Embed Size (px)
Citation preview

ability of exercise echocardi multivesse? disease and to a combined with clinical and exercise test variables.
From the Division of Cardiovascular Diseases and internal Medicine and the Section of Biostatistics, Mayo Clinic and Mayo Foundation. Roth . . *. Minnesota.
Manuscript received October 2, 1993; revised manuscript received I cb- ru 11, 1994.
Dr. Veronique L. Roger, Mayo Clinic, 200 First Street SW, Rochester, Minnesota 55905.
91994 by the American College of Cardiology
variables recorded tic exa~~at~5~ are
use of a
use of ant~ype~e~s~ve medicative. iabetes melkus was
ce ~r~t~c~~ was used for 76% of
ate exercise duration with that of th usual clinical and EC6 data were ret
load was 6.6 2 2.2 metabolic equivalents. ECG was normal, a test was considered positive if it had
0735-1097/941$7.00
110 ROGER ET AL. CORONARY ARTERY DISEASE IN EXERCISE ECHOCARDIOGRAPHY
JACCC Vol. 24, No. I July 1 : 109-14
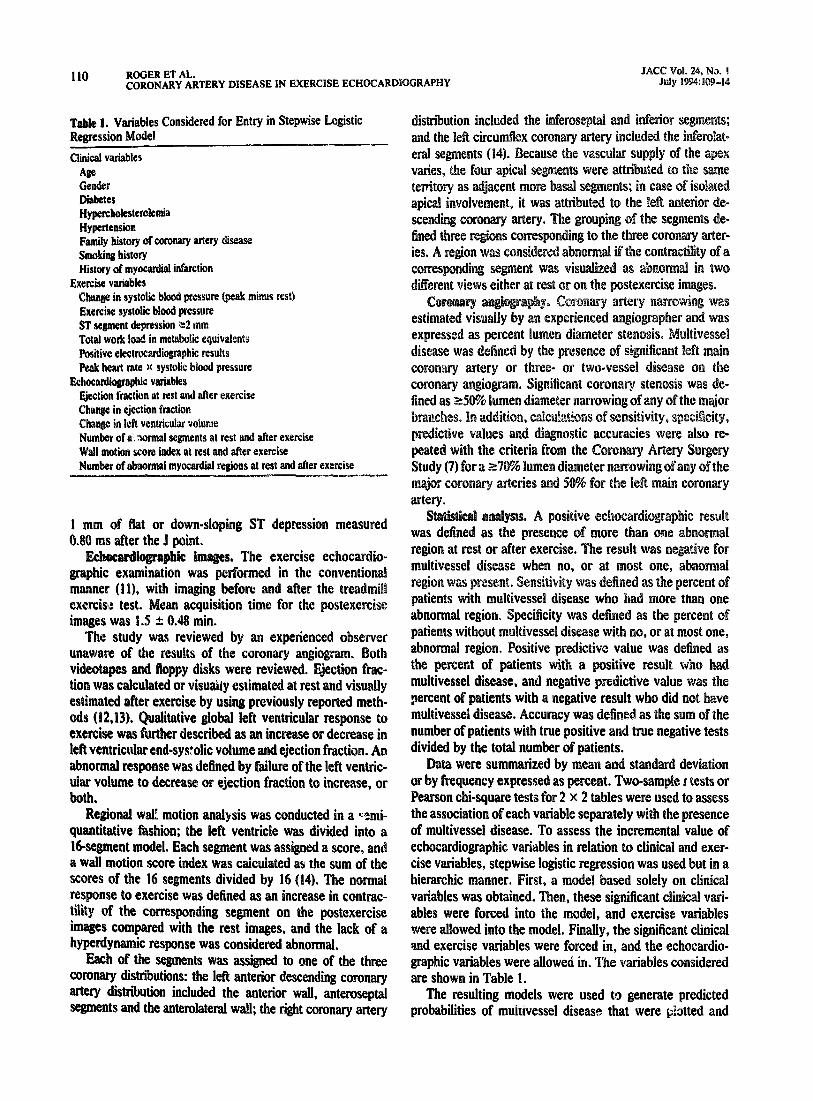
Variables Considered for Entry in Stepwise Logistic
Clinical VariableS
& Gender Diabetes Hypwcboksterolemia
Hypertension
tiun at rest and nftcr exercise
Number of alwnnal mywardial regions at rest and after exercise
1 mm of flat or down-sloping ST depression measured
The exercise ~chocardio- ed in the conventional
and floppy disks were tion was calculated or visWy estimated at rest and visually esti er exercise by using previously reported metb- ods . Qualitative global left ventricular re exercise was further described as an increase or decrease in left ventricular end-sys?olic volume and ejection fraction. An abnormal response was defined by failure of the left ventric- ular volume to decrease or ejection fraction to increase, or both.
Regional walE motion analysis was conducted in a c%mi- quantitative fashion; the left ventricle was divided into a N-segment model. Each segment was assigned a score, and a wall motion score index was calculated as the sum of the scores of the 16 segments divided by I6 (14). The normal response to exercise was defined as an increase in contrac- tility of the corresponding segment on the postexercise
s compared with the rest images, and the lack of a rdynamic response was considered abnormal.
Each of the segments was assigned to one of the three coronary distributions: the left anterior descending coronary artery distriiution included the anterior wall, anteroseptal segments and the anterolateral wall; the right coronary artery
percent of patients with a negative result who did not have multivessel disease. Accuracy was defined as the sum of the number of patients with true positive and true negative tests
the total number of patients. re summarized by mean and standard deviation ncy expressed as percent. Two-sample t tests or
Pearson chi-square tests for 2 x 2 tables were used to assess the association of each variable separately witb the presence of multivessel disease. To assess the incremental value of
phic variables in relation to clinical and exer- stepwise logistic regression was used but in a
hierarchic manner. First, a rn~e~ based solely on clinic variables was obtained. Then, these significant clinical vari- ables were forced into the model, and exercise variables
ed into the model. Finally, the significant clinical e variables were force , and the echocardio-
graphic variables were allowed in. variables considered are shown in Table 1.
The resulting models were used to generate predicted probabilities of multivessel disease that were platted and
JAW Vd. 24. No. t July I -14
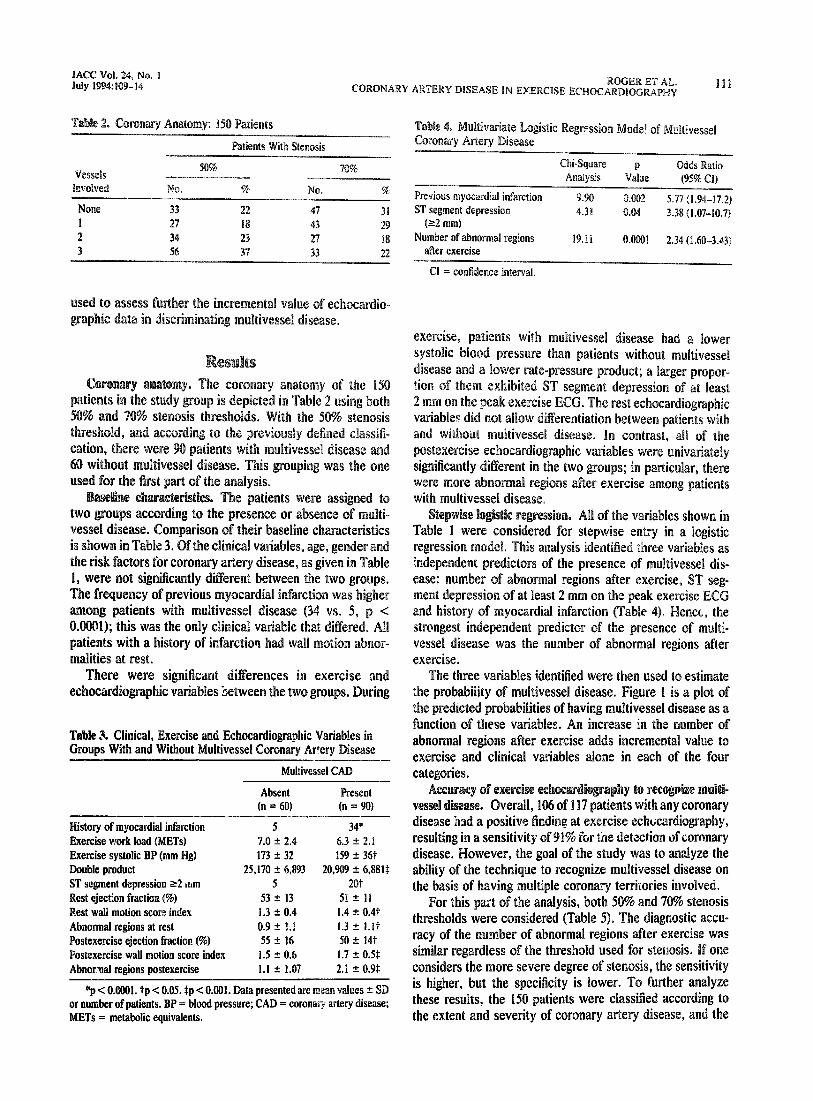
VFXlS 50% 70%
EM3lVtX.l No. 5% No. %
None 33 22 47 31 I 27 18 43 29 2 34 23 27 18 3 .56 37 33 22
- Absent Present (n = 60) (n = 90)
~~~.- History of myocardial infarction 5 34’ Exercise work load (METS) 7.0 f 2.4 6.3 _+ 2.1 Exercise systolic BP (mm Hg) 173 f 32 159 f 36t Double product 25,170 t 6,893 20. 2 6.881$ ST segment depression ~2 atim 5 20t Rest ejection fraction (%) 53 + 13 51 + 11 Rest wall motion score index 1.3 + 0.4 1.4 * 0.4t Abnormal regions at rest 0.9 i: !.! 1.3 + i.it Postexercise ejection fraction (%) 55 zh 16 so + 14t
Postexercise wall motion score index 1.5 z!z 0.6 1.7 f 0.51
Abnor.nal regions postexercise I.1 i: 1.07 2.1 + 0.91:
*p < O.OOOl. tp < 0.05. Sp < 0.001. Data presented are mean values + SD or number of patients. BP = blood pressure; CAD = coronary artery disease; METS = metabolic equivalents.
Chi-Square p
Previous myocardial infarction ST segment depression
(=2 mm)
Number of a~~or~a~ regions after exercise
9. 5.77 :1.94-17.2)
4.39 0.04 3.38 (1.07-10.7)
19.11 0. 2.34 (1.60-3.43)
CI = confidence interval.
ase in the number of
disease kid a positive finding at exercise ec~~card~o~~a~~~y,
considers the more severe degree of stenosis, the sensitivity is higher, but the specificity is lower. To further analyze these results, the 150 patients were classified according to the extent and severity of coronary artery
112 ROGER ET AL. JACC Vol. 24, No. 1
CORONARY ARTERY DISEASE IN EXERCISE ECHOCARDIOGRAPHY July 1 : Km-14
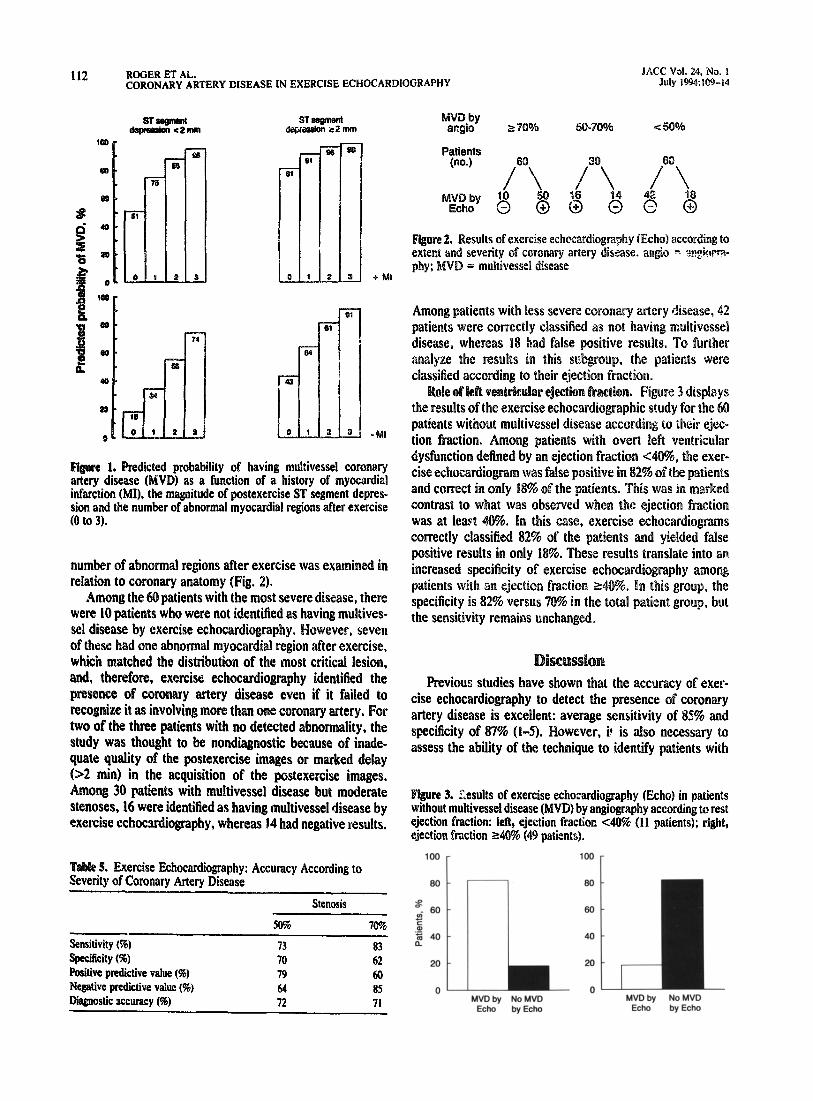
1, Predicted probability of having multivessel coronary disease (MVD) as a function of a history of myocardial
infarction (MI), the magnitude of postexercise ST segment depres- sion and the number of abnormal myocardial regions after exercise (0 to 3).
number of abnormal regions after exercise was examined in ary anatomy (Fig. 2). patients with the most severe disease, there
were 10 patients who w se1 disease by exercise of these had one abnor which matched the distribution of the most critical lesion, and, therefore, exercise echocardiography identified the presence of coronary artery disease even if it failed to
ize it as involving more than one coronary artery. For the three patients with no detected abnormality, the
nostic because of inade- quate quality of the postexercise images or marked deiay
n) in the acquisition of the postexercise images. 30 patients with multivessel disease but moderate
stenoses, 16 were identified as having multivessel disease by exercise echocardiography, whereas 14 had negative results.
5. Exercise Echocardiography: Accuracy According to Severity of Coronary Artery Disease
Stenosis
Sensitivity (%) Specificity (96) Ftsitive pwlictive value (%I Negative predictive value (%) LXagnostic accuracy (%)
50% 70%
73 83 70 62 79 60 64 85 72 71
t-e 2. Results of exercise ~choca~diogra~hy (Echo) according to severity of coronary artery disease. angio - ~~&7+ = multivessel disease
ents with less severe c~~~~a~y a
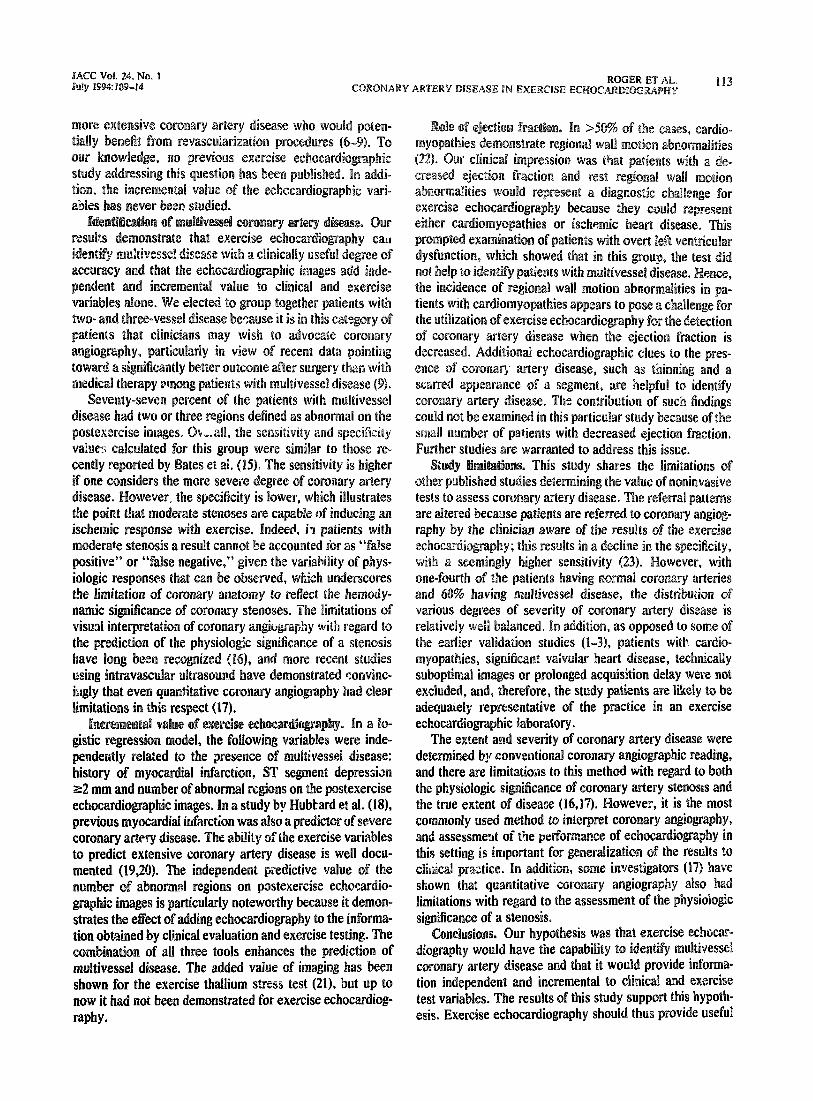
dysfunct~o~ defined by an ejection f~~tiQ~
positive results in only 18%. These results
s~e~ificity is 82% versus 78% in the total patient group, but the sensitivity remains unchanged.
Frevious studies b the accuracy of exer- cise echocardiography to detect the presence of coronar artery disease is excellen average sensitivity of 85% an specificity of 87% (l-5). owever, i* is also necessary to assess the ability of the technique to identify patients with
re 3. Results of exercise echocardiography (Echo) in patients without multivessel disease (MVD) by angiography according to rest ejection fraction: left, ejection fraction 4076 (11 patients); right, ejection fraction r4’o (49 patients).
100 100
80 80
s $M 60
5 ‘5 0. 40 40
20 20
n n MVDby NoMVD MVDby NoMVD
Echo by Echo Echo by Echo
namic sig~ific~~~e of coronary stenoses.
pendeutly related to the presence of rn~~t~v~ss~~ disease: history of myocardial infarction, ST segment depressian 82 mm and number of abnormal regions on the postexercise echocardiographic images. In a study by Hubbard et al. (IS), previous myocardil infarction was also a predictor of severe coronary artery disease. The ability of the exercise variables to predict extensive coronary artery disease is well docu- mented (19,20). The ~n~e~e~d~~t predictive value of number of abnormal regions on poste
particularly notewo~h of adding ecbocard~ogra~by to the info clinical evaluation and exercise testing.
~ornb~~atio~ of ah three tools enhances the prediction of multivessel disease. The ad ed value of imaging has shown for the exercise thallium s?ress test (211, but up to now it had not been demonstrated for exercise echocardiog- raphy .
patients wtth m~~t~vesse~ disease. Hence,
sease. The contributi
ecanse pattents are re to coronary aoggrog-
owever, tt is the most commonly used method to ~~te~ret coronary angiography, and assessmeltt of the performance of echoc~d~ogra~hy in this setting is im~o~a~t for ge~era~i~atio~ of the results !.o clirkal pm&e. In addnt ’ ion, some i~ve5t~gators (17) have
antitative corotaary angi regard to tbe assessment
coronary artery disease a tion independent and inc test variables. The results of this study suppoti this hypoth-
esis. Exercise echocardiography should thus

114 ROGER ET AL. JACC Vol. 24, No. 1 CORONARY ARTERY DISEASE IN EXERCISE ECHOCARDIOGRAPHY
information tu assist in the clinical decision of w~~t~e~ or not to proceed with coronary angiography and revasculariza- tion.
1. Limacher MC, Qmsones iriA, Pohner LR, Nelson JG, Winters WL Jr. disease with exercise two- of a clinically applicable ntriculography. Circulation
5.
3.
5.
6.
‘an JJ, Suarez J. Zo~bbi
he randomized European Coronary
1.
a,
9.
IO.
inv& Stnnerv Study KASS)
tom and their associates. Coals Artery randomized trial of coronarv arterv bv - _
ty; survival data. Circuhition ~~3;~:939-~~ _ , Davis KB, Gillespie MJ. Kitlip T. and the CASS p~ncipa~ and their associates. A r~omi~ed trial ofcoronarv arterv
bY ry: survival of patients with a tow ejection fraction.sN f&l J Med 198.%:312:166s-71. hluhR?aier LH, Fryor DR. Rankin JS. et al. Dbse~at~ona~ co evenbfree survival with medical and surgical therapy in pat coronary artery disease: 2O years of follow-up. Circuhtion 1992
Potlock ML, Witmore JH. Exercise in
ebabi~itatio~~ 2nd ed. ~bilade~~b~a:
Exercise ecb~ardiograpby. J Am Sot ~c~~a~~~~~r 1988;1:161-6.
12. S. Sbiekb A, Gallastepi 9. Rondos 67’. Mason rminafion of left ventricular ejection fraction by visual estimation
ducts real-time lw0~ime~sioma~ echocar apby. Am Heart J 1982;
13. Amico AR. L~c~te~~r~ GS, Reisner SA, Stone eltzer RS. Srtperiority of visaal versus c0mpMte~zed ecboc
esti~tion of radioa~c~~de left ve~t~cu~ar ejection fraction.
14. Craw et at. Omme~datio~s for qua ricfe b imensi ecb~~d~o~m~hy. J A 23358-67.
IS.
17.
18.
19.
20.
21.
22.
to predict the extent 07 cor0~~~ disease witk abnormal wall motion at rest labstractl. Circulation I
in patients
. et al. s visual ~ntet~retati~~ of the
Davidson CJ. Sbeikh isslo RR. et al. ~~l~c0~o~a~ rrltrasound evahratio tervent J Cardiot t991;68: I305-9. ~Mbbard ibbons s~~e~ste~ AR. elements Ii’. ~dent~~cat~o~ of $~vere coron
meters. Arch alter Med isease using simple c~~~i~~
Shetld LT. Exercise stress testing. I ~Mnw~ld E. &or. &afi Disease: A Texlbook of Ca~iovascu~~ icine, 3rd ed. ~~i~ade~phia:
cation of patients with left main and three vessel coronary disease witk clinical and exercise ties1 variables. Am J Cardiol il Polbck SG. Abbott RD.
ict multivessel coronary artery disease from the e
Wallis DE. O’Connell JR, Henkin RR. Cost~nz~~ord~n Setq~retnal waf’ motion ab~o~m~~ties in aviated cardiomyo~a?by: a com- n.. . . . _ - - mon nnamg ana good prognostic sags. J Am Coil Cardiol l9~;~~74-9.
23. rris D. Swan ~culo~a~hy.





























