Embed Size (px)
Citation preview
Identifying & Managing Oral Health Conditions of the Aging Patient
Nels Ewoldsen DDS, MSD
Louisiana Primary Care Association 3rd Annual Clinical Summit
New Orleans Convention Center 2016
Conflict of Interest Disclosure
• I have no financial interest in any of the products or techniques featured in the presentation
• I own no stock in any dental or dental product company
• I have no ongoing sponsorship or speaker funding relationship with any dental company
• I am a member of the Catapult Group, Chicago, IL and evaluate dental products for Catapult
• I am former Clinical Research Director Dentsply Prosthetics (2002-2012) & Directed Technology Transfer GC Corp. (1999-2002)

Nels Ewoldsen DDS, MSDConservative Dental SolutionsWaveland, Indiana (population 420)


Aging in America (& the world)……
Oral Conditions = Caries, Periodontal Disease, Mucositis & Tooth Loss
- Managing Acute Caries & Workforce Expansion
-Biofilm Management (Candidiasis, Pneumonia, Caries)
-Saliva Management (saliva substitutes, pilocarpine, cevimeline)
-Managing Edentulism (Partial & Complete) New Techniques/Technology

Oral Health Needs of the Frail ElderlyFrailty: various levels of dependency resulting from impaired neurologic control & energy levels below a critical threshold
(MacEntee MI, J Canadian Dent Assn 2006) “We must seek simple, relatively inexpensive solutions to tooth loss” …..”chronic, non-communicable impairments including caries, periodontitis,
mucositis & tooth loss constitute the biggest challenge to health care systems everywhere.”
Dr. Margaret Chan (Director-General WHO) “the rising financial burdens of these diseases will reach levels beyond the capacity of even the wealthiest countries in the world to manage”

Coronal polishing, mechanical toothbrushing…………..prior to the oral examination
Midwest RDH Freedom Cordless Prophy System
…yes we do house calls
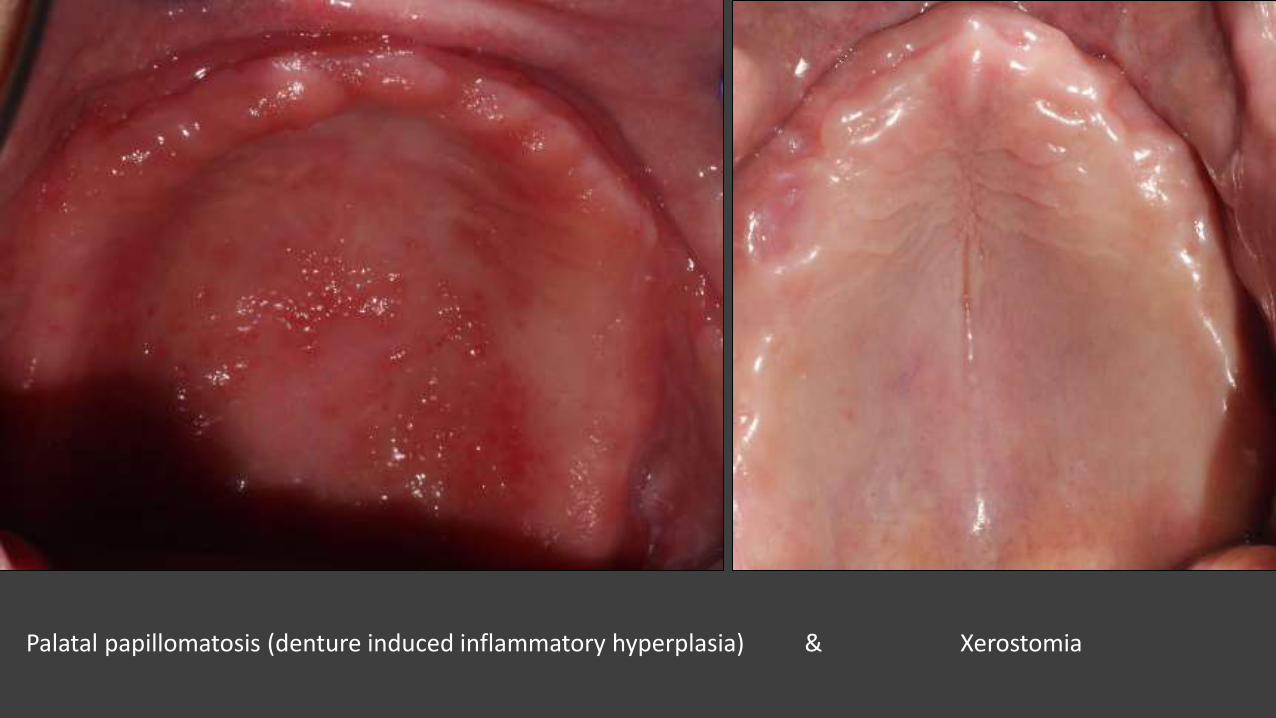
Palatal papillomatosis (denture induced inflammatory hyperplasia) & Xerostomia
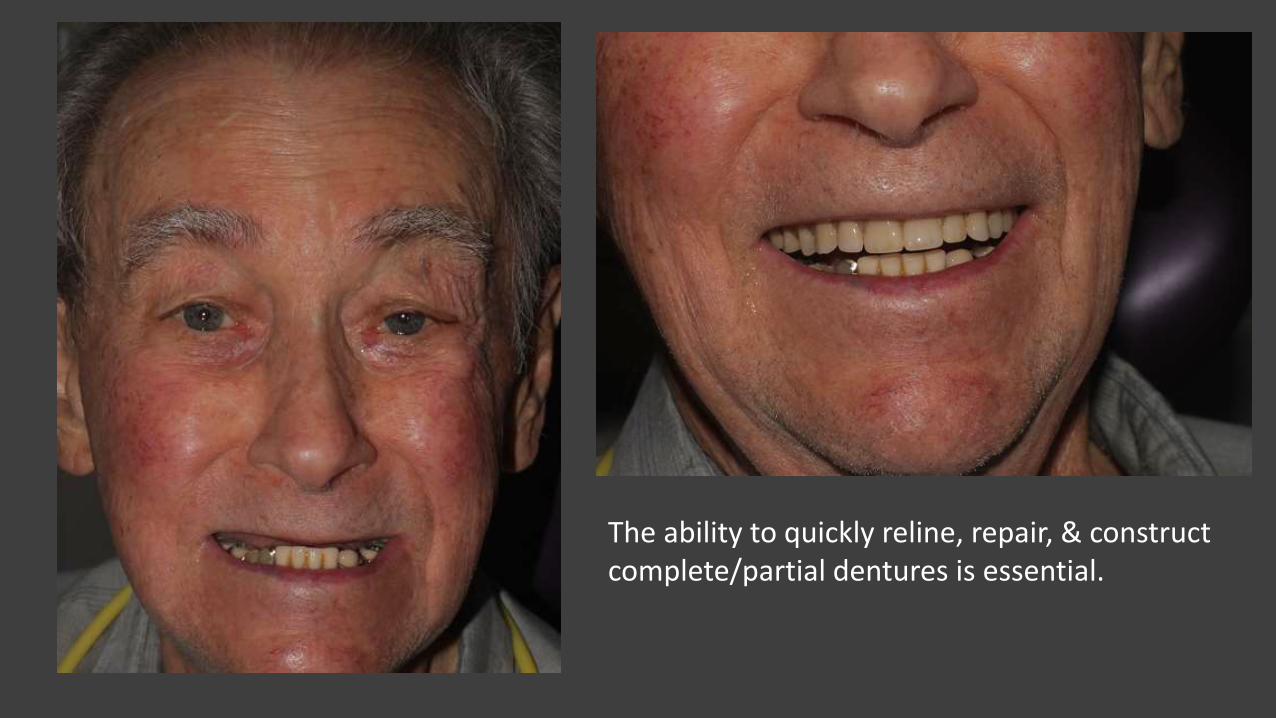
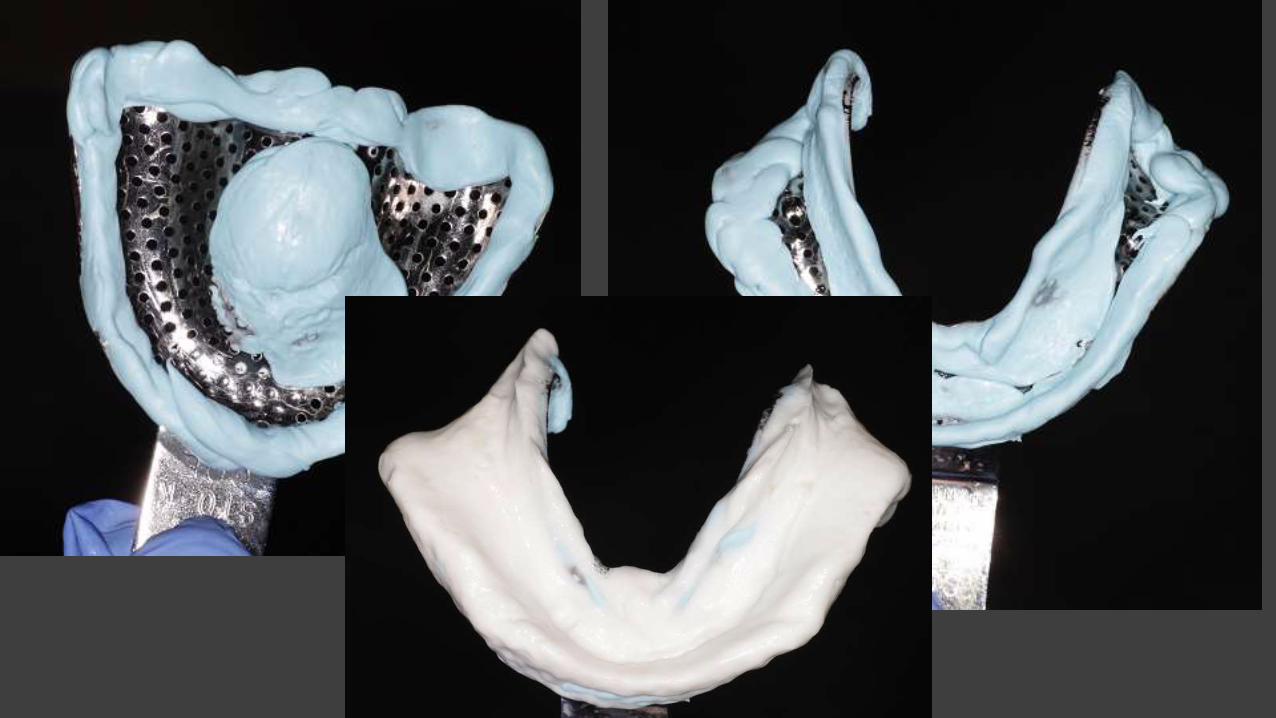
The ability to quickly reline, repair, & construct complete/partial dentures is essential.

“If partially and completely edentulous elderly cannot afford anything other than acrylic-resin prostheses…prosthodontics must provide access to simpler, sound treatment.” P. Owen, 2015 ICP Special Session on Geriatrics


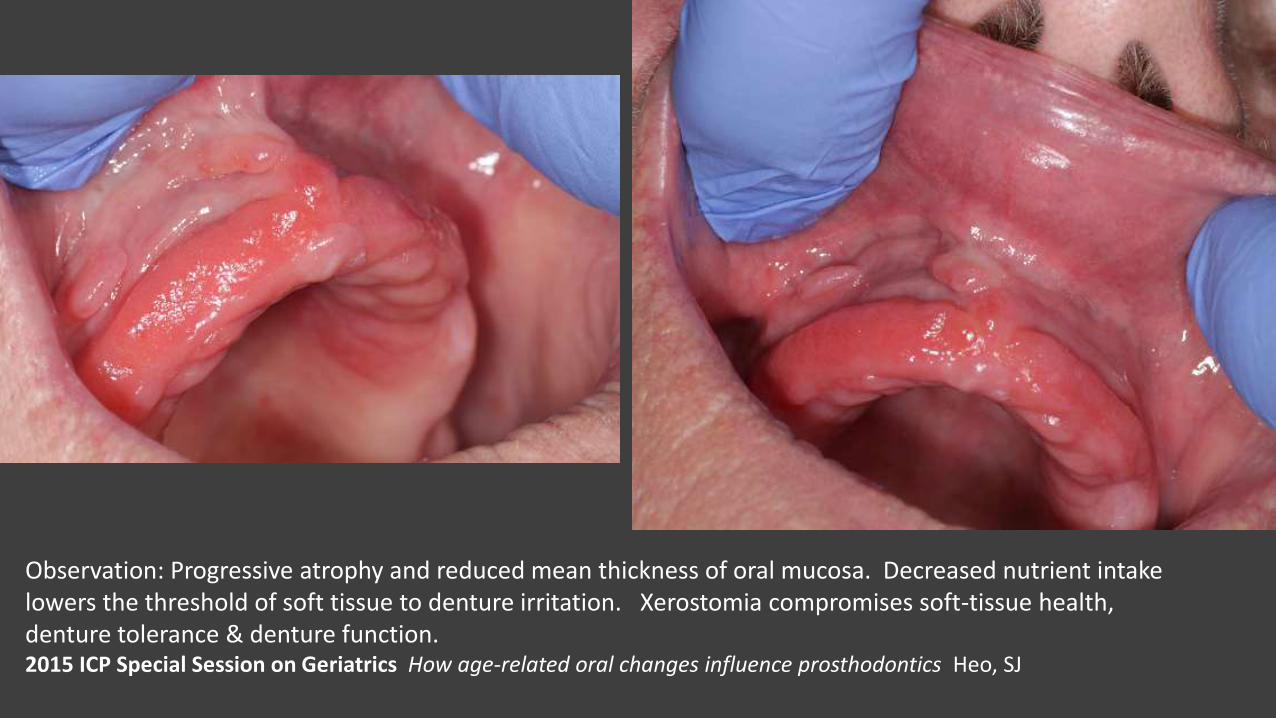
Observation: Progressive atrophy and reduced mean thickness of oral mucosa. Decreased nutrient intake lowers the threshold of soft tissue to denture irritation. Xerostomia compromises soft-tissue health, denture tolerance & denture function.2015 ICP Special Session on Geriatrics How age-related oral changes influence prosthodontics Heo, SJ

Prosthodontic Materials for Eldercare Y. Maeda ICP 2015 Special Session on Geriatrics

“The problem is, I’ve lived too long”
Calvin B. Ewoldsen , Sept 2015

Periodontal health courtesy of 25mg doxycycline daily, 0.12 % CHX rinsefor 1 minute daily, oral irrigator, mechanical toothbrush…….

“The final disease nature inflicts on us will determine the atmosphere in which we take our leave of life,” “but our own choices should be allowed, insofar as possible, to be the decisive factor in the manner of our going.”
“if the classic image of dying with dignity must be modified or even discarded, what is to be salvaged of our hope for the final memories we leave to those who love us?”
“The dignity we seek in dying must be found in the dignity with which we have lived our lives.” Sherwin Nuland, MD
What constitutes “A Natural Death”?Is death with dignity mostly a myth?
Sherwin Nuland, surgeon & bioethicist
Author: “How We Die: Reflections on Life’s Final Chapter”
How We Die
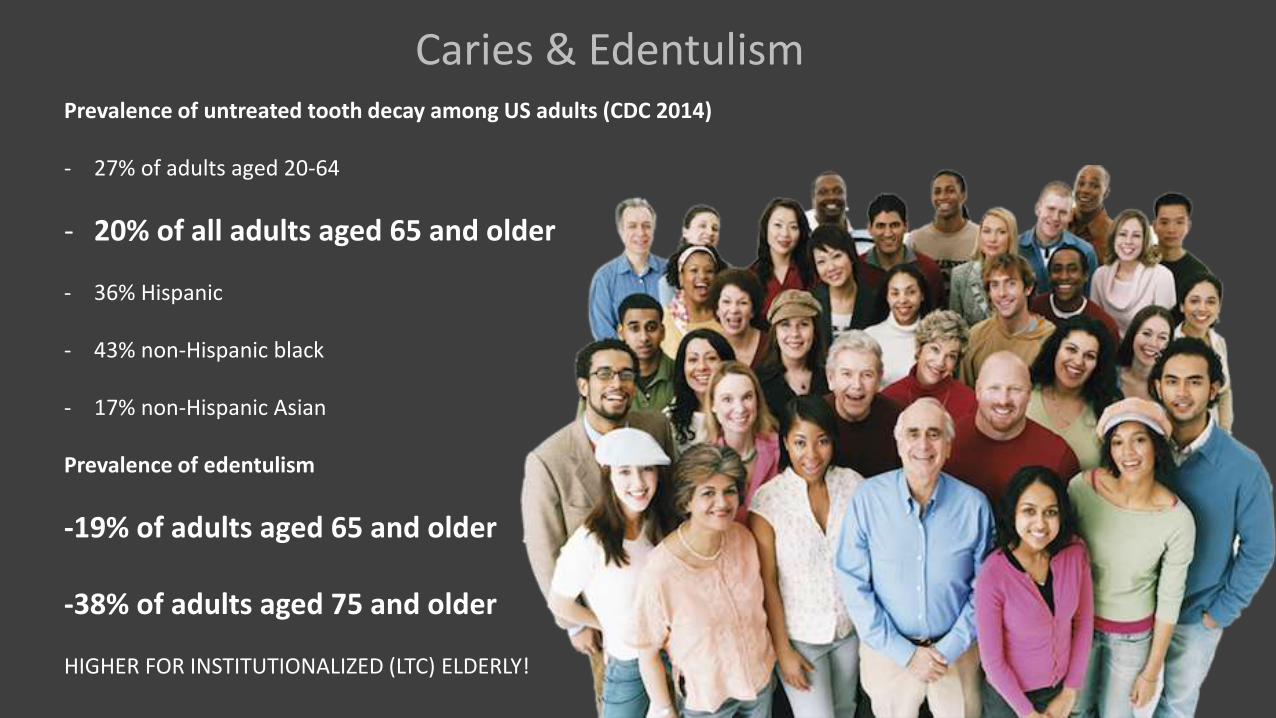
Prevalence of untreated tooth decay among US adults (CDC 2014)
- 27% of adults aged 20-64
- 20% of all adults aged 65 and older
- 36% Hispanic
- 43% non-Hispanic black
- 17% non-Hispanic Asian
Prevalence of edentulism
-19% of adults aged 65 and older
-38% of adults aged 75 and older
HIGHER FOR INSTITUTIONALIZED (LTC) ELDERLY!
Caries & Edentulism
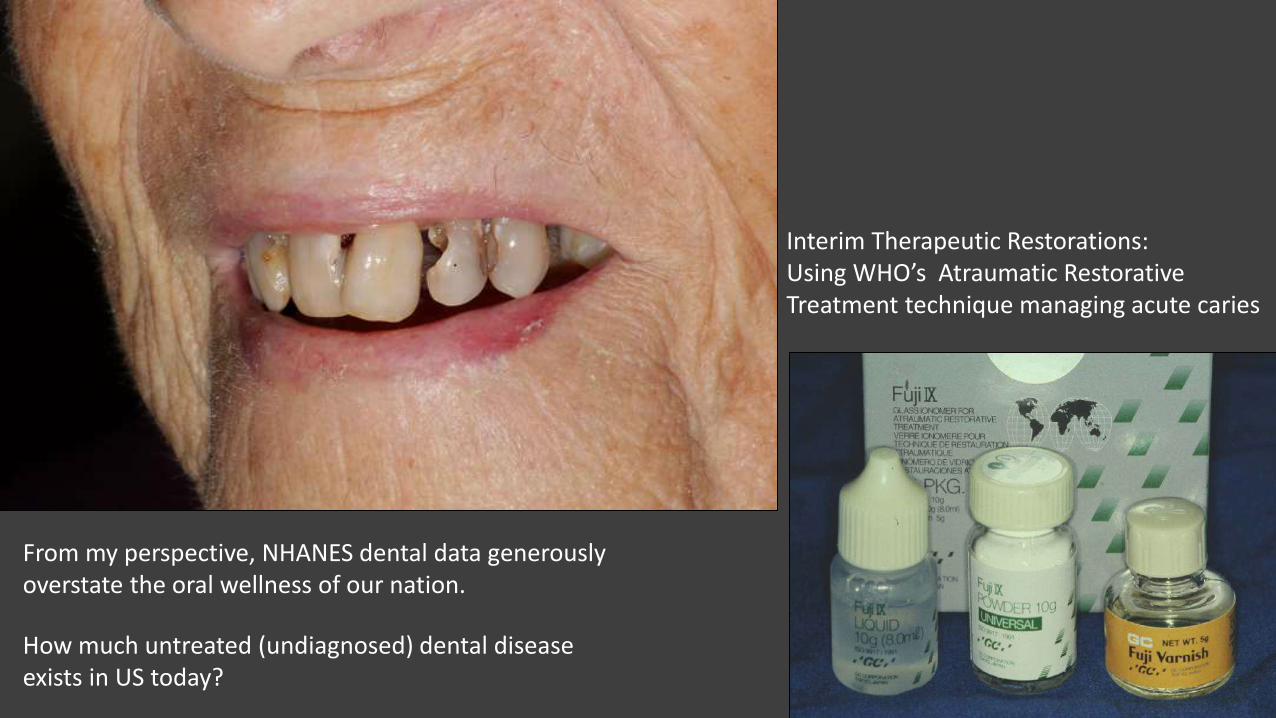
Interim Therapeutic Restorations: Using WHO’s Atraumatic Restorative Treatment technique managing acute caries
From my perspective, NHANES dental data generouslyoverstate the oral wellness of our nation.
How much untreated (undiagnosed) dental disease exists in US today?

ITR set-up for restorative care based on ART technique



“A procedure is considered surgical when it involves cutting of a patient's tissues or closure of a previously sustained wound”

Frail elderly do associate oral hygiene & retention of natural teeth but abandon both with increasing frailty until specific problems require relief. 2015 ICP Session on Geriatrics Frailty Influences Behavior & Perspectives of Elders
Niesten, D

Lo EC, et al . ART & Conventional Root Restorations in Elders J Dent Res 2006 @ 12 mos 91% vs 87%
Biofilms & Mucositis
The formation of multispecies biofilms are influenced by nature of the surface, composition ofpotential colonizing species & fluids that bathe the colonies (Socransky SS. J Periodontol 2012)

Donlan RM. Emerg Infect Dis, 2002 8(9) 881-890Saini R, et al. Biofilm: A dental microbial infection J Nat Sci Bio Med
…. assemblage of microbial cells irreversibly associated (not removed by gentle rinsing) with a ‘slime’ surface in a matrix of primarily polysaccharide material. Non-cellular materials such as mineral crystals, corrosion particles, clay or silt particles, or blood components may be found in the biofilm matrix.
Biofilm: Microbial Life on Surfaces
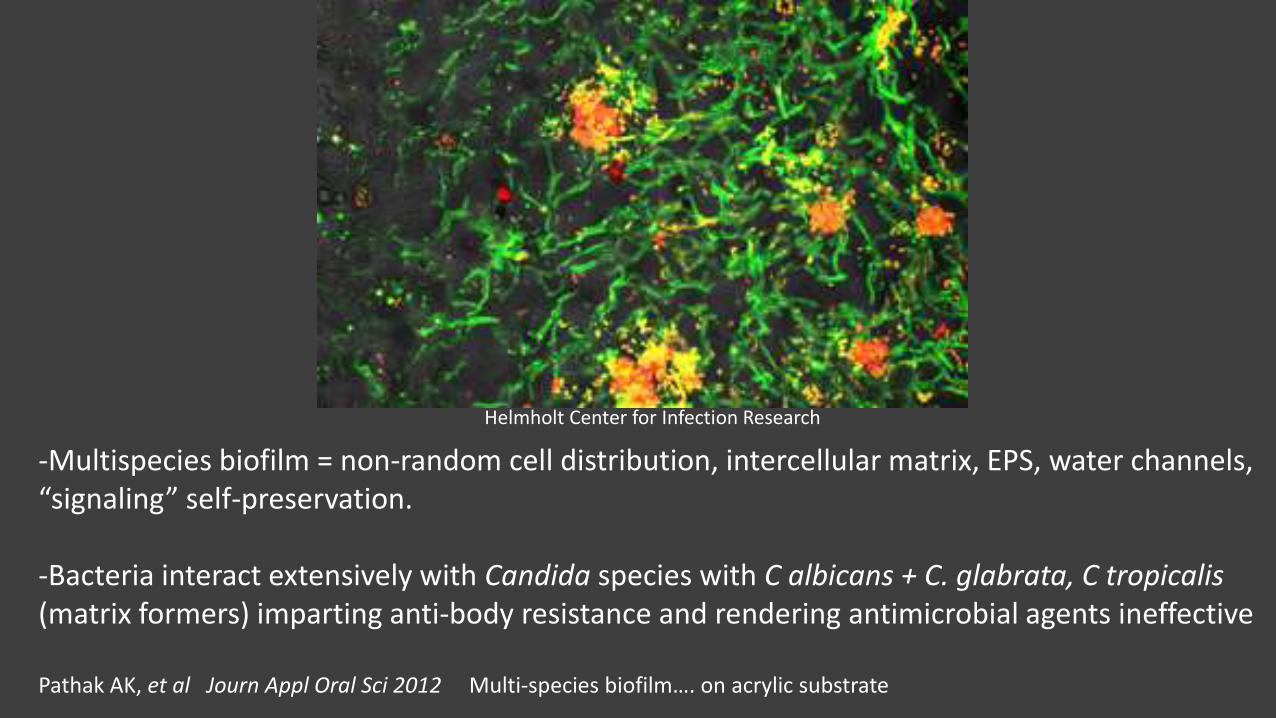
Helmholt Center for Infection Research
-Multispecies biofilm = non-random cell distribution, intercellular matrix, EPS, water channels, “signaling” self-preservation.
-Bacteria interact extensively with Candida species with C albicans + C. glabrata, C tropicalis(matrix formers) imparting anti-body resistance and rendering antimicrobial agents ineffective
Pathak AK, et al Journ Appl Oral Sci 2012 Multi-species biofilm…. on acrylic substrate
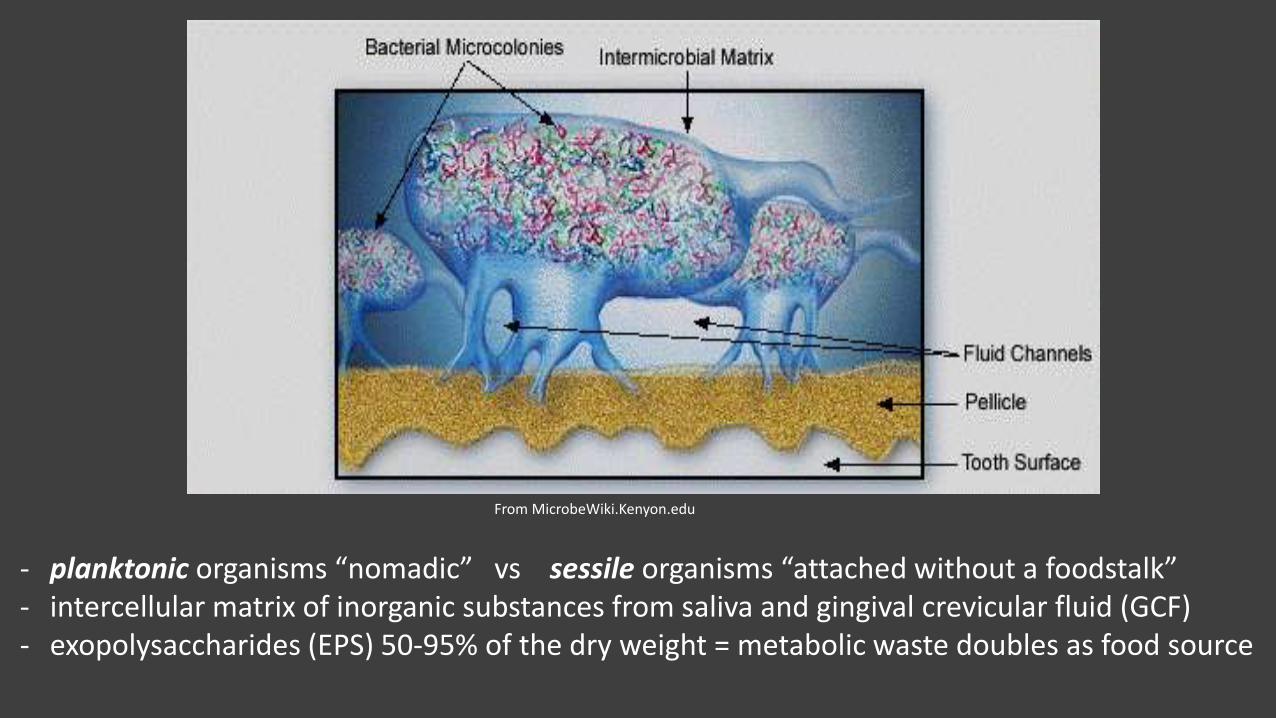
- planktonic organisms “nomadic” vs sessile organisms “attached without a foodstalk”- intercellular matrix of inorganic substances from saliva and gingival crevicular fluid (GCF)- exopolysaccharides (EPS) 50-95% of the dry weight = metabolic waste doubles as food source
From MicrobeWiki.Kenyon.edu
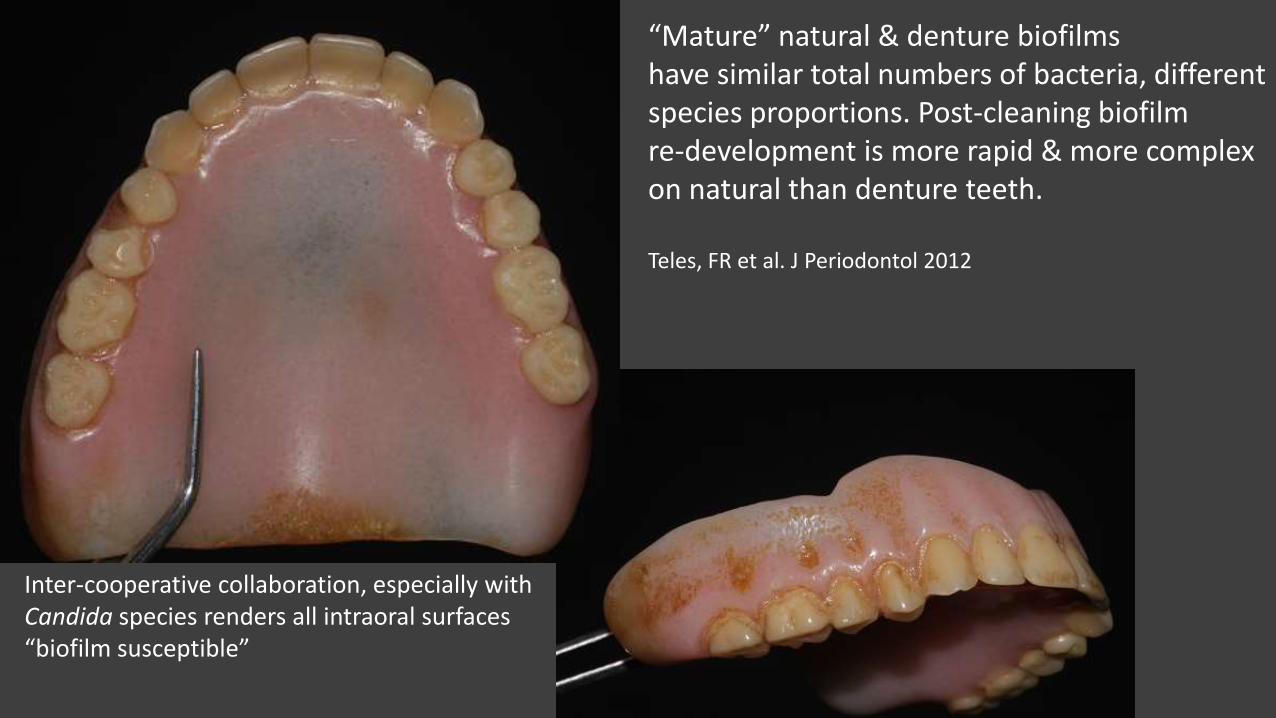
“Mature” natural & denture biofilms have similar total numbers of bacteria, different species proportions. Post-cleaning biofilm re-development is more rapid & more complex on natural than denture teeth.
Teles, FR et al. J Periodontol 2012
Inter-cooperative collaboration, especially with Candida species renders all intraoral surfaces“biofilm susceptible”
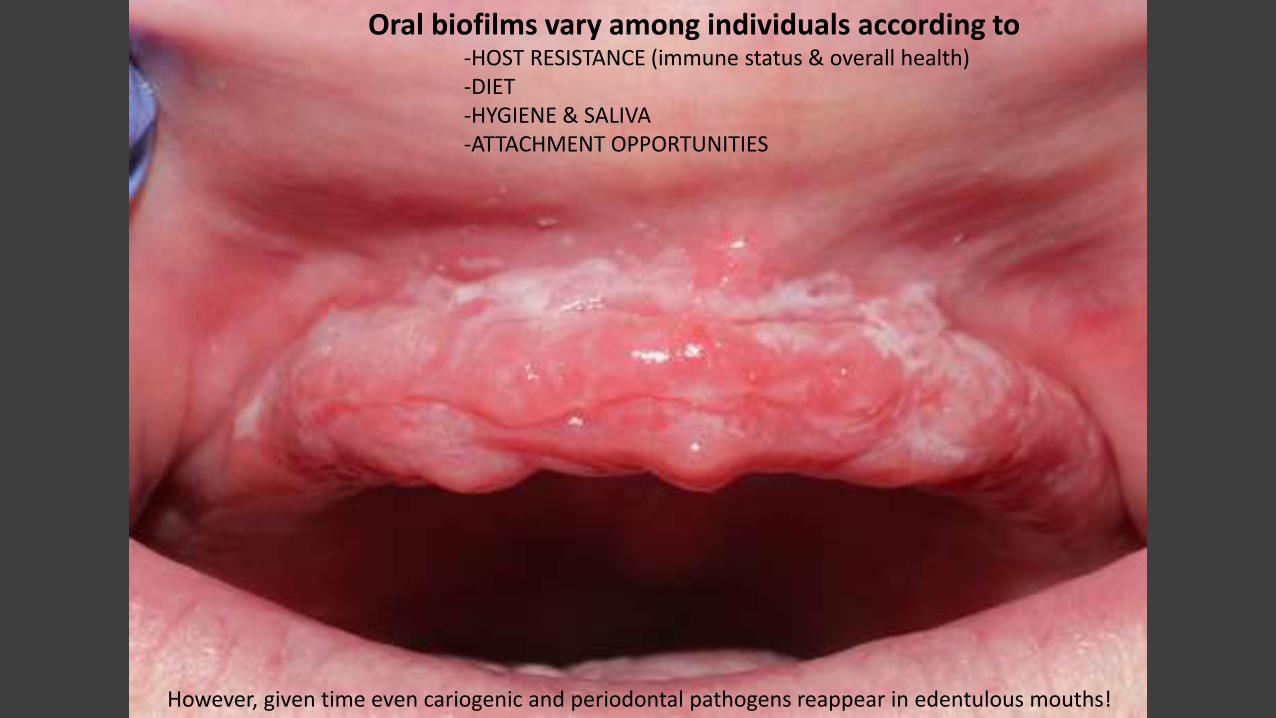
Oral biofilms vary among individuals according to -HOST RESISTANCE (immune status & overall health) -DIET-HYGIENE & SALIVA-ATTACHMENT OPPORTUNITIES
However, given time even cariogenic and periodontal pathogens reappear in edentulous mouths!
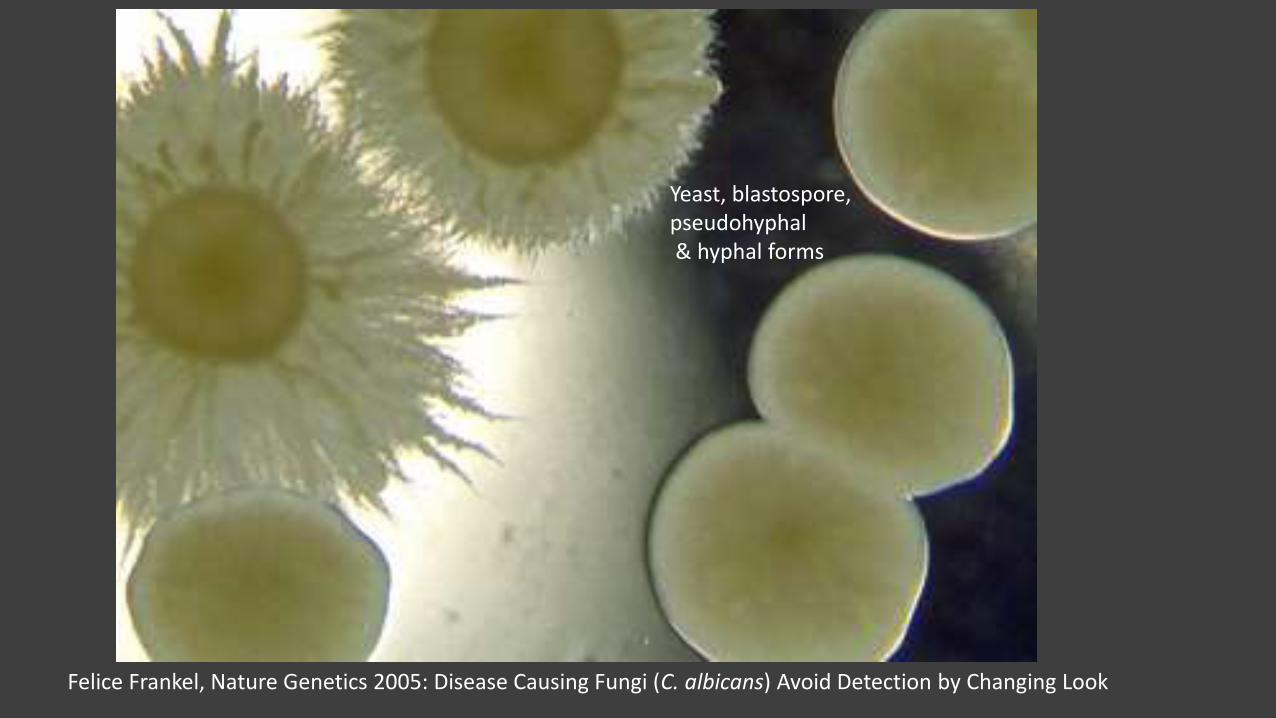
Felice Frankel, Nature Genetics 2005: Disease Causing Fungi (C. albicans) Avoid Detection by Changing Look
Yeast, blastospore, pseudohyphal& hyphal forms
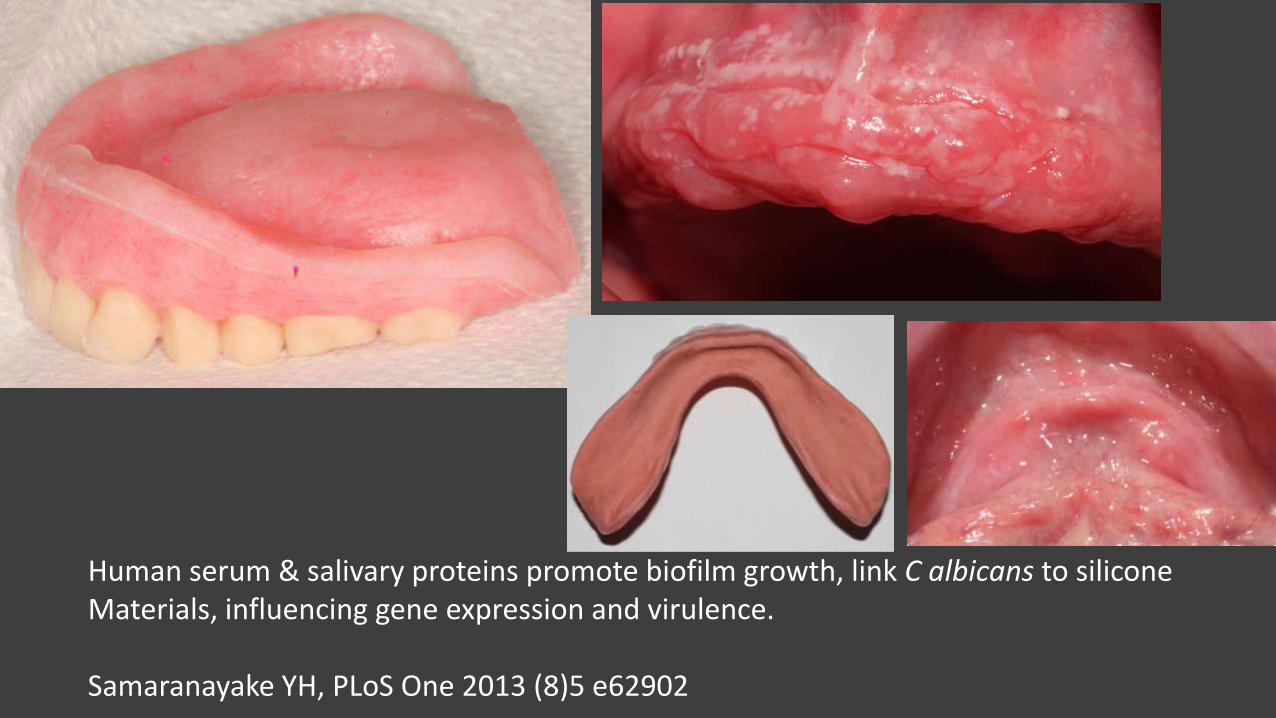
Human serum & salivary proteins promote biofilm growth, link C albicans to silicone Materials, influencing gene expression and virulence.
Samaranayake YH, PLoS One 2013 (8)5 e62902
Predisposing factors for C albicans : -weakened immune system, HIV-diabetes-Sjögren's syndrome-hormone imbalances during pregnancy, oral contraceptives-acidic pH levels, fast foods, stress-removable dental prostheses-antibiotic medications
Treatment Guidelines for Oral Candidiasis • CID 2009:48, 525-64. - disinfection of the denture- mild disease, clotrimazole troches 10 mg 5 X daily, nystatin suspension 100,000 U/mL, 4–6
mL 4 X daily 7–14 days-moderate to severe disease, oral fluconazole 100–200 mg (3 mg/kg) daily, 7–14 days,
What is the real pathogenic potential of oral biofilms in elderly patients?
• Systemic Candidiasis - mature denture biofilm, drug resistance and increasing pathogenesis
• Aspiration pneumonia – sleeping in denture doubles risk of pneumonia among very elderly (Iianuma Y, Journal Dental Research Oct
2104)
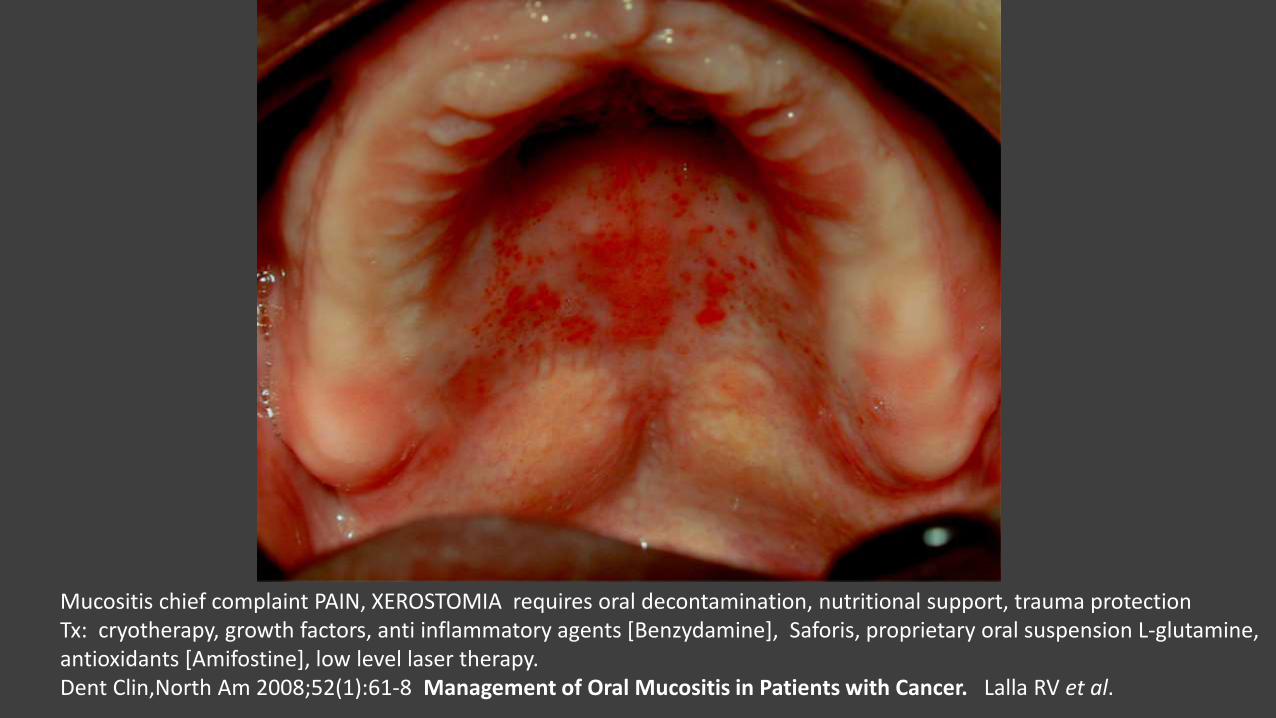
Mucositis chief complaint PAIN, XEROSTOMIA requires oral decontamination, nutritional support, trauma protectionTx: cryotherapy, growth factors, anti inflammatory agents [Benzydamine], Saforis, proprietary oral suspension L-glutamine, antioxidants [Amifostine], low level laser therapy. Dent Clin,North Am 2008;52(1):61-8 Management of Oral Mucositis in Patients with Cancer. Lalla RV et al.
liners!
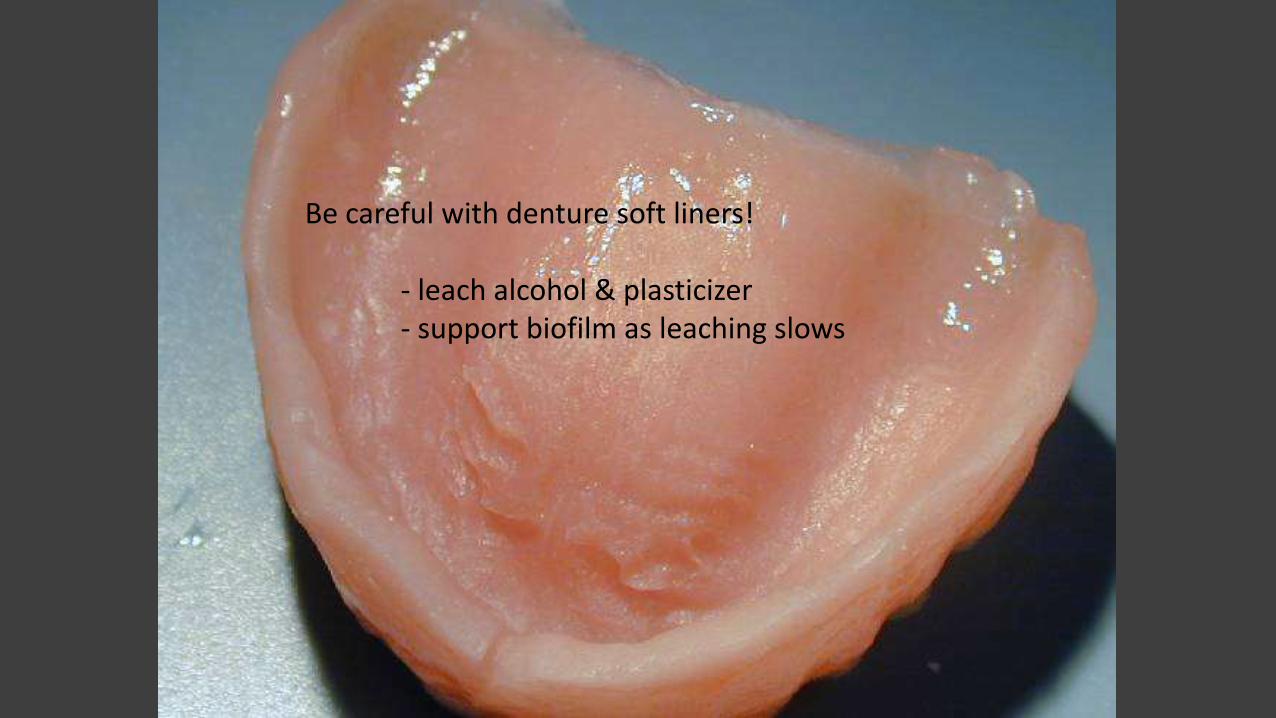
Be careful with denture soft liners!
- leach alcohol & plasticizer- support biofilm as leaching slows
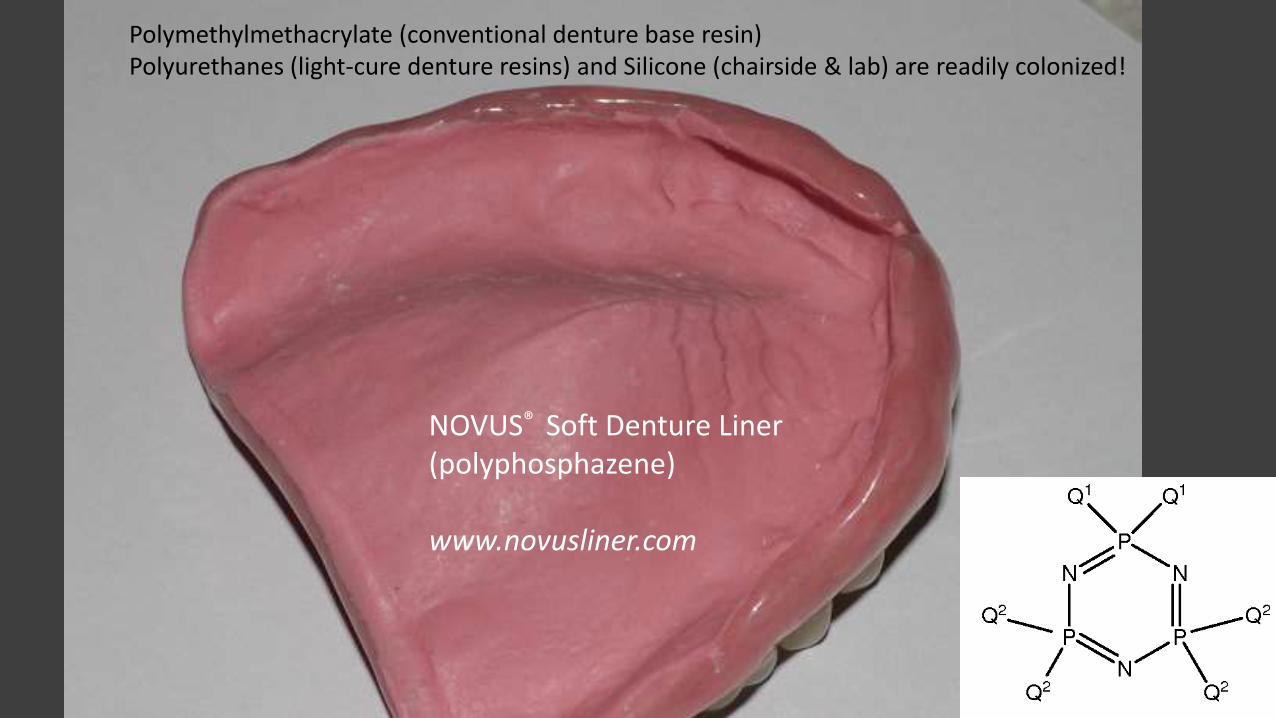
Polymethylmethacrylate (conventional denture base resin) Polyurethanes (light-cure denture resins) and Silicone (chairside & lab) are readily colonized!
NOVUS® Soft Denture Liner(polyphosphazene)
www.novusliner.com
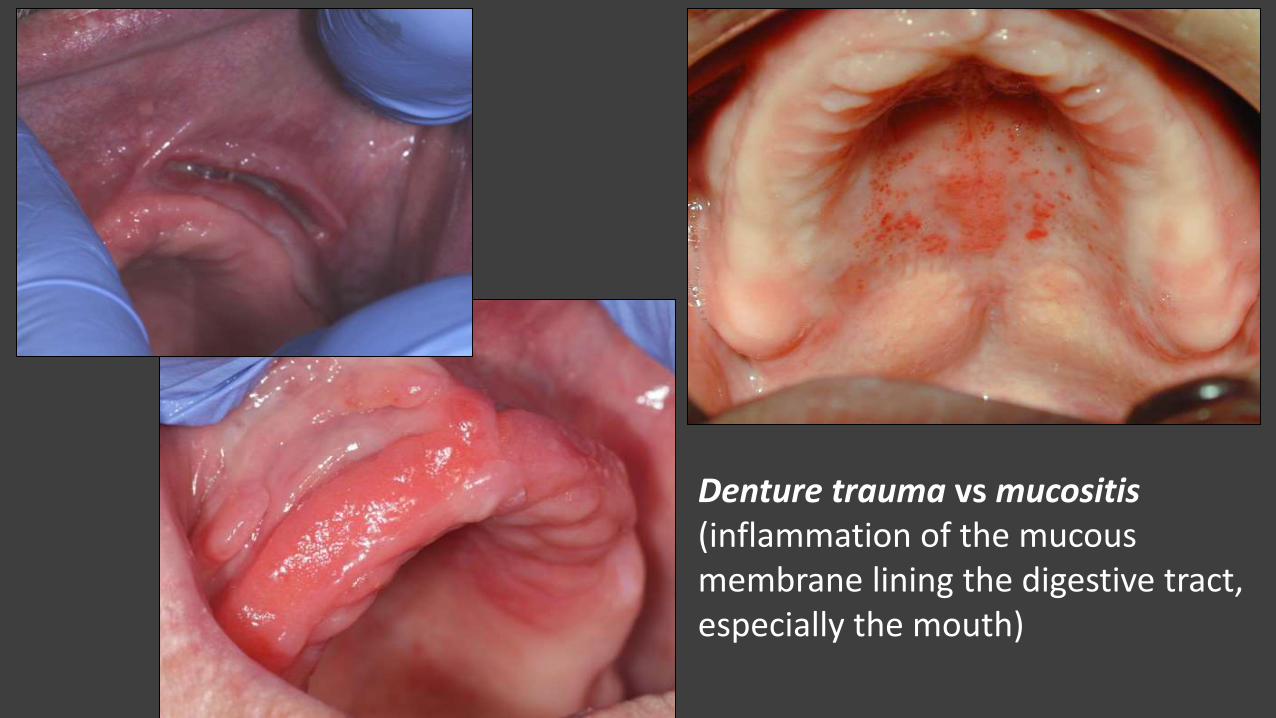
Denture trauma vs mucositis(inflammation of the mucous membrane lining the digestive tract, especially the mouth)
Root Surface Caries (Prevention & Arrest)
• Bacterial etiology of root caries is more complex than that of coronal lesions
• Fluoride varnish and topical fluorides are effective
• Chlorhexadine (CHX) alone is less effective than fluoride
• Glycyrrhizine (Licorice Extract) lollipops appear promising
• Silverdiamine Fluoride is gaining acceptance, discoloration!
0.5 mL “clear, hard surface” varnish delivering 22,600 ppm F
Indications:
-previous caries, WSL
-demand breast feeing @ night or ad-lib prolonged bottle/sippy cup
-developmental disabilities
Contraindications:
-low caries risk
-fluoridated drinking water
-regularly receives in-office F
Advantages:
-simplified armamentarium
-not technique sensitive
-safe, patient friendly, sets on contact w/ saliva
CDT Code D01203
POI: NPO for 30 minutes, non-abrasive diet for remainder of day,
delay tooth brushing until next day
HRSA, Nevada http://health2k.state.nv.us/oral/FVManual.pdfTOXICITY: 5mg F/kg body weight
DMG Mfg

Cervitec Plus (CHX & thymol) 10% after 30 sec drying……less effective than SDF; less effective than F varnish Gluzman R, et al, Spec Care Dentist Prevention of Root Caries 2013
Segal R, et al. Anticariogenic activity of licorice and glycyrrhizine I: Inhibition of in vitro plaque formation by Streptococcus mutans. Pharm Sci. 1985 Jan;74(1):79-81.
Determination of optimal concentration of licorice root extract for preventing dental caries using a bacterial model system Ahn SJ et al, Journal Dental Sci 2014; 9(4).
Glycyrrhizine (Licorice Extract) reduces s mutans

-0.40% stannous fluoride 970 ppm-ACP remineralization-Ultramulsion (protective coating on oral tissues)-Spilanthes extract (herbal salivary stimulant)-No Sodium Lauryl Sulfate (SLS)


• Antimicrobials & remineralization promoters
• povidone iodine
• silver nitrate
• silverdiaminefluoride (SDF) w/wo potassium iodide, nano SDF
• Chlorhexadine + Thymol varnish (with fluoride)
What about arresting caries? (ACT)
Two minute application, 30-40% solution, pH = 9.0 rinsed for 30 seconds
Silverdiamine fluoride (SDF)
Yee R, et al Efficacy of silver diamine fluoride for Arresting Caries Treatment, J Dent Res 2009: 88(7)644-7
Knight GM, et al Inability to form s mutans biofilm on SFD/KI treated dentin, Quint Int. 2009: 40(2) 155-61

Theannguyen.comwww.studyblue.com
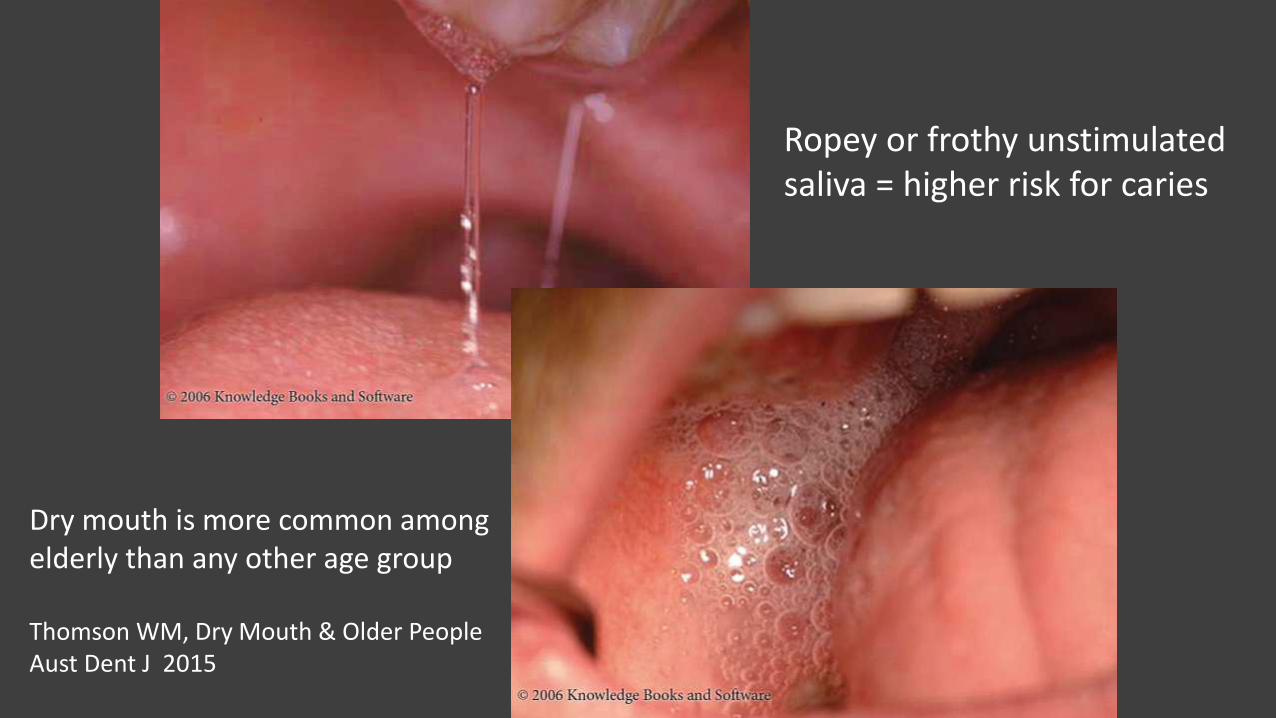
Ropey or frothy unstimulatedsaliva = higher risk for caries
Dry mouth is more common among elderly than any other age group
Thomson WM, Dry Mouth & Older PeopleAust Dent J 2015
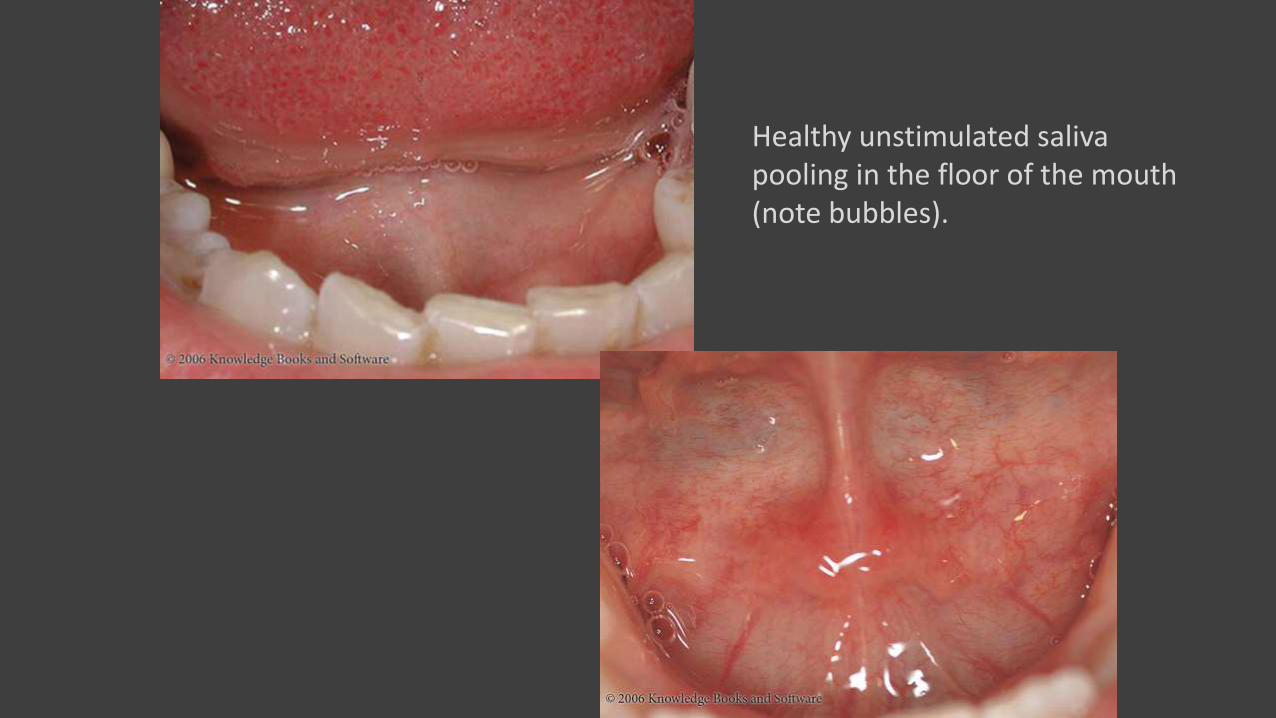
Healthy unstimulated salivapooling in the floor of the mouth(note bubbles).

Boudreaux’s Specialty Pharmacy, Shreveport, LA 71103, 318-631-2005
Stimulating saliva
BioteneTM (Laclede) or Dry Mouth GelTM (GC)
Intraoral remineralization will not occur in a dry field!
(impression + esthetic preview + bite + delivery)
-impressioning, bite records (MMR) & preview
(templates)
-phonetic, esthetic & occlusion
verification (optional wax try-in)
-delivery of finished prosthesis
3-Appointment Dentures

GC Metal Trays (aluminum) can be adjusted slightly by bending


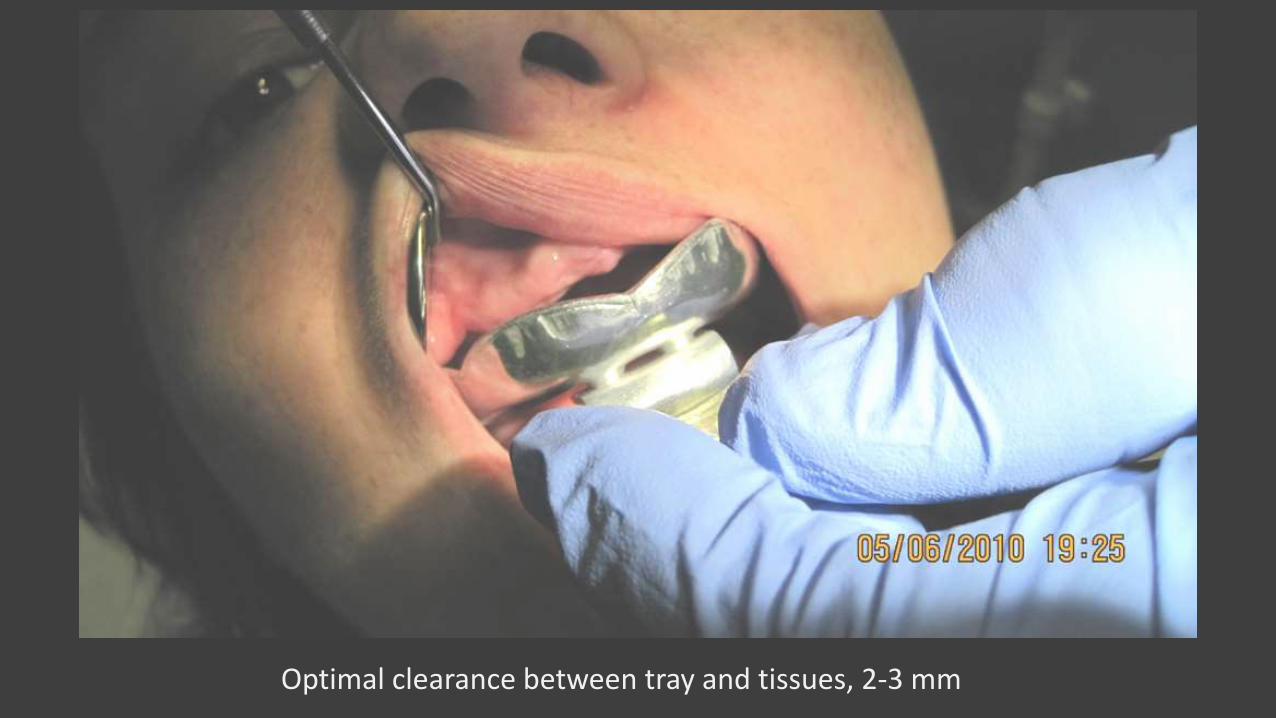
Optimal clearance between tray and tissues, 2-3 mm

Center tray aligning facial midline with tray handle
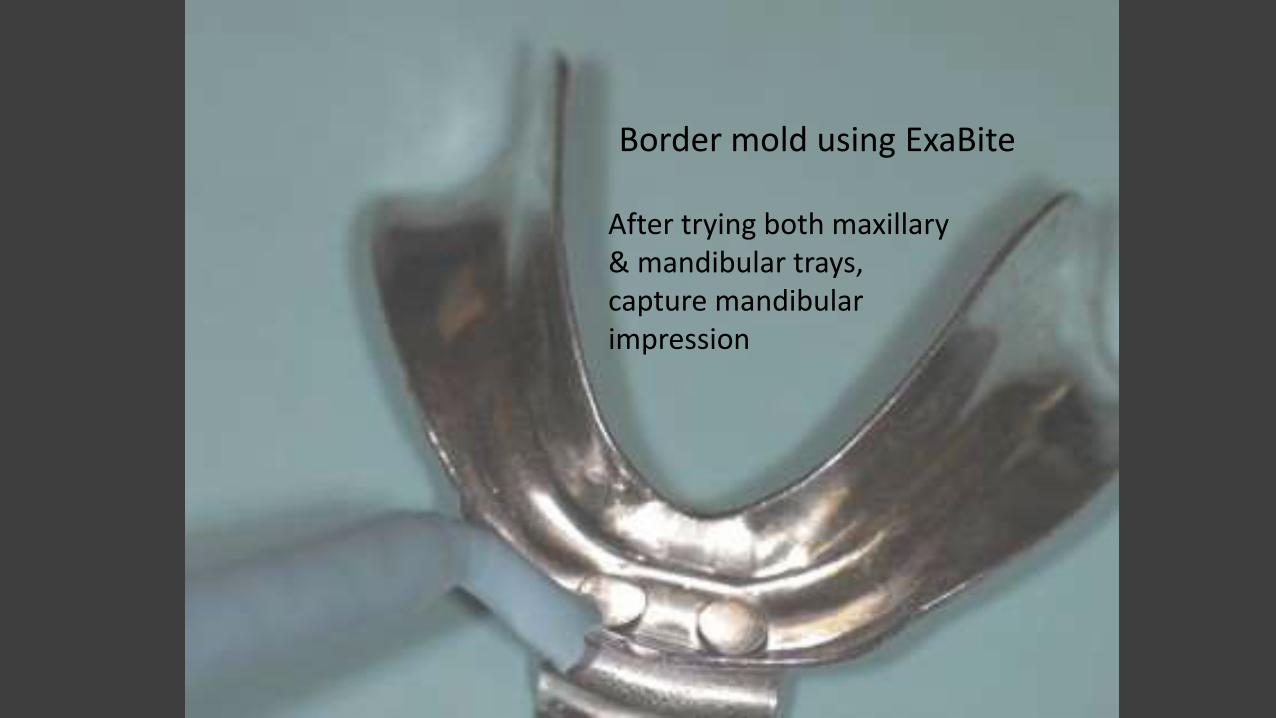
After trying both maxillary & mandibular trays, capture mandibular impression
Border mold using ExaBite
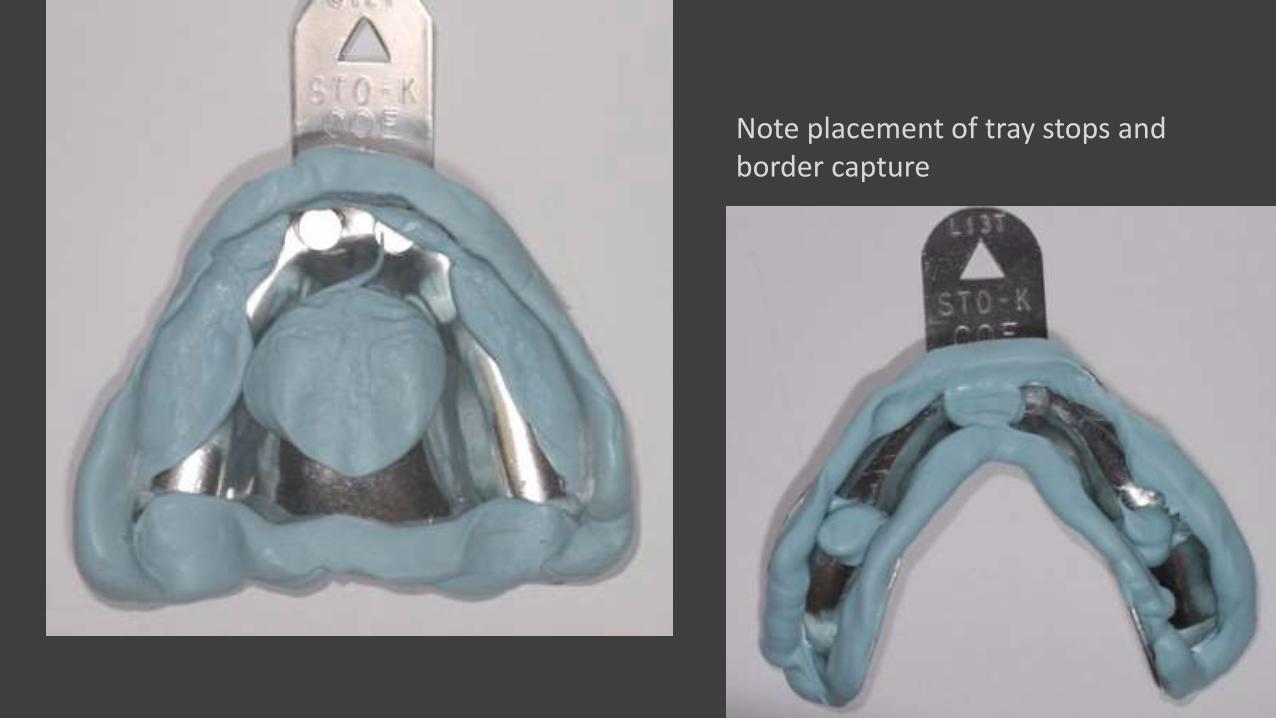
Note placement of tray stops andborder capture

Follow border molding with Exa Monophase


Cut or grind (relieve) interferences& tissue compression areas
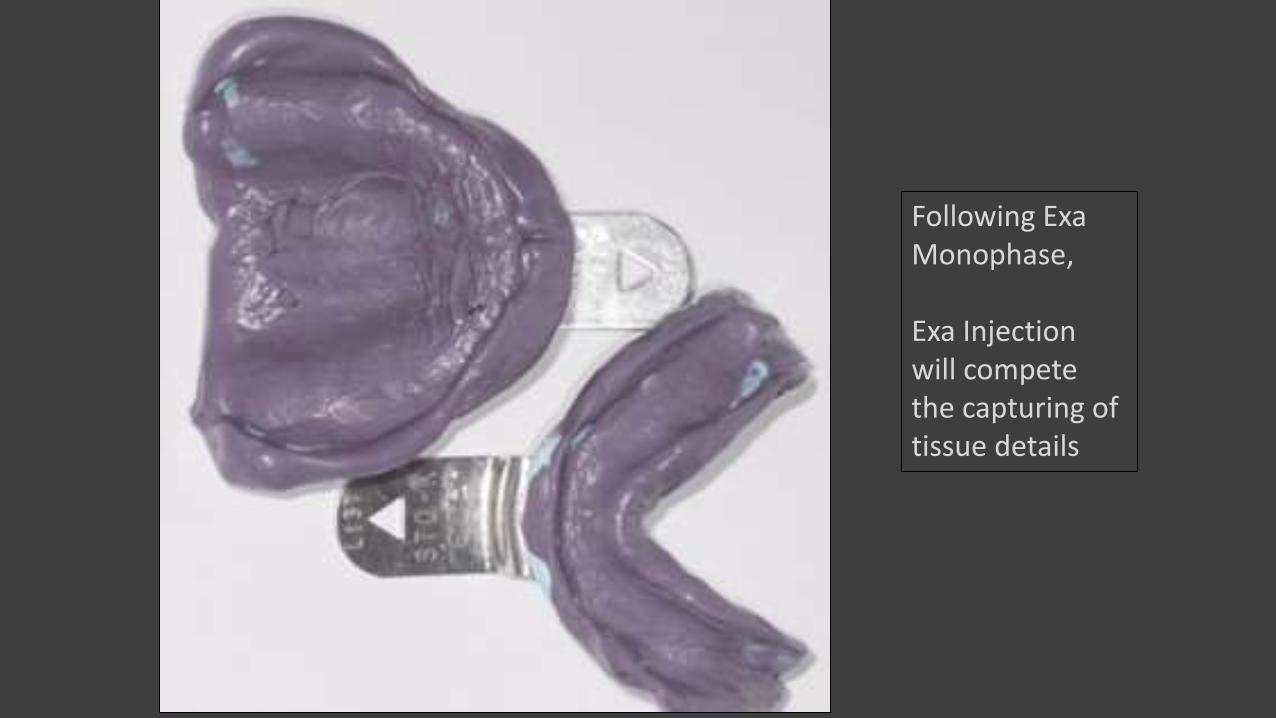
Following ExaMonophase,
Exa Injectionwill competethe capturing of tissue details
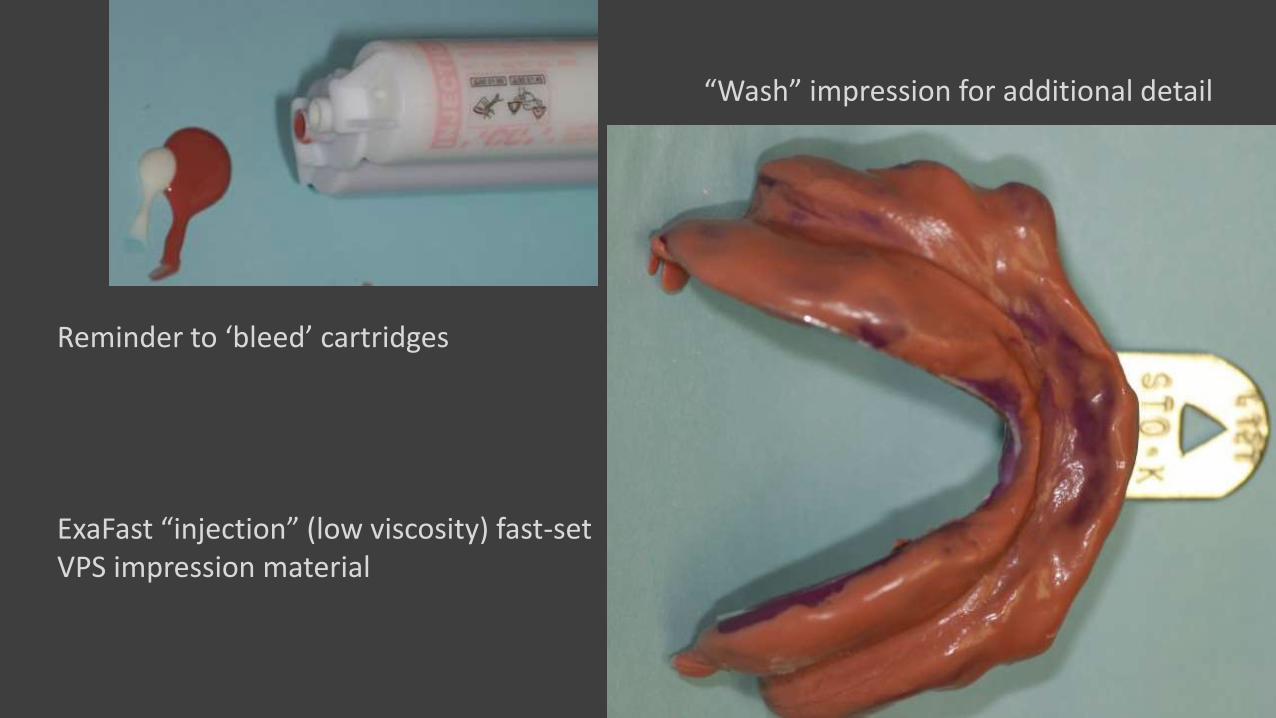
Reminder to ‘bleed’ cartridges
ExaFast “injection” (low viscosity) fast-setVPS impression material
“Wash” impression for additional detail



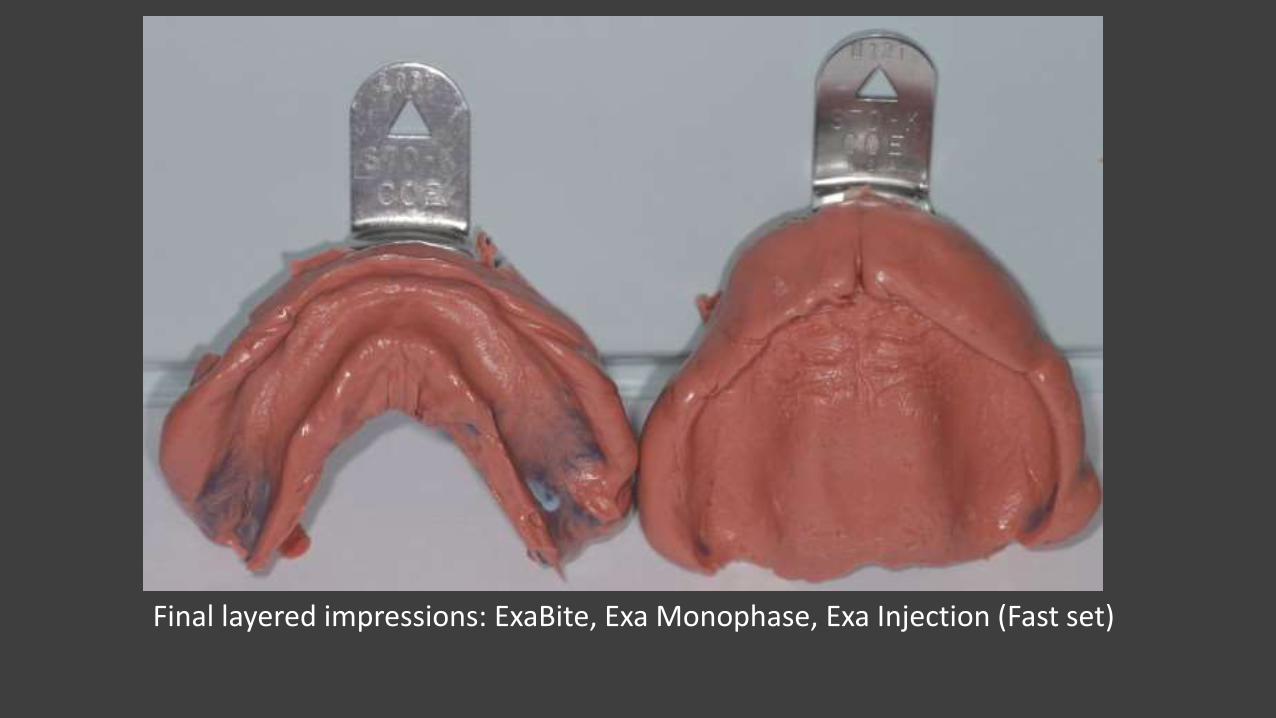
Final layered impressions: ExaBite, Exa Monophase, Exa Injection (Fast set)
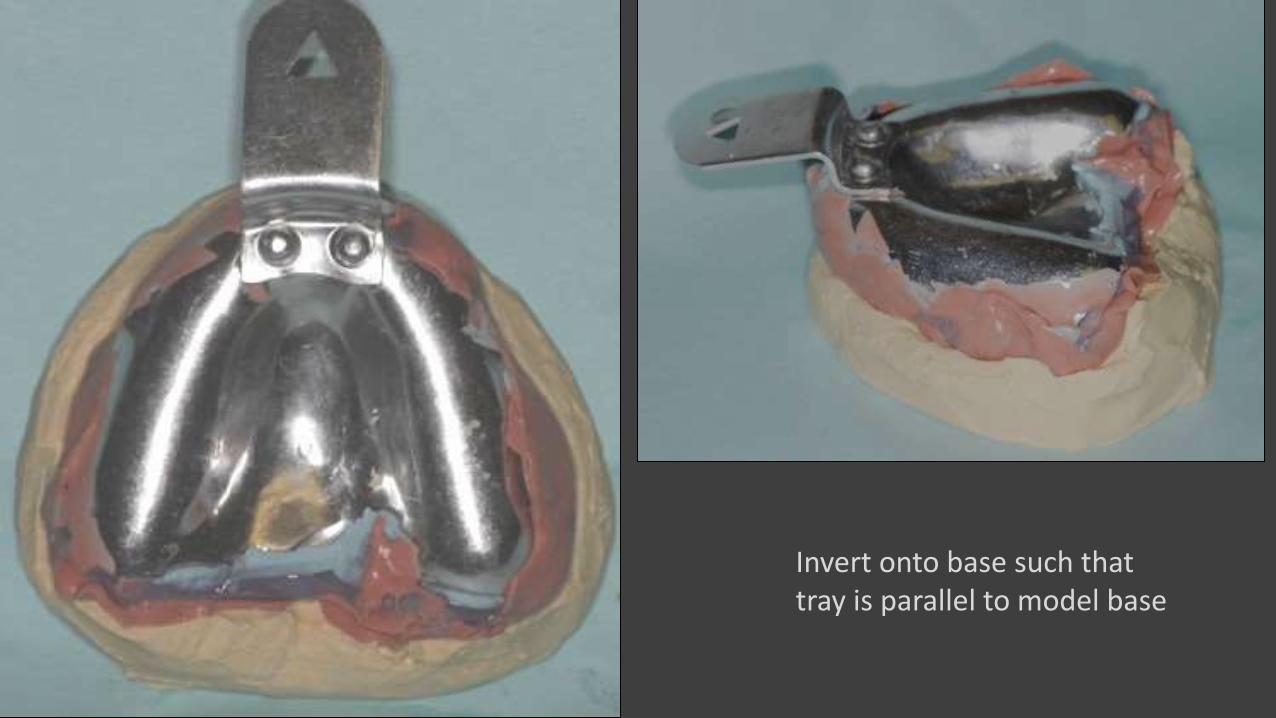
Invert onto base such thattray is parallel to model base
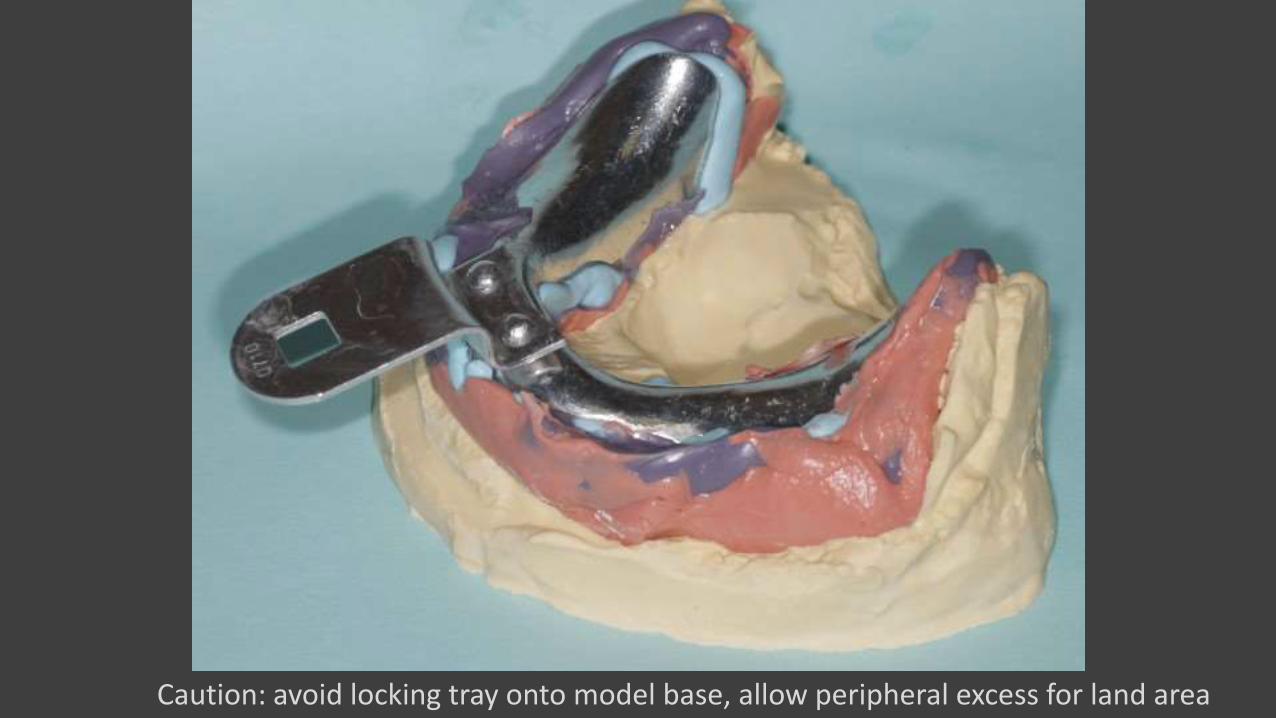
Caution: avoid locking tray onto model base, allow peripheral excess for land area
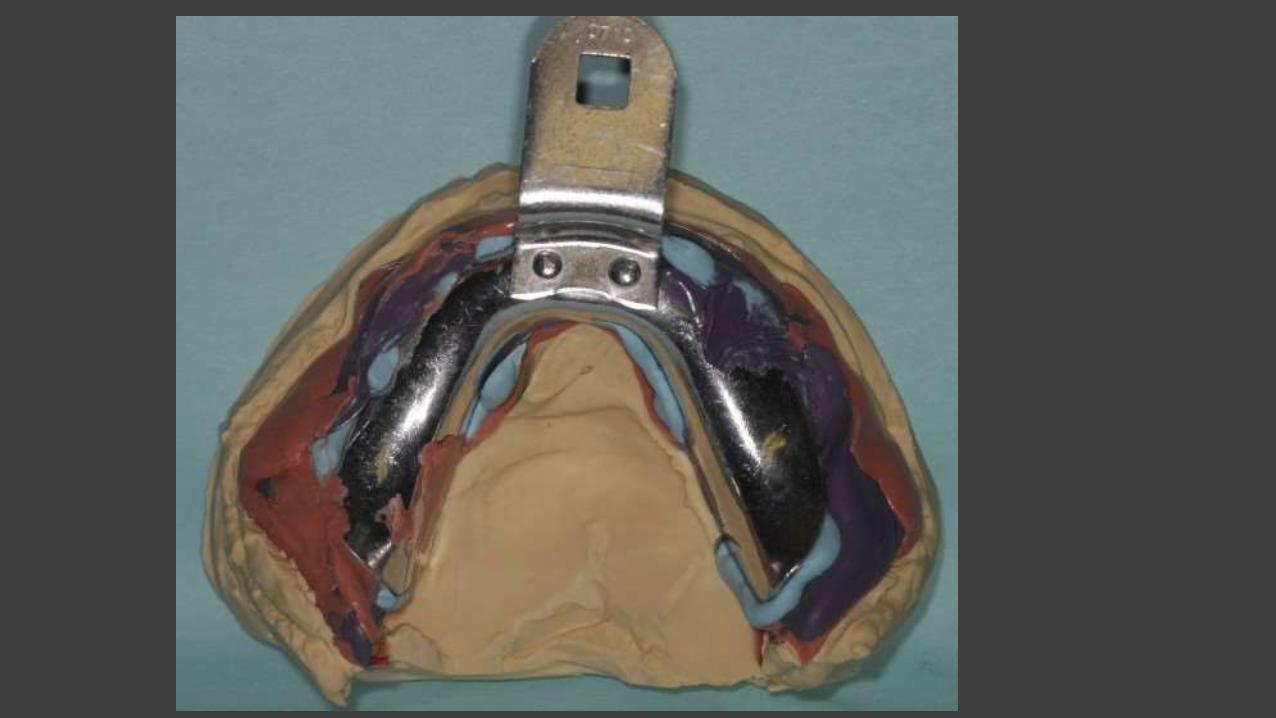

Communicate to the laboratory the vibrating line and configuration of posterior palatal seal

Esthetic determination & preview

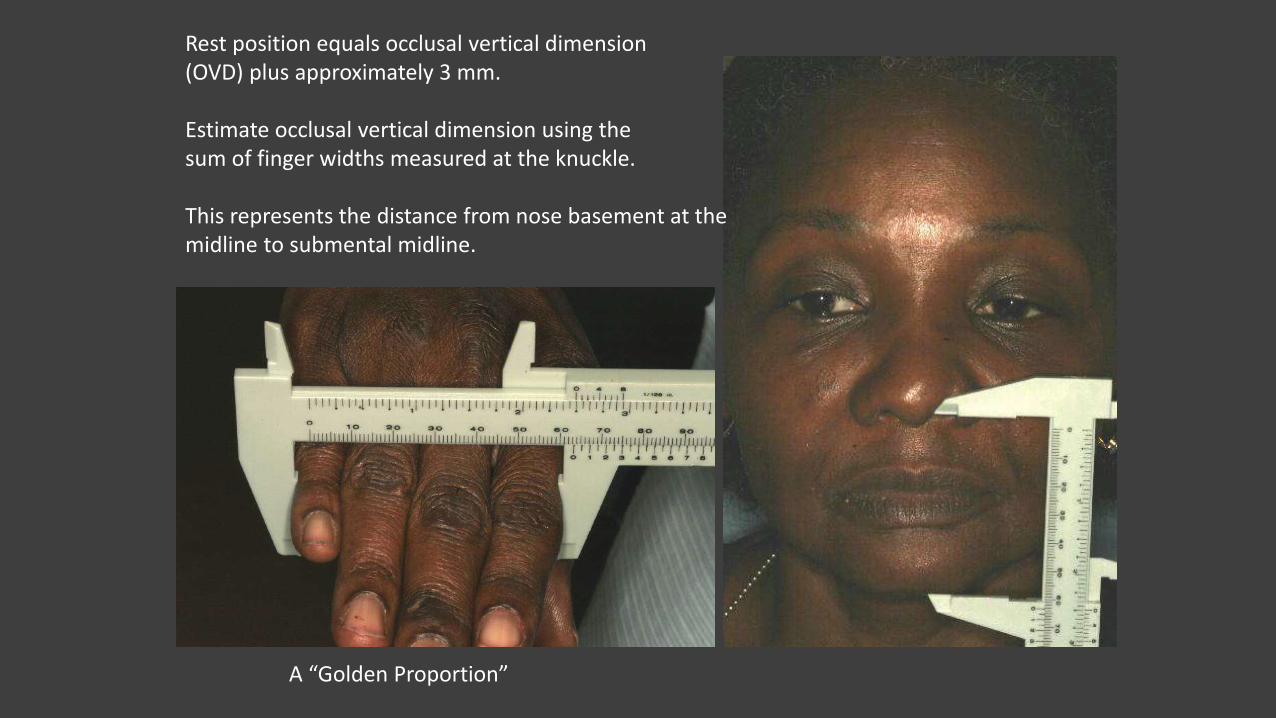
Rest position equals occlusal vertical dimension(OVD) plus approximately 3 mm.
Estimate occlusal vertical dimension using the sum of finger widths measured at the knuckle.
This represents the distance from nose basement at the midline to submental midline.
A “Golden Proportion”

Determine OVD
&
upper lip length
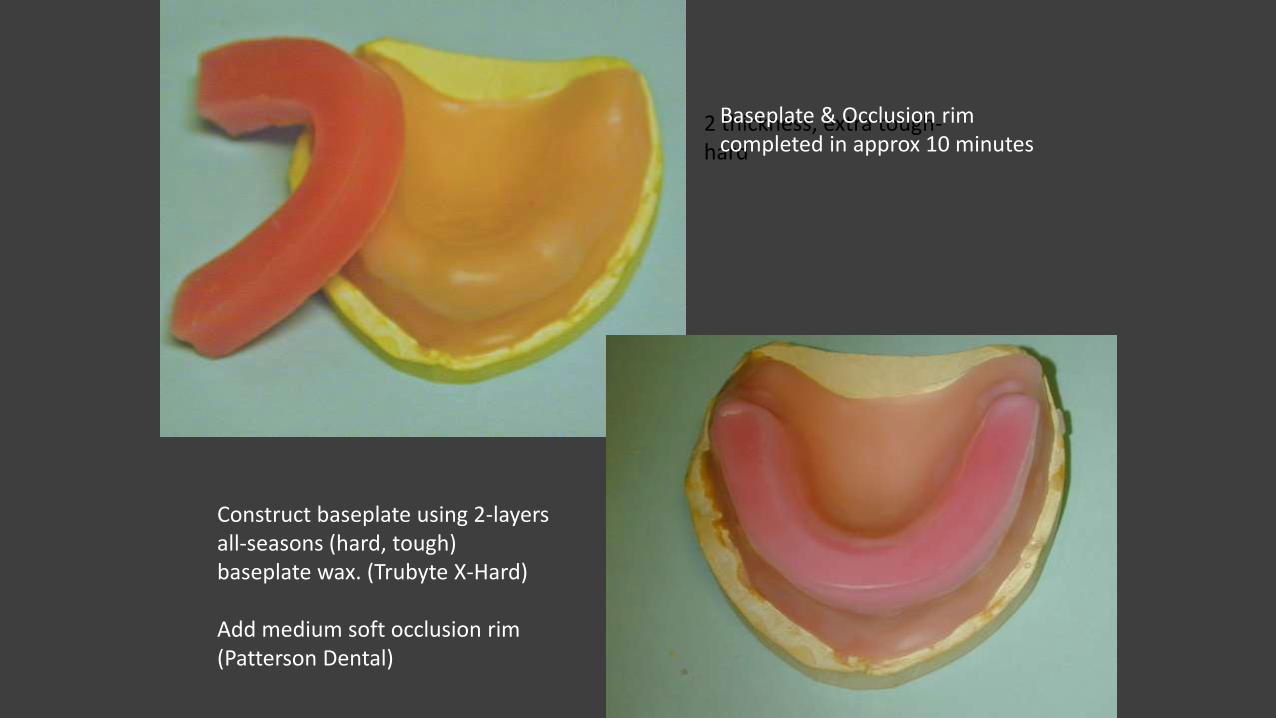
2 thickness, extra tough-hard
Construct baseplate using 2-layersall-seasons (hard, tough) baseplate wax. (Trubyte X-Hard)
Add medium soft occlusion rim(Patterson Dental)
Baseplate & Occlusion rimcompleted in approx 10 minutes

Alma Gage measures the height and facial dimension of wax rimUse Alma Gauge to establish rim at 8 mm below and 4 mm anterior to papilla for recent extraction case. For aged edentulous ridges use 10 mm & 5 mm (Turbyfill)
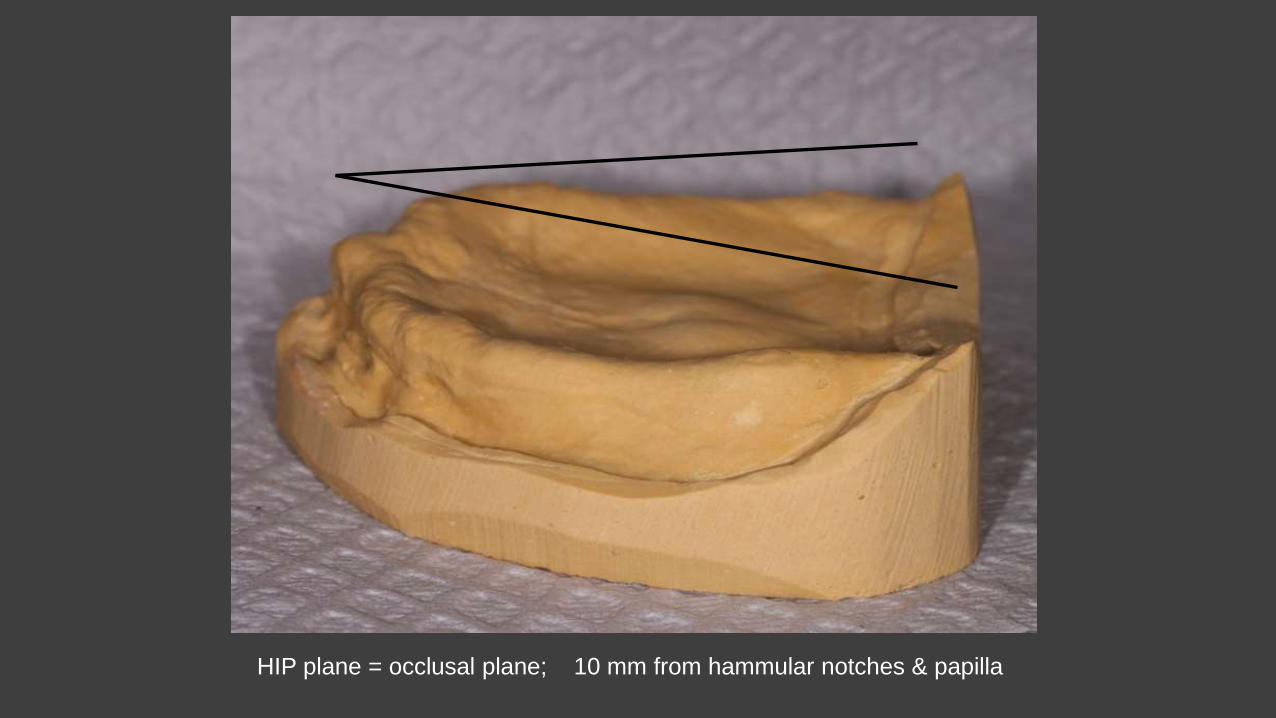
HIP plane = occlusal plane; 10 mm from hammular notches & papilla

Non-metal RPD Materials Nylon (Valplast, FRS)
Acetal Resin (Thermoflex, Duracetal)
Polyetheretherketone, PEEK (Juvora)
Trinia (Fiber-reinforced composite)




Naturcryl Super Hi I (press-pack, 90 min cure) with 14 Ga Co/Cr wrought wire (HR)





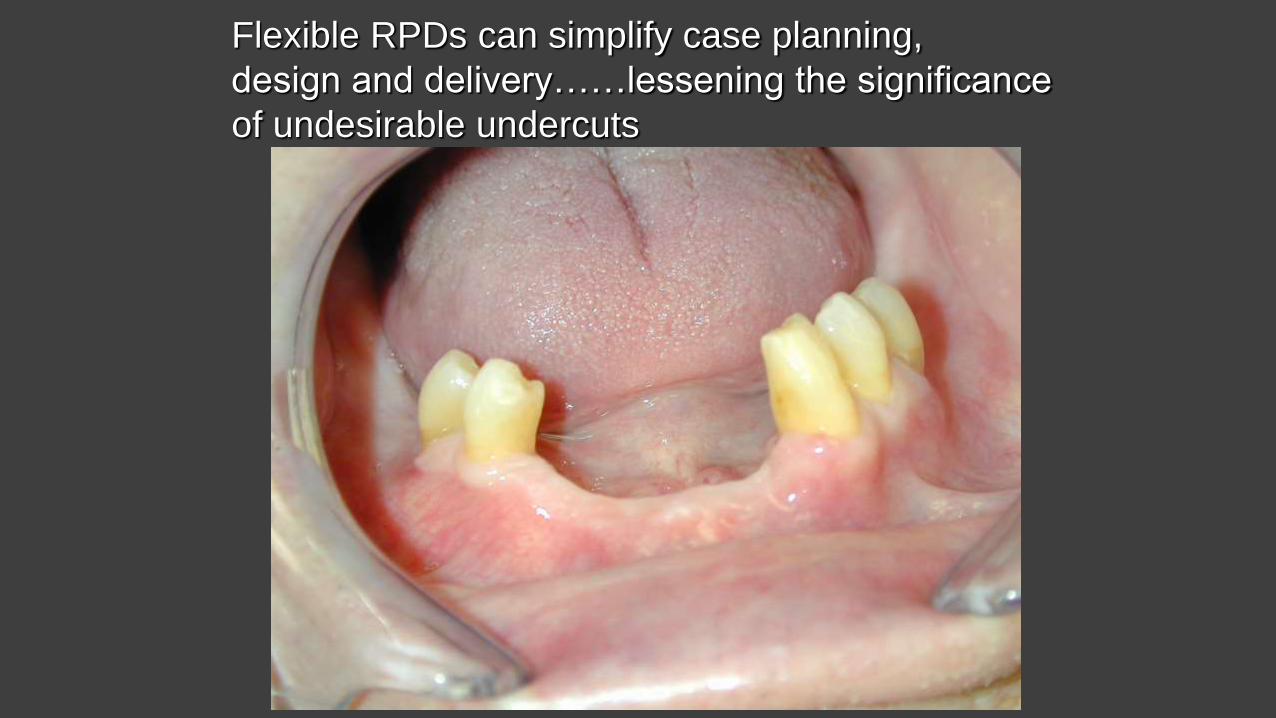
Flexible RPDs can simplify case planning,
design and delivery……lessening the significance
of undesirable undercuts

Major connector
also serves as the direct retainer
Will occlusal rests support this prosthesis, long term?
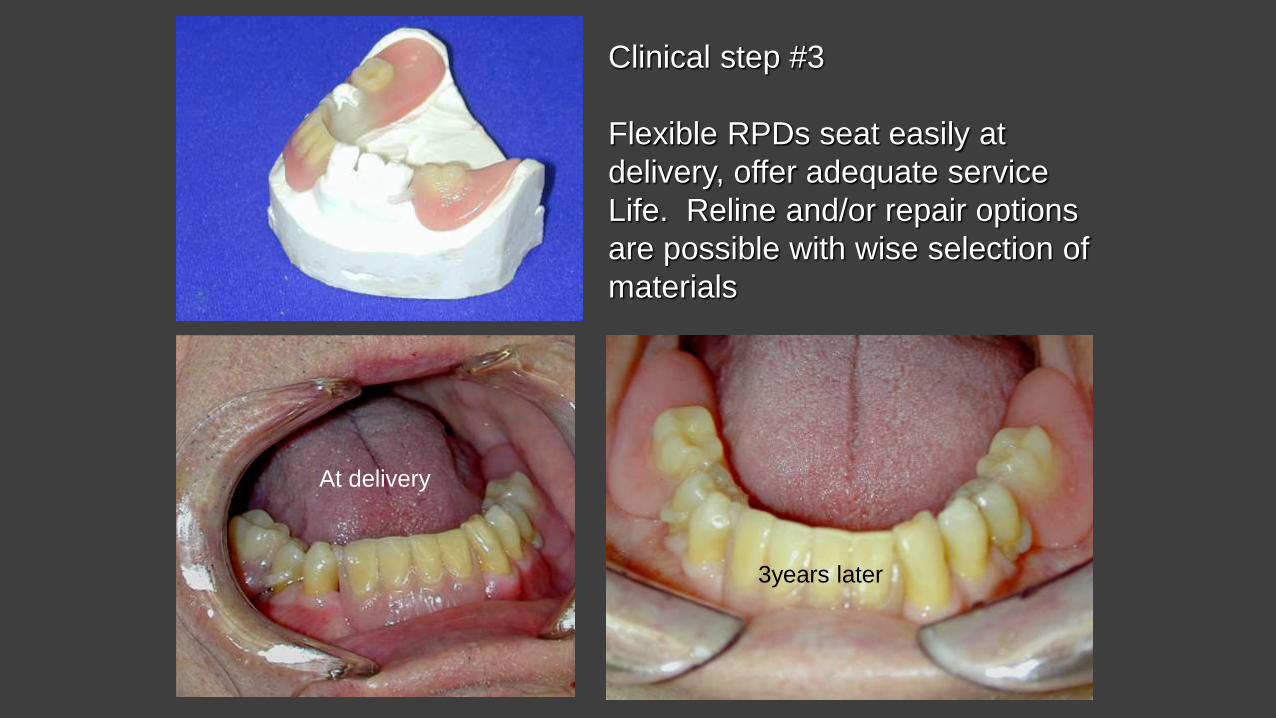
At delivery
3years later
Clinical step #3
Flexible RPDs seat easily at
delivery, offer adequate service
Life. Reline and/or repair options
are possible with wise selection of
materials
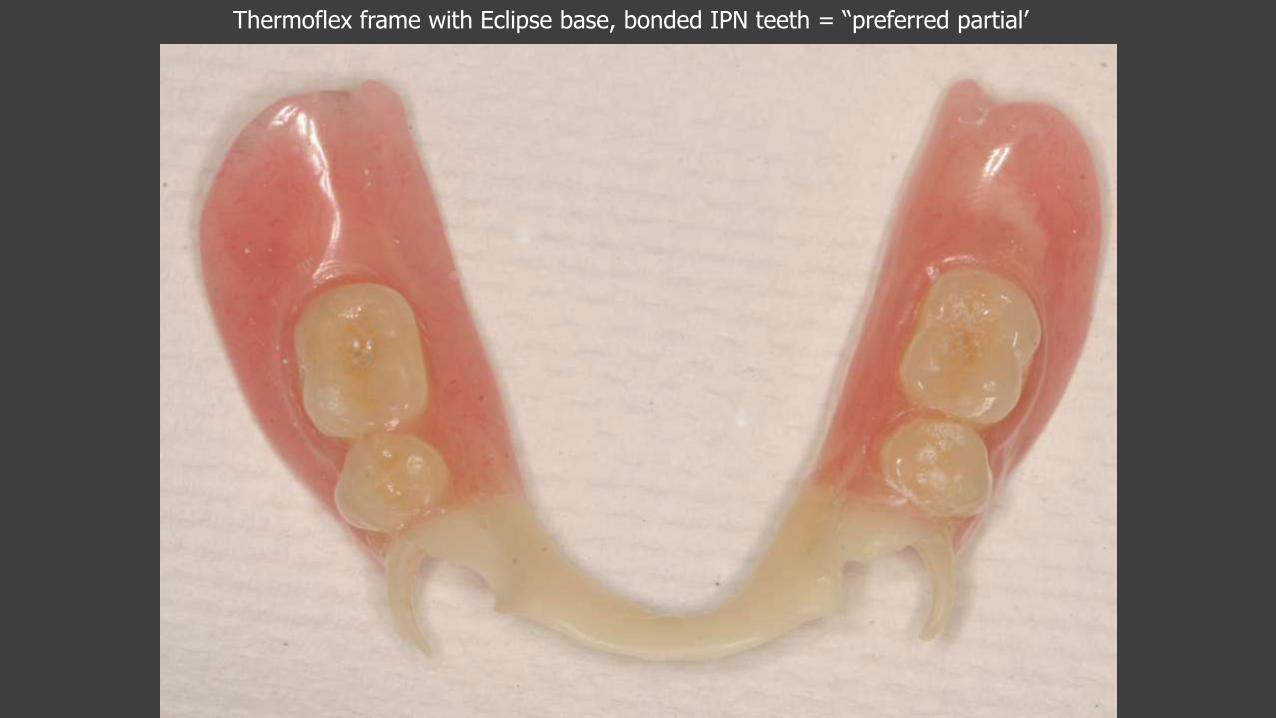
Thermoflex frame with Eclipse base, bonded IPN teeth = “preferred partial’

Acetal & Acrylic @ 2 years

-Bulky, but shape-stable occlusalrests and clasps. -Relinable, repairable bases-Bonded artificial teeth
Clinical Evidence Supporting ART
Frencken JE, et al. Survival of ART and amalgam restorations in permanent teeth of children after 6.3 years. Dent Res. 2006 Jul;85(7):622-6.
ART restorations using highly viscous GIC survive longer than traditionally placed amalgams in young children
van’t Hof, et al. The atraumatic restorative treatment (ART) approach for managing dental caries: a meta-analysis. Int Dent J. 2006 Dec;56(6):345-51.
Single-surface ART restorations using high-viscosity glass-ionomer in both primary and permanent dentitions show high survival rates
Mickenautsch S, Rudolph MJ. Undergraduate training in the atraumaticrestorative treatment (ART) approach--an activity report. SADJ. 2002 Sep;57(9):355-7.
ART should be integrated as part of clinical student training in the BDS curriculum.
Addn. ART References• Schriks MC, van Amerongen WE. Atraumatic perspectives of ART: psychological and
physiological aspects of treatment with and without rotary instruments. Evid Based Dent. 2005;6(1):9.
• Van Palenstein, Helderman W. Priorities in oral health care in non-EME countries Int Dent J. 2002 Feb;52(1):30-4.
• Lo EC, Luo Y, Tan HP, Dyson JE, Corbet EF. ART and conventional root restorations in elders after 12 months. Dent Res. 2006 Oct;85(10):929-32.
• Songpaisan Y, Bratthall D, Phantumvanit P, Somridhivej Y. Effects of glass ionomer cement, resin-based pit and fissure sealant and HF applications on occlusal caries in a developing country field trial. Community Dent Oral Epidemiol. 1995 Feb;23(1):25-9.
• Czarnecka B, Limanowska Shaw H, Nicholson JW. Microscopic evaluation of the interface between glass-ionomer cements and tooth structures prepared using conventional instruments and the atraumatic restorative treatment (ART) technique. Quintessence Int. 2006 Jul-Aug;37(7):557-64.
• Beiruti N, Frencken JE, van't Hof MA, Taifour D, van Palenstein, Helderman, H. Caries-preventive effect of a one-time application of composite resin and glass ionomer sealants after 5 years. Caries Res. 2006;40(1):52-9.


![CARIES MANAGEMENT TECHNIQUES FOR THE CHILD & ADOLESCENT ... Ewoldsen... · CARIES MANAGEMENT TECHNIQUES FOR THE CHILD & ADOLESCENT ... [caries lesion], ... with the floor of deep](https://img.pdfslide.us/doc/110x75/5acc536b7f8b9a73128cb37d/caries-management-techniques-for-the-child-adolescent-ewoldsencaries-management.jpg)