Embed Size (px)
Citation preview

Journal of The Association of Physicians of India ■ Vol. 64 ■ July 2016 83
Hypothyroidism Presenting as Multiple Body Cavity EffusionsGyanendu Kumar1, Amritesh Kumar1, Ram Pratap Bundela1, Rupesh Pokharna2, Prachis Ashdhir3, Sandeep Nijhawan4
1Resident, 2Prof. and Unit Head, 3Asst. Prof., 4Prof. and Head, Dept. of Gastroenterology, Sawai Man Singh Medical College and Hospital, Jaipur, Rajasthan Received: 20.05.2015; Revised: 29.07.2015; Accepted: 31.07.2015
Introduction
Isolated ascites, pericardial effusion or pleural effusion is not unusual in
hypothyroidism. Ascites occurs in < 4% of cases of hypothyroidism.1 Reported incidence of pericardial effusion is 3 to 6% in recent studies.3 Pleural effusion is also rare and its frequency is probably underestimated as the effusions are small and of minor clinical significance. Due to rarity of these conditions, diagnosis is often difficult and delayed.
Multiple effusions involving larger body cavities and tissue edema all occurr ing s imul taneously due to hypothyroidism is extremely rare. We present a case who developed ascites, pericardial, pleural effusions and tissue edema simultaneously.
Case Report
A 6 0 y e a r s o l d m a l e p a t i e n t p r e s e n t e d w i t h s y m p t o m s o f insidious onset, painless, progressive abdominal distension since 2 months and progress ive swel l ing of both
lower chest and dull note on percussion bilaterally. Gastrointestinal system examination revealed ascites.
T h e i n v e s t i g a t i o n s s h o w e d haemoglobin of 10.6 gm%. Complete blood count, erythrocyte sedimentation rate, blood sugar levels, electrolytes, blood urea, serum creat inine and urinalysis were normal. Liver function tests including serum total protein, albumin, globulins and prothrombin time were also within normal range.
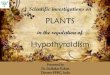
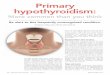
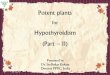
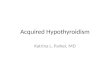
Chest radiograph showed massive cardiomegaly with bilateral pleural effusion. Ultrasonography abdomen showed moderate ascites and computed tomography chest (F igure 1) and abdomen (Figure 2) revealed massive pericardial effusion, bilateral pleural effusion and moderate ascites.
E l e c t r o c a r d i o g r a m s h o w e d l o w v o l t a g e Q R S c o m p l e x e s . 2 D Echocardiogram done subsequently showed a large circumferential echo free space consistent with massive pericardial effusion and evidence of cardiac tamponade (diastolic collapse of right atrium and right ventricle free wall) with preserved left ventricular systolic function, ejection fraction 55%.
Viral serology for both hepatitis B and C were negative, UGI endoscopy and colour doppler abdomen were done to rule out portal hypertension and both were normal.
Ascitic fluid study showed total cells of 100/ cumm with 98% lymphocytes, high protein (3.24 gm%) and high serum ascitic albumin gradient (SAAG - 1.91) and normal adenosine deaminase level (ADA - 6.8 U/L). Pleural fluid examination showed total cells of 200 / cumm with 90% lymphocytes, h igh prote in (3 .97 gm%), normal sugar and normal ADA level (8 .1 U/L). Cytology of both the fluids were negative for malignancy. In view of cardiac tamponade, pericardiocentesis was done with aspiration of about 1500
lower limbs since 1 month. He also had const ipat ion and progressive hoarseness of voice for 2 months. He had no history of chest pain, shortness of breath, orthopnea, paroxysmal nocturnal dyspnea, jaundice, abdominal pain, hematemesis, melena, urinary symptoms, anorexia or weight loss. He was a chronic smoker for last 25 years and non-alcoholic.
E x a m i n a t i o n r e v e a l e d m i l d periorbital and facial puffiness along with bilateral pitting pedal edema. His skin was dry and coarse. Neurological e x a m i n a t i o n r e v e a l e d d e l a y e d relaxation of ankle jerks.
The patient was afebrile with a pulse rate of 75/min, blood pressure 130/80 mm of Hg and elevated jugular venous pressure. On cardiopulmonary examination there was muffled heart sounds with absent breath sounds in
AbstractPrimary hypothyroidism is a common clinical condition in which serous effusions are rare. Isolated cases have been reported in literature about presence of ascites, pleural effusion, pericardial effusion or combination of any two. But combination of all three is extremely rare.
We hereby report a case of multiple body cavity effusions (ascites, pleural and pericardial effusions) and tissue edema (pedal and facial) in a hypothyroid male. He responded well to thyroid hormone replacement therapy.
Fig. 1: CT chest showing massive pericardial effusion and bilateral plerual effusion
Fig. 2: CT abdomen showing the presence of moderate ascites

Journal of The Association of Physicians of India ■ Vol. 64 ■ July 201684
ml straw colour fluid. Analysis of fluid showed total cells of 10 /cumm with high protein (5.3 gm%), normal ADA level (8.3 U/L), and cytology revealed mainly lymphoid and degenerated cells but no malignant cells. Culture of the pericardial fluid was negative for bacteria and acid fast bacilli.
Thyroid function tests showed TSH 137.8 mIU/ml (normal range 0.4 – 4), free T4 0.45 ng/dl (normal range 0.89 – 1.76), and free T3 0.63 pg/ml (normal range 0.92 – 2.78). Ultrasonography revealed atrophic changes in both thyroid lobes. Thyroid peroxidase antibody was negative.
Subsequent hospital course was uncomplicated and he was discharged with gradually escalating dose of levothyroxine from 50 to 100 microgram daily. On 4 weeks follow up he was in good health and had abatement of ascites, pleural effusion and tissue edema and only minimal pericardial effusion left, his TSH was 30.1m IU/ml and he continued on a maintenance dose of 100 microgram with regular follow up.
Discussion
Tissue edema is a common clinical manifestat ion in hypothyroidism. Serous cavity effusions occur with variable but low frequencies. Isolated findings l ike pericardial effusion, pleural effusion or ascites are not unusual whereas combinat ion of multiple body cavity effusions are extremely rare.
P e r i c a r d i a l e f f u s i o n ( P E ) i n hypothyroidism has been reported in old studies with extremely variable incidence ranging from 30% to 80%.2
The recent studies, however, conclude that PE is extremely infrequent in hypothyroidism, with an incidence of 3% to 6%.3 The mainstay of treatment for thyroid PE is simple thyroxine replacement, except in those patients w i t h p e r i c a r d i a l t a m p o n a d e o r impending tamponade, this condition mandates urgent pericardiocentesis.
Pleural e f fus ion per se due to hypothyroidism is rare and requires careful exclusion of other associated conditions. Effusions solely due to hypothyro id i sm have border l ine characteristics between exudates and transudates and show little evidence of inflammation.4
There has been a suggestion that SAAG may exceed 1.1 in patients with myxedema ascites, based on a review of 8 patients.1 A review of the literature revealed up 51 wel l -documented cases of myxedema ascites (Table 1).5 A consistent finding was the high fluid protein level (>2.5 g/dL). Fluid protein levels exceeded 2.5 g/dL in almost all cases, with a mean of 3.9 g/dL. The mean SAAG was 1.5 with a range of 0.8-2.3 g/dL. White blood cell counts were rather low, usually with a predominance of lymphocytes; the mean white blood cell count was 60/ L with a mean of 81% lymphocytes.
T h e a c c e p t e d p a t h o g e n e s i s o f multiple effusions in hypothyroidism is that (a) It is part of the generalized polyserositis. (b) Increased leak of plasma proteins because of abnormal capillary permeability and the lack of a compensatory increase in lymph flow and protein return rate. (c) Exudative polyserosi t is due to a l terat ion in albumin metabolism. (d) Deposition of mucopolysaccharides and protein in
pericardial space. (e) Hyaluronic acid accumulation in the skin which causes edema by a direct hygroscopic effect, and interaction with albumin to form complexes that prevent the lymphatic drainage of extravasated albumin. (f ) Other causes of ascites and pleural effusion are due to cardiac tamponade producing right sided or congestive heart failure. Diagnosis may be delayed but treatment with thyroid hormone replacement therapy leads to complete regression of effusions.
In our case too, patient had high protein, high SAAG ascites as well as high protein fluids in pleural and pericardial spaces. Investigations were done to evaluate other causes of high protein, high SAAG ascites. As patient had clinical as well as echocardiographic evidence of cardiac tamponade, urgent pericardiocentesis was done. After excluding most of the possible causes and with a strong clinical suspicion of hypothyroidism, thyroid function tests were confirmatory. In our patient hypothyroidism itself or the proposed pathogenic mechanisms including cardiac tamponade might be the cause of multiple effusions.
In conclusion hypothyroidism can have rare modes of presentations. It can present with either isolated effusion or in combination of multiple body cavity effusions along with tissue edema. High index of clinical suspicion is required to diagnose such cases. The treatment is simple and gratifying with almost complete regression of findings after thyroid hormone replacement and maintenance of euthyroid state.
References 1. De Castro F, Bonacini M, Walden JM, Schubert TT. Myxedema
ascites. Report of two cases and review of the literature. J Clin Gastroenterol 1991; 13:411-4.
2. Kabadi UM, Kumar SP. Pericardial effusion in primary hypothyroidism. Am Heart J 1990; 120:1393-5.
3. Hayat Al M, Rashid Al B, Massive Pericardial Effusion as a sole Manifestation of Hypothyroidism – A Case Report. Bahrain Medical Bulletin 2000; 22.
4. Andrew G, Jaime R, Gregory GS, Bart C, Steven AS. Hypothyroidism and pleural effusions. Chest 1990; 98:1130-32.
5. Jeong-Seon Ji, Hiun-Suk Chae, Young-Seok Cho, Hyung-Keun Kim, Sung-Soo Kim, Chang-Wook Kim, Myxedema Ascites: Case Report and Literature Review. J Korean Med Sci 2006; 21:761-4.
Table 1: Characteristics of reported patients with myxedema ascites
No. of patients Mean Ranges RemarksAscites protein(g/dl)
49 3.9 1.8-5.1 Forty eight patients (98%) showed ascites protein levels >2.5 g/dl
SAAG (g/dl) 11 1.5 0.8-2.3 Because of the small number of patients, the characteristics were unclear
Ascites WBC count(per μL)
48 60 10-400 Predominance of lymphocytes (mean 81%)
Duration of ascites 51 8 mths 1 mths to 8 yr Response to treatment
51 Regression of ascites
SAAG, serum- to ascites albumin gradient; WBC, white blood cell