Embed Size (px)
Citation preview

Idiopathic isolated unilateral hypoglossal nerve palsy:a diagnosis of exclusionMichael Freedman, BA, BDentSc,a Harsha Jayasundara, BDS (Sri Lanka), MS(OMFS)SL, FFDRCS (Ireland),b andLeo F. A. Stassen, FRCS (Ed), FDSRCS, FTCD, FFSEM (UK), FFDRCSI, MA,c Dublin,IrelandDUBLIN DENTAL SCHOOL AND HOSPITAL AND ST. JAMES’ HOSPITAL DUBLIN
This report describes the rare case of a 22-year-old male with persistent idiopathic isolated hypoglossal nervepalsy. Thorough history, examination, and investigation were needed to rule out the many causes of such apresentation. The clinical presentation showed unilateral atrophy and fibrillation of the affected side and milddeviation on protrusion to the affected side. The differential diagnosis included neoplasia, trauma, infection,endocrine, autoimmune, neurologic, and vascular causes. Investigations included magnetic resonance imaging,computerized tomography scan, chest x-ray, cerebrospinal fluid culture, and a range of hematologic tests. These led toa diagnosis of persistent idiopathic isolated hypoglossal nerve palsy. (Oral Surg Oral Med Oral Pathol Oral Radiol
Endod 2008;106:e22-e26)Isolated hypoglossal nerve palsy (HNP) is an uncom-mon condition.1-3 It may be due to damage to thehypoglossal nucleus in the brain stem or to damage tothe nerve along its course.
A literature review revealed that in most cases iso-lated HNPs indicate the presence of an intracranial orextracranial space–occupying lesion, head and neckinjury, vascular abnormality, infection, autoimmunedisease, or neuropathy. Reports of idiopathic cases arerare. Some authors believe that self-limiting idiopathicHNP mimics Bell’s palsy of the facial nerve.4
The hypoglossal nerve supplies the muscles of thetongue, the infrahyoid muscles (via descendens hypo-glossai), and the thyrohyoid muscle. Unilateral paresiscauses weakness and wasting of the ipsilateral tongue.Any dysarthria and dysphagia are usually mild, becausethe contralateral muscles compensate well.
We report a case of persistent idiopathic unilateralhypoglossal nerve palsy with an emphasis on the in-vestigations necessary to be undertaken on presentationof such a lesion.
aHouse Officer, Dublin Dental School and Hospital.bRegistrar, National Maxillofacial Unit, St. James’ Hospital Dublin.cProfessor, Oral and Maxillofacial Surgery, St. James’ HospitalDublin.Received for publication Jul 31, 2007; returned for revision Feb 15,2008; accepted for publication Feb 20, 2008.1079-2104/$ - see front matter© 2008 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2008.02.024e22
CLINICAL FINDINGSA 22-year-old male maths scholar, complaining of a
lack of control and difficulty moving his tongue, wasreferred to the Oral and Maxillofacial Surgery Departmentof the Dublin Dental School and Hospital by his generaldental practitioner. The patient had first noticed this prob-lem 18 months prior to presentation. He was on a ski tripand had noticed an acute swelling of his tongue anddifficulty speaking lasting 8 days. On presentation, thepatient reported a slight alteration in speech, preventinghim from rolling his Rs and causing him to eject somesaliva on speech. No alteration of taste or para- or anes-thesia of the tongue was reported. There was a history ofrecurrent oral ulceration from a young age, which were ofshort duration and occurred roughly 4 times per year.There was no relevant medical history. There was nohistory of trauma or illness at the time.
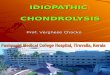
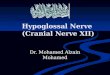
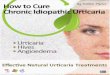
On examination, the patient appeared fit and healthy.No extraoral scarring, swelling, or asymmetry wasnoted. All cranial nerves were intact. Intraorally, onecircular ulcer, 3 mm in diameter, with a white base anderythematous border, was noted on the ventral surfaceof the tongue. Bilateral buccal linea alba were alsovisible. Atrophy and constant fibrillation of the rightside of the tongue were observed. The tongue deviatedto the right on protrusion, but not excessively (Figs.1-3). At this stage, the patient was transfered to theNational Maxillofacial Unit in St. James’ HospitalDublin, for further investigations.
DIFFERENTIAL DIAGNOSISThe differential diagnosis is displayed in Table I.
Neoplasia,5-9 trauma,10-12 infection,5,13-15 autoimmune

OOOOEVolume 106, Number 1 Freedman, Jayasundara, and Stassen e23
disease,16 demyelinating disorders,17 vascular disor-ders,18,19 and endocrine disorders20 have been reportedas causes of hypoglossal nerve palsy and formed thebasis of the differential diagnosis.
The further investigations that were carried out aredisplayed in Table II. Normal full blood count, erythro-cyte sedimentation rate, and C-reactive protein ruled outan infectious cause. Negative viral serology confirmedthese findings. General immunology and autoimmunitytests excluded an autoimmune cause. Renal function tests,liver function tests,and random blood glucose were allnormal. Cerebrospinal fluid (CSF) analysis and culturewere performed to rule out intracranial pathology. Thesewere unremarkable, showing a mildly increased CSF al-bumin. Radiographic examination included a chest x-ray(to rule out sarcoidosis), computerized tomography (CT)scan of thorax, neck, and brain, and magnetic resonanceimaging (MRI) of the head and neck region, in particular
Fig. 1. Tongue at rest. Arrow, atrophy.
Fig. 2. Protrusion of the tongue.
the hypoglossal nerve (Figs. 4-6). The imaging of the head
and neck region was performed to rule out a space-occupying lesion. The hypoglossal nerve was visualized,and no abnormalities were detected using any of thesetechniques.
A diagnosis of idiopathic isolated unilateral hypo-
Fig. 3. Left lateral movement of the tongue.
Table I. Differential diagnosis of causes of hypoglos-sal nerve palsy
NeoplasiaMetastasisChordomaPosterior cranial fossa tumourMeningiomaLymphoma
TraumaPenetrating or blunt head & neck traumaFacial fracturesHead and neck surgery
VascularStrokeDural arterovenous fistula
AutoimmuneNeurologic
Multiple SclerosisInfection
MeningitisEpstein-Barr virusCytomegalovirusHerpes simplex virusPoliomyelitisSyphilisOsteomyelitis
EndocrineDiabetes mellitus
IdiopathicOther
SarcoidosisArnold Chiari malformation
glossal nerve palsy was made.

OOOOEe24 Freedman, Jayasundara, and Stassen July 2008
DISCUSSIONThe hypoglossal nerve is the 12th cranial nerve and
supplies motor innervation to the intrinsic and extrinsicmuscles of the tongue. Anatomically, it leaves the me-dulla and passes along the base of the skull to thehypoglossal canal. Here it exits the skull into the naso-pharyngeal space and travels inferiorly and deep to theinternal carotid artery and internal jugular vein. Itsbranches then travel beneath the digastric muscle be-fore entering the substance of the tongue.21 Hypoglos-sal nerve motor composition is highly complex and notfully understood, with the nucleus consisting of 4 to-pographically distinct subnuclear columns. The occur-rence of isolated hypoglossal nerve palsy is rare be-cause this neuropathy appears concomitantly with otherneurologic abnormalities, and it could be the first oronly sign of more sinister underlying pathology. Clini-cians should be suspicious in such circumstances and
Table II. Special investigations performedHematologic Full blood count
Erythrocyte sedimentation rateC-Reactive proteinCoagulation
PTINRAPTTAPTT Ratio
HematinicsSerum folateRed cell folateSerum vitamin B12
BiochemistryRandom glucoseRenal function testsUrea and electrolytes
General immunologyIgGIgAIgMC3C4Serum electrophoresisIgG index
SerologyHerpes simplex virusCytomegalovirusEpstein-Barr virus
AutoimmunityAntineutrophil cytoplasmic antibodyLiver kidney microsomal antibodiesSmooth muscle antibodiesParietal cell antibodies
CSF Analysis and cultureRadiology Chest x-ray
CT scan of thorax, head and neckMRI of head and neck
be prepared to follow an investigative pathway de-
signed to reveal a possible underlying pathology. In thepresent case, a hypoglossal nerve palsy presented in theabsence of any related historical findings.
Keane reported a retrospective analysis of 100 casesof hypoglossal nerve palsy.5 Almost one-half from thatseries were caused by neoplasia, and over one-half ofthose were malignant. Trauma was the next most com-mon cause. The majority of the palsies were associatedwith damage to 1 or more of the other cranial nerves.Idiopathic palsies of the hypoglossal nerve are veryuncommon and should be regarded as the exceptionrather than the rule.
A detailed history should be taken from patientspresenting with HNP. Particular attention should bedrawn to any instances of trauma or infection aroundthe time that the palsy was first noticed. Ocular symp-toms may be an early feature of multiple sclerosis.22 Asurgical history may also reveal a possible iatrogeniccause. The clinical appearance of HNP is characteristic,
Fig. 4. MRI scan showing hypoglossal nerve.
with atrophy of the affected side and deviation to the

OOOOEVolume 106, Number 1 Freedman, Jayasundara, and Stassen e25
affected side on protrusion.3,5,10 Any local causes fordeviation such as oral cancer should be ruled out. A full
Fig. 5. MRI scan showing hypoglossal canals.
Fig. 6. MRI scan showing atrophy of right side of tongue.
cranial nerve exam will investigate damage to other
cranial nerves, which would point to an intracranialcause. Signs of a posterior cranial fossa tumour includeataxia, nystagmus, intention tremor, and difficulty per-forming rapid repeated movements (dysdiadocokine-sis). The patient should also be examined for any evi-dence of fractures of the facial skeleton. Extra- orintraoral swellings and ulceration should be regardedwith a high index of suspicion.
Viral serology and CSF culture may reveal an infec-tious origin; however, more unusual causes, such aspoliomyelitis, cannot be ruled out. Blood glucose levelsshould be measured to test for diabetes mellitus. He-matologic tests for autoimmune disease may also beperformed.
Thorough radiographic examination is essential incases of HNP. A chest x-ray should be carried out toexclude sarcoidosis. CT scans of the head and neckregion may reveal a space-occupying lesion along thepath of the hypoglossal nerve. MRI is particularly use-ful in providing soft tissue detail and may displaydemyelination of the hypoglossal nerve. These imagingtechniques will also allow any vascular malformationsto be seen.
Few cases of unresolved idiopathic isolated hypo-glossal nerve palsy have been reported. They have anumber of similarities to our case. Ho et al. reported acase of a 25-year-old female with right side idiopathicisolated HNP for almost 5 years, which failed to revealany possible causes after following a similar investiga-tive pathway as used in the present case.1 She wasfollowed-up for 4 years, during which time the condi-tion remained unchanged.
Bagan-Sebastian et al. reported another case of a24-year-old woman who had a similar presentation for10 years. As with the present case, all of the investiga-tions were negative and the etiology of HNP remainedunknown.2
Idiopathic isolated HNP is very rare.1-3 Becausemany of the more common causes of HNP have seriousconsequences, idiopathic HNP should remain a diagno-sis of exclusion. In the present case, despite full inves-tigation, no cause could be found. The fact that thepalsy had been present for 18 months without anydeterioration and that no major functional limitationwas present were good signs. A demyelinating diseaseremains a possibility, so regular follow-up with neuro-logic examination and possibly MRI as indicated, willbe helpful in long-term management.
CONCLUSIONSIsolated HNP is rare but should be regarded with
suspicion. A systematic approach in dealing with thisproblem should be adopted to exclude any serious
underlying pathology.
OOOOEe26 Freedman, Jayasundara, and Stassen July 2008
REFERENCES1. Ho MW, Fardy MJ, Crean SJ. Persistent idiopathic unilateral
isolated hypoglossal nerve palsy: a case report. Br Dent J20048;196:205-7.
2. Bagan-Sebastian JV, Milian-Masanet MA, Penarrocha-Diago M,Lloria de Miguel E. Persistent idiopathic unilateral hypoglossalnerve palsy. J Oral Maxillofac Surg 1998;56:507-10.
3. Pandey VP, Deshpande R, Talati R, Patel A. Isolated idiopathicunilateral XIIth nerve palsy. J Assoc Physicians India2001;49:293-4.
4. Lee SS, Wang SJ, et al. Transient unilateral hypoglossal nervepalsy: a case report. Clin Neurol Neurosurg 1994;96:148-151.
5. Keane JR. Twelfth-nerve palsy. Analysis of 100 cases. ArchNeurol 1996;53:561-6.
6. Barnadas MA, Escartin A, Alomar A. Oral ulcerations as the firstsign of a foramen magnum meningioma. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2000;90:609-11.
7. Aslan Y, Okten A, Demirci A. Primary Burkitt’s lymphoma ofthe cranial vault in a child. Pediatr Radiol 1995;25(Suppl1):S232-3.
8. Millingen K, Prentice M. Isolated unilateral hypoglossal nervepalsy due to a chondroid chordoma. Clin Exp Neurol1987;23:213-7.
9. Pavithran K, Doval DC, Hukku S, Jena A. Isolated hypoglossalnerve palsy due to skull base metastasis from breast cancer.Australas Radiol 2001;45:534-5.
10. Paley MD, Wood GA. Traumatic bilateral hypoglossal nervepalsy. Br J Oral Maxillofac Surg 1995;33:239-41.
11. Muthukumar N. Delayed hypoglossal palsy following occipitalcondyle fracture—case report. J Clin Neurosci 2002;9:580-2.
12. Olzowy B, Lorenzl S, Guerkov R. Bilateral and unilateral inter-nal carotid artery dissection causing isolated hypoglossal nervepalsy: a case report and review of the literature. Eur ArchOtorhinolaryngol 2006;263:390-3.
13. Singh S, Shankar RR, Singhi PD, Kumar L. Isolated hypoglossalnerve palsy in pyogenic meningitis. Indian Pediatr 1988;
25:705-6.14. van Baalen A, Petersen B, Stephani U. Infectious mononucleosisand unilateral tongue writhing. Neurology 2006;66:1110.
15. Nicolai P, Lombardi D, Berlucchi M, Farina D, Zanetti D.Drainage of retro-parapharyngeal abscess: an additional indica-tion for endoscopic sinus surgery. Eur Arch Otorhinolaryngol2005;262:722-30.
16. Ogawa K, Saruya T, Mochizuki Y, Oishi M, Takasu T. A case ofmultiple cranial neuropathy with positive antinuclear antibodyresponded to steroid. No To Shinkei 2000;52:407-11.
17. Tritschler JL, Delouvrier JJ, Khoury M, Dehen H, Masson M.Multiple sclerosis manifested by paralysis of the great hypoglos-sal nerve. Nouv Presse Med 1979;8:2756.
18. Umapathi T, Venketasubramanian N, Leck KJ, Tan CB, Lee WL,Tjia H. Tongue deviation in acute ischaemic stroke: a study ofsupranuclear twelfth cranial nerve palsy in 300 stroke patients.Cerebrovasc Dis 2000;10:462-5.
19. Combarros O, Alvarez de Arcaya A, Berciano J. Isolated unilat-eral hypoglossal nerve palsy: nine cases. J Neurol 1998;245:98-100.
20. Semiz S, Fisenk F, Akcurin S, Bircan I. Temporary multiplecranial nerve palsies in a patient with type 1 diabetes mellitus.Diabetes Metab 2002;28:413-6.
21. Thompson EO, WRK Smoker. Hypoglossal nerve palsy: a seg-mental approach. RadioGraphics 1994;14:939-58.
22. Chen L, Gordon LK. Ocular manifestations of multiple sclerosis.Curr Opin Ophthalmol 2005;16:315-20.
Reprint requests:
Leo F. A. StassenProfessor, Oral and Maxillofacial SurgerySt. James’ Hospital DublinJames’s StreetDublin 8Ireland
[email protected]