Embed Size (px)
Citation preview

All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH. No statement or presentation made is to be regarded as dedicated to the public domain.
IC12-L: Tricks and Techniques to
Maximize Success with Nerve Transfers
Moderator(s): Susan E. Mackinnon, MD
Faculty: Christine B. Novak, PT, PhD and J. Megan Patterson, MD
Session Handouts
Friday, October 02, 2020
75TH VIRTUAL ANNUAL MEETING OF THE ASSH
OCTOBER 1-3, 2020
822 West Washington Blvd
Chicago, IL 60607
Phone: (312) 880-1900
Web: www.assh.org
Email: [email protected]

Reproduced with permission from Susan E. Mackinnon, MD
IC12 – Tricks and Techniques to Maximize Success with Nerve Transfers
American Society for Surgery of the Hand Annual Meeting, October 2, 2020
Susan E. Mackinnon, MD, St. Louis, Missouri J. Megan M. Patterson, Chapel Hill, North Carolina
Christine B. Novak, PT, PhD, Toronto, Ontario Andrew Yee, BS, St. Louis, Missouri
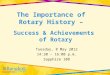
Overview: Following complex nerve injury, motor and sensory recovery can be less than optimal. For high median, ulnar and radial nerve injuries, nerve transfers can provide a distal source of motor and/or sensory innervation closer to the target end organ allowing for faster recovery and improved outcome. This course will focus on techniques to maximize success with upper extremity motor and sensory nerve transfers. Classification of Nerve Injury: Degree of Injury Tinel’s Sign
Present
Recovery Rate of Recovery
Surgical Procedure
I
Neurapraxia No Complete Up to 12 weeks None
II
Axonotmesis Yes Complete 1” per month None
III
Yes Varies * 1” per month None or Neurolysis
IV
Neuroma In-continuity
Yes but no advancement
None None Nerve repair, graft or transfer
V
Neurotmesis Yes but no advancement
None None Nerve repair, graft or transfer
VI
Mixed Injury (I to V)
Some fascicles (II, III)
Some fascicles (II, III)
Depends on degree of injury (I – V)
Neurolysis, nerve repair, graft or transfer
* Recovery can vary from excellent to poor depending on the amount of scarring and the sensory versus motor axon misdirection to target receptors Modified from Mackinnon & Dellon, Surgery of the Peripheral Nerve, 1988.

Reproduced with permission from Susan E. Mackinnon, MD
2
Advantages of Nerve Transfers: 1. Directs a large number of axons to denervated muscle quickly. 2. Provides faster and superior muscle reinnervation then may be seen with primary repair or
grafting.
Surgical Indications and Management: Motor Nerve Transfers: 1. Motor donor nerve must:
• Be expendable. • Be close to the motor end plates of the target muscle. • Contain a large number of motor nerve axons. • Allow for straightforward motor reeducation by using a donor muscles that is synergistic to
the target muscle
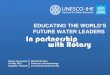
2. Common motor nerve transfers: • Median nerve fascicle and ulnar nerve fascicle to biceps brachii branch and brachialis branch
of musculocutaneous nerve for elbow flexion (Double Fascicular Transfer).

Reproduced with permission from Susan E. Mackinnon, MD
3
• Anterior interosseous nerve to motor branch of ulnar for intrinsic muscle reinnervation.

Reproduced with permission from Susan E. Mackinnon, MD
4
Sensory Nerve Transfers: 1. Sensory donor nerve must:
• Provide sensation to a non-critical area. • Be a pure sensory nerve. • Be a good size match between donor and target nerve.
2. Common sensory nerve transfers:
• Nerve to the 4th webspace to 1st web space transfer to retore sensation to the radial side of the index and ulnar side of the thumb.
• End-to-side repair of 2nd and 3rd web space to ulnar digital nerve to the small to restore sensation to the 2nd and 3rd web spaces.
• End-to-side repair of ulnar sensory and dorsal ulnar sensory nerves to median nerve to restore sensation to the small and ring fingers and ulnar dorsal skin.
Tips and Pearls for the Beginner—in the OR:
• Remind anesthesiologist—no long acting paralytics. • Don’t use Marcaine/lidocaine until after you want to stimulate the nerves. • Avoid use of a tourniquet especially if you are a bit slower—otherwise a tourniquet palsy may
complicate intraoperative direct nerve stimulation. • Donor DISTAL, Recipient PROXIMAL. • ‘Neurolysis with your eyes’.

Reproduced with permission from Susan E. Mackinnon, MD
5
Common injury patterns and treatment options: 1. Upper plexus injury—loss of elbow flexion:
• Nerve transfers: • Double fascicular transfer (median/ulnar to nerve to biceps and brachialis). • Medial pectoral to musculocutaneous nerve. • Thoracodorsal to musculocutaneous nerve.
• Other options: • Steindler flexorplasty. • Long nerve grafts.
2. Upper plexus injury—loss of shoulder function:
• Nerve transfers: • Spinal accessory nerve to suprascapular nerve. • Triceps to axillary nerve. • Medial pectoral nerve to axillary nerve.
• Other options: • Shoulder fusion. • Trapezius transfer (Saha procedure). • Long nerve grafts.
3. Lower plexus injury—loss of pronation:
• Nerve transfers: • Brachialis or ECRB (if C7 is spared) to pronator nerve branch.
• Other options: • Biceps, brachioradialis, or brachialis muscle rerouting.
4. Lower plexus injury—loss of thumb and index finger flexion
• Nerve transfers: • Supinator branch to anterior interosseous nerve transfer. • Brachialis branch to anterior interosseous nerve transfer.
• Other options: • Tendon tranfers (brachioradialis to flexor pollicis longus and extensor carpi radialis longus to
index finger flexor digitorum profundus). 5. Axillary nerve injury:
• Nerve transfers: • Triceps to axillary nerve. • Medial pectoral nerve to axillary nerve. • Thoracodorsal nerve to axiallary nerve.
• Other options: • Shoulder fusion. • Long nerve grafts.

Reproduced with permission from Susan E. Mackinnon, MD
6
6. Radial nerve injury: • Nerve transfers:
• Median (flexor carpi radialis, flexor digitorum superficialis branches) to extensor carpi radialis brevis and posterior interosseous nerve branches.
• Other options: • Tendon transfers (pronator teres to extensor carpi radialis brevis, palmaris longus to extensor
pollicis longus, and flexor carpi ulnaris, flexor carpi radialis or flexor digitorum superficialis to extensor digitorum communis).
7. Loss of median innervated pronation:
• Nerve transfers: • Extensor carpi radialis brevis to pronator teres nerve branch.
• Other options: • Biceps, brachioradialis, or brachialis muscle rerouting.
8. Loss of median innervated thumb and finger flexion:
• Nerve transfers: • Supinator branch to anterior interosseous nerve transfer. • Brachialis branch to anterior interosseous nerve transfer.
• Other options: • Tendon tranfers (brachioradialis to flexor pollicis longus, extensor carpi radialis longus to
index/long finger flexor digitorum profundus, side to side tendodesis to ulnar flexor digitorum profundus).
9. Isolated AIN injury:
• Nerve transfers: • Flexor digitorum superficialis to anterior interosseous nerve branch.
• Other options: • Brachioradialis to flexor pollicis longus tendon transfer and flexor digitorum profundus
tenodesis • Fusion of interphalangeal joint of thumb.
10. Distal median nerve injury:
• Nerve transfers: • AIN to median motor branch.
• Other options: • Opponensplasty.
11. Distal ulnar nerve injury:
• Nerve transfers: • Anterior interosseous nerve to ulnar deep motor branch.
• Other options: • Various static and dynamic claw hand procedures.

Reproduced with permission from Susan E. Mackinnon, MD
7
Rehabilitation following Nerve Transfer: Early Post-operative Management:
• Early range of motion is important to decrease adhesions at the nerve repair site. • Postoperative dressing is removed on POD 2 to 3 and active/passive range of motion of
uninvolved joints is started. • Protect repair site with a splint or sling for 7-14 days. • Following immobilization; regain and maintain full passive range of motion.
Late Stage Rehabilitation - Sensory & Motor Reeducation:
• Alteration in cortical mapping following nerve injury. • Following reinnervation, can regain cortical area by increasing the sensory/motor input. Sensory reeducation: • Begin by increasing the sensory input to the appropriate sensory distribution with different
textures of material. • Progress to localization exercises and finally discriminatory tasks. • Cortical retraining requires repetition and purposeful movement.
Motor reeducation: • Need to increase muscle strength and central mechanisms controlling motor function. • Nerve transfer requires motor reeducation similar to that required with tendon transfers. • Restore muscle balance – be aware of co-contraction of antagonist muscles, strengthen
muscles weakened by disuse. • Biofeedback (visual and audio) more useful than muscle stimulation. • To facilitate relearning begin on unaffected side. • Initially need to contract muscle from donor nerve to achieve a contraction in the recipient
muscle. Aim for control and initiation of muscle contraction. • Begin in gravity assisted or gravity eliminated position and progress to exercises against
gravity and progressive resisted exercises. • Dissociate target muscle from donor muscle contraction.

Reproduced with permission from Susan E. Mackinnon, MD
8
References 1. Anastakis DJ, Malessy MJ, Chen R, Davis KD, Mikulis D. Cortical plasticity following nerve
transfer in the upper extremity. Hand Clin. 2008, 24: 425-44. 2. Barbour J, Yee A, Kahn LC, Mackinnon SE. Supercharged end-to-side anterior interosseous to ulnar
motor nerve transfer for intrinsic musculature reinnervation. J Hand Surg Am. 2012, 37: 2150-9. 3. Battiston B, Lanzetta M. Reconstruction of high ulnar nerve lesions by distal double median to ulnar
nerve transfer. J Hand Surg Am. 1999, 24: 1185-91. 4. Boyd KU, Nimigan AS, Mackinnon SE. Nerve reconstruction in the hand and upper extremity. Clin
Plast Surg. 2011, 38: 643-60. 5. Brown JM, Mackinnon SE. Nerve transfers in the forearm and hand. Hand Clin. 2008, 24: 319-40. 6. Brown JM, Tung TH, Mackinnon SE. Median to radial nerve transfer to restore wrist and finger
extension: technical nuances. Neurosurgery. 2010, 66: 75-83. 7. Cheng J, Mackinnon SE. Nerve transfers for digital sensation. In Slutsky D. (ed.) Masterskills:
Nerve, Chapter 15, American Society for Surgery of the Hand, 2008, 181-192. 8. Cheng J, Mackinnon SE. Nerve transfers to restore pronation. In Slutsky D. (ed.) Masterskills:
Nerve, Chapter 18, American Society for Surgery of the Hand, 2008, 213-226. 9. Davidge KM, Yee A, Kahn LC, Mackinnon SE. Median to radial nerve transfers for restoration of
wrist, finger, and thumb extension. J Hand Surg Am. 2013; 38(9): 1812-27. 10. Dengler J, Dolen U, Patterson JM, Davidge KM, Kahn LC, Yee A, Mackinnon SE. Supercharge
End-to-Side Anterior Interosseous-to-Ulnar Motor Nerve Transfer Restores Intrinsic Function in Cubital Tunnel Syndrome. Plast Reconstr Surg. 2020 Jun 22. doi: 10.1097/PRS.0000000000007167.
11. Domeshek LF, Novak CB, Patterson MM, Hasak JM, Yee A, Kahn LC, Mackinnon SE: Nerve Transfers – A Paradigm Shift in the Reconstructive Ladder. Plastic and Reconstructive Surgery Global Open. 2019 Jun; 7(6):e2290-9.
12. Duff SV. Impact of peripheral nerve injury on sensorimotor control. J Hand Ther. 2005, 18: 277-91. 13. Farber SJ, Glaus SW, Moore AM, Hunter DA, Mackinnon SE, Johnson PJ. Supercharge nerve
transfer to enhance motor recovery: a laboratory study. J Hand Surg Am. 2013, 38: 466-77. 14. Garg R, Merrell GA, Hillstrom HJ, Wolfe SW. Comparison of nerve transfers and nerve grafting for
traumatic upper plexus palsy: a systematic review and analysis. J Bone Joint Surg Am. 2011, 93: 819-29.
15. Haase SC, Chung KC. Anterior interosseous nerve transfer to the motor branch of the ulnar nerve for high ulnar nerve injuries. Ann Plast Surg. 2002, 49: 285-90.
16. Hsiao EC, Fox IK, Tung TH, Mackinnon SE. Motor nerve transfers to restore extrinsic median nerve function: case report. Hand (N Y). 2009, 4: 92-7.
17. Kale SS, Glaus SW, Yee A et al. Reverse end-to-side nerve transfer: from animal model to clinical use. J Hand Surg Am. 2011, 36: 1631-9 e2.
18. Keane GC, Pan D, Roh J, Larson EL, Schellhardt L, Hunter DA, Snyder-Warwick AK, Moore AM, Mackinnon SE, Wood MD. The Effects of Intraoperative Electrical Stimulation on Regeneration and Recovery After Nerve Isograft Repair in a Rat Model. Hand (N Y). 2020 Jul 15:1558944720939200. doi: 10.1177/1558944720939200
19. Lee SK, Wolfe SW. Nerve transfers for the upper extremity: new horizons in nerve reconstruction. J Am Acad Orthop Surg. 2012, 20: 506-17.
20. Leechavengvongs S, Witoonchart K, Uerpairojkit C, et al. Nerve transfer to deltoid muscle using the nerve to the long head of the triceps, part II: a report of 7 cases. J Hand Surg Am. 2003, 28: 633-8.
21. Lowe JB, 3rd, Sen SK, Mackinnon SE. Current approach to radial nerve paralysis. Plast Reconstr Surg. 2002, 110: 1099-113.

Reproduced with permission from Susan E. Mackinnon, MD
9
22. Mackinnon SE. Nerve Surgery. Thieme Medical Publishers, 2015. 23. Mackinnon SE, Colbert SH. Nerve transfers in the hand and upper extremity surgery. Tech Hand Up
Extrem Surg. 2008, 12: 20-33. 24. Mackinnon SE, Novak CB. Nerve transfers. New options for reconstruction following nerve injury.
Hand Clin. 1999, 15: 643-66. 25. Merrell GA, Barrie KA, Katz DL, Wolfe SW. Results of nerve transfer techniques for restoration of
shoulder and elbow function in the context of a meta-analysis of the English literature. J Hand Surg Am. 2001, 26: 303-14.
26. Moore AM, Franco M, Tung TH. Motor and Sensory Nerve Transfers in the Forearm and Hand. Plast Reconstr Surg. 2014; 134(4):721-730.
27. Moore AM, Novak CB. Advances in nerve transfer surgery. J Hand Ther. 2014; 27(2): 96-105. 28. Muratori LM, Lamberg EM, Quinn L, Duff SV. Applying principles of motor learning and control to
upper extremity rehabilitation. J Hand Ther. 2013, 26: 94-103. 29. Murphy RK, Ray WZ, Mackinnon SE. Repair of a median nerve transection injury using multiple
nerve transfers, with long-term functional recovery. J Neurosurg. 2012, 117: 886-9. 30. Novak CB. Rehabilitation following motor nerve transfers. Hand Clin. 2008, 24: 417-23. 31. Novak CB: Rehabilitation Following Nerve Transfer. In: Slutsky, DJ (ed) Upper Extremity Nerve
Repair – Tips and Techniques. Ch 23, Pg 261-266, 2008. 32. Novak CB, Anastakis DJ, Beaton DE, Mackinnon SE, Katz J. Biomedical and psychosocial factors
associated with disability after peripheral nerve injury. J Bone Joint Surg Am. 2011, 93: 929-36. 33. Novak CB, Mackinnon SE. Distal anterior interosseous nerve transfer to the deep motor branch of
the ulnar nerve for reconstruction of high ulnar nerve injuries. J Reconstr Microsurg. 2002, 18: 459-64.
34. Phillips BZ, Franco MJ, Yee A, Tung TH, Mackinnon SE, Fox IK. Direct radial to ulnar nerve transfer to restore intrinsic muscle function in combined proximal median and ulnar nerve injury: case report and surgical technique. J Hand Surg Am. 2014; 39(7): 1358-62.
35. Ray WZ, Mackinnon SE. Clinical outcomes following median to radial nerve transfers. J Hand Surg Am. 2011, 36: 201-8.
36. Ray WZ, Yarbrough CK, Yee A, Mackinnon SE. Clinical outcomes following brachialis to anterior interosseous nerve transfers. J Neurosurg. 2012, 117: 604-9.
37. Taylor KS, Anastakis DJ, Davis KD. Cutting your nerve changes your brain. Brain. 2009, 132: 3122-33.
38. Tung TH, Barbour JR, Gontre G, Daliwal G, Mackinnon SE. Transfer of the extensor digiti minimi and extensor carpi ulnaris branches of the posterior interosseous nerve to restore intrinsic hand function: case report and anatomic study. J Hand Surg Am. 2013, 38: 98-103.
39. Tung TH, Mackinnon SE. Flexor digitorum superficialis nerve transfer to restore pronation: two case reports and anatomic study. J Hand Surg Am. 2001, 26: 1065-72.
40. Tung TH, Mackinnon SE. Nerve transfers: indications, techniques, and outcomes. J Hand Surg Am. 2010, 35: 332-41.
41. Vernadakis AJ, Humphreys DB, Mackinnon SE. Distal anterior interosseous nerve in the recurrent motor branch graft for reconstruction of a median nerve neuroma-in-continuity. J Reconstr Microsurg. 2004, 20: 7-11.
42. Wang Y, Zhu S. Transfer of a branch of the anterior interosseus nerve to the motor branch of the median nerve and ulnar nerve. Chin Med J (Engl). 1997, 110: 216-9.