Embed Size (px)
Citation preview
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 1
“I am Not Sick, I Don’t Need Help!”“I am Not Sick, I Don’t Need Help!”
Research on poor insight and how we can help using LEAP®
American Psychiatric Nurses AssociationClinical Psychopharmacology Institute
June 20, 2014
Xavier Amador, Ph.D.Director, LEAP Institute
www.LEAPinstitute.org
Poor insight and relationships
© LEAP Associates, LLC, 2013
“Denial” of illness in the news
Amador et al. Schizophr Bull.1991;17:113–132; Amador.
I am not sick, I don’t need help! How to help someone with mental
illness accept treatment. New York: Vida Press; 2007
…news stories involving such persons appear nearly every day.
• Poor insight into schizophrenia and bipolar disorder is so common…
© LEAP Associates, LLC, 2013
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 2
Colorado Theatre Shooting
© LEAP Associates, LLC, 2013
The Unabomber – Ted Kaczynski
• More “denial” in the headlines
Amador XF, Reshmi P.Defending the Unabomber: anosognosia and schizophrenia. Psychiatric Quarterly. 2000; 71(4): 363-370.
© LEAP Associates, LLC, 2013
“Denial” of illness
• Denial impairs common-sense judgment about the need for treatment and services. Yes?– But are we dealing with denial?
“Anosognosia”
Diagnostic and Statistical Manual of Mental Disorders. 4th ed (Text Revision). Washington, DC, APA, 2000.
© LEAP Associates, LLC, 2013
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 3
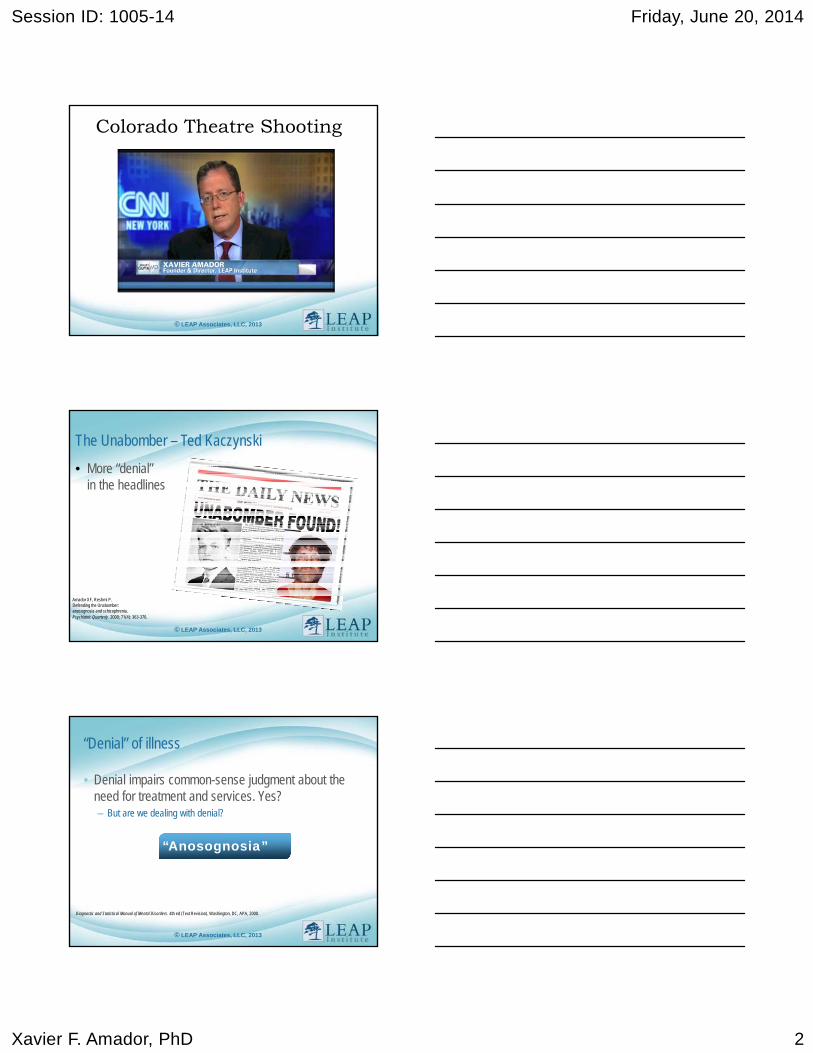
Unawareness of mental disorderDSM-IV field-trial–study patients with schizophrenia (n=221)
Missing data 1.9%
ModeratelyUnaware25.3%
Aware40.7%
Unaware32.1%
Amador XF, et al. Arch Gen Psychiatry. 1994;51(10):826–836.
© LEAP Associates, LLC, 2013
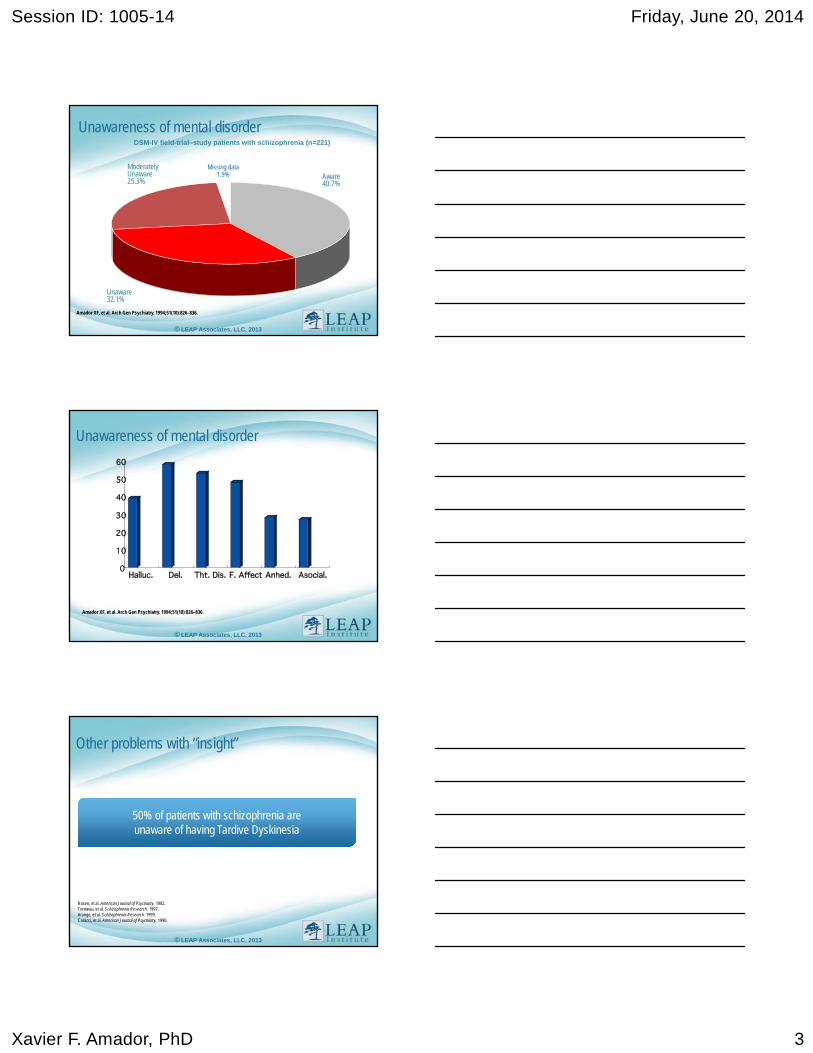
Unawareness of mental disorder
Amador XF, et al. Arch Gen Psychiatry. 1994;51(10):826–836.
© LEAP Associates, LLC, 2013
Other problems with “insight”
50% of patients with schizophrenia are unaware of having Tardive Dyskinesia
Rosen, et al. American Journal of Psychiatry. 1982.Tremeau, et al. Schizophrenia Research. 1997. Arango, et al. Schizophrenia Research. 1999.Caracci, et al. American Journal of Psychiatry. 1990.
© LEAP Associates, LLC, 2013
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 4
The problem with oral antipsychotic medications
• Between 50% and 75% of patients with schizophrenia exhibit full or partial nonadherence to pharmacological treatment (Rummel-Kluge, 2008)
• Within 7 to 10 days of medication initiation (Keith & Kane, 2003) – 25% are noncompliant
– 50% are off medication after 1 year
– Up to 75% after 2 years
• Approximately 33% reliably take medication prescribed (Oehl, 2000)
© LEAP Associates, LLC, 2013
Insight and adherence
• Awareness of being ill (insight) is among the top 2 predictors of long-term medication adherence
• What is the other top predictor?– Relationship with someone who:
• Listens to you without judgment• Respects your point of view• Believes you would benefit from treatment
© LEAP Associates, LLC, 2013
Insight and adherence
• We never “win” on the strength of our argument, we win on the strength of our relationship.
© LEAP Associates, LLC, 2013
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 5
Insight and adherence…
www.LEAPInstitute.org
What causes poor insight
Psychological defense?
“Cultural” and/or education?
Neuropsychological deficits?
DSM-IV-TR™ Schizophrenia and other psychotic disorders
Drs. Xavier Amador and Michael Flaum, co-chairs
• A majority of individuals with schizophrenia have poor insight regarding the fact that they have a psychotic illness. Evidence suggests that poor insight is a manifestation of the illness rather than a coping strategy.
• It may be comparable to the lack of awareness of neurological deficits seen in stroke, termed anosognosia.
• This symptom predisposes the individual to noncompliance with treatment and has been found to be predictive of higher relapse rates, increased number of involuntary hospital admissions, poorer psychosocial functioning, and a poorer course of illness. (page 304)
Diagnostic and Statistical Manual of Mental Disorders. 4th ed (Text Revision). Washington DC, APA, 2000.
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 6
DSM-V™ Schizophrenia and other psychotic disordersDr. William T. Carpenter. Chair (Text submitted by Dr. Xavier Amador)
• Unawareness of illness is typically a symptom rather than a coping strategy. It is comparable to the lack of awareness of neurological deficits following brain damage, termed anosognosia.
• This symptom is the most common predictor of nonadherence to treatment. It has been found to predict higher relapse rates, increased number of involuntary treatments, poorer psychosocial functioning, aggression, and a poorer course of illness. (page 101)
Diagnostic and Statistical Manual of Mental Disorders. 5th ed.. Washington DC, APA, 2013.
www.LEAPInstitute.org
Anosognosia is similar
Very severe lack of awareness
Confabulations are common
The belief persists, despite conflicting evidence
www.LEAPInstitute.org
Anosognosia for mental illness: What it feels like.
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 7
When dealing with anosognosia for mental illness…
• The “doctor knows best” approach does not work, because collaboration is a goal, not a given
Do not expect:• Gratitude• Receptiveness• Adherence
Do expect:• Frustration and anger• Suspiciousness• Overt and secretive “non-compliance”
© LEAP Associates, LLC, 2013
When dealing with anosognosia for mental illness…
Long-Acting Treatments (LAT’s) are indicated:
• 50% on orals stopped medication compared to only
• 17% on long-acting injections– But how can you offer a LAT in a manner that is likely to lead to
acceptance and partnering long-term?
• LEAP and related approaches
Keith & Kane. J Clin Psychiatry 2003;64:1308–1315; Young et. Al., 1999; Zygmunt et al. Am J Psychiatry 2002;159:1653–1664
© LEAP Associates, LLC, 2013
www.LEAPInstitute.org
Motivational interviewing: Studied extensively in patients with substance abuse disorders
• Interventions to Improve Medication Adherence in Schizophrenia1
• Reviewed studies from 1980 through 2000
• “Although interventions and family therapy programs relying on psychoeducation were common in clinical practice, they were typically ineffective”
• “Motivational techniques [such as LEAP] were common features of successful programs”
Please see LEAPInstitute.org “Research” for additional evidence.• Zygmunt, et al. Am J Psychiatry. 2002;1653-1664.
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 8
LEAP
• The LEAP approach– Listen
– Empathize
– Agree
– Partner
2000
2007
2008
Based on MAIT, Amador & Beck.
© LEAP Associates, LLC, 2013
Over the past 10 years LEAP has taught to tens of thousands globally (EU, USA, Asia Pacific)
www.LEAPInstitute.org
ListenLEAP: Listen, Empathize, Agree, Partner
• Reflectively to:
Delusions
Anosognosia
Desires
ListenLEAP: Listen, Empathize, Agree, Partner
• Why do we resist reflecting back many important things our patients tell us?– We fear we will make “it” worse (ie, delusions, insight, attitudes
about medication, etc)
– We do not want to be asked to do something we cannot
– We worry about injuring the therapeutic alliance
– We fear we have to be dishonest
© LEAP Associates, LLC, 2013
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 9
LEAP: Listen, Empathize, Agree, Partner
How to delay giving your opinion
• “I promise to answer your question. If it’s alright with you, I would like to first hear more about _________. Okay?”
• “I will tell you what I think. I would like to keep listening to your views on this, because I am learning a lot I didn’t know. Can I tell you later what I think?”
• “I will tell you. But, I believe your opinion is more important than mineand I would like to learn more before I tell you my opinion. Would that be okay?”
© LEAP Associates, LLC, 2013
When you finally give your opinion, use the 3 AsLEAP: Listen, Empathize, Agree, Partner
Apologize• “I want to apologize, because my views
might feel hurtful or disappointing”
Acknowledgefallibility
• “Also, I could be wrong. I don’t know everything”
Agree• “I hope that we can just agree to
disagree. I respect your point of view and I hope you can respect mine”
© LEAP Associates, LLC, 2013
EmpathizeLEAP: Listen, Empathize, Agree, Partner
• Strategically express empathy for:– Delusional beliefs
– Desire to prove “I’m not sick!”
– Wish to avoid treatment
• Normalize the experience
© LEAP Associates, LLC, 2013
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 10
AgreeLEAP: Listen, Empathize, Agree, Partner
• Discuss only perceived problems and goals• Review advantages and disadvantages of adherence
• Reflect back and highlight the perceived costs and benefits
AGREE TO DISAGREE
© LEAP Associates, LLC, 2013
PartnerLEAP: Listen, Empathize, Agree, Partner
ou
both
agree
can
you
both
agree
Move forward on goals you both agree can be worked on together
© LEAP Associates, LLC, 2013
The 7 LEAP TOOLSLEAP: Listen, Empathize, Agree, Partner
• Listen• Empathize• Agree• Partner
• Delay• Opinion (3 A’s)• Apologize
© LEAP Associates, LLC, 2013
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 11
www.LEAPInstitute.org
• LEAP Practitioner Level-I Trainings
LEAP® LP-I Trainings in Turkey
www.LEAPInstitute.org
Therapeutic Alliance Program: LP-I Trainings• Results of LEAP® Trainings in Turkey (April-June 2010)
20 psychiatrist trainings
1 psychiatric nurse training
Over350 physicians
Over 200 nurses 50 family
caregivers
www.LEAPInstitute.org
LEAP® LP-I trainings
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 12
www.LEAPInstitute.org
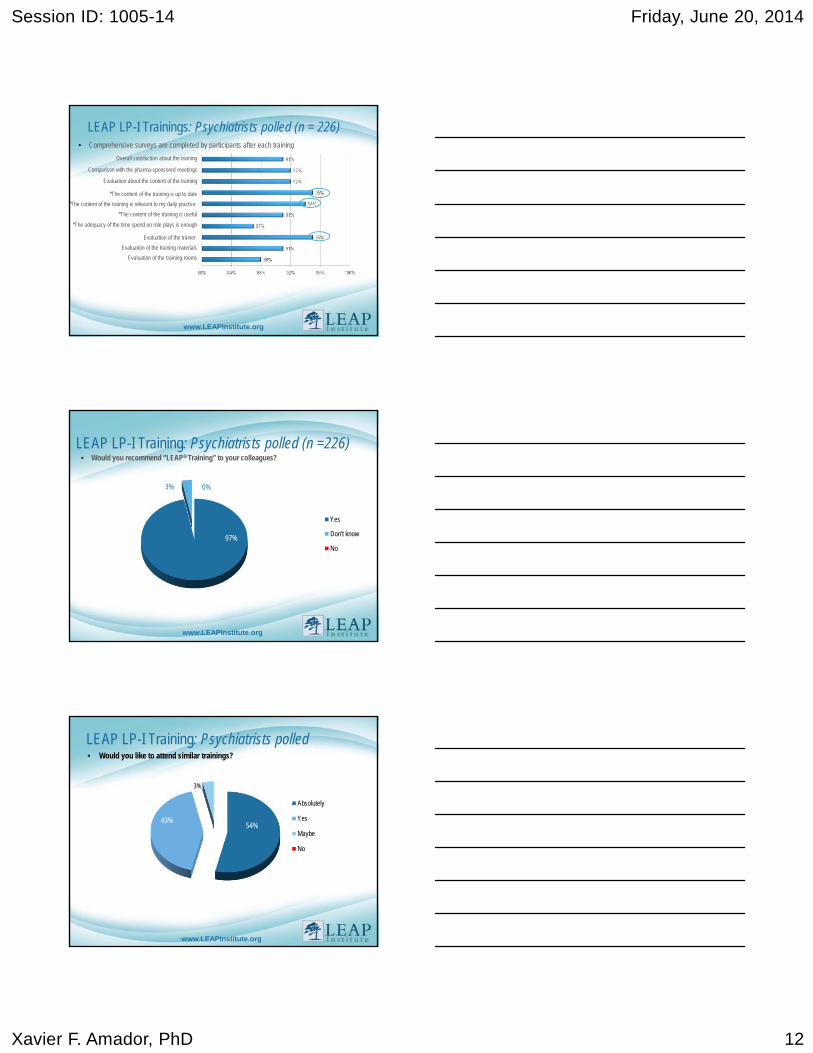
LEAP LP-I Trainings: Psychiatrists polled (n = 226) • Comprehensive surveys are completed by participants after each training
Overall satisfaction about the training
Comparison with the pharma-sponsored meetings
Evaluation about the content of the training
*The content of the training is up to date
*The content of the training is relevant to my daily practice
*The content of the training is useful
*The adequacy of the time spend on role plays is enough
Evaluation of the trainer
Evaluation of the training materials
Evaluation of the training rooms
www.LEAPInstitute.org
LEAP LP-I Training: Psychiatrists polled (n =226)• Would you recommend “LEAP® Training” to your colleagues?
Yes
Don't know
No
3% 0%
97%
97%
www.LEAPInstitute.org
LEAP LP-I Training: Psychiatrists polled• Would you like to attend similar trainings?
Absolutely
Yes
Maybe
No
3%
54%
3%
43%
Session ID: 1005-14 Friday, June 20, 2014
Xavier F. Amador, PhD 13
www.LEAPInstitute.org
LEAPLEAP: Listen, Empathize, Agree, Partner
THANK YOU!
Feel free to visit www.LEAPinstitute.org
For free training resources and so we can support your work.