Embed Size (px)
Citation preview

SHORT REPORT
Iatrogenic cortical aneurysm post-craniotomy
MARCO ANTONIO ZANINI, RODRIGO ALMEIDA BORGES, GUSTAVO HENRIQUE
NUNES AQUINO & CARLOS CLAYTON MACEDO DE FREITAS
Division of Neurosurgery, Botucatu Medical School, Sao Paulo State University (UNESP) Botucatu, SP, Brazil
AbstractTaking into account the number of craniotomies performed every day around the world, iatrogenic aneurysm post-craniotomy is extremely rare with only anecdotal cases reported in literature. We report an iatrogenic aneurysm affecting acortical vessel which probably developed during dural closure of a conventional craniotomy. The aneurysm was discovered 6months after surgery on a routine control angiography. The patient was successfully treated by trapping the parent vessel andexcising the aneurysm. Histopathological findings were compatible with a true type of traumatic aneurysm. The possibility ofthis rare condition occurring highlights the risk of arterial injury during craniotomy.
Key words: Cerebral aneurysm, iatrogenic, cortical vessel, craniotomy, postoperative complications.
Introduction
Traumatic intracranial aneurysms are rare, repre-
senting less than 1% of all aneurysms.1,2 They most
frequently occur after closed or penetrating head
injury, but may also occur after neurosurgical
procedures. Most cases result in immediate haemor-
rhage and subsequent aneurysm dilation that can
result in catastrophic rebleeding days or months
later.1 Delayed diagnosis leads to increased morbid-
ity and mortality, especially if rupture has occurred.
Iatrogenic aneurysm is a form of traumatic
aneurysm resulting from inadvertent direct injury to
the arterial wall following several neurosurgical
procedures. More often reported after trans-sphe-
noidal approach, it can also occur after ventricular
puncture, stereotactic biopsy, shunt insertion, or any
type of craniotomy.3–5 We report a case which
probably developed after peripheral vascular injury
during conventional craniotomy.
Case report
A 48-year-old woman was admitted to our depart-
ment with a spontaneous subarachnoid haemorrhage
due to a left middle cerebral artery aneurysm on the
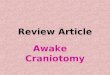
M1 segment (Fig. 1A). The patient underwent
conventional pterional craniotomy and clipping. No
intercurrence occurred during surgery, except for
minor bleeding during dural closure; this was con-
trolled by irrigation. Post-operative CT showed no
abnormality. Postoperative evolution was uneventful.
A routine clip control angiogram performed 6 months
later showed a small aneurysm in the orbitofrontal
branch of the middle cerebral artery. This aneurysm
presented irregular contours, late filling in the arterial
phase, and slow emptying (Fig. 1B). The craniotomy
was reopened and the aneurysm was located in the
lateral part of the orbital surface of the left frontal
lobe, adhering to the inner surface of the duramater
and close to the suture line.
The parent vessel was completely involved by the
aneurysm in a globular fashion. Proximal and distal
ends of the aneurysm were trapped with clips and
excised. Histopathology showed evidence of recent
thrombus in the aneurysm lumen, absence of elastic
lamina and lymphomononuclear inflammatory reac-
tions, siderophils, and mucoid degeneration. These
findings were consistent with a true or dissecting type
aneurysm. Postoperative evolution was uneventful.
Discussion
Iatrogenic traumatic aneurysm can be histologically
classified as true, false, mixed, or dissecting.1–3,5
False aneurysms are more common and result from
the disruption of all 3 vessel wall layers and
hematoma formation, which stops the bleeding by
Correspondence: Marco Antonio Zanini, Department of Neurology, Botucatu Medical School, Sao Paulo State University (UNESP), 18618-970, Botucatu, SP,
Brazil. Tel: þ55 (14) 3814-1299. Fax: þ55 (14) 3811-5965. E-mail: [email protected]
Received for publication 3 August 2009. Accepted 15 November 2009.
British Journal of Neurosurgery, April 2010; 24(2): 214–215
ISSN 0268-8697 print/ISSN 1360-046X online � The Neurosurgical Foundation
DOI: 10.3109/02688690903507505
Br
J N
euro
surg
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.

counterpressure. The blood causes an inflammatory
reaction in the surrounding tissues, with formation of
a fibrous capsular wall and aneurysmal dilation. True
aneurysms arise from variable disruption of the
internal elastic layer and media with an intact
adventitia forming the outer wall of the aneurysm.
Mixed aneurysm is formed after rupture of a true
aneurysm giving rise to a secondary false aneurysm.
A dissecting aneurysm can result from luminal shear
forces and secondary arterial dissection leading to
aneurysm dilation. The relative incidence of these
histological types is not known1
and all of them may
be saccular or fusiform in shape.2
In our case, traumatic origin was defined by
post-surgical development, cortical location, and
angiographic features. An inadvertent direct injury
to the cortical vessel during dural closure was
probably the cause of arterial wall fragility allowing
aneurysm dilation. However, a dissecting lesion to
the cortical vessel during spatula retraction causing
vascular injury and aneurysm could not be ruled
out.
Unlike traumatic aneurysm after head trauma, the
real incidence and natural history of traumatic
aneurysm following intracranial surgery is not well
defined in literature. Although some of these
aneurysms may gradually expand and rupture in a
few weeks or months, others may spontaneously
empty and disappear.5 Considering the risk of late
bleeding, iatrogenic post-craniotomy aneurysm
should be promptly treated. In our case, the
iatrogenic aneurysm presented a silent course and
was only discovered after a routine control angio-
graphy.
Conclusion
Taking into account the number of craniotomies
performed every day around the world, iatrogenic
post-craniotomy aneurysm is extremely rare with
only anecdotal cases reported in literature, suggest-
ing that they may be silent or under diagnosed. To
our knowledge, this is the first case describing a true
iatrogenic aneurysm in the cortical branch of the
middle cerebral artery due to arterial injury during
duramater suture. This case highlights that if any
bleeding is seen during dural closure, the dura needs
reopening to discover what precisely has occurred
and to secure hemostasis.
Declaration of interest: The authors report no
conflicts of interest. The authors alone are respon-
sible for the content and writing of the paper.
References
1 Dubey A, Sung WS, Chen YY, et al. Traumatic intracranial
aneurysm: a brief review. J Clin Neurosci 2008;15:609–12.
2 Jenkinson MD, Basu S, Broome JC, Eldridge PR, Buxton N.
Traumatic cerebral aneurysm formation following ventriculo-
peritoneal shunt insertion. Childs Nerv Syst 2006;22:193–6.
3 Dunn IA, Woodworth GF, Siddiqui AH, et al. Traumatic
pericallosal artery aneurysm: a rare complication of transcallosal
surgery. J Neurosurg (2 suppl Pediatrics) 2007;106:153–7.
4 Stoodley MA, North JB, Reilly PL, Blumbergs PC, Sandhu A,
Cohen PA. False aneurysm following intracranial surgery. Br J
Neurosurg 1994;8:599–602.
5 Tokunaga K, Kusaka N, Nakashima H, Date I, Ohmoto T. Coil
embolization of intradural pseudoaneurysms caused by arterial
injury during surgery: report of two cases. Am J Neuroradiol
2001;22:35–9.
FIG. 1. Left internal carotid angiograms oblique view. (A) Admission angiogram demonstrating an aneurysm of the M1 segment of the
middle cerebral artery at the origin of an early temporal branch. No other cortical aneurysm is present. (B) Routine control angiogram 6
months after craniotomy showing an irregular filled aneurysm in the orbitofrontal branch (cortical) of the middle cerebral artery (arrow). The
M1 aneurysm was excluded from circulation.
Iatrogenic cortical aneurysm post-craniotomy 215
Br
J N
euro
surg
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f T
oron
to o
n 11
/27/
14Fo
r pe
rson
al u
se o
nly.