Embed Size (px)
Citation preview
Idiopathic DVT: How long to treat? Population-based or Personalized
Marc Zumberg Associate Professor
Division of Hematology/Oncology March 2012
Disclosures
• Consultant – Johnson and Johnson Pharmaceuticals
• Speakers bureau and Consultant – Amgen – GlaxoSmithKline
Goals
• Understand the complexities of decision making concerning length of therapy for idiopathic DVT
• Understand the risks for recurrent VTE, as well as bleeding
• Understand the potential benefits of a personalized, risk adapted approach to decision making
Facts • Incidence of venous thrombosis 1-3/1000/yr
– Common in elderly, nearly 1%/yr – 1 in 20 individuals experience a VTE in their lifetime
• One person is diagnosed with a blood clot every minute – 900,000 cases/year in USA – 60,000-300,000 fatalities per year
• 40% of cases are considered idiopathic – Initial thromboembolic event is the strongest single
predictor for recurrent VTE Rosendall. Hematology. 2005
Bauer. JAMA. 2011. 305 Rodger. Blood Reviews. 2010:171-8
www.clotconnect.org
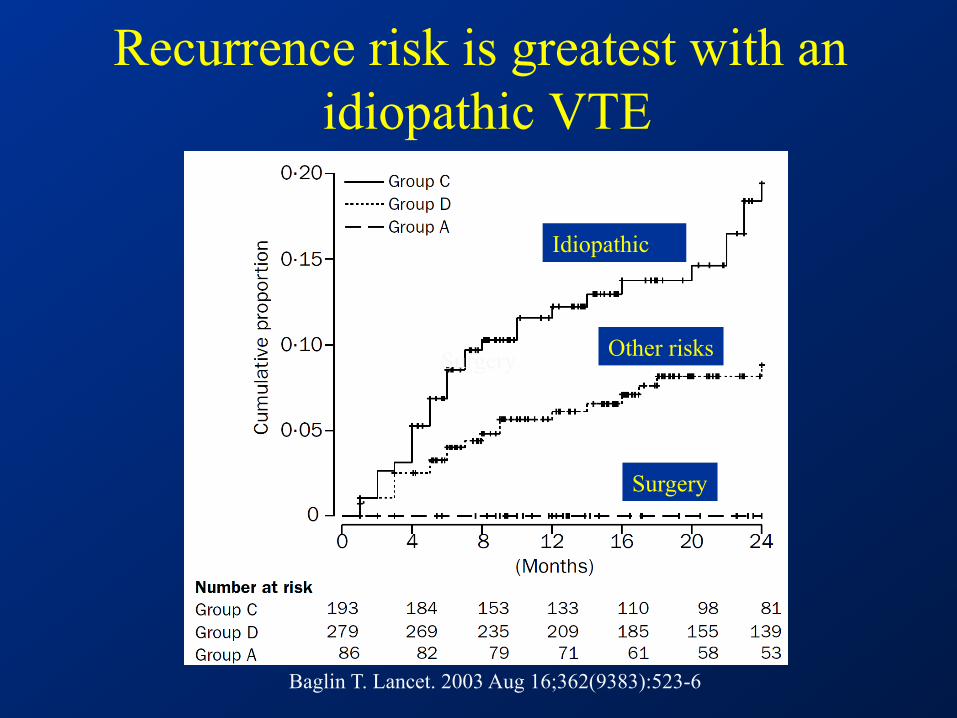
Recurrence risk is greatest with an idiopathic VTE
Idiopathic
Other risks Surgery
Surgery
Baglin T. Lancet. 2003 Aug 16;362(9383):523-6
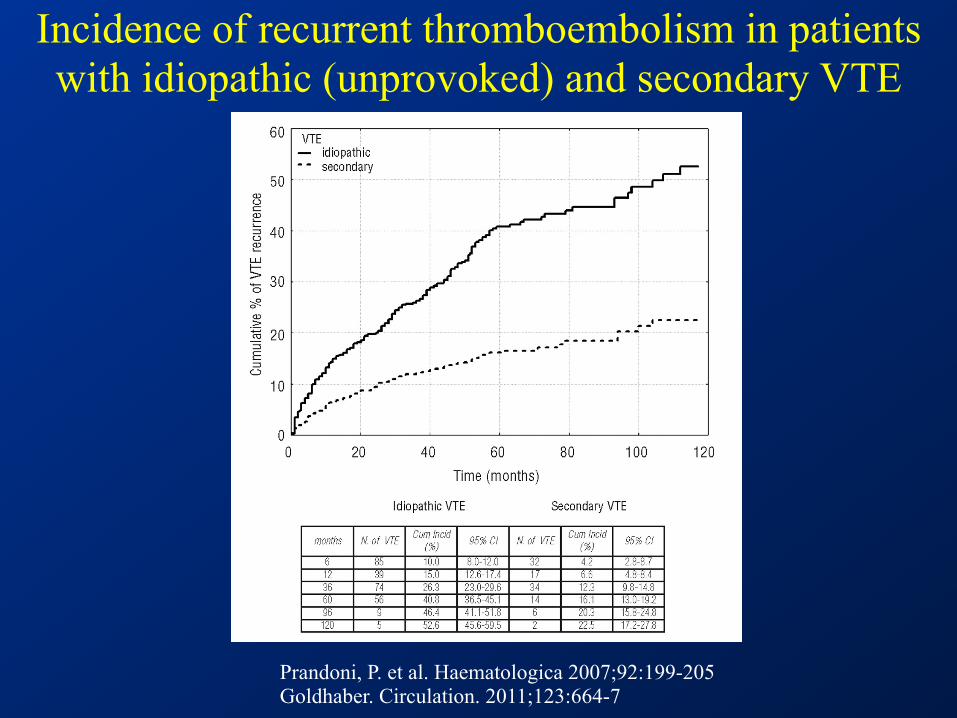
Prandoni, P. et al. Haematologica 2007;92:199-205 Goldhaber. Circulation. 2011;123:664-7
Incidence of recurrent thromboembolism in patients with idiopathic (unprovoked) and secondary VTE
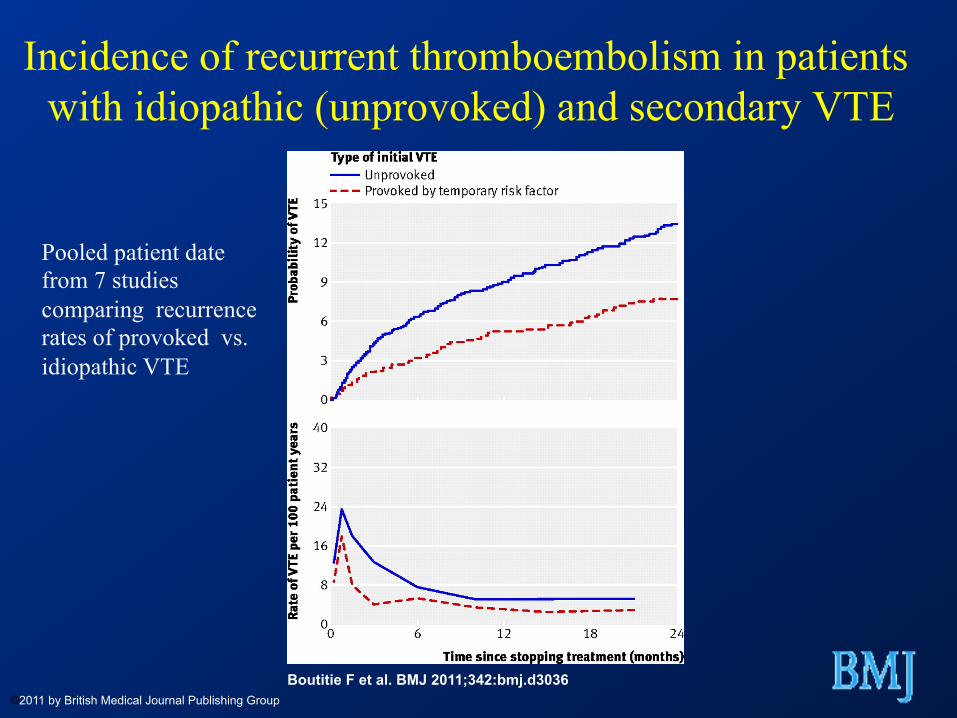
Boutitie F et al. BMJ 2011;342:bmj.d3036 ©2011 by British Medical Journal Publishing Group
Incidence of recurrent thromboembolism in patients
with idiopathic (unprovoked) and secondary VTE
Pooled patient date from 7 studies comparing recurrence rates of provoked vs. idiopathic VTE
Case • 51 year-old previously healthy male seeks consultation
for anticoagulation recommendations
– Idiopathic femoral vein clot and has completed 3 months of warfarin
– Tolerating well with mostly therapeutic INR values – No prior or family history of thrombosis – Up to date on PSA testing and colonoscopy – Nl cbc, electrolytes, LFTs
Do I need to stay on this medicine ??
Risks versus Benefits
Patient Preference
Clotting Bleeding
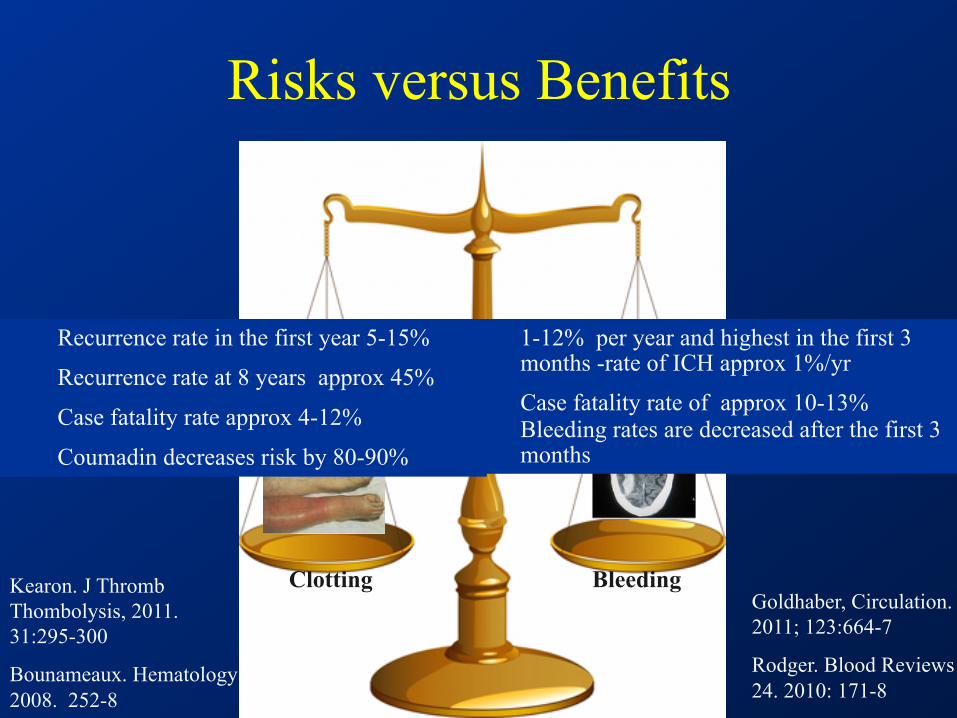
Risks versus Benefits
Clotting Bleeding
1-12% per year and highest in the first 3 months -rate of ICH approx 1%/yr
Case fatality rate of approx 10-13% Bleeding rates are decreased after the first 3 months
Recurrence rate in the first year 5-15%
Recurrence rate at 8 years approx 45%
Case fatality rate approx 4-12%
Coumadin decreases risk by 80-90%
Goldhaber, Circulation. 2011; 123:664-7
Rodger. Blood Reviews 24. 2010: 171-8
Kearon. J Thromb Thombolysis, 2011. 31:295-300
Bounameaux. Hematology 2008. 252-8
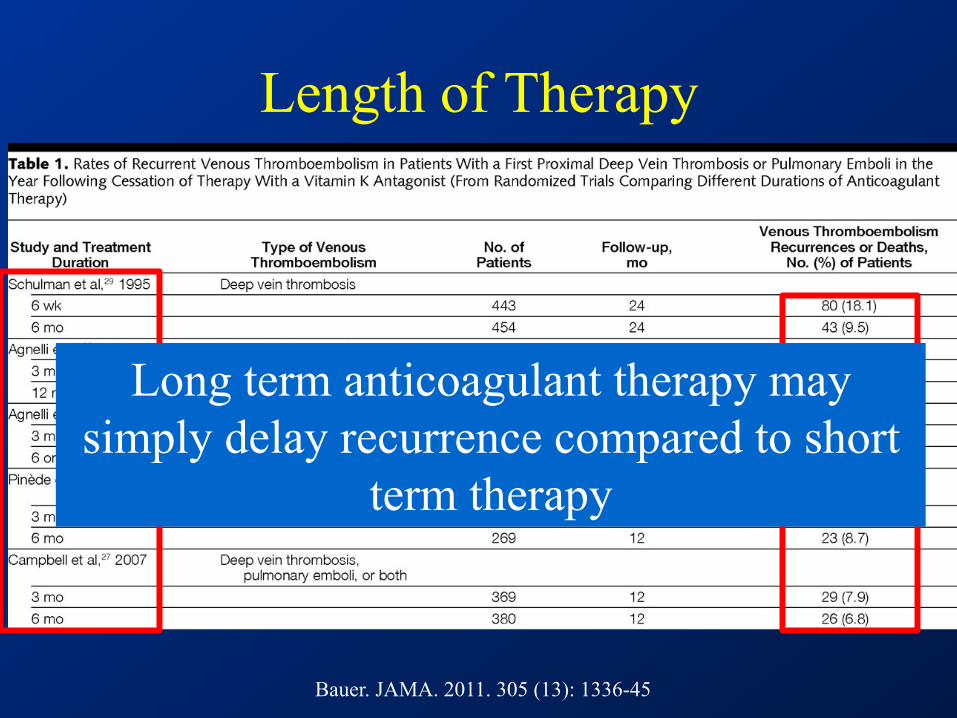
Length of Therapy
Bauer. JAMA. 2011. 305 (13): 1336-45
Long term anticoagulant therapy may simply delay recurrence compared to short
term therapy
Idiopathic DVT: A chronic disease Length of Therapy
• 3 months of anticoagulation better then < 3 months • 3 months no worse than 6-12 months
– Treats acute episode optimally – Recurrence rate is high whenever anticoagulation is
stopped
• The real question should be 3 months vs. indefinite anticoagulation
Kearon. J Thromb Thrombolysis 2011. 31:295-300
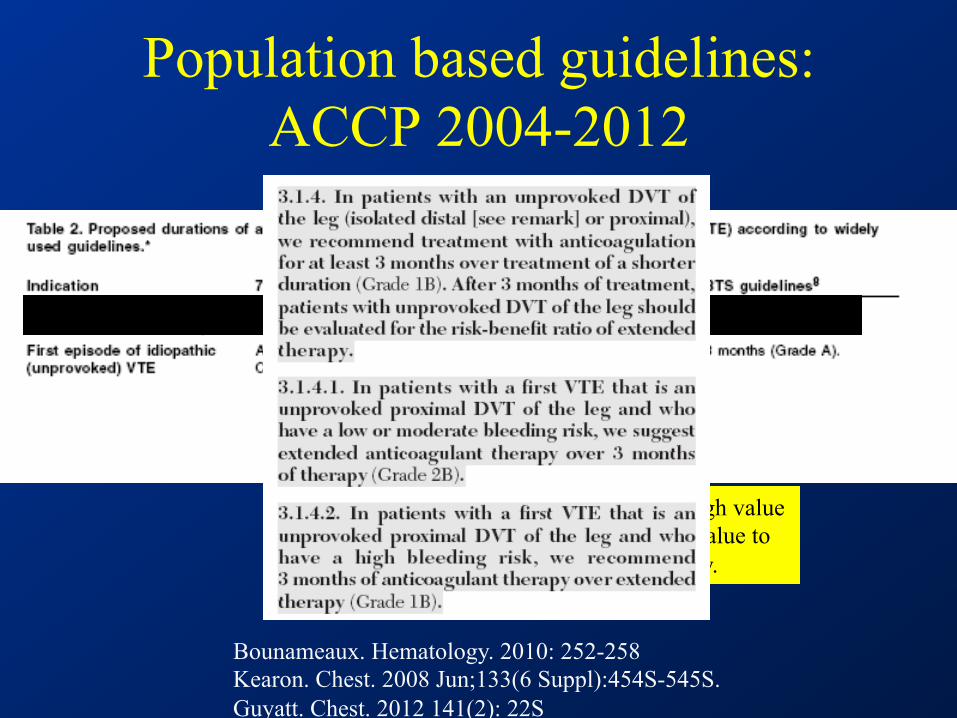
Population based guidelines: ACCP 2004-2012
Bounameaux. Hematology. 2010: 252-258 Kearon. Chest. 2008 Jun;133(6 Suppl):454S-545S. Guyatt. Chest. 2012 141(2): 22S
This recommendation attaches a relatively high value to prevention of recurrent VTE and a lower value to the burden of long-term anticoagulant therapy.
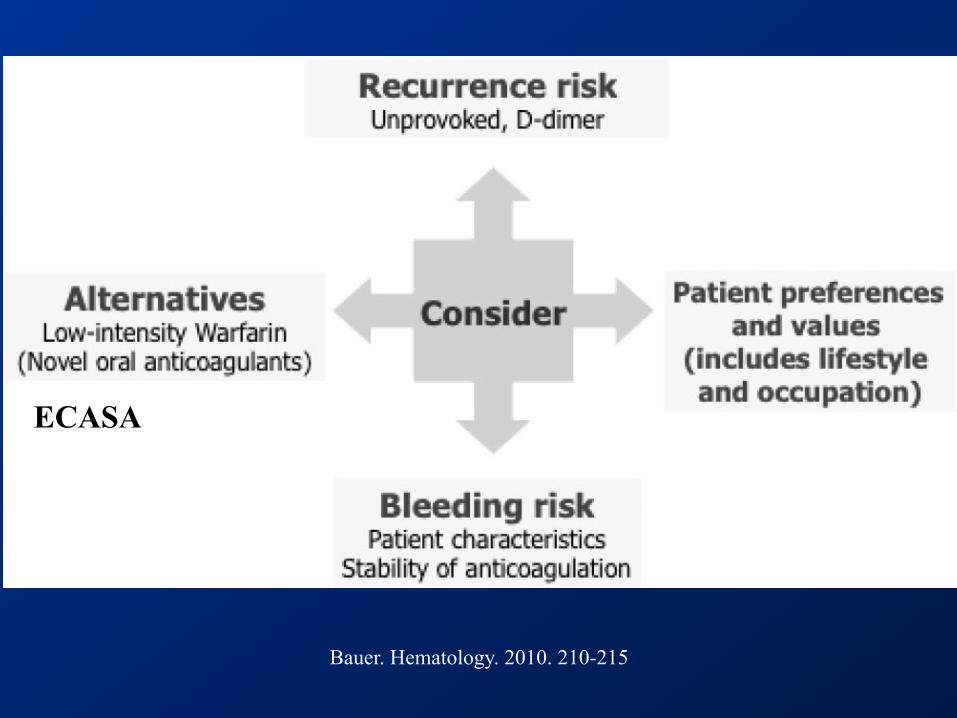
Bauer. Hematology. 2010. 210-215
ECASA

Risk factors for recurrent VTE
• Male gender • Obesity • PE vs. DVT, proximal vs. distal • Elevated D-dimer after discontinuing
anticoagulation • Failure to recanalize leg veins • Thrombophilia • Family History
Goldhaber. Circulation. 2011; 123:664-7
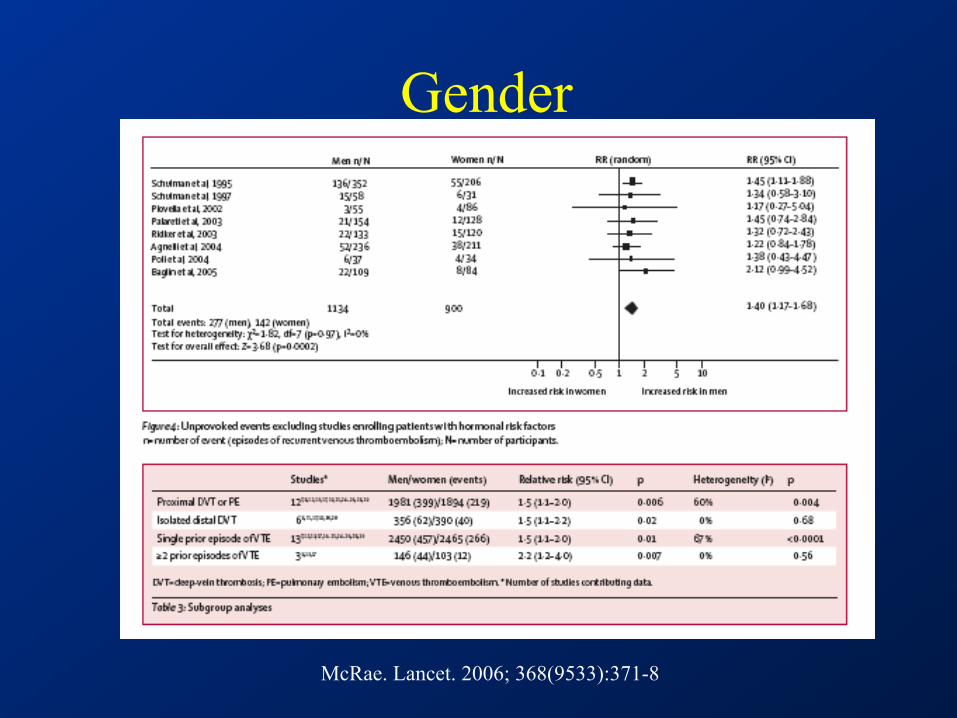
Gender
McRae. Lancet. 2006; 368(9533):371-8
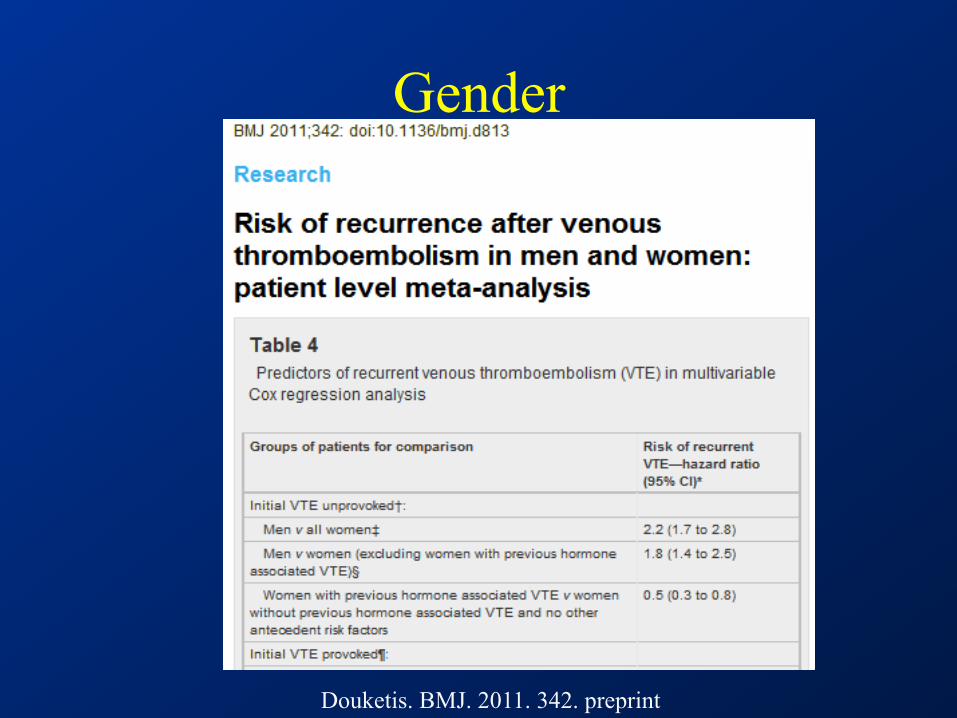
Gender
Douketis. BMJ. 2011. 342. preprint
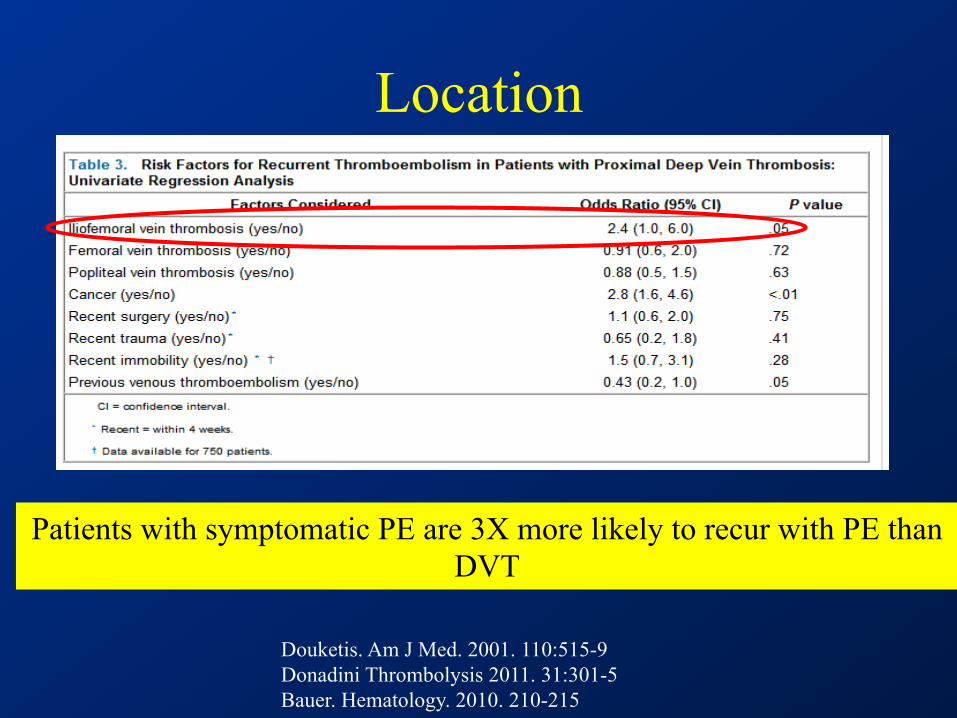
Location
Douketis. Am J Med. 2001. 110:515-9 Donadini Thrombolysis 2011. 31:301-5 Bauer. Hematology. 2010. 210-215
Patients with symptomatic PE are 3X more likely to recur with PE than DVT
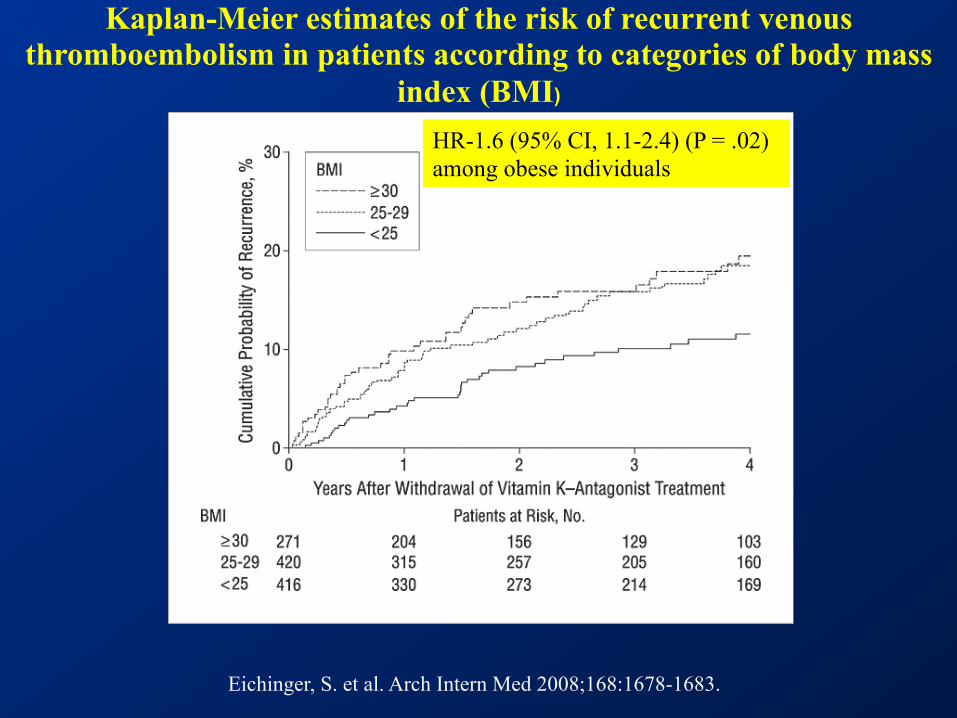
Eichinger, S. et al. Arch Intern Med 2008;168:1678-1683.
Kaplan-Meier estimates of the risk of recurrent venous thromboembolism in patients according to categories of body mass
index (BMI)
HR-1.6 (95% CI, 1.1-2.4) (P = .02) among obese individuals
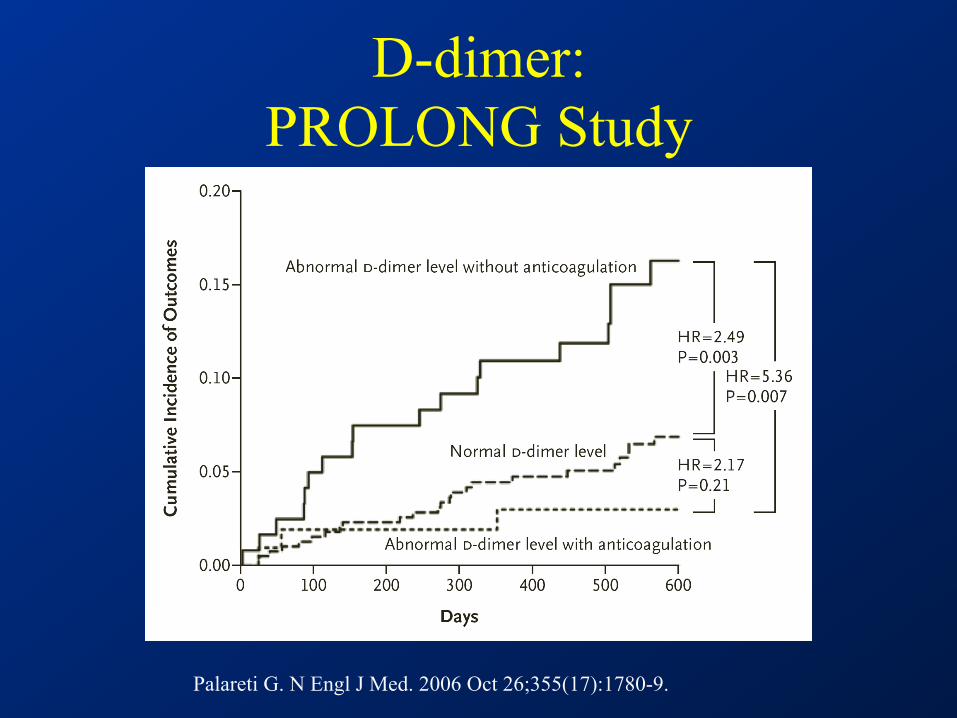
D-dimer: PROLONG Study
Palareti G. N Engl J Med. 2006 Oct 26;355(17):1780-9.
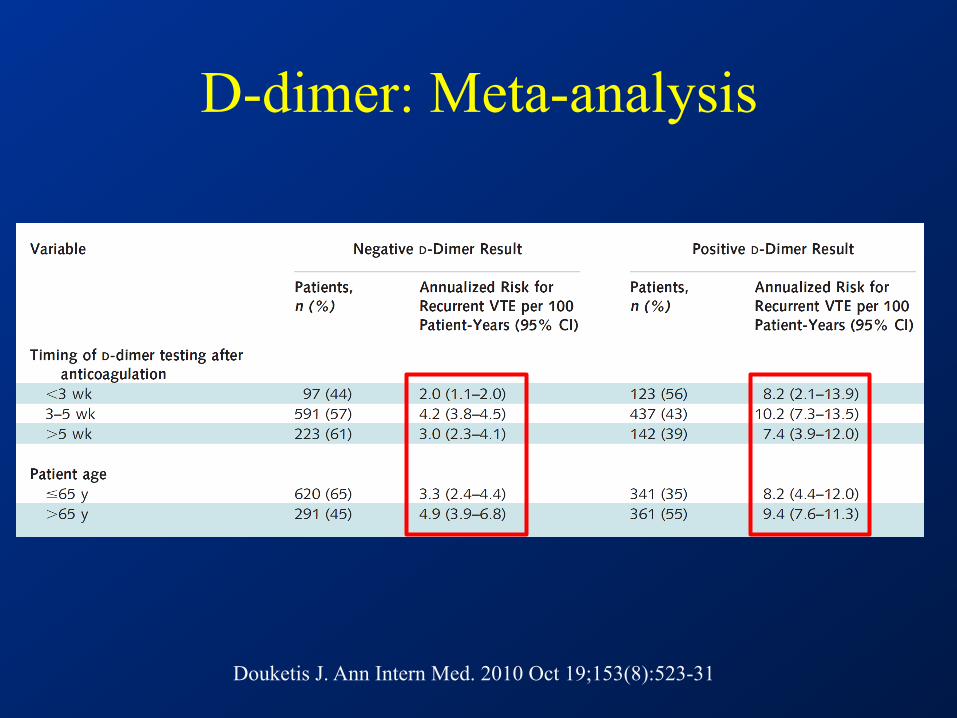
D-dimer: Meta-analysis
Douketis J. Ann Intern Med. 2010 Oct 19;153(8):523-31
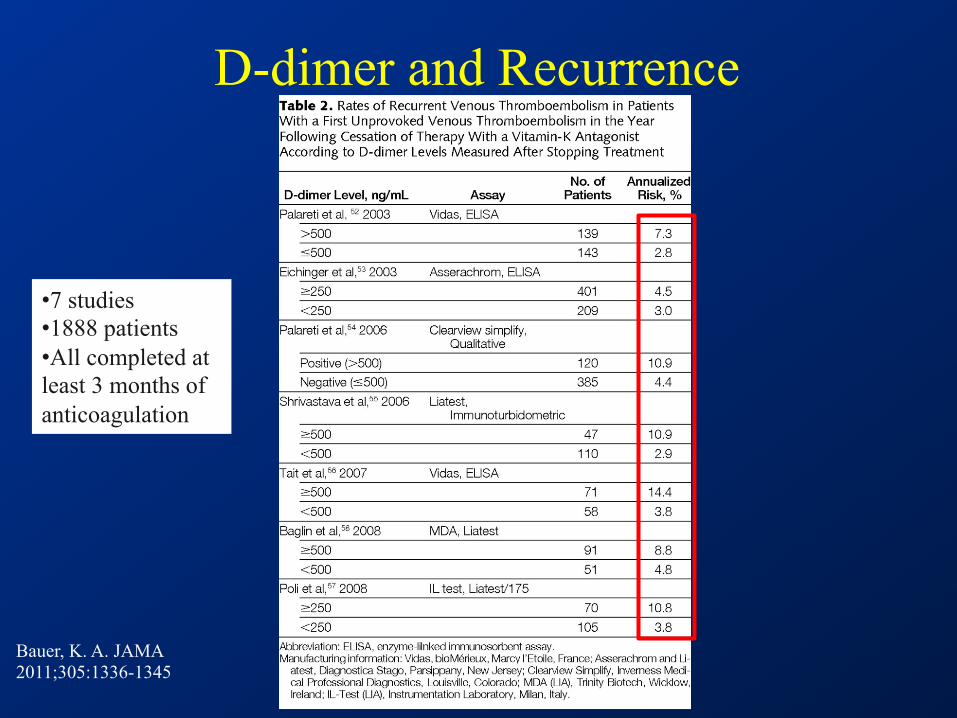
D-dimer and Recurrence
Bauer, K. A. JAMA 2011;305:1336-1345
• 7 studies • 1888 patients • All completed at least 3 months of anticoagulation
Thrombophilia
Among patients with first episode of idiopathic DVT approximately 50% have an identifiable
inherited thrombophilic disorder
Cushman, Hematology. 2005 (1) 452
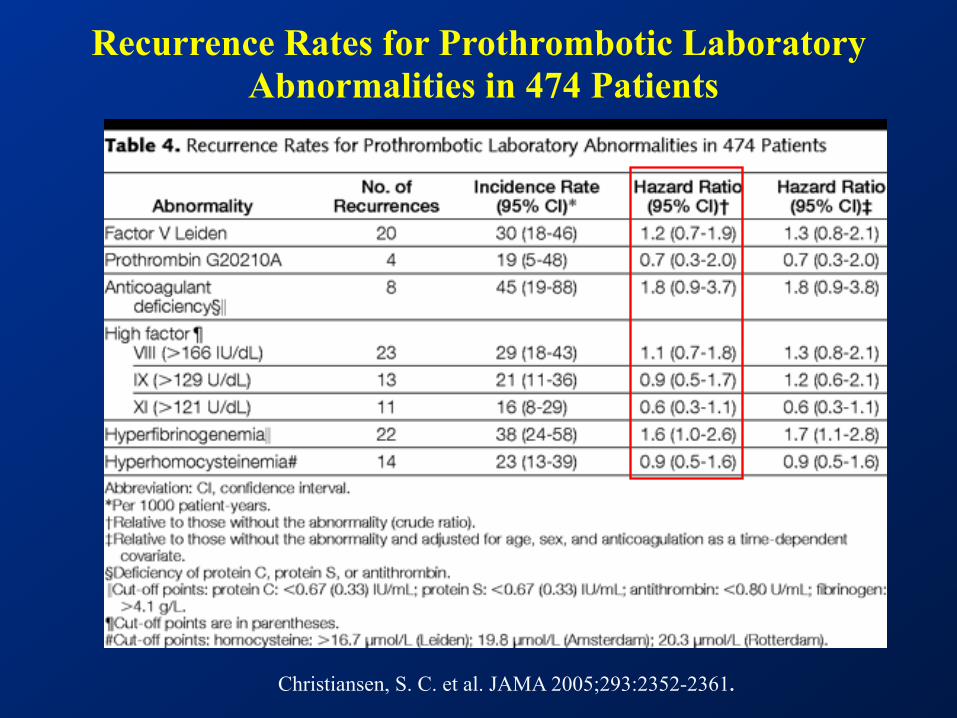
Christiansen, S. C. et al. JAMA 2005;293:2352-2361.
Recurrence Rates for Prothrombotic Laboratory Abnormalities in 474 Patients
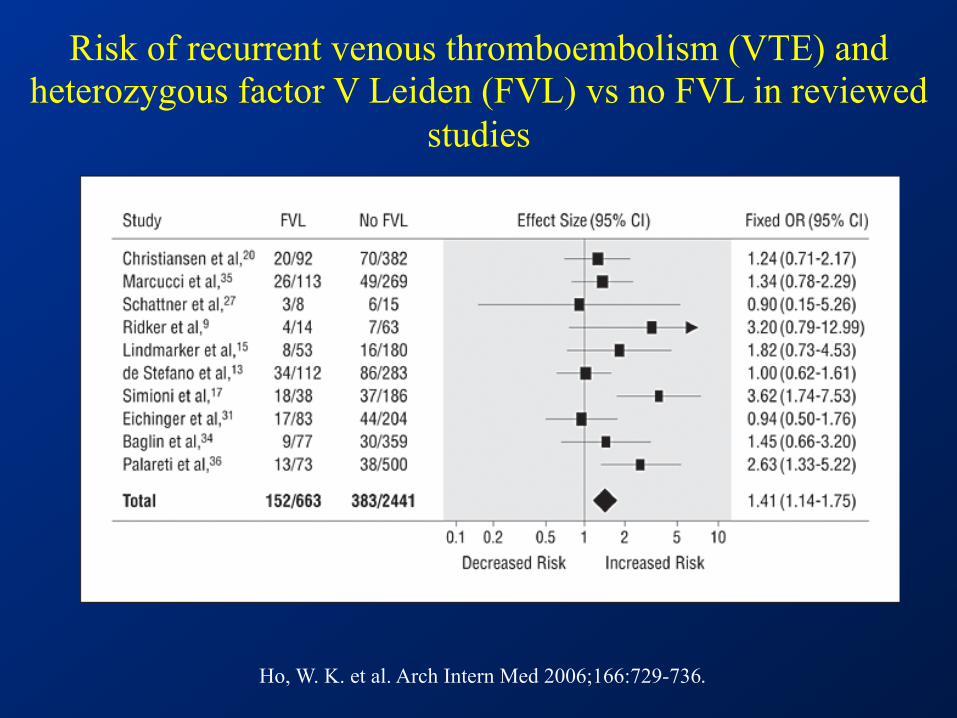
Ho, W. K. et al. Arch Intern Med 2006;166:729-736.
Risk of recurrent venous thromboembolism (VTE) and heterozygous factor V Leiden (FVL) vs no FVL in reviewed
studies
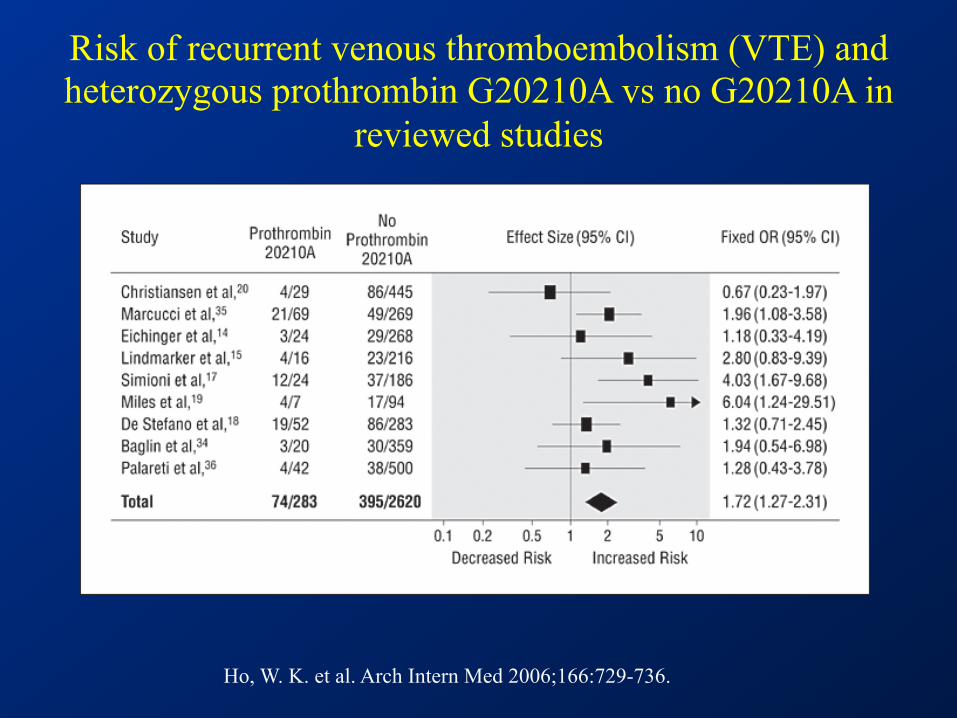
Ho, W. K. et al. Arch Intern Med 2006;166:729-736.
Risk of recurrent venous thromboembolism (VTE) and heterozygous prothrombin G20210A vs no G20210A in
reviewed studies
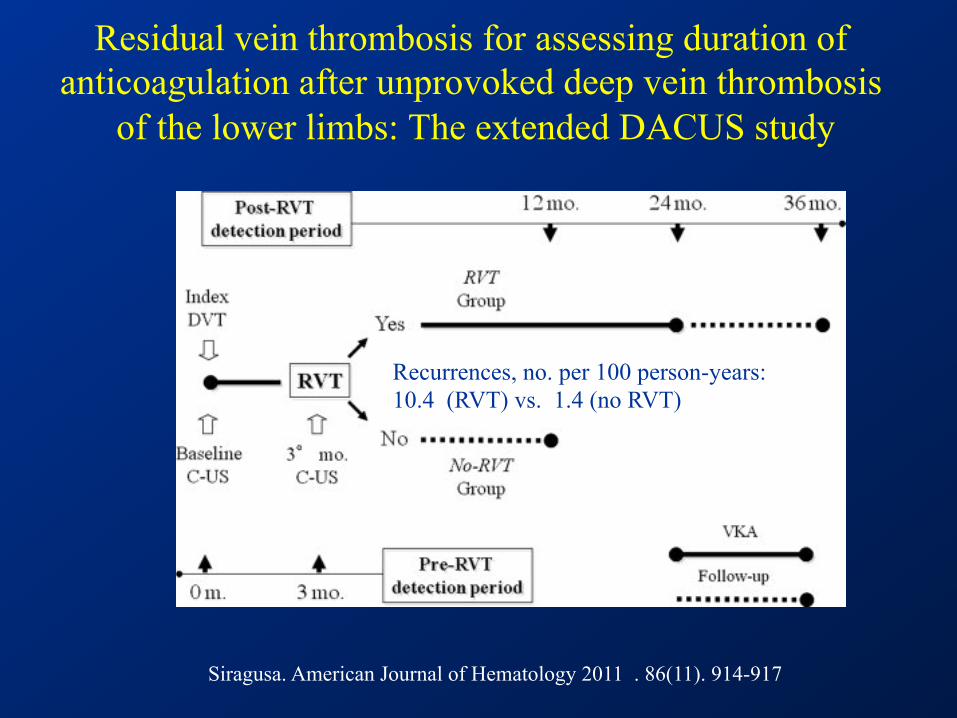
Residual vein thrombosis for assessing duration of anticoagulation after unprovoked deep vein thrombosis
of the lower limbs: The extended DACUS study
Siragusa. American Journal of Hematology 2011 . 86(11). 914-917
Recurrences, no. per 100 person-years: 10.4 (RVT) vs. 1.4 (no RVT)
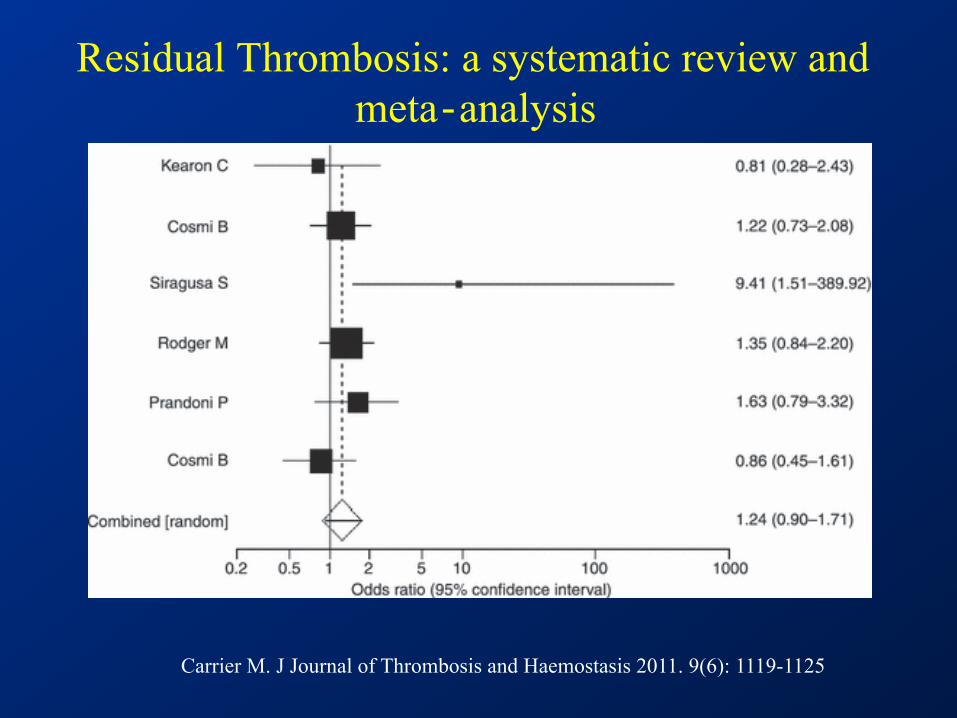
Residual Thrombosis: a systematic review and meta‐analysis
Carrier M. J Journal of Thrombosis and Haemostasis 2011. 9(6): 1119-1125
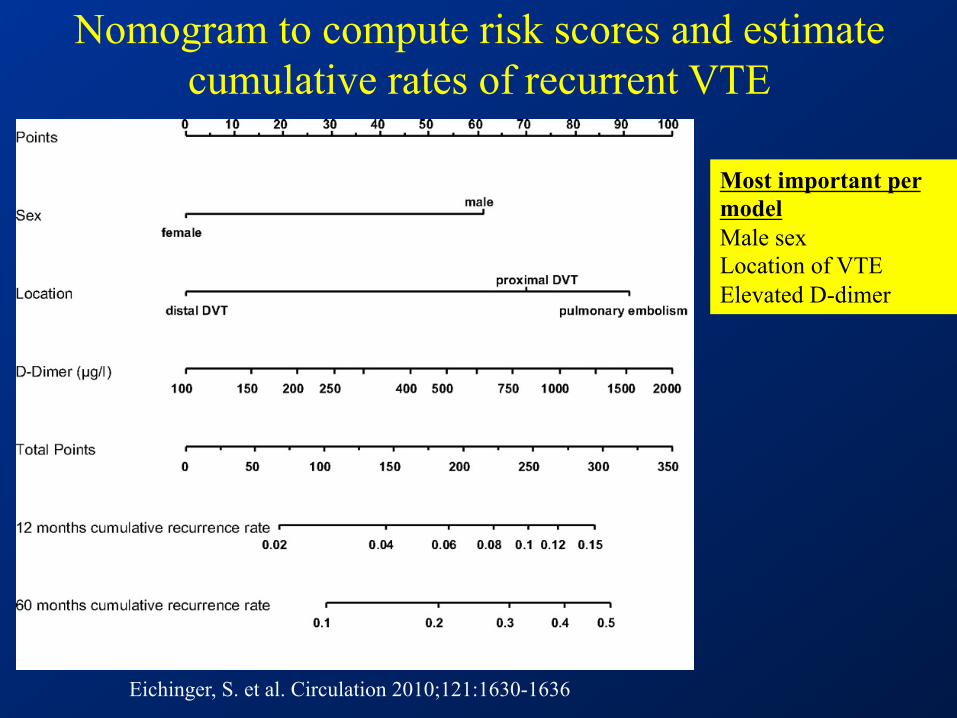
Eichinger, S. et al. Circulation 2010;121:1630-1636
Nomogram to compute risk scores and estimate cumulative rates of recurrent VTE
Most important per model Male sex Location of VTE Elevated D-dimer
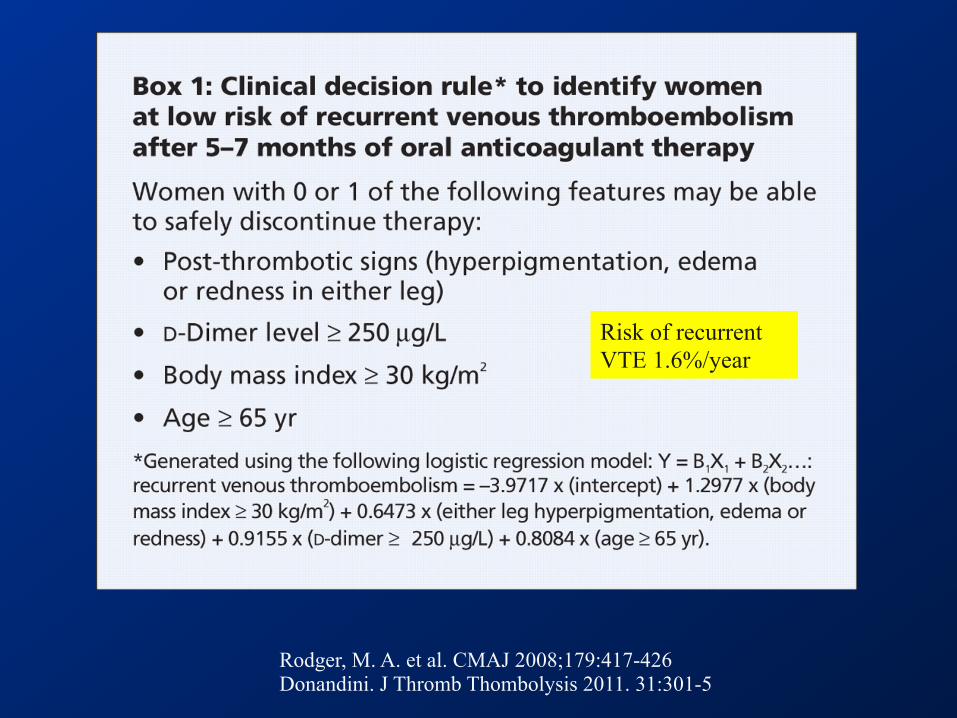
Rodger, M. A. et al. CMAJ 2008;179:417-426 Donandini. J Thromb Thombolysis 2011. 31:301-5
Risk of recurrent VTE 1.6%/year
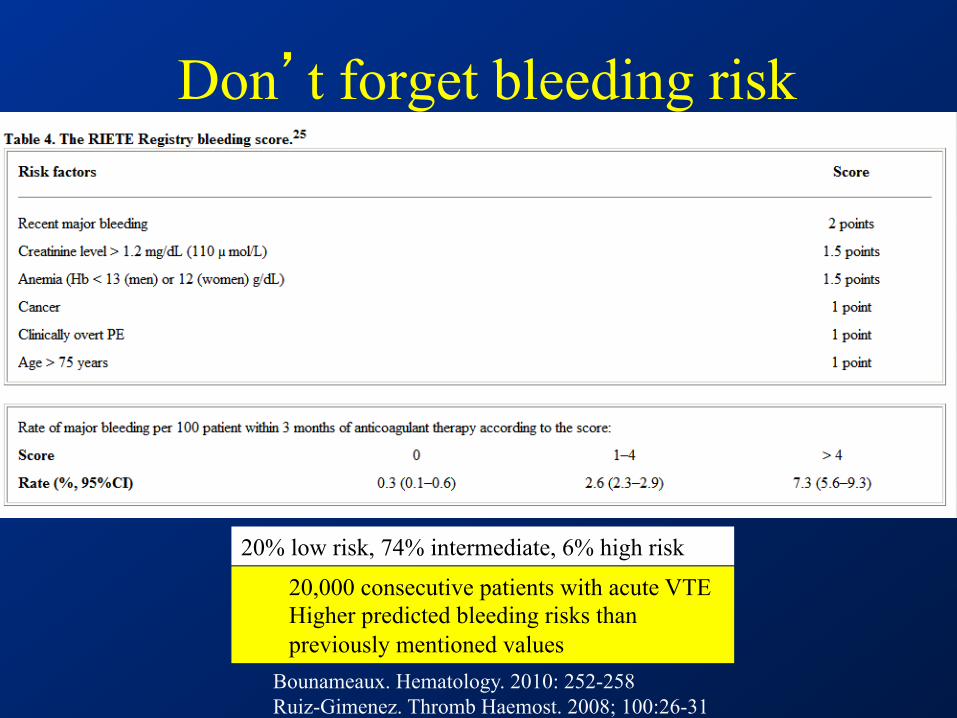
Don’t forget bleeding risk
20,000 consecutive patients with acute VTE Higher predicted bleeding risks than previously mentioned values
Bounameaux. Hematology. 2010: 252-258 Ruiz-Gimenez. Thromb Haemost. 2008; 100:26-31
20% low risk, 74% intermediate, 6% high risk
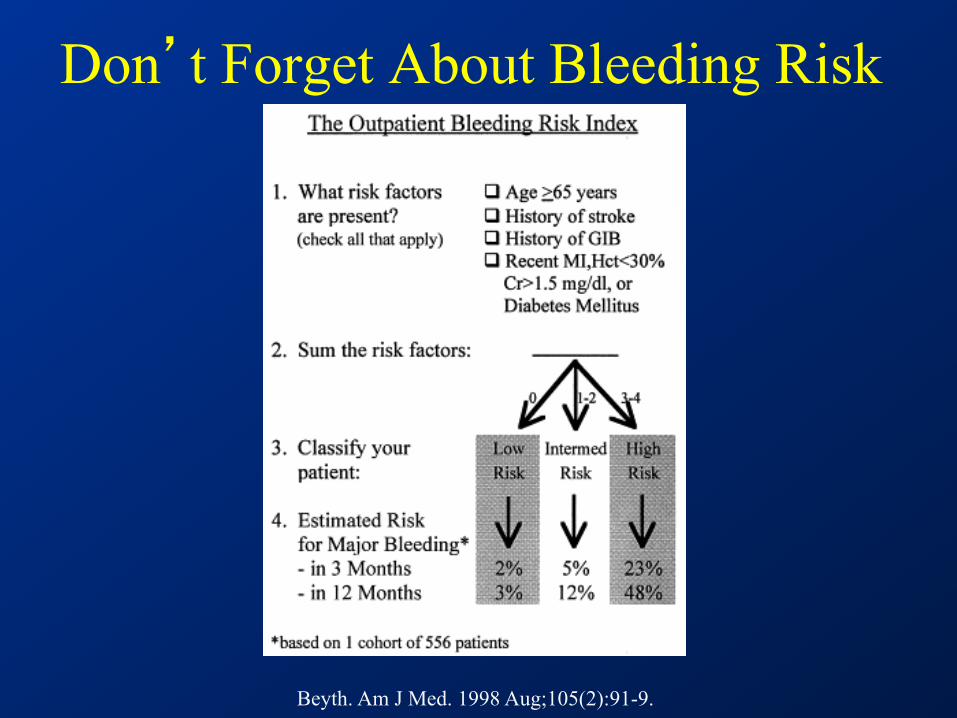
Don’t Forget About Bleeding Risk
Beyth. Am J Med. 1998 Aug;105(2):91-9.
Case • 51 year-old previously healthy male seeks consultation for
anticoagulation recommendations – Idiopathic femoral vein clot 3 months prior – Tolerating warfarin well with mostly therapeutic INR values – No prior or family history of thrombosis – Up to date on PSA testing and colonoscopy – Nl cbc, electrolytes, LFTs
• Additional testing – D-dimer 620 ug/L – Repeat doppler showed resolution of DVT – No thrombophilia testing performed
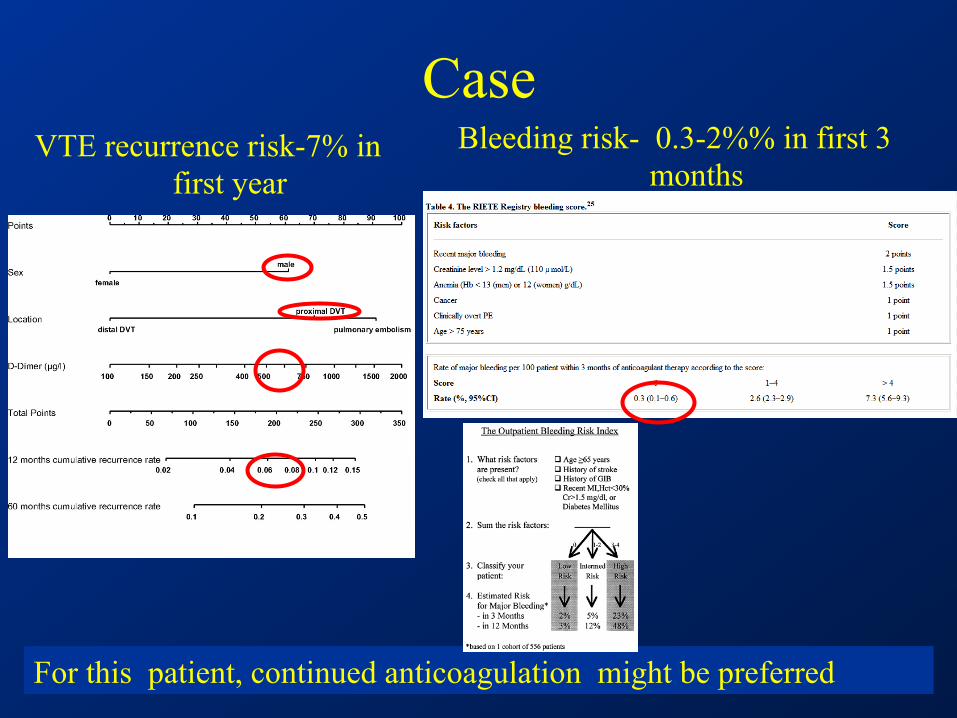
Case VTE recurrence risk-7% in
first year Bleeding risk- 0.3-2%% in first 3
months
For this patient, continued anticoagulation might be preferred
Conclusions • Idiopathic VTE is a chronic condition
– Risk of recurrence remains after discontinuation of anticoagulation
– Treat for 3 months at a minimum – Consider indefinite anticoagulation based on:
• VTE recurrence risk • Bleeding risk • Patient preference
• New oral anticoagulants may change the paradigm • Extended ECASA therapy may be an option
ASH 2011. Abstract 543
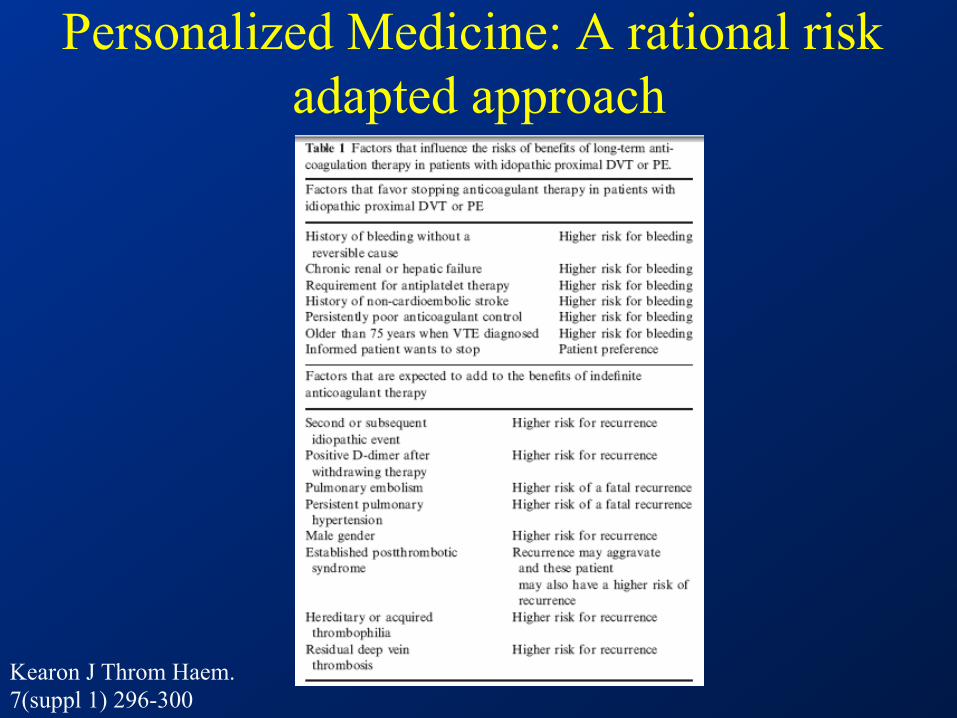
Personalized Medicine: A rational risk adapted approach
Kearon J Throm Haem. 7(suppl 1) 296-300
Computer generated risk assessments ??
What are the benefits of genetic testing
• Subset of patients are at higher risk for recurrent VTE – Anticoagulation will substantially reduce this risk – Testing can help reduce the bleeding risk for those at low risk
• Improved patient understanding of thrombosis – Increased understanding improves QOL – Better done in specialized thrombosis clinics
• Affords the opportunity for family testing – Controversial – Most important to young females considering OCT or pregnancy
Middeldorp. J Thromb Thrombolysis. 2001. 31:275-81
Arguments against genetic testing • Laboratory error/false diagnosis
– Protein C, Protein S, AT-III
• Psychological effects
• Insurance Issues
• Often does not change treatment recommendations
– Idiopathic cases may be anticoagulated long-term no matter what the results
– Strong reversible provocation likely will receive finite anticoagulation no mater the results
– Anyone with an initial VTE should receive aggressive prophylactic anticoagulation with all future risks
Middeldorp. J Thromb Thrombolysis. 2011. 31:275-81