Embed Size (px)
Citation preview

APPLIED AND ENVIRONMENTAL MICROBIOLOGY, Dec. 2005, p. 8738–8743 Vol. 71, No. 120099-2240/05/$08.00�0 doi:10.1128/AEM.71.12.8738–8743.2005Copyright © 2005, American Society for Microbiology. All Rights Reserved.
Identification and Localization of Extraradicular Biofilm-FormingBacteria Associated with Refractory Endodontic Pathogens
Nobuo Noguchi, Yuichiro Noiri,* Masahiro Narimatsu, and Shigeyuki EbisuDepartment of Restorative Dentistry and Endodontology, Osaka University Graduate School of Dentistry,
1-8, Yamadaoka, Suita, Osaka 565-0871, Japan
Received 11 April 2005/Accepted 3 August 2005
Bacterial biofilms have been found to develop on root surfaces outside the apical foramen and be associatedwith refractory periapical periodontitis. However, it is unknown which bacterial species form extraradicularbiofilms. The present study aimed to investigate the identity and localization of bacteria in human extrara-dicular biofilms. Twenty extraradicular biofilms, used to identify bacteria using a PCR-based 16S rRNA geneassay, and seven root-tips, used to observe immunohistochemical localization of three selected bacterialspecies, were taken from 27 patients with refractory periapical periodontitis. Bacterial DNA was detected from14 of the 20 samples, and 113 bacterial species were isolated. Fusobacterium nucleatum (14 of 14), Porphyromo-nas gingivalis (12 of 14), and Tannellera forsythensis (8 of 14) were frequently detected. Unidentified anduncultured bacterial DNA was also detected in 11 of the 14 samples in which DNA was detected. In the biofilms,P. gingivalis was immunohistochemically detected in all parts of the extraradicular biofilms. Positive reactionsto anti-F. nucleatum and anti-T. forsythensis sera were found at specific portions of the biofilm. These findingssuggested that P. gingivalis, T. forsythensis, and F. nucleatum were associated with extraradicular biofilmformation and refractory periapical periodontitis.
More than 300 different bacterial species are known to in-habit the healthy human mouth (9). This multitude of micro-biota can infect the root canal in a nonvital tooth, and themicroorganisms and their components might have etiologicroles in refractory or chronic periodontitis. However, only asmall numbers of species have been consistently isolated frominfected root canals of periapically affected teeth (26). Mixedbacterial biofilms in root canals of periapical periodontitis-affected teeth have been investigated microbiologically (3, 5,10, 17, 25) and morphologically (6, 19).
Clinically, we encounter cases in which periapical periodon-tal disease does not heal despite the debridement of biofilm inthe root canals. It has been believed that bacteria could notexist in periapical lesions at the chronic phase as a conse-quence of the local immune response (7). Recently, though,evidence has been found regarding the presence of bacteriawithin extraradicular areas (29, 30) and periapical lesions (16,23, 24). In general, an extraradicular area is used clinically as aterm that contrasts to a root canal, which ends at the apicalforamen of the root apex. On the boundary of the apicalforamen, moreover, the root canal surface connects to thetooth surface (cementum) outside the root apex or occasion-ally to the extruded root canal filling material from a rootcanal. The solid parts connected with the root canal surface arecalled the extraradicular area; although the area is located inthe periapical lesion, it is expressed as distinguished from thelesion, while the lesions mean the part with the alveolar boneresorption around the root apex in which soft tissue, for ex-ample, granulation tissue, exists in many cases.
It was thought that viable bacteria could not inhabit the areaover the apical foramen without an acute phase of periapicalperiodontitis. We found morphologically that biofilms wereformed in the extraradicular area and proposed that extrara-dicular biofilms, developing from the root canal via an apicalforamen and consisting of multiple morphotypic bacteria, wereattached to the cementum around the root apex (12). It hasbeen reported that gram-positive facultative anaerobes, forexample, Enterococcus faecalis, Streptococcus sanguis, andStreptococcus intermedius, have the ability to colonize and formextracellular matrices on the surface of gutta-percha points,while serum plays a crucial role in biofilm formation in vitro(27). Gutta-percha points were the root canal filling materialswhen debridement of bacteria in the root canal was completed.We found that the surface of these points extruded from theroot canal could also become a scaffold for biofilm formationin vivo (12).
As biofilms are resistant to antibiotic treatment and immuneresponses (4), we speculate that microorganisms may also beable to survive at the extraradicular area. Once biofilms formin the extraradicular area, it is impossible to remove those onthe root surfaces by nonsurgical endodontic treatments. Ex-traradicular biofilms can become refractory periapical patho-gens; however, little is known about the bacterial componentsin extraradicular biofilms. Therefore, human extraradicularbiofilms of refractory periapical periodontitis-affected teethwere used to identify biofilm-forming bacteria and to investi-gate the immunohistochemical localization of detected bacte-ria.
MATERIALS AND METHODS
Subjects and clinical materials. Twenty-seven volunteer patients (eight malesand 19 females, 21 to 72 years of age) with refractory periapical periodontitiswere enrolled in the study. All selected teeth had previously received endodontictreatment, showed a periapical radiolucent area, and had no root fracture or
* Corresponding author. Mailing address: Department of Restor-ative Dentistry and Endodontology, Osaka University GraduateSchool of Dentistry, 1-8, Yamadaoka, Suita, Osaka 565-0871, Japan.Phone: 81-6-6879-2927. Fax: 81-6-6879-2927. E-mail: [email protected].
8738

periodontal pocket formation at the root apex. Samples were obtained frompatients whose periapical lesions could not be healed clinically despite repeatedendodontic treatment at the Osaka University Dental Hospital and thus the teethwere clinically judged as having refractory periapical periodontitis. Table 1 showsthe characteristics and clinical symptoms of all subjects before extraction. In-formed consent was obtained from all patients in accord with the protocolapproved by the Ethics Committee of the Osaka University Graduate School ofDentistry.
Strains, culture conditions, and preparation of antisera. The sources andculture conditions of Porphyromonas gingivalis 381, Fusobacterium nucleatum1436, and Tannerella forsythensis ATCC 43037 used in the present study were aspreviously described (13, 15, 31). P. gingivalis 381 was grown in brain heartinfusion broth (Difco Laboratories, Detroit, Mich) containing 5 �g/ml hemin and1 �g/ml menadione. F. nucleatum 1436 was grown in Todd-Hewitt broth (Difco)containing 0.5 �g/ml L-cysteine. T. forsythensis ATCC 43037 was grown in brainheart infusion broth containing 0.5% yeast exact, 5 �g/ml hemin, 0.5 �g/mlmenadione, 0.001% N-acetylmuramic acid (Sigma Chemical Co., St. Louis, Mo.),and 5% fetal bovine serum (Gibco BRL, Grand Island, N.Y.). Mass cultureswere grown anaerobically (90% N2, 5% CO2, and 5% H2) at 37°C for 48 h. Cellswere also harvested as described (15).
The preparation and purification of the antisera against the three bacterialspecies have been described previously (15, 31). Rabbit antiserum againstT. forsythensis was provided by K. Maeda (Kyushu University, Fukuoka, Japan)(31).
Sampling procedure, DNA extraction and PCR amplification of the 16S rRNAgene. The 20 samples used were nine extracted teeth and 11 apical fragmentsobtained from apicoectomies. The teeth and root tips were immediately washedwith sterile saline to remove blood and planktonic bacteria. Extraradicular bio-film specimens were taken to curettage the root surfaces around the root apex.
The method of Rolph et al. (17) was used for DNA extraction. Solution fromthe Puregene DNA purification kit (Flowgen) was added to samples, which wereincubated at 37°C for 45 min. Samples were pelleted and resuspended in 100 �lof Tris-EDTA buffer and stored at �20°C until required. Negative controlsamples from an intact tooth extracted by orthodontic treatment were processedby the same method. Genomic DNA from P. gingivalis 381 was used as a positivecontrol.
PCR was performed by a previously described method (8). The primers used,which target 16S rRNA, were 63f (5�-CAGGCCTAACACATGCAAGTC-3�)and 1387r (5�-GGGCGGWGTGTACAAGGC-3�) (8).
Cloning of mixed 16S rRNA gene products. Mixed PCR products were ex-tracted after agarose gel electrophoresis, using the QIAEX gel extraction kit(QIAGEN, Hilden, Germany) and ligated into the pDrive cloning vector(QIAGEN), followed by transformation into Escherichia coli DH5� cells(TOYOBO, Osaka, Japan). Usually, more than 300 transformants for each PCRlibrary were obtained. Ninety-six colonies were randomly selected from eachlibrary and then transferred from the transformation plates to Plusgrow (Na-calai-tesque, Kyoto, Japan) liquid medium containing ampicillin. After overnightincubation at 37°C, plasmid DNA was purified with a QIAprep Spin miniprep kit(QIAGEN).
Sequencing analysis. Purified plasmid DNA from the cloning procedure waspartially sequenced using an ABI PRISM 3100 Genetic Analyzer (Applied Bio-systems, Foster City, CA) and a Big Dye Terminator cycle sequencing kit (Ap-plied Biosystems). As previously described by Rolph et al. (17), the sequences ofeach clone were submitted to the NCBI database (http://www.ncbi.nlm.nih.gov/BLAST/) as queries. The BLAST program (version 2.1) (1, 2) was used todetermine the highest identity to known sequences in the database, and clonesequences with from 98 to 100% identity with the database were considered to beof the same bacterial species. In addition, sequences with from 90 to 98% identitywere considered to be of the same bacterial genus, while an identity of 90% wasused as the cutoff for positive identification of taxa. Multiple alignment of
TABLE 1. Characteristics and clinical features of patients beforesample extractiona
Sampleno.
Patientgender
Age(yr)
Toothno.
Surgicaltreatment
Sponta-neouspain
Percus-sionpain
Palpa-tion Fistula
1 F 41 38 E � � � �2 F 27 11 AP � � � �3 F 55 25 E � � � �4 F 59 24 E � � � �5 M 54 25 E � � � �6 F 21 46 E � � � �7 F 25 16 AP � � � �8 F 36 43 AP � � � �9 M 40 46 E � � � �10 F 69 23 E � � � �11 F 62 14 AP � � � �12 F 29 17 E � � � �13 M 72 31 E � � � �14 F 23 21 AP � � � �15 M 62 22 AP � � � �16 F 64 24 AP � � � �17 M 31 12 AP � � � �18 F 49 12 AP � � � �19 F 60 12 AP � � � �20 M 47 21 AP � � � �21 M 47 21 AP � � � �22 F 36 44 AP � � � �23 F 56 15 AP � � � �24 F 48 24 AP � � � �25 F 19 21 AP � � � �26 M 54 22 E � � � �27 F 25 25 E � � � �
a F, female; M, male; E, extraction; AP, apicoectomy.
TABLE 2. Prevalence of bacterial species identified in14 extraradicular samples
Genus or species matchNo. of
samplesdetected
Clone
No. Proportion(% of total)
Fusobacterium nucleatum 14 74 6.13Porphyromonas gingivalis 12 340 28.17Unidentified bacterium 11 73 6.05Prevotella sp. 10 52 4.31Tannerella forsythensis 8 136 11.27Eubacterium sp. 7 32 2.65Porphyromonas sp. 7 19 1.57Prevotella intermedia 7 27 2.24Bacteroides-like sp. 5 42 3.48Bilophila wadsworthia 5 10 0.83Corynebacterium matruchotii 5 5 0.41Desulfobulbus sp. 5 23 1.91Fusobacterium sp. 5 10 0.83Porphyromonas gulae 5 40 3.31Bacteroidales oral clone 4 23 1.91Dialister sp. 4 5 0.41Leptotrichia sp. 4 4 0.33TM7 phylum sp. 4 5 0.41Actinomyces sp. 3 3 0.25Campylobacter gracilis 3 3 0.25Capnocytophaga sp. 3 7 0.58Capnocytophaga sputigena 3 4 0.33Chloroflexi genomosp. 3 12 0.99Haemophilus paraphrophilus 3 12 0.99Lachnospiraceae oral clone 3 3 0.25Rothia dentocariosa 3 6 0.50Unidentified bacterium 3 5 0.41Veillonella sp. 3 9 0.75Actinomyces gerencseriae 2 7 0.58Actinomyces naeslundii 2 3 0.25Atopobium rimae 2 6 0.50Bacteroides sp. 2 12 0.99Capnocytophaga granulose 2 2 0.17Corynebacterium glucuronolyticum 2 8 0.66Corynebacterium sp. 2 3 0.25Human oral bacterium 2 2 0.17Peptostreptococcus sp. 2 6 0.50Prevotella denticola 2 2 0.17Providencia stuartii 2 18 1.49Rahnella sp. 2 2 0.17Unidentified Prevotella sp. 2 22 1.82Unidentified Eubacterium 2 3 0.25
VOL. 71, 2005 EXTRARADICULAR BIOFILM-FORMING BACTERIA 8739

bacterial genes was performed by the CLUSTAL W program (28). Concentration ofthe unrooted phylogenetic tree was carried out by the neighbor-joining method (18).Evaluation of the topology of the phylogenetic tree and determination of the con-fidence values were carried out by previously described methods (17).
Histopathological and immunohistochemical procedures. Five selected teethand two root tips were carefully fixed in 4% paraformaldehyde and 0.1% glu-taraldehyde for 12 h at 4°C and decalcified for 10 days at 4°C with stirring in 10%formic acid-sodium citrate (pH 2.2); 8-�m-thick serial frozen sections wereprepared. Some of the sections were stained by the Brown and Brenn-modifiedGram staining procedure, while others were subjected to the alkaline phos-phatase-conjugated streptavidin-biotin method (13–15). The results of bothstaining methods were observed under a light microscope (Optiphot-2; Nikon,Tokyo, Japan).
RESULTS
Identification of bacteria in extraradicular biofilm. From 14of the 20 extraradicular biofilm samples, 1,207 clones wereanalyzed and 113 bacterial genera and species were identified.
DNA was not detected in the other six extraradicular samples.Table 2 shows that bacterial DNA was detected in at least twoof the 14 positive samples. DNA of F. nucleatum (14 of 14), P.gingivalis (12 of 14), T. forsythensis (8 of 14), and Prevotellaintermedia (7 of 14) were frequently detected in all extrara-dicular samples. Unidentified and uncultured bacterial DNAwas also detected in 11 of the 14 samples in which DNA wasdetected (Table 2). DNA of E. faecalis and Porphyromonasendodontalis was detected in just 1 sample. From the results ofthe partial 16S rRNA sequences of 35 clones from samples 1 to6, 23 bacterial strains were identified and 11 uncultured orunidentified bacteria were detected (Fig. 1).
Specificity of immunohistochemical labeling. Antiseraagainst P. gingivalis, F. nucleatum, and T. forsythensis werereacted with homogenous bacterial cells. Five gram-positivebacteria (Actinomyces naeslundii ATCC 19246, Streptococcus
FIG. 1. Phylogenetic tree of the bacterial genes in an extraradicular biofilm based on 16S rRNA genes. The tree was established from an analysisof the sequences examined in samples 1 to 6. The scale bar indicates neighbor-joining distance and 10% differences in nucleotide sequences.
8740 NOGUCHI ET AL. APPL. ENVIRON. MICROBIOL.

mutans MT 8148, Streptococcus sanguis ST-3R, Staphylococcusaureus FDA 209P, and Propionibacterium acnes ATCC 11829),and three other gram-negative bacterial species (Actinobacillusactinomycetemcomitans ATCC 29522, Prevotella intermediaATCC 33563, and Treponema denticola ATCC 33520) exam-ined for cross-reaction were not labeled with any of the threeantisera used. In healthy root apex tissues (negative control),no background or any reaction with the three antisera wasobserved.
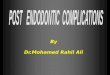
Histopathological and immunohistochemical evaluations.In three of the seven root tip samples, extraradicular biofilmsof 30 to 40 �m thickness were found on the tooth surfacesoutside of the root apex area (Fig. 2a). Red-stained gram-negative bacteria were observed predominantly in the biofilm(Fig. 2b). In the other four samples, microcolonies that formedsmall numbers of bacterial cells were studded around the ce-mentum surfaces of the root apex. In all samples examined,residual microorganisms were detected in the root canals closeto the root apex (Fig. 2a).
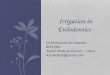
Positive reactions with anti-P. gingivalis, anti-F. nucleatum,and anti-T. forsythensis sera were found in three of the samplesthat had observed extraradicular biofilm (samples 1, 2, and 3).The photographs are typical images, and their distributionshows a similar tendency for each of the bacterial species in thethree positive samples (Fig. 3a to c). Positive reactions with
anti-P. gingivalis were distributed from the cementum to thesuperficial layer of the biofilm, and were scattered throughoutthe extraradicular biofilm (Fig. 3b). Labeled F. nucleatum andT. forsythensis cells are shown at specific parts of the biofilms(Fig. 3a and c).
DISCUSSION
Initially, we speculated that specific bacteria that could resisthost immunocytes might invade in the extraradicular area andform biofilm; because it has been considered that the expan-
FIG. 2. Histopathological evaluation around the root apex (crosssection views). (a) Whole image of a serial section. In the extraradicu-lar area located at the radicular tooth surface outside of the vicinity ofthe root apex, biofilms indicated by arrows are shown. Residual bac-teria, indicated by an arrowhead in the root canal, are detected. RC,root canal. Magnification, �40. (b) High-power view of the inset in a.Arrows indicate that gram-negative rods and filamentous microorgan-isms are located in the extraradicular biofilm. Magnification, �625.
FIG. 3. Immunohistochemical evaluation in extraradicular bio-films. (a, b, and c) Arrowheads indicate the junction between the toothsurface and the biofilm. (a and c) Arrows indicate immunohistochemi-cally positive reactions. (a) In the anti-F. nucleatum-positive sample,positive reactions distribute predominantly at the middle within thebiofilm. Magnification, �400. (b) In the anti-P. gingivalis-positive sam-ple, the reactions are scattered throughout the extraradicular biofilm.Magnification, �400. (c) In the anti-T. forsythensis-positive sample,positive reactions are localized at the most superficial layer. Magnifi-cation, �400.
VOL. 71, 2005 EXTRARADICULAR BIOFILM-FORMING BACTERIA 8741

sion of periapical lesions results from local immune responses(type III and IV allergy), and that bacteria could not inhabitlesions at the chronic phase (21). Various bacterial speciesdetected are associated with biofilm formation at the extrara-dicular area in many cases of chronic and refractory periapicalperiodontitis is a novel finding.
Infected root canal isolates have been investigated by someresearchers using molecular techniques, and F. nucleatum andP. gingivalis were frequently identified (3, 5, 17). However, themethod of identifying bacteria using bacterium-specific PCRprimers is a technique to detect just the DNA of the targetbacterium and is not suitable for qualitative analysis of largenumbers of unknown bacterial species. Several studies havereported that obligate anaerobes are not frequently detected inthe periapical periodontal disease-affected root canal usingconventional culture systems (10, 17, 22, 25). The PCR-based16S rRNA gene assay is useful for identifying a wide range ofanaerobic bacteria that are difficult to grow by standard culturemethods.
Until recently, it was considered that endodontic treatmentfailure was in many cases the result of microorganisms persist-ing in the apical portion of the root canal system. F. nucleatum,P. gingivalis, T. forsythensis, and P. intermedia were detected inthe periapical lesion contents of asymptomatic root-filled teethusing DNA and DNA hybridization and fluorescence in situhybridization (23, 24). In their studies, experimental materialswere obtained from the periapical lesion contents, and bacteriawere detected within the granulation tissues. It was possiblethat bacteria outside of the lesions in the oral cavity invadedthe lesion via the fistula and contaminated it. On the otherhand, we found extraradicular biofilms in both this and previ-ous studies, in 14 of 20 and 9 of 11 (12) samples examined,respectively. Moreover, the bacterial species detected fromextraradicular biofilms were also detected from the root canalin the same teeth at the high rate of 86.7% (data not shown).These results strongly suggested that bacteria that remained inthe root canal but invading from a fistula could become asupply source for extraradicular biofilm formation and that thebacteria inhabiting not only the root canal but also the extrara-dicular area were one of the causes of refractory periapicalperiodontitis.
Recently, P. gingivalis cells adhering to the root surface weredetected at the bottom of human periodontal pockets (11, 14,15), and it has been suggested that P. gingivalis plays a role asan early colonizer in biofilm formation under most anaerobicconditions. It is proposed that P. gingivalis, observed in closecontact with the root surface (Fig. 3b), takes part in the initialadherence as an early colonizer in the extraradicular area, aswell as at the bottom of human periodontal pockets.
Unidentified and uncultivatable bacteria were detected inextraradicular and root canal biofilms in 11 of 20 and five of six(data not shown) samples examined, respectively, althoughabout half the number of bacterial species inhabiting the hu-man oral cavity were uncultivatable (4). The result of tree viewanalysis clearly showed that the clone sequences of unidenti-fied and uncultured bacteria represented ones similar to thesekinds of genera and species. The correlations between thesedetected bacteria and clinical symptoms and endodonticpathogenicity remain undetermined.
In dental practice, the development of new diagnosis meth-
ods and treatments for extraradicular biofilms is needed, sincebiofilms are difficult to remove by routine endodontic therapy,and so their presence encourages and maintains local infec-tions.
ACKNOWLEDGMENTS
Katsumasa Maeda is thanked for anti-T. forsythensis antiserum.This study was supported by Grants-in-Aid for Scientific Research
(14207080 and 15592019) from the Japan Society for the Promotionof Science and via a 21st Century COE program entitled Origination ofFrontier BioDentistry at the Osaka University Graduate School ofDentistry, from the Ministry of Education, Culture, Sports, Scienceand Technology.
REFERENCES
1. Altschul, S. F., W. Gish, W. Miller, E. W. Myers, and D. J. Lipman. 1990.Basic local alignment search tool. J. Mol. Biol. 215:403–410.
2. Altschul, S. F., T. L. Madden, A. A. Schaffer, J. Zhang, Z. Zhang, W. Miller,and D. J. Lipman. 1997. Gapped BLAST and PSI-BLAST: a new generationof protein database search programs. Nucleic Acids Res. 25:3389–3402.
3. Conrads, G., S. E. Gharbia, K. Gulabivala, F. Lampert, and H. N. Shah.1997. The use of a 16s rDNA directed PCR for the detection of endodon-topathogenic bacteria. J. Endodont. 23:433–438.
4. Costerton, J. W., P. S. Stewart, and E. P. Greenberg. 1999. Bacterial biofilms:a common cause of persistent infections. Science 284:1318–1322.
5. Fouad, A. F., J. Barry, M. Caimano, M. Clawson, Q. Zhu, R. Carver, K.Hazlett, and J. D. Radolf. 2002. PCR-based identification of bacteria asso-ciated with endodontic infections. J. Clin. Microbiol. 40:3223–3231.
6. Fukushima, H., K. Yamamoto, K. Hirohata, H. Sagawa, K. P. Leung, andC. B. Walker. 1990. Localization and identification of root canal bacteria inclinically asymptomatic periapical pathosis. J. Endodont. 16:534–538.
7. Langeland, K., R. M. Block, and L. I. Grossman. 1977. A histopathologicand histobacteriologic study of 35 periapical endodontic surgical specimens.J. Endodont. 3:8–23.
8. Marchesi, J. R., T. Sato, A. J. Weightman, T. A. Martin, J. C. Fry, S. J. Hiom,D. Dymock, and W. G. Wade. 1998. Design and evaluation of useful bacte-rium-specific PCR primers that amplify genes coding for bacterial 16SrRNA. Appl. Environ. Microbiol. 64:795–799.
9. Moore, W. E. 1987. Microbiology of periodontal disease. J. Periodont. Res.22:335–341.
10. Munson, M. A., T. Pitt-Ford, B. Chong, A. Weightman, and W. G. Wade.2002. Molecular and cultural analysis of the microflora associated with end-odontic infections. J. Dent. Res. 81:761–766.
11. Noiri, Y., and S. Ebisu. 2000. Identification of periodontal disease-associatedbacteria in the “plaque-free zone”. J. Periodontol. 71:1319–1326.
12. Noiri, Y., A. Ehara, T. Kawahara, N. Takemura, and S. Ebisu. 2002. Partic-ipation of bacterial biofilms in refractory and chronic periapical periodonti-tis. J. Endodont. 28:679–683.
13. Noiri, Y., L. Li, and S. Ebisu. 2001. The localization of periodontal-disease-associated bacteria in human periodontal pockets. J. Dent. Res. 80:1930–1934.
14. Noiri, Y., L. Li, F. Yoshimura, and S. Ebisu. 2004. Localization of Porphy-romonas gingivalis-carrying fimbriae in situ in human periodontal pockets.J. Dent. Res. 83:941–945.
15. Noiri, Y., K. Ozaki, H. Nakae, T. Matsuo, and S. Ebisu. 1997. An immuno-histochemical study on the localization of Porphyromonas gingivalis, Campy-lobacter rectus and Actinomyces viscosus in human periodontal pockets.J. Periodont. Res. 32:598–607.
16. Ramachandran Nair, P. N. 1987. Light and electron microscopic studies ofroot canal flora and periapical lesions. J. Endodont. 13:29–39.
17. Rolph, H. J., A. Lennon, M. P. Riggio, W. P. Saunders, D. MacKenzie, L.Coldero, and J. Bagg. 2001. Molecular identification of microorganisms fromendodontic infections. J. Clin. Microbiol. 39:3282–3289.
18. Saitou, N., and M. Nei. 1987. The neighbor-joining method: a new methodfor reconstructing phylogenetic trees. Mol. Biol. Evol. 4:406–425.
19. Sen, B. H., B. Piskin, and T. Demirci. 1995. Observation of bacteria andfungi in infected root canals and dentinal tubules by SEM. Endodont. Dent.Traumatol. 11:6–9.
20. Socransky, S. S., R. J. Gibbons, A. C. Dale, L. Bortnick, E. Rosenthal, J. B.Macdonald. 1963. The microbiota of the gingival crevice area of man. I.Total microscopic and viable counts and specific organisms. Arch. Oral Biol.8:275–280.
21. Stashenko, P. 1998. Etiology and pathogeneses of pulpitis and apical peri-odontitis, p. 42–67. In D. Ørstavic and T. R. Pitt Ford (ed.), Essentialendodontology, vol. 3. Blackwell Science, Oxford, United Kingdom.
22. Sunde, P. T., I. Olsen, G. J. Debelian, and L. Tronstad. 2002. Microbiota ofperiapical lesions refractory to endodontic therapy. J. Endodont. 28:304–310.
23. Sunde, P. T., I. Olsen, U. B. Gobel, D. Theegarten, S. Winter, G. J. Debelian,
8742 NOGUCHI ET AL. APPL. ENVIRON. MICROBIOL.

L. Tronstad, and A. Moter. 2003. Fluorescence in situ hybridization (FISH)for direct visualization of bacteria in periapical lesions of asymptomaticroot-filled teeth. Microbiology 149:1095–1102.
24. Sunde, P. T., L. Tronstad, E. R. Eribe, P. O. Lind, and I. Olsen. 2000.Assessment of periradicular microbiota by DNA-DNA hybridization. End-odont. Dent. Traumatol. 16:191–196.
25. Sundqvist, G. 1992. Associations between microbial species in dental rootcanal infections. Oral Microbiol. Immunol. 7:257–262.
26. Sundqvist, G. 1994. Taxonomy, ecology, and pathogenicity of the root canalflora. Oral Surg. Oral Med. Oral Pathol. 78:522–530.
27. Takemura, N., Y. Noiri, A. Ehara, T. Kawahara, N. Noguchi, and S. Ebisu.2004. Single species biofilm-forming ability of root canal isolates on gutta-percha points. Eur. J. Oral Sci. 112:523–529.
28. Thompson, J. D., D. G. Higgins, and T. J. Gibson. 1994. CLUSTAL W:improving the sensitivity of progressive multiple sequence alignment throughsequence weighting, position-specific gap penalties and weight matrix choice.Nucleic Acids Res. 22:4673–4680.
29. Tronstad, L., F. Barnett, and F. Cervone. 1990. Periapical bacterial plaque inteeth refractory to endodontic treatment. Endodont. Dent. Traumatol. 6:73–77.
30. Tronstad, L., F. Barnett, K. Riso, and J. Slots. 1987. Extraradicular end-odontic infections. Endodont. Dent. Traumatol. 3:86–90.
31. Yoneda, M., T. Hirofuji, N. Motooka, K. Nozoe, K. Shigenaga, H. Anan, M.Miura, H. Kabashima, A. Matsumoto, and K. Maeda. 2003. Humoral im-mune responses to S-layer-like proteins of Bacteroides forsythus. Clin. Diagn.Lab. Immunol. 10:383–387.
VOL. 71, 2005 EXTRARADICULAR BIOFILM-FORMING BACTERIA 8743