Embed Size (px)
Citation preview
I ORIGINAL ARTICLES I
Drug prescribing for the elderly in Saskatchewan during 1976S.L. SKOLL,* MB, DPH; R.J. AUGUST,t MA; G.E. JOHNSON,. PH D
Over 110/0 of Saskatchewan's population is 65 years of ageor older. To study patterns of prescribing for the elderly acomputer file of more than 3.6 million prescriptions filledin Saskatchewan in 1976 was reviewed. The elderly popula-tion (aged 65 years or more) that year was 102 070, and77.30/0 received at least one prescription drug listed in theSaskatchewan Formulary. In comparison with a "middle.aged" group (persons between the ages of 35 and 54 years)the elderly showed moderately higher average numbers ofprescriptions filled and drugs used per person that year.However, the prescription of antihypertensive agents anddiuretics increased dramatically with age, and barbiturates,in view of their potential toxicity, appeared to be over-prescribed for the elderly.
Plus de 110/o de Ia population de Ia Saskatchewan est Ag6ede 65 ans ou plus. Afin d'etudier le profil de prescriptionchez les gens Ages un registre sur ordinateur de plusde 3.6 millions de prescriptions remplies en Saskatchewanen 1976 a ete pass6 en revue. La population Agee (de 65ans ou plus) cette annee-la etait de 102 070, et 77.30/od'entre eux re9urent au moms un des produits d'ordon-nance inscrits au formulaire de Ia Saskatchewan. En com-paraison avec un groupe d'ige moyen (des personnes dontl'ige etait compris entre 35 et 54 ans) les personnes ig6esont presente un nombre moderement plus elev6 de pres-criptions remplies et de medicaments utilises par personnecette annee-la. Cependant, les prescriptions d'antihyper.tenseurs et de diuretiques augmentaient sensiblement avecl'Age, et les barbituriques, compte tenu de leur toxicitepotentielle, semblerent Atre surprescrits chez les gens Ages.
According to the United Nations definition1 Canadaachieved the status of an aged nation in 1945,2 whenmore than 7% of the population exceeded the age of65 years. The province of Saskatchewan reached this
. Provincial gerontologist, province of SaskatchewantResearch officer, Saskatchewan Prescription Drug Plan4Professor and head, department of pharmacology, Universityof Saskatchewan
Reprint requests to: Dr. G.E. Johnson, Professor and head,Department of pharmacology, University of Saskatchewan,Saskatoon, Sask. S7N OWO
1074 CMA JOURNAL/OCTOBER 20, 1979/VOL. 121
percentage 3 years later.3 Since that time Saskatchewanhas surpassed the Canadian average, and as of June 1,1977 it had the highest percentage of elderly peopleof any province in the country.4The rising number of elderly people in Saskatchewan
has had a particularly profound effect on the healthand social services of the province. For example, theuse of medical and hospital services has risen steadily.5As might be expected too, a disproportionately highrate of prescription drug use is seen in theThe study described in this paper was undertaken toreview patterns of drug prescribing for the elderly.Specifically it sought:* To determine the general level of drug prescribing
for the elderly, compared with the "middle-aged".* To determine which drugs are prescribed par-
ticularly for the elderly and for subgroups within thatbroad category.* To examine these drug prescription patterns in
the light of current knowledge of the pharmacologicproperties of the drugs.* To heighten professional and public awareness
and concerns about both the benefits and the potentialhazards of drug therapy for the elderly.
Methods
In September 1975 the Saskatchewan PrescriptionDrug Plan began providing benefits. It is a universalprovincial health program that in June 1976 coveredan eligible population of 909 714. For drugs listed inthe Saskatchewan Formulary and classified as benefitsthe plan pays the cost of drug materials and a portionof the dispensing fee. The formulary does not list allthe drugs available on the Canadian market butincluded 445 generic drugs in 1976. Products mustqualify for inclusion in the formulary on the basis ofdemonstrated therapeutic effectiveness. Drugs not listedin the formulary may be prescribed by physicians;however, the patients are required to assume the totalfinancial responsibility for these products. Drugs given
in hospital that are covered as benefits under otherhealth service programs are not included in the Sas-katchewan Prescription Drug Plan. In spite of thefact that the restricted formulary does not include allthe products on the Canadian market, the productslisted in the formulary represent 85% to 90% of theprescribed drugs dispensed at retail pharmacies inSaskatchewan (S. Petz, executive director, Saskat-chewan Prescription Drug Plan: personal communica-tion, 1978).
The Saskatchewan Prescription Drug Plan's pres-cription claims are processed by a computer assessmentsystem, with permanent records maintained on magnetictape. The computerized record of payment served asthe data base for this study. The full data file used inthe study, including records of all benefit drugs dis-pensed to all beneficiaries, contained 3 665 481 pres-cription records for the calendar year 1976. Statisticalhandling of the records was accomplished by a series ofCOBOL-language computer programs, most of whichwere written specifically for the study. *Two age groups were established for the purposes
of this study: the elderly, defined as persons 65 yearsof age or older, and the middle-aged, defined as per-sons 35 to 54 years old. The elderly group was brokendown into three subgroups - 65 to 74 years, 75 to84 years and 85 years and over - so that drugprescription trends with increasing age could beobserved.
The analysis was carried out in two stages. In thefirst stage all drugs listed in the Saskatchewan For-mulary were reviewed and their use by age was re-corded. Because of the volume of information providedin this stage it was impossible to pursue in detail theuse of all drugs by the various age groups. Instead itwas decided to study in detail in the second stage theuse of cardiovascular drugs, central nervous systemdrugs and diuretics. To simplify further the handling of*Further details may be obtained by writing to: Mr. S. Petz,Executive director, Saskatchewan Prescription Drug Plan, 3475Albert St., Regina, Sask. S4S 6X6.
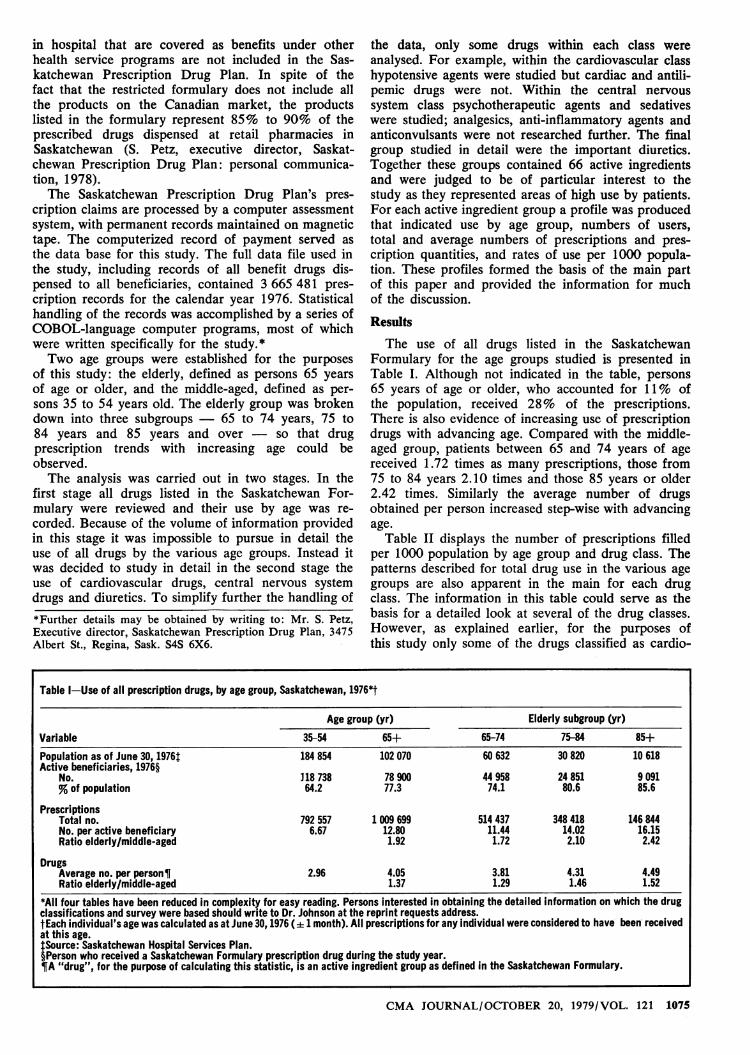
Table I-Use of all prescription drugs, by age group, Saskatchewan, 1976*t
Age group (yr) Elderly subgroup (yr)Variable 35-54 65+ 65-74 75-84 85+Population as of June 30, 1976t 184 854 102 070 60 632 30 820 10 618Active beneficiaries, 1976§
No. 318738 78900 44958 24851 9091% of population 64.2 77.3 74.1 80.6 85.6
PrescriptionsTotal no. 792 557 1 009 699 514 437 348 418 146 844No. per active beneficiary 6.67 12.80 11.44 14.02 16.15Ratio elderly/middle-aged 1.92 1.72 2.10 2.42
DrugsAverage no. per person¶ 2.96 4.05 3.81 4.31 4.49Ratio elderly/middle-aged 1.37 1.29 1.46 1.52
*AII four tables have been reduced in complexity for easy reading. Persons interested in obtaining the detailed information on which the drugclassifications and survey were based should write to Dr. Johnson at the reprint requests address.tEach individual's age was calculated as at June 30, 1976 (i: 1 month). All prescriptions for any individual were considered to have been receivedat this age.1:Source: Saskatchewan Hospital Services Plan.§Person who received a Saskatchewan Formulary prescription drug during the study year.¶A "drug", for the purpose of calculating this statistic, is an active ingredient group as defined in the Saskatchewan Formulary.
GMA JOURNAL/OCTOBER 20, 1979/VOL. 121 1075
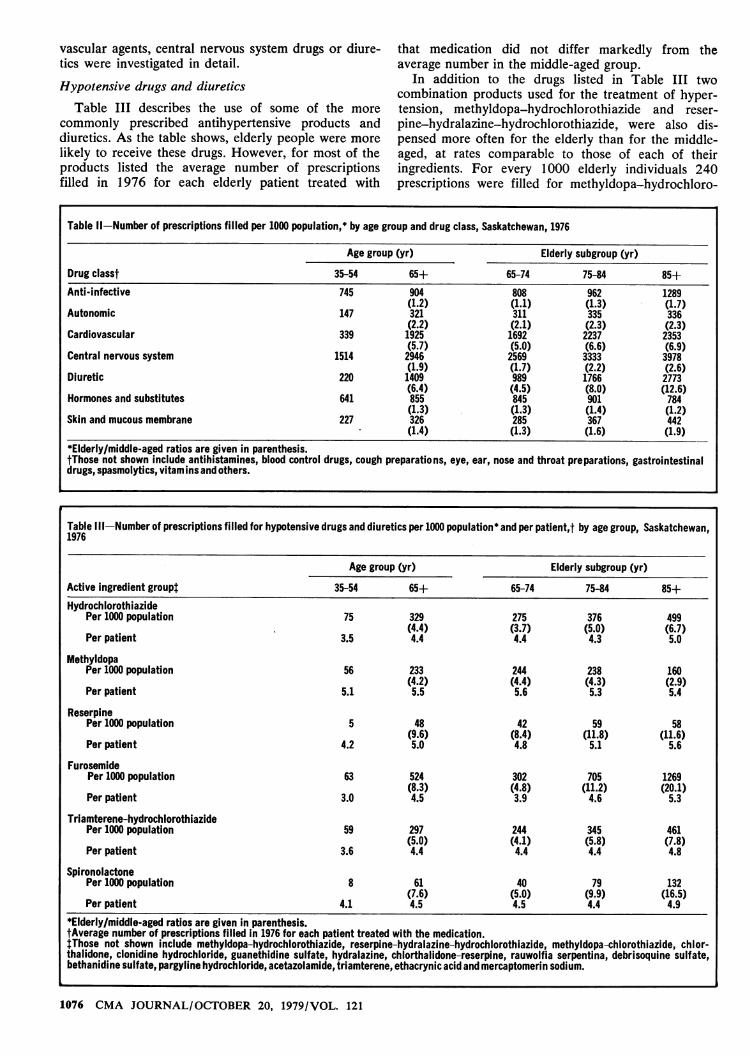
Table Il-Number of prescriptions filled per 1000 population,* by age group and drug class, Saskatchewan, 1976
Age group (yr) Elderly subgroup (yr)
Drug classt 35-54 65+ 65-74 75-84 85+Anti-infective 745 904 808 962 1289
(1.2) (1.1) (1.3) (1.7)Autonomic 147 321 311 335 336
(2.2) (2.1) (2.3) (2.3)Cardiovascular 339 1925 1692 2237 2353
(5.7) (5.0) (6.6) (6.9)Central nervous system 1514 2946 2569 3333 3978
(1.9) (1.7) (2.2) (2.6)Diuretic 220 1409 989 1766 2773
(6.4) (4.5) (8.0) (12.6)Hormones and substitutes 641 855 845 901 784
(1.3) (1.3) (1.4) (1.2)Skin and mucous membrane 227 326 285 367 442
(1.4) (1.3) (1.6) (1.9)*Elderly/middle.aged ratios are given in parenthesis.tThose not shown include antihistamines, blood control drugs, cough preparations, eye, ear, nose and throat preparations, gastrointestinaldrugs, spasmolytics, vitamins and others.
Table Ill-Number of prescriptions filled for hypotensive drugs and diuretics per 1000 population* and per patient,t by age group, Saskatchewan,1976
Age group (yr) Elderly subgroup (yr)
Active ingredient group 35-54 65+ 65-74 75-84 85+Hydrochlorothiazide
Per 1000 population 75 329 275 376 499(4.4) (3.7) (5.0) (6.7)
Per patient 3.5 4.4 4.4 4.3 5.0
MethyldopaPer 1000 population 56 233 244 238 160
(4.2) (4.4) (4.3) (2.9)Per patient 5.1 5.5 5.6 5.3 5.4
ReserpinePer 1000 population 5 48 42 59 58
(9.6) (8.4) (11.8) (11.6)Per patient 4.2 5.0 4.8 5.1 5.6
FurosemidePer 1000 population 63 524 302 705 1269
(8.3) (4.8) (11.2) (20.1)Per patient 3.0 4.5 3.9 4.6 5.3
Triamterene-hydrochlorothiazidePer 1000 population 59 297 244 345 461
(5.0) (4.1) (5.8) (7.8)Per patient 3.6 4.4 4.4 4.4 4.8
SpironolactonePer 1000 population 8 61 40 79 132
(7.6) (5.0) (9.9) (16.5)Per patient 4.1 4.5 4.5 4.4 4.9
*Elderly/middle..aged ratios are given in parenthesis.tAverage number of prescriptions filled in 1976 for each patient treated with the medication.tThose not shown include methyldopa-hydrochlorothiazide, reserpine-hydralazine-hydrochlorothiazide, methyldopa-chlorothiazide, chlor-thalidone, clonidine hydrochloride, guanethidine sulfate, hydralazine, chlorthalidone-reserpine, rauwolfia serpentina, debrisoquine sulfate,bethanidine sulfate, pargyline hydrochloride, acetazolamide, triamterene, ethacrynic acid and mercaptomerin sodium.
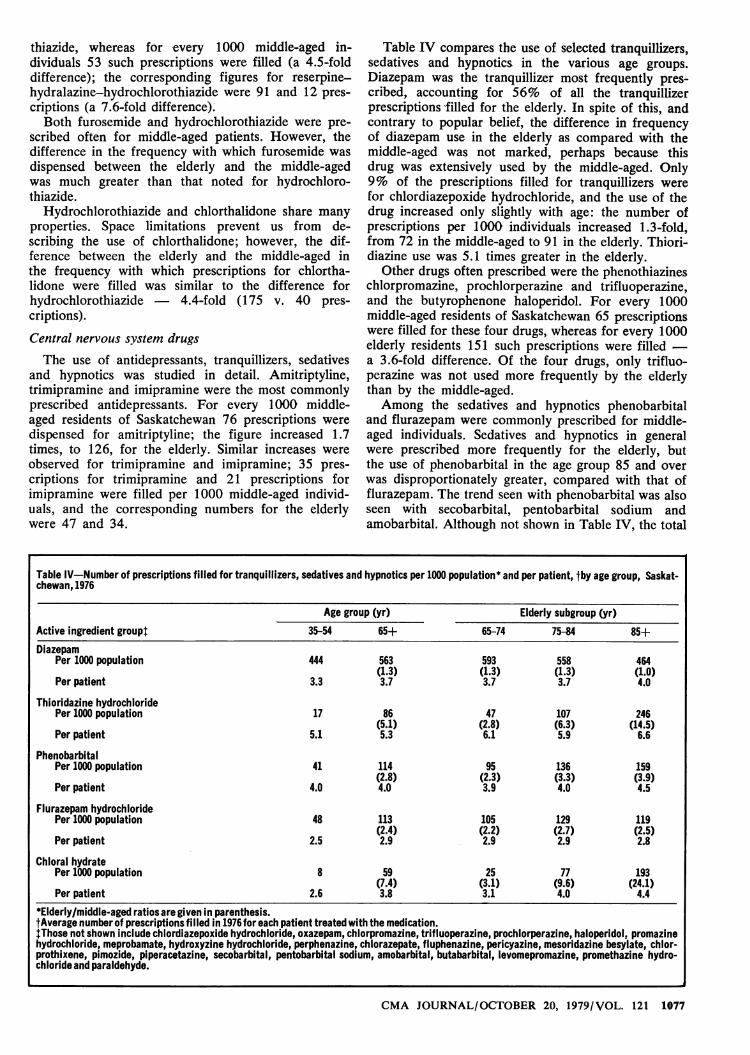
Table lV-Number of prescriptions filled for tranquillizers, sedatives and hypnotics per 1000 population* and per patient, .by age group, Saskat-chewan, 1976
Age group (yr) Elderly subgroup (yr)Active ingredient group. 35-54 65+ 65-74 75-84 85+Diazepam
Per 1000 population 444 563 593 558 464(1.3) (1.3) (1.3) (1.0)
Per patient 3.3 3.7 3.7 3.7 4.0
Thioridazine hydrochloridePer 1000 population 17 86 47 107 246
(5.1) (2.8) (6.3) (14.5)Per patient 5.1 5.3 6.1 5.9 6.6
PhenobarbitalPer 1000 population 41 114 95 136 159
(2.8) (2.3) (3.3) (3.9)Per patient 4.0 4.0 3.9 4.0 4.5
Flurazepam hydrochloridePer 1000 population 48 113 105 129 119
(2.4) (2.2) (2.7) (2.5)Per patient 2.5 2.9 2.9 2.9 2.8
Chloral hydratePer 1000 population 8 59 25 77 193
(7.4) (3.1) (9.6) (24.1)Per patient 2.6 3.8 3.1 4.0 4.4
*Elderly/middle.aged ratios are given in parenthesis.tAverage number of prescriptions filled in 1976 for each patient treated with the medication.Those not shown include chlordiazepoxide hydrochloride, oxazepam, chlorpromazine, trifluoperazine, prochlorperazine, haloperidol, promazinehydrochloride, meprobamate, hydroxyzine hydrochloride, perphenazine, chlorazepate, fluphenazine, pericyazine, mesoridazine besylate, chlor-prothixene, pimozide, piperacetazine, secobarbital, pentobarbital sodium, amobarbital, butabarbital, levomepromazine, promethazine hydro-chloride and paraldehyde.
number of prescriptions filled for these three drugs was24 per 1000 middle-aged individuals but 108 per 1000elderly individuals - a 4.5-fold difference. Thus, thereis still widespread use of barbiturates for older people,and particularly those 85 years of age or older. Chloralhydrate was not prescribed extensively for the middle-aged but was prescribed extensively for the elderly,especially those 85 years of age or older, in whom theuse of this drug exceeded that of flurazepam.
Discussion
General level of drug prescribing for the elderly
This study was the most comprehensive survey everundertaken of drug prescribing for the elderly. Previousreports have dealt with a random sample of the popula-tion,7 an institutional population of the elderly8'9 and ageneral practice survey.'0 Achong and colleagues'1reported on drug use in the elderly, but their invest-igation was in a more restricted sample of the aged.
The Saskatchewan study was unique in severalrespects. First, it was the most comprehensive surveyof its kind, representing the experience over a 12-monthperiod of 102 070 patients over the age of 65, 77.3%of whom were beneficiaries of the SaskatchewanPrescription Drug Plan. Second, it surveyed prescrip-tion drug use in the community rather than in a hos-pital. Almost all prescription drugs other than thoseadministered to hospital inpatients were included inthis study; as a result, the prescribing of most of theprescription drugs issued to the elderly was reviewed.
The review of drug use in the elderly as reportedin Tables I and II provided interesting and perhapssurprising observations. Compared with the rate forthe middle-aged, the rate of drug prescribing for theelderly was lower than one might have expected fromthe literature.'2-" For example, during 1976, 77.3%of the people 65 years of age or older received one ormore prescriptions, compared with 64.2% of thoseaged 35 to 54 years. When one considers the greaterlikelihood of illness and multiple disorders, especiallyof the cardiovascular system, with advancing age, thehigher rate of drug use in the elderly does not appearto be excessive. The greater likelihood of chroniccontinuing illness with advancing years is consistentwith the increase in the prescription rate observed. Itis our feeling that the approximately twofold greaternumber of prescriptions written for the elderly ascompared with the middle-aged is not unexpected.
There is evidence, however (from the 1975-76statistical tables of the medical services division, Sas-katchewan Department of Health), that the number ofprescriptions per person per year calculated for theelderly people in this study, 12.80, was an under-estimate, as was the average number of drugs receivedper elderly person. Older patients in nursing homes orin the community often receive prescriptions for diversedrugs, such as laxatives, vitamins, sedatives, hypnoticsand peripheral vasodilators, that are not included inthe Saskatchewan Formulary. Sedatives and hypnoticscontaining methaqualone, glutethimide, methyprylonand ethchlorvynol were not included in the formulary,nor were laxatives and vitamins, which were cheaperto buy as over-the-counter drugs than through the
1078 CMA JOURNAL/OCTOBER 20, 1979/VOL. 121
Saskatchewan Prescription Drug Plan. Unfortunatelyit was impossible to determine the number of drugsthat may have been prescribed or purchased under theseconditions.
Use of cardiovascular drugs and diureticsin the elderly
Cardiovascular agents, central nervous system drugsand diuretics represented approximately two thirds ofall the drugs prescribed for the elderly in our survey.Although the overprescribing of central nervous systemdepressants for the elderly is emphasized in the litera-ture, this study showed that the greatest increase in thefrequency of prescribing was for cardiovascular agentsand diuretics. The dramatic increase noted for thesedrugs may reflect physicians' intention of controllinghypertension and related disorders.
Approximately 56% of all the cardiovascular drugsprescribed within the Saskatchewan Prescription DrugPlan for persons 65 years of age or older were forthe treatment of hypertension. The most commonhypotensive drugs and diuretics were furosemide,hydrochlorothiazide, triamterene-hydrochlorothiazide,methyldopa-hydrochlorothiazide and methyldopa. It isunfortunate that propranolol, which has recently beenused extensively for the treatment of hypertension, waslisted only as a cardiac drug in the SaskatchewanFormulary in 1976 and not as a hypotensive drug. As aresult its use was not reviewed. It would have beenmost interesting to observe the rate at which it wasprescribed for the elderly at that time.A closer examination of the data suggests some
interesting inconsistencies. Although more of the clderlythan of the middle-aged were treated with hypotensivedrugs and diuretics the number of prescriptions foreach drug per patient in 1976 was between four andfive for both age groups. This is difficult to explain.Each prescription must be renewed every 34 days. Asthe treatment of hypertension is continuous, one wouldexpect that each patient would ideally require 11 or 12prescriptions per year. The fact that the actual figurewas considerably less may reflect poor patient com-pliance or the fact that antihypertensive therapy wasstarted and discontinued in similar numbers of patientsthat year. If rational therapy is sought, neither possibil-ity is acceptable. It is apparent that, although more ofthe elderly than of the middle-aged were receiving treat-ment for hypertension, there is no evidence, on thebasis of the amounts of drugs dispensed, that they werebeing treated more effectively than their youngercounterparts.
The treatment of hypertension in the elderly is acontroversial issue. Several studies have suggested thatsymptomless hypertension in the elderly is not anindication for therapy.'5'7 It has been argued that en-thusiastic antihypertensive regimens in persons withatheromatous and therefore less elastic blood vesselsmay result in a serious reduction in blood pressure anda critical decrease in cerebral blood flow, and mayprecipitate hemiplegia.'8 Judge and Caird'9 advised thathigh blood pressure should only be treated when itremains high after the resolution of cardiac failure orwhen it is accompanied by undoubted signs of cardiacdamage.
These views have not been shared by all workers.Chrysant, Frohlich and Papper20 have maintained that,regardless of the patient's age, a systolic blood pressureabove 160 mm Hg and a diastolic blood pressure above95 mm Hg should be treated. Alderman, Rodman andSeligman,2' quoting from the Framingham study, in-dicated that symptom-free persons with hypertensionwere four times as likely to have an atherothromboticbrain infarction as controls, regardless of age.
It is not the purpose of this discussion to review allthe pros and cons of the treatment of hypertension inthe elderly. Suffice it to say that disagreement existsas to its necessity. Antihypertensive drugs are notwithout their side effects. Postural hypotension is com-mon in the elderly, largely because of an impairedbaroreceptor response22 and a reduction in peripheralvenous tone.23 These factors complicate the use ofantihypertensive medication as well as diuretics inelderly patients since the dose must be titrated evenmore cautiously than in younger patients to avoidsevere orthostatic hypotension and syncope.13 Dolleryand Harington.' reported that older patients are moresensitive to the antihypertensive and central nervoussystem depressant effects of methyldopa. It has alsobeen suggested that the use of reserpine be discouragedbecause of the drug's ability to produce gastric ulcer-ation and psychic depression.13
Hydrochlorothiazide is a valuable agent for thetreatment of hypertension and renal impairment. It isimpossible from our data to determine whether moreof the drug was used to treat one or the other of thesedisorders. It is generally recognized that the elderlyare more susceptible to the complications of diuretictherapy. The side effects of hydrochlorothiazide therapyinclude hypokalemia with associated digitalis toxicity,impaired glucose tolerance, hyperuricemia and occa-sionally symptomatic gout. Hypovolemia with hypoten-sion, dehydration with prerenal azotemia, acid-baseimbalance, hyponatremia, and urinary incontinence andretention have been reported, particularly with furo-semide, but also occasionally with thiazide diuretics.13Caranasos, Stewart and Cluff25 reported that 6% ofadverse drug reactions were related to the use ofdiuretics, and Cheung and Kayne26 found in a surveyof three extended-care facilities that diuretics were in-volved in over 20% of the adverse drug reactions. Itis apparent, therefore, that, although diuretics such ashydrochlorothiazide and furosemide are valuable ther-apeutic tools, care should be taken to reduce the likeli-hood of side effects of their use.
Several approaches may be taken to prevent orreverse the hypokalemic effect of hydrochlorothiazide.One is to incorporate triamterene in the drug regimen.In this regard it is interesting to note that the frequencyof prescription of the hydrochlorothiazide-triamterenecombination was almost equal to that of hydrochloro-thiazide alone. Chlorthalidone mimics in most ways theeffects of the thiazides, and elderly patients are moresubject to the hypokalemic effects of this drug. Anincreased frequency of prescription of chlorthalidone inthe elderly without concomitant potassium supplemen-tation may result in more marked hypokalemia in theelderly.
Furosemide is a potent loop diuretic. Its greater use
in the elderly was striking, and it accounted for ap-proximately 47% of the prescriptions for diureticsfor those 65 years of age or older in our study. It isimpossible to determine the clinical indications for itsuse in the elderly and the reasons for selecting it overa thiazide. However, physicians prescribing furosemideshould be aware of its potent diuretic action and itsside effects, including acute hearing loss,27 beforeprescribing it.
In its review of diuretics in the elderly28 the BritishMedical Journal pointed out that, although diureticshave revolutionized the management of heart failureand most are useful in the treatment of hypertension,they should only be used when there is a good clinicalindication and adequate facilities exist for clinical andbiochemical follow-up.
Use of central nervous system drugs in the elderly
Drugs acting on the central nervous system ac-counted for almost one third of all the formulary drugsprescribed in Saskatchewan during 1976. Because oftheir different therapeutic applications, they will bediscussed in three categories: antidepressants, tran-quillizers, and sedatives and hypnotics.
Depression can usually be classified as endogenousor reactive. Depression in the elderly is often reactive,commonly to bereavement or a change in the environ-ment. Loss of interest, feelings of hopelessness andunworthiness, and magnification of relatively minorsomatic symptoms are also frequent. The tricyclic anti-depressants, such as amitryptyline, trimipramine andimipramine, have not enjoyed great success in thetreatment of reactive depression. It was therefore com-forting in our study to find that they were not usedas frequently in the elderly as one might have expected.The difference in their use in the group aged 85 yearsand over, compared with the middle-aged population,was not pronounced. Physicians should be aware,however, that older patients are often particularly sen-sitive to the central and peripheral side effects of thetricyclic antidepressants. Unless the starting dose issmaller than average the patient may become exces-sively drowsy and later show confusion and psycho-motor excitement.29 The elderly may also be subjectto urinary retention and constipation with the use ofthese drugs. Postural hypotension, cardiac arrhythmiasand glaucoma may also occur.30The benzodiazepines diazepam and chlordiazepoxide
hydrochloride were the psychoactive drugs most oftenprescribed for both the elderly and the middle-agedin our study. Prescriptions for diazepam represented56% of all orders for psychoactive drugs for personsaged 65 years or over, and 66% of those for personsaged 35 to 54 years. Although the high rate of use ofdiazepam in the middle-aged group is disconcerting,some solace can be derived from the fact that adramatic increase in the rate of use of diazepam inthe elderly was not noted. However, an increase in thefrequency of clinical depression of the central nervoussystem by diazepam and chlordiazepoxide with increas-ing age has been noted in the Boston CollaborativeDrug Surveillance Program3' and by Greenblatt,Harmatz and Shader.32
The phenothiazines thioridazine, chlorpromazine, tri-
CMA JOURNAL/OCTOBER 20, 1979/VOL. 121 1079
fluoperazine and prochiorperazine were prescribed lessfrequently for our study population than the benzodia-zepines diazepam and chlordiazepoxide hydrochloride.However, unlike the benzodiazepines, the phenothia-zines and the butyrophenone haloperidol were muchmore frequently prescribed for the elderly than for themiddle-aged. The phenothiazines and haloperidol areclassified as antipsychotic drugs. They also possesssedative and hypnotic properties, and it is likely thattheir increased use in the elderly was for daytimesedation or night-time hypnosis. However, the pheno-thiazines differ in their effects: chlorpromazine isnoted for its sedative effects, whereas trifluoperazineand prochiorperazine are not strongly sedating. Anotherfactor to be considered is the reportedly increasedsusceptibility to the extrapyramidal actions of thesedrugs in the elderly. The peak frequency of akathisiaoccurs between the ages of 40 and 50 years, and thatof akinetic parkinsonism occurs around 80 years.33Choreiform side effects from long-term phenothiazinetherapy are five times more frequent in an aged thana young population.33
Sedatives and hypnotics accounted for 15% of allthe central nervous system drugs prescribed for theage group 65 years or over, but, as was previouslymentioned, the use of these drugs was probably un-derestimated. Of the prescriptions for sedatives andhypnotics more than half (56%) were for a barbiturate.This is disconcerting, for the increased sensitivity ofthe aged to barbiturates is well known.. In a signif-icant proportion of elderly patients paradoxic responsesranging from mild restlessness to frank psychosis havebeen seen.35 As well, these agents have been shown tobe a significant cause of nocturnal falls and femoralfractures in elderly patients.36 Judge and Caird37 havestated that barbiturates should never be used in elderlypeople except those with epilepsy, and in several edi-torials in noted medical journals in both the UnitedKingdom and the United States the use of barbituratesas hypnotics has been condemned.3lA.
Benzodiazepines such as flurazepam and oxazepamhave clinical indications for use in the treatment ofinsomnia. Furthermore, they are less likely thanbarbiturates to produce prolonged depression. This isparticularly true for oxazepam, which has a half-lifeof 3 to 8 hours. Flurazepam is metabolized to an activechemical, desalkylflurazepam, which has a long half-life (47 to 100 hours). Nightly administration of flura-zepam results in accumulation of the slowly eliminatedactive metabolite. As a result, drowsiness may be seenduring long-term use, especially in elderly or debilitatedpatients. Ataxia, confusion and hallucinations are alsomore frequent in these patients.41
The preceding discussion presupposes that pheno-barbital was used as a sedative or hypnotic or both.The drug is also a popular agent for the treatment ofepilepsy. It is impossible to determine how muchthe drug was used for this indication. It is, however,clear that such agents as secobarbital, pentobarbitalsodium, amobarbital and butabarbital were used fortheir sedative and hypnotic properties. Such use shouldbe discouraged.
We thank Mr. R. Abrahamson, who wrote the computer
programs from which the data for this paper were gener-ated, the Saskatchewan Prescription Drug Plan, whose co-operation made the research possible, and Mr. S. Petz,executive director of the plan, for his help.
References
1. United Nations: The Aging of Populations and its Eco-nomic and Social Implications, UN Dept of Economicand Social Affairs, United Nations, New York, 1956, p 7
2. Population 192 1-1966. Revised Annual Estimates of Pop-ulation by Sex and Age, Canada and the Provinces, catno 91-511, census division, Dominion Bureau of Statistics,Ottawa, 1968, p 32
3. Ibid, p 354. Annual Estimates of Population by Sex and Age Group,
Canada and the Provinces, cat no 91-202, Statistics Can-ada, Ottawa, 1977, pp 32-33
5. SKOLL SL: Adding Life to Years: a Report to the Ministerof Health of the Province of Saskatchewan ConcerningServices and Facilities for the Elderly in Britain, the Scan-dinavian Countries, Belgium and Holland and its Relevanceto Saskatchewan, Province of Saskatchewan, Regina, 1976,pp 4-5
6. Saskatchewan Prescription Drug Plan, A nnual Report,1975-76, Province of Saskatchewan, Regina, 1976, p 18
7. MITENKO PA, SURES H, WILSON M: Drug use in theelderly (Manitoba - 1975) (abstr). Ann R Coll PhysiciansSurg Call 11: 36, 1978
8. HuRWITz N: Predisposing factors in adverse reactions todrugs. Br Med J l: 536, 1969
9. SEIDL LG, THORNTON GF, SMITH JW, et al: Studies onthe epidemiology of adverse drug reactions. 3. Reactionsin patients on a general medical service. Bull Johns Hop-kins Hosp 19: 299, 1966
10. LAW R, CHALMERS C: Medicines and elderly people: ageneral practice survey. Br Med J 1: 565, 1976
11. ACHONG MR, BAYNE JRD, GERSON LW, et al: Prescribingof psychoactive drugs for chronically ill patients. Can MedAssoc J 118: 1503, 1978
12. CAIRD FL: Prescribing for the elderly. Br J Hosp Med 17:610, 1977
13. VESTAL RE: Drug use in the elderly: a review of problemsand special considerations. Drugs 16: 358, 1978
14. LAMY PP, VESTAL RE: Drug prescribing for the elderly.Hosp Pract 11: 111, 1976
15. ANDERSON WF, COWAN NR: Arterial blood pressure inhealthy older people. Gerontol Clin 14: 129, 1972
16. CAiRD Fl, DALL JLC: The cardiovascular system, in Text-book of Geriatric Medicine and Gerontology, BROCKLE-HURST JC (ed), Churchill Livingstone, Edinburgh, 1973,p 122
17. FRY J: Natural history of hypertension: a case for selec-tive non-treatment. Lancet 2: 431, 1974
18. JACKSON G, MAHON W, PIERsCIANowsKI TA, et al: In-appropriate antihypertensive therapy in the elderly. Lancet2: 1317, 1976
19. JUDGE TG, CAIRD FL: Drug Treatment of the ElderlyPatient, Pitman, London, 1978, p 47
20. CHRYSANT SG, FROHLICH ED, PAPPER 5: Why hypertensionis so prevalent in the elderly - and how to treat it.Geriatrics 31: 101, 1976
21. ALDERMAN MH, RODMAN J, SELIGMAN A: Inappropriateantihypertensive therapy in the elderly (C). Lancet 1: 259,1977
22. GRIBBON B, PICKERING TG, SLEIGHT P, et al: Effect ofage and high blood pressure on baroreflex sensitivity inman. Circ Res 29: 424, 1971
23. CAIRn Fl, ANDREWS GR, KENNEDY RD: Effect of postureon blood pressure in the elderly. Br Heart J 35: 527, 1973
24. DOLLERY CT, HARINGTON M: Methyldopa in hypertension.Clinical and pharmacological studies. Lancet 1: 759, 1962
25. CARANASOS GJ, STEWART RB, CLUFF LE: Drug-inducedillness leading to hospitalization. JAMA 228: 713, 1974
1080 CMA JOURNAL/OCTOBER 20, 1979/VOL. 121
26. CHEUNG A, KAYNE R: An application of clinical pharmacyservices in extended care facilities. Calif Pharm 23: 22,1975
27. COOPERMAN KB, RUnIN IL: Toxicity of ethacrynic acidand furosemide. Am Heart J 85: 831, 1973
28. Diuretics in the elderly (E). Br Med J 1: 1092, 197829. DAvIES RK, TUCKER GJ, HARROW M, et al: Confusional
episodes and antidepressant medication. Am J Psychiatry128: 95, 1971
30. FANN WE: Pharmacotherapy in older depressed patients.I Gerontol 31: 304, 1976
31. Boston Collaborative Drug Surveillance Program: Clinicaldepression of the central nervous system due to diazepamand chlordiazepoxide in relation to cigarette smoking andage. N Engi I Med 288: 277, 1973
32. GREENBLATT DJ, HARMATZ JS, SHADER RI: Factors in-fluencing diazepam pharmacokinetics: age, sex, and liverdisease. mt I Clin Pharmacol Biopharm 16: 177, 1978
33. SALTZMAN C, SHADER RI, VAN DER KOLK A: Clinical
psychopharmacology and the elderly patient. NY State JMed 76: 71, 1976
34. BENDER AD: Pharmacologic aspects of aging: a survey ofthe effect of increasing age on drug activity in adults.J Am Geriatr Soc 12: 114, 1964
35. EXTON-SMITH AN: The use and abuse of hypnotics.Gerontol Clin 9: 264, 1967
36. MACDONALD JB, MACDONALD ET: Nocturnal femoralfracture and continuing widespread use of barbituratehypnotics. Br Med J 2: 483, 1977
37. JUDGE TG, CAIRD Fl: Drug Treatment of the Elderly Pa-tient, op cit, p 52
38. Barbiturates on the way out (F). Br Med J 3: 725, 197339. Outmoded barbiturates (F). Br Med J 4: 552, 197440. KOCH-WESER J, GREENBLATT DJ: The archaic barbiturate
hypnotics (E). N Engi J Med 291: 790, 197441. MARTILLA JK, HAMMEL RJ, ALEXANDER B, et al: Potential
untoward effects of long-term use of flurazepam in geria-tric patients. J Am Pharm Assoc 17: 692, 1977
Evolution pr&oce et tardive apr.s pontage aortocoronarien:experience de 500 cas
CONRAD PELLETTER,* MD, FRCS[C]; ROBERT COSSETTE,* MD, FRCS[CJ; LI.ON DONTIGNY,* MD, FRCS[C];ROBERT PRIMEAU,t MD, FRCP[C]; JACQUES PROULx,t MD; GI.RARD TREMBLAY,t MD, FRCP[C]
De 1971 A 1976, 500 patients ont subi un pontage aorto-coronarien. II y eut 15 deces operatoires (30/o) et Ia fr6-quence globale d'infarctus peroperatoire fut de 70/0. Dansl'angine instable Ia mortalit6 fut de 7.40/c, comparativement& 1.10/0 dans l'angine stable (P < 0.01). Le taux de per-meabilite des greffons fut de 920/c 2 semaines apres Iachirurgie et de 87.60/c apres 18 mois. L'evolution postopera.toire a ete suivie chez 990/c des operes. II y eut 15 decestardifs (30/c) et les taux de survie a 2 et a 4 ans furent de94.40/c et de 92.10/c respectivement. II n'y a pas de differencesignificative entre Ia courbe actuarielle de survie des op6reset celle de Ia population gen6rale. AprAs une .voIutionmoyenne de 27 mois 730/c des patients demeurent corn-pletement exempts d'angine et l90/c sont nettement ame-liores. Le taux de r6cidive de l'angine fut de IOc/c par ann6eet Ia fr.quence annuelle d'infarctus fut de O.70/c. Ouatorzepatients (30/c) ont dO Atre r6op6res au cours de cettep6riode d'observation. La revascularisation chirurgicale offredonc un soulagement efficace et soutenu de Ia douleurangineuse invalidante et pourrait am6liorer Ia survie siIa mortalit6 operatoire est minime.
Des services de *chirurgje cardiovasculaire et thoraciqueet de tcardiologie de 1'h6pital du Sacr6-Coeur de Montrdal,et des d6partements de chirurgie et de mddecine, facu1t.de m.decine, universit. de Montr.a1
Les demandes de tires & part doivent .tre adress&s auDr Conrad Pelletier, Service de chirurgie cardiovasculaireet thoracique, H6pital du Sacrd-Coeur de Montr.a1,5400 ouest, boul. Gouin, Montr6al, PQ H4J iCS
Between 1971 and 1976, 500 patients underwent aortocoro-nary bypass surgery. There were 15 operative deaths (30/o)and the total frequency of perioperative infarction was 70/0.The operative mortality was 7.40/0 in unstable angina, ascompared with 1.10/0 in stable angina (P < 0.01). The propor-tion of grafts patent at 2 weeks was 920/0 and at 18 months87.60/0. Postoperative follow-up was complete for 990/0 ofthe patients. There were 15 late deaths (30/o) and the ratesof survival at 2 and 4 years were 94.40/o and 92.10/0respectively. The actuarial curve of survival after surgerywas not significantly different from that of the generalpopulation. After a mean follow-up of 27 months 730/o ofthe patients were completely free of angina and 190/o weremarkedly improved. The rate of recurrence of angina aver-aged lO0/o per year and the annual infarction rate wasO.70/o Fourteen patients (30/o) underwent reoperation duringthe follow.up period. Thus, coronary revascularization sur-gery offers effective and sustained relief of incapacitatingangina and might also improve survival if the operativemortality is low.
Depuis 10 ans le pontage aortocoronarien s'est assureune place pr.pond.rante dans le traitement de lamaladie cardiaque isch.mique. Son efficacit6 . sou-lager la douleur angineuse .t court terme est bien .tablieet explique la grande faveur dont elle jouit actuelle-ment.1 Toutefois, malgr. son application extensive onn'a Pu encore d.montrer que le traitement chirurgicalest susceptible de prolonger la vie et de diminuer la
CMA JOURNAL/OCTOBER 20, 1979/VOL. 121 1081