Embed Size (px)
Citation preview

THE EFFECTSOF COMPOUNDA (I1-DEHYDROCORTICOST9RONR)ANDCOMPOUNDF (17-HYDROXYCORTICOSTERONE)ON TOTAL
BODYFAT 1
By LAURENCEH. KYLE, RICHARDJ. MEYER,2 MARCUSSCHAAF,3 ANDEDWARDJ. WERDEIN
(From the Department of Medicine, Georgetown University Medical Center, Washington, D. C.)
(Submitted for publication April 4, 1956; accepted May 17, 1956)
Speculation regarding the influence of adrenalcortical hormones on body fat has engendered littleexperimental scrutiny, a deficiency which undoubt-edly stems from the difficulties in performing invivo measurement of the fat content of the body.Fundamental observations of Behnke, Feen, andWelham (1) on the relationship of body fat tobody specific gravity suggested the possibility ofutilizing serial measurements of body specificgravity for the evaluation of hormonally inducedchanges in body composition (2). Measurementof specific gravity by underwater weighing hasbeen used in this laboratory to study the effects ofACTH, Compound E, Compound F and, to verylimited degree, of Compound A on body fat (3).Because of an apparent increase in fat during treat-ment with Compound F, and because Compound Ahas been implicated as a fat-affecting hormone,more complete study of these hormones was be-lieved desirable.
METHODSAND MATERIALS
The subject of this study was a 37-year-old white manwith chronic dermatitis. He was hospitalized on themetabolic ward for two periods of about 4 months eachunder conditions of constant activity. The first study wasperformed when he was moderately depleted and the sec-ond study was conducted 15 months later after consid-erable repletion of fat and protein had been accomplished.
Body weight was measured each morning before break-fast, following completion of the 24-hour urine collec-tion. The patient was given a constant diet containing2200 calories, 90 grams of protein, 105 grams of fat and
1 This study was supported by the William Wade Hin-shaw Fund and by a contract between Georgetown Uni-versity and the Office of Naval Research. Reproductionin whole or in part is permitted for any purpose of theUnited States Government.
2Formerly a Research Fellow of the National In-stitutes of Health.
Formerly the William Wade Hinshaw Cancer Re-search Fellow.
225 grams of carbohydrate. Intake of sodium and po-tassium was calculated from standard food tables, al-lowance being made for sodium given as sodium thio-cyanate. Rejected portions of the diet were given withthe following meal; unfinished portions of the eveningmeal were given before sleep. The subject was permittedto leave the hospital for a few hours once weekly; thereoccurred only one major and a single minor violation ofthe dietary routine at these times.
Blood for laboratory analysis was drawn in relativelyconstant amounts and at regular intervals to provide uni-form nitrogen loss by this route. Aliquots of 2-daypooled urine collections were refrigerated until analysis.Urinary nitrogen was measured by a micro-Kjeldahl tech-nique. Nitrogen loss from blood sampling and in stoolswas estimated to total 1.6 gm. per day. Urinary sodiumand potassium were measured by an internal standardflame photometer. Water balance was estimated fromthe difference between urine output and fluid intake, con-sisting of the liquid portion of the diet and measuredamounts of distilled water.
Body specific gravity was obtained by the method ofunderwater weighing devised by Behnke, Feen, and Wel-ham (1) as described from these laboratories (2, 3):
Sp Weight in airSp. Gr- Weight in air - true weight in water
Submerged weight was measured at a water temperatureof 32 to 340 C. and corrected for residual lung volume,measured by the helium dilution technique of Willmonand Behnke (4). In correcting for residual lung volume,density of the water was ignored because of the minorerror involved as well as the fact that data were obtainedfrom successive measurements of the subject under thesame standard conditions. At the time of each meas-urement underwater weight was obtained during bothdeep inspiration and full expiration. The difference waschecked against measured vital capacity to insure expira-tion to a relatively constant volume of residual air ateach weighing.
Total body fat was estimated by substitution in theRathbun-Pace equation (5), formulated on the assump-tion that the specific gravity of fat is 0.918:
%Fat = 100( 5548 _ 5.044'0ks~~~p. gr. S04
Total body water was calculated from specific gravityby substitution in the equation derived by Osserman,
1045

L. H. KYLE, R. J. MEYER, M. SCHAAF, AND E. J. WERDEIN
DAY I 1115 71 9 $113 1 Iny I-alml mbl-ti c Mm &
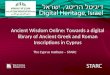
FIG. 1. METABOLIC CHANGESDURING TREATMENTWITH COMPOUNDA
Pitts, Welham, and Behnke (6):
%Water = 100 (4.340 -_ 3g983sp. gr.
Fat free solids were assumed to comprise the differ-ence between body weight and the sum of the weights offat and water.
Because estimation of body composition by the specificgravity method is accurate only in the normally hydratedsubject greatest reliance was placed on those measure-
ments obtained when there existed the least amount ofcompartmental distortion. Parallel measurements ofbody water compartments were made by volume distri-bution techniques, particularly during the second study.Total body water (TBW) was estimated by measure-
ment of antipyrine space, using the technique of Brodie,Axelrod, Soberman, and Levy (7) and by D20 space,using the method of Broida, Morowitz, and Selgin (8).The extracellular fluid compartment (ECF) was assumedto be 70 per cent of the thiocyanate space, measured as
described by Eder (9). Intracellular fluid (ICF) was
assumed to be the difference between TBWand ECF.In all calculations involving total body water the valuesfor antipyrine space were used because these checked
much more closely with estimation of total body waterby the specific gravity method than did the D20 space.
Measurement of these fluid compartments permittedtwo methods of correction of hydration abnormality in
estimating fat from body specific gravity. One con-
sisted of substitution of the value for body density andthat for antipyrine space in the equation derived by Siri(10):
%Fat = 225 (1/D) - 0.76% water - 150.
Proper correction was made for the density of water(0.994 at the temperature used to obtain submergedweight) in conversion of specific gravity to density.The other correction applied was that of variation in ECF(corrected thiocyanate space) in the density equation:
D = Molausse as suggested by Keys and Brozek (11),correcting for the density of water on each occasion.
Calculation of change in body fat was also conductedby application of volume distribution techniques. Theconcept of the fat free body advanced by McCance andWiddowson (12) was utilized as follows:
Fat = weight-T-( A 7 )-0.075 (T + A6T)
1046
ET5:CP2f l' 200. ISS
BODYWEIGHT 6421
_4
0
|000WATER -400
SALANCE o Cetrel
itM1ooegoo 10/k/a
goo
Soo~umO200.
URINE (moq.)1001 Intake
Sodium
801
~ ~ l
SPEOIFIC 6RAvl r Y 1.o0o' ^1.06
--169L-Nfl .- lell I= m an m Kii-M PR pn N
IL

EFFECTS OF COMPOUNDSA AND F ON BODY FAT
DVA
TO
(kg.) Q
-4]
NITROGENBALANCE e
( g .)_ I
-2. gWWk y 0
woc
WATER -o00cBALANCE 0C Control
(m1.) +4
goo
URINE (m q.)
Sodium
.- HF-L---j WL-
20
200.
150Ilat.
RODt 0A~~IOPotusslum Intake
spECIFIc eRA4wry 1.066 1.0611.070
FIG. 2. METABOLIC CHANGESDURING TREATMENTWITH COMPOUNDF
where T is corrected thiocyanate space and A is anti-pyrine space. Change in fat was also determined fromthe difference between total weight change and the sum
of the changes in antipyrine space and nitrogen balancex6.25 (13).
Density of tissue gained was calculated from the ratioof change in the subject's weight to change in his volume.
Oxygen consumption was measured under fasting con-
ditions by a closed circuit clinical apparatus. The aver-
age of two determinations was used in each instance.Urine calcium was measured by the method of Clark andCollip (14).
Compound A acetate was given intramuscularly in 3to 4 divided doses each day. Compound F was adminis-tered orally every 6 to 8 hours.4
RESULTS
The metabolic changes which accompanied treat-ment with Compound A are shown in Figure 1.Nitrogen balance, which was very positive during
4These drugs were obtained through the generosity ofDr. Augustus Gibson of Merck & Co.
the control period, became less positive, but onlytemporarily, when Compound A was started andwhen the dose was increased. Retention of bothwater and sodium occurred at these times. Bodyweight, which was increasing during the controlperiod, rose more sharply during therapy but felloff quickly with the salt and water diuresis whichfollowed cessation of treatment. Body specificgravity was 1.070 at the beginning of treatment-1.068 after the post-treatment diuresis.
The changes with Compound F are depicted inFigure 2. During the control period the patientwas in approximate nitrogen balance and very littlechange resulted from the administration of Com-pound F. Retention of water and sodium was ofsimilar magnitude to that noted with Compound Atherapy. There was acceleration of weight gain,particularly when ACTHwas given briefly at thetermination of treatment. Cessation of all therapywas again followed by diuresis of salt and water
1047
1pFl pq p py p pp lr Ir l loll pol laws WL - Pit --*wTff7A.-- -,.. - --. - -- .-.. - - U-j L-A -.. I-A I.-I V--d %A I..l I..l udmd--V.- ima 1.1 lord lid-mi be kw EirT
M/Y/jl&LLJ21a"
r- gap% P.A C Inn MA.GOO. F ZUU m-. '_!

L. H. KYLE, R. J. MEYER, M. SCHAAF, AND E. J. WERDEIN
with loss of weight. Body specific gravity, whichwas 1.070 at the end of the second control period,fell to 1.061 after the administration of CompoundF.
Figure 3 summarizes the changes in body com-position during the entire study. Here again maybe seen the weight gain during the control period,more rapid gain with Compound A and decreasein weight when therapy was discontinued. Bodyspecific gravity decreased slightly during treat-ment and rose after the post-treatment diu-resis. During the second control period therewas steady increase in weight and slight rise inspecific gravity to the previous control value.WhenCompound F was given there occurred morerapid weight gain and a pronounced lowering ofspecific gravity. This fell to 1.056 with the in-creased water retention accompanying ACTHtherapy and rose moderately after treatment wasdiscontinued.
It may be recalled that this technique of meas-urement is considered most valid when the majorbody constituents are in relatively normal propor-tions, particularly when there is no abnormal hy-dration. Consequently detailed analysis was made
of four specific gravity determinations, selected attimes when hydration abnormality should havebeen absent or minimal: C1-prior to treatmentwith Compound A; A-following the post-treat-ment diuresis when body weight had stabilized;C2-just before treatment with Compound F and;F-after the diuresis which followed cessation oftreatment. At C1 specific gravity was 1.070 indi-cating a total fat content of 8.7 kg. Followingtreatment with Compound A the specific gravitywas 1.068, representative of a total body fat valueof 9.7 kg. At the end of the second control pe-riod (C2) body specific gravity was identical withthe original control value- 1.070; but after theadministration of Compound F, specific gravityfell to 1.061 indicating a 3.5 kg. increase in bodyfat. These changes in body composition are showngraphically at the bottom of Figure 3. Duringtreatment with Compound A there was a moderateincrease in all three major body constituents butfat increased only one kg.-less than can be con-sidered significant by this method of measurement.During the second control period there appearedto be a continued gain in water and fat free solidsand an insignificant loss of fat. During treatment
D'A I f% IOL 13 O,0 MU 30 AO% A0 SQ ..55 - - - -
BODYwwr(4 SPY?R
1Ou
60 1.605S. 5.O4
COMPOSITION(kg.)
WoyPATH -
WYINTER -
ACANswos -
561CHANGE INCOMPOSITION
(to.)
4.-
3.-2-
+1
0--_ -
c
61.68.7
3. I14.8
I p . A I
'B_Sody Specific Gravity
-- --
so so 70 75 90 ao90 too NOF
I - To'd-
F I
ody Weight
t. A
64.29.7
39.215.3
65.0 69.79.2 12.9
40.2 41.515.6 15.3
Ca- F
A .- C2WTER
DII
FIG. 3. CHANGESIN BODY COMPOSITION WITH COMPOUNDSA AND F
I .-
1048
WAr I 0 IV 13 20 Z5 30 35 40 45 50 55
A

EFFECTS OF COMPOUNDSA AND F ON BODY FAT
with Compound F a significant gain in fat isapparent.
These results indicated quite clearly that Com-pound A has no particular effect on body fat.There did appear to be a significant increase intotal body fat during the administration of Com-pound F. Three possible explanations for thesechanges were considered:
1) Fat storage occurred only because proteinrepletion had become complete. Lack of a sig-nificant gain in fat during the second control pe-
riod, when the patient was in approximate nitro-gen balance, was a strong argument against thishypothesis.
2) True acceleration of fat deposition had oc-
curred. This possibility, while more plausible thanthe first, lacked a clear explanation of the mecha-nisms involved. Insignificant protein catabolismand use of an isocaloric diet throughout the studyindicated the absence of liponeogenesis and there-fore some change in energy requirements or inter-mediary metabolism merited consideration.
3) The gain in fat was apparent rather than realbecause of change in other body constituents.Loss of material of high density, such as bonemineral, in sufficient amounts to cause such a sig-nificant change in specific gravity seemed very un-
likely. The possibility of abnormal fluid retentioncould not be entirely discounted for antipyrinespace determinations made throughout the studywere too variable to permit precise correction forminor hydration abnormality. On the other handthe degree of water and sodium retention duringtherapy with Compound F appeared no greaterthan with Compound A, which demonstrated an
insignificant effect on body specific gravity.In view of these possibilities a second study was
conducted, utilizing the same metabolic regimenbut with the inclusion of multiple measurementof fluid compartments, so as to permit better cor-
rection of hydration abnormality and allow ap-
plication of other methods of fat estimation. Inaddition, periodic measurement was made ofoxygen consumption and urinary calcium excre-
tion. During the 15 months' interval betweenstudies the patient was maintained on 20 mg. ofCompound F daily and encouraged to take more
food so as to begin his second study at a higherlevel of body fat and to insure protein repletion.These objectives were accomplished, for at the
beginning of the second study fat had increased to13.5 kg.-nearly 5 kg. more than at the beginningof the first study-and protein stores were nearlyreplenished as indicated by the nitrogen balances.
Figure 4 depicts the metabolic changes andmeasurement of fluid compartments throughoutthe second study. Changes in weight were essen-tially the same as before, i.e., steady slow gainduring each control period, more rapid gain dur-ing treatment with Compound F and loss of weightafter cessation of therapy. Despite the markedincrease in excretion of sodium following the firstcourse of Compound F no retention of sodiumoccurred during treatment; in fact urinary sodiumexceeded that noted in the control period. Duringthe second course of Compound F therapy therewas moderate sodium retention and towards theend and after completion of treatment loss of so-dium was noted. A moderate increase in nitrogenexcretion accompanied the administration of largerdoses of Compound F on one occasion but verylittle protein breakdown occurred during the sec-ond course of Compound F therapy. Total bodywater measurements gave no indication of overhy-dration; in fact, antipyrine and D20 spaces indi-cated the existence of mild dehydration after thediuresis which followed cessation of treatment.
Figure 5 demonstrates the changes in body com-position estimated from specific gravity measure-ments during the entire second study. During thefirst control period there was increase in weightwithout significant variation in specific gravity.Administration of Compound F was accompaniedon both occasions by more precipitous gain inweight and significant lowering of specific gravity.The fall in weight after cessation of therapy wasassociated with but little return of specific gravitytowards control levels.
As in the first study certain periods were se-lected for special analysis, chosen at times whenminimal hydration abnormality was likely: C1-atthe beginning of study; C2-immediately beforethe first course of Compound F; F1-after thepost-treatment diuresis; C3-after a second con-trol period and F2-at the end of treatment.
The results of this study were generally in ac-cord with the first. There occurred significantdecrease in specific gravity indicative of substan-tial increase in fat during the administration ofCompound F. Fat increased 1.9 kg. during F1,
1049

L. H. KYLE, R. J. MEYER, M. SCHAAF, AND E. J. WERDEIN
PERIOD-2 DAYS I 3 5 7 9 11 13 15 17 19 21 23. 25 27 2931 333537 39 41 43 45474951 53
COWCiF mgm/daY _ _t Im 20
t2 BODYWEIGHT_BODY 70 At
(Ks) 66,^0
6--XYGEN CONSUMPTIONNITROGEN - 4 On_
BALANCE + 08 I_URINEI I1.*i122SS1 OlOS
URINE250
SODIUM 2001
501150
POTASSIUM 1001 TKE
mEq/DAY 50J
CALCIUM 2001*g/y 1001
BODYSPVECC L053 L57 11062 OSWLGO1.046 1046 1.049LO4S10461.0431.045 1.0391.041 1.041GRAVITY
T B W(UTERS)SPECFIC 0RAI 34.0 358 352 36.4 365 37.4 38.1 36.5 36.8 36.5 37.2 37.5 376 37.0 35.A4TIPYNE SPACE 36D 36.7 36.0 35.3 36.2 347 38.1 42. 38 36.0D&0 SPACE 43LC 42.7 39.0
SCN SPACEX 0.7 12.0 1IL6 10.9 11.4 12.4 102 102 10.4 125 1t.4
FIG. 4. CHANGESIN METABOLIC BALANCEAND FLUID COMPARTMENTSDURING Two COURSESOF COMPOUNDF
2.0 kg. during F2 and totaled 5.3 kg. from C2 tothe end of the study. There also appeared to be a
continued rapid gain in body fat between the twocourses of Compound F. While this might suggestcontinued lipogenic effect of Compound F aftercessation of treatment, it was more probably dueto fluid reaccumulation. As shown by the deter-minations of total body water (Figure 4), thereappeared to have been restoration of normal hy-dration during the second control period, which,because of addition of a material of low density,would indicate gain in fat. This apparent changein hydration suggests that gain of fat during treat-ment with Compound F was even more pro-
nounced than indicated by the fat estimates de-rived from these specific gravity data.
As shown in Figure 4 oxygen consumptiontended to increase during treatment with Com-pound F and excretion of calcium was insufficientto account for any measurable decrease in bodyspecific gravity.
Table I compares the changes in body fat esti-mated by several different methods during thesecond study: (A) from specific gravity data (B)by substitution of body density and total bodywater (antipyrine space) in the same formula (C)by correction of the density equation for hydrationabnormality as determined by change in thiocya-nate space (D) by use of the technique of McCanceand Widdowson (12) in estimation of the fat-freebody mass and (E) by estimation of change infat from change in body weight, change in totalbody water and nitrogen excretion. Use of thesemethods offers further support for the presence ofa true increase in fat during the administration ofCompound F. They also indicate that the specificgravity method of fat estimation is more uniformthan those techniques which utilize only volumedistribution. Although concurrent application ofmeasurement of total body water to circumventhydration abnormality has definite theoretical ad-vantages it should be pointed out that the use of
CONSUM260[260240220200
cc/mEn
1050

EFFECTS OF COMPOUNDSA AND F ON BODY FAT
DAY I s D 20 25 30 35 40 45 50 56065 70 75 0 65 909 100 IOS 110
CPD. F flf7g]dny)M
WT.(kg.) SP.OR.
?' Ws$__X-->°YSp i+?2 1054 Body Specific Gravity
71 .03|2 C,_ -X , C
?OLOSo- NA
Go 1.044 -
66- ]46,643- 1.040 C61- 1.036
60- 036 ~~C C2 F, C3 F2COMPOSITION(kg.) 1.0531 1.052 1.0491 [1.jJ 1.041
BODYWEKGT - 60.7 63.1 662 68.3 69.3
19.816.4 17.814.5BODYFAT - 13.7
BODYWATER - 332
FAT FREE SOLIDS- 13.2
4
WATER lo -LEANJ SOLIOS5-1
-I.,
CHANGEINCOMPOSITION
(kg.)
FIG. 5. CHANGESIN BODY COMPOSITION WITH COMPOUNDF (SECOND STUDY)
35.0
13.6
36.3 36.3
14.1 14.2
35g6
1M9
Cj-', Fs
U
poorly reproducible techniques, such as antipyrinespace, cannot always strengthen the value of a
readily reproducible method such as measurementof specific gravity.
Table II summarizes the results of both studiesin terms of gain in fat per day and estimation ofthe density of the changed tissue as determinedfrom measurements of body specific gravity. Dur-ing the control period fat was gained at the rate of41 gm. per day-during administration of Com-pound A fat gain averaged 32 gm. per day. WhenCompound F was given, fat increased at a rate of90 gm. per day during the first study and 64 gm.per day during the second, the latter value beingobtained from data which included the control pe-
riod between the two courses of Compound F.Calculation of density of added tissue revealed
a value of 1.026 during the control period and1.040 during treatment with Compound A indi-cating a gain of all major body constituents. WhenCompound F was administered density of addedtissue was 0.940 during the first study and 0.941during the second. Available data indicate that
these values approximate those of adipose tissue(15, 16).6
DISCUSSION
The belief that adrenal horrnones promote anincrease in fatty tissue arose from clinical observa-tion of the abnormal body configuration in Cush-ing's syndrome. Patients with this disorder usu-ally manifest an apparent gain in fat, particularlydistributed in the upper third of the body and fre-quently associated with wasting of the lower ex-tremities. Studies of the relationship of adrenalhormones to body fat in lesser animals are socontradictory and difficult to interpret that com-plete review is redundant for the purpose of thisdiscussion. Concise summaries of published workon the subject, such as those of Thorn and his as-sociates (17), Ingle (18) and Engel and Scott(19) indicate that no clear-cut opinion regardingadrenal-fat relationships can be rendered. Studies
6 It should be noted that adipose tissue consists of fat,water and protein and, consequently, has a greater den-sity than pure fat
millill
1051
C2--w F,
Fi--*C3

L. H. KYLE, R. J. MEYER, M. SCHAAF, AND E. J. WERDEIN
TABLE I
Changes in body fat as estimated by different methods
C,--.C2
C2- Fi
C3-- Fg
C2- F2
A B C D E
SPECIFIC D + TBW CORRECTION FROM FAT- ANTIPYRINEOF D0 M BY FREE BODY S NITROGEN
GRAVITY (SIRI) SCN SPACE MASS BALANCE
+ 0.8 + 1.7 + 1.5 + 1.8 + 2.1
+ 1.9 +3.8 +2.2 +5.4 +5.3
+ L4 -12 +1.4 -3.9 - 1.9
+ 2.0
+ 5.3
+2.9
+ 5.5
+ 1.7
+ 5.3
+ 5.5
+7.0
+ 3.0
+ 6.4
conducted by Kendall (20) indicated a very sig-nificant increase in fat with Compounds A and B,but Kochakian (21) found no lipogenic effectfrom purified Compound A.
Very few data are available on the relationshipsof corticoids and fat in humans. While there doesappear to be a marked increase in fat in Cushing'ssyndrome it remains unknown whether this is a
real gain or merely a redistribution. Neither isit known whether this "obesity" is the result ofover-eating, the product of increased protein ca-
tabolism or tangible evidence of a direct hormonaleffect. In fact we cannot even be sure that thislocal accumulation represents normal adipose tis-sue. Measurement of body fat by the specificgravity technique before and after the surgical cor-
rection of Cushing's syndrome is now underwayin this laboratory. Preliminary observations indi-cate that correction of adrenal hyperfunction re-
sults in a significant decrease in body fat but also
suggest that excessive body water is a major ab-normality in Cushing's syndrome. Kinsell and
his associates (22), from a study of diabetic pa-tients, concluded that adrenal steroids acceleratethe formation of carbohydrate from fat. Ziff,Simson, and Bunim (23) measured antipyrine,bromide and chloride spaces during adrenal stimu-
lation in five patients with rheumatic disorders.In two cases weight gain exceeded the increasein antipyrine space to such degree as to indicate
significant gain in body fat. Using the specificgravity method of fat estimation Doolan, Welham,and Kyle (3) studied the effects of ACTHandadrenal steroids on total body fat. ACTH ap-
TABLE It
Average gain in fat and density of tissue gained
CONTROL Cpd. A Cpd. F (l) Cpd F (2)
Density of 1.026 1.040 0.940 0.941Tissue Gained
Gain in Fat 41 32 90 64(gm./day) I.I_I_ __
peared to induce loss of body fat without signifi-cant change in lean tissue suggesting that the ex-cessive fat catabolism had spared protein. Theadministration of large doses of Compound Eresulted in a marked increase in protein catabolismand an apparent relative sparing of body fat. Dur-ing the administration of Compound F there oc-curred a significant decrease in specific gravity,which, though partly the result of loss of leantissue, also suggested an increase in fat.
The present study indicates quite definitely thatCompound A has no measurable effect on totalbody fat. There did appear to be a significant andrather substantial gain in adipose tissue duringtreatment with Compound F. Because of the diffi-culty in explaining the mechanisms involved andin view of the limited application of these bodycompositional measurements in clinical investiga-tion, it seems pertinent to re-evaluate the metho-dology employed before assuming that the gain infat was real.
As pointed out by Keys and Brozek (11) thespecific gravity of the fat free human body can-not be determined with precision. Furthermore,the fat prediction equation utilized in these stud-ies is derived from measurement of small ani-mals, whose proportional body composition andskeletal mass differs from the human subject. Itis therefore obvious that a single determination ofspecific gravity, or even multiple determinationsin a metabolically stable subject, cannot providedata which will portray the exact amount of bodyfat. In conducting serial determinations on asubject of changing fat content, however, a muchhigher degree of accuracy is possible. In ourhands the summation of possible errors, includingmeasurement of residual lung volume, accuracy ofscale and reproducibility of replicate determina-tions indicate that loss or gain of fat must ap-proach 1.5 kg. to be significant. The gains in fat
1052

EFFECTS OF COMPOUNDSA AND F ON BODY FAT
with Compound F observed here were well in ex-cess of that figure.
Apparent gain in fat, as judged by lowering ofspecific gravity, could also result from addition ofother material of low density, such as water, orloss of body constituents of high density, such asprotein or minerals. In the study reported hereit is obvious that there was insufficient loss ofhigh density body constituents to account for morethan a fraction of the specific gravity change.Consequently the existence of significant overhy-dration remains as the only factor which couldlead to distortion of the data sufficient in degree toproduce an artifactual gain in body fat. In thefirst study variation in total body water determina-tions was of sufficient magnitude to prohibit cor-rection of minor hydration abnormality. How-ever, the changes in weight, sodium excretion andwater retention were nearly identical during treat-ment with Compound A and Compound F andonly in the latter instance did there occur a sig-nificant change in specific gravity. In the secondstudy more accurate measurement of antipyrinespace and the addition of D2O and thiocyanatespace measurements provided a clear indicationthat no significant water retention occurred. Infact, there appeared to be mild dehydration afterthe diuresis which followed cessation of treatmentwith Compound F. Such loss of water wouldtend to minimize the measured gains in body fatwhich occurred during therapy. Consequently allevidence indicates that the gain in fat was trulysignificant during treatment with Compound F.
The mechanisms responsible for the increase inbody fat are completely obscure. Liponeogenesisfrom protein obviously did not occur and, asjudged by oxygen consumption, there was no de-crease in energy production during therapy. Thuswe can only postulate some change in intermediarymetabolism which permitted the addition of fatwithout appreciable change in the measured com-ponents of the metabolic pool. This suppositionobviously lends itself to speculation regarding thehypothesis that some persons, at least under cer-tain circumstances, can maintain their weight oreven become obese on a remarkably small caloricintake. Studies of the type reported here shouldprovide more exact data regarding gain or loss ofbody fat and permit a more objective approach tothe problems of obesity.
SUMMARY
Serial determinations of body specific gravitywere combined with balance study and measure-ment of body water compartments to determine theeffect of Compounds A and F on body fat. Theadministration of Compound A for 26 days hadno demonstrable effect on body fat. The adminis-tration of Compound F for similar periods of timeon three separate occasions was associated with asignificant increase of total body fat. This gain infat was not accompanied by evidence of eitherliponeogenesis from protein or decreased energyproduction.
ACKNOWLEDGMENT
Wewould like to express our appreciation for the as-sistance of the personnel of the Experimental DivingUnit, U. S. Naval Gun Factory in performing thesestudies. The advice of Drs. Albert Behnke and WillSiri has been invaluable in the conduct of this investiga-tion.
REFERENCES
1. Behnke, A. R., Jr., Feen, B. G., and Welham, W. C.,The specific gravity of healthy men. Body weight
+. volume as an index of obesity. J.A.M.A., 1942,118, 495.
2. Kyle, L. H., Welham, W. C., Doolan, P. D., andSchaaf, M., Study of the extrathyroidal effects ofthyroid-stimulating hormone. J. Clin. Endocrinol.& Metab., 1954, 14, 1029.
3. Doolan, P. D., Welham, W. C., and Kyle, L. H.,Studies on the effect of ACTHand certain adrenalsteroids on total body fat. Metabolism, 1955, 4,39.
4. Willmon, T. L., and Behnke, A. R., Residual lungvolume determinations by the methods of heliumsubstitution and volume expansion. Am. J. Phys-iol., 1948, 153, 138.
5. Rathbun, E. N., and Pace, N., Studies on body com-position. I. The determination of total body fat bymeans of the body specific gravity. J. Biol. Chem.,1945, 158, 667.
6. Osserman, E. F., Pitts, G. C., Welham, W. C., andBehnke, A. R., In vivo measurement of body fatand body water in a group of normal men. J.Applied Physiol., 1950, 2, 633.
7. Brodie, B. B., Axelrod, J., Soberman, R., and Levy,B. B., The estimation of antipyrine in biologicalmaterials. J. Biol. Chem., 1949, 179, 25.
8. Broida, H. P., Morowitz, H. J., and Selgin, M., Op-tical spectroscopic determination of hydrogen iso-topes in aqueous mixtures. J. Res. Nat. Bur.Stand., 1954, 52, 293.
9. Eder, H. A., Determination of thiocyanate space.Methods in Med. Research, 1951, 4, 48.
1053

L. H. KYLE, R. J. MEYER, M. SCHAAF, AND E. T. WERDEIN
10. Siri, W., Personal communication.11. Keys, A., and Brozek, J., Body fat in adult man.
Physiol. Rev., 1953, 33, 245.12. McCance, R. A., and Widdowson, E. M., A method
of breaking down the body weights of living per-sons into terms of extracellular fluid, cell mass andfat, and some applications of it to physiology andmedicine. Proc. Roy. Soc., London, Series B,1951, 138, 115.
13. Moore, F. D., Haley, H. B., Bering, E. A., Jr.,Brooks, L., and Edelman, I. S., Further obser-vations on total body water. II. Changes of bodycomnposition in disease. Surg., Gynec. & Obst.,1952, 95, 155.
14. Clark, E. P., and Collip, J. B., A study of the Tisdallmethod for the determination of blood serum cal-cium with a suggested modification. J. Biol. Chem.,1925, 63, 461.
15. Behnke, A. R., Osserman, E. F., and Welham, W. C.,Lean body mass. Its clinical significance andestimation from excess fat and total body waterdeterminations. Arch. Int. Med., 1953, 91, 585.
16. Keys, A., Anderson, J. T., and Broiek, J., Weightgain from simple overeating. I. Character of thetissue gained. Metabolism, 1955, 4, 427.
17. Thorn, G. W., Jenkins, D., Laidlaw, J. C., Goetz,F. C., Dingman, J. F., Arons, W. L., Streeten,
D. H. P., and McCracken, B. H., Pharmacologicaspects of adrenocortical steroids and ACTH inman. (Continued.) New England J. Med., 1953,248, 284.
18. Ingle, D. J., The biologic properties of cortisone:A review. J. Clin. Endocrinol., 1950, 10, 1312.
19. Engel, F. L., and Scott, J. L., The role of hormonesin adipose tissue glycogen synthesis in the rat:The adrenal cortex. Endocrinology, 1951, 48, 56.
20. Kendall, E. C., Influence of the adrenals on car-bohydrate metabolism. Conf., on Metabolic As-pects of Convalescence Including Bone and WoundHealing, 10, 1945, 81.
21. Kochakian, C. D., Adrenal cortical steroids. Conf. onMetabolic Aspects of Convalescence Including Boneand Wound Healing, 6, 1944, 13.
22. Kinsell, L. W., Michaels, G. D., Margen, S., Par-tridge, J. W., Boling, L., and Balch, H. E., Thecase for cortical steroid hormone acceleration ofneoglucogenesis from fat in diabetic subjects. Asummary of five years' investigative work. J. Clin.Endocrinol. & Metab., 1954, 14, 161.
23. Ziff, M., Simson, J., and Bunim, J. J., Effect ofACTH on water distribution in man as meas-ured by antipyrine, T 1824 and bromide. J. Clin.Invest., 1952, 31, 829.
1054

![RESEARCHARTICLE Rugby-SpecificSmall-SidedGamesTraining ... · muscle fibre,andmusclefibre area[12].However, todate, therehasbeennopublishedre- searchdirectly investigating theeffects](https://img.pdfslide.us/doc/110x75/5f5dfc9299447d03974b381b/researcharticle-rugby-specificsmall-sidedgamestraining-muscle-fibreandmusclefibre.jpg)