Embed Size (px)
Citation preview

ID Case Conference
Yvonne L. Carter, MD
11 June 2008
Headaches and Fever 41yo female physician with a 3-day h/o
headaches and fever Began 3 days ago, fever and HA controlled
with Tylenol…after which she feels better, but develops uncontrollable chills ~1 hour after dose
Denies neck stiffness, visual changes, or other neurological symptoms
HA currently 6/10. Pt also reports myalgias, but otherwise feels well, and would like to go home.

History
Pt is a Tropical Medicine Physician. She works in the Rep. Of Congo, and had
been there for four months Had received travelers vaccinations
– Typhoid, Rabies, Japanese Encephalitis, Yellow Fever

PMH– Hepatitis A (remote)– Appendicitis, with
Appendectomy– HIV negative
Meds– Prn Tylenol
Allergies– PCN - rash
SocHx– Married– Lives in Chapel Hill – No pets– Travel: recent travel
to The Republic of Congo, Africa
– Denies tobacco, Etoh, or illicits
– No ill contacts

Physical Examination
VS: T 36.3, P 103, BP 115/76, R 20, Pox 100% on RA Gen: WD, WN thin CF who appears uncomfortable, holding
head, speaking softly HEENT: NCAT, Perrla, Eomi, Sclera anicteric, conj pink, MMM,
OP clear, Neck supple, No LAD. CV: Tachycardic, II/VI SEM at apex w/o radiation Pulm: CTA b/l, no w/r/r Abd: Soft, ND, NT, no organomegaly Ext: No c/c/e Neuro: Normal exam, no focal deficits Skin: No rashes

Laboratory Data
133
4.1
101
23
8
0.879
3.235.2
51
8.5
1.9
1.1
152
2.0252
151
2.2
4.4


Discussion

What I left out… Mefloquine had caused dizziness in the past,
therefore the pt did not take prophylaxis Used bed nets and insect repellants
throughout the trip, with success… Until the last week of her trip, she was bitten
on the Lower Exts, Abdomen, and Back Developed a “tingling sensation” at the site of
the bites on the trunk…locals suggested this was indicative of malaria transmission
Pt was given a dose of an “untraditional” treatment for malaria by local doctors


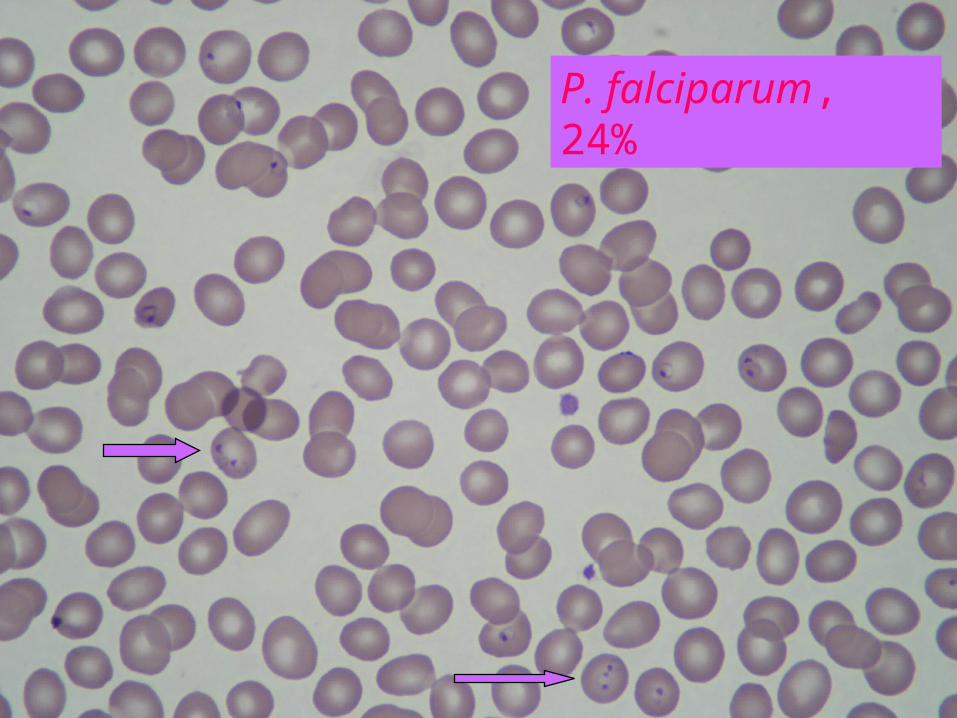
P. falciparum, 24%


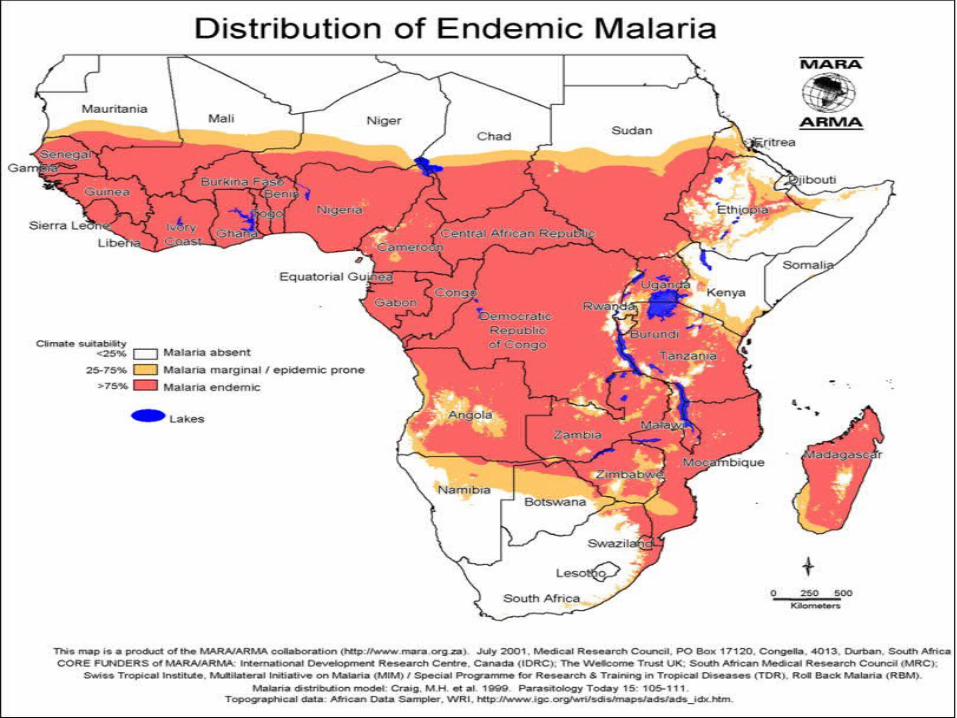


Sub-Saharan Africa (Cases per 1000 patients with syndrome)
Systemic Febrile Illness = 718– Malaria – 622– Dengue – 7– Mononucleosis (EBV/CMV) – 10– Rickettsial infection – 56– Salmonella typhi or S. paratyphi – 7
No specific cause reported = 282
NEJM 354(2):119-130.

Copyright restrictions may apply.
Griffith, K. S. et al. JAMA 2007;297:2264-2277.
Plasmodium Life Cycle

Copyright restrictions may apply. Griffith, K. S. et al. JAMA 2007;297:2264-2277.
Malaria Treatment Algorithm

Severe malaria
Severe malaria if… Parasitemia of >5% Altered consciousness Oliguria Jaundice Severe normocytic
anemia Hypoglycemia Organ failure
Seizures Acute renal failure Fluid and electrolyte
abnormalities Metabolic acidosis Acute respiratory distress
syndrome Circulatory collapse or shock Hemoglobinuria Bleeding


Exchange transfusion Rx
Recommended in P. falciparum infection when… – Parasitemia is greater than 10%– Patients with coma, renal failure or ARDS
regardless of the level of parasitemia. Should be combined with drug therapy Should be continued until the level of
parasitemia is <5% Does not enhance survival

Exchange Transfusion(Meta-Analysis)
Meta-analysis No greater survival rate among patients who
received exchange transfusion compared to antimalarials alone
Patients who received exchange transfusions had higher degrees of parasitemia and more severe disease – not comparable to those receiving medications alone
No RCT has been performed
Clin Infect Dis 2002;34(9):1192-8.


Hospital Course
Pt treated with IV Quinidine and Doxycycline, Exchange Transfusion via Right Subclavian
IV Quinidine initiated ~9:30pm, and bolused over four hours. Pt developed nausea, vomiting, and profuse watery diarrhea.
Exchange transfusion began at ~11pm, pt developed asymptomatic hypotension (SBP 80s), and exchange prematurely discontinued at 7/8 units complete.

Hospital Course, cont.
Pt became bradycardic, with a pulse in 60s. QTc prolonged to 541ms, after IV Quinidine
bolus finished. 1am: Parasitemia 9% 9am: Parasitemia 6%, QTc 510

Hospital Course, cont.
134
4.2
102
22
7
0.6208
2.830.1
33
6.3
3.6
2.2

Discharge
Recommended switch to po Quinine and Doxycycline…Pt refused
Pt discharged on Malarone (Atovaquone/Plaguanil) to complete three day course.
Pt discharged on hospital day #2, with a parasitemia <1%

BUT…
Pt called UNC two days later, complaining of SOB, and was instructed to walk in to the ID Clinic
Orthopnea, Pleuritic CP, and facial swelling
Temp 37.0, BP 105/62, P 89, RR 16 Pox 85%
ABG: 7.49/34/54/89% on RA

136
3.6
102
26
9
0.790
5.731.7
11844
1.5152
152
2.7
LDH 774
Peripheral Smear: NO PARASITES Detected
D-dimer 914
UA Neg




Diagnostic Studies
Cardiac enzymes negative CTA negative for PE TTE Normal Bronchoscopy:
– No gross abnormalities– Gram Stain Negative, Culture Negative

Bronchoscopy
BAL Fluid– Color: Pink– Appearance: Cloudy– TNC: 1100
• Neut 2• Lymph 30• Mono 57
– RBC 6950– Macrophages
present
PCP DF : Neg CMV PCR: Neg Legionella: Neg Cx: Negative Viral Cx: Negative Fungal Cx: Negative C. pna Cx: Negative Mycoplasma:
Negative AFBs: Negative

Differential Diagnosis – Pulmonary Edema
Drug-Induced Alveolitis BOOP (Cryptogenic Organizing Pna) Acute Lung Injury due to Malaria ARDS Atypical Pneumonia Diffuse Aspiration

Discharge
Pt refused to stay longer, and was discharged on Levaquin, for a total course of 14 days.