Embed Size (px)
Citation preview
IN SITU SIMULATION IN THE ED: POWERFUL TOOL FOR QUALITY IMPROVEMENT Julie Mardon
Consultant Emergency Medicine
University Hospital Crosshouse

IN SITU SIMULATION
High fidelity mannequins In the ED Video debrief Real multidisciplinary teams Identify human factors in team working Also latent risks Process evolution
2 PROJECTS
Paediatric asthmatic patients discharged from department
Sepsis 6 bundle delivery

NEAR MISS
8 year old asthmatic Seen in the paeds ED Sent home x2 Both times treated with a nebuliser No observation charts filled out Re-attended on the third occasion unwell and
required a long hospital stay Made a full recovery

CAUSE ANALYSIS
Insufficient understanding of the difference between use of nebulisation and multi-dosing in patients DC home
Non technical skills of nurses vital to ensure safe clinical practice
Poor understanding of indications and techniques required to multi-dose children with wheeze
Lack of PAWS charts, PEFR and discharge information for paediatric asthmatics

SIMULATION SCENARIO DESIGNED
Technical and non technical learning objectives mirrored cause analysis of near miss
Importance of clear communication between nurses and doctors especially around clinical decision making
Technical skills allowing safe patient care were key learning objectives

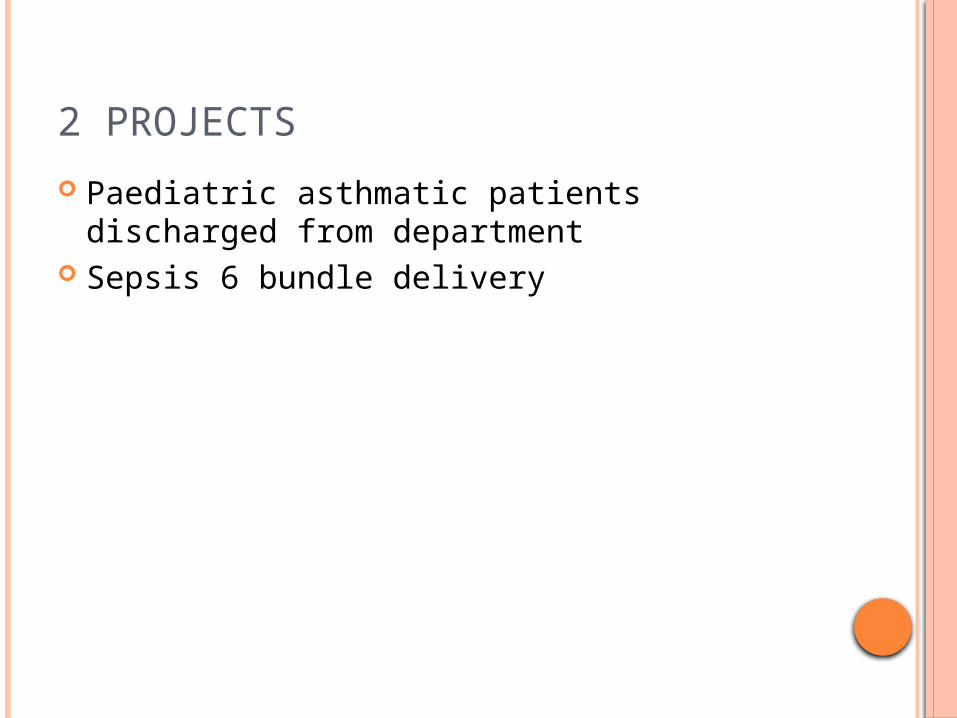
SIMULATION
Wireless sim boy Run in paeds area of the ED Real clinical scenario 65% of nursing staff of all levels ED and ED
Paeds trained across region over 8 teaching days
Medical staff also trained all levels Nursing and medical students and
paramedics also exposed to teaching module Video recording to assist debrief

MULTI DOSING
PAWS CHART

NON TECHNICAL LEARNING
Communication skills Handover Real environmental latent errors uncovered Simulation learning objective mirrored
learners own objectives Examples of non technical skills

HANDOVER TO MEDICAL STAFF
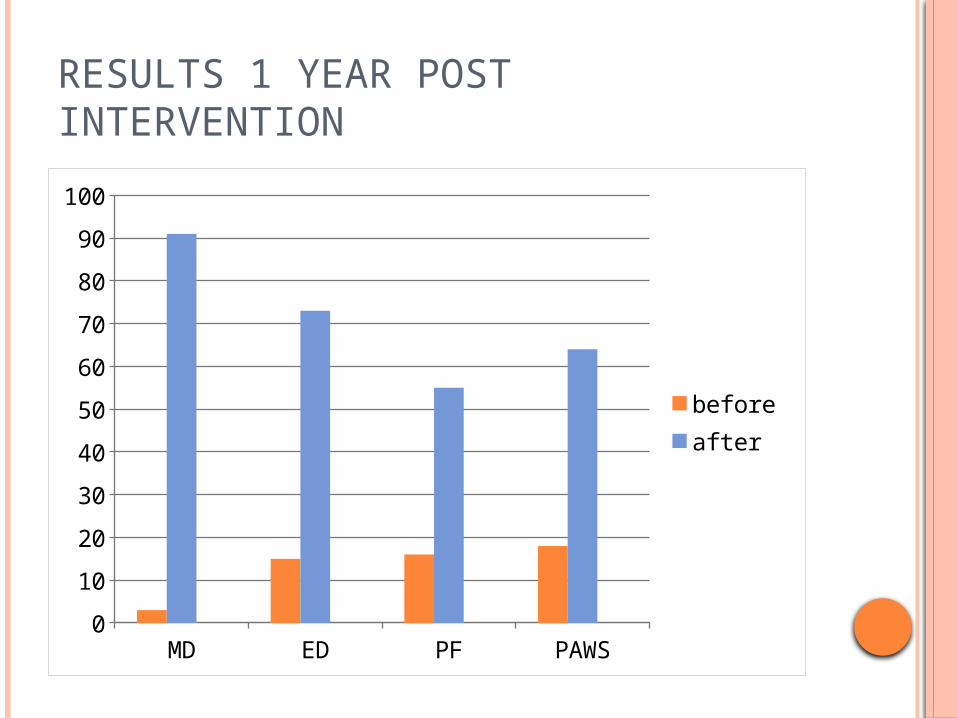
RESULTS 1 YEAR POST INTERVENTION
MD ED PF PAWS0
10
20
30
40
50
60
70
80
90
100
before after

SEPSIS
Delivery of “sepsis 6” within the ED Part of ongoing priority to deliver the bundle
within the ED Based on robust evidence nationally agreed SPSP priority target Challenging within the ED due to conflicting
priorities, overcrowding, complex process requiring multiple steps and clear communication resulting in true sense of urgency around sepsis management

PROCESS MAPPING

SIMULATION SCENARIO
Process Mapping identified the challenging parts of the process
Prioritisation of patient and communication of sense of urgency with team
Scenario designed to reflect these non technical skills as core learning objectives

IN SITU SIMULATION
9 in situ simulation sessions delivered over 1 month period
Real teams in the workplace nurses medical staff undergraduate medical and nursing students radiographers cardiac technicians clinical decision unit staff all participating.
Video debrief allowed analysis of human factors such as team communication situational awareness, decision making, prioritisation, latent challenges to the process
Use of the “simulated box”

THE BOX

TEAM PRIORITISATION




SEPSIS 6 DELIVERY BEFORE IN-SITU SIMULATION
june july august sept0
10
20
30
40
50
60
70
80
90
100

SEPSIS 6 AFTER IN SITU SIMULATION
june july aug sept oct nov dce jan feb0
10
20
30
40
50
60
70
80
90
SUMMARY AND FUTURE
In situ simulation training in human factors in the ED can show improvement in safe patient care in 2 patient groups
Role out to other areas eg Dialysis unit and Frail elderly team
Link with organisational risk management and patient safety governance systems
Repeat sepsis work in Forth Valley ED to show spread in other areas