Embed Size (px)
Citation preview

Identification of Optimal Combinations for Empirical Dual Antimicrobial Therapy ofPseudomonas aeruginosa Infection: Potential Role of a Combination Antibiogram • Author(s): Mari Mizuta , MD; Darren R. Linkin , MD; Irving Nachamkin , DrPH, MPH;Neil O. Fishman , MD; Mark G. Weiner , MD; Angela Sheridan , MPH; Ebbing Lautenbach, MD, MPH, MSCE Source: Infection Control and Hospital Epidemiology, Vol. 27, No. 4 (April 2006), pp. 413-415Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiologyof AmericaStable URL: http://www.jstor.org/stable/10.1086/503175 .
Accessed: 15/05/2014 09:20
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaboratingwith JSTOR to digitize, preserve and extend access to Infection Control and Hospital Epidemiology.
http://www.jstor.org
This content downloaded from 194.29.185.136 on Thu, 15 May 2014 09:20:15 AMAll use subject to JSTOR Terms and Conditions

infection control and hospital epidemiology april 2006, vol. 27, no. 4
c o n c i s e c o m m u n i c a t i o n
Identification of Optimal Combinationsfor Empirical Dual AntimicrobialTherapy of Pseudomonas aeruginosaInfection: Potential Roleof a Combination Antibiogram
Mari Mizuta, MD; Darren R. Linkin, MD;Irving Nachamkin, DrPH, MPH; Neil O. Fishman, MD;Mark G. Weiner, MD; Angela Sheridan, MPH;Ebbing Lautenbach, MD, MPH, MSCE
To better determine the optimal combinations for empirical dual an-timicrobial therapy of Pseudomonas aeruginosa infection, we evaluatedthe utility of a novel combination antibiogram. Although the com-bination antibiogram allowed modest fine-tuning of choices for dualantibiotic therapy, selections based on the 2 antibiograms did not differsubstantively. Drug combinations with the broadest coverage wereconsistently composed of an aminoglycoside and a b-lactam.
Infect Control Hosp Epidemiol 2006; 27:413-415
Infections due to antibiotic-resistant bacteria are associatedwith increased morbidity and mortality.1,2 Administration ofinadequate empirical antibiotic therapy has been frequentlyassociated with increased mortality.3-6 A common cause ofinadequate therapy is infection with an antibiotic-resistantpathogen.5 One potential option is to use empirical dual an-timicrobial therapy, with the hope that at least one of theselected agents will be active against the infecting pathogen.Dual therapy is commonly used when infection due to Pseu-domonas aeruginosa is suspected. The methods by which toidentify the optimal combination of agents remain elusive.In the current best-case scenario, one would consult the localantibiogram to determine the 2 agents to which P. aeruginosais most often susceptible. However, it is unclear whether thisis the optimal way to select the 2 antimicrobials for dualtherapy. For example, if all isolates resistant to drug A arealso resistant to drug B, combining these drugs achieves noincrease in coverage. The optimal antibiogram to consult forcombination therapy would have information regarding whichdual therapy achieves the greatest coverage for P. aeruginosa.To better determine the optimal combination of antimicrobialagents for empirical therapy of P. aeruginosa infection, weevaluated the utility of a novel combination antibiogram. Toour knowledge, no studies have evaluated such a combinationantibiogram.
methods
We identified all clinical inpatient P. aeruginosa isolates ob-tained at our institution from January 1, 1999, through De-
cember 31, 2003. If multiple P. aeruginosa isolates were ob-tained from the same patient from the same anatomic sitewithin the same hospitalization, only the first isolate wasincluded. This study was reviewed and approved by the Uni-versity of Pennsylvania Committee on Studies Involving Hu-man Beings.
Different methods were used to identify P. aeruginosa dur-ing the study period. From January 1, 1999, through De-cember 31, 2002, we used the following criteria of the Clin-ical and Laboratory Standards Institute (CLSI; formerly, theNCCLS): oxidase positive, typical smell, and recognizable col-ony structure.7 Blood isolates were further confirmed usingMicroScan (Dade-Behring). After January 1, 2003, these cri-teria were used for isolates recovered from all anatomic sites.For other oxidase-positive gram-negative rods that did nothave typical characteristics, we used the following commercialidentification systems: MicroScan (Dade-Behring) until Sep-tember 30, 2002, and Vitek II (bioMerieux) after that date.Antimicrobial susceptibility testing was performed using Mi-croScan conventional susceptibility microbroth dilution traysuntil September 1, 2002, and Vitek II susceptibility cards afterthat date. Susceptiblity to the following agents was tested andreported: amikacin, aztreonam (through 2002), cefepime, cef-tazidime (through 2000), ciprofloxacin (through 2000), gen-tamicin, imipenem, levofloxacin, piperacillin, and tobramy-cin. Susceptibility data were interpreted according to CLSIguidelines.8
To compare the combination antibiogram with a standardantibiogram, we created a standard antibiogram for P. aeru-ginosa isolates for each study year. We then constructed an-nual combination antibiograms in a matrix fashion, listingthe tested antimicrobial agents both horizontally and verti-cally. In each box of this matrix, we noted the number andpercentage of isolates susceptible to at least 1 of the 2 agents.
results
A total of 3,143 P. aeruginosa strains were identified duringa 5-year period. Of these, 2,217 (70.5%) were from urine,244 (7.8%) were from blood, and 682 (21.7%) were fromother sites. The number of isolates recovered from specimensobtained in intensive care units was 1,607 (51.1%).
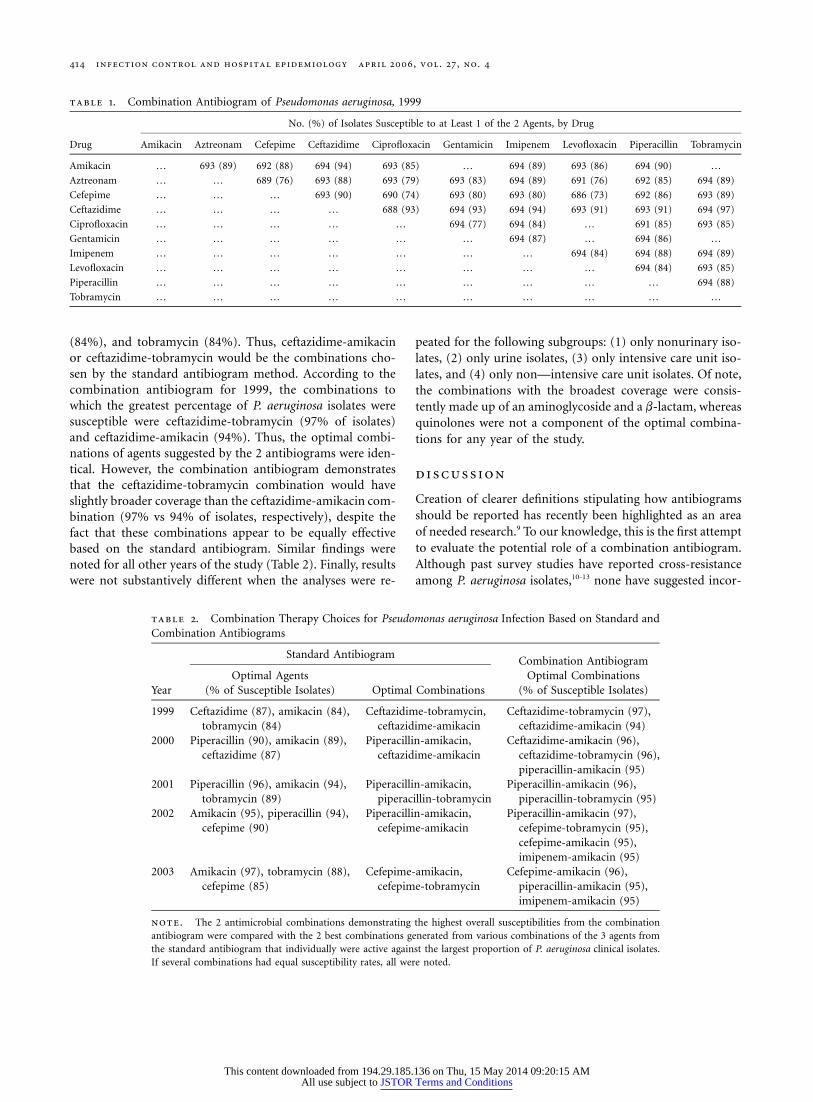
Table 1 is a combination antibiogram for 1999. Compar-isons of the likely choices of dual empirical antimicrobialtherapy based on the 2 antibiogram methods are presentedin Table 2. The comparisons in Table 2 assume that clinicianswho use the standard antibiogram would most likely selectas combination therapy the 2 antimicrobials to which, in-dividually, the greatest percentage of P. aeruginosa isolates wassusceptible. For example, in the standard antibiogram for1999, the agents to which P. aeruginosa isolates were mostoften susceptible were ceftazidime (87% of isolates), amikacin
This content downloaded from 194.29.185.136 on Thu, 15 May 2014 09:20:15 AMAll use subject to JSTOR Terms and Conditions
414 infection control and hospital epidemiology april 2006, vol. 27, no. 4
table 1. Combination Antibiogram of Pseudomonas aeruginosa, 1999
Drug
No. (%) of Isolates Susceptible to at Least 1 of the 2 Agents, by Drug
Amikacin Aztreonam Cefepime Ceftazidime Ciprofloxacin Gentamicin Imipenem Levofloxacin Piperacillin Tobramycin
Amikacin … 693 (89) 692 (88) 694 (94) 693 (85) … 694 (89) 693 (86) 694 (90) …
Aztreonam … … 689 (76) 693 (88) 693 (79) 693 (83) 694 (89) 691 (76) 692 (85) 694 (89)
Cefepime … … … 693 (90) 690 (74) 693 (80) 693 (80) 686 (73) 692 (86) 693 (89)
Ceftazidime … … … … 688 (93) 694 (93) 694 (94) 693 (91) 693 (91) 694 (97)
Ciprofloxacin … … … … … 694 (77) 694 (84) … 691 (85) 693 (85)
Gentamicin … … … … … … 694 (87) … 694 (86) …
Imipenem … … … … … … … 694 (84) 694 (88) 694 (89)
Levofloxacin … … … … … … … … 694 (84) 693 (85)
Piperacillin … … … … … … … … … 694 (88)
Tobramycin … … … … … … … … … …
table 2. Combination Therapy Choices for Pseudomonas aeruginosa Infection Based on Standard andCombination Antibiograms
Year
Standard AntibiogramCombination Antibiogram
Optimal Combinations(% of Susceptible Isolates)
Optimal Agents(% of Susceptible Isolates) Optimal Combinations
1999 Ceftazidime (87), amikacin (84),tobramycin (84)
Ceftazidime-tobramycin,ceftazidime-amikacin
Ceftazidime-tobramycin (97),ceftazidime-amikacin (94)
2000 Piperacillin (90), amikacin (89),ceftazidime (87)
Piperacillin-amikacin,ceftazidime-amikacin
Ceftazidime-amikacin (96),ceftazidime-tobramycin (96),piperacillin-amikacin (95)
2001 Piperacillin (96), amikacin (94),tobramycin (89)
Piperacillin-amikacin,piperacillin-tobramycin
Piperacillin-amikacin (96),piperacillin-tobramycin (95)
2002 Amikacin (95), piperacillin (94),cefepime (90)
Piperacillin-amikacin,cefepime-amikacin
Piperacillin-amikacin (97),cefepime-tobramycin (95),cefepime-amikacin (95),imipenem-amikacin (95)
2003 Amikacin (97), tobramycin (88),cefepime (85)
Cefepime-amikacin,cefepime-tobramycin
Cefepime-amikacin (96),piperacillin-amikacin (95),imipenem-amikacin (95)
note. The 2 antimicrobial combinations demonstrating the highest overall susceptibilities from the combinationantibiogram were compared with the 2 best combinations generated from various combinations of the 3 agents fromthe standard antibiogram that individually were active against the largest proportion of P. aeruginosa clinical isolates.If several combinations had equal susceptibility rates, all were noted.
(84%), and tobramycin (84%). Thus, ceftazidime-amikacinor ceftazidime-tobramycin would be the combinations cho-sen by the standard antibiogram method. According to thecombination antibiogram for 1999, the combinations towhich the greatest percentage of P. aeruginosa isolates weresusceptible were ceftazidime-tobramycin (97% of isolates)and ceftazidime-amikacin (94%). Thus, the optimal combi-nations of agents suggested by the 2 antibiograms were iden-tical. However, the combination antibiogram demonstratesthat the ceftazidime-tobramycin combination would haveslightly broader coverage than the ceftazidime-amikacin com-bination (97% vs 94% of isolates, respectively), despite thefact that these combinations appear to be equally effectivebased on the standard antibiogram. Similar findings werenoted for all other years of the study (Table 2). Finally, resultswere not substantively different when the analyses were re-
peated for the following subgroups: (1) only nonurinary iso-lates, (2) only urine isolates, (3) only intensive care unit iso-lates, and (4) only non—intensive care unit isolates. Of note,the combinations with the broadest coverage were consis-tently made up of an aminoglycoside and a b-lactam, whereasquinolones were not a component of the optimal combina-tions for any year of the study.
discussion
Creation of clearer definitions stipulating how antibiogramsshould be reported has recently been highlighted as an areaof needed research.9 To our knowledge, this is the first attemptto evaluate the potential role of a combination antibiogram.Although past survey studies have reported cross-resistanceamong P. aeruginosa isolates,10-13 none have suggested incor-
This content downloaded from 194.29.185.136 on Thu, 15 May 2014 09:20:15 AMAll use subject to JSTOR Terms and Conditions

combination antibiogram and p. aeruginosa infection 415
porating this information into a combination antibiogram.The finding that the information provided by the standard
antibiogram was largely sufficient to select the optimal an-timicrobial combinations is likely the result of rarity of cross-resistance to both b-lactams and aminoglycosides. Combi-nation of these 2 antimicrobial classes for empirical treatmentagrees with standard recommendations for hospital-acquiredsepsis syndrome.14 Frequent quinolone resistance, also de-scribed in other studies,15,16 resulted in this class of agentsnot being included in the optimal combinations for any yearof our study. However, our study tested a protocol for choos-ing a combination regimen for empirical treatment solely onthe basis of susceptibility results for P. aeruginosa. Ultimatechoice of regimen made by clinicians also rests on otherfactors, such as suspected pathogens, likely site of infection,patient allergies, drug penetration into different tissue sites,and drug toxicity.
There are several potential limitations to the study. Al-though it is desirable to target a variety of gram-negativepathogens when selecting empirical therapy, analyses werelimited to P. aeruginosa isolates. These isolates were chosenas a model, because infections with this virulent pathogenrepresent a significant percentage of healthcare-acquired in-fections.17 Also, isolates from the same patient were includedin the analysis if they were recovered during different hos-pitalizations. However, these repeat isolates would be ex-pected to affect the standard antibiogram and combinationantibiogram similarly. Finally, because microbial resistancepatterns are often institution specific, it is imperative that anyrecommendations for empirical therapy, combination or oth-erwise, be based on local susceptibility data.
In summary, although a novel combination antibiogramallows modest fine-tuning of empirical antimicrobial regi-mens, the antimicrobial choices based on a novel combina-tion antibiogram do not differ substantively from those basedon a standard antibiogram. The optimal combinations wereconsistently found to be a combination of a b-lactam and anaminoglycoside. Future studies investigating other pathogensor, perhaps, evaluating a combination antibiogram that in-cludes simultaneously all gram-negative isolates, are war-ranted to determine the potential role of the combinationantibiogram in selecting empirical therapy directed at abroader range of organisms.
acknowledgments
This work was supported by the Public Health Service grant DK-02987-01from the National Institutes of Health (Dr. Lautenbach) and by the Centersfor Education and Research on Therapeutics grant U18-HS10399 from theAgency for Healthcare Research and Quality.
Drs. Mizuta, Linkin, Fishman, and Lautenbach are from the Division ofInfectious Diseases and Dr. Weiner is from the Division of General InternalMedicine, Department of Medicine, Dr. Lautenbach is from the Departmentof Biostatistics and Epidemiology, Drs. Nachamkin and Sheridan are fromthe Department of Pathology and Laboratory Medicine, and Drs. Linkin and
Lautenbach are from the Center for Clinical Epidemiology and Biostatisticsand the Center for Education and Research on Therapeutics, University ofPennsylvania School of Medicine, Philadelphia, Pennsylvania.
Address reprint requests to Ebbing Lautenbach, MD, MPH, MSCE, Centerfor Clinical Epidemiology and Biostatistics, University of Pennsylvania Schoolof Medicine, 825 Blockley Hall, 423 Guardian Drive, Philadelphia, PA 19104-6021 ([email protected]).
Received September 15, 2004; accepted January 10, 2005; electronicallypublished March 17, 2006.
� 2006 by The Society for Healthcare Epidemiology of America. All rightsreserved. 0899-823X/2006/2704-0016$15.00.
references
1. Cohen ML. Epidemiology of drug resistance: implications for a post-antimicrobial era. Science 1992; 257:1050-1055.
2. Holmberg SD, Solomon SL, Blake PA. Health and economic impacts ofantimicrobial resistance. Rev Infect Dis 1987; 9:1065-1078.
3. Leibovici L, Shraga I, Drucker M, Konigsberger H, Samra Z, Pitlik SD.The benefit of appropriate empirical antibiotic treatment in patients withbloodstream infection. J Intern Med 1998; 244:379-386.
4. Weinstein MP, Towns ML, Quartey SM, et al. The clinical significanceof positive blood cultures in the 1990s: a prospective comprehensiveevaluation of the microbiology, epidemiology, and outcome of bacter-emia and fungemia in adults. Clin Infect Dis 1997; 24:584-602.
5. Ibrahim EH, Sherman G, Ward S, Fraser VJ, Kollef MH. The influenceof inadequate antimicrobial treatment of bloodstream infection on pa-tient outcome in the ICU setting. Chest 2000; 118:146-155.
6. Alvarez-Lerna F. Modification of empiric antibiotic treatment in patientswith pneumonia acquired in the intensive care unit: ICU-Acquired Pneu-monia Study Group. Intensive Care Med 1996; 22:387-394.
7. National Committee for Clinical Laboratory Standards (NCCLS). Ab-breviated Identification of Bacteria and Yeast; Approved Guideline. Wayne,PA: NCCLS; 2002. NCCLS document M35-A.
8. National Committee for Clinical Laboratory Standards (NCCLS). Per-formance Standards for Antimicrobial Susceptibility Testing. Wayne, PA:NCCLS; 2001. NCCLS approved standard M100-S11.
9. Ernst EJ, Diekema DJ, BootsMiller BJ, et al. Are United States hospitalsfollowing national guideline for the analysis and presentation of cu-mulative antimicrobial susceptibility data? Diagn Microbiol Infect Dis2004; 49:141-145.
10. Takigawa K, Fujita J, Negayama K, et al. Comparing antimicrobial activityagainst resistant Pseudomonas aeruginosa using an index for the absenceof cross-resistance. J Antimicrob Chemother 1995; 35:425-427.
11. Bouza E, Garcia-Garrote F, Cercenado E, Martin M, Diaz MS, for theSpanish Pseudomonas aeruginosa Study Group. Pseudomonas aeruginosa:a survey of resistance in 136 hospitals in Spain. Antimicrob Agents Che-mother 1999; 43:981-982.
12. Bonfiglio G, Carciotto V, Russo G, et al. Antibiotic resistance in Pseu-domonas aeruginosa: an Italian study. J Antimicrob Chemother 1998; 41:307-310.
13. Friedland I, Stinson L, Ikaiddi M, Harm S, Woods GL. Phenotypic an-timicrobial resistance patterns in Pseudomonas aeruginosa and Acineto-bacter: results of a multicenter intensive care unit surveillance study,1995-2000. Diagn Microbiol Infect Dis 2003; 45:245-250.
14. Young LS. Sepsis syndrome. In: Mandell GL, Bennett JE, Dolin R, eds.Principles and Practice of Infectious Diseases. 5th ed. Philadelphia, PA:Churchill Livingstone; 2000:806-819.
15. Flamm RK, Weaver MK, Thornsberry C, Jones ME, Karlowsky JA, SahmDF. Factors associated with relative rates of antibiotic resistance in Pseu-domonas aeruginosa isolates in clinical laboratories in the United Statesfrom 1999 to 2002. Antimicrob Agents Chemother 2004; 48:2431-2436.
16. Fluit AC, Verhoef J, Schmitz FJ. Antimicrobial resistance in Europeanisolates of Pseudomonas aeruginosa. European Sentry Participants. Eur JClin Microbiol Infect Dis 2000; 19:370-374.
17. National Nosocomial Infections Surveillance (NNIS) system report, datasummary from January 1992 through June 2003, issued August 2003.Am J Infect Control 2003; 31:481-498.
This content downloaded from 194.29.185.136 on Thu, 15 May 2014 09:20:15 AMAll use subject to JSTOR Terms and Conditions





























