Embed Size (px)
Citation preview

1
I’m in Denial: CDI’s New Role in Denials Management
Shirlivia Parker, MHA, RHIA, CDIPRegional Clinical Documentation Integrity Physician EducatorPSJH Shared ServicesIrvine, CA
Kimberly Huff, BA, CPC‐H, CCDS Clinical Denials Lead CDI/Clinical Documentation Quality AuditorPSJH/Harmony Healthcare, LLCMountain Pine, AR
With contributions from Christopher Zepeda, MHA, BS, CPCExecutive Director of CDI, PSJH Shared Services
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

2
Learning Objectives
• At the completion of this educational activity, learners will be able to:– Differentiate the various types of denials seen in healthcare– Assess their organization’s infrastructure & identify key stakeholders to utilize in a clinical validation denials program
– Outline the steps for implementation of a successful clinical validation denials program
– Apply the appeal letter “tips” (provided within this session) to create appeal templates of their own
– Employ strategies for clinical validation denial prevention– Recognize the importance of collaboration in denial prevention
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

3
Agenda
• Explanation and understanding of different types of denials• Overview of inpatient vs. outpatient denials• An in‐depth definition of clinical validation• Implementing a denials management program• Essential tools for your denials management program and denials prevention
• Next steps: Lessons learned
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

4
PSJH continues a tradition of caring that began 175 years ago
#1 or 2 provider in all our markets
50 hospitalsAmbulatory
7 statesAcuteFootprint
18 ASCs | 800+ clinics
Ranking
20k physicians8M visits
117Kcaregivers
$23Bin 2017
$1.6B benefit
RevenueReachCare Community
6 elite research institutes
20+ incubated investments
12+ HIT companies
ReachInnovation Partnerships Rating AA investor rating 5‐starMedicare Advantage
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

5
Exec Director CDI
Director CDI
QVMC SJE/RMH PVH SRM SJO
SJMC
SMMC
MRH
CMC Children's LEV PLV
CDQI
SJE/RMH
QVMC
SRM/PVH
SJO
MRH
CMC
Physician Educator Team
SCAL Region (1)
NCAL Region (1)
Tx Region (1)
CDI Educator Team
SCAL Region (1)
NCAL Region (1)
Tx Region (1)
CDI Program Manager
CDI Organizational Structure – SJH Legacy
Denials process discussed in this presentation impacts these facilities only and was established in CY 2018
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

6
Abbreviations Used During This Presentation
• PSJH: Providence St. Joseph’s Health• PFS: Patient financial services• CDI: Clinical documentation integrity• LCD: Local coverage determination• CEBD: Clinical evidence‐based definitions• CPGs: Clinical practice guidelines• EHR: Electronic health record• ROI: Release of information• CV: Clinical validation• CY: Calendar year
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

7
Explanation & Understanding of Different Types of Denials• Review the various types of denials • Discuss how clinical validation denials are a distinct entity • CDI’s role in denials
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

8
There Are 5 Types of Denials
• Medical necessity: The payer has determined that the patient’s clinical picture does not warrant an inpatient admission.
• DRG/coding denial: The payer has (or believes they have) identified a coding error that impacts DRG assignment. This may include but is not limited to: principal or secondary diagnosis code assignment, sequencing guidelines, procedural reporting, etc.
• Technical denial: The claim has been rejected for non‐medical reasons. This may include but is not limited to: authorization for the admission or procedure was not obtained in a timely fashion, medical records requested by the payer were not submitted, etc.
• Outpatient claim denial: This can occur for a multitude of reasons that include but are not limited to: incorrect procedure code assignment, incorrect modifier usage, MUE (medically unlikely edits), non‐covered services, medical necessity not met (LCD), etc.
• Clinical validation denial: The payer has determined that 1 or more diagnoses documented within the record could not be clinically substantiated, i.e. clinical findings &/or treatment rendered do not/does not clinically validate the diagnosis(es) in question.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

9
Clinical Validation Denials Are a Detour From Conventional DRG Validation Denials
• The following guidance pertains to traditional DRG validation denials:– ICD‐10 Official Guidelines for Coding and Reporting state in Section I.A.19:Code assignment and clinical criteria: The assignment of a diagnosis code is based on the provider’s diagnostic statement that the condition exists. The provider’s statement that a patient has a particular condition is sufficient. Code assignment is not based on clinical criteria used by the provider to establish the diagnosis.
• However, a different set of rules apply to clinical validation:‒ Both the CMS (Centers for Medicare & Medicaid Services) Recovery Audit
Contractors Scope of Work document & the AHIMA practice brief “Clinical Validation: The Next Level of CDI” describe clinical validation as a process involving “a clinical review of the case to see whether or not the patient truly possesses the conditions that were documented in the record.”
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

10
Coding Clinic for ICD‐10‐CM/PCS, Fourth Quarter 2016 Pages 147–149: Clinical criteria and code assignment
Question:Please explain the intent of the new ICD‐10‐CM guideline regarding code assignment and clinical criteria that reads as follows: "The assignment of a diagnosis code is based on the provider's diagnostic statement that the condition exists. The provider's statement that the patient has a particular condition is sufficient. Code assignment is not based on clinical criteria used by the provider to establish the diagnosis." Some people are interpreting this to mean that clinical documentation improvement (CDI) specialists should no longer question diagnostic statements that don't meet clinical criteria. Is this true?
Coding Clinic provided a 3‐paragraph response which includes (but is not limited to):• Coding must be based on provider documentation. … Only the physician, or other qualified healthcare
practitioner legally accountable for establishing the patient's diagnosis, can "diagnose" the patient.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

11
Coding Clinic for ICD‐10‐CM/PCS, Fourth Quarter 2016 Pages 147–149: Clinical criteria and code assignment (cont.)Coding Clinic response continued:• The guideline noted addresses coding, not clinical validation. It is appropriate for facilities to ensure
that documentation is complete, accurate, and appropriately reflects the patient's clinical conditions. The distinction is described in the Centers for Medicare & Medicaid (CMS) definition of clinical validation from the Recovery Audit Contractors Scope of Work document and cited in the AHIMA Practice Brief ("Clinical Validation: The Next Level of CDI") published in the August issue of JAHIMA: “… Clinical validation involves a clinical review of the case to see whether or not the patient truly possesses the conditions that were documented in the medical record.”
• While physicians may use a particular clinical definition or set of clinical criteria to establish a diagnosis, the code is based on his/her documentation, not on a particular clinical definition or criteria. In other words, regardless of whether a physician uses the new clinical criteria for sepsis, the old criteria, his personal clinical judgment, or something else to decide a patient has sepsis (and document it as such), the code for sepsis is the same—as long as sepsis is documented, regardless of how the diagnosis was arrived at, the code for sepsis can be assigned. … A facility or a payer may require that a physician use a particular clinical definition or set of criteria when establishing a diagnosis, but that is a clinical issue outside the coding system.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

12
Why Are CDI Professionals a “Perfect Fit” for Clinical Validation Denial Reviews & Appeals?
• “Clinical validation means that diagnoses documented in a patient's record must be substantiated by clinical criteria generally accepted by the medical community. Generally accepted clinical criteria typically come from authoritative professional guidelines, consensus, or evidence‐based sources.”
• “If clinicians do not consider the clinical validity of diagnoses for the codes submitted on claims, they will not be in compliance with CMS regulations and policy, will be potentially exposed to claims denials, may be subject to regulatory inquiry and sanctions, and in rare circumstances may be vulnerable to serious allegations of submitting false claims. Hospitals and clinicians must ensure that only codes for “clinically valid” diagnoses are submitted on their claims. The False Claims Act of 1863 imposes severe penalties for the submission of claims to the U.S. government for goods or services not actually rendered.” Source: Dr. Richard Pinson https://www.acphospitalist.org/archives/2016/12/coding‐clinical‐validation.htm
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

13
Why Are CDI Professionals a “Perfect Fit” for Clinical Validation Denial Reviews & Appeals? (cont.)
• Points to ponder:– A record can include a consistently documented diagnosis (beginning in the ER, throughout the stay, as well as the discharge summary) … but if the clinical findings &/or treatment provided do not substantiate the diagnosis in question, you are at risk of a clinical validation denial.
– Clinical validation denials (and appeals) require both a clinically astute mind and an advanced knowledge of DRG methodology. Reconciling records for abnormal findings & determining if the treatment rendered supports a given diagnosis are inherent to the role of CDI.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

14
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

15
Polling Question 1
• As a CDI professional, have you played an integral role in establishing a denials management program?– Yes– No
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

16
Implementing Your Clinical Validation Denials Program• Outlining a workflow • Establishing roles/responsibilities• Key contacts with the process
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

17
Recognized the need
Set the stage by
identifying types
of denials
Worked with PFSto understand
revenue associated with each type of
denial
Distinguished types of denials in which CDI should be leveraged
Established monthly
meetings to implement and cultivate denials mgmt.
program
How Did We Start?
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

18
Coding CDI PFS
HIM/ROI Management Support
Physician Advisor
Whom Did We Identify as Key Stakeholders?
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

19
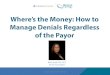
Clinical Validation Denials Process: Hospital #1
1. PFS biller receives denial letter.
2. Denial letter is sent to coding auditor & CDI.
3. CDI evaluates clinical documentation against CEBDs & official coding
guidance.
4. Final edits are made & appeal letter is sent to PFS
biller.
5. Physician advisor (PA) receives template &
provides a “statement” or input/suggestions.
6. Decision is made to appeal or accept denial. Appeal is written vs. PFS notified that
we agree with denial.
7. PFS biller submits appeal letter & applicable medical record documentation.
8. PFS biller monitors status of the appeal & continually updates CDI re: status of
appeal.
9. Continual communication between
CDI & directors of PFS/HIM, as well as exec
director of CDI.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

20
Clinical/DRG Validation denial letter is received by PFS
Step 1
PFS determines if the correspondence is a comprehensive medical record request vs. an inpatient or outpatient claim denial. This information is entered on the PFS spreadsheet & in
the billing/accounts receivable (BAR) section of the EHR.
Comprehensive medical record requests are
emailed to HIM director with letter attached.
Outpatient denials are emailed to HIM director & coding manager with
the denial letter attached.
Inpatient clinical/DRG validation denials (initial & continued denials) are emailed to the clinical
denials lead CDI with the denial letter attached.
If clinical denials lead CDI determines the denial to be coding/DRG validation in
nature it will be forwarded immediately to coding manager. The PFS denials spreadsheet will be updated..
If coding agrees with the denial: coding manager will notify PFS.
If coding wishes to appeal: Coding will prepare a comment/response & send it to clinical denials lead CDI, who will then
incorporate the response into a (uniform) template to maintain consistency.
Step 3
If the denial is based upon clinical validation (CV), the clinical denials lead CDI will review & appeal as
appropriate. BAR & the PFS spreadsheet will be updated throughout the process to keep PFS, etc. informed. Physician advisor will be leveraged for peer to peer–level appeals, as well as a 2nd opinion re: appeal vs. no
appeal, as needed.
If the CV team agrees with the
denial: PFS will be notified.
Step 2
If the CV team opts to appeal the denial: Appeal letter is sent to ROI & PFS is CCed. PFS spreadsheet is
updated.
1 week prior to the deadline: ROI receives the appeal letter & instructions re: supporting documents to send to the payer. ROI updates
PFS spreadsheet upon appeal submission.
Step 4
Step 5
Clinical Validation Denials Process: Hospitals #2–5
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

21
Writing Your First Appeal LetterTips to ensure success
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

22
Polling Question 2
• As a CDI professional, have you written an appeal letter in response to a clinical validation denial?– Yes, and the denial was overturned– Yes, but the denial was upheld– No, I haven’t written an appeal letter
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

23
Step 1: Identify the targeted diagnosis(es) & the payer’s rationale for
denial.
Step 2: Evaluate the record against your organization’s
CEBDs. If none exist, evaluate against widely
accepted CEBDs.
Step 3: Prepare the appeal letter, which should include 3 sections.
Section 1: Summarize the changes made by the payer, as well as their denial rationale.
Section 2: Identify clinical criteria & documentation
that validate the diagnosis(es).
Section 3: Cite the CEBD references that validate the diagnosis(es). Follow this with applicable official
coding guidance.
Reviewing the CV Denial & Preparing the Appeal Letter Summary
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

24
Step 1: Review the Denial Letter
• Identify the targeted diagnoses & the payer’s rationale for the denialExcerpt from a CV denial received by PSJH:
– Denial rationale: The provider assigned G93.40 Encephalopathy, unspecified as a secondary diagnosis. The clinical evidence in the medical record did not support the assignment of G93.40. It was noted that the physician documented encephalopathy in the discharge summary. After investigation, the physicians caring for this patient determined that the alteration in mental status (AMS) experienced by this patient was largely due to the patient’s underlying dementia. AMS associated with neurodegenerative processes should be coded from the F0#.## (dementia with delirium) series & not as encephalopathy. The discharge summary noted the patient was disoriented with a GCS of 14 until discharge on (date redacted). The discharge summary noted the patient returned to baseline mental status & was doing well per family members. There was insufficient clinical evidence & supportive documentation in the records available for review to substantiate the coding of this condition. Therefore, as a result of this review, the diagnosis code(s) G93.40 has been removed from the claim.
– References cited: ICD‐10‐CM Official Guidelines, Section I.B.5, Conditions that are integral part of a disease process; Coding Clinic, Third Quarter 2009, p. 11, Acute Delirium due to Dementia.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

25
Step 2: Research & Development
• A complete medical record review should be conducted for any and all denials. This includes:– Physician orders – Medications (home medication & those given throughout the hospital course)– Laboratory reports (including historical labs, for example baseline creatinine), vital signs, & intake/output
records– Radiology report, nursing notes, other specialty notes (PT, nutrition, etc.) – All physician documentation
• Evaluate the record against your organization’s CEBDs. If none exist, evaluate against widely accepted CPGs.
• Review of this record by the clinical denials lead CDI revealed the following:– Diagnoses for the admission included dementia, UTI, & dehydration– Medications administered included IVF’s, Rocephin®, and Levaquin®– Physician documentation consistently included a diagnosis of acute encephalopathy – Physician documentation specifically stated, “Acute encephalopathy secondary to urinary tract infection,
dehydration, and dementia”
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

26
Step 3: Preparing the Letter• Section 1: Summarize the changes made by the payer, as well as their denial rationale. Pay close
attention to the references they use.
Excerpt from a PSJH clinical validation denial appeal letter:
Dear Reviewer:
We request reconsideration of the Clinical Validation denial of patient ___’s claim (claim number ___).
As per your review, secondary diagnosis G93.40, Encephalopathy, unspecified was removed. This results in a DRG change from DRG ___to DRG ___.
The denial rationale includes the following declarations: • The physician documented encephalopathy due to UTI, dehydration, and dementia within the discharge summary.• After investigation, the physicians caring for the patient determined that the alteration in mental status was largely due to the
patient’s underlying dementia.• AMS associated with neurodegenerative processes should be coded from the F0#.## (dementia with delirium) series and not as
encephalopathy.• Discharge summary noted the patient returned to baseline mental status & was doing well per family members.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

27
Step 3: Preparing the Letter (cont.)• Section 2:
– Identify clinical criteria & documentation that validate the diagnosis(es) and insert into your appeal letter.
Excerpt from a PSJH clinical validation denial appeal letter:
Below are significant medical record entries relevant to the patient’s diagnosis of encephalopathy: H&P: Using a customized template, the reviewer’s attention was drawn to the following (diagnosis specific) clinical findings:
From the HPI, review of systems & exam section, I focused on documentation of/including: ‐”REASON FOR ADMISSION”: Hallucinations and abnormal speech ‐Babbling & incoherent on exam‐History of bronchioalveolar cell carcinoma ‐ ongoing treatment ‐Known metastatic disease to bone‐Yesterday he became acutely not himself ‐Hallucinating, aggressive, labile‐He is unable to provide any history ‐Unable to perform review of systems due to mental status
From the Assessment & Plan section, I targeted the following:‐Likely had a frontal CVA or has an infectious encephalopathy or has metastasis to his brain.‐Labile behavior. This patient has multiple reasons that this may be occurring. I will put him on some antibiotics in case he has a urinary tract infection. ‐Hallucinations. He is somewhat labile. I am going to write for some p.r.n. anxiolytics as well as antipsychotics.‐Metastatic lung cancer.‐Urinary tract infection. It potentially is cause of his current symptoms. I will continue with some antibiotics.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

28
Step 3: Preparing the Letter (cont.)Section 2: Identify clinical criteria & documentation that validate the diagnosis(es).
Excerpt from a PSJH clinical validation denial appeal letter
Discharge Summary: Using a customized template, the reviewer’s attention was drawn to the following (diagnosis specific) clinical findings:
From the HPI section, I focused on documentation of/including: ‐Presented on 05/06/2017 for hallucination and abnormal speech‐Patient had acute deterioration and was unable to produce sensible speech‐Given acute encephalopathy of unclear etiology, patient was admitted to the hospitalist service
From the Hospital Course section, I targeted:‐Urinalysis showed mild UTI. Patient was placed on Ceftriaxone on admission & had good improvement of his clinical symptoms.‐Patient was also placed on IV fluids given patient had poor p.o. intake initially with acute encephalopathy. ‐Following antibiotics & IV fluids, the patient had significant improvement of his symptoms.‐Following his clinical improvement (post antibiotics & IV fluids), the patient was found to have significant memory deficits consistent with dementia. ‐Patient was discharged on Levaquin 500 mg p.o. daily for 5 days.
From the Discharge Diagnoses section, I focused on the following documentation:‐Acute encephalopathy secondary to urinary tract infection, dehydration, and dementia‐Urinary tract infection with E. coli‐Dementia
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

29
Step 3: Preparing the Letter (cont.)
• Section 3: Cite the CEBD references that validate the diagnosis(es). Follow this with applicable official coding guidance.
Excerpt from a PSJH clinical validation denial appeal letter:
The Coding Clinic referenced by the reviewer (Acute Delirium due to Dementia 3rd Quarter 2009, pages 11–12) states:Question: The patient is an 87‐year‐old male with a documented history of dementia, who was admitted to the hospital with transient
changes in his mental status following a medical procedure. He was transferred to a subacute rehab facility for further management of acute delirium and behavior problems. The transfer summary listed delirium secondary to dementia as the final diagnosis. What is the appropriate code assignment for delirium due to dementia? I am reluctant to use code 290.3, Senile dementia with delirium, since the provider does not specifically document senile dementia.Answer: Query the provider regarding the type of dementia (e.g., senile dementia, pre‐senile dementia, etc.) and code accordingly. If the
provider confirms that the patient has senile dementia with delirium, assign only code 290.3, Senile dementia with delirium. If the cause of the delirium or the type of dementia is not known, assign code 294.8, Other persistent mental disorders due to conditions classified elsewhere, and code 293.0, Delirium due to conditions classified elsewhere. Please note that the Coding Clinic referenced by the reviewer does not include a diagnosis of encephalopathy. Coding
guidance instructs us to code to the highest degree of specificity. Therefore, more specific guidance should be sought.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

30
Step 3: Preparing the Letter (cont.)
This CV denial was OVERTURNED at the primary level of appeal.
• Section 3: Cite the CEBD references that validate the diagnosis(es). Follow this with applicable official coding guidance.‒ Multiple clinical articles (which validated the diagnosis of encephalopathy) were cited in this appeal:
Excerpt from a PSJH clinical validation denial appeal letter:
1) UpToDate “Acute toxic‐metabolic encephalopathy in adults” by Dr. Chalela & Dr. Kasner:• For presentation purposes, this citation has been summarized‐Acute toxic‐metabolic encephalopathy (TME) encompasses delirium & the acute confusional state‐Possible risk factors for TME include infection‐Common findings include hallucinations, disorientation, rambling speech, anxiousness, & agitation‐Acute TME is a diagnosis of exclusion within a broad differential diagnosis‐Treatment of TME focuses primarily on correcting the underlying condition‐TMEmanifests clinically as a delirium with agitated confusion or somnolence
Again, we wish to note that the patient’s mental status did not improve until after the patient’s UTI, dehydration, and hyperkalemia had been treated.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

31
Payer Tactics Oh, the games they play …
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

32
Payer Tactics: Legacy SJH Trends Identified
Appeals are a lengthy, resource‐consuming process. Resolution is not always achieved. But we must start the process in order to identify denial trends. This in turn reveals contracting opportunities (such as establishing clinical criteria,
improving your appeals process, etc.).
Medicare Advantage (MA)• Payment may be recouped prior to appeal
process completion.• MA claims are evaluated using Sepsis‐2 criteria.• Review entities (working on behalf of UHC, etc.)
deny claims despite clinical documentation validating satisfying Sepsis‐2 criteria.
• Appeals process is: Written appeal peer‐to‐peer (with review agency) Review by MA medical director
Commercial Payers• Payment may be recouped prior to
appeal process completion.• Commercial claims are evaluated using
Sepsis‐3 criteria.• Commercial payers often include
UR/UM medical necessity appeals as part of the CV appeals process. This in turn allows us to write only one appeal letter in response to a CV denial.– We are working with contracting to improve this
practice.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

33
Sepsis Review by Auditing Company: Targeting Payer Tactics Auditor’s Initial Appeal Response
• We acknowledge that physician documentation includes a diagnosis of sepsis.
• We do not agree that >/= 2 SIRS inclusively clinically support a diagnosis of sepsis.
• In order to accept an elevated lactic acid as evidence of organ dysfunction or hemodynamic compromise, we expect to see a lactate in excess of 3.
• We expect consistent documentation of a systemic response beyond that expected with pneumonia.
• A diagnosis of pneumonia combined with a WBC of 31,000; a temperature of 102.2, & a lactate of 2.9 is not deemed to be sufficient clinical evidence of sepsis.
• Denial upheld.
Auditor’s Second Appeal Response• Confirmed that sepsis was evaluated against Sepsis‐2
criteria. • We acknowledge that physician documentation includes a
diagnosis of sepsis. However, we do not agree that >/= 2 SIRS criteria clinically supports a diagnosis of sepsis.
• In order to accept an elevated lactic acid as evidence of organ dysfunction or hemodynamic compromise, we expect to see a lactate in excess of 3.
• We expect consistent documentation of a systemic response beyond that expected with pneumonia.
• A diagnosis of pneumonia combined with a WBC of 31,000; a temperature of 102.2, & a lactate of 2.9 not deemed to be sufficient clinical evidence of sepsis.
• We expect treatment and LOS (length of stay) to be consistent with a diagnosis of sepsis.
• Denial upheld.
This was a Medicare Advantage (MA) denial. It was OVERTURNED by the MA medical director following a peer‐to‐peer discussion.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

34
Example of Sepsis (Denial) Appeal Time Frame: We Won
9/21/17 Denial received & sent to CDI auditor for
review.
10/5/17CDI auditor appeal letter sent to PFS.
11/6/17 Initial appeal letter sent to review agency.
12/7/17 Appeal dismissed d/t ‘filed outside of 60 day time frame.’ This was clearly
incorrect.
2/5/18 2nd appeal letter sent to review
agency.
3/14/18 PFS calls review agency d/t lack of response to 2nd appeal. They deny receipt
of letter.
3/20/18 2nd appeal denied.
4/11/18 Peer to peer call with review agency’s medical director. Continued denial. Requested review by payer’s medical
director.
6/1/18 Denial overturned by payer’s medical
director.
Consider this: What if we had language in our contracts? Could this 9‐month process have
been eliminated?
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

35
Collaboration: The Key to Denials PreventionWe are all on the same team. So, what can we do to prevent CV denials from occurring?
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

36
PSJH: Collaborating to Prevent CV Denials
Clinical denials lead
CDI
Physician education
CDI education
Service line lead (i.e. registered dietitian mgr.)
In a collaborative effort, the clinical denials lead CDI shares observations made during denial reviews to allow for targeted education of staff. Denial rationale feedback is welcomed by these leaders.Every denial is an educational opportunity!
• Template suggestions• Diagnosis specific tips for
strengthening MDM documentation
• Inappropriate queries• Missed opportunities to
strengthen clinical documentation
• Template suggestions to strengthen the clinical validity of diagnoses such as malnutrition & obesity
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

37
Next Steps and Recommendations
• At PSJH, we are now collaborating with our legal teams. This collaborative effort includes, but isn’t limited to, working towards modifying payer contracts. Contract modifications will ultimately result in CV denial prevention.
• Topics you may wish to consider (when speaking to your contracting team) include:– Establishing an appeals process that is beneficial to your organization
For example: Mandating that after 1 written appeal your denials team can begin communicating directly with the payer (vs. continued appeals to a review agency).
– Establishing clinical evidence‐based definitions as an organizationAgreed‐upon CEBDs should then be included in payer contracts.
Contracts are compelling … do what you can to make them work for you.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

38
Clinical Validation: CY 2018 Outcomes & DataOverturn rate & denied opportunities
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

39
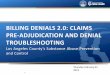
CV Denials: CY 2018 Appeals & Overturn Rate
Appealed, 37
Overturned, 13
Under Review, 2
Pending, 14
Upheld, 8
**Agreed with Denial, 18
Overturn Rate, 35%
Appealed
Overturned
Under Review
Pending
Upheld
Agreed with Denial
Overturn Rate
0 5 10 15 20 25 30 35 40
**Agreed with Denial = we accepted the denial. When this occurs, we view the denial as an educational opportunity. Findings are utilized to educate CDI staff and network with other departments (RDs) and/or physicians.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

40
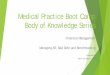
CV: 2018 Denied Opportunities
1211
665443211
55
0 10 20 30 40 50 60
SepsisMalnutrition
EncephalopathyOther
Multiple Dx.AKI
Diagnosis Sequencing (CDQI Reviews)Respiratory Failure
CHFABLA
Procedure Choice
Total
CV denials are our focus; however, we do help coding (if requested) with their denials.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

41
Evidence‐Based Clinical DefinitionsASPEN, Sepsis‐2, & Sepsis‐3
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

42
• Sepsis = suspected or confirmed infection + >/= 2 or more
of the following:
Temp > 100.4 or < 95.0
RR > 20 or PaCO2 < 32 mmHg
HR > 90/min
WBC > 12,000 or < 4,000
This definition of sepsis is used primarily by Medicare &
Medicare Advantage plans.
• Identifies potential sepsis cases via the use of SOFA
(Sequential Organ Failure Assessment) or qSOFA (quick
SOFA).
SOFA: grades the function of 6 organ systems
(respiratory, hematology, hepatic, cardiovascular, CNS,
& renal) on a scale of 0–4 depending upon the
severity of dysfunction using established
measurements.
qSOFA: a score of >/= 2 criteria indicates an increased
risk of a poor outcome.
Altered mental status
RR > 22/minute
Systolic BP < 100 mmHg
This definition of sepsis is used primarily by commercial
plans.
Sepsis‐2 Criteria Sepsis‐3 Criteria
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

43
ASPEN CriteriaRequired: Two or more characteristics • Six characteristics are:
1. Insufficient energy intake2. Weight loss (see #5)3. Loss of muscle mass4. Loss of body fat5. Localized or generalized fluid
accumulation that can mask weight loss (alternative to #2)
6. Diminished functional status as measured by a hand grip (strength) device
Required: One clinical context • Three clinical contexts are:
1. Chronic illness (duration of 3 months or more) such as widespread metastatic cancer, severe malabsorption syndromes, HIV, or chemotherapy
2. Social/environmental circumstance; such as severe debilitation, elderly patient living alone without social support, or lack of care
3. Acute illness or injury (duration of < 3 months) such as GI surgery, multi‐system trauma, intubation, prolonged vomiting, or limited oral food intake
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

44
KDIGO: Acute Kidney Failure Clinical Criteria
• Increase in SCr by x 0.3 mg/dl (x26.5 lmol/l) within 48 hours; OR• Increase in Scr to x 1.5 baseline, which is known or presumed to have occurred within the prior 7 days; OR
• Urine volume < 0.5 ml/kg/h for 6 hours
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

45
References
• ICD‐10‐CM Official Guidelines for Coding and Reporting: https://www.cms.gov/Medicare/Coding/ICD10/2018‐ICD‐10‐CM‐and‐GEMs.html
• AHA Coding Clinic: http://www.ahacentraloffice.org/• RAC Scope of Work: https://www.cms.gov/Research‐Statistics‐Data‐and‐
Systems/Monitoring‐Programs/Medicare‐FFS‐Compliance‐Programs/Recovery‐Audit‐Program/
• AHIMA Practice Brief “Clinical Validation: The Next Level of CDI”: http://library.ahima.org/doc?oid=301756#.XCuxR5V0xVA
• The False Claims Act of 1863: http://uscode.house.gov/view.xhtml?req=(title:31%20section:3729%20edition:prelim
• KDIGO criteria: https://kdigo.org/wp‐content/uploads/2016/10/KDIGO‐2012‐AKI‐Guideline‐English.pdf
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.

46
Thank you. Questions?
[email protected]@stjoe.org
In order to receive your continuing education certificate(s) for this program, you must complete the online evaluation. The link can be found in the continuing education section of the program guide.
2019 Copyright, HCPro, a division of Simplify Compliance LLC, and/or session presenter(s). All rights reserved. These materials may not be copied without written permission.