Embed Size (px)
Citation preview

Prepared by theJoint IAEA/WHO Secretariat
of the SSDL Network
Published by theInternational Atomic Energy Agency
Vienna
ISSN 1011-2669
No. 40 January 1999
IAEA/WHONETWORK OFSECONDARY
STANDARDDOSIMETRY
LABORATORIES
EDITORIAL NOTE .........................................................................2
DOSE DETERMINATION WITH PLANE-PARALLEL
IONIZATION CHAMBERS IN THERAPEUTIC
ELECTRON AND PHOTON BEAMS ....................................4
REPORT OF THE EIGHTH MEETING OF THE
SCIENTIFIC COMMITTEE OF THE IAEA/WHO
NETWORK OF SSDLs........................................................17
COURSES AND MEETINGS TO BE HELD
DURING 1999 .....................................................................31
MEMBER LABORATORIES OF THE IAEA/WHO
NETWORK OF SSDLs........................................................32

2
EDITORIAL NOTE
The Agency has decided to standardize the format of all its Newsletters and we have taken thisopportunity to change the layout of the cover page. The new A4 format was changed at the time ofpublishing the issue No. 38, in July 1998. Two months later, issue No. 39 was also published with the dateof July 1998. Readers have probably noticed this unfortunate mistake. In fact, many readers have expressedtheir confusion regarding the time delay between the date on the cover page of the Newsletter and the dateof its effective publication by the Agency. This time delay has now been resolved and hopefully all futureissues will be published on time, one in January and the other in July of each year.
The Code of Practice IAEA TRS-381 complements and extends the IAEA TRS-277. It describesprocedures that may be used to calibrate plane-parallel chambers against air kerma or absorbed dose towater standards at 60Co gamma ray energy, in order to obtain the absorbed-dose-to-air chamber factor (ND,air)or the absorbed dose to water chamber factor (ND,w). This Code of Practice also updates some of the dataand concepts presented in TRS-277. Soon after the publication of this report, the Agency has launched a Co-ordinated Research Project (CRP) to ascertain that the Code of Practice meets the highest scientificstandards and yields the most accurate results available today. Furthermore, the CRP should offer anopportunity to quantify the differences with the existing recommendations and analyze the possible impactin patient dosimetry. The first Research Co-ordination Meeting (RCM) of this CRP was held in Vienna, 2-5December 1996 and its report published in this Newsletter (No. 36, January 1997). The report of the SecondRCM, held in Barcelona 30 March-3 April 1998 is published in this issue.
The second article is the report of the 8th SSDL Scientific Committee meeting held during 5-9 October1998. The editor wishes to draw the readers' attention to the recommendations of the Scientific Committee.The recommendation “h” to ensure that all SSDLs of the Network comply with the requirements of theSSDL Network Charter will be implemented. In particular, SSDLs that have not yet participated in theAgency audit programmes (TLD or ionization chamber) are highly advised to do so during this year. TheSSDL Scientific Committee also recommends to evaluate the potential use of the calibration services indiagnostic radiology and brachytherapy. For that purpose, the Secretariat of the IAEA/WHO network hasprepared a survey form to be sent to all SSDLs of the network. It is hoped that the network members will fillthe questionnaire and return it to the Secretariat as soon as possible.
All SSDLs, members of the network, are reminded that the Agency’s Dosimetry Laboratory providescost-free calibration services of reference standards for radiotherapy (external and brachytherapy) andradiation protection (including environmental) dose levels. Interested SSDLs are invited to send a request tothe Secretariat for scheduling.
We have observed that the long-term stability of some PTW chambers (type 30001 and 31003)calibrated at the Dosimetry Laboratory has varied up to 1.4%. Comparable results obtained at other SSDLshave been reported to us. PTW was requested to investigate and correct this anomalous behaviour. InNovember 1998, a Technical Note1 D165.200.0/1 on the “Long-term stability of PTW-Ionization Chambers”was prepared by PTW, where the lack of constancy was attributed to an ageing effect of the chambermaterials used during the years 1993-1997. PTW is now using pre-aged parts and chambers delivered in1998 or later should no longer show that behaviour. It is strongly recommended to check the stability of theresponse of all chambers of these types against an ion chamber of well known stability and re calibrate themas often as possible till stability is reached. Readers are encouraged to report the results of their checks ontheses types of chambers to the Secretariat of the network.
The title of the Department of Research and Isotopes (RI) has been changed to “Department ofNuclear Sciences and Applications” (NA), effective 8 December 1998. Consequently, the abbreviation ofthe Division of Human Health changes from RIHU to NAHU and that of the Agency Laboratories fromRIAL to NAAL.
Finally, the Secretariat of the IAEA/WHO network wishes a happy new year to all its members andreaders of this Newsletter.
1 Copies of this note are available on request from the Secretariat of the Network.

3
The present staff at the Dosimetry and Medical Radiation Physics (DMRP) Section is:
Name Position/tasks E-mail address
Andreo, Pedro Head, DMRP Section [email protected]
Bera, Pranabes Laboratory Technician (TLD) [email protected]
Czap, Ladislav Laboratory Technician
(Ionization chamber calibration)
Girzikowsky, Reinhard Laboratory Technician
(high dose dosimetry)
Izewska, Joanna TLD Officer,
Head, Dosimetry Laboratory Unit
Meghzifene, Ahmed SSDL Officer,
Editor SSDL Newsletter
Mehta, Kishor Radiation Processing (high dose)
Dosimetry Officer
Nagaoka, Kazonuri Laboratory Physicist (TLD)
(TA)
Pernicka, Franticek Diagnostic Radiology DosimetryOfficer (TA)
Toelli, Heikki Brachytherapy Dosimetry Officer [email protected]
Salzer, Annelise Secretary [email protected]
Brooks, Alli Orvokki Secretary
(TA)
DMRP Section [email protected]
a This is the general e-mail address of the DMRP Section where all correspondence not related to specific tasks of the
staff above should be addressed. Please note also that there is a considerable circulation of the staff of the Agency, sothat messages addressed to someone who has left might be lost. All incoming messages to this mailbox are internallydistributed to the appropriate staff members.

4
DOSE DETERMINATION WITHPLANE-PARALLEL IONIZATIONCHAMBERS IN THERAPEUTICELECTRON AND PHOTON BEAMS
Report of the 2nd Research Co-ordinatedMeeting (326-E2-RC-641.2), March 30-
April 3, 1998 Barcelona, Spain
Scientific Secretary: P. AndreoDosimetry and Medical Radiation Physics Section,
NAHU
SCIENTIFIC BACKGROUND
In 1987, the IAEA published a report entitled“Absorbed Dose Determination in Photon andElectron Beams: An International Code of Practice”(IAEA Technical Reports Series No. 277) to adviseusers how to obtain the absorbed dose in water fromthe measurements made with an ionization chamber,calibrated in terms of air kerma. For high-energyphotons (energies above 1 MeV) the chambercalibration was at a single photon quality (Cobalt-60gamma rays). The Code of Practice describedprocedures and provided data to use such ionizationchambers to obtain absorbed dose for higher energyphotons and also for electron beams. It was sodesigned that a variety of cylindrical chamberscould be used, which represented the existingconditions world-wide. However, most national andinternational dosimetry protocols recognized theadvantages of plane-parallel ionization chambers,explicitly for electron beams and especially low-energy electron beams (below 10 MeV). Althoughthis was acknowledged in TRS-277, the calibrationand use of these chambers were not fully developed.
Since the publication of TRS-277 in 1987, variousrecommendations for the specific procedures for theuse of plane-parallel ionization chambers have beenpublished. Additional knowledge about the use ofcylindrical chambers has also appeared.Accordingly, the IAEA formed an internationalworking group that prepared a new Code of Practicefor the calibration and use of plane-parallelionization chambers. The new Code of Practice waspublished in 1997 as IAEA TRS-381, whichcomplements and extends IAEA TRS-277. It
describes options on how to calibrate plane-parallelchambers against air-kerma or absorbed dose towater standards at Cobalt-60 gamma ray energies, inorder to obtain ND,air, the absorbed-dose-to-airchamber factor, or ND,w, the chamber absorbed dosecalibration factor, respectively. The procedure forthe use of these chambers to calibrate therapeuticelectron beams, as well as relative dosemeasurements for photon and electron beams, ispresented. It also updates some of the data andconcepts in TRS-277.
SCIENTIFIC SCOPE
The scientific scope of the Co-ordinated ResearchProject is to investigate the accuracy of the new dataand procedures included in the Code of PracticeIAEA TRS-381. Differences with existingrecommendations, published by nationalorganizations, are to be evaluated to analyze thepossible impact on patient dosimetry. The secondResearch Co-ordination Meeting (RCM) wasorganized to revise the activities in the Co-ordinatedResearch Project (CRP) and the status of the variousprojects .
The status of the on-going work under the frame ofthe CRP was presented by the participants in theRCM during the first two days and eachcontribution discussed in detail. During thefollowing days, plans were made on the work leftfor each participant to complete the project and thefeasibility of preparing a report describing in detailthe work done in the project.
Results of the project are scheduled for presentationin the ESTRO-Physics conference in Göttingen,Germany in 1999.

5
MAIN POINTS DISCUSSED
The main points discussed during the meeting were:
• review of work done since the last RCM inDecember 1996 (Vienna),
• comparisons with dosimetry protocols recentlyissued by different national organizations(AAPM TG-39, USA; IPEMB, UK; DIN,Germany) using different types of plane-parallelionization chambers and phantom materials,
• investigation on the performance of variouscommercial plane-parallel ionization chambersfrom the point of view of saturation, polarityeffect, and effective point of measurement,
• comparison of the three methods recommendedin TRS-381 for the calibration of plane-parallelionization chambers in terms of ND,air usingelectron and Co-60 radiation beams in differentphantom materials,
• investigation of the data for converting electronfluence from plastic to water, compiling datameasured by all participants for PMMA,
• investigation of the accuracy of the data andprocedures included in the Code of Practice,comparing absorbed dose to water determinedunder reference conditions with that obtainedfrom absolute methods (Fricke),
• investigation of the fluence perturbationcorrection factors for cylindrical ionizationchambers in electron beams, as these are used asreference detectors for the calibration of plane-parallel ionization chambers.
RESULTS OF THE PROJECT
As a result of the presentations and subsequentdiscussions, the following points are considered tohave the maximum relevance for the project.
FRICKE DOSIMETRY
The use of Fricke dosimetry had been discussed asthe only possible way to resolve the largediscrepancy between IAEA TRS-381 and AAPMTG-39 when measurements are performed in plastic
phantoms. In water the differences areapproximately within 1%. For PMMA thediscrepancy is worse at an energy of approximately10-12 MeV, and has therefore a possible largeimpact in clinical dosimetry.
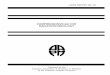
A first set of Fricke data has become available fromone of the participants (AVdP, Belgium), where allmeasurements had been made in plastic, which areshown in figure 1.
It is still necessary:
a) to perform Fricke measurements where thequantity Dw is measured directly in a waterphantom, and
b) to compare it with Dw obtained from ionizationchamber measurements in plastic according toTRS-381 (i.e. with scaling of depths and fluenceconversion).
It is agreed that participants performing Frickedosimetry should use a Co-60 beam as reference forboth Fricke and for a cylindrical ionization chamber,with all measurements performed in water.Measurements with the same Fricke solution shouldthen be compared with a plane-parallel chamber anda cylindrical ion chamber in a high energy electronbeam. Then, measurements at low energy electronscan be performed.
1 2 3 4 5 6 7 8 9 10 11 120,980
0,985
0,990
0,995
1,000
1,005
1,010
1,015
1,020
PTWMarkus
Fig. 1. A comparison of the IAEA TRS-381Code of Practice for plane-parallel ionizationchambers using two different ion chamberswith a dose determination using Frickedosimetry. All measurements made in PMMA

6
SCALING PLASTIC MEASUREMENTS TOWATER
Several participants have measured carefully thefactor hm to convert electron fluence from PMMA towater, as a function of the mean electron energy atdepth. A compilation of the data obtained usingdifferent ionization chambers, mainly of the plane-parallel type, is presented in figures 2 (a-c). It can beobserved that the agreement with the data presentedin TRS-381 Table XVIII, adopted from reference [6]in the Code of Practice, is by no means clear. Thefollowing issues can be raised:
The very large scatter of data at low electronenergies, which has not been shown before inrelated publications, clearly indicates the greatdifficulty to perform this type of measurements in aclinical environment (as in all previous publicationsin the topic).
A dependence on the type of plane-parallelionization chamber used, or even on chamber tochamber variations, seems to be possible although ithas been ignored so far.
The importance of this topic is so large that it is feltit still deserves further investigation. For thispurpose common measurement conditions areagreed: use constant SCD if possible, 15x15 cmfield size, no electron cones, external monitorplaced in the lowest position in the treatment head,avoid use of scaling rules and do measurements atzmax in each medium, perform water/PMMA/wateror PMMA/water/PMMA triple measurements ateach energy during the same session, use fP,T forwater and plastic, perform a minimum of threeindependent measurements for each data point. Allparticipants will perform a new set of measurementsbefore July 1998. The difficulties in performing thistype of measurements is interpreted as ademonstration of how any measurement in plasticwill have an increased uncertainty solely due to thisconversion factor.
0 5 10 15 200,985
0,990
0,995
1,000
1,005
1,010
1,015
1,020
1,025
Roos (BEL) Roos (ARG) Roos (SPA) TRS-381
wat
er /
PM
MA
fluen
ce c
orre
ctio
n fa
ctor
, hm
Mean energy at depth, Ez (MeV)
0 5 10 15 200,985
0,990
0,995
1,000
1,005
1,010
1,015
1,020
1,025
Markus (BEL) Markus (ARG) TRS-381
water
/ PMM
A flue
nce c
orre
ction
facto
r, hm
Mean energy at depth, Ez (MeV)
0 5 10 15 200,985
0,990
0,995
1,000
1,005
1,010
1,015
1,020
1,025
wate
r / P
MMA
fluen
ce co
rrecti
on fa
ctor h
m
cyl. chambers
NACP (SPA) PTW30001 (BEL) NE2571 (BEL) TRS-381
Mean energy at depth, Ez (MeV)
Fig 2 (a-c). A compilation of the data measuredfor the factor hm to convert electron fluence fromPMMA to water, as a function of the meanelectron energy at depth using different ionizationchambers, mainly of the plane-parallel type

7
DETERMINATION OF THE ND,AIR FACTORUSING THE METHODS RECOMMENDED INTRS-381
With regard to the determination of the ND,air factorof plane-parallel ionization chambers, excellentagreement was obtained for all ionization chamberswhen measurements are performed in electron
beams, even of different energies and properties(different clinical accelerators). However, whenmeasurements are made in a Co-60 beam, the ND,air
factor for some of the plane-parallel chambers hasbeen different from that obtained in electron beams.This cannot be excluded in the case of the PTWRoos ionization chamber, see Table I.
Table I. Overall comparison of the ND,air factor of plane-parallel ionization chambers in electron and 60Co beams inwater and PMMA
Ion chamber: NACP PTW-Markus PTW-Roos
BEL(Fricke measurementsconfirm electron results)
all data agree within 0.5% 60Co data in waterdiffer by up to 1.7%
(NCS-protocol used for Dw;requires recalculation)
ARG all data agree within 0.3% 60Co data in waterdiffer by up to 2%(two different cyl refchambers confirm data)
SPA all data agree within 0.1% all data agree within 0.5% 60Co data in PMMAdiffer by up to 2.8%
The discrepancies in ND,air factors were discussed indepth although no clear conclusion could bereached. The need for additional measurements,especially with the PTW-Roos ionization chamber,was emphasized and most participants will increasethe number of data available to allow a morecomprehensive analysis.
EFFECTIVE POINT OF MEASUREMENT
It has been confirmed by measurements performedby two participants that the effective point ofmeasurement of the PTW-Markus plane-parallelionization chamber is not in the front of the aircavity but approximately 0.5 mm below.
FLUENCE PERTURBATION CORRECTIONFACTORS FOR CYLINDRICAL IONCHAMBERS
The correction factors pcav in TRS-277 and TRS-381, which have been taken from Johansson et al(1978), have been confirmed within better than0.5% using the same set of ionization chambers andphantom material (PMMA) as used in the originalwork. A new set of chambers has been built, withgraphite walls instead of PMMA walls with dag (athin lining of graphite and epoxy resin). The air
cavity diameters of the two set of chambers aresimilar (new diameters equal to 2, 4, 7, and 8 mmversus 3, 5, and 7 mm respectively). Measurementshave now been carried out in water. Preliminaryresults show that for a mean energy at depth ofabout 6 MeV and the largest chamber, 7 mmdiameter and therefore similar to a Farmer-type, adifference in pcav close to 1% has been foundbetween the two types of chambers. This points atthe need for further investigations related towall/phantom and other possible interface effects(sleeve, air) of cylindrical ion chambers in electronbeams.
Status reports from the participants are given in thefollowing pages. Extended abstracts of thepresentations are available from the ScientificSecretary.

8
STATUS REPORT FROM ARGENTINA:IMPLEMENTATION OF THE NEW IAEACODE OF PRACTICE FOR DOSEDETERMINATION WITH PLANE-PARALLEL IONIZATION CHAMBERS INTHERAPEUTIC ELECTRON AND PHOTONBEAMS
CALIBRATION OF A PLANE-PARALLELIONIZATION CHAMBER PTW 34001(ROOS) VSA CYLINDRICAL CHAMBER.
Brunetto M.(FaMAF (UNC) - Centro Médico DeanFunes), Germanier A. (CEPROCOR, VélezG.(FaMAF (UNC) - Hospital San Roque).
The ND airpp
, calibration factor for the Roos chamber
was determined following the methodsrecommended by the TRS-381 protocol: 60Co inwater and electron-beam methods.
60Co in water
The ND airpp
, calibration factor was determined in 60Co
beam, using two different cylindrical chambers asreference: NE-2571 and Capintec PR06G.
The effective points of measurement of the(cylindrical) reference chamber and the plane-parallel chamber were placed at the same depth: thispoint is 0.6r in front of the geometrical centre forthe cylindrical chamber and at the center of the frontsurface of the air cavity for the pp-chamber. Theeffect of the PMMA waterproofing sleeve for thepp-chamber was corrected according to the ratio ofthe electron densities between water and PMMA.
The difference between the values of ND airpp
, obtained
was about 0.4% independent of the referencechamber employed.
Electron- beam method
Measurements were performed in a water phantom.Two independent determinations of ND air
pp, factor for
the Roos chamber were done (November,1997 andFebruary, 1998) at the highest electron energy of thelinear accelerator (Varian Clinac 18). In both casesthe reference conditions were the same, and they areshown in the next Table.
Electron Beam
Nominal Energy (MeV) 18
Eo (MeV) 17.5
SSD(cm) 100
Field Size (cmxcm) 15x15
Depth (cm) 2.5
A Farmer-type ionisation chamber NE-2571 wasused as an external reference monitor detector andwas positioned within the phantom close to thechambers.
The difference between the values of ND airpp
, obtained
was 1%.
The difference between the ND airpp
, values obtained
using the Co-60 and the electron beam methods was2%, indicating the need for more measurements andinvestigations for the Roos chamber.
COMPARISON OF ABSORBED DOSE VALUESOBTAINED WITH DIFFERENT IONIZATIONCHAMBERS: PTW 34001(ROOS), PTW 23343(MARKUS) AND NE 2571.
Determinations of the absorbed dose to water inelectron beams were performed using threeionization chambers: a cylindrical NE-2571, with acalibration factor NK given by a SSDL, and twoplane-parallel chambers PTW 34001 (Roos) andPTW 23343 (Markus). Both pp-chambers werecalibrated against the cylindrical chamber followingthe procedures and correction factors of the TRS-381 Code of Practice.
The absorbed dose values were determined in theelectron beam of a Varian Clinac 18 accelerator, atSSD=100cm, and field size =15cmx15cm. Themeasurements were performed in water, atz=12.5 mm for the 6 MeV (nominal energy) electronbeam, and z=24.5 mm for the 9, 12, 15 and 18 MeV(nominal energies) electron beams. These depthscorrespond to the position of maximum dose.
The results showed good agreement (within 1%) inthe values of the absorbed dose obtained using thedifferent chambers at high energies. The biggestdifferences were found at low energies (for

9
example, 2.8% between Markus chamber and Rooschamber at 9MeV). The values obtained using theNE-2571 ionization chamber at low energies wereincluded only as a comparison, since its use is notrecommended at low energies.
EXPERIMENTAL DETERMINATION OF HM INPMMA
The values of hm were obtained as the ratio of theaverage readings at the reference depth in a waterphantom ( zref,w ) to the average readings at theequivalent reference depth in a PMMA phantom(zref,PMMA ), using two pp-chambers PTW 34001-Roosand PTW 23343-Markus. An external monitordetector was positioned in air to normalize thereadings both in water and PMMA.
The results are presented in the table below. Themeasured values of hm are in good agreement with
the values given in TRS-381(better than 0.6%,which is within the experimental uncertainty),except one value for the Markus chamber at 4.6MeV, probably due to an error in the experimentalset-up.
Experimental determination of hm
0.995
1
1.005
1.01
1.015
1.02
1.025
0 2 4 6 8 10 12
Ez (M eV)
hm
hm(Roos)
hm(Markus)
hm(TRS-381)
Enom Ez hm
TRS-381hm
PTW-Markus%dif hm
PTW-Roos% dif
6 2.81 1.008 1.010 0.2 1.014 0.6
6 3.07 1.008 1.003 -0.5 1.011 0.3
9 3.09 1.008 1.014 0.6 1.012 0.4
12 4.60 1.008 1.020 1.2 1.014 0.6
12 5.39 1.007 1.009 0.2 1.011 0.4
15 7.00 1.006 1.012 0.4 1.010 0.4
15 7.79 1.005 1.006 0.1 1.008 0.3
18 11.62 1.003 0.998 -0.5 1.004 0.1
STATUS REPORT FROM BELGIUM:ANALYSIS OF THE TRS-381 CODE OFPRACTICE - VERIFICATION OF THEABSORBED DOSE VALUES DETERMINEDWITH PLANE-PARALLEL IONISATIONCHAMBERS IN THERAPEUTICELECTRON BEAMS USING FERROUSSULPHATE DOSIMETRY
Ann Van der Plaetsen, A.Z Sint Lucas Hospital,Ghent; H. Palmans, H, Thierens, StandardDosimetry Laboratory, University Ghent
RELATIVE DOSE MEASUREMENTS
Relative dose parameters were determined in awater phantom using a PTW/Roos plane-parallel
ionisation chamber. Values obtained for R100, R50
and Rp are in agreement within the statisticaluncertainty with the results obtained previouslywith a PTW/Markus chamber or with diodes or adiamond detector.
Comparison of the values for R100 and R50
determined with the Markus chamber with thosedetermined with the Roos chamber revealed a shiftof the effective point of measurement for theMarkus chamber of 0.5 mm from the front of thechamber towards its centre.
EXPERIMENTAL DETERMINATION OF THEFLUENCE CORRECTION FACTOR HM
When the absorbed dose is determined in aPMMA phantom instead of a water phantom, the

10
hm factor corrects for the difference in the fluence.The first set of measurements resulted in valuesdifferent from those proposed in the TRS-381protocol. We continued this study for a PMMAphantom using the PTW/Markus and thePTW/Roos chambers.
The hm factors obtained with the Roos chamber arein agreement with those from the TRS-381protocol except at low energies. All hm correctionfactors obtained with the Markus chamber are
lower than those proposed by the protocol, up to1.8% for the lowest energy. The results arepresented in the next table. The uncertainties onthe different measurements are given at the levelof 1 SD (i.e., k=1). More measurements need to beperformed, especially with another Markuschamber to see if the hm factor is chamberdependent.
Enom Ezhm
TRS-381hm
PTW-MarkusSD %dif
hm
PTW-RoosSD %dif
4 2.01 1.009 0.991 0.003 1.8 0.995 0.003 -1.4
6 2.73 1.008 0.993 0.0003 1.5 1.002 0.002 -0.7
8 3.45 1.008 0.993 0.001 1.5 1.006 0.002 -0.2
10 4.12 1.008 0.993 0.001 1.5 1.006 0.002 -0.2
12 5.76 1.007 0.996 0.0003 1.2 1.007 0.001 0
15 7.34 1.006 0.995 0.0004 1.1 1.007 0.002 0.09
18 8.8 1.004 0.996 0.0004 0.8 1.005 0.003 0.08
DETERMINATION OF THE ND,AIR
CALIBRATION FACTORS FOR THEPTW/ROOS AND THE PTW/MARKUS PLANEPARALLEL CHAMBERS.
We compared the ND,air calibration factors obtainedfollowing the different methods described in theTRS-381 protocol. The results are summarised inthe next table. The stated uncertainties are for k=1,representing the statistical uncertainties fordifferent measurements.
The measurement conditions for ND,air determinedin a water phantom for 60Co (Standard DosimetryLaboratory) were as follows:
• reference depth: centre of the cylindricalreference chamber at 5 cm, centre of the frontof the plane-parallel chamber at 5 cm,
• SSD = 70cm,
• determination relative to absorbed dose towater secondary standard
The measurement conditions for ND,air determinedin an electron beam against a cylindrical chamberwere as follows:
• reference depth : depth of maximum dose (3cm),
• SSD = 100 cm
• cylindrical chambers: PTW 30001, NE-2571
measurements performed in water and in PMMA.
Markus Roos
ND,air derived fom NK 0.480 (0.002) 0.071 (0.003)
ND,air determined in an electron beam against a cylindrical chamber 0.476 (0.003) 0.0707 (0.003)
ND,air determined in a water phantom in 60Co 0.478 (0.003) 0.0719 (0.0002)
ND,air derived from the Fricke measurement in the 18 MeV electron beam 0.471 (0.003) 0.0705 (0.0003)

11
The ND,air derived fom NK compared to thecalibration factor determined in the electron beam isin agreement within 1%.
The deviation between the ND,air determined in theelectron beam and the ND,air determined in a waterphantom in a Co-60 beam points that the value forpwall of the plane-parallel chamber needs to bereconsidered.
COMPARISON OF THE IONOMETRICALLYDETERMINED ABSORBED DOSE FOLLOWINGTHE TRS-381PROTOCOL WITH THE DOSEVALUES OBTAINED WITH THE FRICKEDOSIMETER
These measurements were performed in a PMMAphantom. The field size and the SSD were10cmx10cm and 100 cm, respectively.
Following the TRS-381 protocol rigorously, weobtained an agreement within 1 % between theFricke dose value and those determined with thePTW/Roos and the PTW/Markus chambers. Usingthe experimentally determined value of the hm
correction factor for PMMA introduced a deviationof more than 2 %. We can therefore conclude thatthese measurements should be performed in water toexclude the effect of PMMA.
STATUS REPORT FROM GERMANY:INVESTIGATION OF THE ACCURACY OFPROCEDURES AND DATA IN IAEA TRS-381
Dr. Martin Roos (PTB)
The accuracy which is achievable with the newprocedures and data of TRS-381 depends stronglyon the performance characteristics of the plane-parallel ionization chambers available. The presentinvestigations include the dependence of theresponse on the polarity (polarity effect) and on theabsolute value of the polarizing voltage (correlatedwith the saturation correction) of commercial plane-parallel chambers.
The polarity effect of various chambers has beenchecked, including its dependence on the depth andthe field size. It has been shown that, in general, it isnot sufficient to relate the polarity effect exclusivelyto the mean energy at the depth of measurement. Ifthe polarity effect is not negligible, it must bedetermined for all sets of irradiation parameters. Inthis case it is particularly important that the
stabilization times after reversing the polarityare short. It has been shown that these timesextend from a few minutes up to about half anhour for dose rates of a few Gy/min, which areusual for clinical accelerators.
Due to the long stabilization times for most ofthe plane-parallel chambers after a change inthe absolute value of the polarizing voltage, theexperimental procedures for the determinationof the saturation correction are also very timeconsuming. It has been demonstrated that,depending on the stabilization time and on theinherent drifts of the accelerator/monitor/dosimeter under test system, the uncertainty ofthe correction may be comparable with itsmagnitude. In this case the analyticalexpression by Boag for conventional beams(ICRU Report 34 (1982)), included in TRS-381, allows a convenient evaluation of thesaturation correction factor. This expression,which so far had been the only one available,takes only volume recombination into account,which is the main source of recombination.
The saturation behaviour of plane-parallelchambers has now been investigated in detailand a formula based on the experimental datahas been deduced which takes account of theinitial recombination and the diffusion loss.The correction factor can be determined fromthe electrode spacing d, the polarizing voltageU, and the dose per pulse Di , for chambers
with an electrode spacing of about 2mm(applicable to most of the commerciallyavailable chambers) according to:
k 1 (0.12 0.46 d D ) / Us2
i= + + ⋅ ⋅
Figure below shows experimental results of thecharge deficit as a function of the pulse chargedensity for an electrode spacing of 2mm and apolarizing voltage of 100V. The solid line andthe dotted line represent the new formula andthe Boag expression, respectively. Thedifference between the Boag expression and thenew formula is mainly caused by the initialrecombination and by the more accurateestimation of the free electron component in thenew expression. Since, in practice, thesaturation correction for conventional beams isusually below 1%, the deviations of the Boag

12
formula, which are of the order of 0.1%, are not tooimportant for practical dosimetry.
It has to be emphasized that both formulas apply toplane-parallel chambers exclusively, i.e. forchambers with a plane-parallel arrangement of theelectrodes. In the case of the PTW-Markus chamber,however, most of the high-voltage electrode isperpendicular to the collecting electrode, increasingthe recombination in comparison with a plane-parallel arrangement of the electrodes. This has beendemonstrated by calculations using the finiteelements method.
Furthermore, the position of the effective point ofmeasurement of the PTW-Markus chamber has beeninvestigated in detail. Measurements at the PTBlinac show that the peculiar cavity properties and thenegligible guard-ring width (both deviating from thedesirable properties given in TRS-381) result in ashift of the effective point of measurement by about0.5-0.6mm (depending on the energy and on thedepth) from the front surface of the air volumetowards the chamber centre in the descending partof the depth-dose distributions. Even in the vicinityof R85, neglecting this effect may cause dosedeviations of various percent at low energies.
The dependence of the chamber response on thepolarity and on the absolute value of the polarizingvoltage for commercial chambers has been studiedin detail. It has been shown that almost all chambersshow a strong curvature of the 1/M over 1/Vrelation, particularly at high voltages. In addition, ithas been shown that the polarity effect shows astrong dependence on the absolute value of thepolarizing voltage for most chambers. Examples ofsevere chamber-to-chamber variations of all theseproperties have been given.
The selection of the stopping power ratios based onthe half-value depth and the depth of measurement,as described in TRS-277 and TRS-381, and theselection according to the new DIN standard 6800-2,which also considers the practical range, have beencompared with the Monte-Carlo results by Ding et
al. (Med. Phys. 22, 1995) for various clinicalaccelerators. According to them, the DINmethod results in a slight improvement in theselection of the stopping power ratios. In beamscontaining a large component of contaminatingphotons, the results may be further improved ifthis is properly taken into account.
In addition, the stopping power ratios accordingto TRS-381 have been compared with thoseaccording to DIN 6800-2 for the beams of thePTB linac. Apart from the selection procedures,additional slight deviations are caused bydifferent fit polynomials to the energy-rangerelationship tables of TRS-277. The maximumdeviation between the two values of thestopping power ratios according to the twoprocedures is, however, not larger than 0.6%.
In order to draw definite conclusions,experimental results (e.g. using Frickedosimeters) from different clinical acceleratorswould be extremely valuable. The mostcomprehensive set of data is still constituted bythe investigations of the energy-dependence ofthe response of the plane-parallel chambers atdifferent types of clinical accelerators byJohansson and Svensson in 1981 (Johansson,Thesis, Univ. of Gothenburg, 1982). Since thattime, however, various new accelerator typeshave entered the market.
STATUS REPORT FROM SPAIN:ELECTRON BEAM DOSIMETRY,CALIBRATION AND USE OF PLANE-PARALLEL IONIZATION CHAMBERSFOLLOWING THE IAEA TRS-381RECOMMENDATIONS AND OTHERPROTOCOLS
Lizuain M.C., Linero D., Picón C., Sánchez P.Institut Català d’Oncologia, Barcelona
INTRODUCTION
The goal of the project is to study the differentfactors related to the determination of absorbeddose to water using the plane-parallel chamberRoos (PTW) in comparison to NACP 02. Thisproject is continuation of the work presented inthe First Research Coordinated Meeting (RCM)for the Co-ordinated Research Project(CRP) onDose determination with plane-parallelionization chambers in therapeutic electronand photon beams.
0.0 0.5 1.0 1.50.0
0.5
1.0
1.5
d = 2 m mU = 100 V
Volum e recom binationICR U REPOR T 34 (1982)
10-5 C /m3
%
charge deficit
pulse charge density

13
Previously we had investigated the differencebetween the absorbed dose determined with Markusand NACP pp-chambers in water and PMMAphantoms, following the formalism of TRS-381,TRS-277 and TG-39 protocols. A significantdifference (up to 3%) was found between TG-39and TRS-381 when measurements were made inPMMA phantoms.
All the measurements were performed at two linearaccelerators: VARIAN Clinac 18 and Clinac 2100C. A Theratron 780 Cobalt unit was also used. Themeasurement conditions are given in the followingtable.
Nominal energy En (MeV) 4 - 18
Mean energy at surface
Eo
MeV( )
3.5 - 17
Reference depth (zeff) Depth of maximum absorbed
dose
Mean energy at depth zeff
E MeVz ( )
1.9 - 12.5
SSD (cm) 100
Reference chamber NE-2571 (cylindrical chamber)
Phantom material Water and PMMA
Monitor chamber NE-2571 (cylindrical chamber)
Dose / pulse (mGy/p) 0.45 - 0.97
DETERMINATION OF ND air
pp
, FOR A ROOS
PLANE-PARALLEL IONIZATION CHAMBER
The determination of this factor has been made inelectron beams, using water and PMMA phantoms,following the method recommended in TRS-381.The measurements were performed at two linearaccelerators, using the highest energy available ateach , with four determinations at each energy. Nosignificant difference was found between theN
D air
pp
,
values obtained for the two electron beams and forthe different phantom materials (0.3%, k= 1).
Three more determinations were made in a Co-60beam with PMMA phantom at 5 cm depth. For thiscase, the N
D air
pp
, factor was 2.8% higher than the value
determined in electron beams. One of the reasonsfor this discrepancy could be the effect of theperturbation factor pwall
pp for the Roos chamber in
PMMA phantoms for the cobalt beam, which wasassumed equal to 1 for the present measurements.
DETERMINATION OF RECOMBINATIONAND POLARITY CORRECTION FACTORSFOR ROOS AND NACP PLANE-PARALLELCHAMBERS
The determination of the recombinationcorrection factor ps for the pp-chambers hasbeen made using the “two voltage” method andthe polynomial fit given in TRS-277.Measurements have been performed in electronbeams under the conditions given in the tableabove. In all cases, one external monitorchamber (NE-2571) was used. The polarisingvoltages used were -300, +300 and -100 V.
The values presented are the average valuesobtained from the measurements in water andPMMA phantoms, using dose/pulse between0.45 and 0.97 mGy.The polarity effect of the Roos chamber isnegligible (ppol =1.0001 ± 0.02% ) and thecalculated saturation (99.2 % -99.7%) agreeswell with the value given by the manufacturer:99.5% for pulsed radiation with dose/pulse upto 0.15 mGy. The influence of the two effects isslightly more important in the case of a NACPchamber.
ELECTRON BEAM QUALITYSPECIFICATION WITH ROOS AND NACPCHAMBERS
The energy parameters that specify the qualityof an electron beam have been determined fromthe depth ionization curve measured in waterphantom with Roos and NACP chambers underthe conditions given in the table above and witha radiation field of 25x25 cm2. No correctionfor polarity and saturation effects was applied.The effective point of measurement was takeninto account. 0E and 0,pE were calculated
from the ranges RJ50 and Rp using the empirical
relationships recommended in TRS-381 andTRS-277. The determined values of the rangesRD
100 , RJ50 and Rp , and the energy parameters
0E ,0,pE from the measurements made with the
two pp-chambers are presented. The shiftbetween the two depth ionisation curves was0.4 - 1.1 mm depending on the beam energy.
ABSORBED DOSE TO WATER
Absorbed dose to water, under the referenceconditions given in the table above, has beendetermined using the four combinations of

14
NACP and Roos chambers in PMMA and waterphantoms in electron beams of mean energy E0
from 3.5 to 17 MeV. This was done according toTRS-381 recommendations. The dispersion (1 SD)in relation to the mean value of the 4 set ofdeterminations varied between 0.5 and 1.0%.
EVALUATION OF THE FLUENCECORRECTION FACTOR: HM
The measurements have been performed with twoplane-parallel ionization chambers, NACP and Ross,under the conditions given in the table above. Thediscrepancy between hm in TRS-381 and the ratioDwater/DPMMA was about 1% for the two chambers.Due to the difficulty of reproducing themeasurement conditions for water phantom andPMMA phantom, this difference is consistent withthe experimental uncertainty obtainable underclinical conditions.A second group of determinations of hm factor wasperformed in May 1998, just after the RCM. Themeasurement conditions were those agreed upon:SCD 100 cm, 15x15 cm2 field, no electron conesand external monitor chamber placed close to thephoton jaws. The results obtained are presented inFigure 8.1 The measured values of hm are alwayslower than the hm in TRS-381 with an averagedifference of about 0.5 %; however, the discrepancyincreases with the energy.
0 2 4 6 8 10 12 140.975
0.980
0.985
0.990
0.995
1.000
1.005
1.010
1.015
1.020
1.025
HM0598.ORG
Fluence correction factor hm vs. Ez
Roos NACPTRS.381
h m
Ez (MeV)
Fig. 8.1. – Factor hm to convert fluence from PMMA towater, as a function of mean energy at depth, estimatedfor the NACP and Roos plane-parallel chambers
COMPARISON BETWEEN TRS-381 AND TG-39CODES OF PRACTICE
The ratio of absorbed dose to water in electronbeams determined according to the TRS-381 and
TG-39 protocols from the measurements inwater and PMMA phantoms using a Rooschamber was calculated for various meanenergies. Results of this determination aregiven in Figures 8.2 and 8.3, together with thevalues obtained in the previous part of thiswork for the NACP, Markus and NE-2571chambers.
0 2 4 6 8 10 12 140,96
0,97
0,98
0,99
1,00
1,01
1,02
1,03
TG-39 / TRS-381 in water vs. Ez
Roos NACP NE.2571
Abs
orbe
d D
ose
Rat
io
Mean Energy Ez (MeV)
Fig. 8.2.- Ratio of absorbed dose to waterdetermined according to TG-39 and TRS-381CoP as a function of mean energy at depthMeasurements performed in a water phantom
0 2 4 6 8 10 12 140,96
0,97
0,98
0,99
1,00
1,01
1,02
1,03
TG-39 / TRS-381 in PMMA vs. Ez
Roos Markus NACP NE.2571
Abso
rbed
Dos
e R
atio
Mean Energy Ez (MeV)
Fig.8.3.- Ratio of absorbed dose to waterdetermined according to TG-39 and the TRS-381 CoP as a function of mean energy atdepth. Measurements performed in a PMMAphantom

15
STATUS REPORT FROM SWEDEN-1:PLANE-PARALLEL IONISATION CHAMBERDOSIMETRY IN CLINICAL ELECTRONBEAMS OF ENERGIES 4-50 MEV
H Svensson, A Björeland (Umeå)
The work by the Umeå group was carried out by MrHåkan Nyström till the end of 1997. As he thenmoved to another department, there has been sometransfer problems. An investigation to determineextreme differences between the different protocols,later to be verified by measurements, wasundertaken in the beginning of 1998. A PhD student,Anders Björeland, was involved in this activityunder the supervision of the head of the RadiationPhysics department, Mr Hans Svensson, who is theofficial participant from Umeå.
It is possible to compare theoretically thedifferences in dosimetry that would be derived usingthe AAPM protocol TG-39 and the IAEA TRS-381,as the same set of measurements is required. Thenumerical values of the interaction coefficients andthe correction factors differ which results indeviations. A complete data set for different types ofchambers is presented. For the so called "electronbeam method", deviations up to 2.5 % were shown.In the "Co-60 in phantom method" deviations up to3.0 % were derived, and for the "Co-60 in air" thelargest deviation was 1.7 %. In all these methodsusing different combinations of plane-parallel andcylindrical chambers, a somewhat higher dosewould generally be determined using the IAEAprotocol.
The methods in IAEA TRS-381 could not becompared directly with the IPEMB 1996 (i.e. UKreport) and NCS report 5 1998 (i.e. the Dutch code)as the procedures to carry out measurements differ.However, some values of the interaction coefficientsused in these protocols could be compared. Thereare some minor deviations (< 0.5 %) for chamberfactors. Further, the stopping power data used forthe electron beam measurements differ by about 0.5% for depths usually relevant for reference dosedetermination. Measurements are needed todetermine the difference in the end results .
It can be concluded that the dose deviations of 1.5 –2.5 % can be attributed to the choice of thedosimetry protocol. In modern radiotherapy, it isoften recommended that the dose to the patientshould be within 3.5 – 5 % (see ESTRO 1997). It istherefore very important to reduce the uncertainty atevery step. Deviations, just due to different values
of the interaction coefficients, of up to 2.5 %seem to be too large and further work isneeded.The Umeå group will therefore continue toimprove and verify the data using the ferroussulphate dosimetry method. A special care mustbe taken to set up the experiment, however, toinvestigate the deviations in the order of 1 – 2%. It should, however, be possible to verify theinconsistencies at least in the energydependence as we intend to carry out plane-parallel and cylindrical chamber measurements,and also ferrous sulphate dosimetermeasurements in both high-energy photon andelectron beams of different energies.
STATUS REPORT FROM SWEDEN-2:PCAV FACTORS FOR CYLINDRICALIONIZATION CHAMBERS INELECTRON BEAMS
Å. Palm and O. Mattsson, SahlgrenskaUniversity Hospital, SE-413 45 Göteborg
The electron beam method for calibratingplane-parallel ionization chambers involvescavity correction factors for cylindricalchambers. The cavity correction factors inTRS-381 are based on the experimental resultsby Johansson et al (1978). In the present worktheir method was used to determine cavitycorrection factors for a new set of cylindricalgraphite chambers in water. The cavity radiiwere 1, 2, 3.5 and 4 mm. Measurements weredone at the recommended reference depth(TRS-381), in photon and electron beams usinga Varian Clinac 2300CD. The procedure wasthen repeated for the depth used by Johanssonet al, i.e. placing the centre of the chamber atthe peak of the depth ionization curve. Furtherstudies involved the same chambers andPMMA phantom previously used by Johanssonet al. The only difference between the two setsof measurements was the accelerator beams. Inaddition, a plane-parallel chamber was used inall measurements.
To obtain the cavity correction factors, themeasured charge was normalised to thesmallest chamber. A plot of the inverse of pcav
as a function of cavity radius was made forvarious electron beam energies. According toJohansson et al this yields a straight line. Thisfunction was renormalised such that pcav isunity for cavity radius of zero.

16
In the first study, with Peff placed at zref, a linearrelation was found for the higher energies only. Thismight be caused by the fall-off in the dose in theregion close to the chamber for the largest chamberin the low energy electron beams, in combinationwith the problems related to the use of the effectivepoint of measurement for the small chambers.However, straight lines were obtained when themeasurements were done, in both water and PMMAphantoms, with the centre of the chamber placed atthe peak of the depth ionization curve.The cavity correction factor can also be determinedusing a plane-parallel chamber as a reference. Aspwall for these chambers is considered to be uncertaina plot for each energy was drawn, yielding thevolume ratio of the plane-parallel chamber to thesmallest cylindrical chamber. The mean value of thesix volume determinations was used to derive pcav.
1,00
1,01
1,02
1,03
1,04
1,05
1,06
0 5 10 15 20 25
Mean energy at depth, E z (MeV)
1/p
cav
TRS 3.5 mm3.5 mm, in PMMA3.5 mm, in waterTRS 2 mm (extrapol)2 mm, in water
Fig. 10.1. 1/pcav determined at the depth of Dmax
using graphite chambers in water and Johanssonet al’s chambers in PMMA, compared with datafrom TRS-381 for cavity radius 2 and 3.5 mm
In figure 10.1, the inverse of pcav as a function of themean energy at the depth of the chamber fordifferent cavity radii is shown. Data for the graphitechambers in water with the centre of the chamber atthe peak of the depth ionization curve are shown.The results are compared with the data from TRS-381. For comparison, the results derived using thesame equipment as Johansson et al are included.These results were obtained using a plane-parallelchamber as a reference. For the watermeasurements, a Roos chamber was used, while forthe PMMA measurements an NACP02 was used. Itcan be concluded that the measurements in PMMAare in good agreement with the original data fromJohansson et al. Compared to TRS-381, a smallercorrection was found (??) for the cavity perturbationfor the graphite chambers used in water. For thehighest energies, that are recommended for thecalibration of the plane-parallel chambers, thedifference is small.
REFERENCES
[1] IAEA International Atomic EnergyAgency, "The use of plane-parallel ionizationchambers in high-energy electron and photonbeams. An International Code of Practice forDosimetry", Technical Report Series no. 381,IAEA, Vienna (1997).
[2] AAPM American Association ofPhysicists in Medicine, Task Group 39: Thecalibration and use of plane-parallel ionizationchambers for dosimetry of electron beams: Anextension of the 1983 protocol, Med. Phys. 21(1994) 1251-1260.
[3] Johansson, K.A., Mattsson, L.O.,Lindborg, L., Svensson, H., "Absorbed-dosedetermination with ionization chambers inelectron and photon beams having energiesbetween 1 and 50 MeV (IAEA-SM-222/35)",National and International Standardization ofRadiation Dosimetry (Proc Symp. Atlanta,1977), Vol. 2, IAEA, Vienna (1978) 243-270.

17
REPORT OF THE EIGHTHMEETING OF THE SCIENTIFICCOMMITTEE OF THE IAEA/WHONETWORK OF SSDLs
IAEA, VIENNA, 5-9 OCTOBER 1998
Scientific Secretary: P. AndreoDosimetry and Medical Radiation Physics Section,
NAHU
FOREWORD
The report of the seventh meeting (held in Sept/Oct., 1996) of the Scientific Committee (SSC) of theIAEA/WHO Network of Secondary StandardDosimetry Laboratories (SSDL) was published inthe SSDL Newsletter No. 36, January 1997.
The eighth meeting was held in Vienna at theAgency headquarters from 5 October to 9 October1998. Opening remarks were made by Professor S.Groth, Director, Division of Human Health(NAHU), Dr. H. Østensen , Co-Secretary of theIAEA/WHO SSDL Network, Dr. P. De Regge,Head, PCI Lab, (NAAL), and Professor P. Andreo,Head, Section of Dosimetry and Medical RadiationPhysics (DMRP). Professor Groth spoke of the role,mission, and functions of the Agency and theDivision, including the particular interest of theDivision in nuclear medicine and diagnosticradiology, and their interest in electronic transfer ofinformation. Dr. De Regge spoke of the importanceof the Dosimetry Laboratory activities withinNAAL. Dr. Østensen stated that he had recentlyjoined WHO and was interested in significantlyimproving the WHO participation in theIAEA/WHO joint programme. He also emphasizedthe importance of quality assurance in diagnosticradiology, which leads to a reduction of the dose tothe patient and physician, without degrading thequality of the image. Professor Andreo introducedthe Agency staff members who presented reports ontheir various activities for the first two days of themeeting and part of the third. The SSC then met inclosed session with Professor Andreo until Fridaynoon, deliberating the accomplishments anddirection of the Agency’s programmes, anddeveloping specific recommendations. The list ofparticipants in the meeting and the meeting agendaare enclosed as Appendices I and II, respectively.
Conforming to its Terms of Reference, the SSCevaluated the activities of the DMRP reported for1997-1998 and discussed the proposed programmefor the Section for 1999-2000. Long range plans for
seminars and teaching courses (until 2002)were also discussed, as well as a strategic planfor the Section. The scope of the evaluationaddressed the questions of:
• the objective of the programme areas,
• the impact (benefit to the Member States),and
• the continuing relevance of Agencyactivities.
Specific recommendations from the SSC areunderlined throughout the text, but also arereiterated at the end of the report.
The committee wishes to commend the DMRPstaff for presenting the various programmes ina clear and concise manner, and for theirstraightforward responses to questions from theSSC. The SSC particularly wishes to thank theDMRP Section Head for providing acomprehensive overview of the activities of theSection for 1997-98 together with a projectionfor 1999-2000. This report gave the SSC a clearoverall picture prior to the meeting and servedas a written reference for discussions during themeeting.

18
INTRODUCTION
The DMRP report and the presentations from thestaff clearly showed the SSC that the DMRP hadresponded to all recommendations of the previousSSC report (Oct 1996) and that significant effortshad been made to establish formal and informallinks with other divisions within the Agency. Ingeneral, the activities of the DMRP support the aimsof the Agency’s Dosimetry Programme.
The DMRP Section’s activities are performed underfour identifiable projects:
• PROJECT E.3.01: Secondary StandardsDosimetry Laboratory (SSDL) Network.
• PROJECT E.3.02: Dose Intercomparison andAssurance
• PROJECT E.3.03: Transfer of DosimetryTechniques
• PROJECT E.3.04: Technical Co-operationActivities
This report begins with a general discussion ofadministrative items and collaborative efforts withinthe Agency. Each project is then discussed in turn.The report summarizes only those activities of theSection for which the SSC has comments orrecommendations. Exclusion of specific activitiesshould be interpreted positively, as concurrence bythe SSC with the activity as reported.
REPORT
GENERAL ORGANIZATIONAL ITEMS
Within the past year the Section of Dosimetry hasbeen renamed the Section of Dosimetry and MedicalRadiation Physics (DMRP), to emphasize the areasof primary expertise and involvement.
The Agency’s Dosimetry LaboratoryThe multiple activities undertaken at the Agency’sDosimetry Laboratory require measurements of highaccuracy. In addition, these programmes have asignificant influence on radiation metrologyworldwide and consequently on doses received byindividual patients or irradiated products.
The Dosimetry Laboratory is integrated into theIAEA’s Siebersdorf Laboratories. The range ofservices provided to the SSDL networkincludes:
• calibration of ionization chambers forradiotherapy, diagnostic x rays includingmammography* and radiation protection,
• calibration of re-entrant ionizationchambers for low dose rate brachytherapysources (137Cs)*,
• TLD dose quality audits for externalradiotherapy beams (for SSDLs and forhospitals),
• ESR-alanine dose quality audits forradiation processing (for SSDLs and forfacilities), and
• TLD dose quality audits for SSDLsproviding dosimetry for personnelmonitoring∗.
Following the recommendations of the last SSCreport, individual professional staff have beenidentified as having responsibilities for thevarious services.
It is the policy of the DMRP Section to operateat the highest possible quality standards. Toachieve this, the DMRP has recently completeda quality assurance (QA) manual documentingthe Dosimetry Laboratory procedures. Thismanual sets out, in compliance with ISO 9000guidelines, the general requirements for theoperation of the laboratory as well as anextensive documentation of its procedures inaccordance with ISO Guide 25 for calibrationlaboratories. The SSC hopes that SSDLs willfind portions of this manual useful as modelsfor their quality manuals.
The Section Head of DMRP has developed aneffective working relationship with the Directorof the Agency Laboratories (NAAL). The SSCcommends the development of this workingarrangement between the two divisions (NAHUand NAAL) with regard to implementation ofthe Agency’s Dosimetry programme. However,the SSC notes that the development of a quality
* Indicates services developed or introduced in thepast two years.

19
system for the metrological activities of the DMRPrequires that the responsibilities and duties of thestaff at NAHU and NAAL be clearly defined. Thisis especially relevant to its laboratory activities.Consequently the SSC recommends that theresponsibilities and duties of the staff at NAHU andNAAL be clearly defined and documented.
The High-Dose Dosimetry ProgrammeThe Agency’s laboratory provides dosimetry qualityassurance services for high-dose irradiation facilitiesin support of programmes sponsored by otherDivisions in the Agency (specifically the Division ofPhysics and Chemistry (NAPC) and the Division forFood and Agriculture (NAFA)). The SSCrecommends that a more formal relationship bedeveloped between NAHU and the other divisionsinterested in high-dose irradiations (NAPC, NAFA)for future collaborative development of the high-dose dosimetry programme.
Radiation Therapy IssuesThe SSC is pleased that, based on the InterofficeMemorandum "Assurance of Quality and Safety inthe implementation of Radiotherapy Projects" dated7 August 1996, Dosimetry and Medical RadiationPhysics (DMRP-NAHU), Applied RadiationBiology and Radiotherapy (ARBR-NAHU), andRadiation Safety (RS-NSRW) are sharinginformation and responsibility for projects inRadiation Therapy that may have some overlap.
Collaboration with the World HealthOrganization (WHO)
Dr. ∅stensen attended his first meeting of the SSCas the representative from WHO. Since joiningWHO, he has demonstrated a commitment and hasdedicated resources to improving turn around timeand participation in the IAEA/WHO postal TLDprogramme. The SSC is pleased to note that theimproved collaboration with WHO has alreadyresulted in an increased involvement of the hospitalsin the programme and hopes that this improvementwill continue. The SSC welcomes the proposal for aWHO seminar for regional officers and recommendsthat this seminar promotes the hospital auditprogramme in radiotherapy dosimetry, andreinforces the importance of the SSDL network.
Collaboration with ESTRO and OtherOrganizationsThe SSC welcomes the IAEA collaboration withESTRO on a number of mutual programmes,
particularly in regard to the Memorandum ofUnderstanding between the IAEA and ESTROon their mutual cooperation in radiotherapydosimetry quality audit programmes, andrecommends that, where possible, similararrangements be made with other externalorganizations, noting that such collaborationsoptimize the use of resources.
PROJECT E.3.01 SECONDARY STANDARDDOSIMETRY LABORATORY (SSDL)NETWORK
The IAEA/WHO SSDL Network presentlyconsists of 69 laboratory members and 6Primary Standard Dosimetry Laboratories(PSDLs) in 58 member states. The SSCwelcomes the new members in Madagascar,Peru and Tunisia. It was noted that five of thelaboratory members are considered asprovisional members, Libya, Nigeria, Sudanand the two SSDLs in Iraq (see Section 3.2.1below). The University of Singapore hasresigned from the Network due to a change inthe direction of its activities.
The active SSDLs provide traceable instrumentcalibrations for radiation therapy anddiagnostic radiology, provide quality audits ofradiotherapy dosimeters by postal TLD andoccasionally on-site measurements, and someperform measurements at radiation processinglevels, and evaluate personnel dosimeters. Theimplementation of such a programme requiresthat the traceability of the SSDLs to a PSDL orto the Agency be verified periodically throughquality audits and intercomparisons organisedby the DMRP.
Within the past several years the DMRP hasfocused efforts on follow up of the results of allof the audit programmes where an SSDL (orhospital) fails the audit with a disagreementwith the Agency exceeding appropriate actionlevels. The SSC recommends that the SSDLNetwork Secretariat establishes Action Levelsfor all audit programmes, and notifies theparticipants of these action levels.
SSDL CharterFollowing a recommendation of the 7th SSC, anSSDL Charter was prepared outlining thebenefits as well as the duties andresponsibilities of an SSDL Network Member.The Charter also establishes a category of'provisional' member for SSDLs who do not

20
fulfil the obligations of full membership. Thiscategory is considered to be temporary while effortsare made by the provisional member to comply withthe Charter.
• The SSC is pleased to see that the SSDL Charterhas been completed and that the IAEA willpublish the Charter jointly with the WHO. TheSSC recommends that the Agency and WHOcollaborate to ensure that all those involved inthe SSDL Network receive a copy of the charter.
• The SSC notes that some SSDLs have notparticipated in any IAEA organized audit forover 2 years. The SSC recommends that theperiodic measurement assurance tests required inthe SSDL Charter be made at a minimum of 2year intervals, and that the Network Secretariatnotifies all members of the network of thisrequirement.
• The SSC has noted that a number of SSDLs havenot resolved dosimetry discrepancies outside theAgency action levels, as required by the Charter.The SSC recommends that SSDLs who do notcomply with the requirements of the NetworkCharter (e.g., participation in external audits orresolution of discrepancies) should be advisedthat they risk losing their traceability tointernational standards unless action is taken.The SSC also recommends that the DMRP takessuch action as necessary to encourage theseSSDLs to comply with the SSDL NetworkCharter. The SSC recommends that, if an SSDLfails to comply within one year of notification,the Member State be informed that the SSDLwill cease to be a full member but rather be listedas a provisional member of the network.
Intercomparison of Therapy Level IonizationChamber Calibration FactorsIn this proficiency test programme, the SSDLcalibrates an ionization chamber of its choice, andforwards it to the DMRP laboratory for theircalibration. This test verifies the ability of an SSDLto transfer a calibration from their standard to theuser. Twenty one SSDLs participated. The resultsare presented in Figure 1. The figure includescalibrations in terms of air kerma and absorbed doseto water. Any difference between the SSDL andDMRP exceeding the indicated action levels ispursued by the Agency for resolution. Three of theSSDLs collaborated with the DMRP to resolve thediscrepancies, while one did not.
0 5 10 15 20 250.92
0.94
0.96
0.98
1.00
1.02
1.04
1.06
1.08
6
13
5
3
60Co beam calibration factors
Air kerma
Abs. dose to water cal fr TRS-277
Abs. dose to water-BIPM
SS
DL/
IAE
A
laboratory no.
Intercomparison of ionization chamber calibration factors
in the IAEA/WHO Network of SSDLs, 1997-1998
Figure 1: Ratios of ion chamber calibrationfactors supplied by the SSDLs to those measuredby the IAEA. Circles correspond to air kermacalibration factors and triangles to absorbed doseto water factors. The arrows correspond to thefour large discrepancies, the results followingcorrections being enclosed in the large circles
The SSC considers this SSDL to have brokenits traceability to international standards andtherefore should be a provisional member ofthe SSDL network, until the discrepancy isresolved. The identification of thediscrepancies and the ability of the DMRP toresolve them, emphasizes the importance ofthis programme in assuring that traceability isnot compromised by the SSDLs.
TLD Monitoring of SSDL Measurements atTherapy Levels
This measurement assurance programme is toverify the ability of the SSDL to transfer theionization chamber calibration to thedetermination of absorbed dose under referenceconditions in a water phantom. The SSDLirradiates TLD at a reference depth in a cobalt-60 or high-energy x-ray beam. The TLDs areevaluated at the Agency’s DosimetryLaboratory. The results for the last 5 cycles(2.5 years) are shown in Figure 2. The 11results outside the Agency action level werepursued to identify and resolve thediscrepancies. One of the SSDLs has, as yet,failed to cooperate with the DMRP to resolvethe discrepancy. The SSC considers this SSDLto have broken its traceability to internationalstandards and therefore should be a provisionalmember of the SSDL network, until thediscrepancy is resolved. The identification ofthe discrepancies, and the ability of the DMRP

21
to resolve the discrepancies, emphasizes theimportance of this programme in assuring thetraceability is not compromised by the SSDLs.
The SSC notes that 4 of the SSDLs havingradiotherapy activities have not participated in theTLD audits in the period 1996 to 1998. The SSCsuggests that these SSDLs have failed to completean appropriate proficiency test, therefore are at riskof losing traceability and, as such, should beidentified as provisional members of the network.
0 10 20 30 40 50 600.8
0.9
1.0
1.1
1.2TLD audits for SSDLs: runs 1996/1-2, 1997/1-2, 1998/1
DTL
D/D
stat
60Co beams
high energy X-rays
laboratory no.
±3.5%
Figure 2: Results of the IAEA/WHO TLD postal doseaudits of SSDLs for the delivery of dose to water underreference conditions for the TLD runs 1996/1, 1996/2,1997/1, 1997/2 and 1998/1. Data in the graphcorrespond to the ratio of the Agency’s determined dosefrom the TL-response (DTLD) to that stated by the SSDL(Dstat). Each data point corresponds to the average ofthree dosimeters. A total of 196 beam calibrations werechecked in 59 laboratories, which include 122 60Co(circles) and 74 high-energy x-ray beams (triangles).The number of therapy beams checked in different TLDruns was: 45 beams in 1996/1, 39 beams in 1996/2, 35beams in 1997/1, 36 beams 1997/2 and 41 beams in1998/1. A total of 11 deviations were found outside theacceptance limit of +3.5% (one large deviation in1996/1 run, 4 in 1996/2, and two in each of 1997/1,1997/2 and 1998/1 runs).
New Calibration Services
The DMRP has introduced three new services sincethe last SSC meeting. The SSC recognizes that thedevelopment of these new technologies was possibleonly because three temporary professional staffwere available from various programmes not on theDMRP budget.
Brachytherapy calibrations
A calibration service for brachytherapy re-entrant (well-type) ionization chambers for137Cs sources has been established. Stabilitychecks of the service suggest reproducibility ofthe order of ± 0.5 %. To date, onebrachytherapy chamber has been submitted forcalibration. In order to evaluate the potentiallevel of use of the brachytherapy calibrationservice at the DMRP, the SSC recommends thatthe Network Secretariat survey brachytherapyservices provided by the SSDLs.
Calibration of ionization chambers atdiagnostic x-ray energies, includingmammography.
There is a growing need for quality control andquality assurance in diagnostic radiology,particularly in mammography, where routinescreening of asymptomatic women could leadto significant radiation doses. DMRP has beendeveloping facilities and procedures for thecalibration of ionization chambers atmammography beam qualities. Seventeen beamqualities with HVL from 0.27 to 0.85 mm Alhave been developed. These represent both Moand Ru target and absorbers for both entranceand exit dose qualities. To evaluate thepotential use of the calibration services indiagnostic x rays at DMRP, the SSCrecommends that the Network Secretariatsurvey the SSDLs to identify the servicesprovided and the equipment used in diagnosticx-ray calibrations, including mammography.
TLD dose quality audits for radiationprotection
Following a recommendation of the 7th SSC,the DMRP laboratory has developed a postalTLD programme to audit the ability of anSSDL to calibrate their 137Cs beam used in theSSDL’s personnel dosimetry programme. Twopilot studies have been performed in which 24SSDLs participated. The results are shown inFigure 3. The SSC commends the DMRP forthe significant amount of work performed at ahigh level of expertise. This will benefitradiation protection services for a significantportion of the world's radiation workers andshould be developed further. The SSCrecommends that the pilot study formeasurement standards in radiation protectiondosimetry using 137Cs be made a regularservice. It further recommends that a similarservice be investigated for 60Co.

22
0 5 10 15 20 250.80
0.85
0.90
0.95
1.00
1.05
1.10
1.15
1.20TLD quality audits for 137Cs radiation protection calibrations
Kair
(SSD
L)/K
air(IA
EA)
SSDL no.
±3.5%
Figure 3: Ratios of the air kerma stated by SSDLs tothe TLD measured value at the Agency’s DosimetryLaboratory
PROJECT E.3.02 DOSE INTERCOMPARISONAND ASSURANCE
The IAEA/WHO TLD Postal Service forHospitalsThe IAEA/WHO TLD postal programme formonitoring the calibration of radiation therapybeams at hospitals in Member States continues. TheSSC applauds the DMRP and WHO on a number ofchanges already implemented or proposed toimprove the efficiency of the programme.
Improved return rate
During recent years the return rate for the TLD hasincreased dramatically as seen in Figure 4. Theaverage return between 1990 and 1996 was 60 %and in 1993 to 1995 it was 70 %. Since the last SSCreport, the average return rate has increased to 90 %due to the joint efforts of the WHO and the DMRP.The SSC is pleased to note this important result.
Benefits of repeat TLD
SSC recognizes the impact of the TLD progammeon the individual hospitals. Typically, only 65 % ofthose hospitals that receive TLD for the first timehave results within the DMRP action levels (± 5 %),while 80 % of institutions that have benefited from aprevious TLD audit are expected to have resultswithin the DMRP action levels.
1990 1991 1992 1993 1994 1995 1996 1997 19980
20
40
60
80
100
Y ear
Pe
rce
nta
ge
of
retu
rne
d T
LD
s
T L D re tu rn fro m h o sp ita ls , Ja n . 1 990 - A u g . 1998
Figure 4: Improvement in return rate from hospitalsin the IAEA/WHO dosimetry programme.
Follow up of hospitals outside the acceptablelimits
The results of 429 beam verifications at 241hospitals are shown in Figure 5. As shown,17 % are outside the ± 5 % action level. On therecommendation of the SSC, the DMRP hasestablished a follow-up programme forhospitals outside acceptable limits, contactingthe hospital either through WHO or directly byDMRP staff. All hospitals were contacted. Theresults of this follow-up are seen in Figure 6.These data pertain to the 72 hospitals where adiscrepancy was discovered. Among thesehospitals, 33 resolved their discrepancies. Forthe rest of the discrepancies (see the darkcircles in Figure 5), 13 continue to beunresolved and 26 hospitals have not yetresponded to efforts by the DMRP to help themidentify and resolve the problem. The SSCrecommends that the successful efforts onefforts on follow-up of hospital TLDdiscrepancies be pursued for those hospitalsstill outside the action levels.
Individual TLD reports
The SSC wishes to commend the DMRP ontheir new policy of providing each hospitalwith an individual TLD report for each beammeasured.

23
0 50 100 150 200 250 300 350 4000.6
0.8
1.0
1.2
1.4
1.79
Th era py be am n o .
DT
LD/D
sta
t
T L D c h e c k s , h o s p ita ls : 1 9 9 7 - 1 9 9 8 ( 60C o a n d X -ra y s )
±5%
Figure 5: Results of the IAEA/WHO TLD postaldose audits of radiotherapy hospitals for thedelivery of absorbed dose to water under referenceconditions during 1997-1998 for the TLD batchesB78 to B95. Data in the graph correspond to ratiosof the Agency’s determined dose (DTLD) relative tothe dose stated by the hospital (Dstat). Each datapoint corresponds to the average of two dosimeters.A total of 429 beam calibrations were checked in241 hospitals. Approximately 17% of the resultswere found outside the +5% action level. Black dotsindicate the deviations which have not beencorrected (before August 98).
36%
18%
46%
Figure 6: Pie chart showing the outcome of follow-up dosimeters sent to hospitals outside the actionlevel: 46 % resolved; 36 % not yet returned; 18 %not yet resolved
Improved cost effectiveness
The SSC also wishes to commend the DMRP onvarious actions taken to improve the costeffectiveness of the TLD programme withoutsignificant compromise on accuracy and precision.These include:
• Utilization of a TLD reader that is essentiallyautomatic.
• Reducing the number of TLD in a givendosimetry pack issued for hospital use.
• Projected change to TLD 100 which issignificantly less expensive that the TLD700 presently used.
Turn-around time
DMRP has been able to reduce significantly thetotal turn-around time for the postal TLD,partly through in-house improvements butprincipally through efforts in dissemination ofthe postal packs as coordinated by WHO. TheSSC was pleased to note these improvements.
Transfer of TLD programmes to member states
There are four Member States (China, India,Argentina, and Algeria) that have establishedTLD programmes to audit hospitals in theircountries and which have a formal link to theDMRP laboratory. Recently three otherMember States have established suchprogrammes (Czech Republic, Israel,Malaysia). The SSC notes the positive resultsfrom the CRP on 'the establishment of nationalprogrammes for quality assurance inradiotherapy dosimetry'. The SSC recommendsthat the Agency continue to assist MemberStates to establish national TLD programmes,that whenever possible the DMRP establisheslinks between the national programmes and theAgency, and that the possibility of TC projectsbe explored for this effort.
Radiation Processing DosimetryThe DMRP continues to provide theInternational Dose Assurance Service (IDAS)at radiation processing dose levels usingalanine dosimeters issued and evaluated at theAgency’s Dosimetry Laboratory. The SSCrecognizes that this is a dosimetry programmewith a high level of accuracy that must berecognized for the value of its services.However, the Agency programmes that benefitmost from these services are not within theDMRP. This dosimetry programme thereforeconsumes more than its fair share of resourcesin the DMRP. The need to spread the supportfor this programme throughout other Divisionsin the Agency has been addressed above. Thereal challenge to DMRP is to impress themerits of this dosimetry programme on thosebenefiting from the programme.
The results of the IDAS programme from 1992to 1998 are shown in Figure 7 where 61 % ofthe results are within ± 5 % and 86 % within± 10 % of the DMRP standard.

24
IDAS results 1992 to 1998( 311 data points )
0
20
40
60
80
100
120
-35
to -
30
-30
to -
25
-25
to -
20
-20
to -
15
-15
to -
10
-10
to -
5
-5 to
0
0 to
+5
+5
to +
10
+10
to +
15
+15
to +
20
+20
to +
25
relative deviation (%)
Num
ber
mean = 0.2std.dev. = 6.9max. = 28.1min. = -32.3
Figure 7: IDAS results from 1992 to 1998
The programme to follow up results outside theaction level includes correspondence by letter andrepeat dosimeter irradiations. The SSC recommendsthat the DMRP define the action level for dosimetrydiscrepancies to be investigated within the IDASprogramme and further recommends that the follow-up procedure be improved.
PROJECT E.3.03: TRANSFER OF DOSIMETRYTECHNIQUES
The transfer of dosimetry techniques in the DMRPdosimetry programme is provided throughcoordinated research programmes (CRPs), trainingcourses, fellowships, seminars, symposia, andpublications. Technical Co-operation projects(TCs), which are an important mechanism totransfer technology to developing countries arecovered under Project E.3.04.
Co-ordinated Research Projects (CRPs)The list of active CRPs is included in Table 1and the list of proposed CRPs is given inTable 2.
The SSC is pleased to see that the developmentof a Code of Practice for radiotherapydosimetry based on an ‘absorbed dose to water’standard in CRP E2 40 09 has been endorsedby the IAEA, WHO and ESTRO and that theDMRP is proceeding to the testing phase. TheSSC recommends that the Code of Practice forradiotherapy dosimetry based on an ‘absorbeddose to water’ standard be published as aTecDoc to ensure the widest possibledistribution. The foreword should indicate thatthe protocol is being distributed for evaluationfor two years.
The CRP E2 40 10 has been formally proposedand approved pending external funding. TheDMRP is encouraged to operate this CRP onthe basis of interested countries self-fundingtheir participation.The proposed CRP E3.01 should be precededby a survey to the SSDLs to ascertain theresearch needs at this stage.
The SSC recognizes the need of developingcountries to have tools for evaluating treatment-planning systems, many of which utilize MonteCarlo calculations and supports the proposal inthe CRP E3.03.
Table 1: Co-ordinated Research Projects (CRPs) currently active:
Year of start Subject Year ofcompletion
ParticipatingInstitutions
1995 E2 40 06 Characterization and evaluation of high-dose dosimetry forquality assurance in radiation processing
1999 10
1996 E2 10 02 Development of a quality assurance programme forSecondary Standard Dosimetry Laboratories.
1998 6
1994 E2 40 07 Development of a quality assurance progamme forradiation therapy dosimetry in developing countries.
1998 9
1996 E2 40 08 Dose determination with plane-parallel ionization chambersin therapeutic electron and photon beams
2000 6
1997 E2 40 09 Development of a Code of Practice for dose determinationin photon, electron, and proton beams based on measurementsstandards of absorbed dose to water.
2000 7
1998 E2 40 11 EPR biodosimetry (jointly with NSRW) 2000 9

25
Table 2:CRP’s proposed for 1999-2000:
Year of start Subject Year ofcompletion
ParticipatingInstitutions
E2 40 10 Alanine-ESR dosimetry for radiotherapy
1999 E3.01 (Task 11) Development of techniques for the disseminationof Absorbed dose to water standards to the Secondary StandardsDosimetry Laboratories.
2000
2000 E3.01 (Task 12) Dosimetry and quality assurance for diagnostic x-rays at SSDLs
2003
E3.03 (Task4) Transport simulation for photon/electrons inradiotherapy. (Jointly with RIPC, Nuclear Data)
Training Courses and Symposia
The following courses have been approved for1999 and proposed for 2000.
1999
• Calibration Procedures and Quality Assurancein SSDLs: Interregional (Cuba)
• Modern Techniques and Dosimetry InBrachytherapy: Regional Africa (Egypt)
2000
• Quality Assurance and Process Control inRadiation Processing: Latin America
• Physical Aspects of Quality Assurance inRadiotherapy: West Asia
• Dosimetry Quality Audits in Radiotherapy:East Asia and Pacific
As the interregional seminar on QA for theSSDLs recommended in the 7th SSC Reportcould not be funded by the Agency, the SSCrecommends that a further training course tocover the remaining SSDLs should be held in theyear 2000.
PROJECT E.3.04 TECHNICAL CO-OPERATION
Technical co-operation projects (TCs) are animportant way to transfer technology todeveloping Member States, and a large fractionof the manpower of the DMRP Section isdedicated to TC tasks. In 1997 DMRP providedsupport to 74 on-going TC projects, either as the
main section responsible for providing therequired technical support or sharing theresponsibilities with other sections, mainlyApplied Radiation Biology and Radiotherapy .Manpower planned for this programme was 20%,however, the true professional manpowerdedicated to TC reached up to 35%.
The SSC notes the significant increase inTechnical Co-operation programmes in thedomain of the DMRP which together with theincrease in services to Member States providedby the DMRP has significantly increased theDMRP workload. The SSC recommends that thewelcome growth in demand for radiationdosimetry input to TC projects and DMRPservices be balanced by an increase in resources.
FUTURE TRENDS
The Head of the DMRP presented a strategicplan listing short-term, medium-term and long-term goals. The SSC appreciates these efforts todevelop a strategic plan for the DMRPprogramme. This will be a valuable document toprovide continuity and guide future activities ofthe DMRP. The short-term goals includecompleting the tasks listed in the Blue Book anddiverting resources from the field of high-dosedosimetry to diagnostic radiology dosimetry, aswell as recruiting a new staff member in thisfield by the end of 1999. The SSC recommendsthat the short-term goals of the DMRP strategicplan be implemented
RECOMMENDATIONS
a) The SSC commends the development of thisworking arrangement between the twodivisions (NAHU and NAAL) with regard to

26
implementation of the Agency’s Dosimetryprogramme. However, the SSC notes that thedevelopment of a quality system for DMRPmetrological activities requires that theresponsibilities and duties of the staff atNAHU and NAAL be clearly defined. This isespecially relevant to its laboratory activities.Consequently the SSC recommends that theresponsibilities and duties of the staff atNAHU and NAAL be clearly defined anddocumented.
b) The SSC recommends that a more formalrelationship be developed between NAHUand the other divisions interested in high-doseirradiations (NAPC, NAFA) for futurecollaborative development of the high-dosedosimetry programme.
c) The SSC welcomes the proposal for a WHOseminar for regional officers and recommendsthat this seminar promotes the hospital auditprogramme in radiotherapy dosimetry, andreinforces the importance of the SSDLnetwork.
d) The SSC welcomes the IAEA collaborationwith ESTRO on a number of mutualprogrammes, particularly in regard to theMemorandum of Understanding between theIAEA and ESTRO on their mutualcooperation in radiotherapy dosimetry qualityaudit programmes, and recommends that,where possible, similar arrangements be madewith other external organizations, noting thatsuch collaborations optimize the use ofresources.
e) The SSC recommends that the SSDL NetworkSecretariat establishes Action Levels for allaudit programmes, and notifies theparticipants of these action levels.
f) The SSC is pleased to see that the SSDLCharter has been completed and that theIAEA will publish the Charter jointly with theWHO. The SSC recommends that the Agencyand WHO collaborate to ensure that all thoseinvolved in the SSDL Network receive a copyof the charter.
g) The SSC recommends that the periodicmeasurement assurance tests required in theSSDL Charter be made at a minimum of 2year intervals, and that the NetworkSecretariat notifies all members of thenetwork of this requirement.
h) The SSC recommends that SSDLs who do notcomply with the requirements of the NetworkCharter (e.g., participation in external auditsor resolution of discrepancies) should beadvised that they risk losing their traceabilityto international standards unless action istaken.
i) The SSC also recommends that the DMRPtake such action as necessary to encouragethese SSDLs to comply with the SSDLNetwork Charter.
j) The SSC recommends that, if an SSDL failsto comply within one year of notification, theMember State be informed that the SSDL willcease to be a full member but rather be listedas a provisional member of the network.
k) In order to evaluate the potential level of useof the brachytherapy calibration at theDMRP, the SSC recommends that theNetwork Secretariat survey brachytherapyservices provided by the SSDLs.
l) To evaluate the potential use of thecalibration services in diagnostic x rays, theSSC recommends that the NetworkSecretariat survey the SSDLs to identify theservices provided and the equipment used indiagnostic x-ray calibrations, includingmammography.
m) The SSC recommends that the pilot study formeasurement standards in radiation protectiondosimetry using 137Cs be made a regularservice. It further recommends that a similarservice be investigated for 60Co.
n) The SSC recommends that the successfulefforts on follow-up of hospital TLDdiscrepancies be pursued for those hospitalsstill outside the action levels.
o) The SSC recommends that the Agencycontinue to assist Member States to establishnational TLD programmes, that wheneverpossible the DMRP establishes links betweenthe national programmes and the Agency, andthat the possibility of TC projects be exploredfor this effort.
p) The SSC recommends that the DMRP definethe action level for dosimetry discrepancies tobe investigated within the IDAS programmeand further recommends that the follow-upprocedure be improved.

27
q) The SSC recommends that the Code ofPractice for radiotherapy dosimetry based onan ‘absorbed dose to water’ standard bepublished as a TecDoc to ensure the widestpossible distribution.
r) As the interregional seminar on QA for theSSDLs recommended in the 7th SSC Reportcould not be funded by the Agency, the SSCrecommends that a further training course tocover the remaining SSDLs should be held inthe year 2000.
s) The SSC recommends that the welcomegrowth in demand for radiation dosimetryinput to TC projects and DMRP services bebalanced by an increase in resources
t) The SSC recommends that the short-termgoals of the DMRP strategic plan beimplemented.
CONCLUDING COMMENTS
The Agency’s DMRP programme is vital toensure the traceability of radiation standards andthe quality of radiation dosimetry over a widerange of dose levels in developing countries.
The present programme makes basic radiationstandards available to the majority of developingcountries. External-beam radiation therapy andradiation processing (high dose) have the longesthistory of robust links to international standards.However, the DMRP has recently implementednew projects providing robust links forcalibration of mammography x-ray beams,
brachytherapy sources, and personnel monitoringprogrammes at the participating SSDLs. Perhapsthe most significant progress has been made inthe follow-up of quality audit measurements inwhich a difference outside the established actionlevels has been recorded between the SSDL orother user and the DMRP. The SSC continues toconsider this a high-priority item and commendsthe DMRP on the efforts that they have made inthe past and encourages them to continue todevelop programmes and expand in this area.The SSC also commends the DMRP on theirefforts to transfer the postal TLD programmes tonational and perhaps sub-regional programmesand establishing and maintaining links betweenthese programmes and the DMRP.
The SSC commends the Agency for theircontinued support for the programmes sponsoredthrough the Dosimetry and Medical RadiationPhysics Section. The SSC wishes to emphasizethat radiation dosimetry is a necessary adjunct tomany programmes that utilize radiation atvarious levels. The SSC therefore commends theDMRP and the Agency for the action alreadytaken to develop communications andprogramme sharing between DMRP and otherDivisions, which can benefit from the expertiseof the DMRP staff and the standards maintainedby the Section.
The SSC again commends the staff of theDosimetry and Medical Radiation PhysicsSection for their clear and comprehensivepresentation of the Agency’s DMRP programme.

28
APPENDIX I
PARTICIPANTS
Committee members:A. Allisy, ICRU, Chairman of the SSCP. Allisy-Roberts, BIPMA. Dutreix, FranceK. Hohlfeld, PTB, GermanyS. M. Seltzer, NIST, USAP. Sharpe, NPL, UKS. Shen, China
WHO:H. Østensen, WHO, Co-Secretary of the SSDL Network
Observers:W. F. Hanson, RPC, USAA. Leitner, BEV, AustriaJ. G. Pereira-Peixoto, IRD, Brazil
IAEA staff members:P. Andreo, Head, Dosimetry and Medical Radiation Physics Section, NAHU, Co-Secretary of the SSDLNetworkR. Anglim, Dosimetry and Medical Radiation Physics SectionP. Bera, Dosimetry Laboratory, NAALL. Czap, Dosimetry and Medical Radiation Physics SectionP. De Regge, Head, Physics and Chemistry Instrumentation Laboratories, NAALR. Girzikowsky, Dosimetry and Medical Radiation Physics SectionJ. Izewska, Dosimetry and Medical Radiation Physics SectionA. Meghzifene, Dosimetry and Medical Radiation Physics SectionK. Mehta, Dosimetry and Medical Radiation Physics SectionK. Nagaoka, Dosimetry and Medical Radiation Physics SectionF. Pernicka, Dosimetry and Medical Radiation Physics SectionH. Toelli, Dosimetry and Medical Radiation Physics Section

29
APPENDIX II
AGENDA for the 8th biennial meeting of the Scientific Committee of the IAEA/WHO Network of Secondary StandardDosimetry Laboratories, IAEA, Vienna, October 5-9, 1998
05/10 am (9:00) Opening address by DIR-NAHU, DIR-NAAL
Introductory remarks by P. Andreo and H. Østensen (WHO), co-secretaries of the IAEA/WHO SSDL Network
Adoption of the Agenda and nomination of rapporteur
OVERVIEW OF THE IAEA DMRP SUBPROGRAMME (E3)
∗ Dosimetry Laboratory, QA Manual
PA
PA, KM
pm (13:30) PROJECT E3.01: SSDL NETWORK
• Information on the Network
• Development and QC of standards
∗ External beam radiotherapy
∗ Brachytherapy
∗ Radiation Protection
∗ Diagnostic radiology (mammography)
• Audits to SSDLs (intercomparisons)
∗ TLD results (RT)
∗ Ionization chambers (RT)
∗ TLD results (RP)
PA
AM
LC
HT
LC
FP
JI
LC
FP
06/10 am (9:00) PROJECT E3.02: DOSE ASSURANCE
• The IAEA/WHO TLD postal service∗ Operation of the TLD postal service∗ Analysis of TLD results for hospitals∗ On-going developments
• The high-dose dosimetry programme
∗ Operation of the IDAS postal service
∗ Analysis of IDAS results
PA
JI
BP
JI
KN
KM
RG
KM
pm (13:30) PROJECT E3.03: TRANSFER OF DOSIMETRY TECHNIQUES
• Co-ordinated Research Projects
• Symposium
• Publications
• DIRAC (Directory RT Centres)
PROJECT E3.04 TECHNICAL CO-OPERATION ACTIVITIES
• Training courses and seminars
• Strategy Plan for the DMRP programme
• Other
PA
All
KM
PA
HT
PA
PA
07-09/10 Meeting of the Committee. Draft report.

30
ABBREVIATIONS
BEV Bundesamt für Eich- und Vermessungwesen (Austria)
BIPM Bureau International des Poids et Mesures
CRP Co-ordinated Research Programme
IAEA International Atomic Energy Agency
DMRP Dosimetry and Medical Radiation Physics Section
ICRU International Commission on Radiation Units and Measurements
IDAS International Dose Assurance Service
NIST National Institute of Standards and Technology (USA)
NPL National Physical Laboratory (UK)
NSRW Division of Radiation and Waste Safety, Department of Nuclear Safety
PTB Physikalisch-Technische Bundesanstalt (Germany)
NA Department of Nuclear Sciences and Applications (formerly, RI) IAEA
NAAL Agency’s Laboratories, Department of Nuclear Sciences and Applications(formerly, RIAL)
NAHU Division of Human Health, Department of Nuclear Sciences and Applications(formerly, RIHU)
NAPC Division of Physics and Chemistry, Department of Nuclear Sciences andApplications (formerly, RIPC)
NAFA Division for Food and Agriculture, Department of Nuclear Sciences andApplications (formerly, RIFA)
RPC Radiological Physics Center, Houston (USA)
SSC SSDL Scientific Committee
SSDL Secondary Standard Dosimetry Laboratory
TC Department of Technical Co-operation.General abbreviation for Technical Co-operation project.
TLD Thermoluminescent Dosimeter
WHO World Health Organization

31
COURSES AND MEETINGS TO BE HELD DURING 1999
Training Courses in the field of Dosimetry and Medical Radiation Physics
• Interregional Training Course on Calibration Procedures and Quality Assurance in SSDLs,27 September-8 October 1999, Havana, Cuba.
• Regional Training Course on Modern Techniques and Dosimetry in Brachytherapy, 1999, Cairo,Egypt (exact date not yet known)
• Regional training Course on Clinical Treatment Planning for Teletherapy and Brachytherapy,Palanga, Lithuania, 7-18 June 1998
• AFRA Workshop on Harmonised Methods of Beam Calibrations in External Radiotherapy, June1999, Rabat, Morocco.
• IAEA/ESTRO Workshop on Quality Assurance Networks for External Audits in Radiotherapy(during the International Conference on Medical Physics), Patras, Greece, 31-August-4 September 1998(workshop duration 1.5 day).
Meetings
Consultant’s Meeting to develop brachytherapy calibrationprocedures for SSDLs
Vienna May 1999
Consultant Meeting on the organization of regional educationprogrammes in medical radiation physics and preparation of a“Primer in Radiotherapy Physics”
Vienna To be scheduled
Consultant Meeting on dosimetry in diagnostic radiology, Vienna May 1999
2nd Research Co-ordination Meeting on development of proceduresfor the determination of absorbed dose with therapeutic photon,electron and proton beams based on measurement standards ofabsorbed dose to water
Brussels 3-7 May
Consultant Meeting on qualify assurance methods for radiotherapydose calculations and computerized treatment planning system
Vienna To be scheduled
Consultant Meeting on the verification of the Code of Practice forradiation measurement with parallel plate ionization chambers
Vienna To be scheduled
Consultant Meeting on quality assurance programmes for radiationtherapy dosimetry in developing countries
Vienna To be scheduled
Consultant Meeting on evaluation of high dose referencedosimetry techniques
Vienna May 1999
3rd Research Co-ordination Meeting on Development of QualityAssurance Procedures for SSDLs.
Vienna 29 November-03December 1999

32
MEMBER LABORATORIES OF THE IAEA/WHO NETWORK OF SSDLs
Country City Contact person Fax E-mailALGERIA Algiers Mr. M. Arib +213 264 8842 [email protected] Buenos Aires Mr. H. Hugliaroli +54 14800615 [email protected] Menai Mr. Claudio Tuniz +612 971732577 [email protected] Vienna Mr. H. Stadtmann +43 [email protected]
BANGLADESH Dhaka Mr. A. Sattar Mollah +880 02863051 [email protected] Gent Mr. H. Thierens +32 92646699BOLIVIA La Paz Mr. Ismael Villca +592 2433063BRAZIL Rio de Janeiro Ms. M. de Araujo +552 14421605 [email protected] Sofia Mr. Z. Buchakliev +359 2443114 [email protected]
CANADA Ottawa Mr. R. P. Bradley +1 6139529646 [email protected] Santiago Mr. Oyarzun Cortes +56 227318723 [email protected]* Beijing Mr. Gan Zeuguei +86 1444304CHINA TaiYuan, Shanxi Mr. Chen MingjunCHINA SIMT, Shanghai Mr. Zhang Limin +86 2164701810 [email protected] LIH, Beijing Mr. Li Kaibao +86 10 [email protected] Kowloon-Hong-KongMr. C. L. Chan +852 29586654 [email protected] RM-IAE, Beijing Mr. Guo Wen +86 19357008
COLOMBIA Santafe de Bogota Mr. H. Olaya Davila +54 12220173CUBA Cuidad Habana Mr. J. Morales +53 7331188 [email protected] Nicosia Mr. S. Christofides +357 2369170 [email protected] REP. * Prague Mr. Kodl +42 2738330CZECH REP. CMI-Prague Mr. P. Dryák +420 2 67008 [email protected] REP. RLD-Prague Mr.D. Olejár +42 267311410 [email protected]
DENMARK Bronshoj Mr. K. Ennow +45 44532773
ECUADOR Quito Mr. H. Altamirano +59 32253097 [email protected],ecEGYPT Cairo Mr. H. M. Eissa +20 23612339
FINLAND Helsinki Mr. H. Jarvinen +358 9 [email protected] Le Vesinet +33 139760896
GERMANY Oberschleissheim Mr. D. F. Regulla +49 8931873062 [email protected] Legon - Accra Mr. C. Schandorf +233 21773807GUATEMALA Guatemala C. A. Mr. J. A.Tovar +502 2762007
HUNGARY* Budapest 126 Mr. I. Csete +36 12120147 [email protected] Budapest XII Mr. G. Kontra +36 11562402HUNGARY Paks Mr. M. Orbán +36 1551332
INDIA Bombay Mr. S.C. Misra +91 225560750 [email protected] Jakarta Selatan Mr. Susetyo Trijoko +621 217657950IRAN Karaj Mr. M. Gavahi +98 213130676IRAN Teheran Mr. H. Gharaati +98 216428655IRAQ ** BaghdadIRAQ ** BaghdadIRELAND Dublin 14 Mr. P.A Colgan +353 12697437 [email protected] Yavneh Mr. S. Margaliot +972 8 434696
KOREA Seoul Mr. Woong Beom Oyum +82 23513726 [email protected]
LIBYA Tripoli Mr Ben Giaber

33
Country City Contact person Fax E-mailMADAGASCAR Antananarivo Mr. R. Andriambololona +261202235583 [email protected] Kajang Mr. Taiman Bin Kadni +60 3 8258262 [email protected] Mexico, D. F. Mr. V. Tovar Munoz +52 53297302 [email protected] ** LagosNORWAY Osteras Mr. H. Bjerke +47 67147407 [email protected] Islamabad Mr. Salman Ahmad +92 51429533 [email protected] Lima Mr. Tony Benavente +51 1 4885233 [email protected]* Diliman, Quezon Mr. E. S. Caseria +63 9201646PHILIPPINES Sta. Cruz, Manila Ms. A Lobriguito +63 27116080POLAND Warsaw Mr. Bulski +48 26449182 [email protected] Sacavem Codex Mr. A.F de Carvalho +351 19941995PORTUGAL Lisboa Codex Mr. D'Assuncao Matos +351 17266307
ROMANIA Bucharest Mr. C. Milu +40 13123426RUSSIA St. Petersburg Mr. V. I. Fominych +7 812113 0114
SAUDI ARABIA Riyadh Mr. A. Al-Haj +966 14424777 [email protected]* Singapore Mr. Eng Wee Hua + 65 7384468SINGAPORE RPEDL-Singapore Mr. S. Chong +65 2262353 [email protected] SGH-Singapore Mr. Chua Eu Jin +65 2221720 [email protected] REP. Bratislava Ms. V. Laginová +42 7323711SUDAN** KhartoumSWEDEN Stockholm Mr. J-E. Grindborg +46 87297108 [email protected] Damascus Mr. M. Takeyeddin +963 116112289
TANZANIA Arusha Mr. W.E. Muhogora +255 578554 [email protected]* Bangkok Mr. K. Bhadrakom +66 25806013THAILAND Bangkok Mr.W. Wattanapong +66 22234674 [email protected] Bangkok Ms. W. Thongmitr +66 25613013TURKEY Istanbul Mr. A. Turer +902125482230 [email protected] Tunis Mrs. L. Bouguerra +216 571 630/653
URUGUAY Montevideo Mrs. Anna Firpo FurthVENEZUELA Caracas Mr. F. Gutt +58 25713164 [email protected] Belgrade Mr. M. Kovacevic +381 11455943 [email protected]
** Provisional Network members* SSDL Organization
Collaborating organizations associated with the IAEA/WHO Network of SSDLsInternational Bureau of Weights and Measures (BIPM)International Commission on Radiation Units and Measurements (ICRU)International Electrotechnical Commission (IEC)International Organization of Legal Metrology (IOLM)International Organization of Medical Physics (IOMP)
Affiliated members of the IAEA/WHO Network of SSDLsBundesamt fur Eich-und Vermessungswesen, Vienna, AUSTRIAAustralian Radiation Laboratory, Melbourne, AUSTRALIANational Research Council, Ottawa, CANADALaboratoire de Metrologie des Rayonnements Ionisants, Saclay, FRANCEPhysikalisch-Technische Bundesanstalt, Braunschweig, GERMANYNational Office of Measures, Budapest, HUNGARYEnte per le Nuove Tecnologie L’Energia e L’Ambiente (ENEA),Rome, ITALYElectrotechical Laboratory, Tokyo, JAPANRijks Institut voor Volksgesundheid, Bilhoven, The NETHERLANDSNational Radiation Laboratory, Christchurch, NEW ZEALANDVNIIFTRI, CIS, Moscow, RUSSIAN FEDERATIONNational Physical Laboratory, Teddington, UNITED KINGDOMNational Institute for Standards and Technology, Gaithersburg, USA

.

.

SSDL NewsletterDosimetry and Medical Radiation Physics Section
Division of Human HealthInternational Atomic Energy AgencyWagramer Strasse 5, P. O. Box 100
A-1400 Vienna, Austria
Printed by the IAEA, in AustriaJanuary 1999
99-00028


![[MS-SSDL]: Store Schema Definition Language File Format · The Store Schema Definition Language (SSDL) file format describes the store schema in the Entity Data Model (EDM). SSDL](https://img.pdfslide.us/doc/110x75/607d1d78bc520b0aa53a3213/ms-ssdl-store-schema-definition-language-file-format-the-store-schema-definition.jpg)