-
I Med Genet 1991; 28: 101-109
Tay-Sachs disease heterozygote detection:use of a centrifugal
analyser for automationof hexosaminidase assays with two
differentartificial substrates
Eleanor C Landels, Ian H Ellis, Martin Bobrow, Anthony H
Fensom
AbstractAn assay for measuring hexosaminidase A in serumand
leucocytes is described in which a centrifugalanalyser is used for
automation of the enzymeassays after manual heat inactivation. The
assaywas used in a screening programme to identifyheterozygotes for
Tay-Sachs disease in AshkenaziJewish subjects in the UK. The first
results fromthis programme indicate a carrier frequency of 1 in27.
Automation of an assay for direct measurementof hexosaminidase A in
serum using 4-methyl-umbelliferyl-,-N-acetylglucosamine-6-sulphate
assubstrate is also described. Comparison of dataobtained from 66
control and 30 obligate carriersera tested by this method and by
heat inactivationshowed improved discrimination using the
sulphatedsubstrate. Results obtained using the sulphatedsubstrate
for screening serum during pregnancy arealso presented.
Tay-Sachs disease (TSD) is an incurable, neuro-degenerative
disorder of autosomal recessiveinheritance, characterised in the
classic form byprogressive mental and motor weakness resulting
indeafness, blindness, generalised paralysis, and death,usually by
4 years of age. 1 The cause is a mutation atthe locus encoding the
a peptide of hexosaminidase A(Hex A), the most biologically
important isoenzymeof the lysosomal hexosaminidases. Affected
homo-zygotes are deficient in Hex A so that the enzyme's
Paediatric Research Unit, Division of Medical andMolecular
Genetics, United Medical and Dental Schoolsof Guy's and St Thomas's
Hospitals, 8th Floor, Guy'sHospital Tower, London SEI 9RT.E C
Landels, I H Ellis, M Bobrow, A H FensomCorrespondence to Dr
Fensom.
substrate, ganglioside GM2, is not degraded andaccumulates in
neuronal cells leading to the character-istic pathology of the
disease.Hex A is composed of a and I6 peptides. The other
major isoenzymes, Hex B, Hex S, and the
intermediatehexosaminidases, are composed of various combina-tions
of a and Pi peptides. Mutation of the locuscoding the , peptide
causes reduction in the activityof all hexosaminidases except Hex S
(which iscomposed ofa peptides only). The resulting
condition,Sandhoff's disease (SHD), is biochemically
distin-guishable from TSD but clinically similar.
Carriers of the TSD gene have reduced Hex Aactivity,2 and are
approximately 10 times morefrequent in the Ashkenazi Jewish
community than inthe general population. This led to the
introduction ofscreening programmes in the early 1970s to
identifycarriers. The method used for carrier testing in
mostlaboratories involves determining the total Hexactivity in
serum, and the proportion of Hex activitywhich is heat labile under
standardised conditions(predominantly Hex A) using the sensitive
fluoro-genic substrate
4-methylumbelliferyl-i-D-N-acetyl-glucosamine. The procedure can be
automatedusing continuous flow equipment with two
matchedfluorimeters reading the product of the reaction ofunheated
and heated serum samples.4 A number offactors (pregnancy,
inflammatory illnesses, oralcontraceptive pill), which alter the
proportion of HexA relative to the other Hex isoenzymes in serum,
canlead to false positive carrier identification.5 6 In
thesecircumstances, assay of Hex A in leucocytes usuallyallows
accurate classification of genotype.
Less empirical methods for assay of Hex A arebased on use of
6-sulphated chromogenic7 or fluoro-genic8 9 substrates. Hex A is
considerably more activetowards these substrates than is Hex B, and
recentwork indicates that use of the substrates has advantagein
classification of Tay-Sachs disease genotypes,including carrier
detection.7 9The recognition of a splice junction defectl' and
a
four base insertion" in the Ashkenazi population,which together
account for about 90% of the TSD
Received for publication 19 April 1990.Revised version accepted
for publication 31 July 1990.
101
on June 22, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.2.101 on 1 F
ebruary 1991. Dow
nloaded from
http://jmg.bmj.com/
-
Landels, Ellis, Bobrow, Fensom
mutations, provides an alternative method forconfirming carrier
status.
Data reported by the National Tay-Sachs andAllied Diseases
Association in San Diego showed thatby 1987 639 880 Ashkenazi
subjects had beenscreened worldwide, and a carrier frequency of 1
in25-6 was deduced. The great majority (over 99%) ofpeople screened
were from the United States, Canada,Israel, and South Africa.
Efforts to introduce screening in the UnitedKingdom were made in
1972 but met with onlylimited success for reasons discussed by
Evans.'2Recendy, however, there has been renewed interest incarrier
screening within the Ashkenazi population ofthe UK. In preparation
for offering screening on alarge scale we have assessed the use of
the Cobas Biocentrifugal analyser (Roche Products Ltd), for
auto-mation of serum and leucocyte Hex A determinations,as an
alternative to use of a continuous flow system.The centrifugal
analyser accurately pipettes sample
and fluorescent substrate (and, after incubation, stopbuffer),
loading them into a rotor where they aremixed by centrifugal force.
The incubation period ofall samples begins and ends at the same
time, afterwhich the fluorescence is measured and converted tonmol
4-methylumbelliferone/ml by the microprocessorwithin the
centrifugal analyser. Samples must be splitand some aliquots heat
inactivated in order todifferentiate Hex A from the other
isoenzymes beforeloading on to the centrifugal analyser. This is
incontrast to the continuous flow system where serumsamples are
split after loading and heat inactivated ina heating coil within
the machine.
Parameter settings for assays performed with the Cobas Bio
9
10111213141516171819
UnitsCalculation factorStandard I concentrationStandard 2
concentrationStandard 3 concentrationStandard 4
concentrationStandard 5 concentrationStandard 6
concentrationLimitTemperature (OC)Type of analysisWavelength
Excitation (nm)
Emission (filter no)Sample volume (,il)Diluent volume
(pl)Reagent volumeIncubation time (sec)Start reagent volume
(l)jtTime of first reading (sec)Time interval (sec)Number of
readingsBlanking modePrintout mode Dens model
Printout mode
We have compared results for obligate carriers ofthe TSD gene
with those of a control group of non-Jewish subjects in order to
establish carrier andnormal percentage Hex A ranges for sera
andleucocyte samples. We describe the operation andevaluation of
this system and report our data on thefirst 2%5 Ashkenazi subjects
to be screened. We alsoreport data on the use in carrier screening
of thesubstrate
4-methylumbellifery1-,3-N-acetylglucosamine-6-sulphate and discuss
the possibility of using serumas the sample for screening during
pregancy in thelight of results obtained with this substrate.
Materials and methodsPREPARATION OF SAMPLESSerum (separated
within 18 hours of being taken andstored at -30°C) was diluted
(1/10) in citrate-phosphate buffer (12 mmol/l citric acid, 20
mmol/lNa2HPO4, pH 4 4). Leucocyte pellets were preparedfrom
heparinised blood (5 ml per pellet) within 18hours (blood stored at
4°C) of being taken, by thedextran sedimentation method,'3 and
stored at-30°C. Each pellet was resuspended in 0-8 to 1-0
mldeionised water and disrupted by sonication (3x 10second bursts,
MSE 150W instrument with micro-probe, amplitude 3, separated by 10
seconds coolingin an ice bath). The sonicate was centrifuged (200
gfor 10 minutes at 4°C) and the supernatant proteinconcentration
assayed by the method of Lowry et al'4using the centrifugal
analyser (with parameters set asin the table, column B). The
sonicate supernatant wasadjusted with deionised water to 1-0 to 1-5
mg
centrifugal analyser.
A Hexosaminidase
smol/l100
5
102030500
37-07-6
3602
502080
360*750 53041
1
B Protein
pg/nil
100010204060801000
25-07-6
750
5020150360*1505
6030I
1
*In the 'substrate start' mode of analysis, a full rotor of
specimens is incubated for an additional four minutes after the set
incubation time whileglycine buffer (for hexosaminidase) or Folin
reagent (for protein) is added to the sample cavities of the
cuvette rotor.fStrictly, stop reagent for hexosamiidase.
102
on June 22, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.2.101 on 1 F
ebruary 1991. Dow
nloaded from
http://jmg.bmj.com/
-
Tay-Sachs camier screening
protein/ml and diluted (1/10) in 0-75% human serumalbumin in
citrate-phosphate buffer, as above.
MANUAL HEXOSAMINIDASE ASSAYThe method was based on the heat
inactivationprocedure of Kaback,'5 the main difference beingthat
inactivation was carried out for three hours at50°C instead of two
and three hours at 52°C, and theenzyme reaction was run for 60
minutes instead of 30minutes. The reaction was stopped with 0-5
mol/lglycine-NaOH buffer, pH 10-3 (3 ml) and fluoresenceread using
a Perkin Elmer LS2B fluorimeter (366 rmfilter, emission wavelength
448 nm).
AUTOMATED HEXOSAMINIDASE ASSAY FOR SERA ANDLEUCOCYTESIn
developing the automated assay for Hex A weattempted to reproduce
as far as possible the con-ditions of our manual assay. The diluted
sera orleucocyte sonicates were aliquoted into four analysersample
cups; two aliquots were heated at 50°C forthree hours to inactivate
Hex A while the otheraliquots remained at 0°C in an ice bath.
All four aliquots were then assayed using thecentrifugal
analyser with the parameters set as shownin the table, column A
(substrate start mode; non-linear chemistry). The concentration of
the substrate-buffer reagent was 3 75 mmol/l
4-methylumbelliferyl-P-D-N-acetylglucosamine (Sigma, St Louis) in
25mmol/l Na2HPO4-15 mmol/l citric acid, pH 4-4. Thestopping reagent
was 0 5 mol/l glycine-NaOH, pH10-3. Standard solutions of
4-methylumbelliferone(Koch-Light, Colnbrook) in water at the
indicatedconcentrations (table) were used for daily calibrationof
the instrument. Time of incubation at 37°C wasusually 10 minutes
for both serum and leucocytes, butwas increased to 20 minutes for
low activity specimens.The Hex activity of the heat inactivated
aliquots wascompared with those kept on ice and the differenceused
to calculate the percentage Hex A for eachsample. Known normal and
heterozygote sampleswere assayed daily for quality control.
AUTOMATED HEXOSAMINIDASE ASSAY USING THE6-SULPHATED SUBSTRATE
FOR SERASerum hexosamimdase activity towards the
substrate4-methylumbelliferyl-,B-D-N-acetylglucosamine-6sul-phate
(4MUGS) (HSC Research Development Cor-poration, Toronto) was
assayed using the centri-fugal analyser with the parameter settings
shown inthe table, column A, except that standard
4-methyl-umbelliferone concentrations were 0-1, 0-5, 1-0, 5-0,10-0,
and 20-0 pmol/l. The concentration of thesubstrate-buffer reagent
was 3 75 mmol/l 4MUGS in
25 mmol/l Na2HPO4-15 mmol/l citric acid, pH 4-4,and the
incubation time was 20 minutes. Serum wasdiluted 1 in 10 with 12
mmol/l citrate-20 mmol/lphosphate buffer for these tests which
enabled assayswith sulphated and unsulphated substrates to becarred
out with the same diluted samples.
ResultsPRELIMINARY ASSESSMENT OF THE CENTRIFUGALANALYSER FOR HEX
DETERMINATIONIn developing the automated assay for hexosaminidaseA
the main change necessary was reduction of volumeof stopping buffer
from 3 ml in the manual assay to75 W1. This was dictated by the
pipetting procedureand rotor cuvette size of the centrifugal
analyser. Inorder to assess the effectiveness of the smaller
volumeof buffer for stopping the enzyme reaction, theanalyser was
set to read the fluorescence of theproduct of the reaction of
heated and unheatednormal and heterozygous sera over a 10 minute
periodat 30 second intervals after addition of the glycine.Results
showed that fluorescence slowly increasedover this time by about 1%
of the initial reading. Itwas concluded that during the 90 second
readingperiod of the standard assay the increase would not
besufficient to introduce a significant error into theresults.The
calibration of the analyser with different
concentrations of 4-methylumbelliferone was found tobe linear
over the range studied (0-204 to 10-2 imol/lfinal
concentration).
200
E~~~~~~~
0~~~~~~~~
E
~100o0
0
0E
0
Time (min)Figure I Effect ofincubatin time on totalHex
activtymeasured in two normal sera using the centrifugal
analyser.
103
on June 22, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.2.101 on 1 F
ebruary 1991. Dow
nloaded from
http://jmg.bmj.com/
-
Landels, Ellis, Bobrow, Fensom
The rate of reaction was found to be constant for 500both normal
serum (fig 1) and normal leucocyteextracts (fig 2) over the time
studied (two to 20minutes). Activity in normal leucocyte extracts
wasproportional to the protein concentration over therange 0-2 to
3-0 mg/ml, equivalent to 1 to 15 pg in the /0/incubation mixture
(fig 3). 400
DIRECT COMPARISON OF MANUAL AND AUTOMATED ASSAYSDilutions of 147
sera and 106 leucocyte specimensfrom subjects with a wide range of
percentage Hex A c(5 to 80%) were assayed simultaneously by the
manual 300/and automated methods, and the results for
thepercentages of Hex A recorded were analysed as E/described by
Bland and Altman.16 The comparison 'showed that the automated
method gave slightly >higher values than the manual method for
both types 200-of specimen, the mean difference between paired
-
Tay-Sachs carrier screening
1200
1100
1000
_ uuv
f 800-0E- 700:v)
n- 600
.EX 5000x
Ir 400
300 -
200
100 -
0
o Controls* Obligate TSD heterozygotes* Obligate Sandhoff's
disease
heterozygotese TSD patients
0oo0o
* CP
0 06 0
01 6v'*
000 0
* 0085002
* 02
*3 .
Infantile0 0 Juvenile
0 10 20 30 40 50 60 70 80 90% Hexosaminidase A
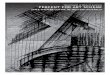
Figure 4 Two dimensional plot ofHexA (measured by the
heatinactivation method) versus percentage Hex A in
serumfromcontrols, obligate TSD heterozygotes, obligate Sandhoffs
diseaseheterozygotes, and TSD patients.
carriers is shown in fig 5. From these data a cut offpoint of
59/o between carriers and non-carriers wastaken, although the value
for one control was 55%.The results of screening 268 Jewish
subjects (mainlypregnant women or those with inconclusive or
carrierserum results) and 28 subjects with a family history ofTSD
yielded the distribution shown in fig 6. Theoverall carrier
frequency found, based on screening2965 subjects using serum,
leucocytes, or bothspecimens, was 1 in 27.
El Ob igate carr,-rs ofTa y Sachs cidisease
8 - [NuE -Jev.^ish contro roicp
z6
LL~ L~ Ul
HEX A IN SERA (SULPHATED SUBSTRATE)A clear discrimination
between obligate TSD carriersand the non-Jewish control group was
obtained whenHex A activity (measured with the sulphated
sub-strate) was plotted against Hex A (measured with thesulphated
substrate) as a fraction of the total Hexactivity (measured with
the unsulphated substrateusing the centrifugal analyser) (fig 7).
There was noclear discrimination if Hex A activity alone
wasconsidered. The same two control subjects who gaveinconclusive
results when tested by heat inactivationappeared near to the
carrier group using the sulphatedsubstrate (they are numbered as in
fig 4). SHDcarriers were not readily identified using the
sulphatedsubstrate. It should be noted that the rate ofhydrolysis
of the sulphated substrate by Hex A islower than the rate with the
unsulphated substrate,and that units on the abscissae of figs 4 and
7 aretherefore not directly comparable.
HEX A IN SERA TAKEN DURING PREGNANCYHex A activity is plotted
against gestational age in fig8 (Hex A measured by heat
inactivation) and fig 9(Hex A measured with the sulphated
substrate). Allsubjects shown had been assigned carrier status
usingthe leucocyte assay. The sulphated substrate gaveclear
discrimination between carriers and non-carriers,whereas there was
overlap of the two groups whenHex A was measured by heat
inactivation.
DiscussionThe results presented here show that the
heatinactivation method for determining Hex A in bothsera and
leucocytes is readily adaptable to a centri-fugal analyser.
Although not a completely automatedprocedure (the heat inactivation
step is manual), themethod has the advantage over a continuous
flowsystem in not requiring dual fluorescence readingsand careful
balancing of instruments. Moreover, theability to use the analyser
to test leucocytes as well as
Figure 5 The percentage HexA recorded in leucocyte extractsfrom
controls and obligate TSD carriers.
o .,I_ :. * i I I42 44 46 48 50 52 54 56 58 60 62 64 66 68 70 72
74 76 78 80 82
0 Hexosamrnidase A
105
ann
on June 22, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.2.101 on 1 F
ebruary 1991. Dow
nloaded from
http://jmg.bmj.com/
-
Landels, Ellis, Bobrow, Fensom
36-
o_ 221'
± 201,LL18
10
8
6
2-
0
El Sutb'cts !Ith f rni:y StQI vElCJ No farniUy histOry
-x,Hre n'diiase A
Figure 6 The percentage HexA recorded in leucocyte extracts from
screened subjects.
o Controls* Obligate TSD heterozygotes* Obligate Sandhoff's
disease
heterozygotes* TSD patients
0 0
0 00
0%00 00 00~00000 0o 00
0 0o 0& 001 (D 000 0
* * 0
0200 0
00000 00 U00.0o
S00* so
1200-
1100
1000
900E
800
E 700
< 600x
I 500
400
300
200
100
0
.a
Infantile/ ,Juvenile0 0
I I I
0-01 0 03 0 05 0 07 0 09 0-11 0-13 0-15Hex A (Hex A as a
fraction of total Hex activity)
Total Hex
Figure 7 Two dimensional plot ofHexA (measured with thesulphated
substrate) versus HexA as afraction oftotal Hexactivity in
serumfrom controls, obligate TSD heterozygotes,obligate Sandhoffs
disease heterozygotes, and TSD patients.
0
0
0
8 0000
008
°0
0 0
0 a'0~~~~o 0^
0
0
0 aU
A
o Pregnant controls* Heterozygotes carrying a TSD fetusA
Heterozygous fetus* Normal fetus* Fetus of unknown genotype
0 4 8 12 16 20 24Gestation (weeks)
Figure 8 Effect ofgestation on serum HexA activity measuredby
the heat inactivation method in pregnant controls andheterozygotes
carrying a TSDfetus, a heterozygousfetus, anormalfetus, or afetus
ofunknown genotype.
76
150140
130_ 120E 110-Co 100C 90-S< 80az
70
' 60C 50
30
20
10n
106
on June 22, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.2.101 on 1 F
ebruary 1991. Dow
nloaded from
http://jmg.bmj.com/
-
Tay-Sachs carier screening
170
160-
150-
140
130
120
110
-a
0
c 90
x 80
70
60
50
40
30
20
10
0
0
0
0 0 80A o
00
0
0 0
o
0 0
0000
0
0
a
0
0
0
A
a
A
o Pregnant controls* Heterozygotes carrying a TSD fetiA
Heterozygous fetus* Normal fetus* Fetus of unknown genotype
0 4 8 12 16Gestation (weeks)
Figure 9 Effect ofgestation on serum HexA actitwith the
sulphated substrate in pregnant controls anaheterozygotes cartying
a TSD fetus, a heterozygous)normalfetus, or afetus ofunknown
genotype. Thejcrepresent subsequent pregnancies in the same
mother.
serum with the same assay conditions is aadvantage. Plasma
cannot be used forbecause the precipitation which occurs wiis
diluted with the citrate-phosphate buffinaccurate pick up of sample
by the sampliHowever, plasma is not usually used forscreening
because Hex activity is lower inthan in serum, so this is not a
serious disWe observed that some serum samplesbeen stored frozen
for many months gaveresults; we attributed this to the greateiwhich
these samples had to form sonprecipitate on thawing for assay,
againinaccuracies in sample pick up. This meacould not use aged
specimens from co]obligate heterozygotes for establishing ouranges,
and all specimens had to be freshlyIt was not a serious
disadvantage for routin4because these specimens were alwayswithin
three weeks of receipt.
For day to day quality control of thealiquoted sample of serum
or a leucocyte penormal control and an obligate TSD he(stored at
-70°C) were included with eactest specimens. The values obtained
for the
usually varied by ± 3 percentage points between runs(for
example, 44 to 490/o Hex A for the heterozygousserum). If a value
outside these limits was obtained inany run, the data for that run
were rejected and the
0whole batch of specimens was reanalysed.A study in which
leucocytes and serum from
normal subjects, TSD and Sandhoff's disease hetero-zygotes,
andTSDpatients wereassayed simultaneouslyusing our standard manual
method and the automatedmethod showed that the mean difference'6
betweenresults was only 0-8 percentage points for analysis
ofleucocytes and 3-2 percentage points for serum. Theautomated
method gave results for serum which were,on average, 3 2 percentage
points higher than thosegiven by the manual method, but the
discriminationbetween normal, heterozygous, and TSD affectedgroups
was not compromised. The 3-2 percentagepoints difference between
manual and automatedmethods found with serum may have been because
ofslight colour quenching occurring when fluorescence
us of samples was read in smaller volumes. The effectwould not
be expected with colourless leucocytesamples.Although our screening
programme was based on
20 24 taking the value for percentage Hex A in serum as
theprimary indicator of genotype, the sera data wereexamined as a
two dimensional plot of Hex A activity
ity measured versus percentage Hex A in an attempt to reducei
misclassification (fig 4). This approach has beenfetu5, a discussed
by Gold,' who presented data for serumoinedpoint hexosaminidase as
a two dimensional plot of Hex A
versus Hex B. We found the approach to be useful inassessing
genotype in borderline subjects (55 to 590/o
particular Hex A in serum) before the leucocyte assay wasthe
assay completed, but in practice always retested using
ien plasma leucocytes. This involved recalling about 3% ofer
leads to subjects initially screened using serum.ing needle. The
carrier frequency found for the UK AshkenaziTay-Sachs population (1
in 27 based on 2965 subjects screened)i this fluid compares with
that reported elsewhere (for example,advantage. 1 in 31 in a North
American Jewish population').which had The assay for Hex A in serum
using the sulphatedunreliable substrate can also be readily
automated. Measurement
r tendency of Hex A activity alone was found to give poorne
protein discrimination between carriers and non-carriers,
butleading to when plotted against Hex A as a fraction of total
Hexmt that we (measured with the centrifugal analyser and thentrols
and unsulphated substrate) good discrimination wasr reference
obtained (fig 7). This assay has the advantage ofy obtained.
avoiding the heat inactivation step and may also detectescreening
carriers of the rare TSD B1 variant who have normalprocessed Hex A
activity when measured by the heat inactivation
method.'8 19 A careful comparison of figs 4 and 7assays, an
shows that the two discriminant test with the sulphated-llet from a
substrate gives better separation between carriers andterozygote
normal subjects than the test based on heat inactivation.,h batch
of Bayleran et al8 also found this to be the case, usingse samples
manual assays and analysing their data to transform
107
on June 22, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.2.101 on 1 F
ebruary 1991. Dow
nloaded from
http://jmg.bmj.com/
-
Landels, Ellis, Bobrow, Fensom
Hex A results obtained with the sulphated substrateto equivalent
units to those obtained with the un-sulphated substrate. However,
these workers, andalso Ben-Yoseph et al,9 obtained good
separationbetween controls (37 and 33 studied in each
series,respectively) and carriers (19 studied in both series)using
serum Hex A activity as a single discriminant.In contrast, we found
that with our larger groups of66 controls and 30 carriers (and
using slightlydifferent assay conditions) poor separation of
geno-types was obtained by measuring activity towards thesulphated
substrate alone.
Screening of pregnant women poses particularproblems since
during pregnancy the serum activityof heat stable intermediate Hex
isoenzymes increases,thus reducing the relative activity of Hex A
andleading to a falsely low percentage Hex A.5 In anattempt to
overcome this problem we assayed absoluteactivity of Hex A in serum
from pregnant carriers andnon-carriers using both the heat
inactivation methodand the sulphated substrate.There was no
discrimination between pregnant
carriers and pregnant non-carriers when Hex A inserum samples
was measured by heat inactivation (fig8). However, discrimination
was improved in thegroup of patients studied when Hex A was
measuredwith the sulphated substrate (fig 9). In using the
heatinactivation method it is assumed that only Hex A
isthermolabile, but other hexosaminidases may also bethermolabile
to a small degree,20 and this will lead toerrors in Hex A
determination. On the other hand,measurement of Hex A activity with
the sulphatedsubstrate relies on its specificity for this
substrate, anderrors will be introduced if any hydrolysis by
otherisoenzymes occurs. On balance, since our studies(Fensom and
Landels, unpublished data) show thatHex B and Hex I separated by
FPLC have negligibleactivity towards the sulphated substrate, it is
likelythat the slight thermolability of other isoenzymesintroduces
more error than non-specific hydrolysis ofthe sulphated substrate,
thus explaining the betterdiscrimination obtained with the
sulphated substrate.
In addition to problems caused during pregnancyby an increase in
Hex I, a further complication arisesfrom increase in Hex A itself.
This increase isprobably the result of transfer of fetal Hex A to
themother. Navon et a12' showed that serum Hex Aremained unchanged
during the second trimester inthree pregnant obligate carriers for
TSD who carriedaffected fetuses, whereas it increased four-fold in
twopregnant mothers affected with adult onset GM2-gangliosidosis
who carried unaffected fetuses. Thiscomplication is likely to
reduce the usefulness ofmeasurement of Hex A in serum with the
sulphatedsubstrate for carrier detection at later gestationaltimes;
however, our results in sera taken earlierduring pregnancy are
encouraging (fig 9). In the caseof one obligate carrier, serum was
sampled during two
pregnancies, one where the fetus was affected withTSD, and the
other where the fetus was a non-carrier.Both sera were taken at 10
weeks' gestation; the HexA levels are very similar (see fig 7; the
two points arejoined). Thus, at 10 weeks' gestation, the
fetalcontribution to maternal serum of Hex A appears tobe very
small, and even when the fetus is a non-carriershould not cause the
maternal serum Hex A level ofcarriers to approach the non-carrier
range. Theseresults, though encouraging, are preliminary; at
anygestation it remains prudent to confirm carrier statuswith the
more reliable leucocyte assay.
We thank the British Tay-Sachs Foundation forgenerous financial
support, Mrs Debbie Seedburghand Mrs Zahavah Heckscher for
secretarial andcommunity screening assistance, and Miss
AdrienneKnight for preparation of the manuscript. Dr MMcLaren
(Roche Diagnostics) provided useful advicein adapting our methods
to the centrifugal analyser.The work of the Paediatric Research
Unit is supportedby the Spastics Society and the Generation
Trust.
1 Sandhoff K, Conzelmann E, Neufeld EF, Kaback MM, SuzukiK. The
GM2 gangliosidoses. In: Scriver CR, Beaudet AL, SlyWS, Valle D,
eds. The metabolic basis of inherited disease. 6th ed.New York:
McGraw-Hill, 1989:1807-39.
2 O'Brien JS, Okada S, Chen A, Fillerup DL. Tay-Sachs
disease:detection of heterozygotes and homozygotes by serum
hexo-saminidase assay. N EnglJ3 Med 1970;283:15-20.
3 Kaback MM, Zeiger RS. Heterozygote detection in
Tay-Sachsdisease: a prototype community screening programme for
theprevention of recessive genetic disorders. Adv Exp Biol
Med1972;19:613-32.
4 Kaback MM, Bailin G, Hirsch P, Roy C. Automated
thermalfractionation of serum hexosaminidase: effect of alteration
inreaction variables and implication for Tay-Sachs
heterozygotescreening. In: Kaback MM, ed. Tay-Sachs disease:
screening andprevention. New York: Alan R Liss, 1977:197-212.
5 Stirling JL. Separation and characterisation of
N-acetyl-fl-gluco-saminidases A and P from maternal serum. Biochim
BiophysActa 1972;271:154-62.
6 Lowden JA, Zuker S, Wilensky AJ, Skomorowski MA. Screen-ing
for carriers of Tay-Sachs disease: a community project. CanMed
AssocJ 1974;111:229-33.
7 Fuchs W, Navon R, Kaback MM, Kresse H. Tay-Sachs
disease:one-step assay of ,l-N-acetylhexosaminidase in serum with
asulfated chromogenic substrate. Clin Chim Acta
1983;133:253-61.
8 Bayleran J, Hechtman P, Saray W. Synthesis of
4-methyl-umbelIiferyl-i-D-N-acetylglucosamine-6-sulfate and its use
inclassification of GM2 gangliosidosis genotypes. Clin Chim
Acta1984;143:73-89.
9 Ben-Yoseph Y, Reid JE, Shapiro B, Nadler H. Diagnosis
andcarrier detection of Tay-Sachs diseases: direct determination
ofhexosaminidase A using 4-methylumbelliferyl derivatives of
IP-N-acetylglucosamine-6-sulfate and
P-N-acetylgalactosamine-6-sulfate. AmJ Hum Genet
1985;37:733-48.
10 Arpaia E, Dumbrille-Ross A, Maler T, et al. Identification of
analtered splice site in Ashkenazi Tay-Sachs disease.
Nature1988;333:85-6.
11 Myerowitz R, Costigan FC. The major defect in Ashkenazi
Jewswith Tay-Sachs disease is an insertion in the gene for the
a-chain of l-hexosaminidase. J Bwl Chem 1988;263:18587-9.
12 Evans P. Tay-Sachs screening in Britain. In: Kaback MM,
ed.Tay-Sachs disease: screening and prevention. New York: Alan
RLiss, 1977:55-9.
13 Dulaney JT, Moser HW. Sulphatide lipidosis: metachromatic
108
on June 22, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.2.101 on 1 F
ebruary 1991. Dow
nloaded from
http://jmg.bmj.com/
-
Tay-Sachs carrier screening
leucodystrophy. In: Stanbury JB, Wyngaarden JB,
FredericksonDS,eds. The metabolic basis ofinheriteddisease. 4thed.
New York:McGraw-Hill, 1978:770-809.
14 Lowry OH, Rosebrough NJ, Farr AL, Randall RJ.
Proteinmeasurement with the Folin phenol reagent. J Biol Chem1951
;193:265-75.
15 Kaback MM. Thermal fractionation of serum
hexosaminidases:applications to heterozygote detection and
diagnosis of Tay-Sachs disease. In: Ginsberg V, ed. Methods in
enzymology. VolXXVIII. New York: Academic Press, 1972:862-7.
16 Bland JM, Altman DG. Statistical methods for assessing
agree-ment between two methods of clinical measurement.
Lancet1986;i:307-10.
17 Gold R. Genetic screening: how to use the data. In: Callahan
JW,Lowden JA, eds. Lysosomes and lysosomal storage diseases.
NewYork: Raven Press, 1981:357-71.
18 Charrow J, Inui K, Wenger D. Late onset GM2-gangliosidosis:
ana-locus genetic compound with near normal hexosaminidaseactivity.
Clin Genet 1985;27:78-84.
19 Besley GTN, Broadhead DM, Young JA. Diagnosis of
hexo-saminidase A deficiency with sulphated substrate: evidence
foran alpha-locus genetic compound in a Tay-Sachs variant.
In:Salvayre R, Douste-Blazy L, Gatt S, eds. Lipid storage
disorders:biological and medical aspects. New York: Plenum
Press,1988:247-52.
20 Dance N, Price RG, Robinson D, Stirling JL. l-galactosidase,
1-glucosidase and N-acetyl-,-glucosaminidase in human kidney.Clin
Chim Acta 1969;24:189-97.
21 Navon R, Lejbkowicz I, Adam A. Fetal hexosaminidase A
inmother's serum: pitfalls for carrier detection and prospects
forprenatal diagnosis of GM2-gangliosidoses. Am J7 Hum
Genet1987;40:60-1.
109
on June 22, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.2.101 on 1 F
ebruary 1991. Dow
nloaded from
http://jmg.bmj.com/