Embed Size (px)
Citation preview
www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1 1
Seminar
HypothyroidismLayal Chaker, Antonio C Bianco, Jacqueline Jonklaas, Robin P Peeters
Hypothyroidism is a common condition of thyroid hormone deficiency, which is readily diagnosed and managed but potentially fatal in severe cases if untreated. The definition of hypothyroidism is based on statistical reference ranges of the relevant biochemical parameters and is increasingly a matter of debate. Clinical manifestations of hypothyroidism range from life threatening to no signs or symptoms. The most common symptoms in adults are fatigue, lethargy, cold intolerance, weight gain, constipation, change in voice, and dry skin, but clinical presentation can differ with age and sex, among other factors. The standard treatment is thyroid hormone replacement therapy with levothyroxine. However, a substantial proportion of patients who reach biochemical treatment targets have persistent complaints. In this Seminar, we discuss the epidemiology, causes, and symptoms of hypothyroidism; summarise evidence on diagnosis, long-term risk, treatment, and management; and highlight future directions for research.
IntroductionHypothyroidism refers to the common pathological condition of thyroid hormone deficiency. If untreated, it can lead to serious adverse health effects and ultimately death. Because of the large variation in clinical presentation and general absence of symptom specificity, the definition of hypothyroidism is predominantly biochemical. Overt or clinical primary hypothyroidism is defined as thyroidstimulating hormone (TSH) concentrations above the reference range and free thyroxine concentrations below the reference range. Mild or subclinical hypothyroidism, which is commonly regarded as a sign of early thyroid failure, is defined by TSH concentrations above the reference range and free thyroxine concentrations within the normal range. Subclinical hypothyroidism has been reviewed in a previous Lancet Seminar1 and is therefore not the focus here.
Whether the existing reference ranges of TSH and free thyroxine should be used to define thyroid dysfunction is a matter of debate. This issue is of clinical importance because the reference ranges are generally used as a threshold for treatment. Thyroid hormone replacement with levothyroxine is the standard treatment for patients with hypothyroidism. However, a substantial proportion of patients treated with levothyroxine have persistent complaints despite reaching the biochemical therapy targets, which has prompted the question of whether levothyroxine treatment is sufficient for all patients or whether alternative therapies (eg, combination with liothyronine preparations) could be adopted. Hypothyroidism in children and pregnant women are considered separate topics and have been discussed elsewhere.2,3
EpidemiologyPrevalence and risk factorsThe prevalence of overt hypothyroidism in the general population varies between 0·3% and 3·7% in the USA and between 0·2% and 5·3% in Europe,4–8 depending on the definition used. A metaanalysis7 of studies across nine European countries estimated the prevalence of undiagnosed hypothyroidism, including both overt and
mild cases, at around 5%. Differences in iodine status affect the prevalence of hypothyroidism, which occurs more frequently both in populations with a relatively high iodine intake and in severely iodinedeficient populations.9,10 Hypothyroidism occurs more frequently in women, in older people (>65 years), and in white individuals, although data on ethnic differences are scarce.5,11,12 Hypothyroidism is more common in patients with autoimmune diseases, such as type 1 diabetes, auto immune gastric atrophy, and coeliac disease, and can occur as part of multiple autoimmune endocrinopathies. Individuals with Downs’ syndrome or Turners’ syndrome have an increased risk of hypothyroidism. By contrast, tobacco smoking and moderate alcohol intake are associated with a reduced risk of hypothyroidism.13,14
Genetic epidemiologyThe heritability of TSH and free thyroxine concentrations in serum is estimated to be 65% and 23–65%, respectively.15,16 Results from genomewide association studies have so far explained only a small proportion of thyroid function variability,17 and only three studies18–20 have focused on hypothyroidism specifically. The loci most consistently implicated in hypothyroidism include autoimmunityrelated genes and thyroidspecific regulatory genes (panel). Most of these loci are also associated with serum TSH concentrations within the reference range.17 Monogenetic disorders leading to congenital hypothyroidism are rare and include TSH
Published Online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1
Academic Centre for Thyroid Disease, Erasmus University Medical Centre, Rotterdam, Netherlands (L Chaker MD, Prof R P Peeters MD); Division of Endocrinology and Metabolism, Rush University Medical Center, Chicago, IL, USA (Prof A C Bianco MD); and
Division of Endocrinology, Georgetown University, Washington, DC, USA (J Jonklaas MD)
Correspondence to: Prof Robin P Peeters, Academic Centre for Thyroid Disease, Erasmus University Medical Center, Rotterdam 3000 CA, Netherlands [email protected]
Search strategy and selection criteria
We searched Embase, MEDLINE, and the Cochrane database between Jan 1, 2000 and Sept 22, 2016, for articles published in or translated into English. The full search and search terms are provided in the appendix. We mainly selected publications from the past 3 years, but did not exclude commonly referenced and highly regarded older publications. We also searched the reference lists of articles identified by this search and selected those we judged relevant. We supplemented the search with mainly older records from personal files. Review articles are cited to provide additional details and references.

Seminar
2 www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1
resistance (due to an inactivating mutation in the TSH receptor), thyroid dysgenesis, and thyroid dyshormonogenesis.21
CausesHypothyroidism can be classified as primary (due to thyroid hormone deficiency), secondary (due to TSH deficiency), tertiary (due to thyrotropinreleasing hormone deficiency), and peripheral (extrathyroidal; panel). Central hypothyroidism (including both secondary and tertiary) and peripheral hypothyroidism are rare and account for less than 1% of cases.22
Primary hypothyroidismIn iodinesufficient areas, the most common cause of hypothyroidism is chronic autoimmune thyroiditis (also known as Hashimoto’s disease). High concentrations of antithyroid antibodies (predominantly thyroid peroxidase antibodies and antithyroglobulin antibodies) are present in most patients with autoimmune thyroiditis. Raised concentrations of thyroid peroxidase antibodies are also detected in about 11% of the general population.8 In patients with subclinical hypothyroidism, thyroid
peroxidase antibody measurements help to predict progression to overt disease.23,24 The exact mechanisms underlying autoimmune thyroiditis are not known, but both genetic and environmental factors are involved. A higher genetic risk score—calculated using five genetic variants for thyroid peroxidase antibodies identified by genomewide association studies—showed a graded association with higher TSH concentrations and clinical hypothyroidism.25,26 Smokers have lower thyroid peroxidase antibody concentrations than nonsmokers, and incidence of autoimmune thyroiditis increases after smoking cessation.27,28 Other environmental factors implicated in autoimmune thyroiditis are vitamin D and selenium deficiency, and moderate alcohol intake.29
Iodine is an essential component of thyroid hormone. Iodine deficiency can result in goitre, thyroid nodules, and hypothyroidism. The most severe consequence of iodine deficiency is cretinism (ie, restricted mental and physical development in utero and during childhood). Iodine fortification programmes are one of the safest and cheapest public health interventions for the prevention of cognitive and physical impairment.30,31 Despite such efforts, suboptimal iodine status still affects large parts of Africa and Asia, as well as specific subpopulations in several highincome countries—most notably, pregnant women in some areas of Italy, USA, and the UK.31–33 In populations that shift from severe to mild iodine deficiency, the prevalence of hypothyroidism decreases; in populations shifting from mild deficiency to optimum or excessive intake of iodine, the prevalence of autoimmune hypothyroidism increases.34,35
Iodinecontaining drugs (eg, amiodarone) can restrict thyroid hormone production through iodine overload, immediately blocking thyroid hormone synthesis (ie, WolffChaikoff effect). About 14% of patients treated with amiodarone develop hypothyroidism.36 Lithium also causes hypothyroidism via effects on thyroid hormone synthesis and release.37 In a large populationbased cohort study,38 6% of patients needed levothyroxine therapy within 18 months of starting lithium treatment. Tyrosine kinase inhibitors are used as targeted therapy for several cancers. An analysis of clinical reports from the US Food and Drug Administration Adverse Event Reporting System,39 found that patients who received sunitinib developed hypothyroidism more frequently than patients treated with sorafenib. Several other drugs—including interferonalfa, thalidomide, some monoclonal antibodies, antiepileptic drugs, and drugs for secondline treatment of multidrugresistant tuberculosis—can also cause primary hypothyroidism (panel).
Hypothyroidism is common after radioiodine treatment, after hemithyroidectomy, and after neck radiation or surgery for cancer therapy.40–44 In the long term, about 80% of patients with Grave’s disease who are treated with radioiodine will develop hypothyroidism, even when low doses are used. Hypothyroidism is reported to occur in
Panel: Causes of hypothyroidism
Primary hypothyroidism• Chronicautoimmunethyroiditis(alsoknownasHashimoto’sthyroiditis)• Iodine—severeiodinedeficiency,mildandsevereiodineexcess• Drugs—eg,amiodarone,lithium,tyrosinekinaseinhibitors,interferon-alfa,
thalidomide, monoclonal antibodies (eg, ipilimumab and nivolumab), antiepileptic drugs (eg, valproate), drugs for second-line treatment of multidrug-resistant tuberculosis
• Iatrogenic—radioiodinetreatment(eg,forGraves’diseaseortoxicnodulardisease),hemithyroidectomy, radiotherapy or surgery in the neck or head region
• Transientthyroiditis—viral(DeQuervain’ssyndrome),post-partum,silentthyroiditis,destructive thyroiditis
• Thyroidglandinfiltration*—infectious(eg,mycoplasma),malignant(eg,thyroidmalignancy, lymphoma, metastasis of malignancy elsewhere), autoimmune (eg,sarcoidosis),inflammatory(eg,Riedels’sthyroiditis)
• Genetic*—autoimmunity-relatedgenes(eg,HLAclassIregion,PTPN22, SH2B3, and VAV3), general and thyroid-specific genes (eg, FOXE1, ATXN2, and PDE8B)
Central hypothyroidism• Pituitarytumours(secretingornon-secreting)• Pituitarydysfunction(eg,Sheehan’ssyndrome)• Hypothalamicdysfunction(eg,post-traumatic)• Resistancetothyroid-stimulatinghormone(TSH)orthyrotropin-releasinghormone• Drugs(eg,dopamine,somatostatins,glucocorticosteroids,andretinoidX
receptor selective ligands)• IncreasedTSHconcentrationduetoleptinstimulation†
Peripheral (extra-thyroidal) hypothyroidism• Consumptivehypothyroidism• Tissue-specifichypothyroidismduetodecreasedsensitivitytothyroidhormone
(eg, mutations in MCT8 [also known as SLC16A2], SECISBP2, THRA, THRB)
*Rarecausesofprimaryhypothyroidism.†Evidencemainlyfromanimalmodels.

Seminar
www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1 3
55% of patients treated for toxic nodular goitre40 and about 8% of patients treated for solitary toxic nodules.45 In a metaanalysis43 of 32 studies, 20% of patients developed hypothyroidism after hemithyroidectomy. Other causes of primary hypothyroidism include transient thyroiditis and infiltrative disease (panel).
Central hypothyroidismCentral hypothyroidism is rare and affects both sexes equally. It is more often associated with pituitary than hypothalamic disorders but frequently involves both.22 Biochemically, central hypothyroidism is defined by low or lowtonormal TSH concentrations and a disproportionately low concentration of free thyroxine. Occasionally, TSH concentration is mildly elevated, probably because of decreased bioactivity.46 Over half of central hypothyroidism cases are caused by pituitary adenomas.22 Other causes of central hypothyroidism include pituitary or hypothalamic dysfunction due to head trauma, pituitary apoplexy, Sheehan’s syndrome, surgery, radiotherapy, genetic, and infiltrative disease. Several drugs are known to affect the hypothalamic–pituitary–thyroid axis (panel).47,48
Peripheral hypothyroidismConsumptive hypothyroidism is caused by aberrant expression of the deiodinase 3 enzyme (which inactivates thyroid hormone) in tumour tissues. Although very rare, such overexpression can induce severe hypothyroidism. Elevated concentration of deiodinase 3 was first described in a newborn baby with infantile hepatic haemangiomatosis, but can also occur in patients with vascular and fibrotic tumours and gastrointestinal stromal tumours.49 Patients with rare genetic syndromes that lead to a reduced sensitivity to thyroid hormone (panel) usually have normal TSH concentrations, but can also present with tissuespecific hypothyroidism.50
Clinical presentation and implicationsMyxedema coma and severe hypothyroidismThe clinical manifestations of hypothyroidism range from life threatening—in the case of myxedema coma—to no signs or symptoms. Myxedema coma, which was first described in the late 1900s as an outcome of longstanding untreated and severe hypothyroidism, has become a rare condition. Nevertheless, because the disease course is striking, with mortality of 40% despite treatment, early recognition is vital.51 Myxedema coma leads to an altered mental status, hypothermia, progressive lethargy, and bradycardia and can eventually result in multiple organ dysfunction syndrome and death. Therefore, early initiation of thyroid hormone therapy and other supportive measures is crucial.52
Although very rare, severe primary hypothyroidism can lead to pituitary hyperplasia with concomitant pituitary pathology (eg, secondary adrenal insufficiency) and symptoms (eg, amenorrhoea).53
Signs and symptomsThe most common symptoms of hypothyroidism in adults are fatigue, lethargy, cold intolerance, weight gain, constipation, change in voice, and dry skin, but the clinical presentation can include a wide variety of symptoms that differ with age, sex, and time between onset and diagnosis (table 1).54,55 The symptoms for the diagnosis of hypothyroidism are nonspecific, especially in elderly patients who present with fewer and less classic signs and symptoms than younger individuals.55 An increase in the severity of symptoms might predict hypothyroidism, since a change in seven or more symptoms in the past year increases the likelihood of hypothyroidism (likelihood ratio 8·7).56 However, in a casecontrol study,57 none of 34 hypothyroidismrelated symptoms could be used to identify patients with hypothyroidism. Furthermore, 15% of patients with autoimmune hypothyroidism are asymptomatic or report only one hypothyroidismassociated symptom, whereas 70% of euthyroid controls have one or more thyroidassociated complaints.57
Hypothyroidism has clinical implications related to nearly all major organs (table 1), but the cardiovascular system is the most robustly studied. Hypothyroidism results in increased vascular resistance, decreased cardiac output, decreased left ventricular function, and changes in several other markers of cardiovascular contractility.
Presentation Signs and implications
Generalmetabolism
Weight gain, cold intolerance, fatigue
Increase in body-mass index, low metabolic rate, myxedema*,hypothermia*
Cardiovascular Fatigue on exertion, shortness of breath
Dyslipidaemia, bradycardia, hypertension, endothelial dysfunctionorincreasedintima–mediathickness*,diastolicdysfunction*,pericardialeffusion*,hyperhomocysteinemia*,electrocardiogramchanges*
Neurosensory Hoarsenessofvoice,decreased taste, vision, or hearing
Neuropathy, cochlear dysfunction, decreased olfactory and gustatory sensitivity
Neurological and psychiatric
Impaired memory, paresthesia, mood impairment
Impaired cognitive function, delayed relaxation of tendonreflexes,depression*,dementia*,ataxia*,Carpal tunnel syndrome and other nerve entrapment syndromes*,myxedemacoma*
Gastrointestinal Constipation Reduced oesophageal motility, non-alcoholic fatty liver disease*,ascites(veryrare)
Endocrinological Infertility and subfertility, menstrual disturbance, galactorrhoea
Goiter,glucosemetabolismdysregulation,infertility,sexual dysfunction, increased prolactin, pituitary hyperplasia*
Musculoskeletal Muscle weakness, muscle cramps, arthralgia
Creatinephosphokinaseelevation,Hoffman’ssyndrome*,osteoporoticfracture*(mostprobablycaused by overtreatment)
Haemostasisandhaematological
Bleeding, fatigue Mildanaemia,acquiredvonWillebranddisease*,decreasedproteinCandS*,increasedredcelldistributionwidth*,increasedmeanplateletvolume*
Skin and hair Dry skin, hair loss Coarseskin,lossoflateraleyebrows*,yellowpalmsofthehand*,alopeciaareata*
Electrolytes and kidney function
Deterioration of kidney function
Decreased estimated glomerular filtration rate, hyponatraemia*
*Uncommonpresentation.
Table 1: Clinical presentation and implications of hypothyroidism

Seminar
4 www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1
Myocardial injuries and pericardial effusions are more common in patients with hypothyroidism than in matched euthyroid controls.58 Furthermore, patients with hypothyroidism have a higher prevalence of cardiovascular risk factors and often have features of metabolic syndrome, including hypertension, increased waist circumference, and dyslipidaemia.59 Hypothyroidism also increases total cholesterol, lowdensity lipoprotein, and homocysteine concentrations.
Patients with acute hypothyroidism, in the context of thyroid cancer treatment, show a decline in mood and quality of life.60 Hypothyroidism is considered a cause of reversible dementia; however, how often this occurs and in what proportion of patients dementia is truly reversible is unclear.61 Other manifestations include neurosensory, musculoskeletal, and gastrointestinal signs and symptoms (table 1). Because of the pleiotropic effects of thyroid hormone, hypothyroidism can also affect the course of other disorders. For example, statin intolerance is more prevalent in individuals with hypothyroidism than in controls without hypothyroidism.62
Long-term outcomesMost longterm consequences of hypothyroidism have been studied in the context of subclinical hypothyroidism, because overt hypothyroidism is generally treated. Few studies63–65 have investigated the association of hypothyroidism with allcause mortality and results are mainly available for subclinical hypothyroidism. Results from a populationbased followup study65 of 599 participants aged 85 years suggested that, in elderly populations, subclinical hypothyroidism might be associated with better survival than euthyroidism or suppressed TSH. However, this finding was not confirmed in a large individual participantbased meta
analysis63 that included more than 2500 participants (aged >80 years). This metaanalysis63 showed an increased risk of coronary heart disease events and mortality in those with higher TSH concentrations, particularly those with TSH concentrations above 10 mIU/L. However, the association between hypothyroidism and coronary artery disease has been recognised for a long time.66 Subclinical hypothyroidism with TSH concentrations above 10 mIU/L has also been associated with an increased risk of heart failure.63,67 Patients with hypothyroidism undergoing percutaneous coronary intervention have more major adverse cardiovascular and cerebral events than those with normal thyroid function and those with adequately treated hypothyroidism.68 By contrast, the association with stroke is less evident and might be apparent only in younger individuals (<65 years).69 Patients with hypothyroidism have fewer neurological deficits poststroke than controls without elevated TSH concentrations;70 normally after a stroke localised hypothyroidism is observed as a result of deiodinase 3 induction in the ischaemic brain area.71,72 The risk of coronary heart disease in patients with subclinical hypothyroidism does not differ by thyroid peroxidase antibody concentrations, suggesting that autoimmunity per se is not a contributing factor to the association.73 Hypothyroidism can present with cognitive impairments and dementia but the association is controversial, because results from several populationbased cohort studies74–77 showed a protective effect of elevated TSH concentrations on the risk of dementia.
Hypothyroidism has also been associated with nonalcoholic fatty liver disease, cancer mortality, arthritis, kidney dysfunction, and diabetes; however, in most cases causality is suggested but not proven.78–82
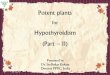
DiagnosisPrimary hypothyroidism is defined by TSH concentrations above the reference range (most commonly used 0·4–4·0 mIU/L) and free thyroxine concentrations below the reference range, which is dependent on the type of assay used and the population studied (figure 1). The US Preventive Service Task Force83 has suggested reserving the term overt hypothyroidism for cases in which patients present with symptoms. However, such a definition is challenging in practice because of the large variability in presentation of even severe hypothyroidism. Additionally, patients might recognise previous symptoms only after the initiation of levothyroxine treatment.
TSH has circadian fluctuations, with higher concentrations towards the evening. Patients with severe hypothyroidism show irregularity of TSH secretion.84 Seasonal variations have also been described, with higher TSH concentrations in winter and spring than in autumn and summer.85 No indications exist for routine measurement of total triiodothyronine, total thyroxine, or free triiodothyronine. Measurement of thyroid peroxidase
Suspected hypothyroidism→ Measure TSH. Measure free thyroxine if TSH elevated or if
suspicion of disorders other than primary hypothyroidism→ Diagnosis based on two measurements
Indication for treatment→ Treat with 1·5–1·8 μg per kg of levothyroxine and initiate
with full dose → Start with 12·5–25·0 μg per day of levothyroxine in patients
with cardiac symptoms and elderly patients with many comorbidities
→ Inform women of childbearing age about the 30% increase in dose required once pregnant
→ Repeat TSH measurement after 4–12 weeks and then every 6 months when stable
Treatment targets not reached→ Consider reasons for treatment
failure
Treatment targets reached→ Annual serum TSH measurement
Figure 1: Diagnosis and treatment of primary hypothyroidismTSH=thryoid-stimulatinghormone.

Seminar
www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1 5
antibody is not strictly necessary to diagnose hypothyroidism but is useful to affirm the diagnosis of autoimmune primary hypothyroidism. Hypothyroidism is often characterised by a hypoechogenic pattern on thyroid sonography, even in the absence of raised thyroid peroxidase antibody concentrations. However, in the absence of additional clinical indications, such as abnormal thyroid palpation, an ultrasound is not required.
Reference ranges of thyroid function testsMost commercially available TSH and free thyroxine assays are immunoassays, and their reference ranges are statistically defined as between the 2·5th and 97·5th percentile in an apparently healthy population. Therefore, the reference ranges do not consider symptoms or the risk of adverse events or disease, which is demonstrated by studies showing an increased risk of adverse events with variations in thyroid function even within these reference ranges.76,86–89 Furthermore, the reference ranges differ with age, sex, and ethnic origin.90 The applied reference ranges for thyroid function have been a matter of debate in recent years.91,92 The upper
limit of TSH reference ranges typically increases with age in adults, and agespecific reference ranges gave conflicting results in younger individuals in studies from the UK and Australia.93,94 Nevertheless, in both studies,93,94 the use of agespecific reference ranges led to a reclassification from abnormal to normal thyroid function predominantly in older individuals. Little information exists about the consequences of treatment and thus no convincing arguments have been put forward to change the applied reference ranges.
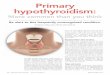
Conditions that interfere with diagnosisSeveral conditions can interfere with the laboratory measurements of thyroid analytes. Interference should be suspected when thyroid function tests do not match the clinical presentation (figure 2). Human antianimal antibodies in patient’s serum can cause falsely high TSH concentrations and can interfere with free thyroxine equilibrium dialysis platform assays. Heparin, including lowmolecularweight heparin, can lead to falsely elevated concentrations of free thyroxine.95 High intake of biotin, a popular overthecounter supplement, can interfere
Increased TSH
Decreased free thyroxine
Normal free thyroxine
Increased free thyroxine
Common reasons• Autoimmune hypothyroidism• Iodine severe deficiency or relative excess• Postradioiodine or thyroidectomy• Drugs (eg, amiodarone, lithium)
Less common reasons• Postradiation of head or neck• Thyroid infiltration• Consumptive hypothyroidism
Common reasons• Subclinical hypothyroidism• Assay interference
Less common reasons• Drugs• Post non-thyroidal illness• TRH or TSH resistance syndrome• Adrenal insufficiency
Common reasons• Non-adherence to therapy• Central hyperthyroidism (eg, pituitary adenoma)• Assay interference• Levothyroxine taken shortly before blood sampling
Less common reasons• Drugs (eg, heparin)• Post non-thyroidal illness• Thyroid hormone resistance
Normal TSH
Decreased free thyroxine
Normal free thyroxine
Increased free thyroxine
Common reasons• Central hypothyroidism• Assay interference
Less common reasons• TSH deficiencies
Euthyroidism
Common reasons• Overtreatment*• Drugs• Assay interference• Levothyroxine taken shortly before blood sampling
Less common reasons• Non-thyroidal illness• TSH-secreting pituitary adenoma• Thyroid hormone metabolism disorders• Thyroid hormone disorders
Figure 2: Interpretation of thyroid function tests associated with hypothyroidismTSH=thryoid-stimulatinghormone.TRH=thyrotropin-releasinghormone.*TSHcanalsobesuppressed.

Seminar
6 www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1
with biotinbased hormone assays, leading to false results of thyroid function tests.
Free thyroxine measurement is important to the diagnosis of hypothyroidism (eg, central hypothyroidism) and during followup and treatment. The accuracy of free thyroxine immunoassays has been questioned in conditions that affect binding protein concentrations (ie, albumin or thyroxinebinding globulin), such as pregnancy or acute illness. However, free thyroxine assays generally perform well in daily clinical practice. Free thyroxine measured by liquid chromatography–tandem mass spectrometry seems to perform better than immunoassays in certain clinical conditions, such as acute illness and pregnancy,96 but is not available in most healthcare facilities.
Independent of measurement artifacts, severe illness is characterised by low thyroid hormone status, but TSH concentration is generally within the normal range, although it can be transiently increased during recovery from a nonthyroidal illness.97 Changes in thyroid hormone metabolism, thyroid hormone transporters, and thyroid hormone receptors all have a role in the pathophysiology of nonthyroidal illness. Nonthyroidal illness occurs in different disease states, but is present in almost all critically ill patients.97 Thyroid function testing should therefore not be done in these patients, unless thyroid disease or central hypothyroidism is suspected. No evidence exists that thyroid hormone replacement therapy is beneficial in critically ill patients.
ScreeningDespite the high prevalence of hypothyroidism, easy diagnostics, and cheap treatment, no consensus has been reached about TSH screening in specific subgroups of the general population. Several organisations—including the American Thyroid Association, American Association of Clinical Endocrinologists, and the Latin American Thyroid Society—recommend screening above a particular age (ranging from every 5 years for individuals aged >35 years to periodically for those aged ≥60 years), especially in women.98,99 The US Preventive Services Task Force83 found no evidence for or against screening, whereas the UK Royal College of Physicians100 suggests that screening of the general population is unjustified. However, evidence98 does support case finding in patients with dementia, infertility, autoimmune diseases, hypercholesterolaemia, dysmenorrhoea, or a family history of autoimmune hypothyroidism, in patients taking amiodarone or lithium, or in those at risk of iatrogenic hypothyroidism (eg, after neck radiation).
TreatmentLevothyroxine monotherapy in solid formulation, taken on an empty stomach, is the treatment of choice. The presence of clinical features of hypothyroidism, with biochemical confirmation of overt hypothyroidism, is the indication for treatment initiation. No rationale
exists for avoiding the prescription of generic preparations, but switches between levothyroxine products in patients who are stable are not recommended.101 The optimal daily dose in overt hypothyroidism is 1·5–1·8 μg per kg of bodyweight.101–103 In patients with coronary artery disease, the starting dose is generally 12·5–25·0 μg per day and should be gradually increased on the basis of symptoms and TSH concentrations.101 This regimen is often preferred in the elderly, especially in patients with many comorbidities.101,102 In younger patients without comorbidities, the full dose can usually be given from the start with adequate monitoring to avoid overtreatment. After the initiation of therapy, TSH measurement is repeated after 4–12 weeks and then every 6 months and, once stabilised, annually. Adjustments should be made according to laboratory findings, keeping in mind that in some patients (ie, those with low bodyweight or older patients) small changes in dose can have substantial effects on serum TSH concentrations. The clinical significance of low triiodothyronine concentrations in some patients despite reaching normal TSH concentrations is unknown. Routine measurement of triiodothyronine should not be used to assess treatment effectiveness.104
Women of childbearing ageBecause of physiological changes during pregnancy, an increase in levothyroxine dose is required to maintain euthyroidism.105 Therefore, women of childbearing age with levothyroxinetreated hypothyroidism should be informed to increase their dose by 30% once pregnant and directly contact their physician for further guidance.106 Screening, the definition of subclinical hypothyroidism, and potential treatment during pregnancy are beyond the scope of this Seminar.107,108
Treatment targetsTreatment targets include normalisation of TSH concentrations and resolution of physical and mental complaints, while avoiding undertreatment or overtreatment.101 Nevertheless, an estimated 35–60% of patients treated with levothyroxine do not reach the target range of TSH (either overtreated or undertreated).109,110 Results from a retrospective cohort study in the UK109 showed that, after 5 years of levothyroxine therapy, almost 6% of patients have TSH concentrations below 0·1 mIU/L and more than 10% have TSH concentrations above 10·0 mIU/L. Overtreatment (ie, iatrogenic subclinical or overt hyperthyroidism) can have deleterious health effects, such as atrial fibrillation and osteoporosis, and should always be avoided, especially in the elderly and postmenopausal women. Undertreatment (ie, persistent thyroid hormone deficiency) can result in an increased risk of cardiovascular disease and persistent signs and symptoms. Treatment targets for central hypothyroidism are different from primary

Seminar
www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1 7
hypothyroidism because clinicians cannot rely on the socalled reflex TSH strategy. Further information on the treatment of central hypothyroidism can be found elsewhere.22
Failure to reach treatment targetsFactors that prevent patients from reaching therapy targets include prescription or intake of inadequate doses, interaction with supplements or medication, concurrent medical conditions, and nonadherence to therapy (table 2). Lower levothyroxine doses are needed to suppress TSH secretion in the elderly and higher doses are needed after thyroidectomy. Levothyroxine treatment and therapy targets in the context of thyroid malignancy are beyond the scope of this Seminar.
Levothyroxine is absorbed in the small intestine and intake is advised in the morning 30–60 min before breakfast. Intake before bedtime (2–3 h after last meal) might improve absorption and can be considered to increase compliance.111 Several drugs can interfere with the absorption, availability, or metabolism of levothyroxine, although evidence for some of these preparations comes from nof1 trials. Gastrointestinal conditions that reduce levothyroxine absorption include Helicobacter pylori gastritis, coeliac disease, and
autoimmune atrophic gastritis. Results from some studies112,113 suggest that liquid and soft gel formulations of levothyroxine do not depend on gastric pH for absorption, and could provide a solution for patients with difficulties ingesting levothyroxine 30–60 min before breakfast. In a doubleblind randomised crossover trial114 of liquid thyroxine in 77 treatmentnaive patients with hypothyroidism, no significant differences in thyroid function tests were seen when the liquid preparation was ingested at breakfast or 30 min before breakfast. However, no studies have compared liquid gel formulations of levothyroxine with solid formulations in relation to clinical outcomes.
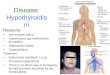
For individuals in whom high TSH concentrations persist and other causes have been excluded, the possibility of nonadherence, a common cause of therapy failure, should be considered and discussed with the patient. High TSH concentrations with normal or highnormal free thyroxine concentrations can be a result of levothyroxine tablets taken shortly before blood sampling. A supervised thyroxine absorption test to distinguish nonadherence from other reasons for undertreatment should be considered. Figure 3 shows a suggested protocol that combines both acute and longterm supervised administration.115,116
Recommendations
Elevated TSH with or without (persistent) symptoms
Inadequate dose Consider higher doses, especially in patients with no remaining functional thyroid capacity(eg,aftertotalthyroidectomyorradioablationtherapyforGraves’disease)
Simultaneous intake of levothyroxine with food can impair absorption Intake 30–60 min before breakfast or at bedtime (2–3 h after evening meal); discuss patient preference
Somedrugscanaffectlevothyroxineabsorption—eg,calciumcarbonate*,ferroussulfate*,protonpumpinhibitors,aluminiumcontaining antacid, sucralfate, and orlistat
Separate intake of levothyroxine from interfering medications and supplements (eg, 4 h)
Somedrugscanaffectlevothyroxineavailabilityandrequirement—eg,oestrogens,androgens,sertraline,phenobartbital†,carbamazepine,phenytoin, and rifampicin
MonitorTSHatinitiationandadjustlevothyroxinedoseifrequired
Malabsorption due to gastrointestinal disease and conditions Helicobacter pylori gastritis, coeliac disease, autoimmune atrophic gastritis, and diabetic gastropathy should be considered and treated if possible
Non-adherence Common cause, but should be suspected after other causes have been excluded; consider thyroxine absorption test
Normal TSH and (persistent) symptoms
Concurrent (autoimmune) disease or causes Autoimmuneatrophicgastritiswithperniciousanaemia,Addison’sdisease,diabetes,and rheumatoid arthritis could be considered
Inadequate thyroid hormone concentrations at the tissue level Acknowledgmentofthepatient’ssymptoms;checkifthepatientfeelsbetteratadifferentTSHconcentrationinthenormalrange(ie,anindividualset-point);atrialoflevothyroxine–liothyronine combination therapy can be considered in adherent patientswithlong-lastingsteadystateofTSHinserum
Low TSH with or without (persistent) symptoms
Overtreatment due to high doses Consider lower doses in elderly individuals and patients with subclinical hypothyroidism; ask if the patient takes any over-the-counter preparations that might contain thyroid hormone
Medicalconditions—certaindrugs(eg,metformin)andweightlosscandecreaseTSHconcentrations
Consider lower doses
TSH=thyroid-stimulatinghormone.*Evidencefromprospectivetrials.†Antiepilepticdrugsacceleratethyroxineandtri-iodothyronineconjugationbutserumconcentrationsofTSHdonotnecessarilyincrease.
Table 2: Reasons for failure to reach levothyroxine treatment goals and recommendations

Seminar
8 www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1
Persistent complaints despite biochemical normalisation of TSHAbout 5–10% of biochemically well controlled patients with levothyroxinetreated hypothyroidism have persistent symptoms, such as depression and impaired mental wellbeing.117 Concurrent diseases or perimenopausal status might cause these complaints and should be excluded. Patients with hypothyroidism have a higher prevalence of autoimmune diseases than the general population, which could give rise to similar symptoms. Autoimmunity per se has been suggested to lead to persistent symptoms.118
Circulating thyroid hormone concentrations are regulated by the hypothalamic–pituitary–thyroid axis with an individually determined setpoint, reflected by a smaller intraindividual variability than interindividual variability.119 Therefore, the TSH concentration needed to achieve similar concentrations of circulating thyroid hormones differs between individuals. Differences in individual setpoint could explain why patients with similar TSH concentrations under treatment respond differently. However, the individual setpoint before hypothyroidism is rarely known. Also, studies120,121 that target different TSH goals generally do not show alterations in wellbeing or other clinical parameters.
An alternative explanation for persistent complaints in specific patients might be the imperfections of levothyroxine monotherapy itself. Generally, levothyroxine can ensure
adequate concentrations of circulating thyroxine that can then be converted into triiodothyronine by deiodination via deiodinase 1 and deiodinase 2. However, in euthyroid patients, about 20% of circulating triiodothyronine is derived from direct thyroidal secretion, whereas in patients on levothyroxine monotherapy all triiodothyronine is derived from the conversion of peripheral thyroxine to triiodothyronine. Consequently, patients on levothyroxine monotherapy have higher free thyroxine to triiodothyronine ratios than euthyroid individuals. Some patients with normalised TSH have serum triiodothyronine concentrations below the reference range, while free thyroxine serum concentrations are high.122–124 The clinical significance of this occurrence is unknown. However, levothyroxine monotherapy cannot restore physiological triiodothyronine concentrations or thyroid hormonedependent biological effects in all tissues of hypothyroid rats.125,126 Although a normal TSH concentration reflects euthyroidism at the level of the pituitary, this might not necessarily reflect euthyroidism in all tissues. Tissuespecific differences in the inactivation of deiodinase 2 could play a part, resulting in the normalisation of triiodothyronine concentrations in the hypothalamus before triiodothyronine concentrations have fully normalised in the rest of the body.125
Levothyroxine–liothyronine combination therapySeveral trials using combined levothyroxine–liothyronine therapy have been done in the past 15 years.127 Although some studies128–131 show a beneficial effect, such as patient preference for combination therapy or an improved metabolic profile, patients on combination therapy generally do not have improved outcomes compared with those on levothyroxine monotherapy.132 Possible explanations include inadequate levothyroxine and liothyronine doses or frequency of administration.133 Liothyronine has a short halflife and no previous studies used a slowrelease triiodothyronine. Additionally, most trials were of short duration (<4 months) and used questionnaires to record patients’ symptoms, which might not have been targeted or sensitive enough.
Alternatively, trials might have failed to identify the appropriate subgroups that would benefit from combination therapy. Most trials did not specifically recruit patients who feel unwell on levothyroxine or those with particularly low serum triiodothyronine concentrations. Individuals with genetic variations in thyroid hormone metabolism have not been specifically targeted.133 A subgroup that could be targeted is individuals with common genetic variations in DIO2, which encodes the deiodinase 2 enzyme that converts thyroxine to triiodothyronine locally in several tissues, including the brain.134 The Thr92Ala polymorphism in DIO2 gives rise to deiodinase 2 with a longer halflife than the wildtype enzyme and ectopic localisation in the Golgi apparatus. It was shown to alter expression profiles in the cerebral cortex in a similar pattern as seen in
Before test• Exclude causes of undertreatment other than non-adherence (table 2)• Ensure that no contraindication to high levothyroxine doses exists (eg, check electrocardiogram)
Day of test• Patient has fasted from midnight and empties bladder immediately before dosing (to ensure
monitoring is possible for 60 min after administration)• Administer an equivalent of 1 week’s dose of levothyroxine in liquid form (preferred) or tablet
form, followed by 200 ml of water• Observe patient for 60 min (fasting) and collect blood samples for measurement of TSH, free
thyroxine*, and free tri-iodothyronine at 0, 30, 45, 60, 90, 120, 240, and 360 min*
After test• Continue weekly supervised administration of the same dose of thyroxine (for 5 weeks) and
60 min observation.† Collect blood samples for measurement of TSH, free thyroxine, and free tri-iodothyronine at 0 and 120 min at weeks 2, 3, 4, 5, and 6
Inadequate free thyroxine rise after administration of levothyroxine†→ Further investigation of
malabsorption (table 2)
TSH normalisation due to non-adherence→ Consider other options
including weekly dosing, liquid formulations, and ingestion at bedtime
Consistent rise in free thyroxinewihout rise in TSH→ Consider dose adjustment or
disorders of thyroid hormone metabolism
Figure 3: Thyroxine absorption testProtocol for supervised thyroxine absorption test, followed by weekly supervised thyroxine administration. Adaptedfromreference115,bypermissionofElsevier.TSH=thryoid-stimulatinghormone.*Laboratorytestvalues,especiallyanincreaseinfreethyroxine,canbeinterpretedalreadyatthisstage.†Adequatefreethyroxinerise is estimated to be roughly 50% from baseline at 120 min.116

Seminar
www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1 9
neurodegenerative disease, without evidence of altered thyroid hormone signalling.135 In a study136 of 552 people, the Thr92Ala polymorphism in DIO2 was associated with lower baseline psychological wellbeing in patients on levothyroxine replacement therapy and with better response to combination therapy, compared with patients without the polymorphism on levothyroxine replacement therapy. However, after appropriate multiple testing correction, the results were not significant. Results from a populationbased cohort study137 showed no effect of the Thr92Ala polymorphism on quality of life or cognitive function measures. Sufficiently powered prospective randomised controlled trials are therefore needed before conclusions can be drawn.
Although the American Thyroid Association101 and European Thyroid Association138 guidelines generally recommend against the routine use of combination therapy in patients with hypothyroidism, the recommendations concerning trials in patients with persistent symptoms differ slightly. The European Thyroid Association states that a 3 month trial of levothyroxine–liothyronine combination might be considered experimentally in adherent, biochemically well controlled patients who have persistent complaints despite levothyroxine treatment138 and provides methods for calculating levothyroxine and liothyronine doses.138 However, treatment should be initiated only by accredited doctors of internal medicine or endocrinologists, closely monitored, and discontinued if no improvement is seen. By contrast, the American Thyroid Association recommends against any routine use of such trials outside of formal research and clinical trials, mainly because of uncertainty regarding benefit and longterm safety.101 Both the European Thyroid Association and American Thyroid Association agree on the need for longterm randomised controlled trials to assess risk–benefit ratios. Such trials would need to incorporate investigation of the ideal thyroid parameters to monitor during combination therapy, and whether triiodothyronine concentrations would be an important parameter. The timing of phlebotomy is also important, particularly if liothyronine is being administered more than once daily.
Little evidence exists to support other therapies for hypothyroidism. The use of thyroid extracts or liothyronine monotherapy is generally not recommended because of potential safety concerns associated with the presence of supraphysiological serum triiodothyronine concentrations and a paucity of longterm safety outcome data. The use of compounded thyroid hormones, dietary supplements, and any overthecounter drug for the treatment of hypothyroidism is discouraged.
Directions for future researchAlthough great advances have been made in the identification of causes, knowledge of clinical implications, diagnosis, and treatment of hypothyroidism, several
unanswered questions remain, especially regarding diagnosis and treatment.
Many risk factors have been identified for abnormal TSH concentrations, free thyroxine concentrations, and thyroid disease, but only a small proportion of the variability is explained.139 Therefore, identification of risk factors is important. Increasing evidence shows that endocrinedisrupting chemicals might be casual factors for endocrine diseases. Thyroiddisrupting chemical exposure can come from sources ranging from environmental (eg, flame retardants) to dietary (eg, food packaging material).140 A transatlantic call for action has been made to answer these questions in a collaborative effort.141
The association of hypothyroidism with cardiovascular disease has been established and replicated in several studies.63,67 However, the mechanisms behind this association remain unclear. The link between hypothyroidism and several cardiovascular diseases seems independent of traditional cardiovascular risk factors.63,67,69 Further research focused on novel cardiovascular risk factors or other pathways could shed light on the exact mechanisms, which would be crucial to support treatment decisions and monitor strategies in patients with asymptomatic hypothyroidism.
The diagnosis of hypothyroidism is currently based on statistically defined reference ranges for TSH and free thyroxine, which do not consider whether patients are at risk to develop disease. Because of the arbitrary nature of the cutoffs that define mild and overt hypothyroidism, an alternative grading system based on thyroid function tests has been proposed. The arbitrary nature of these cutoffs was also highlighted by the US Preventive Service Task Force83 as one of the important factors hampering decision making for screening of thyroid dysfunction in asymptomatic patients. These cutoffs also affect treatment decisions in asymptomatic patients with hypothyroidism. More research is needed to identify which adverse health events occur after longterm thyroid dysfunction. Furthermore, which concentrations of TSH and free thyroxine are accompanied by an increased risk of disease needs to be established. This information can be obtained from collaborative observational cohort studies with sufficiently long followup. Once this information is available, randomised controlled trials can assess whether treatment of thyroid function beyond these cutoffs for thyroid function test concentrations reduces excess risk and also the risk–benefit ratio of treatment.
Levothyroxine monotherapy is the standard treatment for hypothyroidism. However, several unresolved issues exist concerning patients who are biochemically well controlled but unsatisfied with their treatment outcome. Future studies should address whether alternative regimens could provide a solution for at least a proportion of patients with residual symptoms. Research areas most urgently in need of progress include: identification of the causes of persistent symptoms in biochemically well

Seminar
10 www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1
15 Hansen PS, Brix TH, Sørensen TI, Kyvik KO, Hegedüs L. Major genetic influence on the regulation of the pituitarythyroid axis: a study of healthy Danish twins. J Clin Endocrinol Metab 2004; 89: 1181–87.
16 Panicker V, Wilson SG, Spector TD, et al. Heritability of serum TSH, free T4 and free T3 concentrations: a study of a large UK twin cohort. Clin Endocrinol 2008; 68: 652–59.
17 Porcu E, Medici M, Pistis G, et al. A metaanalysis of thyroidrelated traits reveals novel loci and genderspecific differences in the regulation of thyroid function. PLoS Genet 2013; 9: e1003266.
18 Eriksson N, Tung JY, Kiefer AK, et al. Novel associations for hypothyroidism include known autoimmune risk loci. PLoS One 2012; 7: e34442.
19 Denny JC, Crawford DC, Ritchie MD, et al. Variants near FOXE1 are associated with hypothyroidism and other thyroid conditions: using electronic medical records for genome and phenomewide studies. Am J Hum Genet 2011; 89: 529–42.
20 Pickrell JK, Berisa T, Liu JZ, Ségurel L, Tung JY, Hinds DA. Detection and interpretation of shared genetic influences on 42 human traits. Nat Genet 2016; 48: 709–17.
21 Medici M, Visser WE, Visser TJ, Peeters RP. Genetic determination of the hypothalamicpituitarythyroid axis: where do we stand? Endocr Rev 2015; 36: 214–44.
22 Persani L. Clinical review: Central hypothyroidism: pathogenic, diagnostic, and therapeutic challenges. J Clin Endocrinol Metab 2012; 97: 3068–78.
23 Effraimidis G, Strieder TGA, Tijssen JGP, Wiersinga WM. Natural history of the transition from euthyroidism to overt autoimmune hypo or hyperthyroidism: a prospective study. Eur J Endocrinol 2011; 164: 107–13.
24 Walsh JP, Bremner AP, Feddema P, Leedman PJ, Brown SJ, O’Leary P. Thyrotropin and thyroid antibodies as predictors of hypothyroidism: a 13year, longitudinal study of a communitybased cohort using current immunoassay techniques. J Clin Endocrinol Metab 2010; 95: 1095–104.
25 Medici M, Porcu E, Pistis G, et al. Identification of novel genetic Loci associated with thyroid peroxidase antibodies and clinical thyroid disease. PLoS Genet 2014; 10: e1004123.
26 Schultheiss UT, Teumer A, Medici M, et al. A genetic risk score for thyroid peroxidase antibodies associates with clinical thyroid disease in communitybased populations. J Clin Endocrinol Metab 2015; 100: e799–807.
27 Effraimidis G, Tijssen JG, Wiersinga WM. Discontinuation of smoking increases the risk for developing thyroid peroxidase antibodies and/or thyroglobulin antibodies: a prospective study. J Clin Endocrinol Metab 2009; 94: 1324–28.
28 Belin RM, Astor BC, Powe NR, Ladenson PW. Smoke exposure is associated with a lower prevalence of serum thyroid autoantibodies and thyrotropin concentration elevation and a higher prevalence of mild thyrotropin concentration suppression in the third National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab 2004; 89: 6077–86.
29 Wu Q, Rayman MP, Lv H, et al. Low population selenium status is associated with increased prevalence of thyroid disease. J Clin Endocrinol Metab 2015; 100: 4037–47.
30 Bougma K, Aboud FE, Harding KB, Marquis GS. Iodine and mental development of children 5 years old and under: a systematic review and metaanalysis. Nutrients 2013; 5: 1384–416.
31 WHO. Assessment of iodine deficiency disorders and monitoring their elimination. A guide for programme managers, 3rd edn. Geneva: World Health Organization, 2007. http://apps.who.int/iris/bitstream/10665/43781/1/9789241595827_eng.pdf (accessed Jan 30, 2017).
32 Bath SC, Steer CD, Golding J, Emmett P, Rayman MP. Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Lancet 2013; 382: 331–37.
33 Caldwell KL, Pan Y, Mortensen ME, Makhmudov A, Merrill L, Moye J. Iodine status in pregnant women in the National Children’s study and in U.S. women (15–44 years), National Health and Nutrition Examination Survey 2005–2010. Thyroid 2013; 23: 927–37.
34 Teng X, Shan Z, Chen Y, et al. More than adequate iodine intake may increase subclinical hypothyroidism and autoimmune thyroiditis: a crosssectional study based on two Chinese communities with different iodine intake levels. Eur J Endocrinol 2011; 164: 943–50.
controlled patients, assessment of whether a more adequate dose (eg, tailored to patient serum triiodothyronine or to a patient’s own particular TSH setpoint) produces more satisfactory outcomes, investigation of whether new formulations (eg, slowrelease liothyronine) or increased administration frequency of levothyroxine–liothyronine combination therapy (eg, liothyronine three times daily) can ameliorate patient symptoms, and identification of patient subgroups that could benefit from therapies other than levothyroxine monotherapy (eg, by identifying additional genetic polymorphisms that could provide information on the individual thyroid setpoint). Genomewide association studies that include a large number of individuals with detailed genotyping could provide such information.ContributorsAll authors designed the Seminar, drafted and edited the manuscript, approved the final version, and contributed equally to this Seminar.
Declaration of interestsRPP received lecture fees from GoodLife Fertility BV and Institut Biochemique SA. All other authors declare no competing interests.
AcknowledgmentsWe thank Wichor Bramer (Erasmus Medical Center, Rotterdam, Netherlands) for the important contribution to the literature search.
References1 Cooper DS, Biondi B. Subclinical thyroid disease. Lancet 2012;
379: 1142–54.2 Salerno M, Capalbo D, Cerbone M, De Luca F.
Subclinical hypothyroidism in childhood—current knowledge and open issues. Nat Rev Endocrinol 2016; 12: 734–46.
3 Teng W, Shan Z, PatilSisodia K, Cooper DS. Hypothyroidism in pregnancy. Lancet Diabetes Endocrinol 2013; 1: 228–37.
4 Åsvold BO, Vatten LJ, Bjøro T. Changes in the prevalence of hypothyroidism: the HUNT Study in Norway. Eur J Endocrinol 2013; 169: 613–20.
5 Aoki Y, Belin RM, Clickner R, Jeffries R, Phillips L, Mahaffey KR. Serum TSH and total T4 in the United States population and their association with participant characteristics: National Health and Nutrition Examination Survey (NHANES 19992002). Thyroid 2007; 17: 1211–23.
6 Canaris GJ, Manowitz NR, Mayor G, Ridgway EC. The Colorado thyroid disease prevalence study. Arch Intern Med 2000; 160: 526–34.
7 Garmendia Madariaga A, Santos Palacios S, GuillénGrima F, Galofré JC. The incidence and prevalence of thyroid dysfunction in Europe: a metaanalysis. J Clin Endocrinol Metab 2014; 99: 923–31.
8 Hollowell JG, Staehling NW, Flanders WD, et al. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab 2002; 87: 489–99.
9 Laurberg P, Cerqueira C, Ovesen L, et al. Iodine intake as a determinant of thyroid disorders in populations. Best Pract Res Clin Endocrinol Metab 2010; 24: 13–27.
10 Teng W, Shan Z, Teng X, et al. Effect of iodine intake on thyroid diseases in China. N Engl J Med 2006; 354: 2783–93.
11 Sichieri R, Baima J, Marante T, de Vasconcellos MTL, Moura AS, Vaisman M. Low prevalence of hypothyroidism among black and Mulatto people in a populationbased study of Brazilian women. Clin Endocrinol 2007; 66: 803–07.
12 McLeod DS, Caturegli P, Cooper DS, Matos PG, Hutfless S. Variation in rates of autoimmune thyroid disease by race/ethnicity in US military personnel. JAMA 2014; 311: 1563–65.
13 Carlé A, Pedersen IB, Knudsen N, et al. Moderate alcohol consumption may protect against overt autoimmune hypothyroidism: a populationbased casecontrol study. Eur J Endocrinol 2012; 167: 483–90.
14 Asvold BO, Bjøro T, Nilsen TI, Vatten LJ. Tobacco smoking and thyroid function: a populationbased study. Arch Intern Med 2007; 167: 1428–32.

Seminar
www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1 11
35 Zimmermann MB, Boelaert K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol 2015; 3: 286–95.
36 Zhong B, Wang Y, Zhang G, Wang Z. Environmental iodine content, female sex and age are associated with newonset amiodaroneinduced hypothyroidism: a systematic review and metaanalysis of adverse reactions of amiodarone on the thyroid. Cardiology 2016; 134: 366–71.
37 Shine B, McKnight RF, Leaver L, Geddes JR. Longterm effects of lithium on renal, thyroid, and parathyroid function: a retrospective analysis of laboratory data. Lancet 2015; 386: 461–68.
38 Shulman KI, Sykora K, Gill SS, et al. New thyroxine treatment in older adults beginning lithium therapy: implications for clinical practice. Am J Geriatr Psychiatry 2005; 13: 299–304.
39 Shu M, Zai X, Zhang B, Wang R, Lin Z. Hypothyroidism side effect in patients treated with sunitinib or sorafenib: clinical and structural analyses. PLoS One 2016; 11: e0147048.
40 Kahraman D, Keller C, Schneider C, et al. Development of hypothyroidism during longterm followup of patients with toxic nodular goitre after radioiodine therapy. Clin Endocrinol 2012; 76: 297–303.
41 Krohn T, Hänscheid H, Müller B, et al. Maximum dose rate is a determinant of hypothyroidism after 131I therapy of Graves’ disease but the total thyroid absorbed dose is not. J Clin Endocrinol Metab 2014; 99: 4109–15.
42 Lee V, Chan SY, Choi CW, et al. Dosimetric predictors of hypothyroidism after radical intensitymodulated radiation therapy for nonmetastatic nasopharyngeal carcinoma. Clin Oncol (R Coll Radiol) 2016; 28: e52–60.
43 Verloop H, Louwerens M, Schoones JW, Kievit J, Smit JWA, Dekkers OM. Risk of hypothyroidism following hemithyroidectomy: systematic review and metaanalysis of prognostic studies. J Clin Endocrinol Metab 2012; 97: 2243–55.
44 Vogelius IR, Bentzen SM, Maraldo MV, Petersen PM, Specht L. Risk factors for radiationinduced hypothyroidism: a literaturebased metaanalysis. Cancer 2011; 117: 5250–60.
45 Nygaard B, Hegedüs L, Nielsen KG, Ulriksen P, Hansen JM. Longterm effect of radioactive iodine on thyroid function and size in patients with solitary autonomously functioning toxic thyroid nodules. Clin Endocrinol 1999; 50: 197–202.
46 Persani L, Ferretti E, Borgato S, Faglia G, BeckPeccoz P. Circulating thyrotropin bioactivity in sporadic central hypothyroidism. J Clin Endocrinol Metab 2000; 85: 3631–35.
47 GraeppiDulac J, VlaeminckGuillem V, PerierMuzet M, Dalle S, Orgiazzi J. Endocrine sideeffects of anticancer drugs: the impact of retinoids on the thyroid axis. Eur J Endocrinol 2014; 170: R253–62.
48 Grunenwald S, Caron P. Central hypothyroidism in adults: better understanding for better care. Pituitary 2015; 18: 169–75.
49 Huang SA, Tu HM, Harney JW, et al. Severe hypothyroidism caused by type 3 iodothyronine deiodinase in infantile hemangiomas. N Engl J Med 2000; 343: 185–89.
50 Dumitrescu AM, Refetoff S. The syndromes of reduced sensitivity to thyroid hormone. Biochim Biophys Acta 2013; 1830: 3987–4003.
51 Beynon J, Akhtar S, Kearney T. Predictors of outcome in myxoedema coma. Crit Care 2008; 12: 111.
52 Wiersinga WM. Myxedema and coma (severe hypothyroidism). In: De Groot LJ, Chrousos G, Dungan K, et al, eds. Endotext. South Dartmouth, MA: MD Text.com, 2000.
53 Khawaja NM, Taher BM, Barham ME, et al. Pituitary enlargement in patients with primary hypothyroidism. Endocr Pract 2006; 12: 29–34.
54 Carlé A, Pedersen IB, Knudsen N, Perrild H, Ovesen L, Laurberg P. Gender differences in symptoms of hypothyroidism: a populationbased DanThyr study. Clin Endocrinol 2015; 83: 717–25.
55 Carlé A, Pedersen IB, Knudsen N, et al. Hypothyroid symptoms fail to predict thyroid insufficiency in old people: a populationbased casecontrol study. Am J Med 2016; 129: 1082–92.
56 Canaris GJ, Steiner JF, Ridgway EC. Do traditional symptoms of hypothyroidism correlate with biochemical disease? J Gen Intern Med 1997; 12: 544–50.
57 Carlé A, Pedersen IB, Knudsen N, Perrild H, Ovesen L, Laurberg P. Hypothyroid symptoms and the likelihood of overt thyroid failure: a populationbased casecontrol study. Eur J Endocrinol 2014; 171: 593–602.
58 Gao X, Liu M, Qu A, et al. Native magnetic resonance T1mapping identifies diffuse myocardial injury in hypothyroidism. PLoS One 2016; 11: e0151266.
59 Tiller D, Ittermann T, Greiser KH, et al. Association of serum thyrotropin with anthropometric markers of obesity in the general population. Thyroid 2016; 26: 1205–14.
60 Shin YW, Choi YM, Kim HS, et al. Diminished quality of life and increased brain functional connectivity in patients with hypothyroidism after total thyroidectomy. Thyroid 2016; 26: 641–49.
61 Muangpaisan W, Petcharat C, Srinonprasert V. Prevalence of potentially reversible conditions in dementia and mild cognitive impairment in a geriatric clinic. Geriatr Gerontol Int 2012; 12: 59–64.
62 Robison CD, Bair TL, Horne BD, et al. Hypothyroidism as a risk factor for statin intolerance. J Clin Lipidol 2014; 8: 401–07.
63 Rodondi N, den Elzen WPJ, Bauer DC, et al, for the Thyroid Studies Collaboration Study Group. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA 2010; 304: 1365–74.
64 Grossman A, Weiss A, KorenMorag N, Shimon I, Beloosesky Y, Meyerovitch J. Subclinical thyroid disease and mortality in the elderly: a retrospective cohort study. Am J Med 2016; 129: 423–30.
65 Gussekloo J, van Exel E, de Craen AJ, Meinders AE, Frölich M, Westendorp RG. Thyroid status, disability and cognitive function, and survival in old age. JAMA 2004; 292: 2591–99.
66 Vanhaelst L, Neve P, Chailly P, Bastenie PA. Coronaryartery disease in hypothyroidism. Observations in clinical myxoedema. Lancet 1967; 2: 800–02.
67 Gencer B, Collet TH, Virgini V, et al, for the Thyroid Studies Collaboration Study Group. Subclinical thyroid dysfunction and the risk of heart failure events: an individual participant data analysis from 6 prospective cohorts. Circulation 2012; 126: 1040–49.
68 Zhang M, Sara JD, Matsuzawa Y, et al. Clinical outcomes of patients with hypothyroidism undergoing percutaneous coronary intervention. Eur Heart J 2016; 37: 2055–65.
69 Chaker L, Baumgartner C, den Elzen WPJ, et al, for the Thyroid Studies Collaboration Study Group. Subclinical hypothyroidism and the risk of stroke events and fatal stroke: An individual participant data analysis. J Clin Endocrinol Metab 2015; 100: 2181–91.
70 Alevizaki M, Synetou M, Xynos K, Alevizaki CC, Vemmos KN. Hypothyroidism as a protective factor in acute stroke patients. Clin Endocrinol 2006; 65: 369–72.
71 Freitas BC, Gereben B, Castillo M, et al. Paracrine signaling by glial cellderived triiodothyronine activates neuronal gene expression in the rodent brain and human cells. J Clin Invest 2010; 120: 2206–17.
72 Jo S, Kalló I, Bardóczi Z, et al. Neuronal hypoxia induces Hsp40mediated nuclear import of type 3 deiodinase as an adaptive mechanism to reduce cellular metabolism. J Neurosci 2012; 32: 8491–500.
73 Collet TH, Bauer DC, Cappola AR, et al, for the Thyroid Studies Collaboration Study Group. Thyroid antibody status, subclinical hypothyroidism, and the risk of coronary heart disease: an individual participant data analysis. J Clin Endocrinol Metab 2014; 99: 3353–62.
74 Pasqualetti G, Pagano G, Rengo G, Ferrara N, Monzani F. Subclinical hypothyroidism and cognitive impairment: systematic review and metaanalysis. J Clin Endocrinol Metab 2015; 100: 4240–48.
75 Tan ZS, Beiser A, Vasan RS, et al. Thyroid function and the risk of Alzheimer disease: the Framingham Study. Arch Intern Med 2008; 168: 1514–20.
76 Chaker L, Wolters FJ, Bos D, et al. Thyroid function and the risk of dementia: the Rotterdam study. Neurology 2016; 87: 1688–95.
77 Rieben C, Segna D, da Costa BR, et al. Subclinical thyroid dysfunction and the risk of cognitive decline: a metaanalysis of prospective cohort studies. J Clin Endocrinol Metab 2016; 101: 4945–54.
78 Tseng FY, Lin WY, Li CI, Li TC, Lin CC, Huang KC. Subclinical hypothyroidism is associated with increased risk for cancer mortality in adult Taiwanese—a 10 years populationbased cohort. PLoS One 2015; 10: e0122955.
79 Bano A, Chaker L, Plompen EP, et al. Thyroid function and the risk of nonalcoholic fatty liver disease: the Rotterdam study. J Clin Endocrinol Metab 2016; 101: 3204–11.

Seminar
12 www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1
80 Zhang Y, Chang Y, Ryu S, et al. Thyroid hormone levels and incident chronic kidney disease in euthyroid individuals: the Kangbuk Samsung health study. Int J Epidemiol 2014; 43: 1624–32.
81 Gronich N, Deftereos SN, Lavi I, Persidis AS, Abernethy DR, Rennert G. Hypothyroidism is a risk factor for newonset diabetes: a cohort study. Diabetes Care 2015; 38: 1657–64.
82 Abrahamsen B, Jørgensen HL, Laulund AS, et al. The excess risk of major osteoporotic fractures in hypothyroidism is driven by cumulative hyperthyroid as opposed to hypothyroid time: an observational registerbased timeresolved cohort analysis. J Bone Miner Res 2015; 30: 898–905.
83 LeFevre ML, the U.S. Preventive Services Task Force. Screening for thyroid dysfunction: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2015; 162: 641–50.
84 Roelfsema F, Pereira AM, Adriaanse R, et al. Thyrotropin secretion in mild and severe primary hypothyroidism is distinguished by amplified burst mass and Basal secretion with increased spikiness and approximate entropy. J Clin Endocrinol Metab 2010; 95: 928–34.
85 Kim TH, Kim KW, Ahn HY, et al. Effect of seasonal changes on the transition between subclinical hypothyroid and euthyroid status. J Clin Endocrinol Metab 2013; 98: 3420–29.
86 Chaker L, Baumgartner C, den Elzen WP, et al, for the Thyroid Studies Collaboration Study Group. Thyroid function within the reference range and the risk of stroke: an individual participant data analysis. J Clin Endocrinol Metab 2016; 101: 4270–82.
87 Chaker L, van den Berg ME, Niemeijer MN, et al. Thyroid function and sudden cardiac death: a prospective populationbased cohort study. Circulation 2016; 134: 713–22.
88 Cappola AR, Arnold AM, Wulczyn K, Carlson M, Robbins J, Psaty BM. Thyroid function in the euthyroid range and adverse outcomes in older adults. J Clin Endocrinol Metab 2015; 100: 1088–96.
89 Inoue K, Tsujimoto T, Saito J, Sugiyama T. Association between serum thyrotropin levels and mortality among euthyroid adults in the United States. Thyroid 2016; 26: 1457–65.
90 Surks MI, Boucai L. Age and racebased serum thyrotropin reference limits. J Clin Endocrinol Metab 2010; 95: 496–502.
91 Surks MI. TSH reference limits: new concepts and implications for diagnosis of subclinical hypothyroidism. Endocr Pract 2013; 19: 1066–69.
92 Wartofsky L, Dickey RA. The evidence for a narrower thyrotropin reference range is compelling. J Clin Endocrinol Metab 2005; 90: 5483–88.
93 KahapolaArachchige KM, Hadlow N, Wardrop R, Lim EM, Walsh JP. Agespecific TSH reference ranges have minimal impact on the diagnosis of thyroid dysfunction. Clin Endocrinol 2012; 77: 773–79.
94 Vadiveloo T, Donnan PT, Murphy MJ, Leese GP. Age and genderspecific TSH reference intervals in people with no obvious thyroid disease in Tayside, Scotland: the Thyroid Epidemiology, Audit, and Research Study (TEARS). J Clin Endocrinol Metab 2013; 98: 1147–53.
95 Jaume JC, Mendel CM, Frost PH, Greenspan FS, Laughton CW. Extremely low doses of heparin release lipase activity into the plasma and can thereby cause artifactual elevations in the serumfree thyroxine concentration as measured by equilibrium dialysis. Thyroid 1996; 6: 79–83.
96 van Deventer HE, Mendu DR, Remaley AT, Soldin SJ. Inverse loglinear relationship between thyroidstimulating hormone and free thyroxine measured by direct analog immunoassay and tandem mass spectrometry. Clin Chem 2011; 57: 122–27.
97 Fliers E, Bianco AC, Langouche L, Boelen A. Thyroid function in critically ill patients. Lancet Diabetes Endocrinol 2015; 3: 816–25.
98 Garber JR, Cobin RH, Gharib H, et al, for the American Association of Clinical Endocrinologists and American Thyroid Association Taskforce on Hypothyroidism in Adults Study Groups. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Endocr Pract 2012; 18: 988–1028.
99 Brenta G, Vaisman M, Sgarbi JA, et al, for the Task Force on Hypothyroidism of the Latin American Thyroid Society (LATS) Study Group. Clinical practice guidelines for the management of hypothyroidism. Arq Bras Endocrinol Metabol 2013; 57: 265–91.
100 Vanderpump MP, Ahlquist JA, Franklyn JA, Clayton RN. Consensus statement for good practice and audit measures in the management of hypothyroidism and hyperthyroidism. The Research Unit of the Royal College of Physicians of London, the Endocrinology and Diabetes Committee of the Royal College of Physicians of London, and the Society for Endocrinology. BMJ 1996; 313: 539–44.
101 Jonklaas J, Bianco AC, Bauer AJ, et al, for the American Thyroid Association Task Force on Thyroid Hormone Replacement Study Group. Guidelines for the treatment of hypothyroidism: prepared by the American Thyroid Association Task Force on thyroid hormone replacement. Thyroid 2014; 24: 1670–751.
102 Pearce SHS, Brabant G, Duntas LH, et al. 2013 ETA Guideline: management of subclinical hypothyroidism. Eur Thyroid J 2013; 2: 215–28.
103 Roos A, LinnRasker SP, van Domburg RT, Tijssen JP, Berghout A. The starting dose of levothyroxine in primary hypothyroidism treatment: a prospective, randomized, doubleblind trial. Arch Intern Med 2005; 165: 1714–20.
104 Abdalla SM, Bianco AC. Defending plasma T3 is a biological priority. Clin Endocrinol 2014; 81: 633–41.
105 Alexander EK, Marqusee E, Lawrence J, Jarolim P, Fischer GA, Larsen PR. Timing and magnitude of increases in levothyroxine requirements during pregnancy in women with hypothyroidism. N Engl J Med 2004; 351: 241–49.
106 StagnaroGreen A, Abalovich M, Alexander E, et al, for the American Thyroid Association Taskforce on Thyroid Disease During Pregnancy and Postpartum Study Group. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid 2011; 21: 1081–125.
107 Chan S, Boelaert K. Optimal management of hypothyroidism, hypothyroxinaemia and euthyroid TPO antibody positivity preconception and in pregnancy. Clin Endocrinol 2015; 82: 313–26.
108 Medici M, Korevaar TI, Visser WE, Visser TJ, Peeters RP. Thyroid function in pregnancy: what is normal? Clin Chem 2015; 61: 704–13.
109 Taylor PN, Iqbal A, Minassian C, et al. Falling threshold for treatment of borderline elevated thyrotropin levelsbalancing benefits and risks: evidence from a large communitybased study. JAMA Intern Med 2014; 174: 32–39.
110 Somwaru LL, Arnold AM, Joshi N, Fried LP, Cappola AR. High frequency of and factors associated with thyroid hormone overreplacement and underreplacement in men and women aged 65 and over. J Clin Endocrinol Metab 2009; 94: 1342–45.
111 Bolk N, Visser TJ, Nijman J, Jongste IJ, Tijssen JGP, Berghout A. Effects of evening vs morning levothyroxine intake: a randomized doubleblind crossover trial. Arch Intern Med 2010; 170: 1996–2003.
112 Vita R, Saraceno G, Trimarchi F, Benvenga S. Switching levothyroxine from the tablet to the oral solution formulation corrects the impaired absorption of levothyroxine induced by protonpump inhibitors. J Clin Endocrinol Metab 2014; 99: 4481–86.
113 Seng Yue C, Benvenga S, Scarsi C, Loprete L, Ducharme MP. When bioequivalence in healthy volunteers may not translate to bioequivalence in patients: differential effects of increased gastric pH on the pharmacokinetics of levothyroxine capsules and tablets. J Pharm Pharm Sci 2015; 18: 844–55.
114 Cappelli C, Pirola I, Daffini L, et al. A doubleblind placebocontrolled trial of liquid thyroxine ingested at breakfast: results of the TICO Study. Thyroid 2016; 26: 197–202.
115 Koulouri O, Moran C, Halsall D, Chatterjee K, Gurnell M. Pitfalls in the measurement and interpretation of thyroid function tests. Best Pract Res Clin Endocrinol Metab 2013; 27: 745–62.
116 Walker JN, Shillo P, Ibbotson V, et al. A thyroxine absorption test followed by weekly thyroxine administration: a method to assess nonadherence to treatment. Eur J Endocrinol 2013; 168: 913–17.
117 Saravanan P, Chau WF, Roberts N, Vedhara K, Greenwood R, Dayan CM. Psychological wellbeing in patients on ‘adequate’ doses of lthyroxine: results of a large, controlled communitybased questionnaire study. Clin Endocrinol 2002; 57: 577–85.
118 Ott J, Promberger R, Kober F, et al. Hashimoto’s thyroiditis affects symptom load and quality of life unrelated to hypothyroidism: a prospective casecontrol study in women undergoing thyroidectomy for benign goiter. Thyroid 2011; 21: 161–67.

Seminar
www.thelancet.com Published online March 20, 2017 http://dx.doi.org/10.1016/S0140-6736(17)30703-1 13
119 Andersen S, Pedersen KM, Bruun NH, Laurberg P. Narrow individual variations in serum T(4) and T(3) in normal subjects: a clue to the understanding of subclinical thyroid disease. J Clin Endocrinol Metab 2002; 87: 1068–72.
120 Walsh JP, Ward LC, Burke V, et al. Small changes in thyroxine dosage do not produce measurable changes in hypothyroid symptoms, wellbeing, or quality of life: results of a doubleblind, randomized clinical trial. J Clin Endocrinol Metab 2006; 91: 2624–30.
121 Boeving A, PazFilho G, Radominski RB, Graf H, Amaral de Carvalho G. Lownormal or highnormal thyrotropin target levels during treatment of hypothyroidism: a prospective, comparative study. Thyroid 2011; 21: 355–60.
122 Gullo D, Latina A, Frasca F, Le Moli R, Pellegriti G, Vigneri R. Levothyroxine monotherapy cannot guarantee euthyroidism in all athyreotic patients. PLoS One 2011; 6: e22552.
123 Ito M, Miyauchi A, Morita S, et al. TSHsuppressive doses of levothyroxine are required to achieve preoperative native serum triiodothyronine levels in patients who have undergone total thyroidectomy. Eur J Endocrinol 2012; 167: 373–78.
124 Jonklaas J, Davidson B, Bhagat S, Soldin SJ. Triiodothyronine levels in athyreotic individuals during levothyroxine therapy. JAMA 2008; 299: 769–77.
125 Werneck de Castro JP, Fonseca TL, Ueta CB, et al. Differences in hypothalamic type 2 deiodinase ubiquitination explain localized sensitivity to thyroxine. J Clin Invest 2015; 125: 769–81.
126 EscobarMorreale HF, del Rey FE, Obregón MJ, de Escobar GM. Only the combined treatment with thyroxine and triiodothyronine ensures euthyroidism in all tissues of the thyroidectomized rat. Endocrinology 1996; 137: 2490–502.
127 Bunevicius R, Kazanavicius G, Zalinkevicius R, Prange AJ Jr. Effects of thyroxine as compared with thyroxine plus triiodothyronine in patients with hypothyroidism. N Engl J Med 1999; 340: 424–29.
128 Nygaard B, Jensen EW, Kvetny J, Jarløv A, Faber J. Effect of combination therapy with thyroxine (T4) and 3,5,3�triiodothyronine versus T4 monotherapy in patients with hypothyroidism, a doubleblind, randomised crossover study. Eur J Endocrinol 2009; 161: 895–902.
129 Walsh JP, Shiels L, Lim EM, et al. Combined thyroxine/liothyronine treatment does not improve wellbeing, quality of life, or cognitive function compared to thyroxine alone: a randomized controlled trial in patients with primary hypothyroidism. J Clin Endocrinol Metab 2003; 88: 4543–50.
130 EscobarMorreale HF, BotellaCarretero JI, GómezBueno M, Galán JM, Barrios V, Sancho J. Thyroid hormone replacement therapy in primary hypothyroidism: a randomized trial comparing Lthyroxine plus liothyronine with Lthyroxine alone. Ann Intern Med 2005; 142: 412–24.
131 Appelhof BC, Fliers E, Wekking EM, et al. Combined therapy with levothyroxine and liothyronine in two ratios, compared with levothyroxine monotherapy in primary hypothyroidism: a doubleblind, randomized, controlled clinical trial. J Clin Endocrinol Metab 2005; 90: 2666–74.
132 GrozinskyGlasberg S, Fraser A, Nahshoni E, Weizman A, Leibovici L. Thyroxinetriiodothyronine combination therapy versus thyroxine monotherapy for clinical hypothyroidism: metaanalysis of randomized controlled trials. J Clin Endocrinol Metab 2006; 91: 2592–99.
133 Wiersinga WM. Paradigm shifts in thyroid hormone replacement therapies for hypothyroidism. Nat Rev Endocrinol 2014; 10: 164–74.
134 McAninch EA, Bianco AC. New insights into the variable effectiveness of levothyroxine monotherapy for hypothyroidism. Lancet Diabetes Endocrinol 2015; 3: 756–58.
135 McAninch EA, Jo S, Preite NZ, et al. Prevalent polymorphism in thyroid hormoneactivating enzyme leaves a genetic fingerprint that underlies associated clinical syndromes. J Clin Endocrinol Metab 2015; 100: 920–33.
136 Panicker V, Saravanan P, Vaidya B, et al. Common variation in the DIO2 gene predicts baseline psychological wellbeing and response to combination thyroxine plus triiodothyronine therapy in hypothyroid patient. J Clin Endocrinol Metab 2009; 94: 1623–29.
137 Wouters HJ, van Loon HC, van der Klauw MM, et al. No effect of the Thr92Ala polymorphism of deiodinase2 on thyroid hormone parameters, healthrelated quality of life, and cognitive functioning in a large populationbased cohort study. Thyroid 2016; published online Oct 27. DOI:10.1089/thy.2016.0199.
138 Wiersinga WM, Duntas L, Fadeyev V, Nygaard B, Vanderpump MP. 2012 ETA guidelines: the use of LT4 + LT3 in the treatment of hypothyroidism. Eur Thyroid J 2012; 1: 55–71.
139 Chaker L, Korevaar TI, Medici M, et al. Thyroid function characteristics and determinants: the Rotterdam study. Thyroid 2016; 26: 1195–204.
140 Boas M, FeldtRasmussen U, Main KM. Thyroid effects of endocrine disrupting chemicals. Mol Cell Endocrinol 2012; 355: 240–48.
141 Leung AM, Korevaar TI, Peeters RP, et al. Exposure to thyroiddisrupting chemicals: a transatlantic call for action. Thyroid 2016; 26: 479–80.