Embed Size (px)
Citation preview

I & O Charting Current Practices and Recommendations for Change
Purpose• Analyze the actual practice of I&O charting on three
patient care units• Compare the perceptions of providers, and nurses
regarding I&O practices• Describe ancillary staff perceptions regarding I&O
practices
Methods Written Questionnaire • Questionnaires sent to all providers and staff on
sample units • Instrument adapted from Chung, et al (2002) using a
Likert 1 to 4 scale • PCTs have added open ended questions
Retrospective Chart Review • 63 medical records based on 20% of average number
of patient discharges stratified/unit average • Chart selection using random table • Chart Review Instrument and protocol adapted from
Chung, et al (2002)
Statistics • Descriptive • t-test for independent groups to compare providers
and nurses
Research protocol, instruments, consent, and human subjects participation approved by University of Rochester Medical Center RSRB and Highland Hospital Administration.
Limitations • Sample: convenience and size • Chart review: interrater reliability • Too many DRGs to adequately correlate with practices
Questionnaire: PCT/PSAPCT / PSA Perceptions of Fluid Balance Charting• I&O is always recorded accurately.
• I&O totals are always accurately
calculated.
• The method of recording I&Os is easy.
• I&Os are accurately recorded after
each meal.
• Monitoring I&O is important for
planning patient treatment.
• Weights are recorded as often
as ordered.
• The method of recording weights
is easy.
Why are I&Os done?
Why might patient weights be
ordered daily?
Questionnaire: Provider/NurseMedical Providers Perceptions of Fluid Balance Charting• I&O is always ordered appropriate to a patient’s condition.
• The I&O is always discontinued when it is not required.
• I&O is often done as a routine.
• I&O is used to estimate the fluid balance of the patient
• I&O is used to decide the treatment of the patient
• The data entry is always accurate for charting I&O.
• I&Os are accurately recorded after each meal.
• The calculation is always accurate for I&O totals.
• The method of recording I&Os is easy.
• It is appropriate for the 24 hour I&O total to be done
at 10 p.m.
• Weighing a patient is always ordered appropriate to
the patient’s condition.
• Weighing a patient is an accurate measure of fluid
balance.
• Weights are recorded as often as ordered.
• The method of recording weights is easy.
AbstractStaff members of the Highland Hospital Nursing Practice Committee brought forth clinical
questions regarding the purpose, importance, and accuracy of Intake and Output (I&O)
documentation, and whether the measurement of I&O is valued by medical providers and
nursing personnel for clinical decision-making in patient care. At this facility it is typical practice
to measure I&O on all patients who have IV fluids and/or drainage catheters. An extensive
literature review revealed case reports of I&O practices, but minimal reported research.
Therefore a research study was implemented at the facility that adapted a study done in Hong
Kong by Chung, Chong, and French (2002). The specific aims of the study were to review actual
I&O documentation practices in the medical record and to evaluate provider, nurse and
technician perceptions of the value of I&O accuracy. The study involved a retrospective chart
review conducted on 63 medical records to analyze I&O charting practices on a medical, a surgi-
cal and a geriatric unit. Perceptions regarding I&O practices were obtained through a survey
distributed to nurses, patient care technicians, and medical providers on the three units. Descrip-
tive statistics were reported and a T-test for independent groups compared responses between
medical providers and nurses. The chart review revealed that I&O forms were present 100% of
the time in the medical record, but measurement was accurate in only 30% of the medical
records. Infusion of IV fluids was the most frequent reason for I&O measurement (45% of the
time). Medical providers and nurses agreed that I&O is used to estimate fluid balance, but 37%
of charts had no reference to I&O measurements in progress notes and generally orders were not
written for initiating or discontinuing I&O. Accuracy in measuring and documenting I&O was
better on the surgical unit compared to the other two medical units. Surveys reveal that patient
care technicians have a good understanding of the importance of I&O measurement, and that
they believe the recording of I&O is more accurate than do nurses and medical providers. Study
findings currently are being shared with various clinical practice councils for recommendations.
Some recommendations for practice change include ordering and measuring I&O only when the
information gathered will be used to make specific treatment decisions; specific orders for I&O
would be written by medical providers or nurses; I&O orders would include a reason for the
measurement; and if I&O is ordered there would be an expectation that documentation of
I&O-based treatment decisions are recorded in the patient’s progress notes. Future plans include
a follow-up chart review to assess whether these recommendations have improved accuracy of
I&O charting. Further research is suggested to compare daily weights to I&O as an accurate
measure of fluid balance.
Primary Investigator Mary Ann Emerson, MS, RN, AOCN
Co-investigators Charlene Smith, Doctoral Candidate, WHNP, BC Barbara Schrage, MS, FNP-C Barbara Trill, RN Tracie Ewing, BSN, CNM, MSEd Daniel Mendelson, MS, MD
Summary & Conclusions• Perceived that I&O measurement is not accurate• Belief that monitoring is important for treatment• Some differences in perceptions between providers/nurses• PCTs understand purpose of I&O• PCTs generally have higher scores than providers/nurses• Differences between surgery and medicine• Weights may be preferred over I&O but equipment access and manpower to do is an issue
Recommendations for I&O Practice Change• I&O will be measured only when ordered• I&O measurement will be discontinued after 48 hours unless renewed• Progress notes will reflect that I&O data is used to make treatment decisions• IVF intake will always be measured and output from tubes will always be measured, full I&O will not be measured routinely• Weights consistently done on admission and as ordered to monitor fluid blance• Education regarding change in practice• Further research
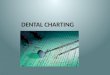
Significant Mean Differences Between Groups: t test (p<.o5)
0
0.5
1
1.5
2
2.5
3
3.5
4
I&O Ordered appropriateto patient condition
I&O often done as routine I&O used to estimatepatient fluid balance
I&O used to decide patienttreatment
Method for recording I&Ois easy
Appropriate that 24 hourI&O is done at 2200 hours
Val
ues
MD/PA Mean Value
RN/LPN Mean Value