Embed Size (px)
Citation preview
Brit. J. vener. Dis. (1958), 34, 219.
CHRONIC BENIGN CIRCUMSCRIBED PLASMA CELLBALANO-POSTHITIS*
BY
W. FOWLERThe Royal Hospital, Wolverhamtlpton
Chronic benign circumscribed plasma cell balano-posthitis is the name given by Zoon (1952) to adisease which clinically resembles the erythroplasiadescribed by Queyrat (1911) but has a distinctivehistology.Zoon (1952) studied the disease in eight patients;
two of these were in the third decade of life, one was58 years old, and the others 60 years or more. Theduration of the disease was unknown in two cases,one year in two cases, and 12, 15, and 20 years in theremainder. In the majority of cases both the glanspenis and the prepuce were affected. In one case thedisease was limited to the inferior surface of theprepuce and in another to the area around theurinary meatus.
Histologically one case showed a moderate,benign acanthosis, and in the others the epidermistended to be atrophied and was usually reduced to afew layers of cells. In some areas there was intra- andextra-cellular oedema. Some of the epidermal cellswere vacuolated and resembled dyskeratotic cells.The granular layer was absent in every case andthere was no hyperkeratosis. The dermal papillaewere absent and the epidermo-dermal junction was astraight line. There was an inflammatory infiltrationin the upper part of the corium, consisting of plasmacells with a few lymphocytes, eosinophils, andfibroblasts. There were many dilated capillaries, thewalls of which were often thickened. The connectivetissue was oedematous. The elastic tissue fibresstained normally. The prussian blue reaction wasnegative. Two patients received no treatment, oneresponded to contact x-ray therapy, and five resistedall treatment including radiotherapy.Zoon (1952) was unable to discover the aetiology
of the disease which was neither a toxic eruption,nor due to venereal disease, tuberculosis, or externalirritation.As chronic benign circumscribed plasma cell
balano-posthitis does not appear to be very com-mon, the following cases may be of interest.
Case ReportsCase 1, a widower aged 75 years, attended hospital onApril 16, 1955, complaining of swelling and inflammation
* Received for publicat'nn March 29, 1958.
of the penis of a few days' duration. Recently he hadnoticed that it was becoming increasingly difficult toretract the prepuce. There was no history of recent coitusand he had never suffered from venereal disease.
Examination.-The condition appeared to be a simpleparaphimosis with secondary balano-posthitis.
Treatment.-The paraphimosis was reduced easily.The balano-posthitis responded slowly to treatment withsimple antiseptics, and by May 16, 1955, the prepuce wasnormal and the glans was also normal except for somebrown staining on the right side of the dorsum. Thisstaining disappeared during the next week and thepatient was discharged as cured on June 25. The prepucewas tight but could be retracted and circumcision was notindicated in view of his age.
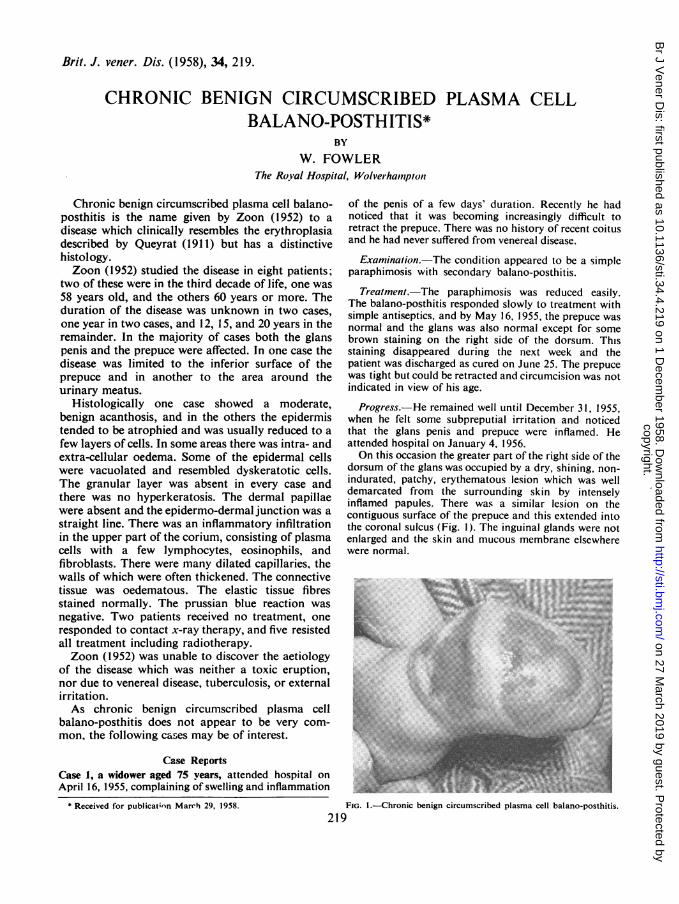
Progress.-He remained well until December 31, 1955,when he felt some subpreputial irritation and noticedthat the glans penis and prepuce were inflamed. Heattended hospital on January 4, 1956.On this occasion the greater part of the right side of the
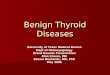
dorsum of the glans was occupied by a dry, shining, non-indurated, patchy, erythematous lesion which was welldemarcated from the surrounding skin by intenselyinflamed papules. There was a similar lesion on thecontiguous surface of the prepuce and this extended intothe coronal sulcus (Fig. 1). The inguinal glands were notenlarged and the skin and mucous membrane elsewherewere normal.
"IsA
PIN !I
6\i. .: 2 . o
F.1-hron.ic-ben c cVibp s a -.bo
FIG. I.-hronic benign circumscribed plasma cell balano-posthitis.219
copyright. on 27 M
arch 2019 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.34.4.219 on 1 Decem
ber 1958. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
Arrangements for biopsy were made, but when thepatient attended for this investigation the conditionshowed so much improvement that biopsy was post-poned. Calamine liniment was prescribed and onFebruary 11 the glans and prepuce again appearednormal.The patient was next seen on January 7, 1957, when he
complained of severe subpreputial irritation, and statedthat during the previous 11 months there had beenperiodic attacks of slight balano-posthitis which dis-appeared spontaneously.On examination the condition was essentially the same
as on January 4th, 1956. Biopsy was carried out onJanuary 10.
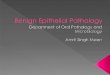
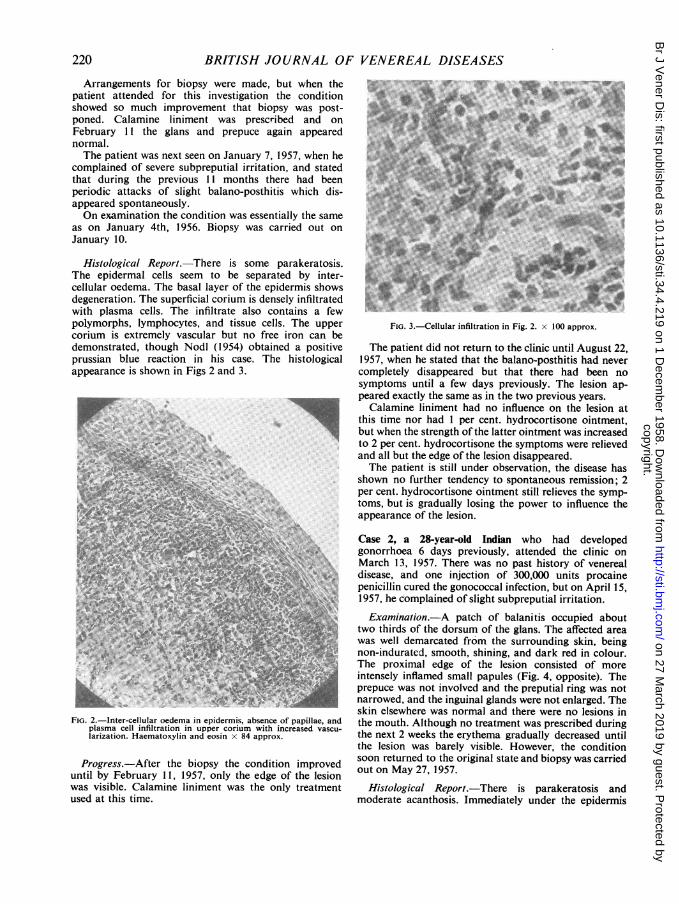
Histological Report.-There is some parakeratosis.The epidermal cells seem to be separated by inter-cellular oedema. The basal layer of the epidermis showsdegeneration. The superficial corium is densely infiltratedwith plasma cells. The infiltrate also contains a fewpolymorphs, lymphocytes, and tissue cells. The uppercorium is extremely vascular but no free iron can bedemonstrated, though NodI (1954) obtained a positiveprussian blue reaction in his case. The histologicalappearance is shown in Figs 2 and 3.
i...*d. ;WT .v. P..'
FIG. 2.-Inter-cellular oedema in epidermis, absence of papillae, andplasma cell infiltration in upper corium with increased vascu-larization. Haematoxylin and eosin x 84 approx.
Progress.-After the biopsy the condition improveduntil by February 11, 1957, only the edge of the lesionwas visible. Calamine liniment was the only treatmentused at this time.
FIG. 3.-Cellular infiltration in Fig. 2. x 100 approx.
The patient did not return to the clinic until August 22,1957, when he stated that the balano-posthitis had nevercompletely disappeared but that there had been nosymptoms until a few days previously. The lesion ap-peared exactly the same as in the two previous years.Calamine liniment had no influence on the lesion at
this time nor had 1 per cent. hydrocortisone ointment,but when the strength of the latter ointment was increasedto 2 per cent. hydrocortisone the symptoms were relievedand all but the edge of the lesion disappeared.The patient is still under observation, the disease has
shown no further tendency to spontaneous remission; 2per cent. hydrocortisone ointment still relieves the symp-toms, but is gradually losing the power to influence theappearance of the lesion.
Case 2, a 28-year-old Indian who had developedgonorrhoea 6 days previously, attended the clinic onMarch 13, 1957. There was no past history of venerealdisease, and one injection of 300,000 units procainepenicillin cured the gonococcal infection, but on April 15,1957, he complained of slight subpreputial irritation.
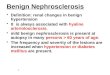
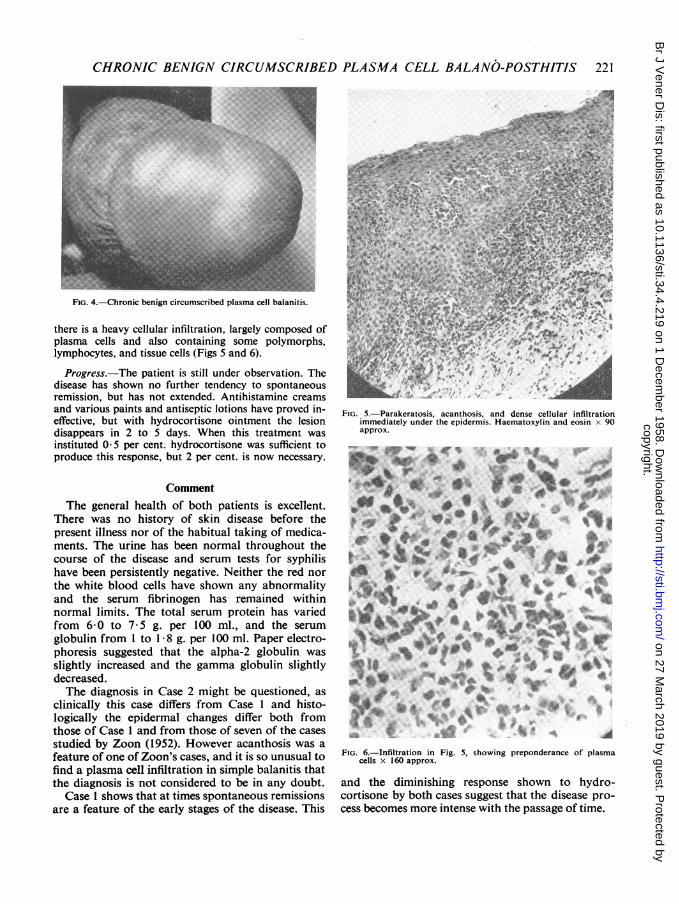
Examination.-A patch of balanitis occupied abouttwo thirds of the dorsum of the glans. The affected areawas well demarcated from the surrounding skin, beingnon-indurated, smooth, shining, and dark red in colour.The proximal edge of the lesion consisted of moreintensely inflamed small papules (Fig. 4, opposite). Theprepuce was not involved and the preputial ring was notnarrowed, and the inguinal glands were not enlarged. Theskin elsewhere was normal and there were no lesions inthe mouth. Although no treatment was prescribed duringthe next 2 weeks the erythema gradually decreased untilthe lesion was barely visible. However, the conditionsoon returned to the original state and biopsy was carriedout on May 27, 1957.
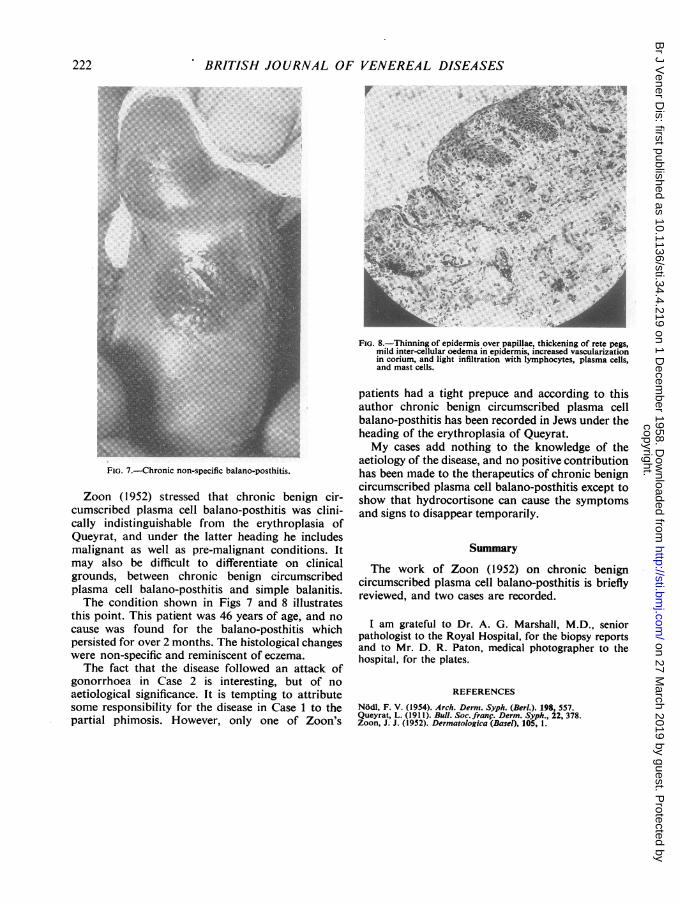
Histological Report.-There is parakeratosis andmoderate acanthosis. Immediately under the epidermis
220
copyright. on 27 M
arch 2019 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.34.4.219 on 1 Decem
ber 1958. Dow
nloaded from
CHRONIC BENIGN CIRCUMSCRIBED PLASMA CELL BALANO-POSTHITIS 221
FIG. 4.-Chronic benign circumscribed plasma cell balanitis.
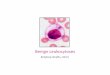
there is a heavy cellular infiltration, largely composed ofplasma cells and also containing some polymorphs,lymphocytes, and tissue cells (Figs 5 and 6).
Progress.-The patient is still under observation. Thedisease has shown no further tendency to spontaneousremission, but has not extended. Antihistamine creamsand various paints and antiseptic lotions have proved in-effective, but with hydrocortisone ointment the lesiondisappears in 2 to 5 days. When this treatment wasinstituted 0 5 per cent. hydrocortisone was sufficient toproduce this response, but 2 per cent. is now necessary.
CommentThe general health of both patients is excellent.
There was no history of skin disease before thepresent illness nor of the habitual taking of medica-ments. The urine has been normal throughout thecourse of the disease and serum tests for syphilishave been persistently negative. Neither the red northe white blood cells have shown any abnormalityand the serum fibrinogen has remained withinnormal limits. The total serum protein has variedfrom 6-0 to 7 5 g. per 100 ml., and the serumglobulin from 1 to 1 8 g. per 100 ml. Paper electro-phoresis suggested that the alpha-2 globulin, wasslightly increased and the gamma globulin slightlydecreased.The diagnosis in Case 2 might be questioned, as
clinically this case differs from Case I and histo-logically the epidermal changes differ both fromthose of Case 1 and from those of seven of the casesstudied by Zoon (1952). However acanthosis was afeature of one of Zoon's cases, and it is so unusual tofind a plasma cell infiltration in simple balanitis thatthe diagnosis is not considered to be in any doubt.
Case 1 shows that at times spontaneous remissionsare a feature of the early stages of the disease. This
.. i, ,, X ,, ,t4k~~ :s4$}.A.*. .i "t ..,1r;Ms9
. A>. @
A
FIG. 5.-Parakeratosis, acanthosis, and dense cellular infiltrationimmediately under the epidermis. Haematoxylin and eosin x 90approx.
4k
A
F A~~~~~~~~~~A
FIo 6Ifilrto in Fi 5,showing prpodrac of plasm
cellsx-16 approx>
adth dimini..vshn resoe shown.to8 hyro
ces beoe mor ines wit th pasg of time
*̂* {: *. .. #t .* * ;#~~~~~~b.WAO ,e o/.S.Wi*s+4t t*~>:
*wM A!jC %.
FIG. 6.-Infiltration in Fig. 5, showing preponderance of plasmacells x 160 approx.
and the diminishing response shown to hydro-cortisone by both cases suggest that the disease pro-cess becomes more intense with the passage of time.
copyright. on 27 M
arch 2019 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.34.4.219 on 1 Decem
ber 1958. Dow
nloaded from
22BRITISH JOURNAL OF VENEREAL DISEASES
4.P¢Si; ' b.e '> .
AJIF~~~~~
9.5k'.P _
.9~~~~~~~~~~~~~~~O
FIG. 8.-Thinning of epidermis over papillae, thickening of rete pegs,mild inter-cellular oedema in epidermis, increased vascularizationin corium, and light infiltration with lymphocytes, plasma cells,and mast cells.
FIG. 7.-Chronic non-specific balano-posthitis.
Zoon (1952) stressed that chronic benign cir-cumscribed plasma cell balano-posthitis was clini-cally indistinguishable from the erythroplasia ofQueyrat, and under the latter heading he includesmalignant as well as pre-malignant conditions. Itmay also be difficult to differentiate on clinicalgrounds, between chronic benign circumscribedplasma cell balano-posthitis and simple balanitis.The condition shown in Figs 7 and 8 illustrates
this point. This patient was 46 years of age, and nocause was found for the balano-posthitis whichpersisted for over 2 months. The histological changeswere non-specific and reminiscent of eczema.The fact that the disease followed an attack of
gonorrhoea in Case 2 is interesting, but of noaetiological significance. It is tempting to attributesome responsibility for the disease in Case 1 to thepartial phimosis. However, only one of Zoon's
patients had a tight prepuce and according to thisauthor chronic benign circumscribed plasma cellbalano-posthitis has been recorded in Jews under theheading of the erythroplasia of Queyrat.My cases add nothing to the knowledge of the
aetiology of the disease, and no positive contributionhas been made to the therapeutics of chronic benigncircumscribed plasma cell balano-posthitis except toshow that hydrocortisone can cause the symptomsand signs to disappear temporarily.
Summary
The work of Zoon (1952) on chronic benigncircumscribed plasma cell balano-posthitis is brieflyreviewed, and two cases are recorded.
I am grateful to Dr. A. G. Marshall, M.D., seniorpathologist to the Royal Hospital, for the biopsy reportsand to Mr. D. R. Paton, medical photographer to thehospital, for the plates.
REFERENCES
NOdM, F. V. (1954). Arch. Derm. Syph. (Berl.). 198, 557.Queyrat, L. (191 1). Bull. Soc. franc. Derm. Syph., 22, 378.Zoon, J. J. (1952). Dermatologica (Basel), 105, 1.
222
copyright. on 27 M
arch 2019 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.34.4.219 on 1 Decem
ber 1958. Dow
nloaded from