Embed Size (px)
Citation preview

HypothyroidismUpdate
2020
Michael T. McDermott MDDirector, Endocrinology and Diabetes Practice
University of Colorado Hospital
Disclosures
§ Michael T. McDermott MD is on an Advisory Board
for Novo Nordisk.
§ Any unlabeled/unapproved uses of drugs or
products referenced will be disclosed.
§ Explain the diagnostic tests for primary and central
hypothyroidism.
§ Discuss the clinical significance of overt and subclinical
hypothyroidism.
§ Review the management recommendations for hypothyroidism.
§ Discuss management strategies for patients who have persistent
symptoms while on biochemically adequate treatment.
Hypothyroidism Update 2020Learning Objectives

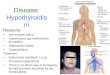
TRH
T3 + T4
Hypothalamus
TSH
Thyroid Hormone Regulation
T36 ug/d
T320 ug/d
T4101 ug/d
T326 ug/d
Pilo A, Am J Physiol 1990; 258:E715-26
Secretion Ratio T4:T3 = 14:1
Thyroid Hormone Production
D1
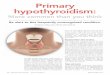
Screening / Case Finding
i TSH h TSH
TSH
Free T4Total T3
Free T4
Hyperthyroidism Hypothyroidism
Thyroid Function Testing
McDermott MT. Ann Intern Med 2009; 151 (11):ITC61McDermott MT. Ann Intern Med 2012; 157:ITC-1-14.

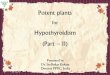
h TRH
Hypothalamus
h TSH
i T3 + i T4
h TSHFree T4 Low
h TSHFree T4 Normal
Overt
Primary Hypothyroidism
Subclinical
Mild Hypothyroidism
i TRH
Hypothalamus
i TSH
i T3 + i T4
TSH Low/NormalFree T4 Low
Central (Secondary) Hypothyroidism

HypothyroidismClinical Features
Symptom Frequency (1997)Dry Skin 76%Cold Intolerance 64%Coarse Skin 60%Puffy Eyelids 60%Weight Gain 54%Symptom Frequency (2014)Fatigue 81%Dry Skin 63%Shortness of Breath 51%
Zulewski H. J Clin Endocrinol Metab 1997; 82:771-776Carlé A. Eur J Endocrinol 2014;171:593-602
Number of hypothyroidism-associated symptoms reported by hypothyroid patients at disease onset and by their region-, age- and sex-matched controls
Carlé A. Eur J Endocrinol 2014;171:593-602
Thyroid Related Symptoms Common in Euthyroid Subjects
A 33 year old woman complains of fatigue and weight gain of 15 lbover the past 6 months. PMH: Type 1 Diabetes Mellitus Meds: Insulin Pump TherapyPE: BP 134/80 P 64 Ht 5’6’’ Wt 154 lb. (70 kg)Thyroid: firm, granular thyroid Eyes: periorbital edema Reflexes: delayed reflex relaxation
Lab: TSH 112 mU/L (nl: 0.45-4.5) Free T4 0.3 ng/ml (nl: 0.8-1.8)TPO antibodies 72.5 units (nl < 0.3)
Case 1
Which of the following to you recommend as starting therapy?A. Levothyroxine 112 mcg daily (1.6 mcg/kg)B. Levothyroxine 50 mcg dailyC. Levothyroxine 100 mcg daily plus Liothyronine 5 mcg BIDD. Desiccated thyroid extract 60 mg daily

Answer: A. Levothyroxine 112 mcg daily (1.6 mcg/kg)
Case 1
Levothyroxine (LT4) is the hypothyroidism treatment of choice; it effectively and safely relieves symptoms and normalizes laboratory tests in the majority of patients.
After absorption in the duodenum, circulating LT4 is converted to T3 by peripheral tissue deiodinases at a rate that is regulated by the metabolic needs of each organ and tissue. The long serum half-life of LT4 (5 days) yields stable TSH, T4, and T3 levels.
Average LT4 replacement dose in healthy adults with overt hypothyroidism: 1.6 mcg/kg/day. Lean body mass [approximate body weight that would yield a body mass index (BMI) of 24-25 kg/m2 for the individual’s height] is a better predictor of dose requirements than total body weight.
Jonklaas J, et al. Guidelines for the treatment of hypothyroidism: prepared by the American Thyroid Association Task Force on thyroid hormone replacement. Thyroid 2014; 24:1670-751.McDermott MT. In The Clinic: Hypothyroidism. Ann Intern Med 2020; (in press)
Primary HypothyroidismEtiology
Lymphocytic Thyroiditis (Hashimoto’s Thyroiditis)
ThyroidectomyI-131 AblationMedications:
§ Lithium§ Amiodarone§ Alpha Interferon§ Multi-Kinase Inhibitors § Immune Checkpoint Inhibitors
§ Levothyroxine: 1.6 mcg/kg QD
§ TSH Recheck: 6 Weeks
§ Dose Titration: TSH in Reference Range
Age < 60 Years and No CAD
Overt HypothyroidismTreatment
Jonklass J. Thyroid 2014; 24: 1670-1751 McDermott M. Ann Intern Med 2020; XX: ITC (in press)

Jonklass J, Thyroid 2014; 24: 1670-1751
Hypothyroidism GuidelinesATA 2014
Efficacy in resolving hypothyroid symptomsLong-term experience of its benefitsFavorable side effect profileGood intestinal absorptionEase of administrationLong serum half-lifeLow cost
Levothyroxine is Recommended as the Treatment of Choice
§ Take dose 1 hour before or 4 hours after a meal
§ Separate at least 4 hours from iron, calcium and soy
§ If you miss
§ One dose: take 2 pills the next day
§ Two doses: take 2 pills a day the next 2 days
McDermott M. Ann Intern Med 2020; XX: ITC (in press)
Levothyroxine Dosing Instructions
HO O CH2
NH2
C
H
I
C OH
OI
I
I
Thyroxine Structure
HO O CH2
NH2
C
H
I
C O-
OI
I
I
Levothyroxine Sodium
Na+

Optimal TSH Goal: 0.5-2.0 mU/L ?
Not Validated by Evidence
TSH Distribution in Normal Population
TSH Variation Within and Above Normal RangeEffect on Symptoms in Hypothyroid Subjects
Samuels MH. Effects of altering levothyroxine (LT4) doses on quality of life, mood and cognition in LT4 treated patients. J Clin Endocrinol Metab 2018; 103:1997-2008.
138 Patients: Hypothyroidism on LT4 Replacement
RCT: TSH Target Low Nl, High Nl or Slightly High x 6 months
Outcomes: Health Survey (SF-36), Quality of Life, Mood,
Cognition
TSH Variation Within and Above Normal RangeEffect on Symptoms in Hypothyroid Subjects
Outcomes - No Difference Among the 3 Groups
General Health (SF-36) Thyroid Related Quality of Life
Mood Cognition
138 Patients (RCT 6 Mos): Hypothyroidism on LT4 Replacement
Group (TSH) Low Nl High Nl Slightly High P
TSH Level (mU/L) 1.85 3.93 9.49 < .001
LT4 Dose (ug/kg) 1.50 1.32 0.78 < .001
Samuels MH. Effects of altering levothyroxine (LT4) doses on quality of life, mood and cognition in LT4 treated patients. J Clin Endocrinol Metab 2018; 103:1997-2008.

Evidence does not support targeting specific
TSH values within the normal reference range
Hypothyroidism Treatment GuidelinesATA/AACE 2012 and ATA 2014
Garber J, Endocr Pract 2012; 18:988-1028Jonklass J, Thyroid 2014; 24: 1670-1751
Optimal TSH Goal
This includes the following types of patients:Obese, Depressed, Athyreotic
A 72 year old woman complains of fatigue, mild depression andpoor memory that have been progressive over 3 years span.PMH: DJD, GERD Meds: ASA, H2 BlockerPE: BP 150/86 P 80 Ht 5’9” Wt 172 lb. (78 kg) Exam: normalLab: TSH 43.6 mU/L (nl: 0.45-4.5) Free T4 0.5 ng/dl (nl: 0.8-1.8)
Chol 255 TG 165 HDL 45 LDL 177
Case 2
Which of the following to you recommend as starting therapy?A. Levothyroxine 112 mcg daily (1.6 mcg/kg)B. Levothyroxine 50 mcg dailyC. Levothyroxine 100 mcg daily plus Liothyronine 5 mcg BIDD. Desiccated thyroid extract 60 mg daily
Answer: B. Levothyroxine 50 mcg daily
Case 2
Levothyroxine (LT4) is the hypothyroidism treatment of choice; it effectively and safely relieves symptoms and normalizes laboratory tests in the majority of patients.
After absorption in the duodenum, circulating LT4 is converted to T3 by peripheral tissue deiodinases at a rate that is regulated by the metabolic needs of each organ and tissue. The long serum half-life (5 days) of LT4 yields stable TSH, T4, and T3 levels.
Patients > 60 years old or with known CAD: start on low LT4 dose (25-50 mcg/day) with dose titrations of 12.5-25 mcg/day every 6-8 weeks until the goal TSH level is reached. “Start low, go slow” approach is recommended to prevent the development of dysrhythmias or ischemic events when full replacement doses are abruptly started or when the dose is increased too rapidly.
Jonklaas J, et al. Guidelines for the treatment of hypothyroidism: prepared by the American Thyroid Association Task Force on thyroid hormone replacement. Thyroid 2014; 24:1670-751.McDermott MT. In The Clinic: Hypothyroidism. Ann Intern Med 2020; (in press)

Age > 60 Years or CAD
Jonklass J. Thyroid 2014; 24: 1670-1751 McDermott M. Ann Intern Med 2020; XX: ITC (in press)
§ Levothyroxine: 25-50 mcg QD
§ TSH Recheck: 6 Weeks
§ Dose Titration: TSH in Reference Range
§ Age > 70: 4.0 < TSH < 6.0 mU/L
Overt HypothyroidismTreatment
Surks MI, J Clin Endocrinol Metab 2007; 92:4575-82
TSH Distribution Changes with Age
Hypothyroidism Treatment GuidelinesATA/AACE 2012 and ATA 2014
TSH Goals in the Elderly
Garber J, Endocr Pract 2012; 18:988-1028Jonklass J, Thyroid 2014; 24: 1670-1751
Based on the current evidence, it is reasonable to raise the target TSH to 4 – 6 mU/L in persons
greater than age 70 – 80 years

A 76 year old man complains of recent fatigue, weight gain anddecreased memory for current events.PMH: DM2, HTN Meds: Metformin, LisinoprilPE: BP 138/77 P 78 Ht 6’1” Wt 188 lb. (85 kg) Exam: normalLab: TSH 9.6 mU/L (nl: 0.45-4.5) Free T4 0.9 ng/dl (nl: 0.8-1.8)
Chol 212 TG 121 HDL 56 LDL 132
Case 3
Which of the following statements is true?A. Levothyroxine treatment will improve his symptomsB. Levothyroxine treatment will lower his LDL cholesterolC. Levothyroxine treatment will lower his CVD riskD. Levothyroxine treatment will reduce his mortality risk
Answer: B. Levothyroxine treatment will lower his LDL cholesterol
Case 3
LT4 treatment lowers LDL cholesterol levels in patients with subclinical hypothyroidism (SCH).
Patients with mild SCH do not experience symptom improvement with LT4 therapy if at baseline they have minimal symptoms and only slight TSH elevations. Two recent RCTs in elderly subjects > age 65 years and > age 80 years reported that LT4 treatment of mild SCH conferred no benefit for thyroid symptoms or fatigue and yielded secondary outcome improvement (BP, weight, waist circumference, grip strength). Treatment may benefit patients with more prominent baseline symptoms and when serum TSH levels are > 10 mU/L. Prospective, adequately powered RCTs have not yet been conducted to address whether LT4 treatment of SCH reduces the increased risk of CAD events and mortality that has been identified in the younger population. One cohort study reported a CVD benefit from LT4 treatment in younger patients but not in elderly subjects. Another study found that LT4 treatment of elderly subjects with SCH may even be associated with increased mortality.
References: next slide
Answer: B. Levothyroxine treatment will lower his LDL cholesterol
Case 3
McDermott MT. In The Clinic: Hypothyroidism. Ann Intern Med 2020; (in press). Peeters RP. Subclinical hypothyroidism. N Engl J Med 2017; 376:2556-65.Stott DJ. Thyroid hormone therapy for older adults with subclinical hypothyroidism. N Engl J Med 2017; 376:2534-44.Mooijaart SP. Association between levothyroxine treatment and thyroid related symptoms among adults aged 80 years and older with subclinical hypothyroidism. JAMA. 2019 Oct 30:1-11. doi: 10.1001/jama.2019.17274. [Epub ahead of print]Razvi S. Levothyroxine treatment of subclinical hypothyroidism, fatal and nonfatal cardiovascular events, and mortality. Arch Intern Med 2012; 172:811-7. Grossman A. Treatment with levothyroxine in subclinical hypothyroidism is associated with increased mortality in the elderly. Eur J Intern Med 2018; 50:65-68.

SubclinicalHypothyroidism
.01 0.45 4.5 10.0TSH mU/L
Free T4 ng/dl0.8 1.8
Mild Hypothyroidism
Subclinical HypothyroidismTreatment in Elderly Patients: TRUST Study
Subclinical Hypothyroidism: 737 Subjects > Age 65 TSH: 4.99-19.99 mU/L Free T4: in Reference RangeRCT: LT4 Rx (N=368) vs Placebo (N=369) x 1 Year
Primary Outcomes Hypothyroid Symptoms ScoreTiredness Score (Thyroid Related QOL Questionnaire)
Stott DJ. N Engl J Med 2017; 376:2534-44
Subclinical HypothyroidismTreatment in Elderly Patients: TRUST Study
Stott DJ. N Engl J Med 2017; 376:2534-44

Subclinical HypothyroidismTreatment in Elderly Patients: TRUST Study
Primary Outcome (1 Year) LT4 Placebo P
Hypothyroid Symptoms Score 16.6+16.9 16.7+17.5 0.99
Tiredness Score 28.7+20.2 28.6+19.5 0.40
Secondary Outcomes PBlood Pressure NSBody Mass Index NSWaist Circumference NSGrip Strength NSHyperthyroid Symptoms NS
Stott DJ. N Engl J Med 2017; 376:2534-44
Razvi S, J Clin Endocrinol Metab 2008; 93:2998-3007
Patients < 65 yrCVM Increased
Patients > 65 yrNo Increase CVM
Meta-Analysis (N = 15): 2,531 SCH Patients; 26,491 ControlsGroup 1: Included Patients < 65 years; Group 2: Only Patients > 65 years
Age < 65 vs > 65
Subclinical HypothyroidismCVD Mortality
4.5 10.0TSH mU/L
Subclinical HypothyroidismTreatment Recommendations
Clinical JudgmentRx Based on Symptoms
TreatmentRecommended
Age > 65: Controversy if Treatment Beneficial
Pregnant Women: Treat All to Trimester Specific Goals
Jonklass J, Thyroid 2014; 24: 1670-1751McDermott M. Ann Intern Med 2020; XX: ITC (in press)

Subclinical HypothyroidismTreatment
§ Levothyroxine: 25-50 mcg QD
§ TSH Recheck: 6 Weeks
§ Dose Titration: TSH in Reference Range
§ Age > 70: 4.0 < TSH < 6.0 mU/L
Jonklass J, Thyroid 2014; 24: 1670-1751McDermott M. Ann Intern Med 2020; XX: ITC (in press)

Reason for Dissatisfaction
Fatigue / Low Energy 75%
Body Weight Issues 70%
Memory Problems 55%
Mood Problems 45%
Other 35%
Satisfaction with Rx – Visual Analog (VA) Scale (1-10): 5 (mean)ATA Survey: 12,000 Respondents (95% Women)
Peterson SJ. Thyroid 2018;28:707-721
Persistent Symptoms on LT4 Therapy
Satisfaction with Doctor - VA Scale (1-10): 5-6 (mean)
Doctor Knowledgeable - VA Scale (1-10): 5-6 (mean)
How Often Have You Changed Doctors1-4 Times 45%5-10 Times 10%
Peterson SJ. Thyroid 2018;28:707-721
Persistent Symptoms on LT4 Therapy
Peterson S, McAninch E, Bianco A. J Clin Endocrinol Metab 2016; 101:4964-73
LT4 Patients Controls
(469) (469) P-Value
TSH (mU/L) 2.13 2.15 0.83
Free T3 (pg/ml) 2.85 3.01 < 0.001
Free T4 (ng/ml) 0.94 0.80 < 0.001FT3/FT4 Ratio 3.18 3.85 < 0.001
NHANES Survey
HypothyroidismAltered Circulating T3 / T4 Ratio on LT4 Therapy

LT4 Patients Controls
(469) (469) P-Value
BMI 29.8 28.2 < 0.001
Kcal Consumption 1761 1759 0.98
Physical Activity 41% 32% < 0.01Anti-Depressant Use 22% 15% < 0.01
Peterson S, McAninch E, Bianco A. J Clin Endocrinol Metab 2016; 101:4964-73
HypothyroidismAltered Circulating T3 / T4 Ratio on LT4 Therapy
552 Subjects GenotypedD2: Thr92Ala Homozygotes = 16%Thr92Ala: D2 instability loop related to ubiquitination
General Health Questionnaire: Thr92Ala HomozygotesBaseline: Worse GHQ (p = 0.03)
Panicker V, J Clin Endocrinol Metab 2009; 94:1623-9
LT4 / LT3 TherapySubjects: 697 Gender: 84%W Age: 18-75 Dx: HypothyroidDesign: RCT Double Blind x 52 WeeksDosing: (Usual LT4 – 50 ug) + LT4 50 ug
(Usual LT4 – 50 ug) + LT3 10 ug
General Health Questionnaire: Thr92Ala HomozygotesLT4/LT3 c/w LT4 Rx: Improved GHQ (p = 0.03)
Jonklass J, Thyroid 2014; 24: 1670-1751
Hypothyroidism Treatment GuidelinesATA 2014
No consistently strong evidence of superiority of LT4/LT3 combination therapy over LT4 alone.
Recommend against routine use of combination LT4/LT3 therapy.
Combination LT4/LT3 Therapy

Jonklass J, Thyroid 2014; 24: 1670-1751
Hypothyroidism Treatment GuidelinesATA 2014
Potential Safety Concerns of DTE:1. Supraphysiologic serum T3 levels.
2. Paucity of long-term safety outcome data.
Recommend against routine use of combination DTE therapy.
Desiccated Thyroid Extract Therapy
Jonklass J, Thyroid 2014; 24: 1670-1751McDermott M. Ann Intern Med 2020; XX: ITC (in press)
Combination LT4/LT3 Therapy
Desiccated Thyroid Extract Therapy
§ Some patients prefer combined LT4/LT3 or DTE
§ Reasonable to use in patients with persistent symptoms if
done safely (maintain TSH in reference range)
§ Optimal T4:T3 Ratio: 14:1 – 10:1
Hypothyroidism TreatmentPatients with Persistent Symptoms on LT4 Therapy
§ Lifestyle Measures (Sleep, Exercise, Diet, i Stress)
§ Medical Illness / Depression Management
§ Regular Follow-up and Support
§ May Consider Combination T4/T3 or DTE
§ Levothyroxine (T4) + Liothyronine (T3) (10:1 ratio)
§ Desiccated Thyroid Extract (Porcine Thyroid)
§ Maintain TSH within Reference Range
Hypothyroidism TreatmentPatients with Persistent Symptoms on LT4 Therapy

Ott J, Thyroid 2011; 21:161-7
426 Euthyroid Women with Goiter: Thyroidectomy
TPO Ab Pos TPO Ab Neg P
TSH mU/L 1.7 1.5 NS
Symptom 6.7 + 2.5* 4.1 + 2.8 < .001Score
Symptoms Associated with TPO AntibodiesFatigue, Irritability, Nervousness, Dry Hair,
Lower Quality of Life
Chronic Lymphocytic ThyroiditisAre Some Symptoms Independent of Thyroid Hormone Levels?
Guldvog I. Ann Intern Med 2019; 170:453-64
150 Patients with Hashimoto’s Thyroiditis (age: 18-79 years):
persistent symptoms, euthyroid on thyroid hormone replacement
therapy with serum anti-TPO titers > 1000 IU/ml.
RCT: Thyroidectomy vs Thyroid Hormone Therapy x 18 months
Primary Outcome: General Health Score (SF-36) at 18 monthsSecondary Outcomes: Adverse Surgery Affects, 7 SF-36 sub-
scores, fatigue scores, anti-TPO titers (6, 12, 18 months)
Thyroidectomy for Hashimoto’s Thyroiditis
Serum Anti-TPO Antibody Titer
Thyroidectomy for Hashimoto’s Thyroiditis
Individual Data
Mean Data
Guldvog I. Ann Intern Med 2019; 170:453-64

Thyroidectomy for Hashimoto’s Thyroiditis
Surgery Medical Rx
Before After (1 yr) After (1 yr) P
General Health (SF36) 38 64 37 < 0.001
Fatigue Score 23 15 23 < 0.001
Chronic Fatigue (%) 83 33 73 < 0.001
Guldvog I. Ann Intern Med 2019; 170:453-64
§ TSH - best test to detect hypothyroidism
§ Hashimoto’s Thyroiditis is the most common cause
§ Treat hypothyroidism with LT4 to normalize TSH
§ TSH goal for elderly can be 4.0-6.0 mU/L
§ Mild hypothyroidism increases CVD risk/mortality in
patients < 65 years old but not > 65 years old
§ Treatment of patients with persistent symptoms
requires an individualized approach
Hypothyroidism Update 2020Summary
Thank You