Embed Size (px)
Citation preview

Aus
tral
asia
n Ps
ychi
atry
• V
ol 1
2, N
o 1
•
Mar
ch 2
004
36
RURAL AND REMOTE PSYCHIATRY
RURAL and REMOTE PSYCHIATRY
Identifying marginal housing for people with a mental illness living in rural and regional areas
Margaret Grigg, Fiona Judd, Lisa Ryan and Angela Komiti
Objective:
Homelessness among people with a mental illness is a seriousissue. The purpose of the present study was to identify the types of housingavailable for people with a mental illness in the region, to develop an audittool to assess the housing of patients of the mental health service, and topilot this audit tool.
Methods:
Key informants were interviewed to obtain information about thetype of housing options available in the Loddon Campaspe Southern MalleeRegion, Victoria, Australia. This information was used to develop a survey toaudit the housing status of existing patients of the area mental health service.A pilot study using the survey was completed by case managers for 81 patientswho were being case managed by the area mental health service
Results:
There was a wide variety of housing options in the region buthousing availability was not evenly distributed. Although most patients livedin owned or rented accommodation, a substantial proportion of patients haddifficulties with accessing the required services, the affordability of their hous-ing, uncertainty of tenure or were at risk of violence within their housing.
Conclusions:
A substantial proportion of patients treated by a rural areamental health service had lived in impoverished housing.
Key words:
homelessness, mental illness, rural psychiatry.
omelessness has been widely researched over the past two decadesyet there is no consistent definition of the term. Most agree thathomelessness refers to more than just a lack of residence. Inade-
quate, unsafe or temporary housing is a form of homelessness.
1
People may be transiently, episodically, or chronically homeless
2
and sohomelessness may consist of a series of states that exists along acontinuum of time and place. Furthermore, entry to or exit from thehomeless state is commonly part of a process rather than a sudden orisolated event.
In Australia, cultural standards of adequacy and acceptability are impor-tant components of the definition of homelessness. For the purpose of
The Supported Accommodation Assistance Act No. 162 1994
,
3
homelessnessis defined as follows.
A person is homeless if, and only if, he/she has inadequate access to safeand secure housing. A person is taken to have inadequate access to safe andsecure housing if the only housing to which the person has access:(a) damages, or is likely to damage a person’s health; or (b) threatens aperson’s safety; or (c) marginalizes the person by failing to provide:adequate personal amenities; or economic and social support that a homenormally affords; or (d) places the person in circumstances which threaten oradversely affect adequacy, safety, security and affordability of that housing.
Marginal accommodation has been used to refer to residential accom-modation that is affordable on a pension and characterized by a lack of
Margaret Grigg
Psychiatric Nurse, Centre for Rural Mental Health, Bendigo Health Care Group, Bendigo and School of Health and Environment, Latrobe University, Bendigo, Vic., Australia.
Fiona Judd
Consultant Psychiatrist, Centre for Rural Mental Health, Bendigo Health Care Group, Bendigo and School of Psychology, Psychiatry and Psychological Medicine, Monash University, Vic., Australia.
Lisa Ryan
Social Worker, Centre for Rural Mental Health, Bendigo Health Care Group, Bendigo, Vic., Australia.
Angela Komiti
Research Assistant, Centre for Rural Mental Health, Bendigo Health Care Group, Bendigo and Department of Psychiatry, University of Melbourne, Vic., Australia.
Correspondence
: Professor Fiona Judd, Centre for Rural Mental Health, Bendigo Health Care Group, PO Box 126, Bendigo, Vic. 3552, Australia.Email: [email protected]
H

Australasian Psychiatry
• Vol 12, N
o 1 •
March 2004
37
secure tenure, little privacy, and shared kitchen andbathroom facilities. In urban areas this includesliving in a rooming house, boarding house, hostel,hotel/rented room, emergency accommodation, andshelters for the homeless.
4
In rural areas, other formsof housing such as caravan parks and houseboatsneed to be added to the list. This concept is consist-ent with the aforementioned broad definition ofhomelessness and enables the development of acommonsense continuum of categories of accommo-dation (Table 1).
Homelessness is the result of a number of differentfactors. These include housing-related factors such aslack of affordable housing, economic causes, andgovernment policies. In addition, personal circum-stances such as a mental illness, family breakdown orpropensity to addiction contribute to the risk ofhomelessness.
5
In recent years, changes in the factorscontributing to homelessness have seen a decline inthe proportion of older men experiencing homeless-ness and an increase in homelessness among singlewomen, families and young people.
6
Although there is substantial evidence highlightingthe prevalence of mental illness among people whoare homeless, and effective interventions for prevent-ing homelessness among mentally ill people andpromoting housing stability for those people who
become homeless, the majority of research has beenconducted in urban environments. For example,a study in inner Melbourne found that almost half ofthe residents of three marginal accommodation ser-vices (shelters for homeless people, special accom-modation houses, and low-cost rooming houses)received diagnoses of a current mental disorder, while70% received a lifetime diagnosis.
7
In a more recentAustralian study, 75% of people interviewed in emer-gency accommodation had at least one mental dis-order.
8
Homeless mentally ill people with psychoticdisorders tend to have high rates of previous contactwith traditional psychiatric services, but poor currentcontact and low rates of psychotropic medicationuse.
9
Specialist services for homeless people, includ-ing outreach services, can enhance contact withmental health services.
10
Effective treatment forpeople with psychotic disorders early in their illnesscan prevent homelessness.
11
Services most likely to beused by homeless people with mental illness are thosethat have adapted service delivery and treatmentapproaches in view of the experiences and reports oftheir homeless clients.
12
By contrast, very little is known about the prevalenceof homelessness among people who are mentally illin regional and rural communities. The present studyaimed to (i) identify the housing options availablefor people with a mental illness in a regional/ruralsetting in Victoria; (ii) develop an audit tool to assessthe housing status of current patients of the mentalhealth service in that region; and (iii) pilot the audittool with a community mental health team.
SETTING: LODDON CAMPASPE SOUTHERN MALLEE REGION
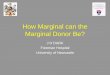
The Loddon Campaspe Southern Mallee Region islocated in North Central Victoria (Figure 1). Theregion stretches from Gisborne in the south to
Figure 1: Map of Victoria showing Loddon Campaspe
Southern Mallee Region.
Mildura
Ouyen
Wodonga
Sale
SheppartonEchuca
Swan Hill
Bendigo
Castlemaine
Ballarat
Horsham
Ararat
GeelongWarrnambool
MELBOURNEHamilton
Table 1: Continuum of categories of accommodation
Category Accommodation
Institution HospitalNursing homeCommunity care unitsPrison
Supported Residential disability support servicesGroup home
Marginal Rooming houseBoarding houseHostelHotel/rented roomEmergency accommodationShelters for the homelessLiving with friendsCaravan park, houseboatNo fixed address
Rented Private rentalPublic housing
Own home Own homeFamily home
Source: adapted from ref.
4

Aus
tral
asia
n Ps
ychi
atry
• V
ol 1
2, N
o 1
•
Mar
ch 2
004
38
beyond Swan Hill in the north and has a populationof approximately 241 000 people. The regionincludes communities with diverse social, culturaland economic characteristics.
The central sector includes the regional city ofBendigo and surrounding suburbs and has a popula-tion of 97 136. The northern sector includes thetownships of Swan Hill, Echuca and Kerang with apopulation of 71 744. It is characterized by signifi-cant areas of socioeconomic disadvantage and has asignificant proportion of Indigenous residents. Thesouthern sector includes rural townships such asCastlemaine and Kyneton and the urban fringeregions of Gisborne, Woodend and Macedon with apopulation of 72 118.
13
METHOD
Information on housing
Key informants who worked with homeless peopleand/or people with a mental illness were interviewedto obtain information about the housing options,including marginal housing, for people with a mentalillness. These informants included representativesfrom housing and tenancy support services, crisishousing services, clinical mental health and disabilitysupport services. A semistructured interview schedulewas developed to guide the interviews. Informantswere identified in a sequential manner, beginningwith identifiable ‘experts’. Interviews continued untildata saturation occurred. Further information wasobtained from an audit undertaken by the LoddonMallee Supported Accommodation and AssistanceProgram (SAAP) Network in 2002 of the types ofhousing to which people sometimes have access inthe Region, and from the 2001 Census data collectedby the Australian Bureau of Statistics.
Survey development
Information from the key informant interviews wasused to develop a survey to audit the housing statusof existing patients of the mental health service.The survey included the demographics of the patient(gender, age, treating team); the housing type (forexample, rented flat, public housing, caravan); theliving arrangements of the patient (that is, who theyhad been living with over the last 2 weeks); housingcharacteristics as assessed by the patient’s case man-ager (affordability of housing, risk of violence, secu-rity of tenure, ability to access services, structuralsafety of the housing, and appropriateness of thehousing to the patient’s needs); and an overall assess-ment by the case manager of the impact that thehousing would have on the patient’s mental disorder.Assessment of the housing characteristics was madeby using a visual analogue scale. Each characteristicwas rated on a five-point scale from 0 ‘never true’ to4 ‘always true’.
Pilot of survey
The survey was completed by case managers in thecontinuing care and intensive case managementteams located in the central region (Bendigo). Theseteams mostly care for patients with psychotic andsevere affective disorders, often with comorbid sub-stance abuse. Case managers were asked to completethe housing audit on all patients seen during a 2 weekperiod in January 2003. Where clients lived in morethan one address during the period, both housingtypes/situations were listed.
In determining whether a property was affordable,case managers made a judgement guided by theapproach used by the Office of Housing. Thisapproach considers as affordable the properties thatare within 30% of income including rent assistancefor low-income households that will not be over-crowded. Other judgements about housing character-istics were made by the case manager based on theirknowledge of the patient and the geographical loca-tion of their housing.
14
RESULTS
Information on housing
Housing options in the region, other than privateowned/rented house/flat included public housing,community housing (such as group housing, transi-tional housing, and crisis housing managed by non-government organizations on a not-for-profit basis),caravan parks, motels and hotels. The number ofpublic housing properties varied markedly across theregion (north, n = 1605; central, n = 1810; south,n = 651). In addition, there were large numbers ofpeople on waiting lists for these properties (north,n = 466; central, n = 980; south, n = 201). There isalso very limited supported accommodation avail-able. Richmond Fellowship has one property provid-ing residential disability support services in Bendigofor 10 residents and there is a limited number ofproperties where support is provided by SAAPworkers. Marginal housing options include a range ofcommunity housing properties, caravan parks, house-boats, motels, hotels and hostels. Table 2 shows thenumber of properties in each of these categories.
Pilot survey
The pilot survey was completed for 81 patients(n = 36, 44% male; n = 45, 66% female; average age:38.5 years) who were seen by a case manager. Thissample was similar to the current clients (n = 143,56% male; n = 113, 44% female) managed by bothteams.
As shown in Table 3, the majority of clients lived ina private house or flat, either rented or owned (28%and 42%, respectively). Two case-managed clientswere residing in sheds during the audit period.

Australasian Psychiatry
• Vol 12, N
o 1 •
March 2004
39
The living arrangements of the patients varied(Table 4). Where clients resided in more than oneaddress during the audit, both housing types werelisted. Most patients lived with family (40%), either aparent, child or other. One-third lived alone, 11%with partner and 13% with co-tenants or friends.
Ratings of housing characteristics revealed that broadlymore than two-thirds of patients had housing that wasaffordable, secure, safe and appropriate to their needs.Of concern, 16% reported problems with affordabilityof housing, 12% reported uncertainty regarding tenureof housing, and 4% expressed concerns regarding‘structural stability’. One-third reported difficultyaccessing services, 15% reported that the housing didnot meet their physical needs, and 14% reported thatthey were at risk of violence in their household.
As expected, affordability of housing varied accordingto type of housing. Greatest difficulty was reportedby those renting accommodation; 22% of thosein private rental properties and 18% of those inpublic housing were judged to have problems withaffordability.
The majority of those living alone were in privatelyrented accommodation (12/29, 41%), in rented pub-lic housing (7/29, 24%) or privately owned accommo-dation (7/29, 24%). The majority of those living withfamily or partner were in privately owned accommo-dation (13/19, 68%; and 7/9, 78%; respectively). Theoverall rating by case managers of the effect ofcurrent housing on the patient’s mental health wasthat in most instances housing did not contribute tothe patient’s mental illness.
Table 2: Marginal housing in the Loddon Campaspe Southern Mallee Region
Northern Central Southern
Community housing (total) 213 147 96Rooming houses 0 2 0Local Government community housing properties 41 24 45Group housing 2 15 1Interim/long-term housing 9 5 3Aboriginal Housing Board properties 135 25 0Transitional housing 17 68 45Crisis and refuge housing 9 8 2
Caravan parks 14 20 3Motels and hotels 40 70 27Hostels 1 0 0Population of area 71 744 97 136 72 118
Table 3: Housing type of case management patients (n = 81)
n %
Private house/flatOwned 34 42Rented 23 28
Department of Housing: rented 11 14Supported residential service 7 9Co-op rental residence 1 1Aged care hostel 1 1Shed 2 2Missing 2 2
Total 81 100
Table 4: Living arrangements of case management patients (n = 81)
n %
Lives alone 29 35Lives with family (parent) 19 23Lives with family (child) 11 13Lives with family (other) 4 4Lives with co-tenants/residents 9 11Lives with partner 9 11Lives with friends 2 2
Total 83 100
The total is >81 because two participants lived in more than one addressduring the audit period.

Aus
tral
asia
n Ps
ychi
atry
• V
ol 1
2, N
o 1
•
Mar
ch 2
004
40
DISCUSSION
The low prevalence component of the NationalSurvey of Mental Health and Wellbeing definedmarginal accommodation as ‘residential accommoda-tion affordable on a pension and characterized by alack of secure tenure, little privacy and sharedkitchen and bathroom facilities’ (p. 30).
4
The studyincluded rooming houses, boarding houses, hostels,emergency accommodation, and homeless shelters,and those in the situation of being roofless in thisdefinition. Although such a definition may be con-sistent with urban marginal housing models, in therural communities caravan parks and houseboatswere more common. The type of marginal housingavailable to people with a mental disorder reflects thecharacteristics of the community in which they areliving.
The study has revealed that there is a lack of appro-priate and affordable housing in the Loddon Cam-paspe Southern Mallee Region of Victoria. Not onlywas there insufficient housing as exemplified by thenumbers on waiting lists to access public housing, butthe housing that was available was inequitably dis-tributed. The variation in the housing availabilitywithin the region highlights the diversity of rural andregional areas. Even within one area mental healthservice catchment area, differences in housing typeand affordability were noted. Not surprisingly, areasoutside Bendigo had fewer housing options than theregional centre of Bendigo.
The relatively high proportion of patients living inDepartment of Housing accommodation (14%) andlow proportion of people who were living in theirown or privately rented accommodation in thepresent study was consistent with previous studies.
15
The National Survey of Mental Health and Well-being’s low prevalence study, undertaken in urbancatchment areas, found that of those interviewed,24% were living in marginal accommodation mostrecently or at some point in the past year. Our study,of a regional centre (Bendigo) and surrounding sub-urbs, found that many more people lived in their ownhome (house/flat) or rented premises than in the lowprevalence study (84% vs 54%). Despite this, manywere in marginal accommodation due to one or moreof lack of secure tenure, marginalization from amen-ities, lack of safety and detrimental effects on health.
Despite the impoverished housing circumstances ofmany patients included in the present study, mostcase managers did not state that the patient’s housinghad an effect on the patient’s mental disorder. Casemanagers appear to be either desensitized to impov-erished housing conditions of their patients and/orunaware of the relationship between housing qualityand mental health. It is essential that effectivetraining and education programmes are developed to
ensure that case managers use effective strategies tomaximize the quality of their patients’ housing.
There are a number of limitations of this pilot study.The study was concentrated in the regional city ofBendigo. It is not known whether the housingcircumstances of patients living in rural areas arebetter or worse than those in a regional city. Asignificant proportion of the patients in the pilotstudy were receiving intensive case management.The intensity of the programme and focus onpsychosocial support may have a positive impact onthe patients’ housing circumstances and so thesefindings may not be generalizable to other case-managed clients. The study is currently beingextended to include all mental health teams in theregion, including the inpatient unit. Finally, thestudy relied on information from professionals. It isnot known whether patients’ self-reports would haveyielded similar results.
CONCLUSION
The marginal housing construct assists in exposingthe impoverished housing circumstances of manypatients who are treated by an area mental healthservice. The housing options for patients with amental disorder living in a large rural and regionalarea varied. Although the majority of patients lived intheir own or rented accommodation, a substantialnumber of patients who were being case managedexperienced difficulties with accessing services,affordability of housing, were not able to stay in theirhousing as long as they wanted to or were at risk ofviolence, and so appeared to be living in housing thatcould be defined as marginal.
In response to the issues of homelessness amongpeople with a mental illness, the Loddon SouthernMallee Region has recently commenced a project toprevent people with a mental illness being dischargedinto homelessness; this has been funded by theVictorian Homelessness Strategy. The project is a jointinitiative of the area mental health service, disabilitysupport services and homelessness services in theregion. The project aims to facilitate care pathwaysbetween the area mental health service, psychiatricdisability support services and Supported Accommo-dation Assistance Program-funded agencies. Dischargeplanning from the inpatient unit and education andtraining are key features of the initiative.
ACKNOWLEDGEMENTS
This study was funded by a Latrobe University Bendigo Larger Grants Scheme grant.
REFERENCES
1. Lipton F, Sabatini A. Constructing support systems for homeless chronic patients.In: Lamb H, ed.
The Homeless Mentally Ill. A Taskforce Report of the AmericanPsychiatric Association
. Washington, DC: American Psychiatric Association, 1984;153–172.

Australasian Psychiatry
• Vol 12, N
o 1 •
March 2004
41
2. Arce A, Vergare M. Identifying and characterizing the mentally ill among thehomeless. In: Lamb H, ed.
The Homeless Mentally Ill. A Taskforce Report of theAmerican Psychiatric Association
. Washington, DC: American Psychiatric Associa-tion, 1984; 75–89.
3.
Supported Assistance Act no.
162
1994.
4. Harvey C, Evert H, Herman H, Pinzonem T, Gureje O.
Low Prevalence DisorderComponent of the National Study of Mental Health and Wellbeing Bulletin 5: Disability,Homelessness and Social Relationships Among People Living with Psychosis inAustralia.
Canberra: Commonwealth Department of Health and Ageing, 2002.
5. Lipton F, Nutt S, Sabatini A. Housing the homeless mentally ill: a longitudinal studyof a treatment approach.
Hospital and Community Psychiatry
1988;
39
: 40–45.
6. Victorian Homelessness Strategy Ministerial Advisory Committee.
BuildingSolutions for Individuals and Families Who Experience Homelessness: Workingreport of the Victorian Homelessness Strategy.
Melbourne: Victorian GovernmentDepartment of Human Services, 2001.
7. Herman H, McGorry P, Bennett P, van Riel R, Singh B. Prevalence of severe mentaldisorders in disaffiliated and homeless people in inner Melbourne.
AmericanJournal of Psychiatry
1989;
146
: 1179–1184.
8. Hodder T, Teeson M, Buhrich N.
Down and Out in Sydney: Prevalence of MentalDisorders, Disability and Health Use Among Homeless People in Inner Sydney
.Sydney: Sydney City Mission, 1998.
9. Herman H, McGorry P, Bennett P, Varnavides K, Singh B. Use of services by homelessand disaffiliated individuals with severe mental disorders: a study in Melbourne.In: Cooper B, Eastwood R, eds.
Primary Health Care and Psychiatric Epidemiology
.London: Tavistock/Routledge, 1992; 142–159.
10. Buhrich N, Teeson M. Impact of a psychiatric outreach service for homeless personswith schizophrenia.
Psychiatric Services
1996;
47
: 644–646.
11. Herman DB, Susser ES, Jandorf L, Lavelle J, Bromet J. Homelessness amongindividuals with psychotic disorders hospitalized for the first time: findings from theSuffolk county mental health project.
American Journal of Psychiatry
1998;
155
:109–113.
12. Goldfinger SM, Schutt RK. Housing placement and subsequent homelessness amongformerly homeless adults with mental illness.
Psychiatric Services
1999;
50
:674–679.
13. Australian Bureau of Statistics.
2001 Census of Population and Housing
. Canberra:Australian Bureau of Statistics, 2001.
14. Chamberlain C.
Homelessness in Victoria: A Report Prepared for the Office ofHousing
. Melbourne: Department of Human Services, 2000.
15. Lake P. Preventing homelessness among public tenants. In: 3rd National Home-lessness Conference ‘Beyond the Divide’, Brisbane 6–8 April 2003. AustralianFederation of Homelessness Organisation, 2003.