Embed Size (px)
Citation preview

Cancer Therapy: Preclinical
Identification of an Immunogenic Subset ofMetastatic Uveal MelanomaLuke D. Rothermel1, Arvind C. Sabesan1, Daniel J. Stephens1, Smita S. Chandran1,Biman C. Paria1, Abhishek K. Srivastava1, Robert Somerville1, John R.Wunderlich1,Chyi-Chia R. Lee2, Liqiang Xi2, Trinh H. Pham2, Mark Raffeld2, Parthav Jailwala3,Manjula Kasoji3, and Udai S. Kammula1
Abstract
Purpose: Uveal melanoma is a rare melanoma variant with noeffective therapies once metastases develop. Although durablecancer regression can be achieved in metastatic cutaneous mela-noma with immunotherapies that augment naturally existingantitumor T-cell responses, the role of these treatments for met-astatic uveal melanoma remains unclear. We sought to define therelative immunogenicity of these two melanoma variants anddetermine whether endogenous antitumor immune responsesexist against uveal melanoma.
Experimental Design: We surgically procured liver metastasesfrom uveal melanoma (n ¼ 16) and cutaneous melanoma(n ¼ 35) patients and compared the attributes of their respectivetumor cell populations and their infiltrating T cells (TIL) usingclinical radiology, histopathology, immune assays, and whole-exomic sequencing.
Results: Despite having common melanocytic lineage, uvealmelanoma and cutaneous melanoma metastases differed in their
melanin content, tumor differentiation antigen expression, andsomatic mutational profile. Immunologic analysis of TIL culturesexpanded from these divergent forms of melanoma revealed cuta-neous melanoma TIL were predominantly composed of CD8þ
T cells, whereas uveal melanoma TIL were CD4þ dominant. Reac-tivity against autologous tumor was significantly greater in cutane-ous melanoma TIL compared with uveal melanoma TIL. However,we identified TIL from a subset of uveal melanoma patients whichhad robust antitumor reactivity comparable in magnitude withcutaneous melanoma TIL. Interestingly, the absence of melaninpigmentation in the parental tumor strongly correlated with thegeneration of highly reactive uveal melanoma TIL.
Conclusions: The discovery of this immunogenic group ofuveal melanoma metastases should prompt clinical efforts todetermine whether patients who harbor these unique tumors canbenefit from immunotherapies that exploit endogenous antitu-mor T-cell populations. Clin Cancer Res; 22(9); 2237–49.�2015 AACR.
IntroductionUveal melanoma is a rare and aggressive variant of melano-
ma that has specific origin within the vascular layers of the eye,including the choroid, ciliary body, and iris (collectively knownas the uvea; ref. 1). Although uveal melanoma is the mostcommon intraocular tumor in adults, it accounts for only 3% ofall melanomas (2). With an annual incidence of 5.1 per millionin the United States, uveal melanoma is significantly lesscommon than cutaneous melanomas. Interestingly, uveal
melanoma and cutaneous melanoma have a shared lineage,with each arising from neural crest-derived melanocytes that areresident to their respective tissues of origin (3). Both forms ofmelanoma, consequently, share prominent expression of pro-totypic melanocytic differentiation antigens (MDA), such asMART-1, gp100, and tyrosinase (4–6). Despite these similari-ties, uveal melanoma can be distinguished from cutaneousmelanoma by characteristic cytogenetic changes (7) and anunusual predilection to primarily metastasize to the liver(1). Further, there exists a striking dichotomy between theclinical management of patients with advanced uveal melano-ma and cutaneous melanoma. Immunotherapies have becomethe main treatment modality for metastatic cutaneous mela-noma based upon substantial evidence that tumor antigensexpressed by cutaneous melanoma can be vigorously recog-nized by T-cell populations endogenous to the host immunesystem (8). By clinically augmenting these immune responseswith either systemic cytokines (9), antibodies targeting T-cellcheckpoint molecules (10, 11), or adoptive transfer of autol-ogous tumor-infiltrating lymphocytes (TIL; ref. 12), significantand potentially curative cancer regression can now be achievedin advanced cutaneous melanoma patients. However, the roleof these immune-based therapies for the treatment of meta-static uveal melanoma remains unclear. Patients with uvealmelanoma are frequently excluded from metastatic melanomaimmunotherapy clinical trials because uveal melanoma is
1Surgery Branch, Center for Cancer Research, National Cancer Insti-tute, National Institutes of Health, Bethesda, Maryland. 2Laboratory ofPathology, National Cancer Institute, National Institutes of Health,Bethesda, Maryland. 3Advanced Biomedical Computing Center, Fre-derick National Laboratory for Cancer Research (FNLCR), LeidosBiomedical Research Inc., Frederick, Maryland.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
L.D. Rothermel, A.C. Sabesan, D.J. Stephens, and U.S. Kammula share firstauthorship.
Corresponding Author: Udai S. Kammula, National Cancer Institute, 10 CenterDrive, Bethesda, MD 20892-1201. Phone: 301-435-8606; Fax: 301-435-5167;E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-15-2294
�2015 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 2237
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294

generally thought to be an immunotherapy-resistant subtype ofmelanoma. It has been speculated that because the primarytumor arises in the eye, an immune-privileged site, the tumorand its metastases harbor local immunosuppressive or cellularimmuno-evasive factors that render immunotherapies unsuc-cessful (13–16). Another theory proposes that because uvealmelanoma tumors have far fewer somatic mutations comparedwith sun-exposed cutaneous melanoma tumors (17), there areconsequentially fewer potential mutated neoepitope targets foreffective antitumor immunity. The poor immunogenicity ofuveal melanoma has been further suggested based upon thecomparatively low response rates seen in uveal melanomapatients enrolled into small pilot trials of immune-modulatingagents, such as IL2 (18) and anti–CTLA-4 antibody (19–21).Collectively, these observations have fostered the prevalentbelief that uveal melanoma, in distinction to cutaneous mel-anoma, is a nonimmunogenic form of melanoma. However,this hypothesis has largely been based upon inference withoutformal comparative studies performed directly upon uvealmelanoma and cutaneous melanoma metastases to accuratelyassess their relative immunogenicity. In this study, we aimed toaddress this deficiency by comparing tumor antigen expression,tumor mutational load, and endogenous antitumor immuno-logic reactivity found in fresh surgically resected uveal mela-noma versus cutaneous melanoma metastases. By determiningwhether tumor-specific immune responses naturally existagainst uveal melanoma metastases, we sought to provideinsight into the management of this rare melanoma variantwith immunotherapies that can exploit these endogenous T-cellpopulations.
Materials and MethodsStudy population
A retrospective review of a prospectively maintained data-base identified 49 patients who underwent liver metastasect-omy with a diagnosis of metastatic melanoma at the SurgeryBranch of the NCI between 2004 and 2014. All patients signedan Institutional Review Board–approved consent for tumortissue procurement and participation in subsequent immuno-therapy protocols if the patient required further systemic
therapy. Inclusion criteria included pathologically confirmedmelanoma, 16 years of age or older, negative serology for HIV,Hepatitis B and C, good performance status (Eastern Cooper-ative Oncology Group �2), and life expectancy greater than3 months. Patients were stratified into two cohorts based uponthe anatomic origin of their primary melanoma. The cutaneousmelanoma cohort included 35 patients; 33 of these patientshad documented primary tumors arising from the cutaneousepithelium and 2 additional patients had primary tumors ofunknown origin. The uveal melanoma cohort included 14 pati-ents who had ophthalmologic documentation that their pri-mary melanoma tumors arose specifically from the uveal tract.Patients with documented primary tumors arising from muco-sal and conjunctival sites were excluded from analysis.
Tumor procurementPatients typically underwent resection of a single metastatic
liver deposit or a closely approximated cluster of tumors usingstandardized hepatobiliary surgical techniques. Immediatelyupon resection, the fresh tumor underwent pathologic assess-ment, dissection, and processing in the Surgery Branch CellProduction facility in conjunction with a clinical surgical patho-logist and research staff. Tumor tissue was assigned a unique livermetastasis identification number (ID #) and allocated for grossandhistopathologic analysis,mutational analysis, and TIL cultureestablishment using methods as described below. Although themain study exclusively focused upon liver metastases, a set ofextrahepatic metastases from 8 additional uveal melanomapatients were incorporated into the tumor driver mutationalanalysis, as described below.
In-situ MRI assessment of tumor melanin contentAll patients underwent preoperative MRI liver imaging as part
of their radiographic tumor staging. Quantitative T1-weightedsignal intensity measurements (without gadolinium enhance-ment) of the in-situ liver metastases and adjacent normal tissuewere obtained using clinical radiology imaging software (Care-stream Vue Solutions; version 11.3). Mean tumor and normalintensity were calculated by averaging three separate signalintensity measurements. Hyperintense tumors were defined ashaving a mean tumor/normal (T/N) intensity ratio > 1.5.Hypointense tumors had amean T/N ratio < 0.7. Mixed intensitytumors had both hyperintense and hypointense components.The T/N signal intensity ratio for each liver metastasis wasobjectively calculated for each metastasis and scored as eitherhyperintense (2þ), mixed intensity (1þ), or hypointense (0), asillustrated in Supplementary Fig. S1.
Gross pathologic assessment of tumor melanin pigmentationAfter surgical resection, all liver metastases underwent inde-
pendent gross pathologic assessment and photo documentationby a board-certified pathologist who was blinded to the compar-ative analysis. Each metastasis underwent serial sectioning toassess their melanin pigmentation. Tumors were scored basedon their level of pigmentation as either hyperpigmented (2þ),mixed pigmented (1þ), or hypopigmented (0).
Immunohistochemical staining analysis of tumor metastasesSurgically resected tumor specimens were fixed in 10%neutral-
buffered formalin for up to 24 hours and routinely processed.Paraffin-embedded tissue sections of 5 mm were deparaffinized
Translational Relevance
Although remarkable strides have been achieved inthe management of metastatic cutaneous melanoma withT-cell–based immunotherapies, limited progress has beenmade with metastatic uveal melanoma, a rare and aggressivevariant that is hypothesized to be immunotherapy-resistant. Inthis study, we sought to formally define the relative immu-nogenicity of these two melanoma variants and determinewhether endogenous antitumor immune responses existagainst uveal melanoma. Here, we report the novel identifi-cation of TIL froma subset of uvealmelanomametastaseswithrobust antitumor reactivity, comparable in magnitude withthat of cutaneous melanoma TIL. The discovery of this immu-nogenic group of uveal melanoma metastases has importantclinical implications for the role of immunotherapies in thetreatment of patients who harbor these unique tumors.
Rothermel et al.
Clin Cancer Res; 22(9) May 1, 2016 Clinical Cancer Research2238
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294

through xylene and graded series of alcohols. Immunohistochem-ical staining was performed following heat-induced epitoperetrieval with target retrieval solution (low pH; DAKO). Slideswere incubated in Tris with 3% goat serum for 15 minutes andthen incubated at room temperature with primary antibody for1 to 2 hours. Immunohistochemical staining was carried outusing the Dako Autostainer or Ventana BenchMark XT SlideStainer (for CD3 antibody) using the manufacturer-suppliedreagents and standard protocols with the following primaryantibodies: MART-1 (no. CMC756, 1:200; Cell Marque); HMB45(no. 30930, 1:4; Enzo Life Sciences); Tyrosinase (no.NCL-TYROS,1:20; Novocastra Division, Leica Microsystems); MHC Class I(HC-10, 1:1,000; provided by Dr. Soldano Ferrone); HLA-DR(TAL.1B5, 1:200;DAKO);CD20 (L26, 1:500;DAKO);CD8 (CD8/144B, 1:50; DAKO); CD4 (1F6, 1:80; Novacastra); CD3 (2GV6,prediluted; Ventana). Detection was carried out using an auto-mated slide stainer (Autostainer; DAKO) with either horseradishperoxidase/3,30-diaminobenzidine polymer–based detection sys-tem (Envisionþ; DAKO) or a red chromogen (Liquid PermanentRed Substrate-Chromogen; DAKO) for darkly pigmented tumors.The immunohistochemical staining was prospectively assessedand quantitated by two board-certified pathologists who wereblinded to the comparative analysis of the study. The percentageof viable tumor cells expressing a given marker was quantified as0% to5%,6%to50%,or>50%. Staining intensity for eachmarkerwas graded on a scale of 0 (no staining), 1þ, 2þ, or 3þ (highintensity staining). Lymphocytic infiltrate was assessed with CD4,CD8, CD3, and CD20 staining and quantified based upon thepercentage of tumor occupied by infiltrating lymphocytes as 0 (nolymphocytes detected), 1þ (<5%of tumorfield), 2þ (5%–50%oftumor field), or 3þ (extensive lymphoid aggregation occupyingover 50% of the tumor field).
Generation and assessment of TIL culturesGeographically discrete 1 to 2 mm3 tumor fragments (n ¼
24) were freshly dissected from each tumor metastasis andplaced individually in wells of a 24-well culture plate contain-ing complete media with human AB serum and recombinantIL2 (3,000 IU/mL) as previously described (22). After approx-imately 2 weeks of culturing, each of the wells was assessed forsuccessful TIL expansion based upon cell count and visualinspection. Expanded TIL cultures underwent flow cytometricphenotypic analysis after staining with anti-human CD3, CD8,and CD4 monoclonal antibodies and their respective isotypecontrols (BD Biosciences). Immunofluorescence, analyzed asthe relative log fluorescence of live cells, was measured using aFACSCanto II flow cytometer with FACSDiva software (BDBiosciences) and FlowJo software (Tree Star, Inc.). The specificantitumor reactivity of individual TIL cultures was assessed bycoculture with autologous tumor digest which had been freshlycryopreserved at the time of surgical procurement. Briefly, TILcells (1� 105 cells) and autologous tumor digest (1� 105 cells)were coincubated in a 0.2-mL volume in individual wells ofa 96-well plate. Supernatants were harvested from duplicatewells after 20 to 24 hours, and IFNg secretion was measured inculture supernatants using commercially available IFNg ELISAkits (Endogen). All data are presented as a mean of duplicatesamples. Cultures with IFNg production greater than 100 pg/mL and twice background of unstimulated TIL and autologoustumor digest alone were considered as having specific antitu-mor reactivity.
Whole-exomic sequencing and driver mutational analysisExome libraries were prepared from paired uveal melanoma
metastasis and normal samples using the Agilent SureSelectXTHuman All Exon V5þUTR target enrichment Kit as per themanufacturer's protocols (Agilent). The samples were pooledthree samples per lane and sequenced on an IlluminaHiSeq2000 sequencer with TruSeq V3 chemistry (paired-end,101 bp read length). Basecalling was carried out using IlluminaRTA 1.12.4.2 run-time analysis software, and demultiplexingwas carried out using Casava 1.8.2. Each sample had >99million pass filtered reads, with >92% bases having a basequality value >Q30 (Q30: The percentage of bases called withan inferred accuracy of 99.9% or above, a measure of base-calling quality). The percentage of unique library fragments was>90% across all samples. The capture efficiency as measured bythe percentage of the reads mapping on the target regions was>60%. The mean coverage on target regions for all samples wasbetween 60� to 90� with >82.9% of the target regions havingat least 30� coverage. The quality of the raw reads was assessedusing FastQC (23) and NGS QC toolkit (24). Reads weretrimmed and filtered for adapters using Trimmomatic (25).Alignment was carried out to the human Hg19 referencesequence using BWA-0.7.4 (26). Alignment files were indexed,sorted, and duplicates were removed. Realignment aroundInDels and base-quality score recalibration was carried outas per the GATK best practices for exome-seq analysis (27).MuTect was used in the high-confidence (HC) mode forcalling somatic point mutations (28). The subset of calls thatpassed the HC filters after the statistical analysis within MuTectwas annotated using Annovar (29) to find both the locationand the functional significance of the mutations. Mutationswere filtered to keep only those that had Mutation_info: exonicor splicing only; Consequence: non-synonymous or stop-gain_SNV. To serve as a reference group, whole-exomic sequenc-ing (WES) data were obtained for 278 cutaneous melanomametastases via the "Skin Cutaneous Melanoma" (SKCM) dataportal of The Cancer Genome Atlas (TCGA). Somatic mutationcounts for the metastatic patient samples for the SKCM cohortwere extracted from the Level 2 MAF file downloaded off theGDAC Firehose resource (30). As only somatic point mutationswere of interest while comparing the distribution of somaticmutations between cutaneous melanoma and uveal melanomacohorts, InDel calls (1.2%) were removed from the TCGA-SKCMcohort. As the annotations for the point mutations in the TCGA-SKCM cohort did not have the same terminology as for theuveal melanoma cohort, the SKCMmutations were reannotatedusing Annovar, with the same filters applied based on thecombination of "Consequence" and "Mutation_info" columns.The frequency among the cutaneous melanoma and uvealmelanoma tumors for specific mutations in BRAF, GNAQ, andGNA11 was determined primarily from WES analysis. As vali-dation in selected samples, library preparation with 10 to 20 nggenomic DNA was performed using Ion AmpliSeq CancerHotspot, Panel V2 and Ion AmpliSeq Library Kit 2.0, using thecorresponding User Guide (Life Technologies). The ampliconpanel includes 207 primer sets covering approximately 2,800COSMIC hotspot mutations in 50 genes. Next-generationsequencing was performed in an Ion Torrent Personal genomemachine, and analyzed with Torrent Suite Software (Life Tech-nologies). Annotation and interpretation of all variants wereperformed in Ion Reporter that links to multiple databases,
Identification of an Immunogenic Subset of Uveal Melanoma
www.aacrjournals.org Clin Cancer Res; 22(9) May 1, 2016 2239
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294

such as RefSeq, OMIM, Oncomine, COSMIC, and dbSNP. Re-ported mutations were confirmed by inspection of alignmentsusing the Integrative Genomics Viewer (31).
Statistical analysisThe Fisher exact test was used to determine associations
between dichotomous demographic parameters, and the Wil-coxon rank-sum test was utilized for the comparison of con-tinuous parameters such as patient age. Nonparametric com-parisons between the uveal melanoma and cutaneous melano-ma cohorts were performed with the Mann–Whitney test. TheStudent t test was used to compare the means of parametricvariables. Linear regression analysis was used for correlationstudies and presented as R2 values. All P values are two-tailedand have not been adjusted for multiple comparisons. In view ofthe exploratory analyses performed, P < 0.05 would be consid-ered statistically significant, whereas 0.05 < P < 0.1 would beconsidered a trend. Excel and GraphPad Prism (v6.01) wereused for analyses.
ResultsPatient demographics and procurement of liver metastases
Between 2004 and 2014, a total of 49 patients with metastaticmelanoma underwent liver metastasectomy in the context ofapproved clinical trials in the Surgery Branch, NCI. The currentstudy selectively analyzed liver metastases because of our pre-vious finding that human melanoma metastases demonstratesignificant heterogeneity in tumor antigen expression and lym-phocytic infiltrate when stratified based upon their anatomiclocation in the body (6). Further, because uveal melanomapredominantly metastasizes to the liver, this homogeneoussource of metastases would prevent potential site-specific biasin our comparative assessment of tumors. Patients undergoingliver metastasectomy were stratified into two cohorts, cutaneousmelanoma and uveal melanoma, based upon the anatomicorigin of their primary melanomas. The cutaneous melanomacohort included 35 patients; 33 of whom had documentedprimary tumors arising from the cutaneous epithelium and 2additional patients had primary tumors of unknown origin.Patients with melanoma of unknown origin were included inthe cutaneous melanoma cohort based upon recent moleculargenetic studies which revealed these tumors strongly resembledcutaneous melanomas (32). The uveal melanoma cohort includ-ed 14 patients who had ophthalmologic documentation thattheir primary melanoma arose specifically from the uveal tract.The characteristics for each of the patients who underwent livermetastasectomy are shown in Table 1, and the comparison ofthe cutaneous melanoma and uveal melanoma cohorts is shownin Table 2. The age (mean and range) and gender distributionof the patients in the two cohorts were similar. At the time ofreferral to our center, there was a greater trend for the uvealmelanoma patients to have not received prior systemic therapyfor their metastatic disease when compared with the cutaneousmelanoma patients (uveal melanoma: 71% vs. cutaneous mela-noma: 37%, P ¼ 0.06). This finding likely reflected the growingavailability of approved systemic agents and clinical trial oppor-tunities for patients with metastatic cutaneous melanoma dur-ing the study period. Of note, 63% of the cutaneous melanomapatients had undergone prior systemic immunotherapy, where-as only 21% of uveal melanoma patients had received such
treatments (cutaneous melanoma vs. uveal melanoma, P ¼0.01). Although both melanoma cohorts demonstrated meta-static spread to extrahepatic sites, the uveal melanoma patientshad metastases more often confined to the liver (uveal mela-noma: 43% vs. cutaneous melanoma: 14%, P ¼ 0.05), whereasthe cutaneous melanoma patients demonstrated a trend towardmore frequent metastases to lymph nodes and soft tissues(cutaneous melanoma: 60% vs. uveal melanoma: 29%, P ¼0.06). For surgical tumor procurement, patients typically under-went resection of a single metastatic liver deposit or a closelyapproximated cluster of tumors. The size (mean/median) ofthe tumor deposits resected from the patients was not signi-ficantly different between the groups (cutaneous melanoma:6.2/6.0 cm vs. uveal melanoma: 7.2/5.5 cm, P ¼ 0.50). Thecumulative metastatic tissue that was procured at operation wasassigned a unique liver metastasis identification number (ID #)for subsequent analysis. Two uveal melanoma patients (1 and 3)developed metachronous liver metastases during the studyperiod. These patients underwent two independent liver metas-tasectomy operations, and their individual tumor procurementswere assigned unique liver metastasis ID #. Thus, in sum, therewere 35 cutaneous melanoma liver metastases and 16 uvealmelanoma liver metastases that were available for direct com-parative analysis.
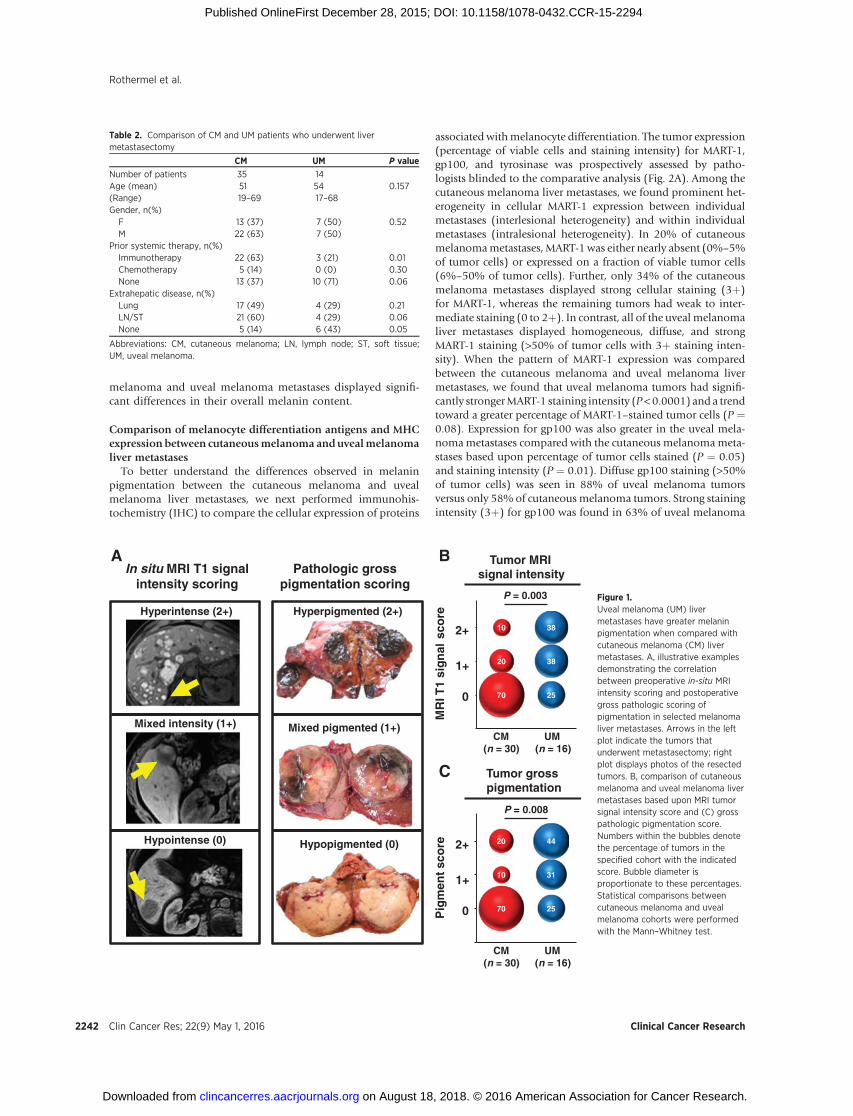
Radiographic and pathologic comparison of the melanincontent between cutaneous melanoma and uveal melanomaliver metastases
Both cutaneous melanoma and uveal melanoma primarytumors arise from transformed melanocytes. Yet, despite thiscommon origin frommelanin-producing cells, the metastases ofthese tumors can display significant heterogeneity in the quanti-tative expression of prototypic melanin-associated proteins(6). These prior findings prompted us to ask whether cutane-ous melanoma and uveal melanoma metastases demonstratedfundamental differences in their melanin pigmentation. Toaddress this question, we utilized preoperative clinical radio-graphic imaging and postoperative gross pathologic examina-tion to evaluate the melanin content found in the liver metas-tases procured from cutaneous melanoma and uveal melanomapatients. A prior study characterizing melanomametastases withclinical MRI imaging found the in-situ tumor signal intensityfrom T1-weighted sequences strongly correlated with the degreeof melanin pigmentation found in those tumors after resection(33). For the current study, we utilized these defined MRIparameters to perform in-situ characterization of 30 liver metas-tases identified in cutaneous melanoma patients and 16 livermetastases in uveal melanoma patients. Quantitative T1-weight-ed signal intensity measurements (without gadolinium en-hancement) of the in-situ tumor and adjacent normal tissuewere obtained using clinical radiology imaging software (Care-stream Vue Solutions; version 11.3). The normalized tumorsignal intensity (relative to normal liver) was objectively calcu-lated for each metastasis and scored as either hyperintense (2þ),mixed intensity (1þ), or hypointense (0), as illustrated inSupplementary Fig. S1. In addition, after surgical resection,metastases underwent independent gross pathologic examina-tion, and tumor pigmentation was visually scored as eitherhyperpigmented (2þ), mixed pigmented (1þ), or hypopigmen-ted (0). The comparison of preoperative in-situ MRI intensityscoring and postoperative pathologic pigmentation scoring for
Rothermel et al.
Clin Cancer Res; 22(9) May 1, 2016 Clinical Cancer Research2240
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294

representative liver metastases is shown in Fig. 1A. Analysis ofthe entire population of liver metastases (n ¼ 46) revealed astrong and direct correlation between the MRI and the patho-logic scoring of pigmentation (R2 ¼ 0.88, P < 0.0001) for theindividual tumors. Next, we used these two parameters toindependently compare the melanin content found in thecutaneous melanoma and uveal melanoma liver metastases.In-situ MRI tumor signal intensity was significantly differentbetween the two melanoma cohorts (P ¼ 0.003; Fig. 1B).Whereas, 70% of cutaneous melanoma metastases had hypoin-tense (0) MRI signal, only 25% of uveal melanoma metastasesdisplayed this low signal intensity. Conversely, the uveal
melanoma cohort demonstrated a greater frequency of metas-tases with hyperintense (2þ) MRI signal (uveal melanoma: 38%vs. cutaneous melanoma: 10%). When these same uveal mel-anoma and cutaneous melanoma metastases underwent path-ologic examination after resection, we similarly found a signif-icant difference in their gross pigmentation (P ¼ 0.008; Fig. 1C).Cutaneous melanoma metastases were more often visuallyhypopigmented (0; cutaneous melanoma: 70% vs. uveal mel-anoma: 25%), and uveal melanoma metastases were more oftenhyperpigmentated (2þ; uveal melanoma: 44% vs. cutaneousmelanoma: 20%). Thus, we concluded that despite havingcommon lineage from melanin-producing cells, cutaneous
Table 1. Patient demographics and procurement of liver metastases
Patient ID # Age Gender Primary site Sites of metastasis Prior systemic therapies Liver metastasis ID #
Cutaneous melanoma1 35 M Neck Li Immuno L-CM12 51 F Arm Li, Lu None L-CM23 46 F Scalp Li, Lu Immuno, chemo L-CM34 62 F Shoulder Li, Lu, ST None L-CM45 44 F Hip Li, Lu, kidney, LN Immuno, chemo L-CM56 66 M Back Li, LN Immune L-CM67 61 M Back Li, LN Immuno L-CM78 44 M Sacral Li, Lu, LN Immune L-CM89 64 M Back Li, ST None L-CM910 37 F Back Li, Lu, Bn, LN Immuno L-CM1011 54 M Shoulder Li Immuno L-CM1112 42 M Back Li, LN Immuno L-CM1213 47 F Infra-auricular Li, Lu None L-CM1314 35 M Unknown Li, Lu, LN Immuno, chemo L-CM1415 64 F Parotid Li Immuno L-CM1516 62 M Ear Li, Lu Immuno L-CM1617 50 F Neck Li, Spl, Panc Immuno, chemo L-CM1718 62 M Foot Li, Lu, Spl, LN None L-CM1819 45 M Shoulder Li, LN None L-CM1920 57 M Back Li Immuno L-CM2021 54 F Back Li, ST None L-CM2122 50 M Back Li, Lu Immuno L-CM2223 57 M Back Li, Lu, ST None L-CM2324 69 F Scalp Lu Immuno L-CM2425 48 M Unknown Li, LN, ST, Bn None L-CM2526 55 M Leg Li, Lu, LN None L-CM2627 65 M Scalp Li, Lu, LN Immuno L-CM2728 53 M Shoulder Li, Bn None L-CM2829 34 M Jaw Li, Lu, LN, Bn Immuno L-CM2930 46 F Flank Li Immuno, chemo, targeted L-CM3031 52 M Thigh Li, LN, Adrenal Immuno L-CM3132 62 M Back Li, LN None L-CM3233 56 M Leg Li, LN Immuno L-CM3334 19 F Preauricular Li, LN, Spl, Bn Immuno L-CM3435 27 F Ear Li, Lu None L-CM35Uveal melanoma1 56 F Uveal tract Li, Bn Immuno, TACE L-UM1a, L-UM1b2 56 F Uveal tract Li TACE L-UM23 47 F Uveal tract Li, Lu, Panc, Bn None L-UM3a, L-UM3b4 68 M Uveal tract Li None L-UM45 60 M Uveal tract Li, Lu, ST, LN, Per Immuno L-UM56 55 F Uveal tract Li None L-UM67 64 M Uveal tract Li None L-UM78 56 M Uveal tract Li None L-UM89 17 F Uveal tract Li, Lu, heart, LN Immuno L-UM910 54 F Uveal tract Li, LN None L-UM1011 58 M Uveal tract Li, ST None L-UM1112 53 F Uveal tract Li, Bn, Per, Om None L-UM1213 52 M Uveal tract Li None L-UM1314 62 M Uveal tract Li, Lu None L-UM14
Abbreviations: Bn, Bone; Li, Liver; LN, lymph node; Lu, lung; Om, omentum; Panc, pancreas; Per, peritoneum; Spl, spleen; ST, soft tissue.
Identification of an Immunogenic Subset of Uveal Melanoma
www.aacrjournals.org Clin Cancer Res; 22(9) May 1, 2016 2241
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294
melanoma and uveal melanoma metastases displayed signifi-cant differences in their overall melanin content.
Comparison of melanocyte differentiation antigens and MHCexpression between cutaneousmelanoma anduvealmelanomaliver metastases
To better understand the differences observed in melaninpigmentation between the cutaneous melanoma and uvealmelanoma liver metastases, we next performed immunohis-tochemistry (IHC) to compare the cellular expression of proteins
associated withmelanocyte differentiation. The tumor expression(percentage of viable cells and staining intensity) for MART-1,gp100, and tyrosinase was prospectively assessed by patho-logists blinded to the comparative analysis (Fig. 2A). Among thecutaneous melanoma liver metastases, we found prominent het-erogeneity in cellular MART-1 expression between individualmetastases (interlesional heterogeneity) and within individualmetastases (intralesional heterogeneity). In 20% of cutaneousmelanomametastases, MART-1was either nearly absent (0%–5%of tumor cells) or expressed on a fraction of viable tumor cells(6%–50% of tumor cells). Further, only 34% of the cutaneousmelanoma metastases displayed strong cellular staining (3þ)for MART-1, whereas the remaining tumors had weak to inter-mediate staining (0 to 2þ). In contrast, all of the uveal melanomaliver metastases displayed homogeneous, diffuse, and strongMART-1 staining (>50% of tumor cells with 3þ staining inten-sity). When the pattern of MART-1 expression was comparedbetween the cutaneous melanoma and uveal melanoma livermetastases, we found that uveal melanoma tumors had signifi-cantly strongerMART-1 staining intensity (P<0.0001) and a trendtoward a greater percentage of MART-1–stained tumor cells (P ¼0.08). Expression for gp100 was also greater in the uveal mela-nomametastases compared with the cutaneous melanomameta-stases based upon percentage of tumor cells stained (P ¼ 0.05)and staining intensity (P ¼ 0.01). Diffuse gp100 staining (>50%of tumor cells) was seen in 88% of uveal melanoma tumorsversus only 58% of cutaneous melanoma tumors. Strong stainingintensity (3þ) for gp100 was found in 63% of uveal melanoma
Table 2. Comparison of CM and UM patients who underwent livermetastasectomy
CM UM P value
Number of patients 35 14Age (mean) 51 54 0.157(Range) 19–69 17–68Gender, n(%)F 13 (37) 7 (50) 0.52M 22 (63) 7 (50)
Prior systemic therapy, n(%)Immunotherapy 22 (63) 3 (21) 0.01Chemotherapy 5 (14) 0 (0) 0.30None 13 (37) 10 (71) 0.06
Extrahepatic disease, n(%)Lung 17 (49) 4 (29) 0.21LN/ST 21 (60) 4 (29) 0.06None 5 (14) 6 (43) 0.05
Abbreviations: CM, cutaneous melanoma; LN, lymph node; ST, soft tissue;UM, uveal melanoma.
70
10
20
25
31
44
CM(n = 30)
UM(n = 16)
Pig
men
t sc
ore
0
1+
2+
Tumor grosspigmentation
P = 0.008
Hyperpigmented (2+)
Mixed pigmented (1+)
Hypopigmented (0)
Hyperintense (2+)
Mixed intensity (1+)
Hypointense (0)
Pathologic grosspigmentation scoring
In situ MRI T1 signal intensity scoring
70
20
10
25
38
38
CM(n = 30)
UM(n = 16)
MR
I T1
sig
nal
sco
re
0
1+
2+
Tumor MRI signal intensity
P = 0.003
A B
C
Figure 1.Uveal melanoma (UM) livermetastases have greater melaninpigmentation when compared withcutaneous melanoma (CM) livermetastases. A, illustrative examplesdemonstrating the correlationbetween preoperative in-situ MRIintensity scoring and postoperativegross pathologic scoring ofpigmentation in selected melanomaliver metastases. Arrows in the leftplot indicate the tumors thatunderwent metastasectomy; rightplot displays photos of the resectedtumors. B, comparison of cutaneousmelanoma and uveal melanoma livermetastases based upon MRI tumorsignal intensity score and (C) grosspathologic pigmentation score.Numbers within the bubbles denotethe percentage of tumors in thespecified cohort with the indicatedscore. Bubble diameter isproportionate to these percentages.Statistical comparisons betweencutaneous melanoma and uvealmelanoma cohorts were performedwith the Mann–Whitney test.
Rothermel et al.
Clin Cancer Res; 22(9) May 1, 2016 Clinical Cancer Research2242
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294
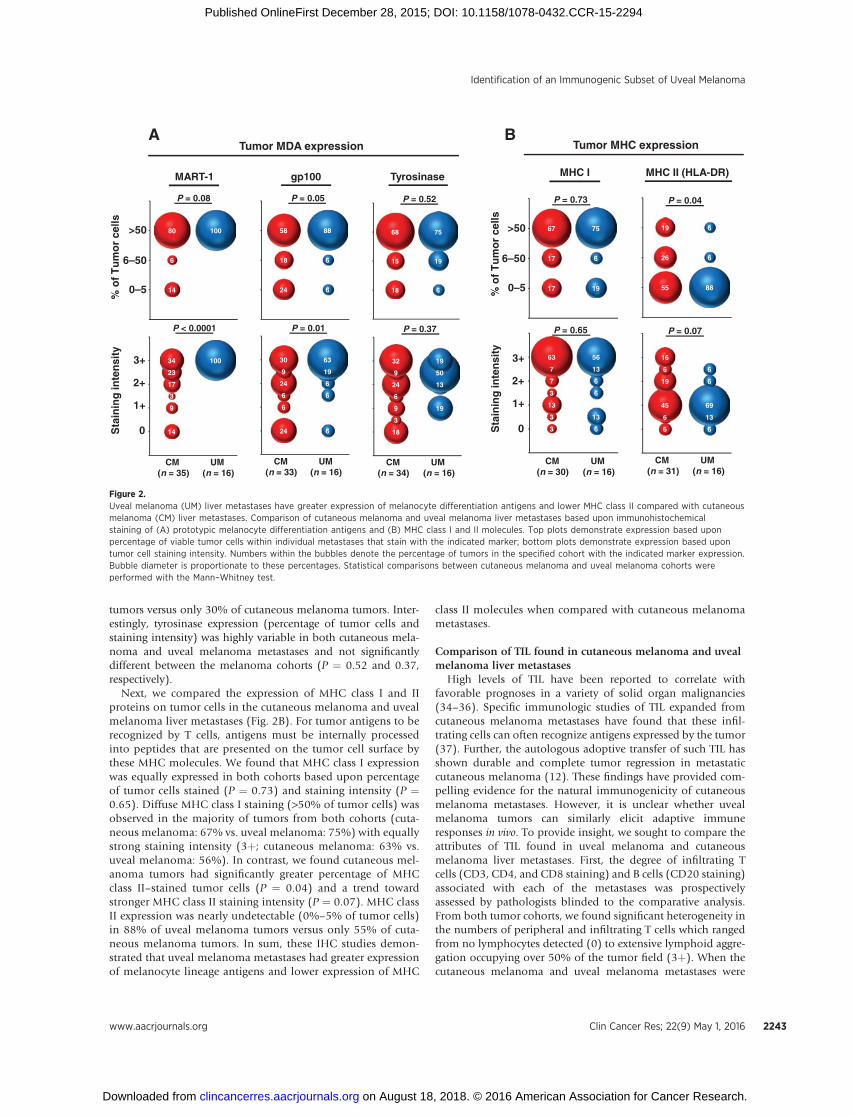
tumors versus only 30% of cutaneous melanoma tumors. Inter-estingly, tyrosinase expression (percentage of tumor cells andstaining intensity) was highly variable in both cutaneous mela-noma and uveal melanoma metastases and not significantlydifferent between the melanoma cohorts (P ¼ 0.52 and 0.37,respectively).
Next, we compared the expression of MHC class I and IIproteins on tumor cells in the cutaneous melanoma and uvealmelanoma liver metastases (Fig. 2B). For tumor antigens to berecognized by T cells, antigens must be internally processedinto peptides that are presented on the tumor cell surface bythese MHC molecules. We found that MHC class I expressionwas equally expressed in both cohorts based upon percentageof tumor cells stained (P ¼ 0.73) and staining intensity (P ¼0.65). Diffuse MHC class I staining (>50% of tumor cells) wasobserved in the majority of tumors from both cohorts (cuta-neous melanoma: 67% vs. uveal melanoma: 75%) with equallystrong staining intensity (3þ; cutaneous melanoma: 63% vs.uveal melanoma: 56%). In contrast, we found cutaneous mel-anoma tumors had significantly greater percentage of MHCclass II–stained tumor cells (P ¼ 0.04) and a trend towardstronger MHC class II staining intensity (P ¼ 0.07). MHC classII expression was nearly undetectable (0%–5% of tumor cells)in 88% of uveal melanoma tumors versus only 55% of cuta-neous melanoma tumors. In sum, these IHC studies demon-strated that uveal melanoma metastases had greater expressionof melanocyte lineage antigens and lower expression of MHC
class II molecules when compared with cutaneous melanomametastases.
Comparison of TIL found in cutaneous melanoma and uvealmelanoma liver metastases
High levels of TIL have been reported to correlate withfavorable prognoses in a variety of solid organ malignancies(34–36). Specific immunologic studies of TIL expanded fromcutaneous melanoma metastases have found that these infil-trating cells can often recognize antigens expressed by the tumor(37). Further, the autologous adoptive transfer of such TIL hasshown durable and complete tumor regression in metastaticcutaneous melanoma (12). These findings have provided com-pelling evidence for the natural immunogenicity of cutaneousmelanoma metastases. However, it is unclear whether uvealmelanoma tumors can similarly elicit adaptive immuneresponses in vivo. To provide insight, we sought to compare theattributes of TIL found in uveal melanoma and cutaneousmelanoma liver metastases. First, the degree of infiltrating Tcells (CD3, CD4, and CD8 staining) and B cells (CD20 staining)associated with each of the metastases was prospectivelyassessed by pathologists blinded to the comparative analysis.From both tumor cohorts, we found significant heterogeneity inthe numbers of peripheral and infiltrating T cells which rangedfrom no lymphocytes detected (0) to extensive lymphoid aggre-gation occupying over 50% of the tumor field (3þ). When thecutaneous melanoma and uveal melanoma metastases were
ATumor MHC expression
6
6
45
19
6
16
6
13
69
6
6
55
26
19
88
6
6
3
3
13
3
7
7
63
6
13
6
6
13
56
17
17
67
19
6
75
Sta
inin
g in
ten
sity
0
1+
2+
3+
CM(n = 30)
UM(n = 16)
% o
f T
um
or
cells
Sta
inin
g in
ten
sity
0
1+
2+
3+
% o
f T
um
or
cells
0–5
6–50
>50
0–5
6–50
>50
CM(n = 31)
UM(n = 16)
MHC I MHC II (HLA-DR)
P = 0.65 P = 0.07
P = 0.73 P = 0.04
18
3
9
6
24
9
32
19
13
50
19
18
15
68
6
19
75
14
6
80 100
14
9
3
17
23
34 100
CM(n = 35)
UM(n = 16)
MART-1 gp100 Tyrosinase
24
18
58
6
6
88
24
6
6
24
9
30
6
6
6
19
63
CM(n = 33)
UM(n = 16)
CM(n = 34)
UM(n = 16)
P < 0.0001 P = 0.01 P = 0.37
P = 0.08 P = 0.05 P = 0.52
Tumor MDA expressionB
Figure 2.Uveal melanoma (UM) liver metastases have greater expression of melanocyte differentiation antigens and lower MHC class II compared with cutaneousmelanoma (CM) liver metastases. Comparison of cutaneous melanoma and uveal melanoma liver metastases based upon immunohistochemicalstaining of (A) prototypic melanocyte differentiation antigens and (B) MHC class I and II molecules. Top plots demonstrate expression based uponpercentage of viable tumor cells within individual metastases that stain with the indicated marker; bottom plots demonstrate expression based upontumor cell staining intensity. Numbers within the bubbles denote the percentage of tumors in the specified cohort with the indicated marker expression.Bubble diameter is proportionate to these percentages. Statistical comparisons between cutaneous melanoma and uveal melanoma cohorts wereperformed with the Mann–Whitney test.
Identification of an Immunogenic Subset of Uveal Melanoma
www.aacrjournals.org Clin Cancer Res; 22(9) May 1, 2016 2243
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294
compared, we found no significant differences in the levels ofperipheral and infiltrating CD3þ, CD4þ, or CD8þ T cellsbetween the cohorts (Supplementary Fig. S2). Further, B cells(CD20þ cells) were undetectable in the majority of tumors andalso not significantly different between the cohorts.
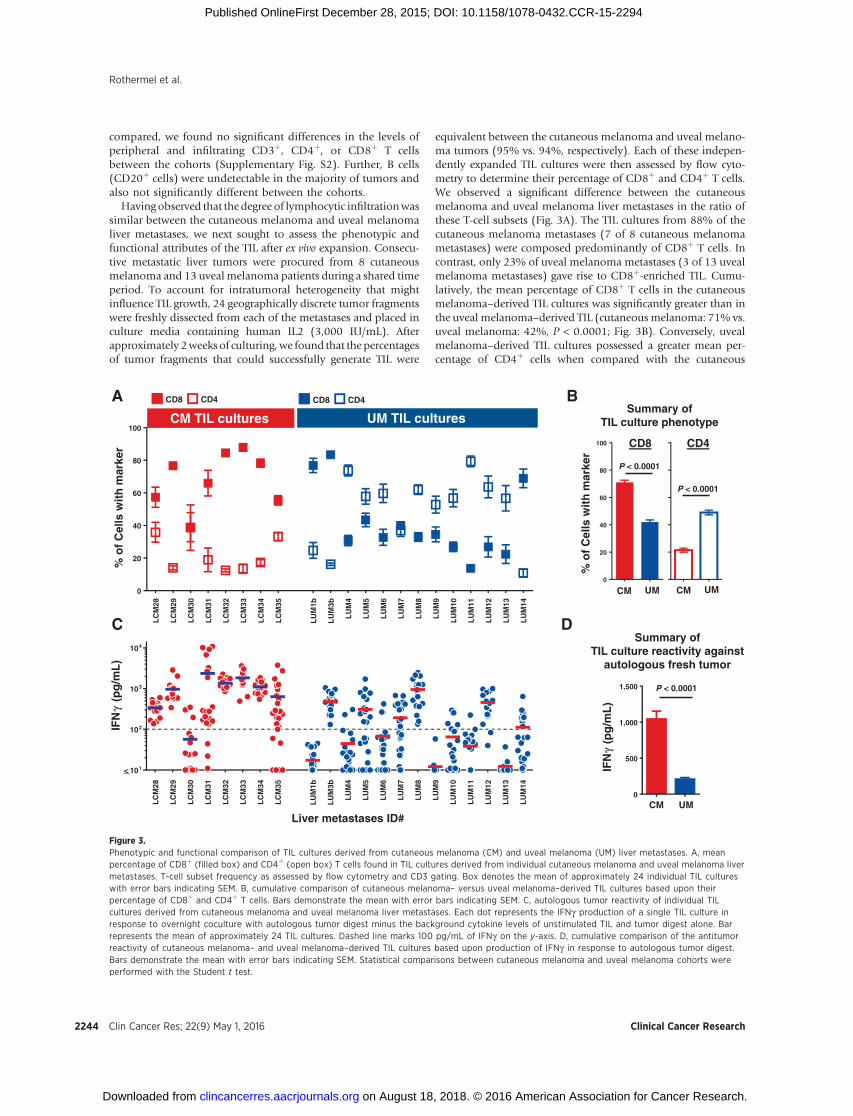
Having observed that the degree of lymphocytic infiltrationwassimilar between the cutaneous melanoma and uveal melanomaliver metastases, we next sought to assess the phenotypic andfunctional attributes of the TIL after ex vivo expansion. Consecu-tive metastatic liver tumors were procured from 8 cutaneousmelanoma and 13 uveal melanoma patients during a shared timeperiod. To account for intratumoral heterogeneity that mightinfluence TIL growth, 24 geographically discrete tumor fragmentswere freshly dissected from each of the metastases and placed inculture media containing human IL2 (3,000 IU/mL). Afterapproximately 2weeks of culturing, we found that the percentagesof tumor fragments that could successfully generate TIL were
equivalent between the cutaneous melanoma and uveal melano-ma tumors (95% vs. 94%, respectively). Each of these indepen-dently expanded TIL cultures were then assessed by flow cyto-metry to determine their percentage of CD8þ and CD4þ T cells.We observed a significant difference between the cutaneousmelanoma and uveal melanoma liver metastases in the ratio ofthese T-cell subsets (Fig. 3A). The TIL cultures from 88% of thecutaneous melanoma metastases (7 of 8 cutaneous melanomametastases) were composed predominantly of CD8þ T cells. Incontrast, only 23% of uveal melanoma metastases (3 of 13 uvealmelanoma metastases) gave rise to CD8þ-enriched TIL. Cumu-latively, the mean percentage of CD8þ T cells in the cutaneousmelanoma–derived TIL cultures was significantly greater than inthe uveal melanoma–derived TIL (cutaneous melanoma: 71% vs.uveal melanoma: 42%, P < 0.0001; Fig. 3B). Conversely, uvealmelanoma–derived TIL cultures possessed a greater mean per-centage of CD4þ cells when compared with the cutaneous
LC
M28
LC
M29
LC
M30
LC
M31
LC
M32
LC
M33
LC
M34
LC
M35
LU
M1b
LU
M3b
LU
M4
LU
M5
LU
M6
LU
M7
LU
M8
LU
M9
LU
M10
LU
M11
LU
M12
LU
M13
LU
M14
101
102
103
104
<
LC
M28
LC
M29
LC
M30
LC
M31
LC
M32
LC
M33
LC
M34
LC
M35
LU
M1b
LU
M3b
LU
M4
LU
M5
LU
M6
LU
M7
LU
M8
LU
M9
LU
M10
LU
M11
LU
M12
LU
M13
LU
M14
0
20
40
60
80
100CM TIL cultures UM TIL cultures
% o
f C
ells
wit
h m
arke
r
CD8 CD4 CD8 CD4
IFN
γ(p
g/m
L)
Liver metastases ID#
0
500
1,000
1,500 P < 0.0001
IFN
γ(p
g/m
L)
CM UM
0
20
40
60
80
100
Summary of TIL culture phenotype
CD8
P < 0.0001
CD4
P < 0.0001
CM UM CM UM
Summary of TIL culture reactivity against
autologous fresh tumor
% o
f C
ells
wit
h m
arke
r
A B
C D
Figure 3.Phenotypic and functional comparison of TIL cultures derived from cutaneous melanoma (CM) and uveal melanoma (UM) liver metastases. A, meanpercentage of CD8þ (filled box) and CD4þ (open box) T cells found in TIL cultures derived from individual cutaneous melanoma and uveal melanoma livermetastases. T-cell subset frequency as assessed by flow cytometry and CD3 gating. Box denotes the mean of approximately 24 individual TIL cultureswith error bars indicating SEM. B, cumulative comparison of cutaneous melanoma– versus uveal melanoma–derived TIL cultures based upon theirpercentage of CD8þ and CD4þ T cells. Bars demonstrate the mean with error bars indicating SEM. C, autologous tumor reactivity of individual TILcultures derived from cutaneous melanoma and uveal melanoma liver metastases. Each dot represents the IFNg production of a single TIL culture inresponse to overnight coculture with autologous tumor digest minus the background cytokine levels of unstimulated TIL and tumor digest alone. Barrepresents the mean of approximately 24 TIL cultures. Dashed line marks 100 pg/mL of IFNg on the y-axis. D, cumulative comparison of the antitumorreactivity of cutaneous melanoma– and uveal melanoma–derived TIL cultures based upon production of IFNg in response to autologous tumor digest.Bars demonstrate the mean with error bars indicating SEM. Statistical comparisons between cutaneous melanoma and uveal melanoma cohorts wereperformed with the Student t test.
Rothermel et al.
Clin Cancer Res; 22(9) May 1, 2016 Clinical Cancer Research2244
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294
melanoma–derived TIL cultures (uveal melanoma: 49% vs. cuta-neous melanoma: 21%, P < 0.0001; Fig. 3B).
Next, we compared the antitumor reactivity of the individualcutaneous melanoma and uveal melanoma TIL cultures by over-night coculture with tumor digests of their respective parentaltumors which had been freshly cryopreserved at the time ofsurgical procurement. Reactive TIL cultureswere defined as havingtumor-induced IFNg production �100 pg/mL and twice thebackground of unstimulated TIL and tumor digest alone. Theautologous antitumor reactivity for each of the TIL cultures fromtheir respective metastases is shown in Fig. 3C. The TIL culturesfrom 88% of the cutaneous melanoma metastases (7 of 8 cuta-neousmelanomametastases) demonstratedmean tumor-specificIFNg production �100 pg/mL. In contrast, 46% of uveal mela-nomametastases (6 of 13 uvealmelanomametastases) hadmeanreactivity above this threshold. Cumulatively, cutaneous mela-noma–derived TIL cultures produced higher mean levels of IFNgin response to autologous tumor digest when compared withuveal melanoma–derived TIL cultures (cutaneous melanoma:1,044 pg/mL vs. uveal melanoma: 209 pg/mL, P < 0.0001;Fig. 3D). Interestingly, however, we identified individual TILcultures from 46% of uveal melanoma metastases (6 of 13 uvealmelanoma metastases; L-UM 3b, 5, 7, 8, 12, and 14), with IFNgproduction which was comparable in magnitude with theresponses identified from cutaneous melanoma TIL (Fig. 3C).Thus, although specific autologous antitumor T-cell responseswere more prevalent among the cutaneous melanoma livermetastases, there was a subset of uveal melanoma tumors thatcould also elicit strong tumor reactive T-cell responses.
Metastasis hypopigmentation identifies an immunogenicsubset of uveal melanoma
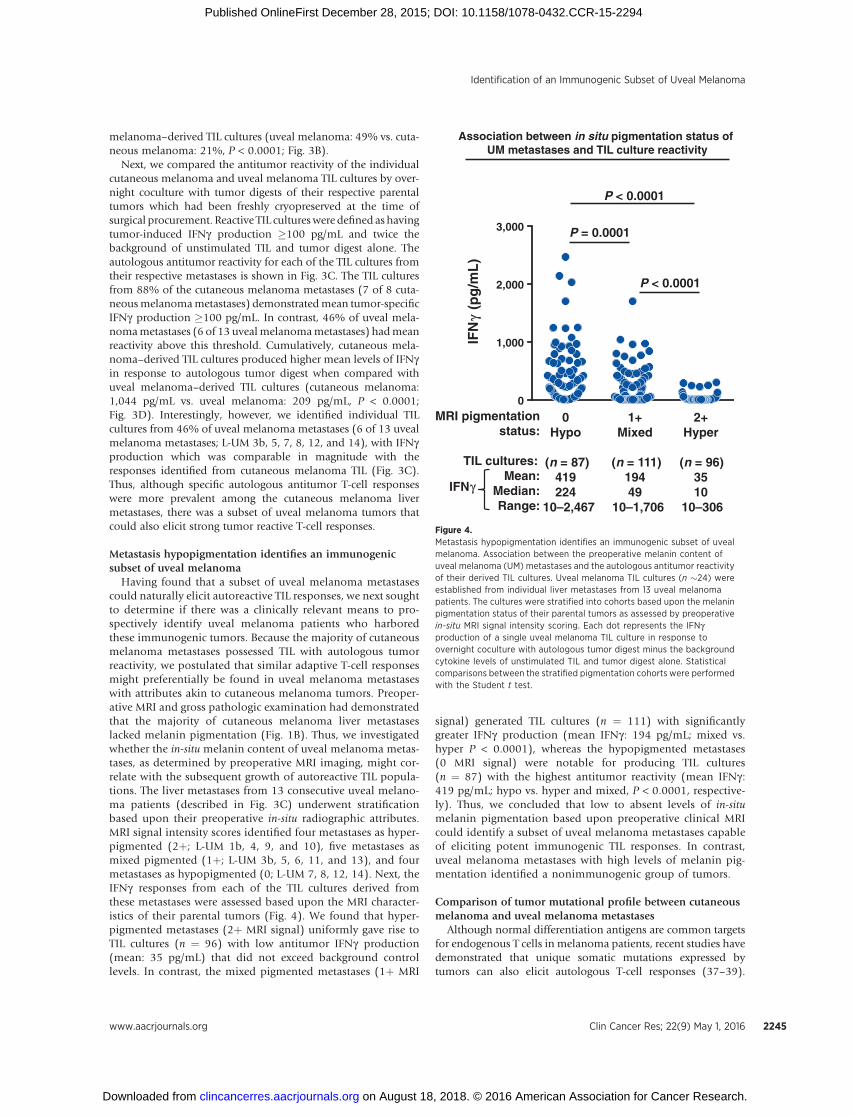
Having found that a subset of uveal melanoma metastasescould naturally elicit autoreactive TIL responses, we next soughtto determine if there was a clinically relevant means to pro-spectively identify uveal melanoma patients who harboredthese immunogenic tumors. Because the majority of cutaneousmelanoma metastases possessed TIL with autologous tumorreactivity, we postulated that similar adaptive T-cell responsesmight preferentially be found in uveal melanoma metastaseswith attributes akin to cutaneous melanoma tumors. Preoper-ative MRI and gross pathologic examination had demonstratedthat the majority of cutaneous melanoma liver metastaseslacked melanin pigmentation (Fig. 1B). Thus, we investigatedwhether the in-situ melanin content of uveal melanoma metas-tases, as determined by preoperative MRI imaging, might cor-relate with the subsequent growth of autoreactive TIL popula-tions. The liver metastases from 13 consecutive uveal melano-ma patients (described in Fig. 3C) underwent stratificationbased upon their preoperative in-situ radiographic attributes.MRI signal intensity scores identified four metastases as hyper-pigmented (2þ; L-UM 1b, 4, 9, and 10), five metastases asmixed pigmented (1þ; L-UM 3b, 5, 6, 11, and 13), and fourmetastases as hypopigmented (0; L-UM 7, 8, 12, 14). Next, theIFNg responses from each of the TIL cultures derived fromthese metastases were assessed based upon the MRI character-istics of their parental tumors (Fig. 4). We found that hyper-pigmented metastases (2þ MRI signal) uniformly gave rise toTIL cultures (n ¼ 96) with low antitumor IFNg production(mean: 35 pg/mL) that did not exceed background controllevels. In contrast, the mixed pigmented metastases (1þ MRI
signal) generated TIL cultures (n ¼ 111) with significantlygreater IFNg production (mean IFNg : 194 pg/mL; mixed vs.hyper P < 0.0001), whereas the hypopigmented metastases(0 MRI signal) were notable for producing TIL cultures(n ¼ 87) with the highest antitumor reactivity (mean IFNg :419 pg/mL; hypo vs. hyper and mixed, P < 0.0001, respective-ly). Thus, we concluded that low to absent levels of in-situmelanin pigmentation based upon preoperative clinical MRIcould identify a subset of uveal melanoma metastases capableof eliciting potent immunogenic TIL responses. In contrast,uveal melanoma metastases with high levels of melanin pig-mentation identified a nonimmunogenic group of tumors.
Comparison of tumor mutational profile between cutaneousmelanoma and uveal melanoma metastases
Although normal differentiation antigens are common targetsfor endogenous T cells in melanoma patients, recent studies havedemonstrated that unique somatic mutations expressed bytumors can also elicit autologous T-cell responses (37–39).
Association between in situ pigmentation status ofUM metastases and TIL culture reactivity
IFN
γ(p
g/m
L)
0Hypo
(n = 87)419224
10–2,467
1+Mixed
(n = 111)19449
10–1,706
MRI pigmentationstatus:
TIL cultures:Mean:
Median:Range:
2+Hyper
(n = 96)3510
10–306
0
1,000
2,000
3,000 P = 0.0001
P < 0.0001
P < 0.0001
IFNγ
Figure 4.Metastasis hypopigmentation identifies an immunogenic subset of uvealmelanoma. Association between the preoperative melanin content ofuveal melanoma (UM) metastases and the autologous antitumor reactivityof their derived TIL cultures. Uveal melanoma TIL cultures (n �24) wereestablished from individual liver metastases from 13 uveal melanomapatients. The cultures were stratified into cohorts based upon the melaninpigmentation status of their parental tumors as assessed by preoperativein-situ MRI signal intensity scoring. Each dot represents the IFNgproduction of a single uveal melanoma TIL culture in response toovernight coculture with autologous tumor digest minus the backgroundcytokine levels of unstimulated TIL and tumor digest alone. Statisticalcomparisons between the stratified pigmentation cohorts were performedwith the Student t test.
Identification of an Immunogenic Subset of Uveal Melanoma
www.aacrjournals.org Clin Cancer Res; 22(9) May 1, 2016 2245
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294

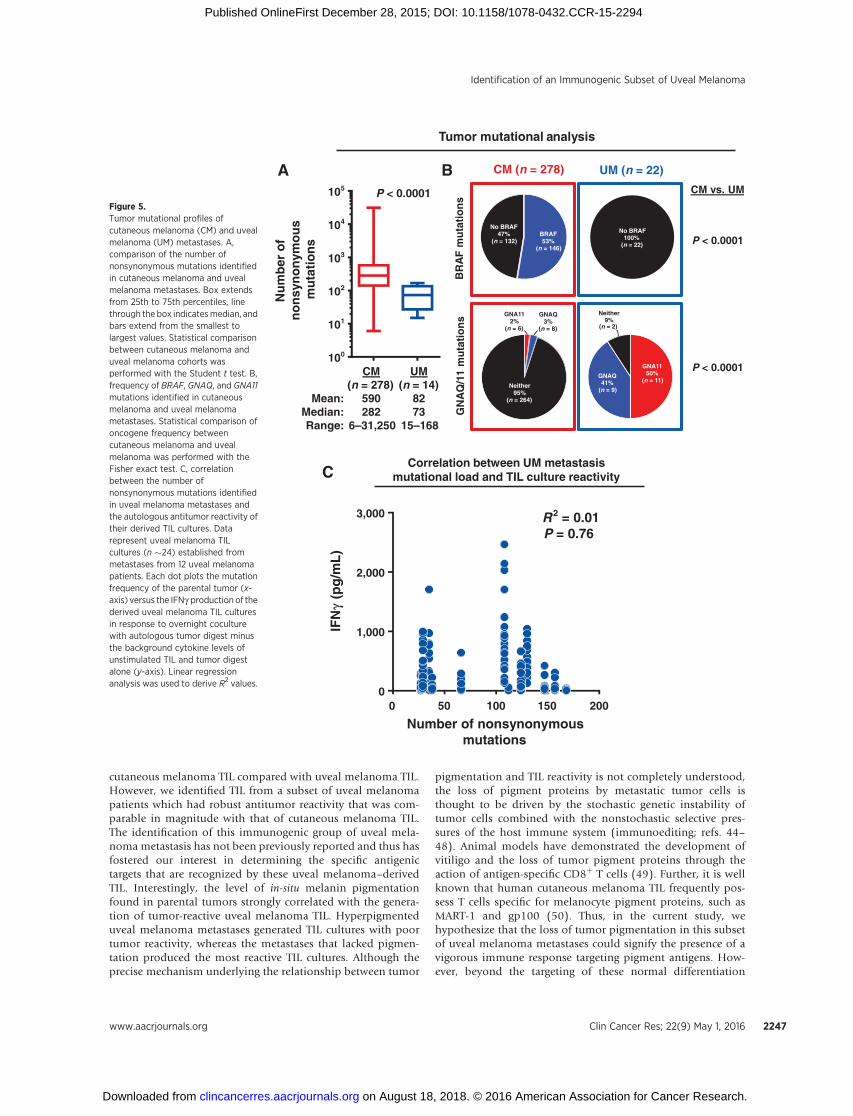
Further, comparative WES has revealed sun-exposed cutaneousmelanoma tumors to have the highest number of somatic muta-tions among common malignancies (40). These observationshave fostered the theory that the unique responsiveness of met-astatic cutaneous melanoma to a variety of immunotherapyapproaches is a direct consequence of endogenous immuneresponses against neoepitopes encoded by these large numbersof mutations. Thus, we next sought to determine if the identifiedsubset of immunogenic uveal melanoma metastases also har-bored a greatermutational load thatmight explain their enhancedT-cell recognition. Previously, it has been reported that sun-shielded melanomas, including uveal melanoma, have far fewernonsynonymous mutations when directly compared with sun-exposed cutaneous melanoma tumors (17). However, these anal-yses were based upon a limited number of uveal melanomasamples which included a mixture of primary and metastatictumors. Thus, we first sought to better determine the frequencyand characteristics of the nonsynonymousmutations occurring incutaneous melanoma and uveal melanoma metastases. To pro-vide adequate sample numbers for this analysis, we obtainedWESdata for 278 cutaneous melanoma metastases via TCGA dataportal and compared these against data from 14 uveal melanomametastases from our cohort. Of note, because the TCGA databasedoes not denote the anatomic site of themetastases, the cutaneousmelanoma data represent metastases from a variety of sites.Protein-altering somatic point mutations for each tumor weredetermined using a common analytical workflow based uponcomparison with matched germline DNA. We found that cuta-neous melanoma metastases had a broad range in mutationnumber (range: 6–31,250)when comparedwithuvealmelanomametastases (range: 15–168). Further, as a group, cutaneous mel-anoma metastases had significantly more somatic mutationswhen compared with uveal melanoma metastases (mediancounts; cutaneous melanoma: 282 vs. uveal melanoma: 73, P <0.0001; Fig. 5A).
Next, we compared the tumor cohorts for the frequency ofprototypic melanoma associated oncogenic driver mutations,including, BRAF, GNAQ, and GNA11 (Fig. 5B). We found BRAFmutations in 53% of the cutaneous melanoma metastases(n ¼ 278). However, BRAF was not mutated in any of theuveal melanoma tumors (n ¼ 22; BRAF mutation frequency;cutaneous melanoma vs. uveal melanoma metastases, P <0.0001). In contrast, activating mutations in either of thehomologous genes, GNAQ or GNA11, were identified in91% of the uveal melanoma metastases, but in only 5% ofthe cutaneous melanoma metastases (GNAQ/GNA11mutationfrequency; cutaneous melanoma vs. uveal melanoma meta-stases, P < 0.0001).
Finally, we investigated in 12 uveal melanoma patientswhether the mutational frequency identified in their metastasescorrelated with the autologous antitumor reactivity of theirrespectively derived TIL cultures (n �24 cultures/tumor). Whenthe tumor-induced IFNg production from each of the TILcultures was assessed against the number of nonsynonymousmutations identified in their respective parental tumors, wefound no correlation between the parameters (Fig. 5C).
DiscussionThe last 30 years have provided substantial evidence that
the human immune system can naturally generate potent
immunologic responses against tumor antigens expressed bymetastatic cutaneous melanoma (8). Cancer regression cannow be achieved in patients with metastatic cutaneous mela-noma with mechanistically diverse forms of immunotherapythat augment naturally existing tumor-specific T-cell responses(9–12). However, the role of these immune-based therapies forthe treatment of metastatic uveal melanoma patients remainsunclear. Patients with uveal melanoma are frequently excludedfrom metastatic melanoma immunotherapy clinical trialsbecause uveal melanoma is generally thought to be a nonim-munogenic form of melanoma (13–16). However, there havenot been formal comparative studies performed directly uponuveal melanoma and cutaneous melanoma metastases to accu-rately assess their relative immunogenicity. In this study, wecompared the tumor antigen expression, tumor mutationalload, and endogenous antitumor immunologic reactivityfound in fresh surgically resected uveal melanoma and cuta-neous melanoma metastases. By defining the tumor-specificimmune responses that are naturally found in these metastases,we sought to provide insight into the role for immune-basedtherapies for the management of uveal melanoma patients. Wepreviously reported that melanoma metastases demon-strate significant heterogeneity in tumor antigen expressionand lymphocytic infiltrate based upon their anatomic locationin the body (6). Thus, to avoid potential site-specific bias inthe current study, we focused our comparative analysis selec-tively upon liver metastases resected from uveal melanomaand cutaneous melanoma patients. Our findings revealed thatdespite having common melanocytic lineage, uveal mela-noma and cutaneous melanoma liver metastases were highlydichotomous in their melanin content, tumor differentiationantigen expression, and somatic mutational profile. The major-ity of cutaneous melanoma liver metastases lacked gross mel-anin pigmentation, whereas uveal melanoma liver metastaseswere more commonly hyperpigmented in appearance. In sup-port of this observation, immunohistochemical profilingrevealed that cutaneous melanoma metastases had lower cel-lular expression of proteins associated with melanocyte differ-entiation, including MART-1 and gp100. Further, we foundsignificant differences in the overall somatic mutational profilebetween cutaneous melanoma and uveal melanoma livermetastases. Comparative whole-exomic sequencing revealedthat cutaneous melanoma metastases had significantly greatermutational burden compared with uveal melanoma metastaseswith the melanoma variants also possessing quite differentoncogenic driver mutations of the MAPK pathway. Similar toprevious reports (41–43), nearly all of the uveal melanomametastases had GNAQ and GNA11 mutations, whereas cuta-neous melanoma metastases commonly had BRAF mutations.Collectively, these comparative studies demonstrate cutaneousmelanoma metastases to be far more dedifferentiated fromtheir melanocytic origin when compared with uveal melanomametastases in terms of their mutational profile, tumor antigenexpression, and gross melanin pigmentation.
When endogenous immune responses in these highly diver-gent forms of melanoma were characterized, we further iden-tified marked differences in the phenotype and antitumorreactivity of their respective infiltrating lymphocytes. Cutane-ous melanoma TIL were predominantly composed of CD8þ
T cells, whereas uveal melanoma TIL were CD4þ dominant.Reactivity against autologous tumor was significantly greater in
Rothermel et al.
Clin Cancer Res; 22(9) May 1, 2016 Clinical Cancer Research2246
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294
cutaneous melanoma TIL compared with uveal melanoma TIL.However, we identified TIL from a subset of uveal melanomapatients which had robust antitumor reactivity that was com-parable in magnitude with that of cutaneous melanoma TIL.The identification of this immunogenic group of uveal mela-noma metastasis has not been previously reported and thus hasfostered our interest in determining the specific antigenictargets that are recognized by these uveal melanoma–derivedTIL. Interestingly, the level of in-situ melanin pigmentationfound in parental tumors strongly correlated with the genera-tion of tumor-reactive uveal melanoma TIL. Hyperpigmenteduveal melanoma metastases generated TIL cultures with poortumor reactivity, whereas the metastases that lacked pigmen-tation produced the most reactive TIL cultures. Although theprecise mechanism underlying the relationship between tumor
pigmentation and TIL reactivity is not completely understood,the loss of pigment proteins by metastatic tumor cells isthought to be driven by the stochastic genetic instability oftumor cells combined with the nonstochastic selective pres-sures of the host immune system (immunoediting; refs. 44–48). Animal models have demonstrated the development ofvitiligo and the loss of tumor pigment proteins through theaction of antigen-specific CD8þ T cells (49). Further, it is wellknown that human cutaneous melanoma TIL frequently pos-sess T cells specific for melanocyte pigment proteins, such asMART-1 and gp100 (50). Thus, in the current study, wehypothesize that the loss of tumor pigmentation in this subsetof uveal melanoma metastases could signify the presence of avigorous immune response targeting pigment antigens. How-ever, beyond the targeting of these normal differentiation
CM(n = 278)
590282
6–31,250
UM(n = 14)
8273
15–168
P < 0.0001
Nu
mb
er o
f n
on
syn
on
ymo
us
mu
tati
on
s
100
101
102
103
104
105
Mean: Median:Range:
GNA1150%
(n = 11)GNAQ41%
(n = 9)
Neither9%
(n = 2)
No BRAF100%
(n = 22)
CM (n = 278)
BRAF53%
(n = 146)
No BRAF47%
(n = 132)
GNA112%
(n = 6)
GNAQ3%
(n = 8)
Neither95%
(n = 264)
UM (n = 22)
BR
AF
mu
tati
on
sG
NA
Q/1
1 m
uta
tio
ns
CM vs. UM
P < 0.0001
P < 0.0001
Tumor mutational analysis
A B
IFN
γ(p
g/m
L)
Number of nonsynonymous mutations
R2 = 0.01P = 0.76
Correlation between UM metastasis mutational load and TIL culture reactivity
0 50 100 150 2000
1,000
2,000
3,000
C
Figure 5.Tumor mutational profiles ofcutaneous melanoma (CM) and uvealmelanoma (UM) metastases. A,comparison of the number ofnonsynonymous mutations identifiedin cutaneous melanoma and uvealmelanoma metastases. Box extendsfrom 25th to 75th percentiles, linethrough the box indicatesmedian, andbars extend from the smallest tolargest values. Statistical comparisonbetween cutaneous melanoma anduveal melanoma cohorts wasperformed with the Student t test. B,frequency of BRAF, GNAQ, and GNA11mutations identified in cutaneousmelanoma and uveal melanomametastases. Statistical comparison ofoncogene frequency betweencutaneous melanoma and uvealmelanoma was performed with theFisher exact test. C, correlationbetween the number ofnonsynonymous mutations identifiedin uveal melanoma metastases andthe autologous antitumor reactivity oftheir derived TIL cultures. Datarepresent uveal melanoma TILcultures (n �24) established frommetastases from 12 uveal melanomapatients. Each dot plots the mutationfrequency of the parental tumor (x-axis) versus the IFNg production of thederived uveal melanoma TIL culturesin response to overnight coculturewith autologous tumor digest minusthe background cytokine levels ofunstimulated TIL and tumor digestalone (y-axis). Linear regressionanalysis was used to derive R2 values.
Identification of an Immunogenic Subset of Uveal Melanoma
www.aacrjournals.org Clin Cancer Res; 22(9) May 1, 2016 2247
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294

antigens, recent analyses have found that unique somaticmutations expressed by tumors can generate neoepitopes thatalso elicit robust autologous T-cell responses (37–39).Although our study found no correlation between the muta-tional frequencies identified in uveal melanomametastases andthe autologous antitumor reactivity of their respectively derivedTIL cultures, there may still be individual mutations that arerecognized. Thus, we have begun studies to assess the tumor-reactive uveal melanoma TIL for recognition of both nonmu-tated and mutated antigen targets.
Although not completely validated as a clinical biomarker, theMRI assessment of melanin content in uveal melanoma metas-taseswas found in this study to accurately identify tumors that canelicit a strong endogenous immune response. We are, thus,interested in determining whether immune-based therapies maybe more effective in the subset of uveal melanoma patients whoharbor these unique immunogenic tumors. To help address thesequestions, we are conducting the first-in-human adoptive T-celltransfer trial dedicated to patients with metastatic uveal melano-ma (NCT01814046). In this phase II study, patients with meta-static uveal melanoma undergo surgical metastasectomy toprocure tumor tissue for TIL generation. The expanded lympho-cytes are then adoptively transferred back into the host in con-junctionwith a nonmyeloablative lymphodepleting regimen. Theprimary endpoint of this study is to define the objective responserate of TIL immunotherapy in patients with metastatic uvealmelanoma. The results of this trial should provide valuableinsight into the role of immune-based therapies for the treatmentof metastatic uveal melanoma.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: L.D. Rothermel, A.C. Sabesan, D.J. Stephens,U.S. Kammula, T.H. PhamDevelopment of methodology: L.D. Rothermel, A.C. Sabesan, D.J. Stephens,S.S. Chandran, B.C. Paria, A.K. Srivastava, U.S. Kammula, L. Xi, T.H. PhamAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): L.D. Rothermel, A.C. Sabesan, D.J. Stephens,S.S. Chandran, B.C. Paria, A.K. Srivastava, J.R. Wunderlich, C.-C.R. Lee,M. Raffeld, U.S. Kammula, L. XiAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): L.D. Rothermel, A.C. Sabesan, D.J. Stephens,S.S. Chandran, B.C. Paria, A.K. Srivastava, M. Raffeld, P. Jailwala, M. Kasoji,U.S. Kammula, L. Xi, T.H. PhamWriting, review, and/or revision of the manuscript: L.D. Rothermel,A.C. Sabesan, D.J. Stephens, S.S. Chandran, B.C. Paria, A.K. Srivastava,C.-C.R. Lee, M. Raffeld, U.S. Kammula, L. XiAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): L.D. Rothermel, A.C. Sabesan,D.J. Stephens, R. Somerville, P. Jailwala, U.S. Kammula, T.H. PhamStudy supervision: U.S. Kammula
AcknowledgmentsThe authors thank the Surgery Branch cell production facility and the
immunotherapy clinical and support staff for their contributions. They alsothank Li Jia for assistance in bioinformatics analysis. The ProspectiveProcurement of Solid Tumor Tissue to Identify Novel Therapeutic studywas supported by the Intramural Research Program of the NCI, NIH,Department of Health and Human Services. Whole-exome raw data wereuploaded to the NIH database for Genotypes and Phenotypes (dbGaP)under accession number phs001003.v1.p1.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received September 21, 2015; revised November 11, 2015; acceptedDecember 7, 2015; published OnlineFirst December 28, 2015.
References1. Woll E, Bedikian A, Legha SS. Uveal melanoma: natural history and
treatment options for metastatic disease. Melanoma Res 1999;9:575–81.2. Singh AD, Turell ME, Topham AK. Uveal melanoma: trends in incidence,
treatment, and survival. Ophthalmology 2011;118:1881–5.3. Woodman SE. Metastatic uveal melanoma: biology and emerging treat-
ments. Cancer J 2012;18:148–52.4. de Vries TJ, Fourkour A, Wobbes T, Verkroost G, Ruiter DJ, vanMuijen GN.
Heterogeneous expression of immunotherapy candidate proteins gp100,MART-1, and tyrosinase in human melanoma cell lines and in humanmelanocytic lesions. Cancer Res 1997;57:3223–9.
5. de Vries TJ, Trancikova D, Ruiter DJ, van Muijen GN. High expression ofimmunotherapy candidate proteins gp100, MART-1, tyrosinase and TRP-1in uveal melanoma. Br J Cancer 1998;78:1156–61.
6. Bartlett EK, Fetsch PA, Filie AC, Abati A, Steinberg SM,Wunderlich JR, et al.Human melanoma metastases demonstrate nonstochastic site-specificantigen heterogeneity that correlates with T-cell infiltration. Clin CancerRes 2014;20:2607–16.
7. Harbour JW. The genetics of uveal melanoma: an emerging framework fortargeted therapy. Pigment Cell Melanoma Res 2012;25:171–81.
8. Coulie PG, Van den Eynde BJ, van der Bruggen P, Boon T. Tumour antigensrecognized by T lymphocytes: at the core of cancer immunotherapy.Nat Rev Cancer 2014;14:135–46.
9. Atkins MB, Lotze MT, Dutcher JP, Fisher RI, Weiss G, Margolin K, et al.High-dose recombinant interleukin 2 therapy for patients with meta-static melanoma: analysis of 270 patients treated between 1985 and1993. J Clin Oncol 1999;17:2105–16.
10. Hodi FS,O'Day SJ,McDermottDF,Weber RW, Sosman JA,Haanen JB, et al.Improved survival with ipilimumab inpatientswithmetastaticmelanoma.N Engl J Med 2010;363:711–23.
11. Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R, et al. Safetyand tumor responses with lambrolizumab (anti-PD-1) in melanoma.N Engl J Med 2013;369:134–44.
12. Rosenberg SA, Yang JC, Sherry RM, Kammula US, Hughes MS, Phan GQ,et al. Durable complete responses in heavily pretreated patientswith metastatic melanoma using T-cell transfer immunotherapy.Clin Cancer Res 2011;17:4550–7.
13. Yang W, Chen PW, Li H, Alizadeh H, Niederkorn JY. PD-L1: PD-1 inter-action contributes to the functional suppression of T-cell responsesto human uveal melanoma cells in vitro. Invest Ophthalmol Vis Sci2008;49:2518–25.
14. McKenna KC, Chen PW. Influence of immune privilege on ocular tumordevelopment. Ocul Immunol Inflamm 2010;18:80–90.
15. Niederkorn JY. Ocular immune privilege and ocular melanoma: paralleluniverses or immunological plagiarism? Front Immunol 2012;3:148.
16. Chen PW, Mellon JK, Mayhew E, Wang S, He YG, Hogan N, et al. Uvealmelanoma expression of indoleamine 2,3-deoxygenase: establishment ofan immune privileged environment by tryptophan depletion. Exp Eye Res2007;85:617–25.
17. Krauthammer M, Kong Y, Ha BH, Evans P, Bacchiocchi A, McCusker JP,et al. Exome sequencing identifies recurrent somatic RAC1 mutations inmelanoma. Nat Genet 2012;44:1006–14.
18. Dorval T, Fridman WH, Mathiot C, Pouillart P. Interleukin-2 therapy formetastatic uveal melanoma. Eur J Cancer 1992;28A:2087.
19. Luke JJ, Callahan MK, Postow MA, Romano E, Ramaiya N, Bluth M, et al.Clinical activity of ipilimumab for metastatic uveal melanoma: a retro-spective review of theDana-Farber Cancer Institute,Massachusetts GeneralHospital, Memorial Sloan-Kettering Cancer Center, and University Hos-pital of Lausanne experience. Cancer 2013;119:3687–95.
Rothermel et al.
Clin Cancer Res; 22(9) May 1, 2016 Clinical Cancer Research2248
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294
20. Maio M, Danielli R, Chiarion-Sileni V, Pigozzo J, Parmiani G, Ridolfi R,et al. Efficacy and safety of ipilimumab in patients with pre-treated, uvealmelanoma. Ann Oncol 2013;24:2911–5.
21. JoshuaAM,Monzon JG,MihalcioiuC,HoggD, SmylieM,Cheng T. Aphase2 study of tremelimumab in patients with advanced uveal melanoma.Melanoma Res 2015;25:342–7.
22. Dudley ME, Wunderlich JR, Shelton TE, Even J, Rosenberg SA. Generationof tumor-infiltrating lymphocyte cultures for use in adoptive transfertherapy for melanoma patients. J Immunother 2003;26:332–42.
23. Bioinformatics.babraham.ac.uk. Babraham Bioinformatics - FastQC AQuality Control tool for High Throughput Sequence Data [Internet].2015 [cited 2015 March 20]; Available from: http://www.bioinformat-ics.babraham.ac.uk/projects/fastqc/.
24. Patel RK, Jain M. NGS QC Toolkit: a toolkit for quality control of nextgeneration sequencing data. PLoS One 2012;7:e30619.
25. Bolger AM, Lohse M, Usadel B. Trimmomatic: a flexible trimmer forIllumina sequence data. Bioinformatics 2014;30:2114–20.
26. Li H, Durbin R. Fast and accurate long-read alignment with Burrows-Wheeler transform. Bioinformatics 2010;26:589–95.
27. Institute G. GATK j Best Practice Workflows [Internet]. Broadinstituteorg;2015 [cited 2015 March 30]. Available from: https://www.broadinstitute.org/gatk/guide/best-practices.
28. Cibulskis K, LawrenceMS,Carter SL, SivachenkoA, JaffeD, SougnezC, et al.Sensitive detection of somatic point mutations in impure and heteroge-neous cancer samples. Nat Biotechnol 2013;31:213–9.
29. WangK, LiM,HakonarsonH.ANNOVAR: functional annotationof geneticvariants from high-throughput sequencing data. Nucleic Acids Res 2010;38:e164.
30. Gdac.broadinstitute.org. [Internet] 2015 [cited 2015 March 20]; Avail-able from: http://gdac.broadinstitute.org/runs/stddata__2014_07_15/data/SKCM/20140715/gdac.broadinstitute.org_SKCM.Mutation_Packager_Calls.Level_3.2014071500.0.0.tar.gz.
31. Thorvaldsdottir H, Robinson JT, Mesirov JP. Integrative Genomics Viewer(IGV): high-performance genomics data visualization and exploration.Brief Bioinform 2013;14:178–92.
32. Egberts F, Bergner I, Kruger S, Haag J, Behrens HM, Hauschild A, et al.Metastatic melanoma of unknown primary resembles the genotype ofcutaneous melanomas. Ann Oncol 2014;25:246–50.
33. Premkumar A, Marincola F, Taubenberger J, Chow C, Venzon D, Schwart-zentruber D. Metastatic melanoma: correlation of MRI characteristics andhistopathology. J Magn Reson Imaging 1996;6:190–4.
34. Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, Lagorce-PagesC, et al. Type, density, and location of immune cells within humancolorectal tumors predict clinical outcome. Science 2006;313:1960–4.
35. Liu H, Zhang T, Ye J, Li H, Huang J, Li X, et al. Tumor-infiltratinglymphocytes predict response to chemotherapy in patients withadvance non-small cell lung cancer. Cancer Immunol Immunother2012;61:1849–56.
36. Adams S, Gray RJ, Demaria S, Goldstein L, Perez EA, Shulman LN,et al. Prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancers from two phase III randomized adjuvantbreast cancer trials: ECOG 2197 and ECOG 1199. J Clin Oncol2014;32:2959–66.
37. Robbins PF, Lu YC, El-Gamil M, Li YF, Gross C, Gartner J, et al. Miningexomic sequencing data to identify mutated antigens recognizedby adoptively transferred tumor-reactive T cells. Nat Med 2013;19:747–52.
38. Schumacher TN, Schreiber RD. Neoantigens in cancer immunotherapy.Science 2015;348:69–74.
39. Tran E, Turcotte S, Gros A, Robbins PF, Lu YC, Dudley ME, et al. Cancerimmunotherapy based onmutation-specific CD4þ T cells in a patient withepithelial cancer. Science 2014;344:641–5.
40. LawrenceMS, Stojanov P, Polak P, Kryukov GV, Cibulskis K, Sivachenko A,et al. Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature 2013;499:214–8.
41. Van Raamsdonk CD, Bezrookove V, Green G, Bauer J, Gaugler L, O'BrienJM, et al. Frequent somatic mutations of GNAQ in uveal melanoma andblue naevi. Nature 2009;457:599–602.
42. Van Raamsdonk CD, Griewank KG, Crosby MB, Garrido MC, Vemula S,Wiesner T, et al. Mutations in GNA11 in uveal melanoma. N Engl J Med2010;363:2191–9.
43. ColombinoM, CaponeM, Lissia A, Cossu A, Rubino C, DeGV, et al. BRAF/NRAS mutation frequencies among primary tumors and metastases inpatients with melanoma. J Clin Oncol 2012;30:2522–9.
44. MatsushitaH, VeselyMD, Koboldt DC, Rickert CG, Uppaluri R,Magrini VJ,et al. Cancer exome analysis reveals a T-cell-dependent mechanism ofcancer immunoediting. Nature 2012;482:400–4.
45. Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integratingimmunity's roles in cancer suppression and promotion. Science 2011;331:1565–70.
46. Swann JB, Smyth MJ. Immune surveillance of tumors. J Clin Invest2007;117:1137–46.
47. Landsberg J, Kohlmeyer J, Renn M, Bald T, Rogava M, Cron M, et al.Melanomas resist T-cell therapy through inflammation-induced reversiblededifferentiation. Nature 2012;490:412–6.
48. Shankaran V, Ikeda H, Bruce AT, White JM, Swanson PE, Old LJ, et al.IFNgamma and lymphocytes prevent primary tumour development andshape tumour immunogenicity. Nature 2001;410:1107–11.
49. Overwijk WW, Theoret MR, Finkelstein SE, Surman DR, de Jong LA, Vyth-Dreese FA, et al. Tumor regression and autoimmunity after reversal of afunctionally tolerant state of self-reactive CD8þ T cells. J Exp Med 2003;198:569–80.
50. Kawakami Y, Dang N, Wang X, Tupesis J, Robbins PF, Wang RF, et al.Recognition of shared melanoma antigens in association withmajor HLA-A alleles by tumor infiltrating T lymphocytes from 123 patients withmelanoma. J Immunother 2000;23:17–27.
www.aacrjournals.org Clin Cancer Res; 22(9) May 1, 2016 2249
Identification of an Immunogenic Subset of Uveal Melanoma
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294
2016;22:2237-2249. Published OnlineFirst December 28, 2015.Clin Cancer Res Luke D. Rothermel, Arvind C. Sabesan, Daniel J. Stephens, et al. MelanomaIdentification of an Immunogenic Subset of Metastatic Uveal
Updated version
10.1158/1078-0432.CCR-15-2294doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2015/12/23/1078-0432.CCR-15-2294.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/22/9/2237.full#ref-list-1
This article cites 47 articles, 12 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/22/9/2237.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/22/9/2237To request permission to re-use all or part of this article, use this link
on August 18, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 28, 2015; DOI: 10.1158/1078-0432.CCR-15-2294