Embed Size (px)
DESCRIPTION
ICD-10 Update: Analytic Community Involvement - Critical to Implementation Success. BUMED M3 Medical Operations. BLUF. - PowerPoint PPT Presentation
Citation preview
ICD-10 Update: Analytic Community
Involvement - Critical to Implementation Success
BUMED M3 Medical Operations
BLUF The Centers for Medicare and Medicaid Services (CMS) has mandated
International Classification of Diseases Revision 10 (ICD-10) diagnosis and procedure coding standards for all discharges effective 1 October 2014 (proposed). Conforming to these new standards will require careful planning, coordination, and execution.
Key operational and technology areas potentially impacted include:o End-to-end operations including ordering/scheduling, clinical
documentation by providers, diagnosis coding (inpatient/outpatient/APV), procedure coding (inpatient), and third party billing and collections
o Military Health System (MHS) funding mechanisms and resulting business planning
o Any information system that contains clinical data (including Navy-specific systems)
o Reporting and statistical databases (including ability to trend data)
Anyone who generates or uses clinical data for analytics will need to be trained on ICD-10 and update their processes as appropriate
The infrastructure is in place to ensure people will be trained, processes will be optimized, technology will be improved, and policy will be updated to meet ICD-10 standards.
2
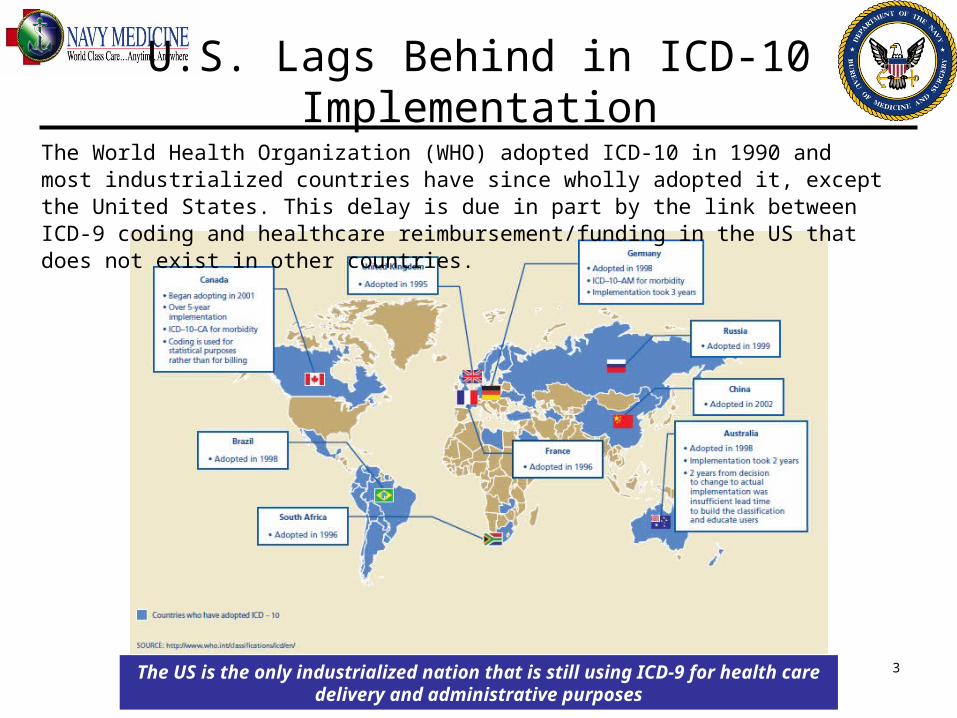
U.S. Lags Behind in ICD-10 Implementation
The US is the only industrialized nation that is still using ICD-9 for health care delivery and administrative purposes
The World Health Organization (WHO) adopted ICD-10 in 1990 and most industrialized countries have since wholly adopted it, except the United States. This delay is due in part by the link between ICD-9 coding and healthcare reimbursement/funding in the US that does not exist in other countries.
3
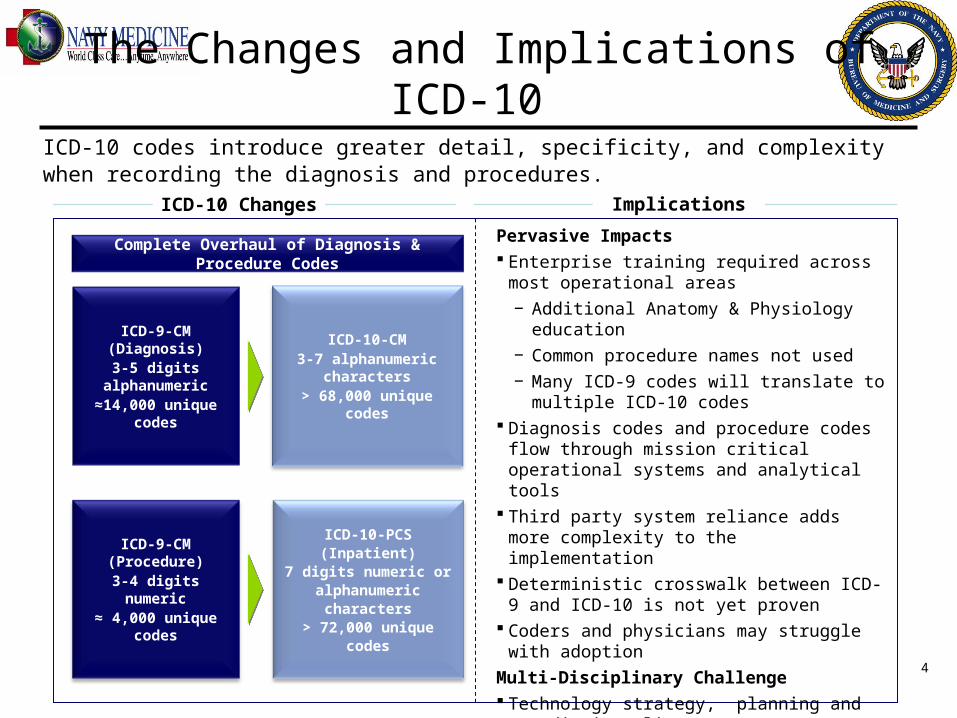
The Changes and Implications of ICD-10
ImplicationsICD-10 Changes
Pervasive Impacts Enterprise training required across most
operational areas− Additional Anatomy & Physiology
education− Common procedure names not used− Many ICD-9 codes will translate to
multiple ICD-10 codes Diagnosis codes and procedure codes flow
through mission critical operational systems and analytical tools
Third party system reliance adds more complexity to the implementation
Deterministic crosswalk between ICD-9 and ICD-10 is not yet proven
Coders and physicians may struggle with adoption
Multi-Disciplinary Challenge Technology strategy, planning and
remediation alignment Workflow reengineering, training and
change management is essential
ICD-10 codes introduce greater detail, specificity, and complexity when recording the diagnosis and procedures.
Complete Overhaul of Diagnosis & Procedure Codes
ICD-9-CM (Diagnosis)3-5 digits
alphanumeric≈14,000 unique
codes
ICD-9-CM (Procedure)
3-4 digits numeric
≈ 4,000 unique codes
ICD-10-CM3-7 alphanumeric
characters> 68,000 unique
codes
ICD-10-PCS (Inpatient)
7 digits numeric or alphanumeric
characters> 72,000 unique
codes4
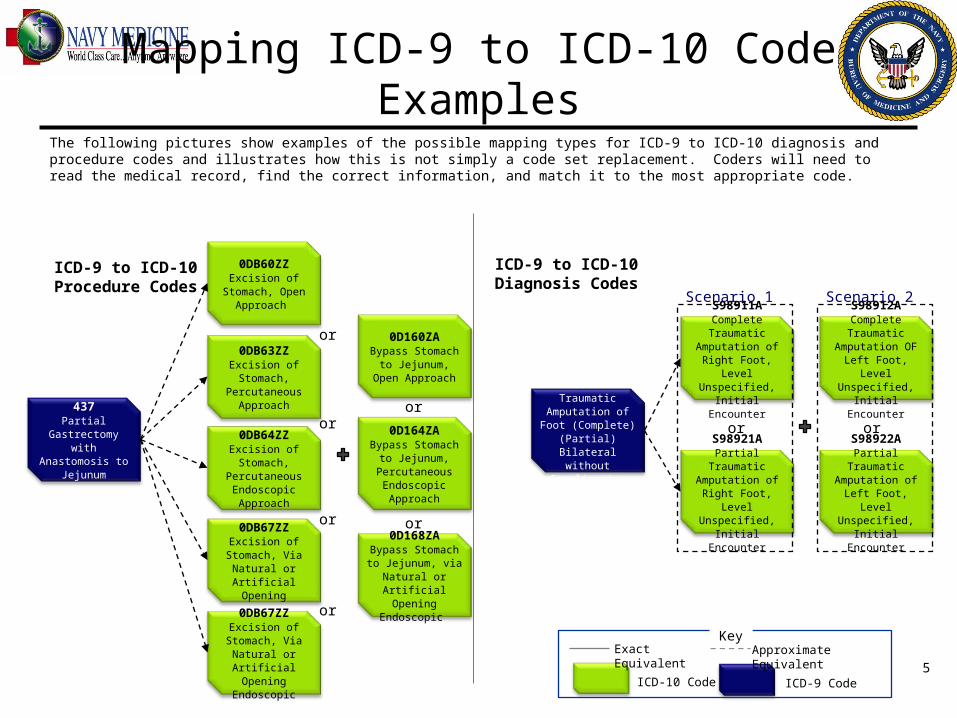
Mapping ICD-9 to ICD-10 Code Examples
The following pictures show examples of the possible mapping types for ICD-9 to ICD-10 diagnosis and procedure codes and illustrates how this is not simply a code set replacement. Coders will need to read the medical record, find the correct information, and match it to the most appropriate code.
ICD-9 to ICD-10Procedure Codes
ICD-9 to ICD-10 Diagnosis Codes
ICD-9 CodeICD-10 Code
Exact Equivalent
Approximate Equivalent
Key
437Partial
Gastrectomy with Anastomosis to
Jejunum
0DB60ZZExcision of
Stomach, Open Approach
0DB63ZZExcision of Stomach,
Percutaneous Approach
0DB64ZZExcision of Stomach,
Percutaneous Endoscopic Approach
0DB67ZZExcision of
Stomach, Via Natural or
Artificial Opening
0DB67ZZExcision of
Stomach, Via Natural or
Artificial Opening Endoscopic
0D160ZABypass Stomach to Jejunum, Open
Approach
0D164ZABypass Stomach
to Jejunum, Percutaneous Endoscopic Approach
0D168ZABypass Stomach to Jejunum, via
Natural or Artificial Opening
Endoscopic
8962Traumatic
Amputation of Foot (Complete) (Partial) Bilateral
without Complication
S98911AComplete Traumatic
Amputation of Right Foot, Level
Unspecified, Initial Encounter
S98921APartial Traumatic
Amputation of Right Foot, Level
Unspecified, Initial Encounter
S98912AComplete Traumatic
Amputation OF Left Foot, Level
Unspecified, Initial Encounter
S98922APartial Traumatic
Amputation of Left Foot, Level
Unspecified, Initial Encounter
Scenario 1 Scenario 2
ororor
or
or
or
or
or
5
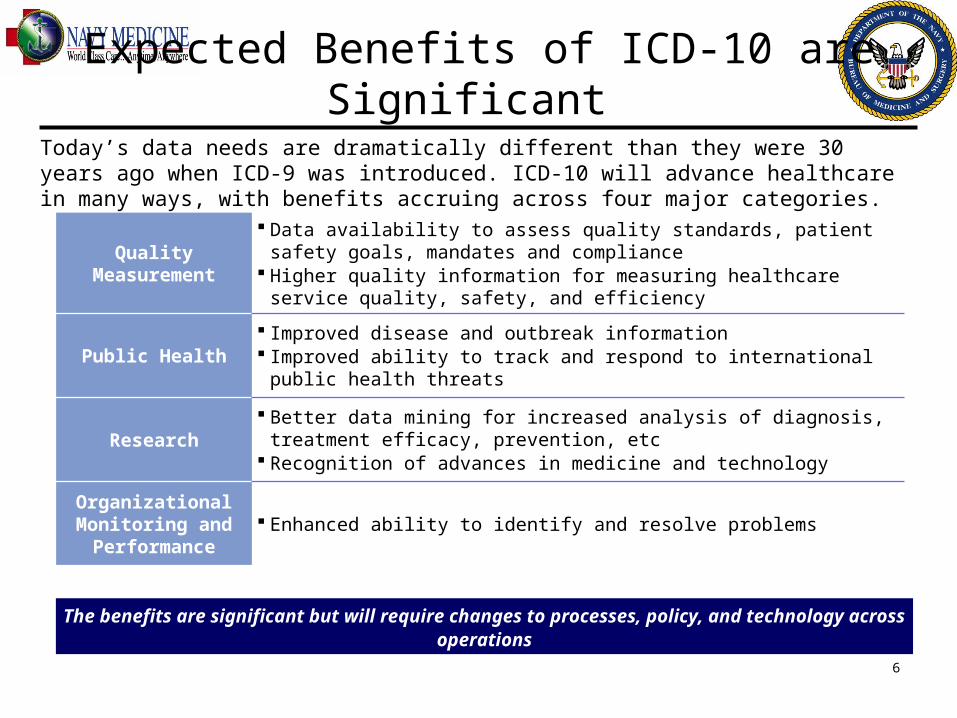
Expected Benefits of ICD-10 are Significant
Today’s data needs are dramatically different than they were 30 years ago when ICD-9 was introduced. ICD-10 will advance healthcare in many ways, with benefits accruing across four major categories.
Quality Measurement
Data availability to assess quality standards, patient safety goals, mandates and compliance
Higher quality information for measuring healthcare service quality, safety, and efficiency
Public Health Improved disease and outbreak information Improved ability to track and respond to international public
health threats
Research Better data mining for increased analysis of diagnosis, treatment
efficacy, prevention, etc Recognition of advances in medicine and technology
Organizational Monitoring and
Performance Enhanced ability to identify and resolve problems
The benefits are significant but will require changes to processes, policy, and technology across operations
6
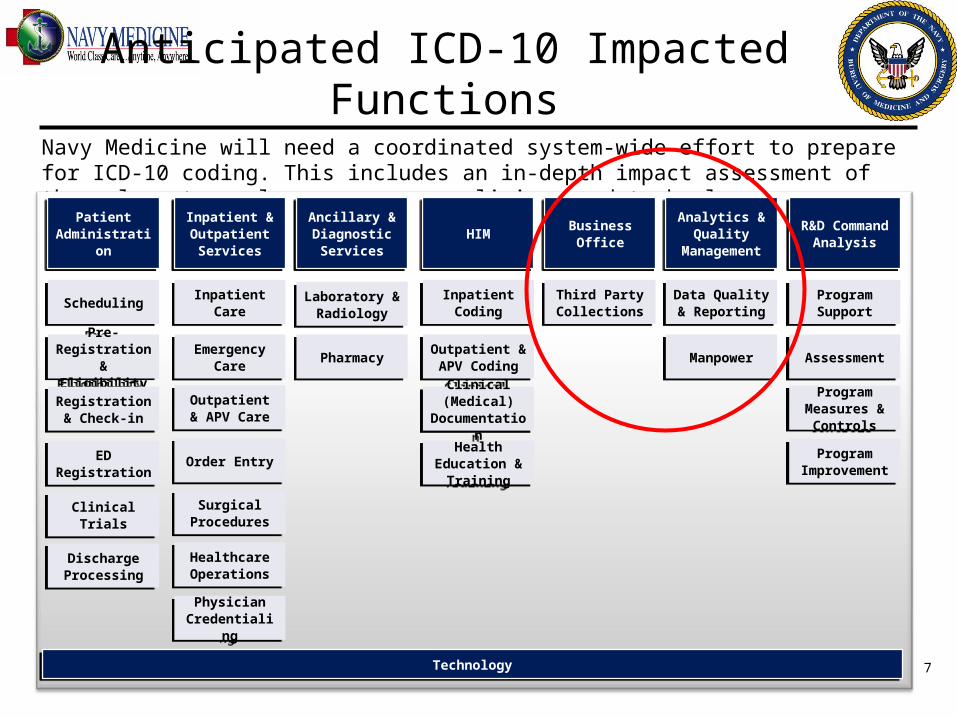
Anticipated ICD-10 Impacted Functions
Navy Medicine will need a coordinated system-wide effort to prepare for ICD-10 coding. This includes an in-depth impact assessment of the relevant people, processes, policies, and technology.
TechnologyTechnology
Discharge Processing
Discharge Processing
Laboratory & Radiology
Laboratory & Radiology
Physician Credentialin
g
Physician Credentialin
g
Health Education &
Training
Health Education &
Training
Patient Administrati
on
Patient Administrati
on
Inpatient & Outpatient Services
Inpatient & Outpatient Services
Business Office
Business Office
Analytics & Quality
Management
Analytics & Quality
Management
Ancillary & Diagnostic Services
Ancillary & Diagnostic Services
HIMHIMR&D
Command Analysis
R&D Command Analysis
Pre-Registration & Eligibility
Pre-Registration & Eligibility
Registration & Check-in
Registration & Check-in
ED Registration
ED Registration
SchedulingScheduling
Emergency Care
Emergency Care
Outpatient & APV Care
Outpatient & APV Care
Order EntryOrder Entry
Surgical Procedures
Surgical Procedures
Inpatient Care
Inpatient Care
Healthcare Operations
Healthcare Operations
Inpatient Coding
Inpatient Coding
Outpatient & APV Coding
Outpatient & APV Coding
Clinical (Medical)
Documentation
Clinical (Medical)
Documentation
Third Party Collections
Third Party Collections
Data Quality & Reporting
Data Quality & Reporting
ManpowerManpower
Program Support
Program Support
AssessmentAssessment
Program Measures &
Controls
Program Measures &
Controls
Program Improvemen
t
Program Improvemen
t
Clinical Trials
Clinical Trials
PharmacyPharmacy
7
8
Impacts to Data and Analytics• Explosion in data – providers and coders will be choosing from EIGHT times as
many codes and may require more codes to be used in parallel to capture the full set of information
• Impact to accuracy – initial decreases in coding accuracy can be anticipated as providers and coders adjust to the new coding methodology
• Changes in queries – Many reports are used in data analytics today that rely on queries including ICD data. These will need to be updated.
• Trending – comparing “apples to oranges” after the change will be a challenge; ICD-9 and ICD-10 data will initially be mixed in the M2 depending on service date
• Revenue modeling – third party reimbursement and PPS revenue will be impacted if less specific codes are used
• Research databases / Quality Measures – any reporting on disease incidence and other clinical measures will be impacted (including standalone Navy systems)
• Mapping – TMA has adopted CMS back-mapping between ICD-9 and ICD-10; BUMED is investigating appropriate use of mapping for M2
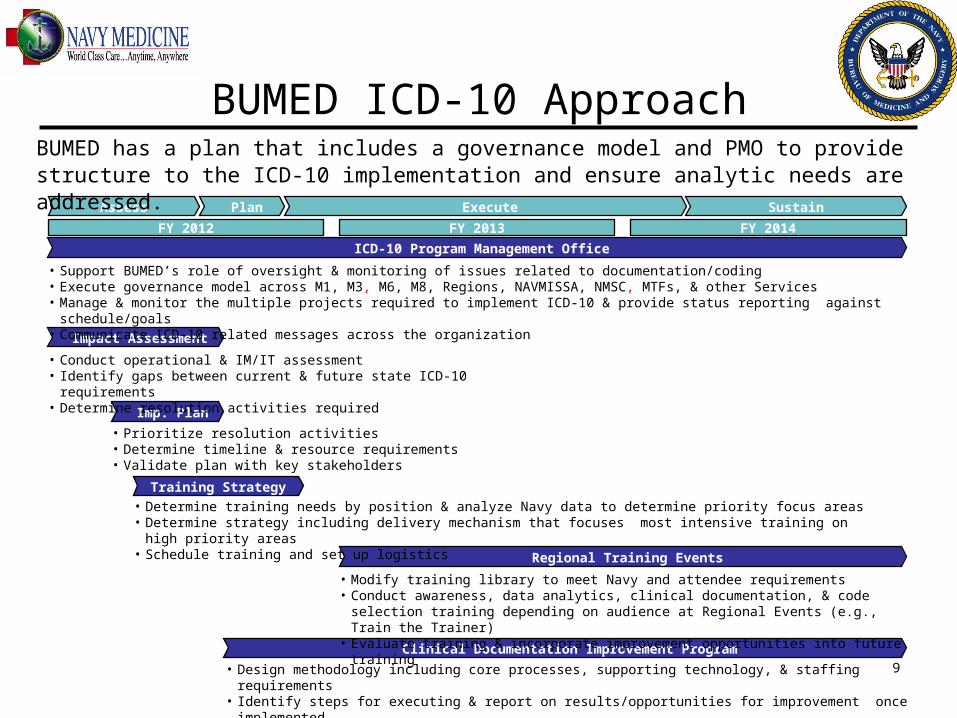
BUMED ICD-10 Approach
Assess Plan Execute Sustain
FY 2012 FY 2013 FY 2014
Impact Assessment
Imp. Plan
Training Strategy
Regional Training Events
Clinical Documentation Improvement Program
• Conduct operational & IM/IT assessment• Identify gaps between current & future state ICD-10 requirements• Determine resolution activities required
• Prioritize resolution activities• Determine timeline & resource requirements• Validate plan with key stakeholders
• Determine training needs by position & analyze Navy data to determine priority focus areas• Determine strategy including delivery mechanism that focuses most intensive training on high priority
areas• Schedule training and set up logistics
• Modify training library to meet Navy and attendee requirements• Conduct awareness, data analytics, clinical documentation, & code selection
training depending on audience at Regional Events (e.g., Train the Trainer)• Evaluate training & incorporate improvement opportunities into future training
• Design methodology including core processes, supporting technology, & staffing requirements• Identify steps for executing & report on results/opportunities for improvement once implemented
ICD-10 Program Management Office
• Support BUMED’s role of oversight & monitoring of issues related to documentation/coding• Execute governance model across M1, M3, M6, M8, Regions, NAVMISSA, NMSC, MTFs, & other Services• Manage & monitor the multiple projects required to implement ICD-10 & provide status reporting against schedule/goals• Communicate ICD-10 related messages across the organization
BUMED has a plan that includes a governance model and PMO to provide structure to the ICD-10 implementation and ensure analytic needs are addressed.
9
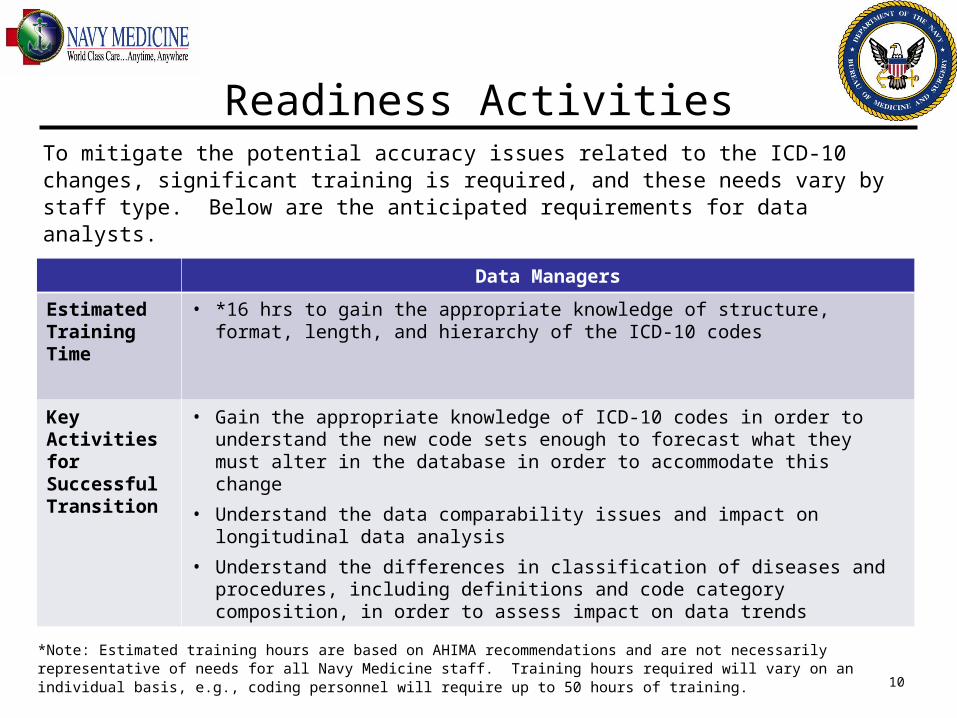
Readiness Activities
Data Managers
Estimated Training Time
• *16 hrs to gain the appropriate knowledge of structure, format, length, and hierarchy of the ICD-10 codes
Key Activities for Successful Transition
• Gain the appropriate knowledge of ICD-10 codes in order to understand the new code sets enough to forecast what they must alter in the database in order to accommodate this change
• Understand the data comparability issues and impact on longitudinal data analysis
• Understand the differences in classification of diseases and procedures, including definitions and code category composition, in order to assess impact on data trends
*Note: Estimated training hours are based on AHIMA recommendations and are not necessarily representative of needs for all Navy Medicine staff. Training hours required will vary on an individual basis, e.g., coding personnel will require up to 50 hours of training.
To mitigate the potential accuracy issues related to the ICD-10 changes, significant training is required, and these needs vary by staff type. Below are the anticipated requirements for data analysts.
10
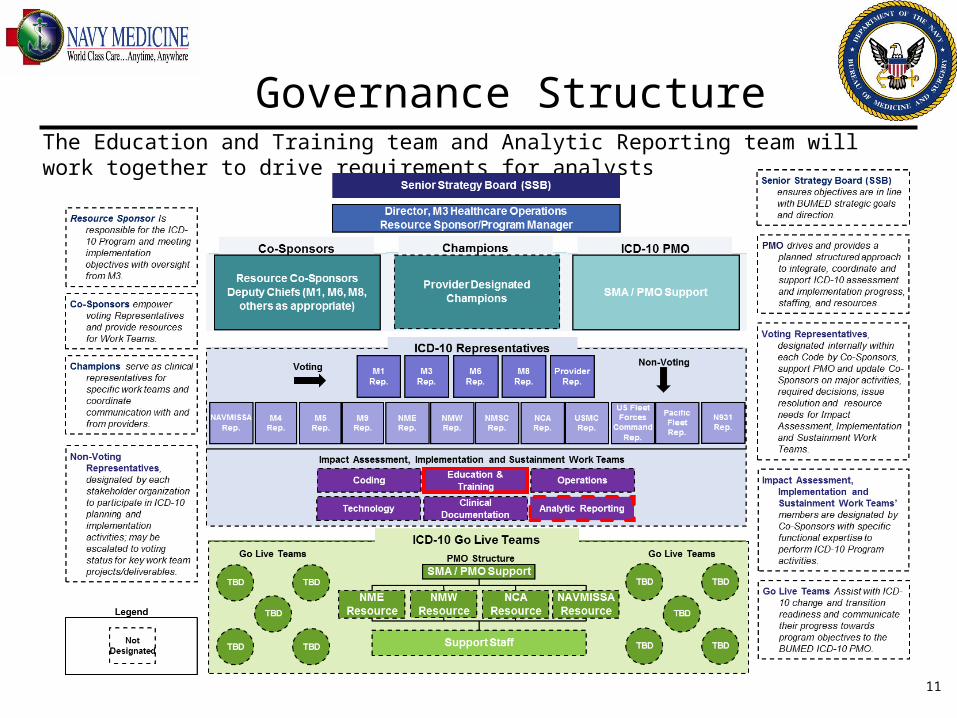
The Education and Training team and Analytic Reporting team will work together to drive requirements for analysts
Governance Structure
11
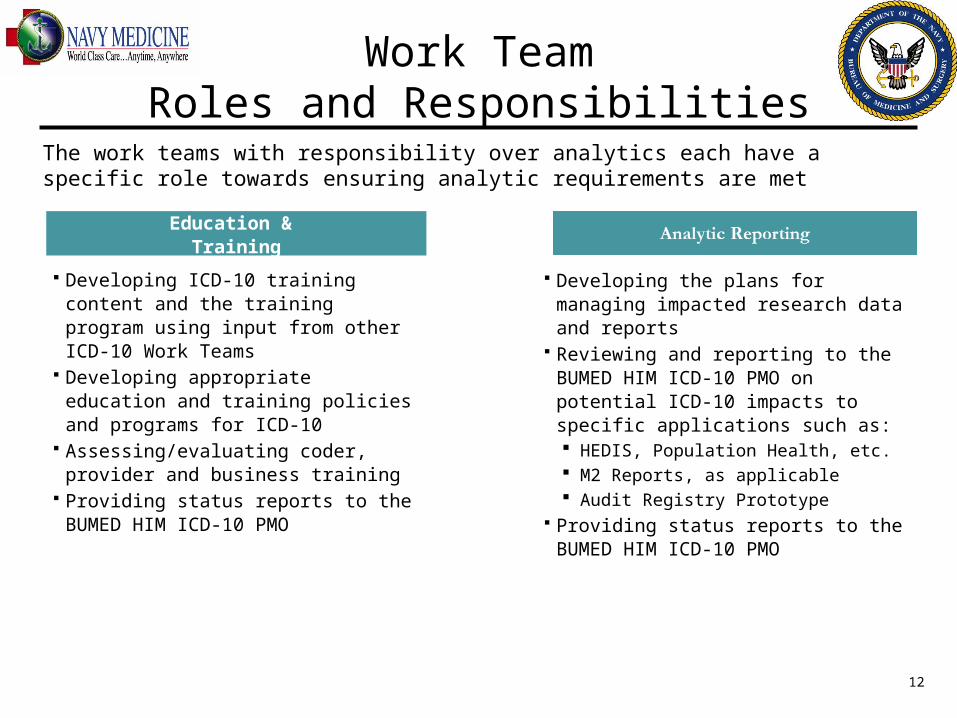
Work TeamRoles and Responsibilities
Education & Training
Developing ICD-10 training content and the training program using input from other ICD-10 Work Teams
Developing appropriate education and training policies and programs for ICD-10
Assessing/evaluating coder, provider and business training
Providing status reports to the BUMED HIM ICD-10 PMO
The work teams with responsibility over analytics each have a specific role towards ensuring analytic requirements are met
Developing the plans for managing impacted research data and reports
Reviewing and reporting to the BUMED HIM ICD-10 PMO on potential ICD-10 impacts to specific applications such as: HEDIS, Population Health, etc. M2 Reports, as applicable Audit Registry Prototype
Providing status reports to the BUMED HIM ICD-10 PMO
12
Discussion
• How do you currently use ICD-9 and other clinical data?
• What challenges do you foresee for maintaining your data analytic capabilities in the transition to ICD-10?
• What mitigation strategies can you think of?
• At every Region/MTF the Patient Admin Officer and Medical Records Administrator are your ICD-10 leads, funnel your thoughts/questions to them who will route to the Regions and ultimately the Health Info Mgmt (HIM) Department at BUMED.
13
Who to ContactCAPT Mary Jenkins Phone – (703) 681-6615 E-mail – [email protected]
LCDR Jori Brajer Phone – (703) 681-9239 E-mail – [email protected]
Ms. Shannon McConnell-Lamptey Phone – (703) 681-9193 E-mail – [email protected]
Ms. Jane Cunningham Phone – (703) 681-9138 email –
Mr. Dan Edwards – Deloitte
Phone – (202) 431-5167
E-mail – [email protected]
14
BACKUP SLIDES
15
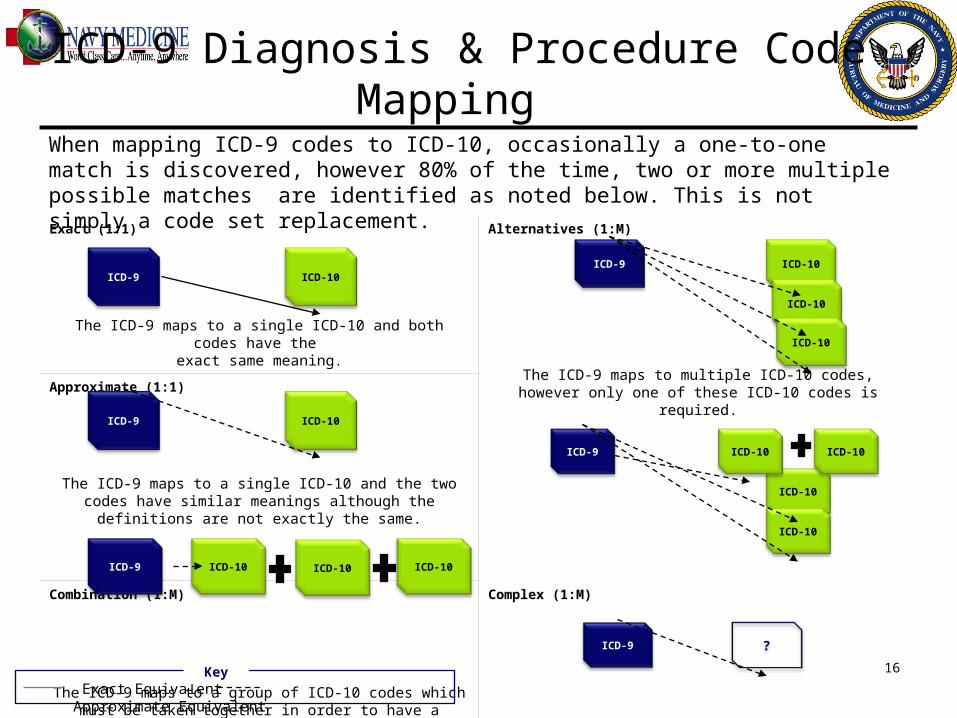
ICD-9 Diagnosis & Procedure Code
Mapping
Exact (1:1)
The ICD-9 maps to a single ICD-10 and both codes have the
exact same meaning.
Alternatives (1:M)
The ICD-9 maps to multiple ICD-10 codes, however only one of these ICD-10 codes is required.Approximate (1:1)
The ICD-9 maps to a single ICD-10 and the two codes have similar meanings although the definitions are not
exactly the same.
Complex (1:M)
The ICD-9 to ICD-10 mapping consists of both combinations and
alternative mappings.
Combination (1:M)
The ICD-9 maps to a group of ICD-10 codes which must be taken together in order to have a similar meaning to
the ICD-10.
Other (No Mapping)
There is no CMS published mappings from ICD-9 to ICD-10 (e.g., injury codes, extender codes)
ICD-9 ICD-10
ICD-10
ICD-10
ICD-9 ICD-10
ICD-9 ICD-10
ICD-9 ICD-10 ICD-10 ICD-10
ICD-9
ICD-10
ICD-10
ICD-10 ICD-10
Exact Equivalent Approximate Equivalent
ICD-9 ?
Key
When mapping ICD-9 codes to ICD-10, occasionally a one-to-one match is discovered, however 80% of the time, two or more multiple possible matches are identified as noted below. This is not simply a code set replacement.
16