Embed Size (px)
Citation preview

IDCIDC
New Therapeutic Interventions New Therapeutic Interventions in Diabetes Managementin Diabetes Management
• Insulin analogsInsulin analogs
• Oral AgentsOral Agents
• Medical Nutrition InterventionMedical Nutrition Intervention

IDCIDC
Pathophysiology of DiabetesPathophysiology of DiabetesPeripheral TissuesPeripheral Tissues(Muscle and Fat)(Muscle and Fat)
GlucoseGlucoseLiverLiver
Impaired or no insulin secretionImpaired or no insulin secretionincreased or normal glucagon increased or normal glucagon
secretionsecretion
Increased glucose Increased glucose productionproduction
Receptor +Receptor +postreceptor defectpostreceptor defect
InsulinInsulinresistanceresistance
PancreasPancreas
Nutrition
(carbohydrates)
IDCIDC
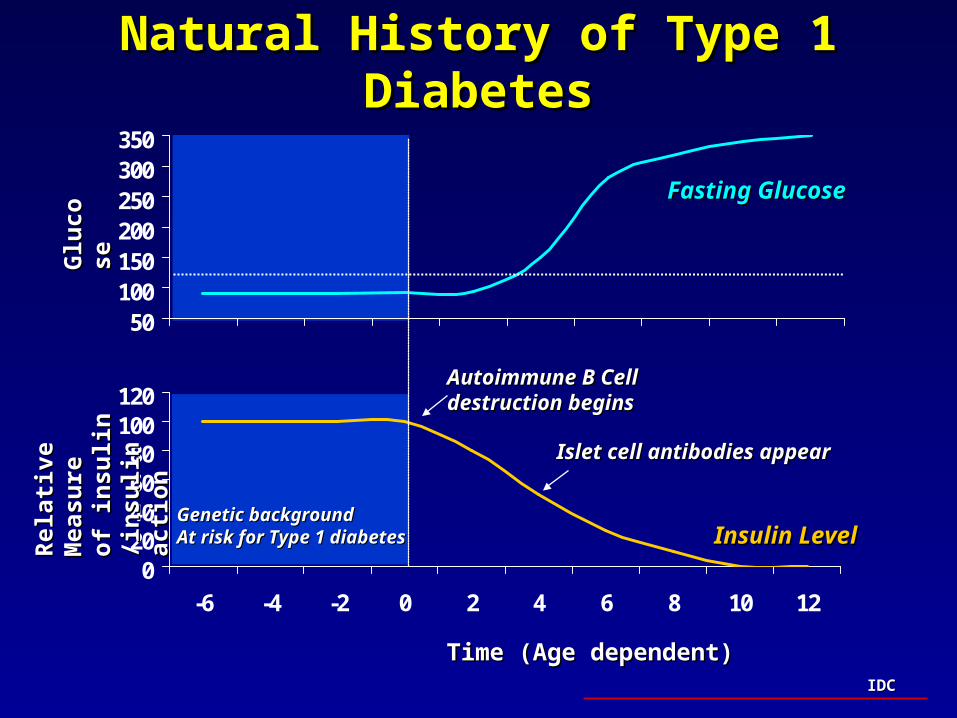
Natural History of Type 1 DiabetesNatural History of Type 1 Diabetes
020406080
100120
-6 -4 -2 0 2 4 6 8 10 12
50100150200250300350
Time (Age dependent)Time (Age dependent)
Glu
cose
Glu
cose
Rel
ativ
e M
easu
reR
elat
ive
Mea
sure
of in
suli
n /i
nsu
lin
of
insu
lin
/ins
uli
n
acti
onac
tion
Insulin LevelInsulin Level
Fasting GlucoseFasting Glucose
Autoimmune B Cell Autoimmune B Cell destruction beginsdestruction begins
Genetic backgroundGenetic backgroundAt risk for Type 1 diabetesAt risk for Type 1 diabetes
Islet cell antibodies appearIslet cell antibodies appear

IDCIDC
Natural History of Type 2 DiabetesNatural History of Type 2 Diabetes
0
50
100
150
200
250
-15 -10 -5 0 5 10 15 20 25 30
50100150200250300350
Years of DiabetesYears of Diabetes
Glu
cose
Glu
cose
Rel
ativ
e M
easu
reR
elat
ive
Mea
sure
of in
suli
n /i
nsu
lin
of
insu
lin
/ins
uli
n
acti
onac
tion
Insulin ResistanceInsulin Resistance
Insulin LevelInsulin Level
Fasting GlucoseFasting Glucose
Beta cell failureBeta cell failure
Post Meal GlucosePost Meal Glucose
Adapted from: DeFronzo RA. Adapted from: DeFronzo RA. DiabetesDiabetes. 37:667, 1988. . 37:667, 1988.
Saltiel J. Saltiel J. Diabetes. Diabetes. 45:1661-1669, 199645:1661-1669, 1996. . Robertson RP. Robertson RP. Diabetes. 43:1085, 1994.
Tokuyama Y. Tokuyama Y. DiabetesDiabetes 44:1447, 1995. Polonsky KS. 44:1447, 1995. Polonsky KS. N Engl J Med N Engl J Med 1996;334:777.1996;334:777.
At risk for DiabetesAt risk for Diabetes
normal
IDCIDC
Pharmacologic Therapies for DiabetesPharmacologic Therapies for Diabetes
• Insulin Therapy-Insulin Therapy-Type 1, Type 2, and GDMType 1, Type 2, and GDM
– Human/AnimalHuman/Animal– Insulin AnalogsInsulin Analogs
• Lispro, AspartLispro, Aspart• HOE-901HOE-901
• Oral Agents Oral Agents - for Type 2 diabetes- for Type 2 diabetes– Sulfonylureas (1st, 2nd and 3rd generation) Sulfonylureas (1st, 2nd and 3rd generation) – Acarbose Acarbose – Metformin Metformin – ThiazolidinedionesThiazolidinediones
• Troglitazone, Rosiglitazone*and Pioglitazone*Troglitazone, Rosiglitazone*and Pioglitazone*
– RepaglinideRepaglinide
IDCIDC
Selecting Insulin TherapySelecting Insulin TherapyType 1, Type 2 Diabetes and GDMType 1, Type 2 Diabetes and GDM
• There is no limit to the blood glucose lowering There is no limit to the blood glucose lowering action of insulinaction of insulin
• Food plans and exercise (medical nutrition Food plans and exercise (medical nutrition interventions) must be synchronized with interventions) must be synchronized with insulin to optimize the glucose lowering ability insulin to optimize the glucose lowering ability of insulin of insulin
• Therefore, insulin and medical nutrition Therefore, insulin and medical nutrition intervention must be approached as an intervention must be approached as an integrated therapyintegrated therapy
IDCIDC
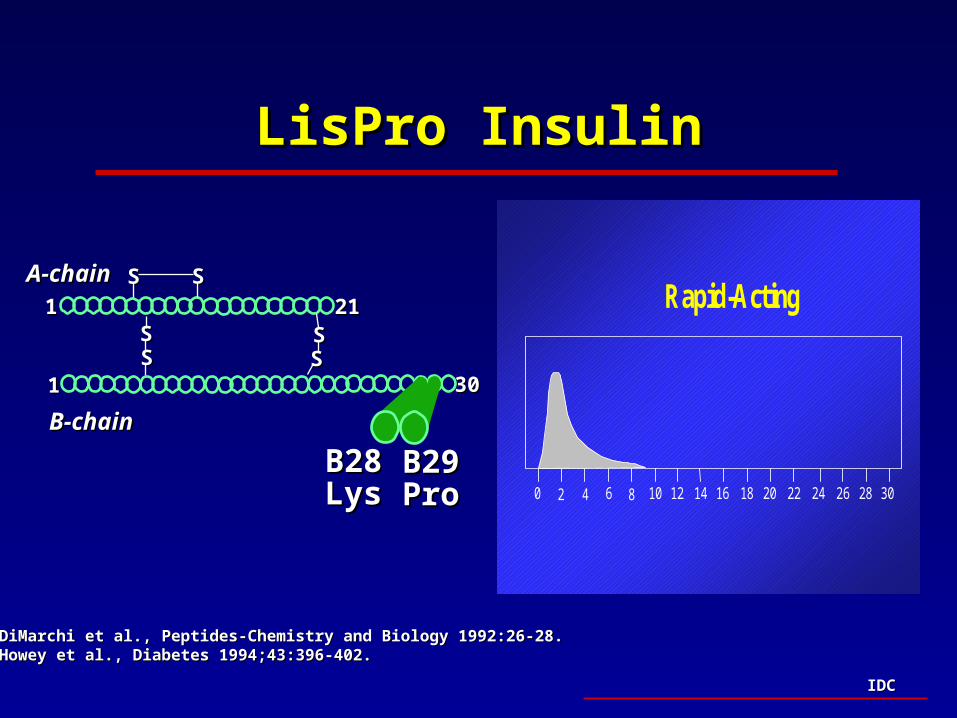
Insulin Analogs: Lispro InsulinInsulin Analogs: Lispro Insulin
• Modification of human insulinModification of human insulin (Lys-Pro) (Lys-Pro)– Increased rate of subcutaneous absorption (more Increased rate of subcutaneous absorption (more
physiological)physiological)
• Equivalent glycemic controlEquivalent glycemic control• Reduced rates of hypoglycemiaReduced rates of hypoglycemia• Convenience - improved flexibilityConvenience - improved flexibility
– Taken with meal (onset of action ~ 15 minutes)Taken with meal (onset of action ~ 15 minutes)
– Reduced risk of exercise-induced hypoglycemiaReduced risk of exercise-induced hypoglycemia
– Limits need for snacksLimits need for snacks
– Can be used to cover snacksCan be used to cover snacks
IDCIDC
A-chainA-chain11 2121
SS SS
SSSS
SSSS
B-chainB-chain
11 3030
B29B29ProPro
B28B28LysLys
DiMarchi et al., Peptides-Chemistry and Biology 1992:26-28.DiMarchi et al., Peptides-Chemistry and Biology 1992:26-28.Howey et al., Diabetes 1994;43:396-402.Howey et al., Diabetes 1994;43:396-402.
Rapid-Acting
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30
LisPro InsulinLisPro Insulin
IDCIDC
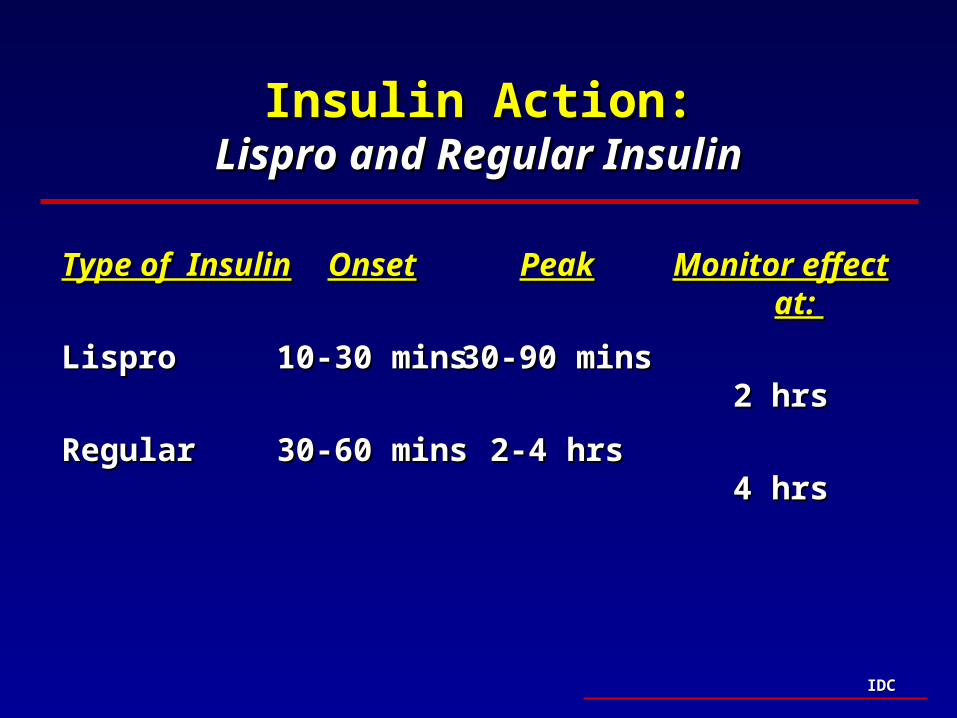
Insulin Action:Insulin Action:Lispro and Regular InsulinLispro and Regular Insulin
Type of InsulinType of Insulin
Lispro Lispro
RegularRegular
Monitor effect at: Monitor effect at:
2 hrs2 hrs
4 hrs4 hrs
OnsetOnset
10-30 mins10-30 mins
30-60 mins30-60 mins
PeakPeak
30-90 mins30-90 mins
2-4 hrs2-4 hrs
IDCIDC
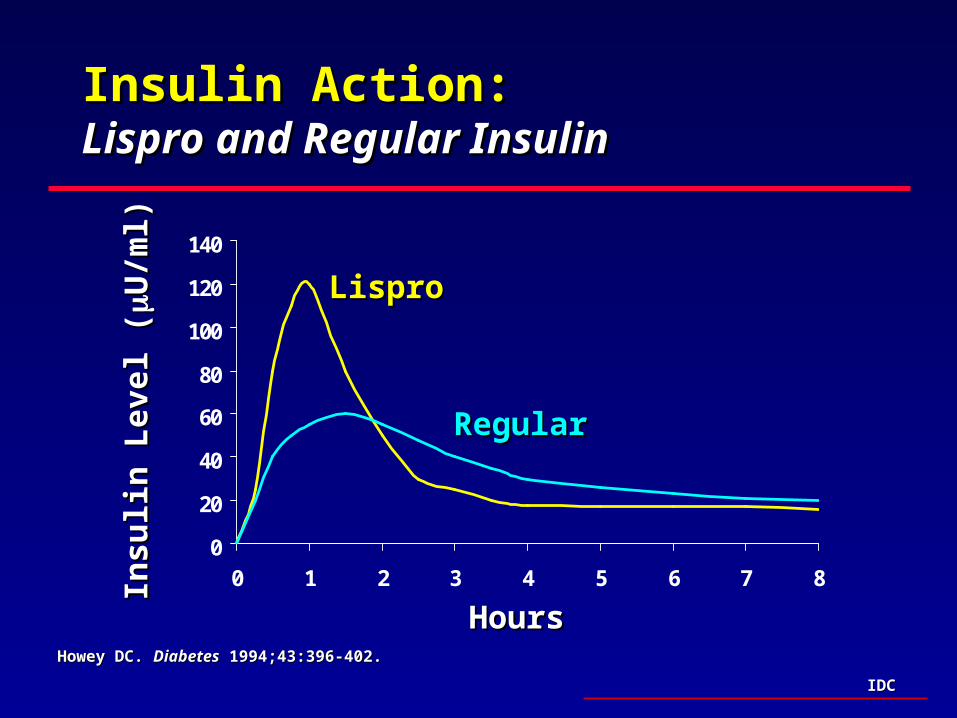
Insulin Action:Insulin Action:Lispro and Regular InsulinLispro and Regular Insulin
0
20
40
60
80
100
120
140
0 1 2 3 4 5 6 7 8
RegularRegular
LisproLispro
Insu
lin
Lev
el (
Insu
lin
Lev
el (
U/m
l)U
/ml)
HoursHoursHowey DC. Howey DC. DiabetesDiabetes 1994;43:396-402. 1994;43:396-402.
IDCIDC
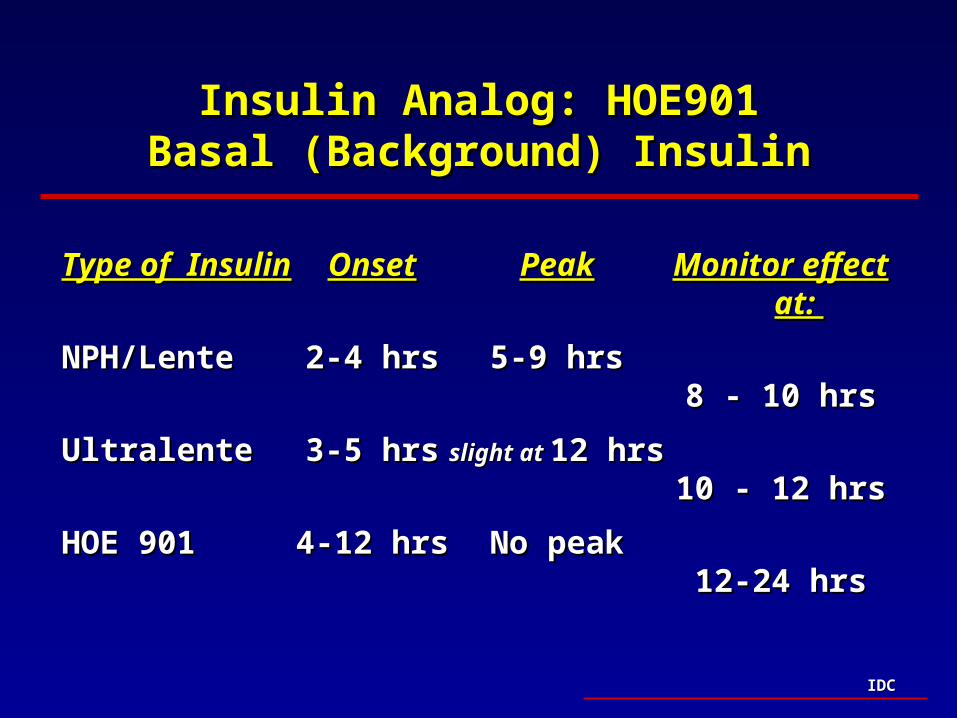
Insulin Analog: HOE901Insulin Analog: HOE901Basal (Background) InsulinBasal (Background) Insulin
Type of InsulinType of Insulin
NPH/Lente NPH/Lente
UltralenteUltralente
HOE 901HOE 901
Monitor effect at: Monitor effect at:
8 - 10 hrs8 - 10 hrs
10 - 12 hrs10 - 12 hrs
12-24 hrs12-24 hrs
OnsetOnset
2-4 hrs2-4 hrs
3-5 hrs3-5 hrs
4-12 hrs4-12 hrs
PeakPeak
5-9 hrs5-9 hrs
slight at slight at 12 hrs12 hrs
No peakNo peak
IDCIDC
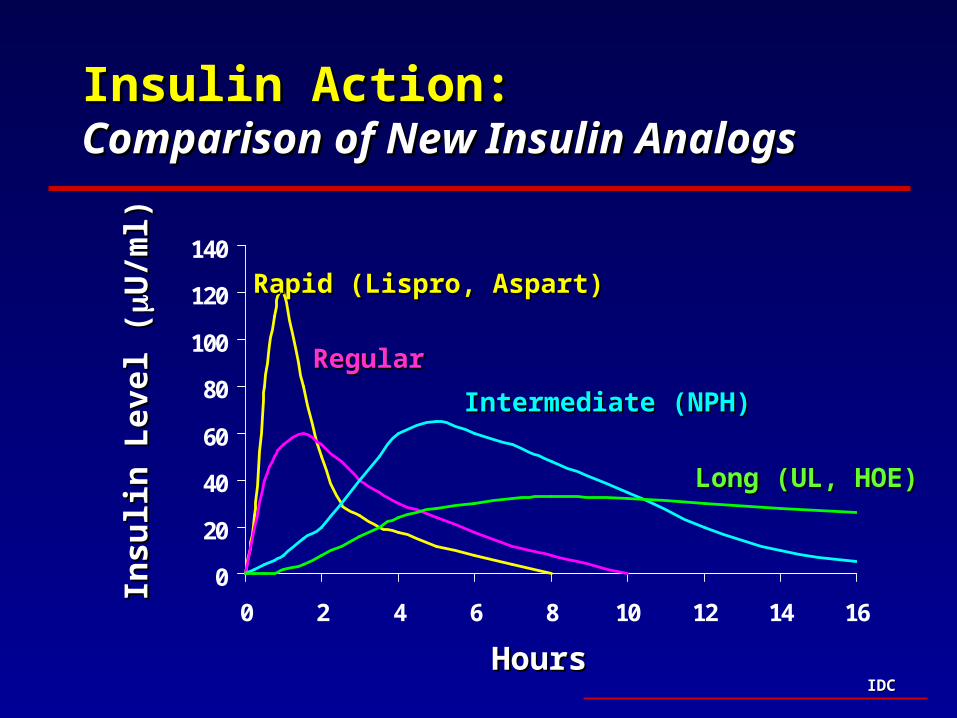
Insulin Action: Insulin Action: Comparison of New Insulin Analogs Comparison of New Insulin Analogs
0
20
40
60
80
100
120
140
0 2 4 6 8 10 12 14 16
RegularRegular
Rapid (Lispro, Aspart)Rapid (Lispro, Aspart)
Insu
lin
Lev
el (
Insu
lin
Lev
el (
U/m
l)U
/ml)
HoursHours
Intermediate (NPH)Intermediate (NPH)
Long (UL, HOE)Long (UL, HOE)
IDCIDC
Choosing the Best Therapy--Type 2Choosing the Best Therapy--Type 2
• Food plan and exercise (medical nutrition) Food plan and exercise (medical nutrition) – lower BG by up to 100 mg/dL when used as a lower BG by up to 100 mg/dL when used as a
monotherapymonotherapy
• Oral agents alone or in combination Oral agents alone or in combination – lower BG by no greater than 80-100 mg/dLlower BG by no greater than 80-100 mg/dL
• Therefore, food plan and oral agents will lower BG Therefore, food plan and oral agents will lower BG by up to 200 mg/dLby up to 200 mg/dL
There is no limit to the blood glucose lowering action of There is no limit to the blood glucose lowering action of insulininsulin
IDCIDC
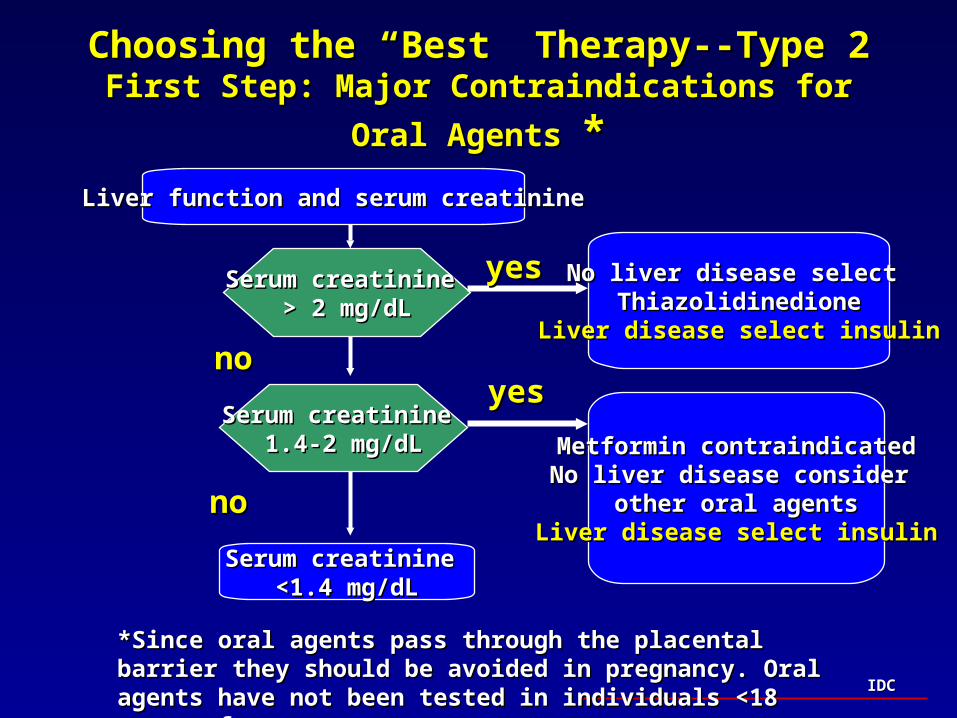
Choosing the “Best” Therapy--Type 2Choosing the “Best” Therapy--Type 2First Step: Major Contraindications for Oral Agents First Step: Major Contraindications for Oral Agents **
Liver function and serum creatinineLiver function and serum creatinine
Serum creatinine Serum creatinine > 2 mg/dL> 2 mg/dL
Serum creatinine Serum creatinine 1.4-2 mg/dL1.4-2 mg/dL
Serum creatinine Serum creatinine <1.4 mg/dL<1.4 mg/dL
Metformin contraindicatedMetformin contraindicatedNo liver disease consider No liver disease consider
other oral agentsother oral agentsLiver disease select insulinLiver disease select insulin
No liver disease select No liver disease select ThiazolidinedioneThiazolidinedione
Liver disease select insulinLiver disease select insulinnono
nono
yesyes
*Since oral agents pass through the placental barrier they should be *Since oral agents pass through the placental barrier they should be avoided in pregnancy. Oral agents have not been tested in individuals avoided in pregnancy. Oral agents have not been tested in individuals <18 years of age. <18 years of age.
yesyes
IDCIDC
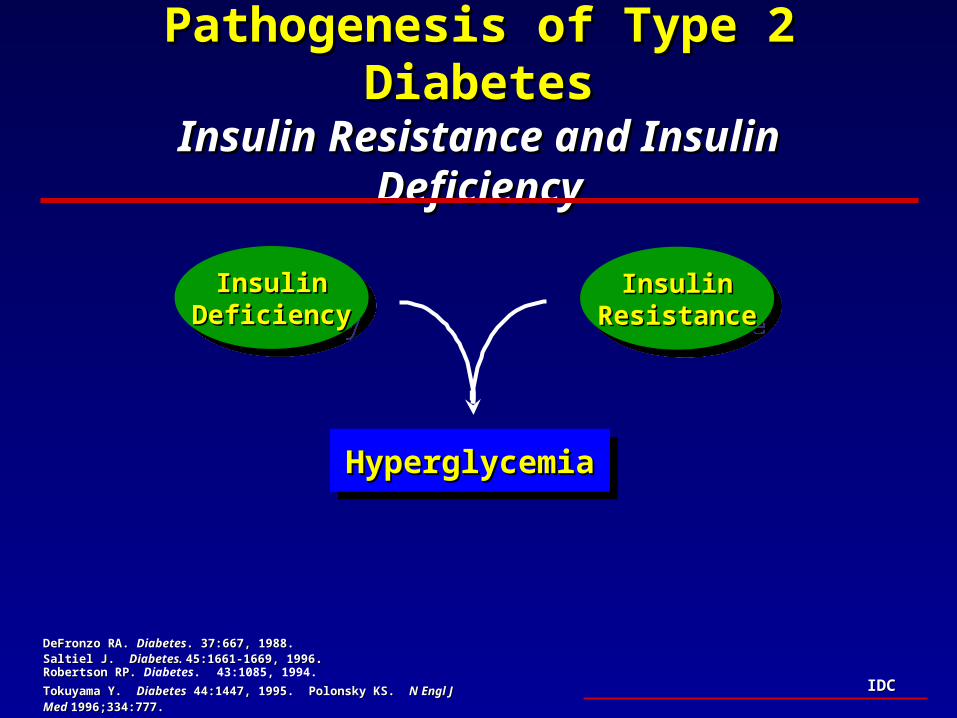
Pathogenesis of Type 2 DiabetesPathogenesis of Type 2 DiabetesInsulin Resistance and Insulin DeficiencyInsulin Resistance and Insulin Deficiency
DeFronzo RA. DeFronzo RA. DiabetesDiabetes. 37:667, 1988. . 37:667, 1988. Saltiel J. Saltiel J. Diabetes. Diabetes. 45:1661-1669, 199645:1661-1669, 1996. . Robertson RP. Robertson RP. Diabetes. 43:1085, 1994.
Tokuyama Y. Tokuyama Y. DiabetesDiabetes 44:1447, 1995. Polonsky KS. 44:1447, 1995. Polonsky KS. N Engl J Med N Engl J Med 1996;334:777.1996;334:777.
InsulinInsulinResistanceResistance
InsulinInsulinResistanceResistance
InsulinInsulinDeficiencyDeficiency
InsulinInsulinDeficiencyDeficiency
HyperglycemiaHyperglycemiaHyperglycemiaHyperglycemia
IDCIDC
SulfonylureasSulfonylureasClinical Indications and UseClinical Indications and Use
• Multiple agents availableMultiple agents available– Stimulate insulin releaseStimulate insulin release– 2nd generation agents, clinically effective dose 5-20 mg/d 2nd generation agents, clinically effective dose 5-20 mg/d
(gliclazide, glibenclamide, glipizide)(gliclazide, glibenclamide, glipizide)– 3rd generation agent - glimepiride, once daily 3rd generation agent - glimepiride, once daily (1-8 mg/d)(1-8 mg/d)
• Clinical UseClinical Use– Initial therapy (glucose > 200), lean patientInitial therapy (glucose > 200), lean patient– Most effective Most effective earlyearly in course of disease in course of disease– Combination therapy with metformin, troglitazoneCombination therapy with metformin, troglitazone
• Side Effects/RisksSide Effects/Risks – Hypoglycemia, weight gainHypoglycemia, weight gain

IDCIDC
MetforminMetforminClinical ConsiderationsClinical Considerations
• Patient SelectionPatient Selection– Use as mono or combination therapy with SU, insulinUse as mono or combination therapy with SU, insulin
– Initial therapy in obese, insulin resistant patientInitial therapy in obese, insulin resistant patient
– Consider use if dyslipidemia, high risk of CVDConsider use if dyslipidemia, high risk of CVD
– Less hypoglycemia, limited weight gainLess hypoglycemia, limited weight gain
• Side EffectsSide Effects– GI intolerance = limited if dose titrated slowlyGI intolerance = limited if dose titrated slowly
– Lactic acidosis = rare Lactic acidosis = rare
• Contraindications/PrecautionsContraindications/Precautions– Renal insufficiency (Cr>1.5), significant hepatic diseaseRenal insufficiency (Cr>1.5), significant hepatic disease
– CHF or active coronary artery diseaseCHF or active coronary artery disease
IDCIDC
Thiazolidinediones - TroglitazoneThiazolidinediones - Troglitazone Clinical ConsiderationsClinical Considerations
• Patient SelectionPatient Selection– Use as Use as Combination therapyCombination therapy: SU or insulin: SU or insulin
– Use in insulin resistant individual or those requiring > 0.7-1.0 Use in insulin resistant individual or those requiring > 0.7-1.0 unit/kg insulin, can use in renal insufficiency unit/kg insulin, can use in renal insufficiency
– Alternative to metformin Alternative to metformin (intolerance, CHF, ASCVD)(intolerance, CHF, ASCVD)
• Side EffectsSide Effects– Weight gain Weight gain (2-10 lbs.),(2-10 lbs.), modest increase in LDL modest increase in LDL
– Abnormal liver functionAbnormal liver function
• Contraindications/PrecautionsContraindications/Precautions– Hepatic disease Hepatic disease (rare cases of severe hepatic dysfunction)(rare cases of severe hepatic dysfunction)
– Routine monitoring of liver function advisedRoutine monitoring of liver function advised
IDCIDC
Newer ThiazolidinedionesNewer Thiazolidinediones
• RosiglitazoneRosiglitazone– Similar insulin-enhancing effect to troglitazoneSimilar insulin-enhancing effect to troglitazone
– Monotherapy - reduces glucose 30-70 mg/dlMonotherapy - reduces glucose 30-70 mg/dl
– Combination therapy (metformin, sulfonylureas)Combination therapy (metformin, sulfonylureas)
– Lower risk of hepatic dysfunction ? Lower risk of hepatic dysfunction ?
• PioglitazonePioglitazone– Similar insulin-enhancing effect to troglitazoneSimilar insulin-enhancing effect to troglitazone
– Limited clinical data availableLimited clinical data available

IDCIDC
RepaglinideRepaglinide
• Patient SelectionPatient Selection– Insulin deficientInsulin deficient
– Rapid acting, alternative to sulfonylureaRapid acting, alternative to sulfonylurea• Targets post-meal glucoseTargets post-meal glucose• Variable scheduleVariable schedule• ? Lower risk of hypoglycemia? Lower risk of hypoglycemia
– Monotherapy or combination (metformin)Monotherapy or combination (metformin)
– Can be used in renal insufficiencyCan be used in renal insufficiency
• Side EffectsSide Effects– Weight gain, hypoglycemiaWeight gain, hypoglycemia
IDCIDC
AcarboseAcarbose
• Patient SelectionPatient Selection– Targets post meal hyperglycemiaTargets post meal hyperglycemia– Need for limited blood glucose lowering Need for limited blood glucose lowering (A1c (A1c 0.5-1.0%) 0.5-1.0%)
– Use in combination with any other therapyUse in combination with any other therapy
• Side EffectsSide Effects– GI side effects common (flatulence, abdominal pain and GI side effects common (flatulence, abdominal pain and
diarrhea) - less with dose titrationdiarrhea) - less with dose titration
• Contraindications/PrecautionsContraindications/Precautions– Other bowel diseaseOther bowel disease– Intolerance (GI effects)Intolerance (GI effects)

IDCIDC
RepaglinideRepaglinidePost-meal hyperglycemiaPost-meal hyperglycemia
Variable scheduleVariable scheduleAlternative to SUAlternative to SU
May use in renal insufficiencyMay use in renal insufficiency
RepaglinideRepaglinidePost-meal hyperglycemiaPost-meal hyperglycemia
Variable scheduleVariable scheduleAlternative to SUAlternative to SU
May use in renal insufficiencyMay use in renal insufficiency
AcarboseAcarbosePost meal hyperglycemiaPost meal hyperglycemia
No hypoglycemiaNo hypoglycemiaLimited potencyLimited potency
AcarboseAcarbosePost meal hyperglycemiaPost meal hyperglycemia
No hypoglycemiaNo hypoglycemiaLimited potencyLimited potency
Oral Agent - MonotherapyOral Agent - MonotherapyOral Agent - MonotherapyOral Agent - Monotherapy
MetforminMetforminObese, insulin resistantObese, insulin resistant
DyslipidemiaDyslipidemiaCr <1.5Cr <1.5
MetforminMetforminObese, insulin resistantObese, insulin resistant
DyslipidemiaDyslipidemiaCr <1.5Cr <1.5
? Thiazolidinediones? ThiazolidinedionesInsulin resistantInsulin resistant
Inappropriate for metforminInappropriate for metforminCan use in renal insufficiencyCan use in renal insufficiency
Troglitazone not advised as MonoRxTroglitazone not advised as MonoRx
? Thiazolidinediones? ThiazolidinedionesInsulin resistantInsulin resistant
Inappropriate for metforminInappropriate for metforminCan use in renal insufficiencyCan use in renal insufficiency
Troglitazone not advised as MonoRxTroglitazone not advised as MonoRx
SulfonylureaSulfonylureaLean patientLean patient
Initial Rx-early in disease Initial Rx-early in disease Use with caution in renal diseaseUse with caution in renal disease
SulfonylureaSulfonylureaLean patientLean patient
Initial Rx-early in disease Initial Rx-early in disease Use with caution in renal diseaseUse with caution in renal disease
Alt
ern
ate
Rx
Alt
ern
ate
Rx
Fir
st L
ine
Rx
Fir
st L
ine
Rx
IDCIDC
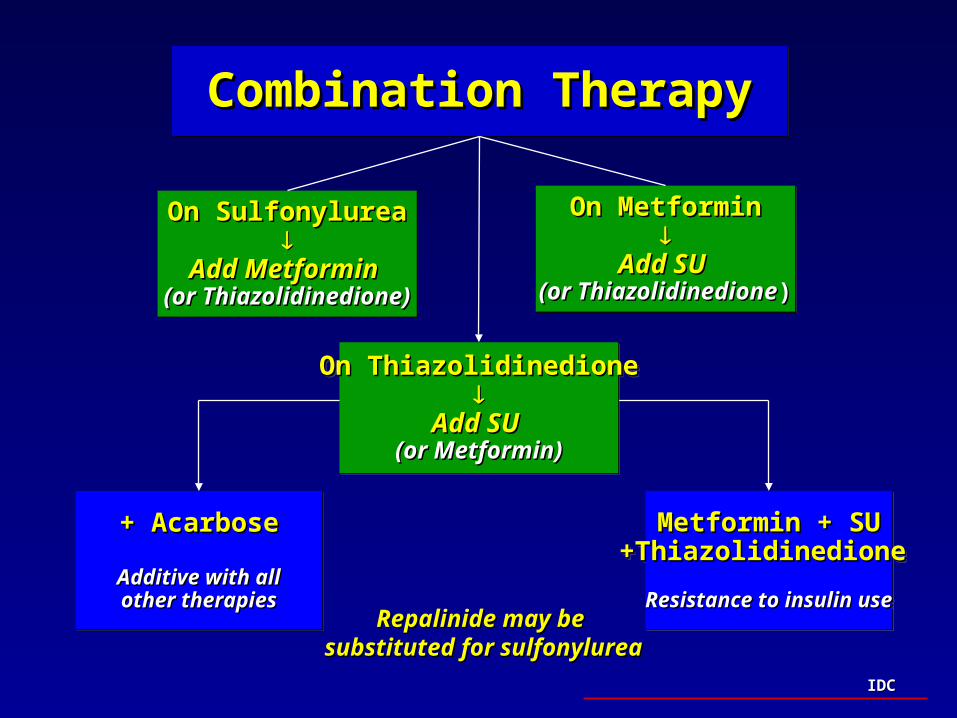
+ Acarbose+ Acarbose
Additive with allAdditive with allother therapiesother therapies
+ Acarbose+ Acarbose
Additive with allAdditive with allother therapiesother therapies
Metformin + SUMetformin + SU+Thiazolidinedione+Thiazolidinedione
Resistance to insulin useResistance to insulin use
Metformin + SUMetformin + SU+Thiazolidinedione+Thiazolidinedione
Resistance to insulin useResistance to insulin use
Combination TherapyCombination TherapyCombination TherapyCombination Therapy
On MetforminOn Metformin
Add SUAdd SU (or Thiazolidinedione(or Thiazolidinedione))
On MetforminOn Metformin
Add SUAdd SU (or Thiazolidinedione(or Thiazolidinedione))
On ThiazolidinedioneOn Thiazolidinedione
Add SUAdd SU (or Metformin)(or Metformin)
On ThiazolidinedioneOn Thiazolidinedione
Add SUAdd SU (or Metformin)(or Metformin)
On SulfonylureaOn Sulfonylurea
Add Metformin Add Metformin (or Thiazolidinedione)(or Thiazolidinedione)
On SulfonylureaOn Sulfonylurea
Add Metformin Add Metformin (or Thiazolidinedione)(or Thiazolidinedione)
Repalinide may be Repalinide may be substituted for sulfonylureasubstituted for sulfonylurea
IDCIDC
Insulin Therapy in Type 2 DiabetesInsulin Therapy in Type 2 Diabetes
Insulin Use in Type 2 DiabetesInsulin Use in Type 2 Diabetes
Combination Insulin - Oral Agent TherapyCombination Insulin - Oral Agent Therapy

IDCIDC
Rationale for Insulin Use in Type 2 DiabetesRationale for Insulin Use in Type 2 Diabetes
• Significant insulin deficiency occurs in up to Significant insulin deficiency occurs in up to 50% of those with Type 2 diabetes50% of those with Type 2 diabetes
• Insulin = most potent glucose lowering effect of Insulin = most potent glucose lowering effect of available agentsavailable agents
• Combination insulin - oral agent therapy may Combination insulin - oral agent therapy may be appropriate for many individualsbe appropriate for many individuals
Only insulin can replace insulinOnly insulin can replace insulin

IDCIDCADA. Medical Management of Non–Insulin Dependent ADA. Medical Management of Non–Insulin Dependent (Type II) Diabetes. 3rd ed. 1994: 40-49.(Type II) Diabetes. 3rd ed. 1994: 40-49.
Indications for Insulin UseIndications for Insulin UseType 2 DiabetesType 2 Diabetes
• Patients inadequately controlled by combination Patients inadequately controlled by combination oral agent therapyoral agent therapy
• Symptomatic hyperglycemia Symptomatic hyperglycemia • Assymptomatic hyperglycemia exceeding glucose Assymptomatic hyperglycemia exceeding glucose
lowering potential of oral therapieslowering potential of oral therapies• Hospitalized patient, acute physiologic stressHospitalized patient, acute physiologic stress
– InfectionInfection
– SurgerySurgery
• PregnancyPregnancy
IDCIDC
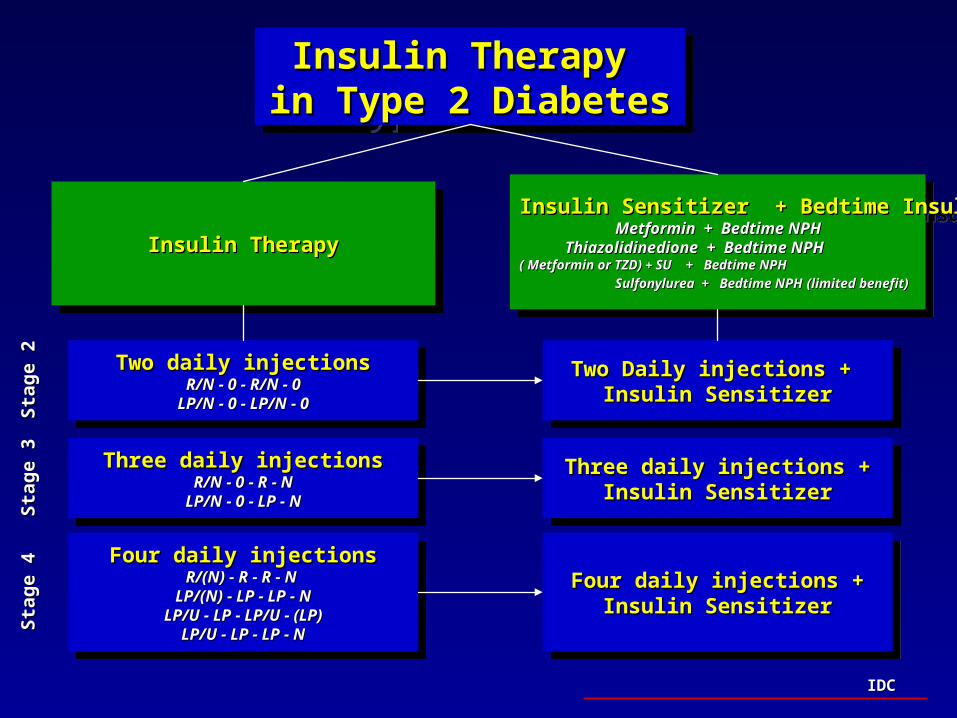
Insulin Therapy Insulin Therapy in Type 2 Diabetesin Type 2 DiabetesInsulin Therapy Insulin Therapy
in Type 2 Diabetesin Type 2 Diabetes
Insulin TherapyInsulin TherapyInsulin TherapyInsulin Therapy
Two daily injectionsTwo daily injectionsR/N - 0 - R/N - 0R/N - 0 - R/N - 0
LP/N - 0 - LP/N - 0LP/N - 0 - LP/N - 0
Two daily injectionsTwo daily injectionsR/N - 0 - R/N - 0R/N - 0 - R/N - 0
LP/N - 0 - LP/N - 0LP/N - 0 - LP/N - 0
Insulin Sensitizer + Bedtime Insulin Insulin Sensitizer + Bedtime Insulin Metformin + Bedtime NPH Metformin + Bedtime NPH
Thiazolidinedione + Bedtime NPH Thiazolidinedione + Bedtime NPH ( Metformin or TZD) ( Metformin or TZD) + + SU + Bedtime NPHSU + Bedtime NPH
Sulfonylurea + Bedtime NPHSulfonylurea + Bedtime NPH (limited benefit)(limited benefit)
Insulin Sensitizer + Bedtime Insulin Insulin Sensitizer + Bedtime Insulin Metformin + Bedtime NPH Metformin + Bedtime NPH
Thiazolidinedione + Bedtime NPH Thiazolidinedione + Bedtime NPH ( Metformin or TZD) ( Metformin or TZD) + + SU + Bedtime NPHSU + Bedtime NPH
Sulfonylurea + Bedtime NPHSulfonylurea + Bedtime NPH (limited benefit)(limited benefit)
Two Daily injections + Two Daily injections + Insulin SensitizerInsulin Sensitizer
Two Daily injections + Two Daily injections + Insulin SensitizerInsulin Sensitizer
Three daily injectionsThree daily injectionsR/N - 0 - R - NR/N - 0 - R - N
LP/N - 0 - LP - NLP/N - 0 - LP - N
Three daily injectionsThree daily injectionsR/N - 0 - R - NR/N - 0 - R - N
LP/N - 0 - LP - NLP/N - 0 - LP - N
Three daily injections +Three daily injections +Insulin SensitizerInsulin Sensitizer
Three daily injections +Three daily injections +Insulin SensitizerInsulin Sensitizer
Four daily injectionsFour daily injectionsR/(N) - R - R - N R/(N) - R - R - N
LP/(N) - LP - LP - NLP/(N) - LP - LP - NLP/U - LP - LP/U - (LP)LP/U - LP - LP/U - (LP)
LP/U - LP - LP - NLP/U - LP - LP - N
Four daily injectionsFour daily injectionsR/(N) - R - R - N R/(N) - R - R - N
LP/(N) - LP - LP - NLP/(N) - LP - LP - NLP/U - LP - LP/U - (LP)LP/U - LP - LP/U - (LP)
LP/U - LP - LP - NLP/U - LP - LP - N
Four daily injections +Four daily injections +Insulin SensitizerInsulin Sensitizer
Four daily injections +Four daily injections +Insulin SensitizerInsulin Sensitizer
Sta
ge 2
Sta
ge 2
Sta
ge 3
Sta
ge 3
Sta
ge 4
Sta
ge 4

IDCIDC
Insulin + Sulfonylurea Insulin + Sulfonylurea Combination Therapy in Type 2 DiabetesCombination Therapy in Type 2 Diabetes
• Limited rationale for useLimited rationale for use– Both are “insulin-providing” therapiesBoth are “insulin-providing” therapies
• Achieves modest improvement in glucose controlAchieves modest improvement in glucose control– Does not alter total insulin dosesDoes not alter total insulin doses
– Lowers A1c by maximum of 0.5%Lowers A1c by maximum of 0.5%**
• May be used during transition to insulin therapyMay be used during transition to insulin therapy– Rapid transition to multiple dose if control inadequateRapid transition to multiple dose if control inadequate
**Shank HL, et al. Shank HL, et al. DiabetesDiabetes. 1995;44:165-172.. 1995;44:165-172.
IDCIDC
Insulin + MetforminInsulin + MetforminCombination Therapy in Type 2 DiabetesCombination Therapy in Type 2 Diabetes
• Treats both insulin resistance and deficiencyTreats both insulin resistance and deficiency– Obese, insulin resistant patientObese, insulin resistant patient
– High dose insulin requirementsHigh dose insulin requirements
• Improves glucose controlImproves glucose control– Use with bedtime NPH insulin or multiple injectionsUse with bedtime NPH insulin or multiple injections
– Limits weight gain (anorectic effect)Limits weight gain (anorectic effect)
– Lowers LDL cholesterol (in combo with intensive insulin)Lowers LDL cholesterol (in combo with intensive insulin)
• May be used during transition to insulin therapyMay be used during transition to insulin therapy
Yki Järvinen H. Yki Järvinen H. Ann Intern MedAnn Intern Med 130:389-396, 1999 130:389-396, 1999
Aviles-Santa L. Aviles-Santa L. DiabetesDiabetes 47 (Suppl 1):A89. 1998 47 (Suppl 1):A89. 1998
Bergenstal R. Bergenstal R. Diabetes Diabetes 47(Suppl 1):A89. 347, 199847(Suppl 1):A89. 347, 1998

IDCIDC
Glucose-Lowering Potential or Effect of Glucose-Lowering Potential or Effect of Diabetes Therapies*Diabetes Therapies*
TreatmentTreatment Change in FPG Change in FPG HbA1c Reduction HbA1c ReductionSulfonylureasSulfonylureas 50-60 mg/dl50-60 mg/dl 1-2%1-2%MetforminMetformin 50-60 mg/dl50-60 mg/dl 1-2%1-2%CombinationCombination 63.5 mg/dl63.5 mg/dl 1.7%1.7%(Metformin/Sulfonylurea)(Metformin/Sulfonylurea)AcarboseAcarbose 15-30 mg/dl15-30 mg/dl 0.5-1%0.5-1%RepaglinideRepaglinide 63 mg/dl63 mg/dl 1.7%1.7%Troglitazone/InsulinTroglitazone/Insulin 49 mg/dl49 mg/dl 1.4%1.4%Troglitazone/SulfonylureaTroglitazone/Sulfonylurea 61-80 mg/dl61-80 mg/dl 1.8%1.8%Troglitazone AloneTroglitazone Alone 42 mg/dl42 mg/dl 1.4%1.4%InsulinInsulin UnlimitedUnlimited UnlimitedUnlimited**based on published studiesbased on published studies

IDCIDC
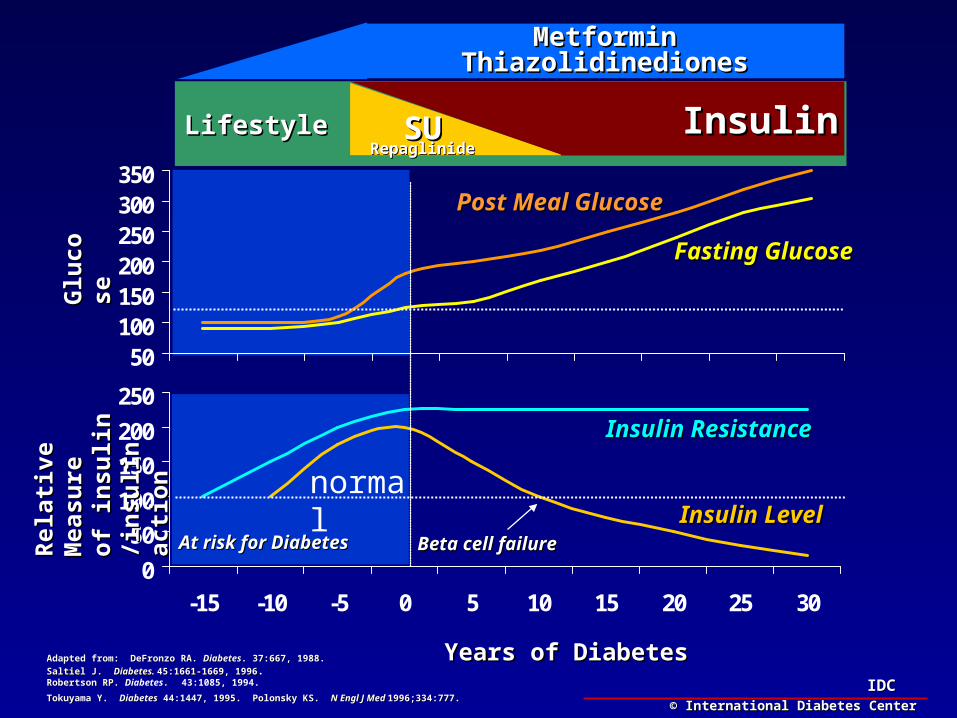
Natural History of Type 2 DiabetesNatural History of Type 2 Diabetes
0
50
100
150
200
250
-15 -10 -5 0 5 10 15 20 25 30
50100150200250300350
Years of DiabetesYears of Diabetes
Glu
cose
Glu
cose
Rel
ativ
e M
easu
reR
elat
ive
Mea
sure
of in
suli
n /i
nsu
lin
of
insu
lin
/ins
uli
n
acti
onac
tion
Insulin ResistanceInsulin Resistance
Insulin LevelInsulin Level
Fasting GlucoseFasting Glucose
Beta cell failureBeta cell failure
Post Meal GlucosePost Meal Glucose
© International Diabetes Center© International Diabetes Center
Adapted from: DeFronzo RA. Adapted from: DeFronzo RA. DiabetesDiabetes. 37:667, 1988. . 37:667, 1988.
Saltiel J. Saltiel J. Diabetes. Diabetes. 45:1661-1669, 199645:1661-1669, 1996. . Robertson RP. Robertson RP. Diabetes. 43:1085, 1994.
Tokuyama Y. Tokuyama Y. DiabetesDiabetes 44:1447, 1995. Polonsky KS. 44:1447, 1995. Polonsky KS. N Engl J Med N Engl J Med 1996;334:777.1996;334:777.
At risk for DiabetesAt risk for Diabetes
normal
IDCIDC
0
50
100
150
200
250
-15 -10 -5 0 5 10 15 20 25 30
50100150200250300350
Years of DiabetesYears of Diabetes
Glu
cose
Glu
cose
Rel
ativ
e M
easu
reR
elat
ive
Mea
sure
of in
suli
n /i
nsu
lin
of
insu
lin
/ins
uli
n
acti
onac
tion
Insulin ResistanceInsulin Resistance
Insulin LevelInsulin Level
Fasting GlucoseFasting Glucose
Beta cell failureBeta cell failure
Post Meal GlucosePost Meal Glucose
© International Diabetes Center© International Diabetes Center
Adapted from: DeFronzo RA. Adapted from: DeFronzo RA. DiabetesDiabetes. 37:667, 1988. . 37:667, 1988.
Saltiel J. Saltiel J. Diabetes. Diabetes. 45:1661-1669, 199645:1661-1669, 1996. . Robertson RP. Robertson RP. Diabetes. 43:1085, 1994.
Tokuyama Y. Tokuyama Y. DiabetesDiabetes 44:1447, 1995. Polonsky KS. 44:1447, 1995. Polonsky KS. N Engl J Med N Engl J Med 1996;334:777.1996;334:777.
At risk for DiabetesAt risk for Diabetes
normal
LifestyleLifestyle SUSURepaglinideRepaglinide
InsulinInsulin
MetforminMetforminThiazolidinedionesThiazolidinediones
IDCIDC
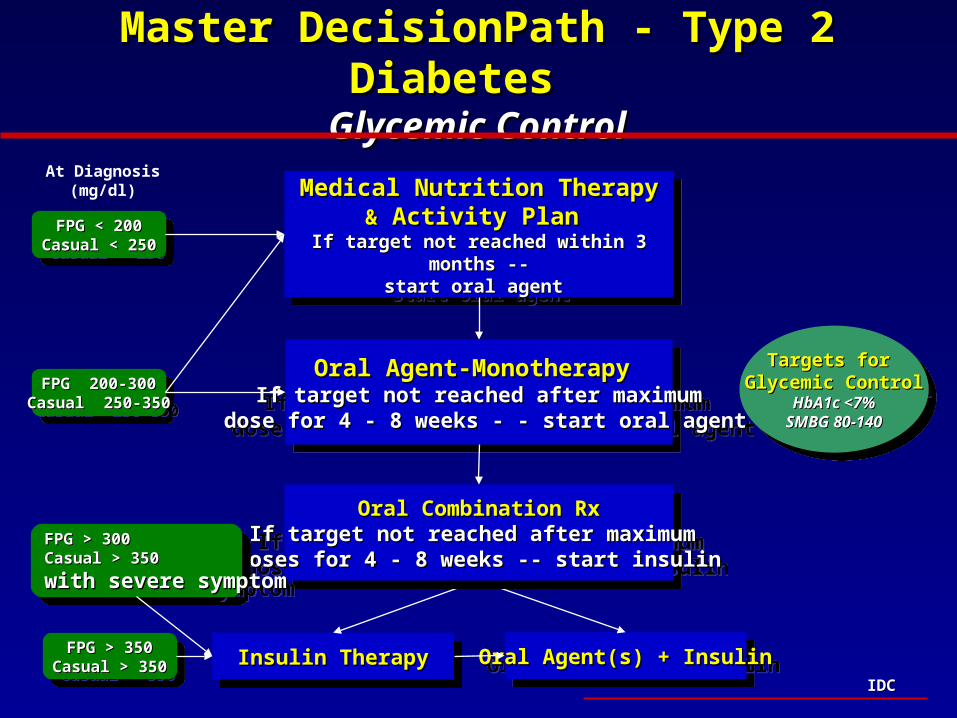
Master DecisionPath - Type 2 Diabetes Master DecisionPath - Type 2 Diabetes Glycemic ControlGlycemic Control
Medical Nutrition TherapyMedical Nutrition Therapy&& Activity Plan Activity Plan
If target not reached within 3 months --If target not reached within 3 months --start oral agent start oral agent
Medical Nutrition TherapyMedical Nutrition Therapy&& Activity Plan Activity Plan
If target not reached within 3 months --If target not reached within 3 months --start oral agent start oral agent
Oral Agent-Monotherapy Oral Agent-Monotherapy If target not reached after maximumIf target not reached after maximum
dose for 4 - 8 weeks - - start oral agentdose for 4 - 8 weeks - - start oral agent
Oral Agent-Monotherapy Oral Agent-Monotherapy If target not reached after maximumIf target not reached after maximum
dose for 4 - 8 weeks - - start oral agentdose for 4 - 8 weeks - - start oral agent
Insulin TherapyInsulin TherapyInsulin TherapyInsulin Therapy Oral Agent(s) + InsulinOral Agent(s) + InsulinOral Agent(s) + InsulinOral Agent(s) + Insulin
Oral Combination RxOral Combination RxIf target not reached after maximum If target not reached after maximum doses for 4 - 8 weeks -- start insulindoses for 4 - 8 weeks -- start insulin
Oral Combination RxOral Combination RxIf target not reached after maximum If target not reached after maximum doses for 4 - 8 weeks -- start insulindoses for 4 - 8 weeks -- start insulin
FPG < 200FPG < 200Casual < 250Casual < 250
FPG < 200FPG < 200Casual < 250Casual < 250
FPG 200-300FPG 200-300Casual 250-350Casual 250-350
FPG 200-300FPG 200-300Casual 250-350Casual 250-350
FPG > 350FPG > 350Casual > 350Casual > 350
FPG > 350FPG > 350Casual > 350Casual > 350
At Diagnosis(mg/dl)
Targets for Targets for Glycemic ControlGlycemic Control
HbA1c <7%HbA1c <7%SMBG 80-140SMBG 80-140
Targets for Targets for Glycemic ControlGlycemic Control
HbA1c <7%HbA1c <7%SMBG 80-140SMBG 80-140
FPG > 300FPG > 300Casual > 350Casual > 350
with severe symptomwith severe symptom
FPG > 300FPG > 300Casual > 350Casual > 350
with severe symptomwith severe symptom
IDCIDC
Choosing the Best TherapyChoosing the Best TherapyPre-Pregnancy and GDMPre-Pregnancy and GDM
• Food plan and exercise (medical nutrition) Food plan and exercise (medical nutrition) – lower BG by up to 100 mg/dL when used as a lower BG by up to 100 mg/dL when used as a
monotherapymonotherapy
• Oral agents pass through the placental barrier and Oral agents pass through the placental barrier and are contraindicated in pregnancyare contraindicated in pregnancy
• No limit to the blood glucose lowering potential of No limit to the blood glucose lowering potential of insulin insulin
Therefore, food plan alone or in combination with Therefore, food plan alone or in combination with insulin is necessary to achieve glycemic controlinsulin is necessary to achieve glycemic control

IDCIDC
Master DecisionPath - Type 2 Diabetes in Master DecisionPath - Type 2 Diabetes in Pregnancy and GDM Pregnancy and GDM
Glycemic ControlGlycemic Control
Medical Nutrition TherapyMedical Nutrition Therapy&& Activity Plan Activity Plan
If target not reached within 1 week If target not reached within 1 week start insulin therapy start insulin therapy
Medical Nutrition TherapyMedical Nutrition Therapy&& Activity Plan Activity Plan
If target not reached within 1 week If target not reached within 1 week start insulin therapy start insulin therapy
Insulin Stage 2 *Insulin Stage 2 *(R/N-0-R/N-0)(R/N-0-R/N-0)
If target not reached after 1 week If target not reached after 1 week or persistent fasting hyperglycemia, or persistent fasting hyperglycemia,
start 3Astart 3A
Insulin Stage 2 *Insulin Stage 2 *(R/N-0-R/N-0)(R/N-0-R/N-0)
If target not reached after 1 week If target not reached after 1 week or persistent fasting hyperglycemia, or persistent fasting hyperglycemia,
start 3Astart 3A
FPG <95FPG <95Casual <120Casual <120
FPG <95FPG <95Casual <120Casual <120
FPG FPG >>9595Casual Casual >> 120 120
FPG FPG >>9595Casual Casual >> 120 120
At Diagnosis(mg/dl)
Targets for Targets for Glycemic ControlGlycemic Control
SMBG 70-110SMBG 70-110
Targets for Targets for Glycemic ControlGlycemic Control
SMBG 70-110SMBG 70-110
Insulin Stage 3A Insulin Stage 3A (R/N-0-R-N)(R/N-0-R-N)
Increase insulin dose at 10%/3days untilIncrease insulin dose at 10%/3days untiltarget is reached target is reached
Insulin Stage 3A Insulin Stage 3A (R/N-0-R-N)(R/N-0-R-N)
Increase insulin dose at 10%/3days untilIncrease insulin dose at 10%/3days untiltarget is reached target is reached
IDCIDC
Medical Nutrition InterventionMedical Nutrition Intervention
• As a means of lowering blood As a means of lowering blood glucose glucose
• As a means of managing weightAs a means of managing weight
IDCIDC
Balancing EnergyBalancing Energy
EnergyEnergyInputInput
EnergyEnergyOutputOutput
ActivityActivityExerciseExerciseBasal metabolicBasal metabolicraterate
FoodFoodHepatic glucose Hepatic glucose output output
Cultural, social, economic, Cultural, social, economic, religious, behavioral factorsreligious, behavioral factors
IDCIDC
0
10
20
30
40
50
0 2 4 6 8 10 12 14 16 18 20 22 24
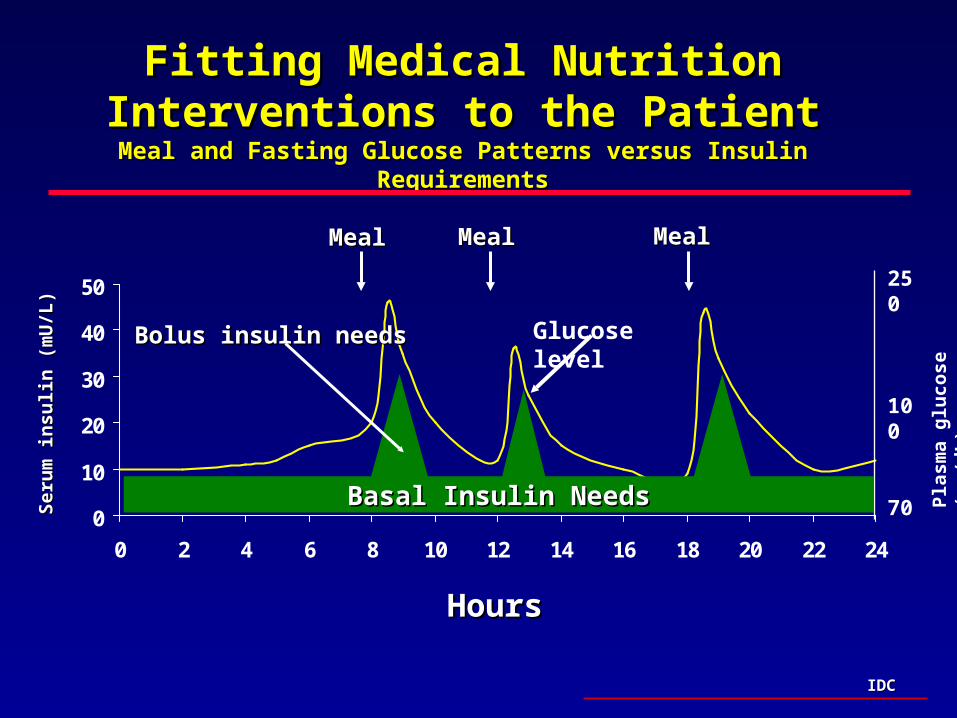
Fitting Medical Nutrition Interventions to Fitting Medical Nutrition Interventions to the Patientthe Patient
Meal and Fasting Glucose Patterns versus Insulin RequirementsMeal and Fasting Glucose Patterns versus Insulin Requirements
Ser
um
insu
lin
(m
U/L
)S
eru
m in
suli
n (
mU
/L)
HoursHours
MealMeal MealMeal MealMeal
Basal Insulin NeedsBasal Insulin Needs
Bolus insulin needsBolus insulin needs Glucose level
250
100
70
Pla
sma
glu
cose
(m
g/d
L)
IDCIDC
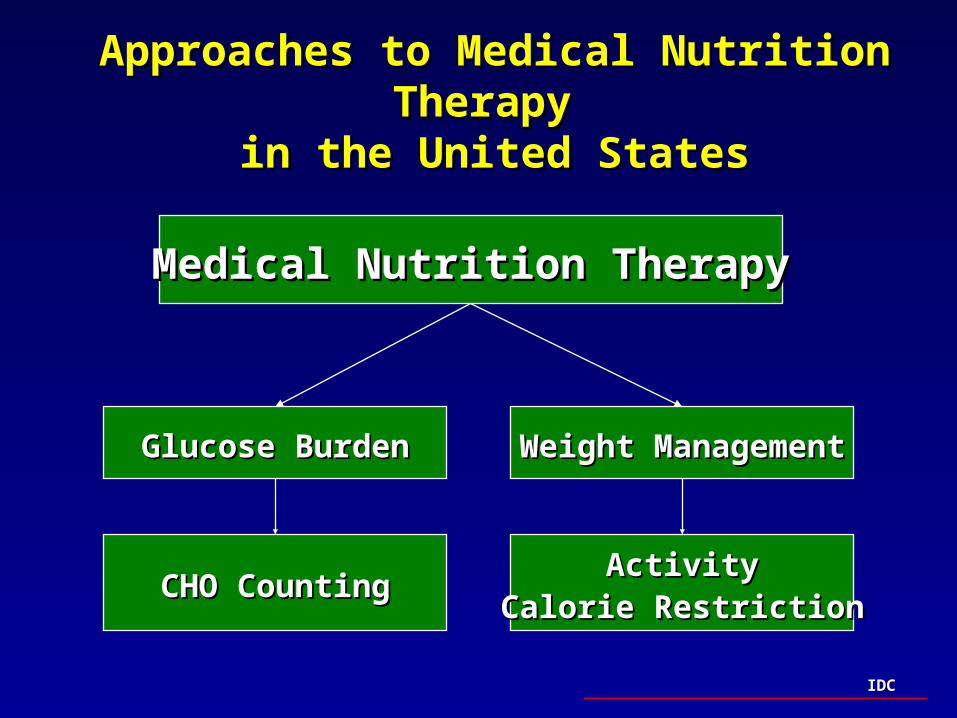
Approaches to Medical Nutrition Therapy Approaches to Medical Nutrition Therapy in the United Statesin the United States
Glucose BurdenGlucose Burden Weight ManagementWeight Management
Medical Nutrition TherapyMedical Nutrition Therapy
CHO CountingCHO CountingActivityActivity
Calorie RestrictionCalorie Restriction
IDCIDC
Focus on Blood Glucose Control not Focus on Blood Glucose Control not Weight LossWeight Loss
• Improving blood glucose control is a higher Improving blood glucose control is a higher priority than weight losspriority than weight loss
• Weight loss may be more important for the Weight loss may be more important for the prevention of a chronic disease, including type prevention of a chronic disease, including type 2 diabetes, than for treatment2 diabetes, than for treatment
• Once a chronic disease develops, treatment Once a chronic disease develops, treatment should focus on correcting metabolic should focus on correcting metabolic abnormalitiesabnormalities
IDCIDC
Carbohydrate CountingCarbohydrate Counting
• Sources of carbohydrate are simple and complex Sources of carbohydrate are simple and complex sugars and dairy products sugars and dairy products
• Carbohydrates are the principal dietary source of Carbohydrates are the principal dietary source of glucoseglucose
• Emphasizes total amount of carbohydrate (not calories Emphasizes total amount of carbohydrate (not calories derived from protein and fat)derived from protein and fat)
• One carbohydrate serving = 15 grams (60 kcals)One carbohydrate serving = 15 grams (60 kcals)
• Total carbohydrate intake equally divided among all Total carbohydrate intake equally divided among all meals (45-60 grams/meal) and snacks (15-30 meals (45-60 grams/meal) and snacks (15-30 grams/snack)grams/snack)
IDCIDC
Activity/FitnessActivity/Fitness
EnergyEnergyInputInput EnergyEnergy
OutputOutput
ActivityActivityExerciseExerciseBasal metabolicBasal metabolicraterate
FoodFoodEndogenousEndogenousglucose outputglucose output
IDCIDC
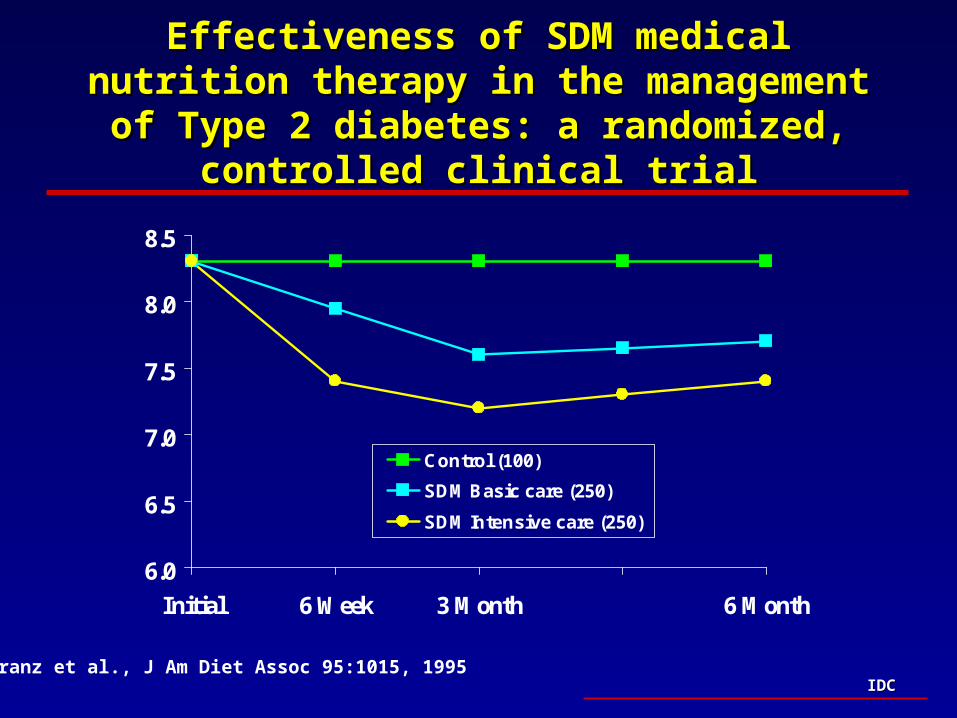
Effectiveness of SDM medical nutrition therapy Effectiveness of SDM medical nutrition therapy in the management of Type 2 diabetes: a in the management of Type 2 diabetes: a
randomized, controlled clinical trialrandomized, controlled clinical trial
6.0
6.5
7.0
7.5
8.0
8.5
Initial 6 Week 3 Month 6 Month
Control (100)
SDM Basic care (250)
SDM Intensive care (250)
Franz et al., J Am Diet Assoc 95:1015, 1995
IDCIDC
New Therapeutic InterventionsNew Therapeutic Interventionsin Diabetes Managementin Diabetes Management
• Intensive glycemic control in diabetesIntensive glycemic control in diabetes– ESSENTIAL to reduce risk of microvascular diseaseESSENTIAL to reduce risk of microvascular disease
– DOES NOT increase the risk of macrovascular diseaseDOES NOT increase the risk of macrovascular disease
• Therapies must be customized to fit both the patient and the Therapies must be customized to fit both the patient and the care communitycare community– Staged approach to care to achieve appropriate targetsStaged approach to care to achieve appropriate targets
• Multiple therapeutic optionsMultiple therapeutic options– Insulin therapiesInsulin therapies– Oral therapies for Type 2 diabetesOral therapies for Type 2 diabetes
• Use of Medical Nutrition therapyUse of Medical Nutrition therapy – Glucose controlGlucose control– Weight managementWeight management





























