-
7/28/2019 hypoxemic Resp. Failure
1/52
-
7/28/2019 hypoxemic Resp. Failure
2/52
Outline
1. Review of Pathophysiology
2. Clinical presentation and differential
diagnosis
3. ARDS
4. Reversible causes of ARDS Descriptionand Treatment
-
7/28/2019 hypoxemic Resp. Failure
3/52
Pathophysiology
Acute hypoxic respiratory failure (AHRF) is alsocalled Type I
Respiratory Failure.
Marked by severe hypoxemia that isunresponsive to supplemental
oxygen.
This results from widespread flooding andcollapse of alveoli
that causes blood to flow pastunventilated alveoli (V/Q ratio of
zero).
Also called shunt.
-
7/28/2019 hypoxemic Resp. Failure
4/52
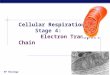
As can be seen above, blood passing through theright alveoli
does not pick up any oxygen while theleft is normal and fully
saturated.
The reduced oxygen content from the right mixeswith the left and
reduces the overall oxygen of the
blood returning to the heart.
-
7/28/2019 hypoxemic Resp. Failure
5/52
Pathophysiology
The intra-alveolar fluid and increased interstitialfluid
decreases overall lung compliance.
This imposes a larger elastic work of breathingresulted in
increased respiratory muscle oxygenconsumption.
A vicious cycle of increased O2 demand, muscle
fatigue and hypoxemia leads to respiratoryarrest and death if
mechanical assistance is notinstituted.
-
7/28/2019 hypoxemic Resp. Failure
6/52
-
7/28/2019 hypoxemic Resp. Failure
7/52
Differential Diagnosis of AHRF
1. Acute lung injury or ARDS
2. Acute cardiogenic pulmonary edema
3. Bilateral aspiration pneumonia4. Lobar atelectasis of both
lower lobes
5. Severe unilateral lower lobe atelectasis,especially when the
patient is receiving
vasodilators such as nitrates, calcium channelblockers, or
nitroprusside that blunt hypoxicvasoconstriction.
-
7/28/2019 hypoxemic Resp. Failure
8/52
Differential Diagnosis of AHRF
6. Main stem bronchus obstruction from mucousplug or blood
clot.
7. Bilateral or unilateral pneumothorax8. Large unilateral or
bilateral pleural effusions
9. Diffuse alveolar hemorrhage
10. Massive pulmonary embolus
11. Opening of patent foramen ovale with pre-existing pulmonary
hypertension.
-
7/28/2019 hypoxemic Resp. Failure
9/52
-
7/28/2019 hypoxemic Resp. Failure
10/52
Clinical Setting
Review of intravascular volume administrationwill often suggest
an explanation for pulmonary
edema in patients with left ventricular or renaldysfunction.
ALI or ARDS commonly arises in a typical clinicalcontext with
direct and indirect causes
(differential to be discussed soon).
-
7/28/2019 hypoxemic Resp. Failure
11/52
-
7/28/2019 hypoxemic Resp. Failure
12/52
Clinical Setting
Echocardiography is helpful in distinguishingcardiogenic from
noncardiogenic pulmonaryedema.
Echocardiography also helps identify leftventricular wall motion
abnormalities, mitralvalve dysfunction, and ventricular
dilation.
Early bronchoscopy is critical to identifyreversible causes and
guide therapy.
Bronchoscopy can help diagnose some causes ofAHRF including
diffuse alveolar hemorrhage,
pneumonia, and acute eosinophillic pneumonia.
-
7/28/2019 hypoxemic Resp. Failure
13/52
Acute Respiratory Distress
Syndrome (ARDS)Acute lung injury (ALI) and ARDS are
common causes of AHRF.
Both are defined by acute onset, bilateralpulmonary infiltrates
on chest x-rayconsistent with pulmonary edema,
hypoxemia and the absence of evidence ofleft atrial
hypertension.
-
7/28/2019 hypoxemic Resp. Failure
14/52
ARDS - Definition
The ratio of arterial oxygen (PaO2) to fraction ofinspired
oxygen (FiO2), also called the P/F ratio,
reflects the degree of hypoxemia at differentlevels of FiO2.
The syndrome is called ALI when the ratio is 60%) which is toxic
in itself. Higher levels of PEEP also prevents surfactant poor
alveoli from repeatedly opening and collapsing which isalso
injurious to the lungs.
-
7/28/2019 hypoxemic Resp. Failure
24/52
ARDS/ALI Ventilation Goals
Conventional ventilation strategy usually requires a tidalvolume
of 10-12 mL/kg in order to maintain minuteventilation and hence,
normal PaCO2.
However, in an injured lung, that volume causes excessstretch
and perpetuates the injury. Therefore, the current goal is a low
tidal volume strategy
of 6 mL/kg. If this tidal volume is insufficient for minute
ventilation
(even at a higher respiratory rate) then the resultantelevated
PaCO2 is tolerated as long as the pH is > 7.20. This is called
permissive hypercapnia.
-
7/28/2019 hypoxemic Resp. Failure
25/52
ARDS/ALI Other Adjuvant
Measures Prone Position Increases FRC, redistributes
perfusion
and better secretion clearance. Recruitment Maneuvers Open
partially collapsed alveoli
which is then kept inflated by a high level of PEEP. Other
savage measures:
NO Steroids during fibroproliferative stage High frequency
oscillation EMCO Partial liquid ventilation Surfactant
-
7/28/2019 hypoxemic Resp. Failure
26/52
Reversible Causes of ARDS/ALI
Bacterial pneumonia
Viral pneumonia
Fungal pneumonia PJP
Diffuse alveolar hemorrhage
Eosinophillic pneumonia Lupus pneumonitis
Toxic drug reaction
-
7/28/2019 hypoxemic Resp. Failure
27/52
Community Acquired Pneumonia
There are more than 100 microbes (bacteria,viruses, fungi, and
parasites) that can causeCAP.
Most cases of pneumonia are caused by 4 or 5microbes.
Bacteria are the most common cause of CAP andare divided into
two groups:
Typical S. pneumoniae, H. influenzae, S. aureus,GAS, M.
catarrhalis, anaerobes, and GNB. Atypical Legionella, Mycoplasma
and Chlamydophila
pneumoniae.
-
7/28/2019 hypoxemic Resp. Failure
28/52
Community Acquired Pneumonia
A microbiological diagnosis is confirmed in only20% of
cases.
There are a few clinical clues that must beconsidered for the
etiology of CAP
Know your local epidemiology
Be aware of outbreaks
Never forget TB and PJP
MRSA is an increasingly recognized cause of severe,necrotizing
CAP
-
7/28/2019 hypoxemic Resp. Failure
29/52
Community Acquired Pneumonia
Bacteria are the most common cause of CAP. S. pneumoniae: Most
common cause overall H. influenzae: Important in the elderly, COPD
and
CF. M. pneumoniae: The most common cause of
atypical pneumonias. C. pneumoniae: Accounts for 5-10% of
cases.
Most common in the elderly. Legionella: Causes 2-8% of cases
either
sporadically or outbreaks. Klebsiella: Should be considered as a
cause in
patients who have significant underlying diseasessuch as COPD,
diabetes, and alcohol abuse.
-
7/28/2019 hypoxemic Resp. Failure
30/52
Community Acquired Pneumonia
Pseudomonas: Community acquired Pseudomonasoccurs mainly in
immunocompromised patients orthose with structural lung
abnormalities such as
CF or bronchiectasis. Acinetobacter: Typically seen in
hospitalized
patients but starting to emerge in the community.
S. aureus: Usually seen in the elderly and young
who are recovering from influenza. GAS: Can cause a fulminant
pneumonia with early
empyema formation even in healthy patients.
-
7/28/2019 hypoxemic Resp. Failure
31/52
Community Acquired Pneumonia
Anaerobes: May be the cause of aspirationpneumonia and lung
abscesses. Role is notclear since detection in routine cultures is
not
possible. N. meningitidis: An uncommon cause of CAP
but is reportable to public health andprophylaxis must be
given.
TB: Missed diagnosis is common and manypatients are initially
treated for presumedCAP.
-
7/28/2019 hypoxemic Resp. Failure
32/52
Community Acquired Pneumonia -
Treatment The selection of specific antibiotics for
empiric therapy is based on a number of
principles: The most likely pathogen
Clinical trials proving efficacy
Risk factors for the presence of resistance Presence of medical
co-morbidities
-
7/28/2019 hypoxemic Resp. Failure
33/52
Community Acquired Pneumonia -
TreatmentAntibiotic recommendations for
hospitalized patients are divided between
ICU and non-ICU and whether the patientis admitted from a long
term care facility.
When the etiology of CAP is identified,
treatment regimen must be simplified anddirected to that
pathogen.
-
7/28/2019 hypoxemic Resp. Failure
34/52
Community Acquired Pneumonia -
Treatment Not in the ICU Cefotaxime 1 g q8h and azithromycin 500
mg daily
Levofloxicin 750 mg daily or moxifloxacin 400 mg daily
Admitted to ICU (high risk for resistant organisms)
Pipericillin/tazobactum 4.5 g q6h or imipenem 500 mg q6h
or meropenem 1 g q8h or cefepime 2 g q8h or ceftazidime 2g q8h
PLUS
Ciprofloxicin 400 mg q12h or levofloxicin 750 mg daily
oraminoglycoside
Penicillin allergy use aztreonam, an aminoglycoside,
andlevofloxicin
If initial gram strain suggests S. aureus then addvancomycin 15
mg/kg q12h
-
7/28/2019 hypoxemic Resp. Failure
35/52
Viral Pneumonia
Viruses are estimated to cause adult CAP in 10to 31% of
cases.
Influenza A or B occurs in outbreaks and
epidemics. They can cause pneumonia althoughthey are more likely
to cause a URTI and thenpredispose to a secondary pneumonia.
High risk patients include patients with heart
and lung disease, diabetes, renal diseases,immunosuppression,
nursing home residentsand over 65.
-
7/28/2019 hypoxemic Resp. Failure
36/52
Viral Pneumonia
Parainfluenza are important in theimmunocompromised patients
causing lifethreatening lower respiratory tract infections.
RSV is more common in children but can causeCAP in elderly.
Adenovirus presents with fever, cough, andperibronchial markings
with patchy alveolar
infiltrates. Metapneumovirus is an emerging pathogen and
causes disease in young children and theelderly.
-
7/28/2019 hypoxemic Resp. Failure
37/52
Viral Pneumonia
SARS is a coronavirus that caused an outbreak after itjumped
species in 2002. Currently quiescent.
Hantavirus is spread from the feces of infected mice.The illness
is preceded by prodromal flu-like symptomsfollowed by ARDS. The
virus does not cause pneumoniaand the ARDS is from the host
response.
Avian influenza currently causes sporadic outbreaks butWHO and
CDC consider it to be a potential source forthe next global
pandemic.
Varicella pneumonia is the most frequent complication
ofvaricella infection in healthy adults with a case fatalityrate of
10-30%.
-
7/28/2019 hypoxemic Resp. Failure
38/52
Fungal Pneumonia Fungal infections are an unusual cause of CAP
inimmunocompetent patients but should be considered
in those with neutropenia, organ transplant, and HIV.
Cyptococcus is mostly asymptomatic and usually
discovered incidentally on CXR in normal patients. It
is usually symptomatic in immunocompromisedpatients. Histoplasma
proliferates in soil contaminated with
bird and bat droppings. Symptomatic patientspresent with
flu-like illness and radiographic
abnormalities such as bronchopneumonia andinterstitial
pneumonitis. Coccidioides typically presents with chest pain,
cough, and fever with a normal CXR in up to 50% ofpatients. It
is endemic in the deserts ofsouthwestern North America.
-
7/28/2019 hypoxemic Resp. Failure
39/52
PJP Infection in HIV Patients
Most common opportunistic infection in patientswith HIV.
Frequently presents as the first manifestation of
HIV infection. 75% of the population are infected by age 4.
The primary infection is asymptomatic andremains latent
throughout life unless the patient
becomes immunosuppressed. PJP does not occur until the CD4 count
falls
below 200 cells/mL.
-
7/28/2019 hypoxemic Resp. Failure
40/52
PJP Infection in HIV Patients
PJP is generally gradual n onset and characterized byfever,
cough, and progressive dyspnea andtachypnea.
The most common radiographic abnormalities are
diffuse, bilateral interstitial or alveolar infiltrates. Other
less common presentations include:
Pneumothoraces
Lobar infiltrates
Cysts Nodules
Pleural effusions
Infection is also associated with a high LDH.
-
7/28/2019 hypoxemic Resp. Failure
41/52
PJP Infection in HIV Patients
Unlike CAP, establishing the diagnosisbefore starting therapy is
important
PJP is less common and may have atypicalpresentation
Therapy may have complications such assteroids with undiagnosed
TB
BAL is the procedure of choice fordiagnosis with a yield of 97
to 100%
-
7/28/2019 hypoxemic Resp. Failure
42/52
-
7/28/2019 hypoxemic Resp. Failure
43/52
Diffuse Alveolar Hemorrhage
Hemoptysis is usually due from thebronchial circulation but DAH
causes
alveolar bleeding from injury to thealveolar-capillary
membrane.
Even severe DAH may not have
hemoptysis.
-
7/28/2019 hypoxemic Resp. Failure
44/52
Diffuse Alveolar Hemorrhage
One of three histological patterns may be seen:
Pulmonary capillaritis Neutrophillic infiltration of thealveolar
septa then capillary necrosis
Bland alveolar hemorrhage Characterized byhemorrhage into the
alveolar space withoutinflammation
Diffuse alveolar damage The underlying lesions ofARDS can
occasionally cause hemorrhage.
-
7/28/2019 hypoxemic Resp. Failure
45/52
Diffuse Alveolar Hemorrhage
The onset of DAH is often abrupt.
Hemoptysis can be absent at presentation in a
third of DAH cases. The CXR commonly demonstrates new patchy
or
diffuse alveolar opacities. Recurrent episodescan lead to
fibrosis.
BAL demonstrates progressive hemorrhagicreturn and hemosiderin
laden macrophages.
-
7/28/2019 hypoxemic Resp. Failure
46/52
-
7/28/2019 hypoxemic Resp. Failure
47/52
-
7/28/2019 hypoxemic Resp. Failure
48/52
Diffuse Alveolar Hemorrhage -Treatment
Steroids are the mainstay for DAH due tosystemic vasculitis,
collagen vascular disease
and isolated pulmonary capillaritis. Start with Solu-medrol
500-2000 mg daily for 5
days followed by gradual tapering andmaintenance on an oral
preparation.
Do not delay therapy, especially in the face ofrenal
dysfunction, as the renal injury is morelikely to be irreversible
than the lung disease.
-
7/28/2019 hypoxemic Resp. Failure
49/52
Diffuse Alveolar Hemorrhage -Treatment
Cyclophosphamide or azathioprine is addedbased on the response
to steroids or ifWegeners disease is the etiology.
Start with a single dose of 0.75 gm/m2 andfollow the WBC
Plasmapheresis is used in Goodpastures disease
although its role may expand in other vasculitis
syndromes Treatment for massive hemoptysis is covered in
a separate lecture
-
7/28/2019 hypoxemic Resp. Failure
50/52
Idiopathic Eosinophillic Pneumonia
Characterized by eosinophillic infiltration of thepulmonary
parenchyma.
The cause remains unknown but thought to be
an acute hypersensitivity reaction to anunidentified inhaled
antigen. Patients present with an acute febrile illness of