Embed Size (px)
Citation preview

Gregory Y. Lauwers, M.D. Vice Chairman
Department of Pathology
Director, Gastrointestinal Pathology Service
Massachusetts General Hospital
Professor of Pathology
Harvard Medical School, Boston, MA
Iatrogenic Pathology of the Intestines:
The More You Look, The More You Find!

• Various (but limited) GI side-effect: diarrhea,
constipation, nausea and vomiting.
• Entire gut is variably affected.
• Various mechanisms & patterns of injury: o Erosions/ulcerations/necrosis/fibrosis & stenosis
o Hyperplastic/reactive changes
o Inflammatory infiltrate (lymphocytes/eosinophils)
o Crystals deposition
o Apoptosis / Mitotic arrest / abnormal mitoses
Iatrogenic gut damages are common:
2-8% of pts receiving drugs experience an adverse reaction.
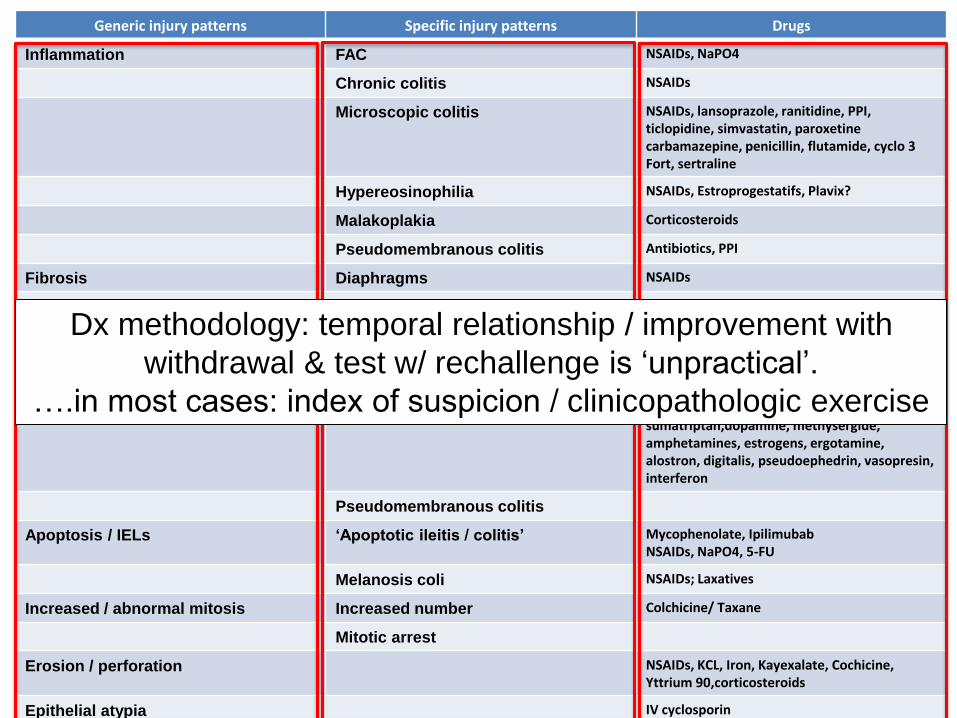
Generic injury patterns Specific injury patterns Drugs
Inflammation FAC NSAIDs, NaPO4
Chronic colitis NSAIDs
Microscopic colitis NSAIDs, lansoprazole, ranitidine, PPI, ticlopidine, simvastatin, paroxetine carbamazepine, penicillin, flutamide, cyclo 3 Fort, sertraline
Hypereosinophilia NSAIDs, Estroprogestatifs, Plavix?
Malakoplakia Corticosteroids
Pseudomembranous colitis Antibiotics, PPI
Fibrosis Diaphragms NSAIDs
Strictures KCL, Pancreatic enzymes
Architectural Dilated/damaged crypts
Villous atrophy Sulindac, Mycophenolate, NSAIDs, azathioprine, Olmesartan
Ischemia Ischemic colitis NSAIDs, kayexalate, cocaine, diuretics, sumatriptan,dopamine, methysergide, amphetamines, estrogens, ergotamine, alostron, digitalis, pseudoephedrin, vasopresin, interferon
Pseudomembranous colitis
Apoptosis / IELs ‘Apoptotic ileitis / colitis’ Mycophenolate, Ipilimubab NSAIDs, NaPO4, 5-FU
Melanosis coli NSAIDs; Laxatives
Increased / abnormal mitosis Increased number Colchicine/ Taxane
Mitotic arrest
Erosion / perforation NSAIDs, KCL, Iron, Kayexalate, Cochicine, Yttrium 90,corticosteroids
Epithelial atypia IV cyclosporin
Dx methodology: temporal relationship / improvement with
withdrawal & test w/ rechallenge is ‘unpractical’.
….in most cases: index of suspicion / clinicopathologic exercise


Mimics of Enteropathies (e.g., celiac disease)
• Various drugs can elicit intraepithelial
lymphocytosis with or without epithelial
damage,
– Olmesartan, angiotensin II receptor antagonist
(Benicar®)
– CTLA-4 monoclonal antibody (ipilimumab®)
adjuvant to tumor vaccination therapy
(melanoma, RCC, ovarian Ca).

Original report 22pts : chronic diarrhea & weight loss with 10-40/mg/day
Gastric and colonic manifestations
Sx /histology reversed to normal after cessation
Various degrees of blunting, intraepithelial lymphocytosis and apoptosis
Olmesartan
Rubio-Tapia A. Mayo Clin Proc 2012

Ileitis w/ collagen depositon colitis
Olmesartan
Menne J. Mayo Clinic Proc 2012 Follow up study: probably a rare
association. Role of HLA-DQ2/8?

APOPTOTIC & EROSIVE PATTERNS OF
INJURY
• Immunosuppressive or antineoplastic agents
(predominantly).
– Mycophenolic Acid
– CTLA-4 monoclonal antibody
– Anti-metabolites (methotrexate; capecitabine)
– TNF-α antagonists (infliximab)
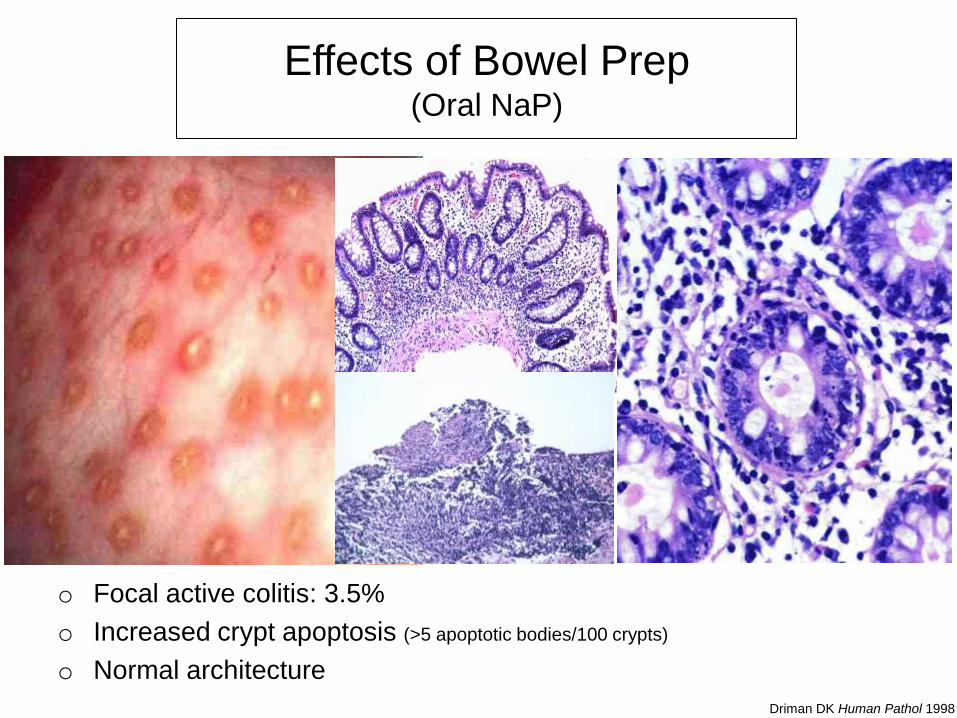
Effects of Bowel Prep (Oral NaP)
Driman DK Human Pathol 1998
o Focal active colitis: 3.5%
o Increased crypt apoptosis (>5 apoptotic bodies/100 crypts)
o Normal architecture

Mycophenolic Acid (MPA)
• B&T lymphocytes depend almost completely on the pathway & results in cytotoxic T lymphocytes inhibition
• Enterocytes are less dependent on this pathway but still damaged
• Inhibits purine synthesis for DNA synthesis in the de novo pathway.

• mycophenolate mofetil (CellCept®),
• mycophenolate sodium (Myofortic®)
• Gastrointestinal injuries in ~45% of pts:
o GVHD like alterations throughout the GIT
o Active esophagitis with ulceration or erosion,
o Chemical gastropathy; focally enhanced gastritis,
o Crohn-like damages in the duodenum.
o Cryptitis, crypt withering and distortion, reparative
changes and increased neuroendocrine cells in colon.
Mycophenolic Acid (MPA)
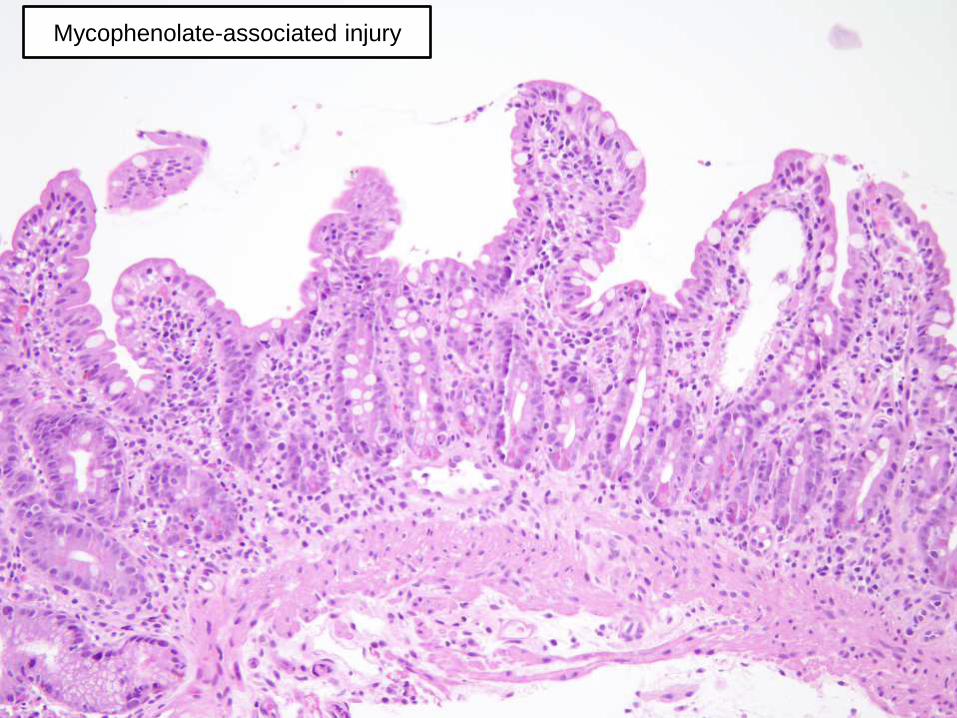
Mycophenolate-associated injury

Mycophenolate-associated injury

Mycophenolate-associated injury
Colon

Iatrogenic injury v. GVHD in BMT
pts?
• Eosinophils more commonly
associated w/ MPA
• Esophageal mucosa is less
dependent on de novo pathway
that columnar mucosa, thus its
involvement suggests GVHD
Mycophenolate-associated injury
Increased risk of CMV colitis; associated in 6-11% of pts
CTLA-4 monoclonal antibody (ipilimumab®)
• How does if works? – CTLA-4 is expressed on Tregs and following antigenic
stimulation, it inhibits T cell signaling and proliferation.
– mAb against CTLA-4 result in increased expansion of tumor-specific T cells & enhancing tumor destruction.
• Complications: – Dermatitis and vitiligo.
– Enterocolitis.
Villous blunting of small bowel / cryptitis in colon
Lymphoplasmacytic expansion of lamina propria, intraepithelial lymphocytosis and apoptosis.

CTLA-4 monoclonal antibody (ipilimumab®)

CTLA-4 monoclonal antibody (ipilimumab®)

CTLA-4 monoclonal antibody (ipilimumab®)

CTLA-4 monoclonal antibody (ipilimumab®)
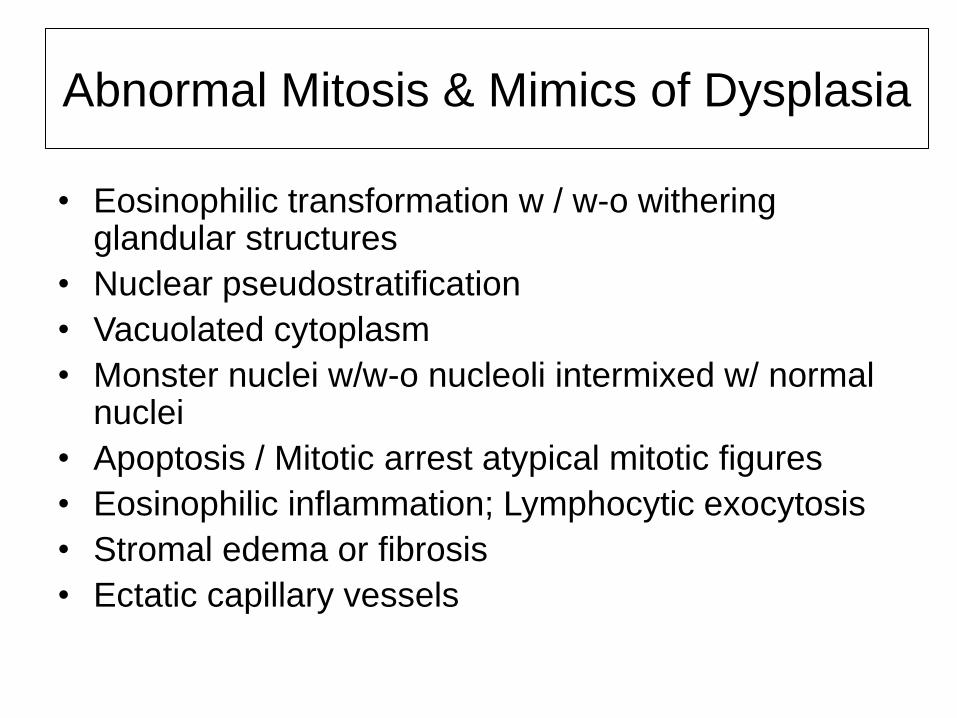
Abnormal Mitosis & Mimics of Dysplasia
• Eosinophilic transformation w / w-o withering glandular structures
• Nuclear pseudostratification
• Vacuolated cytoplasm
• Monster nuclei w/w-o nucleoli intermixed w/ normal nuclei
• Apoptosis / Mitotic arrest atypical mitotic figures
• Eosinophilic inflammation; Lymphocytic exocytosis
• Stromal edema or fibrosis
• Ectatic capillary vessels

Colchicine Toxicity
Alkaloid that binds to tubulin with antimitotic ability
• Pts with renal or
hepatic insufficiency
and cannot clear the
drug [long ½ life]. – cholera-like sd. w/
dehydration, shock.
– bone marrow suppression.
– acute renal failure.
• Can lead to multi-organ
failure.
Mitotic arrest in normal mucosa in toxic
patients (proliferative zone) but it is seen in
neoplasms in pts w/ therapeutic levels.

Taxane Effect [Taxol (paclitaxel); taxotere (docetaxel]
• Histology similar as
colchicine toxicity:
– ring mitoses
– apoptosis in
proliferative
compartment
– Noted 2-3 days after
initiation or in
toxicity
• Daniels JA. Am J Surg Pathol. 2008;32:473-7.
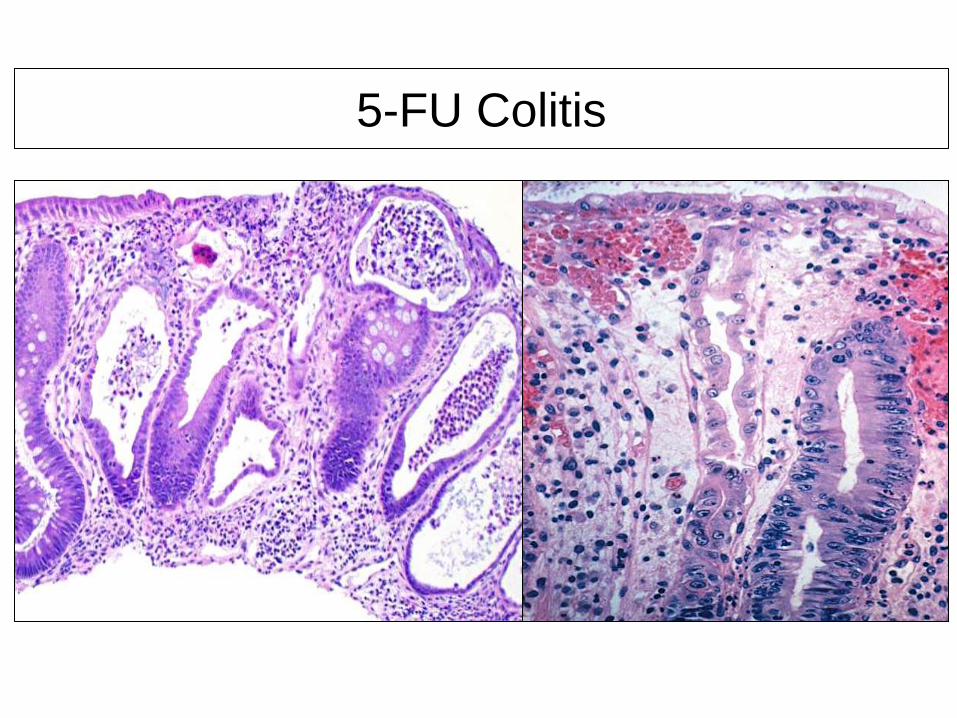
5-FU Colitis
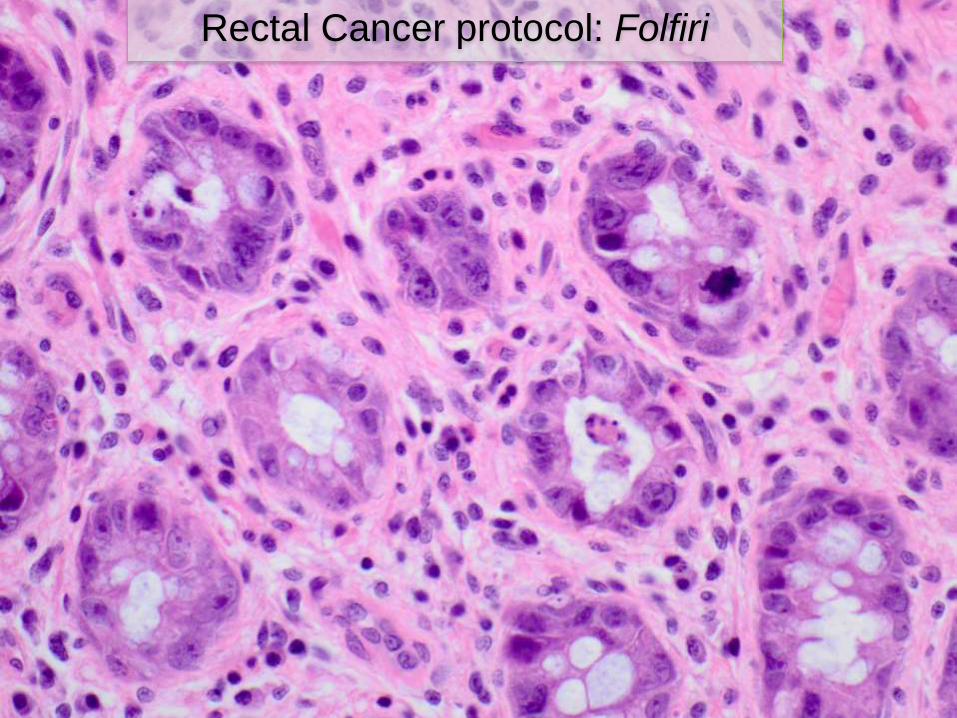
Rectal Cancer protocol: Folfiri

Ulcerative & Chronic Ileitis / Colitis
Pattern of Injury
• NSAIDs and other compounds can present w/ an
ulcerative & chronic patterns of mucosal injury.
• NSAIDs block cyclo-oxygenases 1 and 2.
– Incidence of adverse effects reported in up to
70% with long-term Rx
– Major pathology: ulceration and hemorrhage,
more likely with high doses.

Prevalence of NSAID-induced enteropathy is
underestimated. – > 50% of pts have
mucosal damage in the
Small Bowel (Video
capsule endoscopy).
– Mucosal erythema,
– Erosions, ulcers,
perforation
– Diaphragm disease and
strictures.
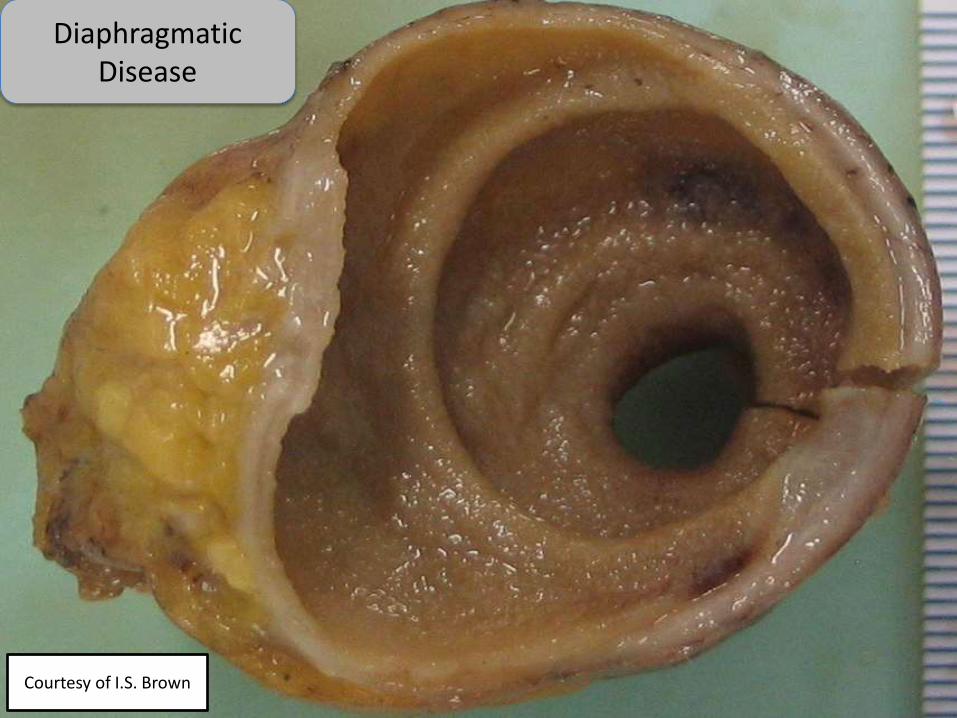
Diaphragmatic Disease
Courtesy of I.S. Brown

1 2
3
NSAIDs-induced
ulcer at top of small
bowel mucosal fold
NSAIDs-induced diaphragm disease—
circumferential narrowing caused by concentric
submucosal fibrosis, most likely a result of
ulceration the top of mucosal folds.

NSAIDs and colonic damage: a long tale
Possibly increasing due to use of enteric coated or
sustained (slow) release formulation (higher concentrations in
the prox. colon)
• Various types of Colitis
– Focal active colitis and chronic colitis.
– Collagenous colitis and Lymphocytic colitis
– Pseudomembranous colitis (Diclofenac®)
– Eosinophilic colitis (Naproxen®)
– Ulcers (Rt colon)
– Diaphragm disease
– Exacerbation of pre-existing IBD or diverticular disease (or
perforation)
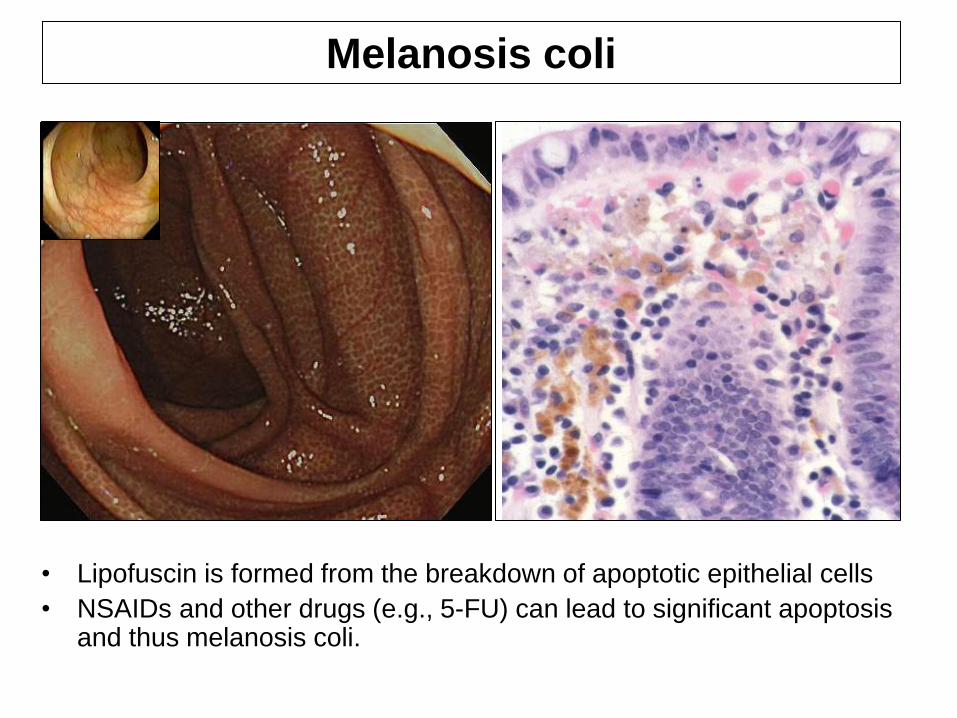
• Lipofuscin is formed from the breakdown of apoptotic epithelial cells
• NSAIDs and other drugs (e.g., 5-FU) can lead to significant apoptosis and thus melanosis coli.
Melanosis coli

Focal active colitis Right sided ‘NSAIDs chronic colitis’

• NSAIDS – Ulcer can occur
anywhere in colon, but more
common on right side.
• sharply circumscribed
with ischemic-type
histology
Solitary cecal ulceration, ulceration secondary to a diverticulum, local ischemia,
stercoral ulceration and solitary rectal ulcer syndrome need to be ruled
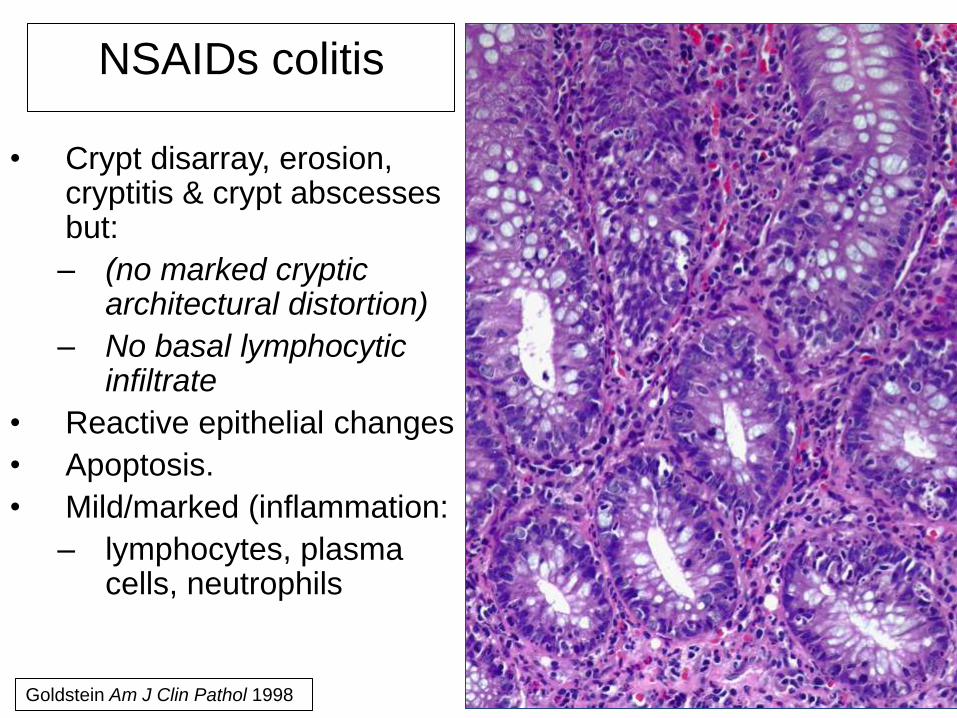
• Crypt disarray, erosion, cryptitis & crypt abscesses but:
– (no marked cryptic architectural distortion)
– No basal lymphocytic infiltrate
• Reactive epithelial changes
• Apoptosis.
• Mild/marked (inflammation:
– lymphocytes, plasma cells, neutrophils
NSAIDs colitis
Goldstein Am J Clin Pathol 1998
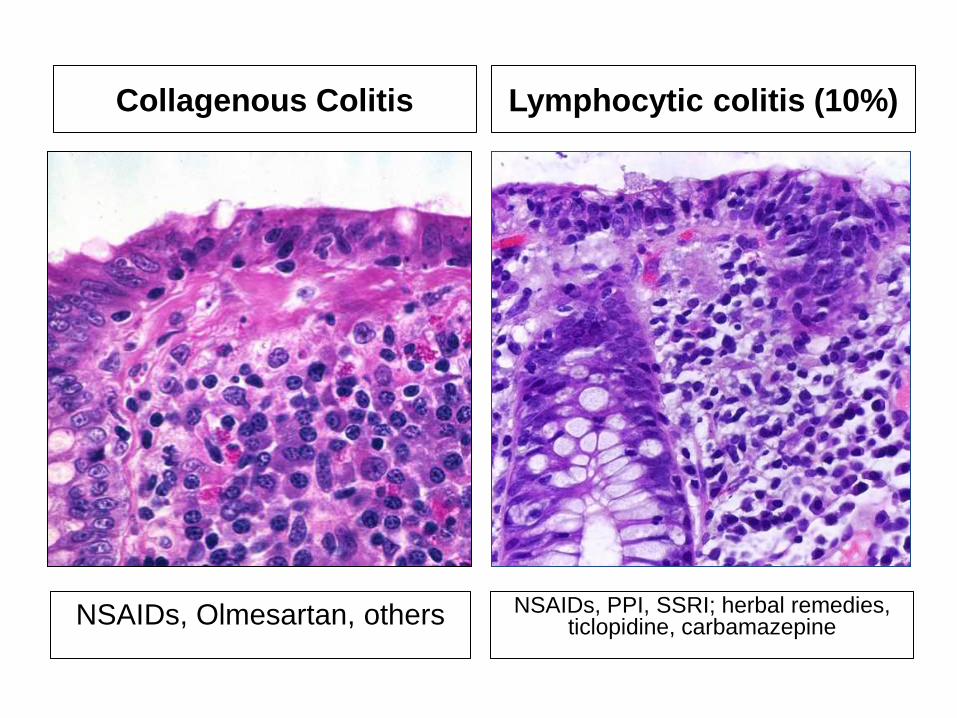
Collagenous Colitis Lymphocytic colitis (10%)
NSAIDs, PPI, SSRI; herbal remedies, ticlopidine, carbamazepine
NSAIDs, Olmesartan, others

NSAIDS and ‘microscopic colitis’
Collagenous colitis
• Case control study of 31
pts w/ collagenous colitis
– 19 patients using NSAIDs
(vs. 4 controls)
– All developed diarrhea after
beginning NSAID therapy
– 3 improved with
discontinuation of NSAIDs
– 1 re-challenged: recurrence
of diarrhea
• 40 pts w/ lymphocytic
colitis
– Half taking NSAIDs
– Patients on NSAIDs had
higher intraepithelial
lymphocyte counts
– However, no correlation
between NSAID use and
clinical course
Riddell et al. Gut 1992 Wang N, et al. Am J Surg Pathol 1999
Lymphocytic colitis

NSAIDs,Digoxin, Cocaine,
Pseudoephedrine
vasopressors
OCP/estrogenic compounds
Eosinophilic colitis Ischemic colitis
Am J Gastroenterol 2004:1175 Aliment Pharmacol Ther 2009;29:535-541
NSAIDs, Gold, L-Tryptophan,
Carbamazepine, Methotrexate,
Tacrolimus, Azothioprine,
Rifampicin, Clozapine
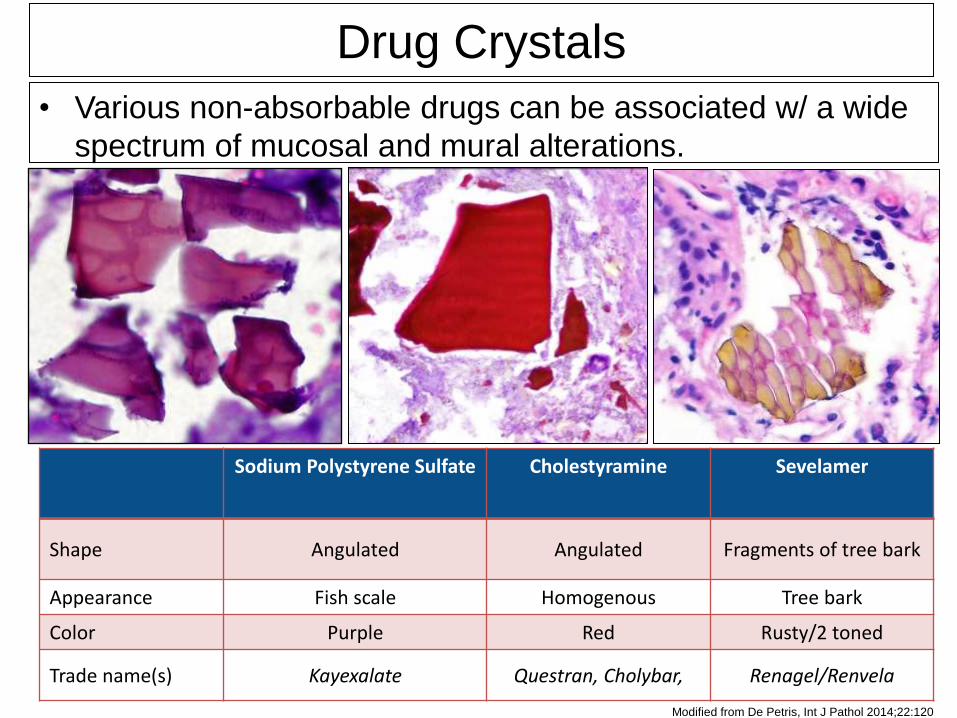
Sodium Polystyrene Sulfate Cholestyramine Sevelamer
Shape Angulated Angulated Fragments of tree bark
Appearance Fish scale Homogenous Tree bark
Color Purple Red Rusty/2 toned
Trade name(s) Kayexalate Questran, Cholybar, Renagel/Renvela
Modified from De Petris, Int J Pathol 2014;22:120
• Various non-absorbable drugs can be associated w/ a wide
spectrum of mucosal and mural alterations.
Drug Crystals

Kayexalate (in Sorbitol!)
• Cation exchange resin used to treat
hyperkalemia
• Administered w/ sorbitol an hyperosmotic
agent to prevent impaction
– Colonic necrosis
– Injury reported in upper GIT but commonly
milder.

Kayexalate (in Sorbitol!)

DIAGNOSIS OF DRUG INDUCED INJURY IS
(CAN BE) DIFFICULT
• Some compounds are associated w/
characteristic patterns of injury (many
don’t)
• Since the gut has a limited set of response
patterns to injuries
– overlapping features with primary GI
pathology
– clinical correlation is always important (clinical
adverse reaction?).

DIAGNOSIS OF DRUG INDUCED INJURY IS
(CAN BE) DIFFICULT
• ….when little or no clinical information is
usually provided!
• Always consider in atypical “itis”.
• Pointers:
– Marked nuclear pleomorphism / cytologic
atypia.
– Atypical mitoses.
– Apoptosis.
– Withering crypts.



![Laxatives for the management of constipation in …...[Intervention Review] Laxatives for the management of constipation in people receiving palliative care Bridget Candy 1, Louise](https://img.pdfslide.us/doc/110x75/5f0b91c17e708231d43128fb/laxatives-for-the-management-of-constipation-in-intervention-review-laxatives.jpg)

























