Embed Size (px)
Citation preview

International Emergency Nursing 21 (2013) 168–172
Contents lists available at SciVerse ScienceDirect
International Emergency Nursing
journal homepage: www.elsevier .com/locate /aaen
Identifying and correcting communication failures among healthprofessionals working in the Emergency Department
1755-599X/$ - see front matter � 2012 Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.ienj.2012.07.005
⇑ Corresponding author. Tel.: +39 3472721175.E-mail address: [email protected] (A. Bagnasco).
Annamaria Bagnasco PhD in Nursing (Nursing Researcher) a,⇑, Barbara Tubino Masters Degree in Medicine,University of Genoa, Italy, (Quality Reference Doctor Director) b, Emanuela Piccotti Masters Degree inMedicine, University of Genoa, Italy, (DEA Officer Doctor Director) b, Francesca Rosa MSN Student, CatholicUniversity of Rome, RN a, Giuseppe Aleo, Masters Degree in Languages (Lecturer of Scientific English) a,Pasquale Di Pietro Masters Degree in Medicine and Surgery, (Physician and surgeon Doctor Director) b,Loredana Sasso Masters Degree in Education Sciences, University of Genoa, Italy, (Associate Professor ofNursing) b, Donatella Passalacqua, Laura Gambino and all the nursing and medical staff of the Emergencyand Urgency Department of the IRCCS Giannina Gaslini in Genova, Italya Health Sciences Department, University of Genoa, Via Pastore 1, 16132 Genova, Italyb G. Gaslini Paediatric Teaching Hospital, Largo Gerolamo Gaslini 5, 16147 Genova, Italy
a r t i c l e i n f o a b s t r a c t
Article history:Received 19 December 2011Received in revised form 3 July 2012Accepted 12 July 2012
Keywords:Patient safetyCommunication failuresPaediatric Emergency DepartmentNon-technical skills
Objective: The aim of this study was to identify effective corrective measures to ensure patient safety inthe Paediatric Emergency Department (ED).Methods: In order to outline a clear picture of these risks, we conducted a Failure Mode and Effects Anal-ysis (FMEA) and a Failure Mode, Effects, and Criticality Analysis (FMECA), at a Emergency Department of aChildren’s Teaching Hospital in Northern Italy. The Error Modes were categorised according to Vincent’sTaxonomy of Causal Factors and correlated with the Risk Priority Number (RPN) to determine the prioritycriteria for the implementation of corrective actions.Results: The analysis of the process and outlining the risks allowed to identify 22 possible failures of theprocess. We came up with a mean RPN of 182, and values >100 were considered to have a high impactand therefore entailed a corrective action.Conclusions: Mapping the process allowed to identify risks linked to health professionals’ non-technicalskills. In particular, we found that the most dangerous Failure Modes for their frequency and harmfulnesswere those related to communication among health professionals.
� 2012 Elsevier Ltd. All rights reserved.
Introduction
Patient safety depends on the ability to design and run highlyreliable organisations (Smits, 2008), which means that such organ-isations ought to be able to reduce the risk of errors (prevention),and recover and limit the effects of errors when they occur (protec-tion). The actions may be directed towards patients (provision ofadequate care, decision support), towards staff (training, commu-nication, availability of policies/protocols), towards the organisa-tion (improved leadership/guidance, proactive risk assessment),and towards therapeutic agents and equipment (regular audits)(WHO, 2009).
In high-risk industries such as aviation, skills not directly re-lated to technical expertise, but crucial for ensuring safety (e.g.teamwork) have been categorised as ‘non-technical skills’ (Reader,2006). Non-technical skills are components of competencies andunderlie a specific ability. The first study on Non-Technical Skillsin the health-care setting was conducted in laparoscopic surgery(Mishra et al., 2008) and was drawn from other disciplines suchas aviation. This study focused on the link between technical com-petence and reliability (behavioural characteristics) and is an indexof competence. A variety of non-technical skill measures are avail-able, but only a few have been used in the emergency care area It isevident from a number of patient safety reports that teamworkskills (Mishra, 2009) and communication are essential aspects ofpatient safety (Cooper et al., 2010; Kilner and Sheppard, 2010;Department of Health, 2000). Communication among health

A. Bagnasco et al. / International Emergency Nursing 21 (2013) 168–172 169
professionals is a non-technical skill that allows to ensure thesafety for paediatric patients as well, allowing the gathering ofinformation and data that must be reported in the medical records.
In particular, Emergency Department (ED) is, by its intrinsicnature, a facility at high risk due to its specific organisational fea-tures (Redfern et al., 2009a,b), such as the need to provideunscheduled emergency care, high turnover, unfamiliar patientsand care processes exasperated by stress, noise and time pressures(Burley, 2011; Maisoon and Chi Keu Wong, 2006; Coiera andTombs, 1998).
In the UK, communication in the emergency setting has beeninvestigated through the introduction of ‘Performance Indicators’(Redfern et al., 2009a,b). The study showed high levels of commu-nication failure when transferring written information from theambulance crew. For this reason, countermeasures were intro-duced. There was a threefold improvement in the number of cor-
Ambulance
Reception of the patient
TRIAGE
NURSE
Time managementadmissions roo
assessment
PHYSICIANMedication
manageme
PHYSICIAN
Discharged Admitted to
Emergency
Clinical and nursi
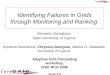
Fig. 1. Communication diagram for patient
rect clinical documents used by doctors in the resuscitation roomand a reduction of missing and incorrect information. Performanceindicators, when used for measuring the amount of time it took fora patient to go through the ED, established that it should not takemore than 4 h for the patient to go through the ED and be eitherdischarged or hospitalised (House of Commons, Committee ofPublic Accounts, 2005). This put an enormous pressure on the EDwhere risk assessment became very important in relation topatient turnover, task complexity, and left little time forcommunication.
Organisational culture influences many aspects of performanceincluding patient safety (Westrum, 1993, 2004). Organisations findsafety culture a critical factor that sets the tone for implementationof safety within their workplaces (Choudhry et al., 2007).
Communication failures are adverse events that have a negativeimpact on patient safety, a negative emotional impact on patients
NURSE
Own means
in the m
NURSE
Transferred
nt
Dept.
ng
arriving in the Emergency Department.

1. Analysis of the phases of the health care process.
2. Identification of the functions/activities.
170 A. Bagnasco et al. / International Emergency Nursing 21 (2013) 168–172
and caregivers, as well as on costs in terms of extra treatment,longer hospital stay, and lawsuits (Linda et al., 2000).
The aim of this study was to identify effective corrective mea-sures to ensure patient safety in the Paediatric Emergency Depart-ment. This study is only a part of a bigger one.
3. Identification of the error modes.
4. Calculation of the RPI Index
5. Identification of possible causes.
7. Implementation of the corrective actions
6. Identification of the corrective actions.
Methods
We conducted a prospective cohort study from April 2008 toMay 2009 including a group of 43 healthcare workers (physiciansand nurses) working in the Paediatric ED of a large Children’sTeaching Hospital.
After reviewing the literature, we divided the health care pro-cess required to go through the Emergency Department into fivedifferent phases: arrival of the patient/child; assessment of thechild’s needs and those of his/her parents; traceability of the pa-tient; transfer of the patient; and patient discharge (Fig. 1). In thisway, we could identify in which phase of the ED process presentedthe highest number of actual or potential communication errorsand defects (communication failures).
In order to identify communication failures, we adopted theFailure Mode and Effects Analysis (FMEA) and the Risk PriorityNumber (RPN) methodology. A ‘failure mode’ can be any potentialor actual error or defect in a process that affects its user. The RPN isa technique for analysing the risk associated with potential prob-lems previously identified by a FMEA analysis.
8. Evaluation of the RPI after reviewing the critical points.
IMPROVEMENT OF THE CARE PROVIDED
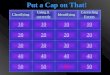
Fig. 2. The FMECA steps.
The Risk Priority Number (RPN)
RPN is a measure used when assessing risk to help identify crit-ical failure modes associated with your design or process. Failuremodes means the ways, or modes, in which something might fail.Failures are any errors or defects, especially ones that affect thecustomer, and can be potential or actual. RPN is the product ofSeverity (S), Occurrence (O), Detection (D).
After identifying which activities had a higher RPN score, wewent onto identify and analyse the possible causes of adverseevents and planned the corrective actions to be implemented toeliminate or minimise risk.
No set RPN value was established to determine when to inter-vene. For this reason, corrective actions consisted in monitoringactivities having a higher RPN score, regardless of their absolutevalue.
For ‘severity’ and ‘occurrence’, a scale from 1 to 10 was used,whereas for error detection we used a scale that went from 10 to1; so the higher the score the more it was difficult to detect an er-ror/failure and thus to control it. After assigning a score to eachitem, the RPN was calculated by multiplying the three Scores (S,O, D). Therefore, the score ranged between a maximum of 1000(10 � 10 � 10: multiplication of the top scores of S, O, D) and aminimum score of 1 (1 � 1 � 1: multiplication of the minimumscores of S, O, D). The issues, identified with the RPN scores, wereanalysed by using the Joint Commission International (JCI) stan-dards (Joint Commission International, 2009 ComprehensiveAccreditation Manual for Hospitals). The JCI standards, which wereidentified as potentially frail were used to define the priorities forthe implementation of the corrective actions. For instance, the JCIstandards ‘patient education upon discharge (the JCI InformationManagement standards) allowed the introduction of an educationassessment chart in the discharge documentation (the JCI Recordof Care, Treatment, and Services standard).
To understand if the communication was effective, we observedthe health professionals while they worked and recorded for howlong and how they communicated.
To identify the Failure Modes and the Error Modes, we con-ducted a Failure Mode and Effects Analysis (FMEA) and a FailureMode, Effects, and Criticality Analysis (FMECA) (Fig. 2).
The Failure Mode and Effects Analysis (FMEA)
Originally, FMEA was a systematic technique used to identifyand prevent problems on products or processes. FMEA has beenused for over 30 years in car, aviation, and nuclear industries(Helmreich, 2000). More recently, in 2001 JCI suggested the intro-duction of FMEA in the healthcare sector, so that it could be used asa risk prevention tool. A successful FMEA activity contributes toidentifying potential failure modes based on previous experiencewith similar products or processes, designing those failures outof the system with the minimum effort and resource expenditure,reducing development processing time and costs.
FMECA is the acronym for Failure Modes and Effects CriticalityAnalysis
The American Society for Quality (Stamatis, 2003) defines it as aprocedure that is performed after a failure mode effects analysis toclassify each potential failure effect according to its severity andprobability of occurrence.
Results
Almost 400 communication events were recorded on a grid in12 months of observation by the researchers. By analysing the

Table 1Ranking of the first eight failures modes.
Activity Severity Occurrence Detection RPN
Clinical assessment upondischarge. Untidy clinicalrecord
4 6 5 120
Assisting foreign users 6 4 8 172Assisting psychiatric users or
referred by court; socio-cultural assessment
6 4 8 172
Information for parents. Littleinformation
7 6 5 210
Filling in chart for transfer/discharge. Chart not shared
8 6 7 366
Drug administration 8 6 8 384Report on Admission to Accident
Emergency dept. lack ofinformation on nursing careand service provided
8 8 8 512
Education for caregivers 8 6 7 366Total RPN 3994 Mean 182
A. Bagnasco et al. / International Emergency Nursing 21 (2013) 168–172 171
communication events and outlining the risks, we identified 22possible process failures – Failure Modes (Table 1) ranks the first6. We came up with a mean RPN score of 182. All values with ascore >100 required a corrective action based on RP due to theirhigh impact. After analysing these data, we found that the riskswith the highest risk priority included the lack of non-technicalskills among health workers and that the most dangerous ones,for their frequency and harmfulness, included poor communica-tion, especially during transfer and discharge.
The risks we identified were grouped into three levels accordingto the RPN (Graph 1): Low risk if <100, and high risk if >100. Ateach level, we included the respective categories of risk.
Corrective actions
Corrective actions consisted in reorganizing the communicationactivities by identifying the minimum requirements of the Situa-tion–Background–Assessment–Recommendation (SBAR) tool (Haiget al., 2006), and by reviewing the clinical reports resulting fromthe implementation of the communication activities. A furthercorrective action consisted in training a multidisciplinary team
76.1
17
Average :°filling in admission forms ° incomplete communication wit ° incomplete information on form ° wrong data input ° triage assessment ° measurements made during tr ° drugs administered during triag ° social and cultural assessmen ° care for foreign patients ° little information given to paren ° untidy medical record
Low :° patient lying on a stretcher ° communication difficulties ° long waiting time ° computer system downtime ° admission time ° health services
Graph 1. Mean estimate of activity vulnerabili
(physicians, paediatric nurses and support healthcare workers) toenhance the attitude to teamwork and standardise verbal andnon-verbal communication through role-playing and simulation.The study of the error modes showed a correlation in 100% of thefailures when defining the requirements for internal communica-tion, that is, of the data needed to perform the assessment andtherefore plan the patient’s therapeutic pathway from admissionto discharge.
Our results supported the need for more appropriate communi-cation training for health professionals working in EmergencyDepartments and other similar workplaces.
Discussion
Patient safety is a critical component of health care quality. Ashealth care organisations continually strive to improve, there is agrowing recognition of the importance of establishing a cultureof patient safety (Agency for Healthcare Research and Quality,2009).
We found that the major patient safety issues had often to dowith internal communication patterns, that is, when using thetools available to plan the patient’s discharge and in ensuring theobjectiveness of the information/communication activities.
There is evidence in literature that medication errors are fre-quent in the Emergency Department (ED). The unique operationalcharacteristics of the ED may exacerbate their rate and severity(Croskerry et al., 2004; Jain et al., 2009; Patanwala, 2010).
In addition, there is evidence in literature (Yu and Green, 2009)that the Emergency Department (ED) chart is the only lasting re-cord of an ED examination, and ED documentation and communi-cation are important aspects of the prevention of errors. Deficits incommunication and information transfer at hospital discharge arecommon and may adversely affect patient care (Kriplalani et al.,2007).
Information and support should be provided to the family dur-ing nursing interventions regardless of the family’s decision to bepresent or not (Patricia, 2008; Porter et al., 2011).
We shall test the SBAR technique (Mishra et al., 2009) as correc-tive measure with respect to communication errors. This tool in-cludes standard communication requirements to test the efficacyof information transmission. The tool was built with the NO-TECHtaxonomy and sets the standards of health workers’ non-technical
392.0
2.1
High :° drug administration ° filling in discharge card ° filling in chart for transfer to Emergency Medicine ° Parent education
h parentss
iagee
t
ts
ty according to the PRI Index (risk index).

172 A. Bagnasco et al. / International Emergency Nursing 21 (2013) 168–172
skills. Educational interventions on communication standards shallalso include relational skills.
An interesting aspect deserving further research may involvethe analysis of some communication issues identified during tri-age, even though they had a lower RPN.
Limitations
The main limitation of our study was that we only focused onpaediatric nurses and physicians working in the Paediatric ED,excluding patients/children and their parents.
Conclusions
Paediatric Accident and Emergency Departments are by natureplaces with a high turnover of patients and time-pressured work-ing conditions, leaving health workers with very little time to ob-tain full information on patients and the risk of making mistakesis high. The present study highlighted the risks raised by healthworkers’ poor communication skills during patient dischargeand/or transfer.
Recommendations
The tools we identified to mitigate risk and in particular mem-ory failures were the SBAR technique and ‘‘rapid briefing’’, whichcan uniform different styles of communication and optimise tim-ing and communication patterns among health workers. GianninaGaslini Institute introduced a patient transfer and discharge chart,since the mean RPN was 392.0 (Table 1) and also organised a train-ing session for physicians and paediatric nurses to develop thecommunication SBARs (2009–2010).
Ethical approval
This study was approved by the Ethical Committee of the‘Giannina Gaslini’ Children’s Teaching Hospital in Genoa, Italy.
Acknowledgements
We thank the health care professionals working in the Paediat-ric Emergency Department of the Children’s Teaching Hospital‘Giannina Gaslini’ of Genoa, in Italy, and particularly the Collabora-tive Group: Donatella Passalacqua, Laura Gambino, DanielaMarchesi, Laura Peresi, Sonia Bianchi, and Daniela Soddu.
References
Agency for Healthcare Research and Quality, 2009. Hospital Survey on PatientSafety Culture: Comparative Database Report.
American Society for Quality: FMEA. <http://www.asq.org/info/glossary/f.html>(28.04.05).
Burley, D., 2011. Better communication in the emergency department. Emerg.Nurse 19 (2), 32–36.
Choudhry, R.M., Fang, D., Mohamed, S., 2007. The nature of safety culture: a surveyof the state-of-the-art. Saf. Sci. 45, 993–1012.
Coiera, E., Tombs, V., 1998. Communication behaviours in a hospital setting: anobservational study. BMJ 316, 673–676.
Cooper, S., Endacott, R., Cant, R., 2010. Measuring non-technical skills in medicalemergency care: a review of assessment measures. Emerg. Med. 2, 7–16.
Croskerry, P., Shapiro, M., Campbel, S., LeBlanc, C., Sinclair, D., Wren, P., Marcoux, M.,2004. Profiles in patient safety: medication errors in the emergencydepartment. Acad. Emerg. Med. 11 (3), 289–299.
Department of Health, 2000. An Organisation with a Memory. Department ofHealth, London.
Haig, K.M., Sutton, S., Whittington, J., 2006. SBAR: a shared mental model forimproving communication between clinicians joint commission. J. Qual. PatientSaf. 32 (3), 167–175(9).
Helmreich, R.L., 2000. On error management: lessons from aviation. BMJ 320, 781–785.
House of Commons Committee of Public Accounts Department of Health, 2004–05.Improving Emergency Care in England 16th Report of Session 2004–05.
Jain, S., Basu, S., Parmar, V.R., 2009. Medication errors in neonates admitted inintensive care unit and emergency department. Indian J. Med. Sci. 63 (4), 145–151.
Joint Commission International, 2009. Comprehensive Accreditation Manual forHospitals.
Kilner, E., Sheppard, L.A., 2010. The role of teamwork and communication in theemergency department: a systematic review. Int. Emerg. Nurs. 18 (3), 127–137.
Kriplalani, S., LeFevre, F., Phillips, C.O., 2007. Deficits in communication andinformation transfer between hospital-based and primary care physicians:implications for patient safety and continuity of care. JAMA 297 (8), 831–841.
Linda, T., Corrigan, J.M., Donaldson, M.S., 2000. To Err is Human Building a SaferHealth System. Institute of Medicine.
Maisoon, A.G., Chi Keu Wong, I., 2006. Medication errors in paediatric patients.Arch. Dis. Child Educ. Pract. Ed. 91, ep20.
Mishra, A., 2009. The Oxford NOTECHS system: reliability and behaviour in theoperating theatre validity of a tool for measuring teamwork, 18, 104–108. doi:http://dx.doi.org/10.1136/qshc.2007.024760.
Mishra, A., Catchpole, K., Dale, T., McCulloch, P., 2008. The influence of non-technical performance on technical outcome in laparoscopic cholecystectomy.Surg. Endosc. 22, 68–73.
Patanwala, A.E., 2010. A prospective observational study of medication errors in atertiary care emergency department. Ann. Emerg. Med. 55 (6), 522–526 (Epub2010 January 15).
Patricia, J., 2008. Patient- and family-centered care of children in the emergencydepartment. Pediatrics 122 (2), e511–e521.
Porter, S.C., Johnston, P., Parry, G., Damian, F., 2011. Improving parent-providercommunication in the pediatric emergency department: results from the clearand concise communication campaign. Pediatr. Emerg. Care 27 (2), 75–80.
Reader, T., 2006. Non-technical skills in the intensive care unit. Br. J. Anaesth. 96 (5),551–559.
Redfern, E., Brown, R., Vincent, C.A., et al., 2009a. Improving communication in theemergency department. Emerg. Med. J. 26, 658–661.
Redfern, E., Brown, R., Vincent, C.A., 2009b. Identifying vulnerabilities incommunication in the emergency department. Emerg. Med. J. 26, 653–657.
Smits, M., 2008. Exploring the causes of adverse events in hospitals and potentialprevention strategies. Qual. Saf. Health Care 2010 (19), 1–7. http://dx.doi.org/10.1136/qshc.030726.
Stamatis, D.H., 2003. DH Failure Mode Effect Analysis: FMEA from Theory toExecution, second ed. American Society for Quality, Quality Press, Milwakee,53203.
WHO, 2009. Final Technical Report: Conceptual Framework for the InternationalClassification for Patient Safety.
Yu, K.T., Green, R.B., 2009. Critical aspects of emergency department documentationand communication. Emerg. Med. Clin. North Am. 27 (4), 641–54, ix.