, 2018http://circ.ahajournals.org/
Dow
nloaded from

IDIOVENTRICULAR RHYTHM
ectopic activity subsided. His figure 1 is strik-ingly similar to our examples of IVR in pa-tients with acute myocardial infarction.Bashour and associates4 have recently re-
viewed ventricular arrhythmias in 42 patientswith acute myocardial infarction. Ectopic ven-tricular rhythm occurred in 70% of their caseswith true ventricular tachycardia recorded in15 patients and a "slow ectopic ventricularrhythm" seen in six. Their figure 3 shows aslow ectopic ventricular rhythm which is sim-ilar to that of our tracings. Unlike our series,the slow ectopic ventricular rhythm occurredmore commonly in anterior myocardial in-farction and in patients with higher meanSGOT levels. Their figure 6 purports to dem-onstrate suppression of slow ventricularrhythm by intravenous diphenylhydantointherapy. We are somewhat dubious aboutthis result because of the frequency of spon-taneous termination of this mechanism.Spann and co-workers7 noted ventricular
tachycardia in 15 of 30 patients with acutemyocardial infarction whom they monitoredfor an average of 52 hours. Eleven had ven-tricular tachycardia with a rate in excess of100, while four had a "slower ectopic ven-tricular rhythm" with a rate of 60 to 100/min. Most were transient and clinically un-apparent and were absent on restudy 3 weeksto 12 months after the infarction. Ventriculararrhythmias were the most frequently seendisturbances in rhythm in this series. Un-fortunately, no electrocardiograms were pub-lished.
In a series of 130 patients reported byLown and associates,5 29% had ventriculartachycardia, and it was the most frequent ofthe serious arrhythmias. He described twotypes: a potentially malignant form withabrupt onset, rapid rate, and serious dynamicconsequences, and a more benign varietywith brief runs of 4 to 20 beats. The rate ofthe latter ranged from 70 to 250/min, andvariations in rate at the onset were attributedto "exit block from the ectopic site withWenckebach's structure." In a recent sym-posium Gazes19 also commented on ventricu-lar tachycardia with slow rates presumablyCirculation, Volume XXXVII, February 1968
due to varying degrees of exit block. Althoughmost of our examples of IVR demonstratedslight variations in rate, no abrupt changeswere observed in any of them, and we haveno evidence to substantiate the possibility ofconstant or varying exit block.Kurland and Pressman20 documented ven-
tricular tachycardia in 25% of their patientsmonitored for 1 to 3 weeks. Their figure 2shows a ventricular mechanism in which theonset occurred after slowing of the supra-ventricular rhythm and in which the ratewas only slightly in excess of the latter.
Ventricular tachycardia was documented in22 of 150 patients studied by Goble and co-workers6 and was the most common arrhyth-mia in this series. Others have concurred inthis high incidence, but details regarding rateand mechanism are not available.2'The mechanism of production of IVR and
PVT can be postulated on the basis of recentinvestigations by Hoffman and Cranefield.22Cardiac cells are classified as automatic orself-excitatory, and nonautomatic or excit-able only by a propagated impulse. Auto-matic cells are characterized by spontaneousdiastolic depolarization which lowers thetransmembrane potential to the level of thethreshold potential. This phenomenon is re-ferred to as phase 4 depolarization. Normallyautomatic cells are found in the sinoatrialnode, other areas of the atria, and in theHis-Purkinje system, while the muscle fibersof the atria and ventricles are not automatic.Since many automatic cells coexist, these au-thors have subdivided them into actual pace-makers, those which initiate a propagatedimpulse, and latent or potential pacemakerswhich have the capacity for spontaneous im-pulse formation. Arrhythmias are producedby changes in the activity of normally auto-matic cells with or without changes in con-ductivity. In IVR there is an increase in thefiring rate of a latent pacemaker, intramyo-cardial Purkinje fibers, related to enhancedphase 4 depolarization in these cells. Thisis associated with a decrease in the automatic-ity of the normal pacemaker in the sinusnode allowing the idioventricular mechanism
207
by guest on July 2, 2018http://circ.ahajournals.org/
Dow
nloaded from

ROTHFELD ET AL.
to escape and gain control of ventricular ac-tivation. In PVT there is an abrupt andmarked increase in the rate of automaticventricular cells causing a rapid ventricularrhythm, without appreciable change in therate of impulse formation in sinus nodalfibers.
Rational management of the patient withIVR is related to knowledge of its mode ofproduction and its consequences. If it repre-sents a potentially rapid ventricular tachy-cardia with varying degrees of exit block,then cardiosuppressive drugs or electricalcardioversion are clearly indicated. But wehave seen no evidence of rapid accelerationof the rate, varying exit block, or progressionto ventricular fibrillation. With the exceptionof one case, IVR was not sustained and usual-ly lasted less than 30 beats.Based on the present experience, we think
that patients with uncomplicated IVR shouldnot be treated with cardiosuppressive drugsfor several reasons: First, IVR has not beenassociated with rapid ventricular rates andhas not progressed to ventricular fibrillation,at least in this group of patients. Second,IVR may actually be a protective mechanismto prevent sustained bradycardia as suggest-ed by Pick and Dominguez12 for nonparoxys-mal A-V nodal rhythm. Finally, these drugsshould be withheld because their effects arelargely unpredictable in the face of increasedphase 4 depolarization in Purkinje cells. AsHoffman and Cranefield23 have demonstratedchanges in conduction induced by drugs likequinidine or procainamide vary greatly de-pending on alterations in the slope of phase4 depolarization and the level of the mem-brane potential.
References1. ARMBRUST, C. A., AND LEVINE, S. A.: Paroxysmal
ventricular tachycardia: A study of one hun-dred and seven cases. Circulation 1: 28, 1950.
2. ROSENBAUM, F. F., AND LEVINE, S. A.: Prognos-tic value of various clinical and electrocar-diographic features of acute myocardial in-farction. Arch Intern Med 68: 913, 1941.
3. MASTER, A. M., DACK, S., AND JAFFE, H. L.:Disturbances of rate and rhythm in acute cor-
onary artery thrombosis. Ann Intern Med 11:735, 1937.
4. BASHOUR, F. A., JONEs, E., AND EDMONSON, R.:Cardiac arrhythmias in acute myocardial in-farction: II. Incidence of the common ar-
rhythmias with special reference to ventricu-lar tachyeardia. Dis Chest 51: 520, 1967.
5. LOWN, B., FAmmo, A. M., HOOD, W. B., ANDTHORN, G. W.: Coronary care unit. JAMA199: 188, 1967.
6. GOBLE, A. J., SLOMAN, G., AND ROBINSON, J. S.:Mortality reduction in a coronary care unit.Brit Med J 1: 1005, 1966.
7. SPANN, J. F., MOELLERING, R. C., HABER, E.,AND WHEELER, E. 0.: Arrhythmias in acutemyocardial infarction. New Eng J Med 271:427, 1964.
8. HAJRIS, A. S.: Delayed development of ventricu-lar ectopic rhythms following experimentalcoronary occlusion. Circulation 1: 1318, 1950.
9. ROTHFELD, E. L., BERNSTEIN, A., Cmws, A. H.,PARSONNET, V., AND ZUCKER, I. R.: Telemetricmonitoring of arrhythmias in acute myocardialinfarction. Amer J Cardiol 15: 38, 1965.
10. ROTHFELD, E. L., BERNSTEIN, A., PARSONNET,V., ZUCKER, I. R., AND ALINSONORIN, C. A.:Telemetric monitoring of the electrocardio-gram in acute myocardial infarction. DisChest 51: 193, 1967.
11. ROTHFELD, E. L., AND ZUCKER, I. R.: Nonpar-oxysmal ventricular tachycardia. Clin Res 15:220, 1967.
12. PICK, A., AND DOMINGUEZ, P.: NonparoxysmalA-V nodal tachyeardia. Circulation 16: 1022,1957.
13. SMIRK, R. H., AND PALMER, D. G.: Myocar-dial syndrome with particular reference to theoccurrence of sudden death and of prematuresystoles interrupting antecedent T waves.Amer J Cardiol 6: 620, 1960.
14. LESCH, M., LEWIS, E., HUMPHRJES, J. O., AND
Ross, R. S.: Paroxysmal ventricular tachy-cardia in the absence of organic heart disease.Ann Intern Med 66: 950, 1967.
15. BELLET, S.: Clinical Disorders of the Heart Beat.Philadelphia, Lea & Febiger, 1963.
16. KITCHELL, J. R.: In The Current Status of In-tensive Coronary Care. New York, The CharlesPress, 1966, p. 46.
17. KILLIP, T.: Op cit., p. 88.18. HIss, R. G., AVERILL, K. H., AND LAMB, L. E.:
Electrocardiographic findings in 67,375 asymp-tomatic subjects: III. Ventricular rhythms.Amer J Cardiol 6: 96, 1960.
19. GAZES, P.: In The Current Status of IntensiveCoronary Care. New York, The Charles Press,1966, p. 71.
Circulation, Volume XXXVII, February 1968
208
by guest on July 2, 2018http://circ.ahajournals.org/
Dow
nloaded from

IDIOVENTRICULAR RHYTHM
20. KULRLAND, G. S., AND PRESSMIAN, D.: Incidenceof arrhythmias in acute myocardial infarc-tion studied with a constant monitoring sys-tem. Circulation 31: 834, 1965.
21. YU, P. N., IMBODEN, C. A., Fox, S. M., ANDKILLrP, T.: Coronary care unit: I. A special-ized intensive care unit for acute myocardial
infarction. Mod Cone Cardiov Dis 34: 23, 1965.22. HOFFMAN, B. F., AND CRANEFIELD, P. F.: Physi-
ological basis of cardiac arrhythmias. AmerJ Med 37: 670, 1964.
23. HOFFMAN, B. F., AND CRANEFIELD, P. F.: Elee-trophysiology of the Heart. New York, Mc-Graw-Hill Book Co., 1960.
AV
1812-Trotting Horse Method of Resuscitationfrom Near-Drowning
From A. S. GORDON: Cardiopulmonary Resuscitation-Conference Proceedings. Washington, D. C., Na-tional Academy of Sciences, National Research Coun-cil, 1967, p. 12.
Circulation, Volume XXXVII, February 1968
209
by guest on July 2, 2018http://circ.ahajournals.org/
Dow
nloaded from

CESAR A. ALINSONORINEDWIN L. ROTHFELD, I. RICHARD ZUCKER, VICTOR PARSONNET and
Idioventricular Rhythm in Acute Myocardial Infarction
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1968 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.37.2.203
1968;37:203-209Circulation.
http://circ.ahajournals.org/content/37/2/203located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 2, 2018http://circ.ahajournals.org/
Dow
nloaded from