Embed Size (px)
Citation preview
© 2011, The Board of Trustees of the University of Illinois and The University of Tokyo. Last update: 03/01/2011 v7 (MEdP)
_____________________________________________________________________________________________________________________
J. Otaki, MD, DMedSc Department of General Medicine & Primary Care, Tokyo Medical University Hospital
H. Nishigori, MD, MMEd, PhD International Research Center for Medical Education, The University of Tokyo
G. Bordage, MD, PhD Department of Medical Education R. Yudkowsky, MD, MHPE University of Illinois at Chicago J. Riddle, MD
T. Lowenstein, MD Department of Family Medicine Clalit Health Services, Haifa University _____________________________________________________________________________________________________________________ A Japanese version of this handbook can be found at: http://www.ircme.u-tokyo.ac.jp/activity/hdpe.html
Hypothesis-Driven Physical Exam _________________________________________________
Student Handbook
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
2
This project was funded in part by grants from:
- The Edward J. Stemmler Medical Education Research Fund, National Board of Medical Examiners (NBME), Philadelphia, USA. This publication does not necessarily reflect NBME policy and NBME support provides no official endorsement. - Aid for Scientific Research, Ministry of Education, Culture, Sports, Science, & Technology, Government of Japan, Tokyo, Japan.
This document may be reproduced in part or in whole with the understanding that proper reference and attribution to the authors and title of the document will be explicit. Please send any comments or suggestions to Dr. R. Yudkowsky at [email protected].

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
3
Table of content Context 4 How to use this handbook 5 Validation 7 Complaints and Prototypical Diagnoses 8 1. Heart murmur 10 2. Itchy Scalp 12 3. Stuffy Nose and Sore Throat 14 4. Swollen Neck and Fatigue 16 5. Blurred Vision 17 6. Hearing Loss 18 7. Funny Feeling Face 19 8. Shortness of Breath 20 9. Lump in Breast 22 10. Leg Pain on Exertion 23 11. Upper Abdominal Pain 24 12. Lower Abdominal Pain 25 13. Painful Wrist 26 14. Painful Shoulder 28 15. Sore Knee 29 16. Painful Hip 30 17. Painful Ankle 31 18. Unsteadiness 32 19. Back Pain 34 List of maneuvers 36

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
4
Context
The set of complaints and prototypical diagnoses contained in this handbook were
developed as part of a hypothesis-driven approach to assessing the complete, head-to-
toe physical exam in order to better integrate the technical and cognitive aspects of the
physical examination. In a nutshell, you are asked to learn the physical exam
maneuvers in the context of chief complaints, limited prototypical diagnoses, and
discriminating features. When tested on your physical exam skills, you are presented
with a short history and an accompanying differential diagnosis consisting of two
alternative diagnoses; the history is kept short because the emphasis here is on
anticipating and performing a physical exam with specific discriminating signs in mind.
Your task is then:
a) To anticipate the positive physical findings for each diagnosis in the differential
and identify the discriminating findings between the diagnoses;
b) To perform the physical exam maneuvers on a patient instructor exhibiting
certain positive findings (Patient instructors are highly trained standardized
patients who not only simulate clinical findings but also provide instruction to the
students when needed, for example, correcting a poorly or incorrectly executed
physical exam maneuver.);
c) To interpret the findings by proposing a most likely diagnosis;
d) To correct any physical exam maneuvers, as prompted by the patient instructor if
needed, that were incorrectly executed or omitted initially and to revise your
working diagnosis if needed; and
e) To document the findings associated with your physical exam.
We selected 160 physical exam maneuvers that were grouped according to 19 chief
complaints (e.g., blurred vision, shortness of breath) and 60 distinct diagnoses.
Typically, there are three to four prototypical diagnoses for each chief complaint. The
main purpose is to learn the maneuvers in the context of a differential diagnosis and
discriminating features. Special attention was paid to include frequent or prototypical

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
5
diagnoses. As part of your learning experience, you are given in this handbook the
diagnoses and the list of maneuvers associated with each complaint.
How to use this handbook.
On your own, look up the maneuvers associated with each diagnosis and identify the
discriminating positive and negative findings associated with various pairs of diagnoses.
Although the chief complaints may refer initially to a specific anatomical region (e.g., the
neck or lungs), other anatomical structures and systems may be involved as dictated by
the differential diagnosis. For example, if you are examining the lungs for congestive
heart failure, the neck (JVP) and the lower limbs (pedal edema) are also included in that
chief complaint.
As an example, the table below illustrates the discriminating findings associated with a
clinical scenario suggesting a lateral epicondylitis (tennis elbow) compared to an
olecranon bursitis; a diagnosis of septic arthritis could also be possible in an elbow.
The discriminating findings for a lateral epicondylitis and an olecranon bursitis are
highlighted in yellow shadings in the table.
Note. The diagnoses in this example come from a differential diagnosis that is not part
of this handbook.
Clinical scenario: Tina, a 42-year-old women, came to the clinic because her right
elbow has been bothering her for the last 10 days. The discomfort is worse with activity.
You are thinking about a possible lateral epicondylitis (tennis elbow) or an olecranon
bursitis. In anticipation of your physical exam of the upper extremities, list the positive
sign(s) associate with each diagnostic hypothesis.

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
6
Lateral epicondylitis (tennis elbow)
Olecranon bursitis Septic arthritis
M1 Wash hands √ √ √ MA10: Have patient point out location of pain
Points to lateral epicondyle
Points to olecranon process
M90: Assess range of motion of elbows bilaterally
Normal Decreased at the end of extension when large effusion present
M91: Inspect and palpate elbows bilaterally
- Normal to inspection - Tender lateral
epicondyle on palpation
- Swollen, fluid filled sac; possibly warm & erythematous
-Painless swelling
M88: Assess range of motion of wrists bilaterally
Normal Normal
M118: Test grip strength bilaterally
Normal Normal
M120: Test biceps strength bilaterally
Normal or possibly painful at lateral epicondyle
Normal
M121: Test triceps strength bilaterally
Normal Normal
M161: Tennis elbow (Cozen’s) test
Painful Not painful
Avoid the temptation of simply copying the set of discriminating findings from fellow
students. The active search and organization of discriminating findings will help you
better understand the significance of each maneuver and associated discriminating
signs.
A complete list of the 160 maneuvers associated with this hypothesis-driven physical
exam approach is provided at the end of the handbook. Please note that some
maneuvers will include some sub-routines, such as measuring the blood pressure,
checking the jugular venous pulse, or testing sharp and dull sensation. Be sure to

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
7
execute all the sub-routines when examining the patient in order to be fully credited for
having executed the maneuver correctly.
Validation
The prototypical diagnoses and physical exam maneuvers were validated by an
international panel of eight physicians closely involved in teaching the physical
examination to medical students.1 They came from the USA, Canada, Belgium,
Switzerland, and Japan. They judged the appropriateness of the prototypical diagnoses
and the completeness of the physical exam maneuvers selected for an introductory
course. We are most grateful for their input. Their comments and suggestions were
incorporated in the current document. We are however solely responsible for the final
selection. In addition, references accompany each complaint, concerning the
reproducibility, sensitivity, and specificity of the signs.2
_________________________________________
1. Yudkowsky, R, Otaki, J, Lowenstein, T, Riddle, J, Nishigori, H, Bordage, G. A Hypothesis-Driven Physical Exam for Medical Students: Initial Gathering of Validity Evidence. Medical Education, 2009; 43:729-40. 2. Additional suggested readings: ER Black, DR Bordley, TG Tape, RJ Panzer. (eds.) Diagnostic Strategies for Common Medical Problems. Philadelphia: American College of Physicians. 1999. SR McGee. Evidence-based physical diagnosis. (2nd ed.) Philadelhpia: Saunders/Elsivier. 2007. DL Simel, D. Rennie, SA Keitz. The Rational Clinical Examination: Evidence-based Clinical Diagnosis. McGraw-Hill, 2008.

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
8
Complaints and Prototypical Diagnoses
Complaint 1: Heart murmur 1. Mitral regurgitation 2. Aortic stenosis
3. Aortic sclerosis 4. Tricuspid regurgitation
Complaint 2: Itchy Scalp 1. Seborrheic dermatitis 2. Lice
3. Tinea capitis Complaint 3: Stuffy Nose and Sore Throat 1. Acute sinusitis 2. Allergic rhinitis 3. Streptococcal pharyngitis 4. Viral URI (rhinosinitis) Complaint 4: Swollen Neck and Fatigue 1. Hypothyroidism
2. Anemia Complaint 5: Blurred Vision 1. Diabetic retinopathy 2. Transient ischemic attack (TIA)
3. Retinal artery or vein occlusion 4. Cataracts
Complaint 6: Hearing Loss 1. Serous otitis media 2. Sudden viral hearing loss 3. Cerumen impaction 4. Tympanic membrane perforation Complaint 7: Funny Feeling Face 1. Trigeminal neuralgia (V) 2. Bell’s palsy (VII): peripheral facial nerve palsy 3. Stroke: central facial nerve palsy Complaint 8: Shortness of Breath 1. Asthma
2. Congestive heart failure (CHF) (class 3) secondary to ischemic coronary artery disease (CAD)
3. Chronic obstructive pulmonary disease (COPD)
4. Panic attack 5. Pneumonia 6. Pulmonary embolism

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
9
Complaint 9: Lump in Breast 1. Breast cancer 2. Fibrocystic changes
Complaint 10: Leg Pain on Exertion 1. Spinal stenosis
2. Peripheral arterial disease
Complaint 11: Upper Abdominal Pain 1. Alcoholic hepatitis 2. Cholangitis - cholecystitis
3. Small bowel obstruction Complaint 12: Lower Abdominal Pain 1. Appendicitis
2. Colitis 3. Ectopic pregnancy
4. Pyelonephritis Complaint 13: Painful Wrist 1. Carpal tunnel syndrome
2. Rheumatoid arthritis 3. Osteoarthritis 4. Gout 5. Septic (infectious) arthritis
Complaint 14: Painful Shoulder 1. Adhesive capsulitis
2. Bicipital tendonitis 3. Rotator cuff tendonitis 4. Referred pain
Complaint 15: Sore Knee 1. Cruciate ligament injury
2. Meniscus injury 3. Osteoarthritis 4. Gout
Complaint 16: Painful Hip 1. Osteoarthritis 2. Trochanteric bursitis Complaint 17: Painful Ankle 1. Ankle fracture
2. Gout 3. Septic (infectious) arthritis 4. Second-degree ankle sprain
Complaint 18: Unsteadiness 1. Cerebral stroke 2. Cerebellar stroke 3. Acute labyrinthitis (vestibular neuronitis)
Complaint 19: Back Pain 1. Herniated disc L4-5
2. Muscle strain 3. Compression fracture

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
10
Complaint 1: Heart Murmur Prototypical diagnoses: 1. Mitral regurgitation 2. Aortic stenosis
3. Aortic sclerosis 4. Tricuspid regurgitation
Mitral
regurgitation Aortic
stenosis Aortic
sclerosis Tricuspid
regurgitation M1 Wash hands
√
√
√
√
M55: Check for jugular venous distension (JVP)
M56: Palpate aortic area
M57: Palpate pulmonic area
M58: Palpate tricuspid area
M59: Palpate mitral area
M60: Auscultate aortic area (diaphragm)
M61: Auscultate pulmonic area (diaphragm)
M62: Auscultate tricuspid area (diaphragm)
M63: Auscultate mitral area (diaphragm)
M64: Auscultate aortic area (bell)
M65: Auscultate pulmonic area (bell)
M66: Auscultate tricuspid area (bell)
M67: Auscultate mitral area (bell)
M68: Auscultate carotid artery bilaterally
M69: Palpate carotid artery bilaterally
M46: Auscultate posterior lungs fields bilaterally & symmetrically
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
11
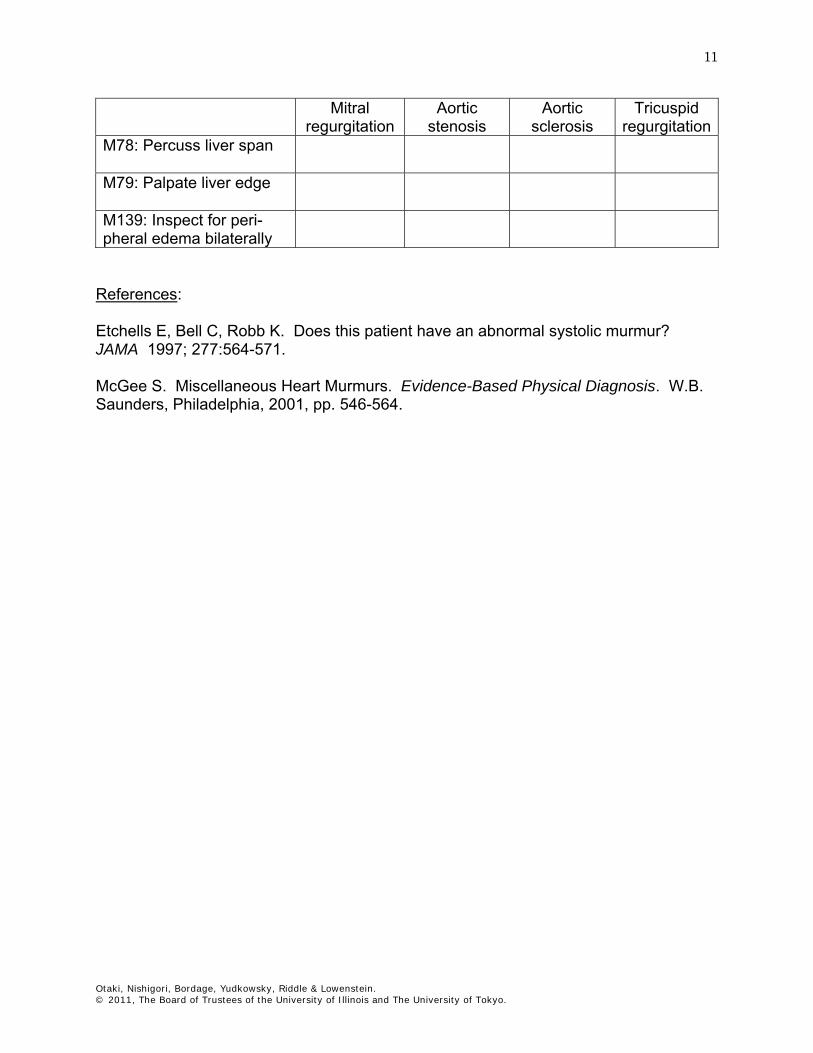
Mitral regurgitation
Aortic stenosis
Aortic sclerosis
Tricuspid regurgitation
M78: Percuss liver span
M79: Palpate liver edge
M139: Inspect for peri-pheral edema bilaterally
References: Etchells E, Bell C, Robb K. Does this patient have an abnormal systolic murmur? JAMA 1997; 277:564-571. McGee S. Miscellaneous Heart Murmurs. Evidence-Based Physical Diagnosis. W.B. Saunders, Philadelphia, 2001, pp. 546-564.
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
12
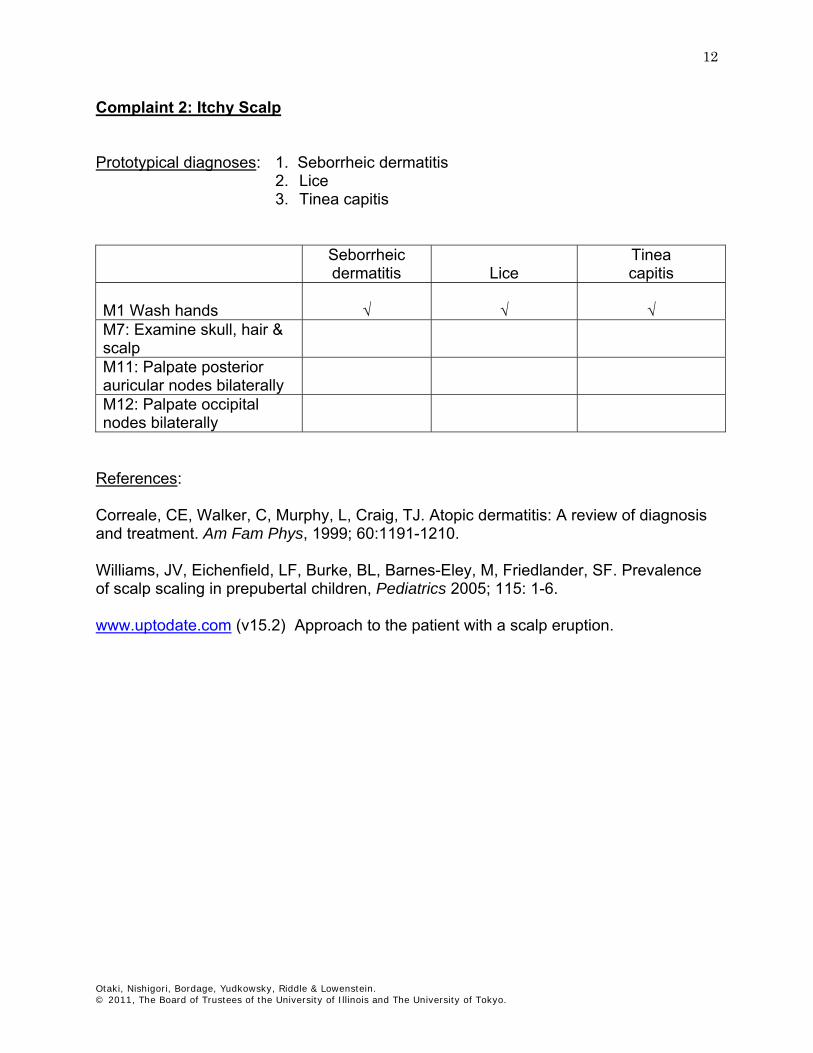
Complaint 2: Itchy Scalp Prototypical diagnoses: 1. Seborrheic dermatitis
2. Lice 3. Tinea capitis
Seborrheic
dermatitis
Lice Tinea capitis
M1 Wash hands
√
√
√
M7: Examine skull, hair & scalp
M11: Palpate posterior auricular nodes bilaterally
M12: Palpate occipital nodes bilaterally
References: Correale, CE, Walker, C, Murphy, L, Craig, TJ. Atopic dermatitis: A review of diagnosis and treatment. Am Fam Phys, 1999; 60:1191-1210. Williams, JV, Eichenfield, LF, Burke, BL, Barnes-Eley, M, Friedlander, SF. Prevalence of scalp scaling in prepubertal children, Pediatrics 2005; 115: 1-6. www.uptodate.com (v15.2) Approach to the patient with a scalp eruption.

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
13
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
14
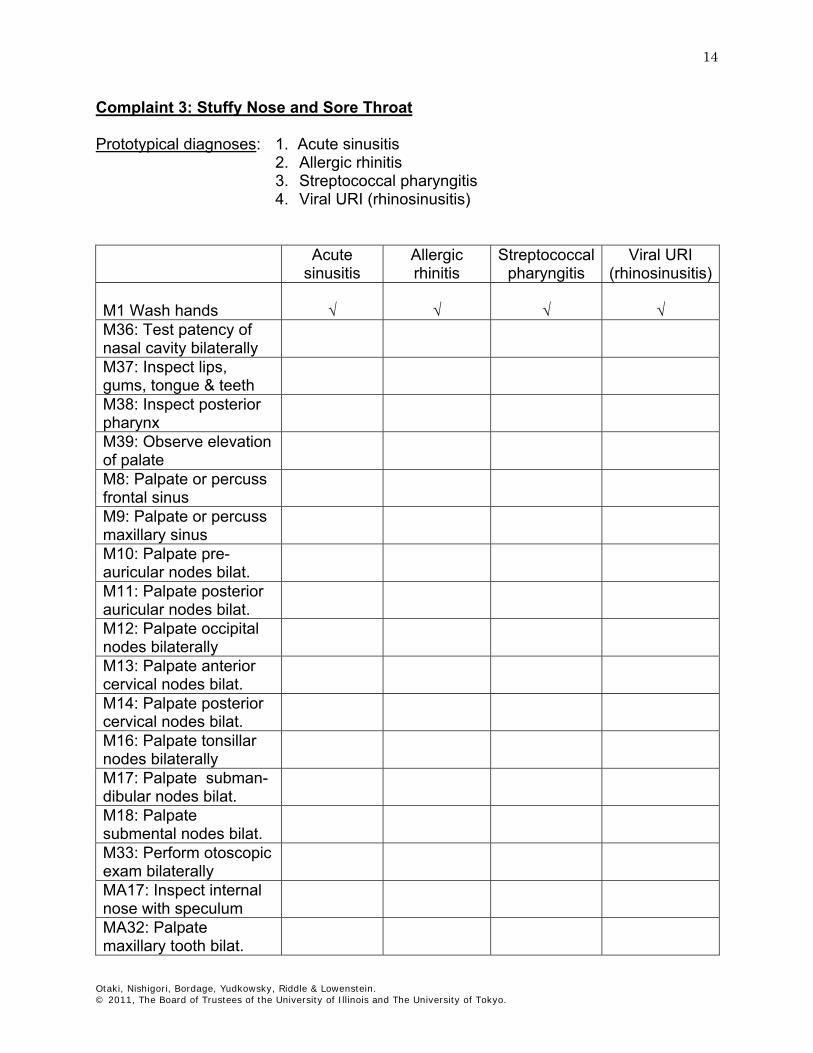
Complaint 3: Stuffy Nose and Sore Throat Prototypical diagnoses: 1. Acute sinusitis
2. Allergic rhinitis 3. Streptococcal pharyngitis 4. Viral URI (rhinosinusitis)
Acute
sinusitis Allergic rhinitis
Streptococcal pharyngitis
Viral URI (rhinosinusitis)
M1 Wash hands
√
√
√
√
M36: Test patency of nasal cavity bilaterally
M37: Inspect lips, gums, tongue & teeth
M38: Inspect posterior pharynx
M39: Observe elevation of palate
M8: Palpate or percuss frontal sinus
M9: Palpate or percuss maxillary sinus
M10: Palpate pre-auricular nodes bilat.
M11: Palpate posterior auricular nodes bilat.
M12: Palpate occipital nodes bilaterally
M13: Palpate anterior cervical nodes bilat.
M14: Palpate posterior cervical nodes bilat.
M16: Palpate tonsillar nodes bilaterally
M17: Palpate subman-dibular nodes bilat.
M18: Palpate submental nodes bilat.
M33: Perform otoscopic exam bilaterally
MA17: Inspect internal nose with speculum
MA32: Palpate maxillary tooth bilat.
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
15
References: Komaroff, AL. Some Throat and Acute Infections Mononucleosis in Adults, In Black, E.R., Bordley, D.R., Tape, T.G., & Panzer, R.J. (eds.) Diagnostic Strategies for Common Medical Problems, 2nd Edition. Philadelphia: American College of Physicians-American Society of Internal Medicine. 1999, p. 229-242. Chodosh, J. Acute Sinusitis. In Black, ER, Bordley, DR, Tape, TG, & Panzer, RJ (Eds) Diagnostic Strategies for Common Medical Problems, 2nd Ed.. Philadelphia: American College of Physicians-American Society of Internal Medicine. 1999, p. 293-296 Scheid, DC, Hamm, RM. Acute bacterial rhinosinusitis in adults. Pt I: Evaluation. Am Fam Phys, 2004; 70:1685-92. www.uptodate.com (v15.2) Clinical manifestations and evaluation of allergic rhinitis (rhinosinusitis)

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
16
Complaint 4: Swollen Neck and Fatigue Prototypical diagnoses: 1. Hypothyroidism 2. Anemia Hypothyroidism Anemia M1 Wash hands
√
√
MA10: Point out swollen area
M19: Observe thyroid gland by asking patient to swallow
M20: Palpate thyroid gland without and with swallowing
M124: Test biceps reflex bilaterally
M125: Test brachio-adialis reflex bilaterally
M126: Test triceps reflex bilaterally
M127: Test patellar reflex bilaterally
M128: Test Achilles reflex bilaterally
M27: Inspect lid, cornea & conjunctiva bilaterally
References: McGee, S. The Thyroid and Its Disorders. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 270-280 Siminoski, K. The rational clinical examination. Does this patient have a goiter? The JAMA, 1995; 273:813-817.
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
17
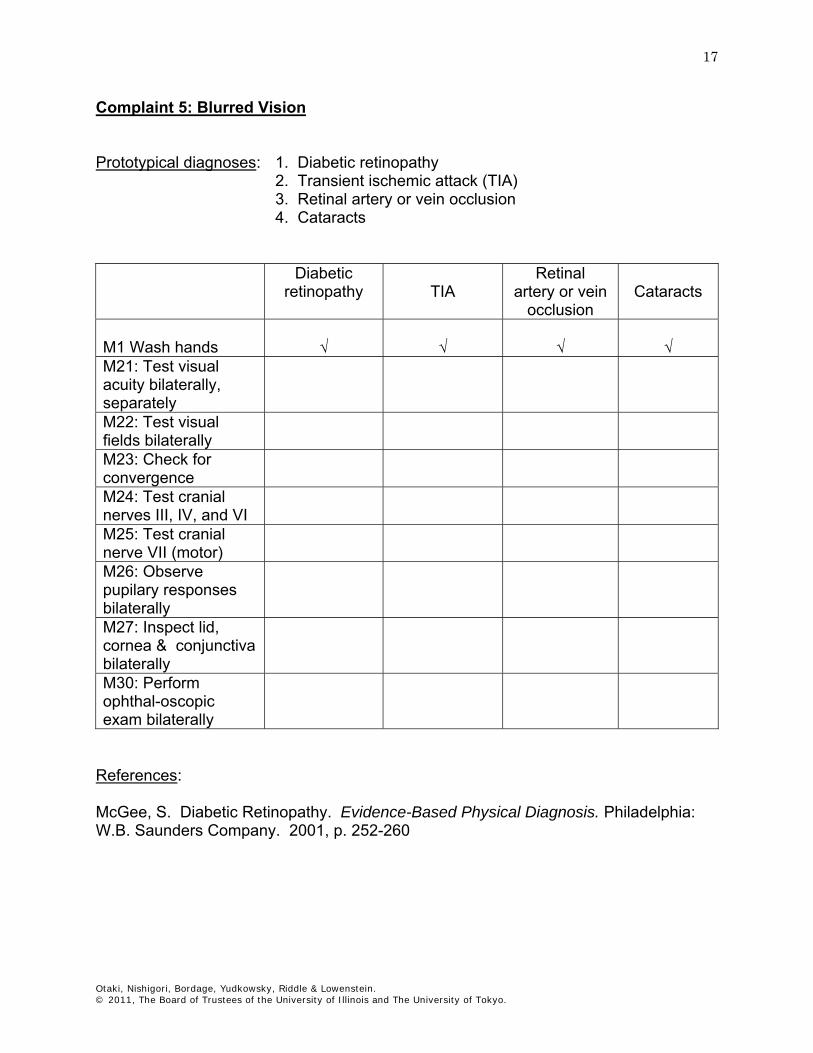
Complaint 5: Blurred Vision Prototypical diagnoses: 1. Diabetic retinopathy 2. Transient ischemic attack (TIA)
3. Retinal artery or vein occlusion 4. Cataracts
Diabetic
retinopathy
TIA Retinal
artery or vein occlusion
Cataracts
M1 Wash hands
√
√
√
√
M21: Test visual acuity bilaterally, separately
M22: Test visual fields bilaterally
M23: Check for convergence
M24: Test cranial nerves III, IV, and VI
M25: Test cranial nerve VII (motor)
M26: Observe pupilary responses bilaterally
M27: Inspect lid, cornea & conjunctiva bilaterally
M30: Perform ophthal-oscopic exam bilaterally
References: McGee, S. Diabetic Retinopathy. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 252-260
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
18
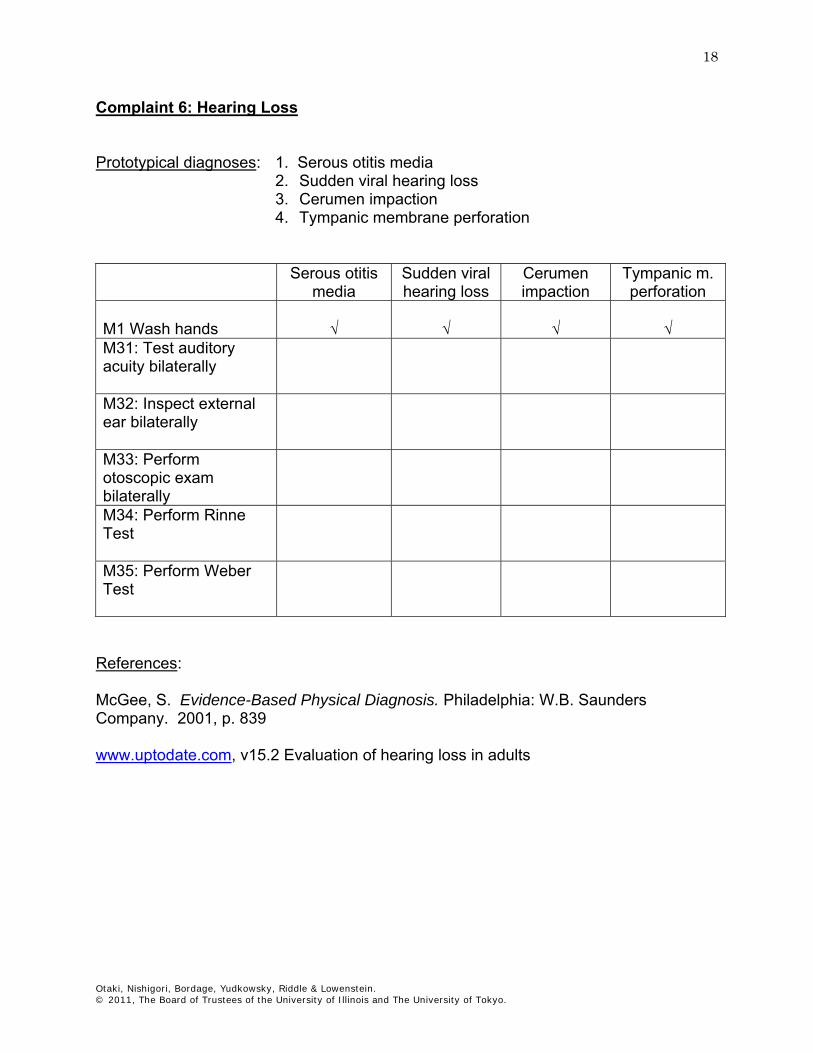
Complaint 6: Hearing Loss Prototypical diagnoses: 1. Serous otitis media
2. Sudden viral hearing loss 3. Cerumen impaction 4. Tympanic membrane perforation
Serous otitis
media Sudden viral hearing loss
Cerumen impaction
Tympanic m. perforation
M1 Wash hands
√
√
√
√
M31: Test auditory acuity bilaterally
M32: Inspect external ear bilaterally
M33: Perform otoscopic exam bilaterally
M34: Perform Rinne Test
M35: Perform Weber Test
References: McGee, S. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 839 www.uptodate.com, v15.2 Evaluation of hearing loss in adults
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
19
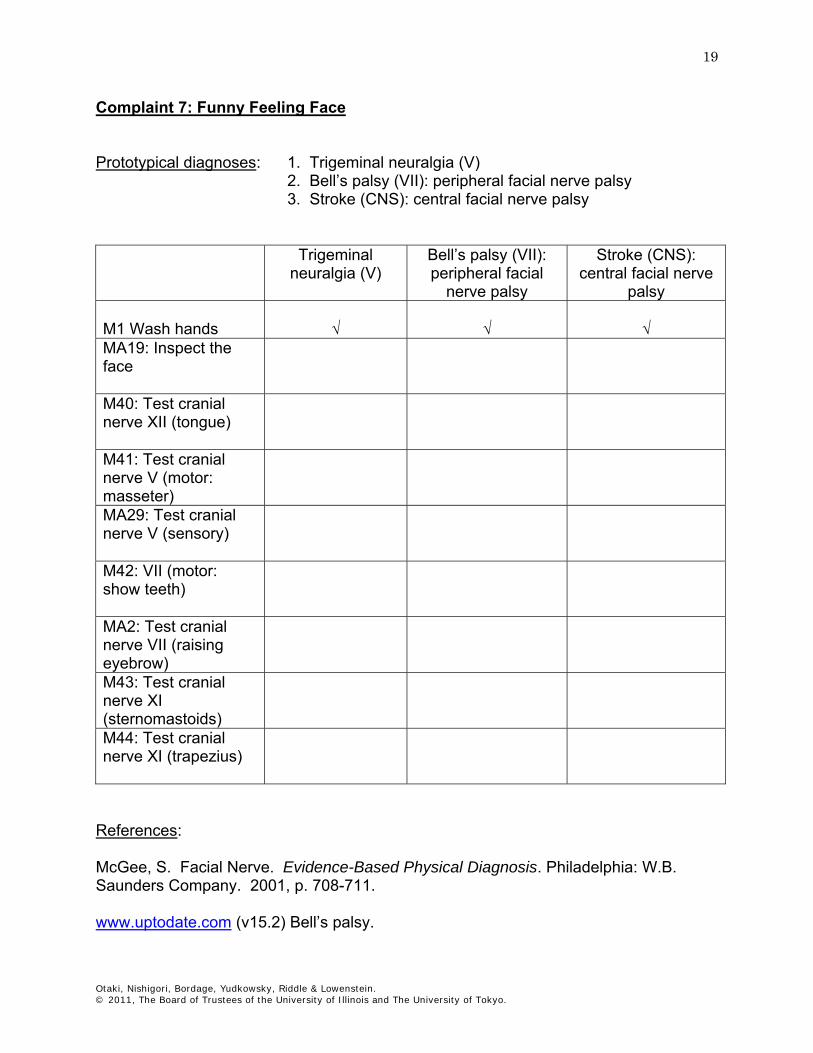
Complaint 7: Funny Feeling Face Prototypical diagnoses: 1. Trigeminal neuralgia (V)
2. Bell’s palsy (VII): peripheral facial nerve palsy 3. Stroke (CNS): central facial nerve palsy
Trigeminal
neuralgia (V) Bell’s palsy (VII): peripheral facial
nerve palsy
Stroke (CNS): central facial nerve
palsy M1 Wash hands
√
√
√
MA19: Inspect the face
M40: Test cranial nerve XII (tongue)
M41: Test cranial nerve V (motor: masseter)
MA29: Test cranial nerve V (sensory)
M42: VII (motor: show teeth)
MA2: Test cranial nerve VII (raising eyebrow)
M43: Test cranial nerve XI (sternomastoids)
M44: Test cranial nerve XI (trapezius)
References: McGee, S. Facial Nerve. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 708-711. www.uptodate.com (v15.2) Bell’s palsy.

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
20
Complaint 8: Shortness of Breath Prototypical diagnoses: 1. Asthma
2. Congestive heart failure (CHF; class 3) secondary to ischemic coronary artery disease (CAD) 3. Chronic obstructive pulmonary disease (COPD) 4. Panic attack
5. Pneumonia 6. Pulmonary embolism
Asthma CHF
secondary to ICAD
COPD Panic attack
Pneumonia Pulmonary embolism
M1 Wash hands
√
√
√
√
√
√
M4: Measure blood pressure bilaterally
M5: Palpate radial pulse
M6: Measure respiratory rate
M45: Percuss posterior lungs fields bilaterally
M46: Auscultate posterior lungs fields bilaterally
M47: Percuss anterior lung fields bilat. & symmetrical.
M48: Auscultate anterior lung fields bilat. & symmetrical.
M55: Check for jugular venous distension (JVD)
M56: Palpate aortic area
M57: Palpate pulmonic area

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
21
Asthma CHF secondary to ICAD
COPD Panic attack
Pneumonia Pulmonary embolism
M58: Palpate tricuspid area
M59: Palpate mitral area
M60: Auscultate aortic area (diaphragm)
M61: Auscultate pulmonic area (diaphragm)
M62: Auscultate tricuspid area (diaphragm)
M63: Auscultate mitral area (diaphragm)
M64: Auscultate aortic area (bell)
M65: Auscultate pulmonic area (bell)
M66: Auscultate tricuspid area (bell)
M67: Auscultate mitral area (bell)
M139:Inspect for peripheral edema bilat.
References: Badgett RG, Lucey CR, Hulvour CD. Can the clinical examination diagnose left-sided heart failure in adults? JAMA, 1997; 277:1712-9. McGee, S. Diabetic Retinopathy. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 262-260. Wang, CS, FitzGerald, JM, Schulzer, M, Mak, E, Ayas, NT. Does this dyspneic patient in the emergency department have congestive heart failure? JAMA, 2005; 294:1944- 1956.

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
22
Complaint 9: Lump in Breast Prototypical diagnoses: 1. Breast cancer
2. Fibrocystic changes Breast cancer Fibrocystic changes M1 Wash hands
√
√
M49: Inspect breasts
M50: Inspect breasts while patient raises arms outstretched above the head
M51: Inspect breasts while patient hold hands against hips
M52: Palpate auxiliary nodes (anterior, post., & prox. humerus) bilat.
M53: Inspect breasts while patient raises ipsilateral arm above head
M54: Palpate breasts bilaterally
M15: Palpate supraclavicular nodes bilaterally
References: Barton MB, Harris R, Fletcher SW. Does this patient have breast cancer? The screening clinical breast examination: should it be done? How? JAMA. 1999; 282:1270-1280. Kouides, RW, Mushlin, AI. Breast Cancer. In Black, ER, Bordley, DR, Tape, TG, Panzer, RJ (eds.) Diagnostic Strategies for Common Medical Problems, Second Edition,. Philadelphia: American College of Physicians-American Society of Internal Medicine. 1999, p. 493-496. www.uptodate.com (v15.2) Evaluation of breast lumps in primary care.
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
23
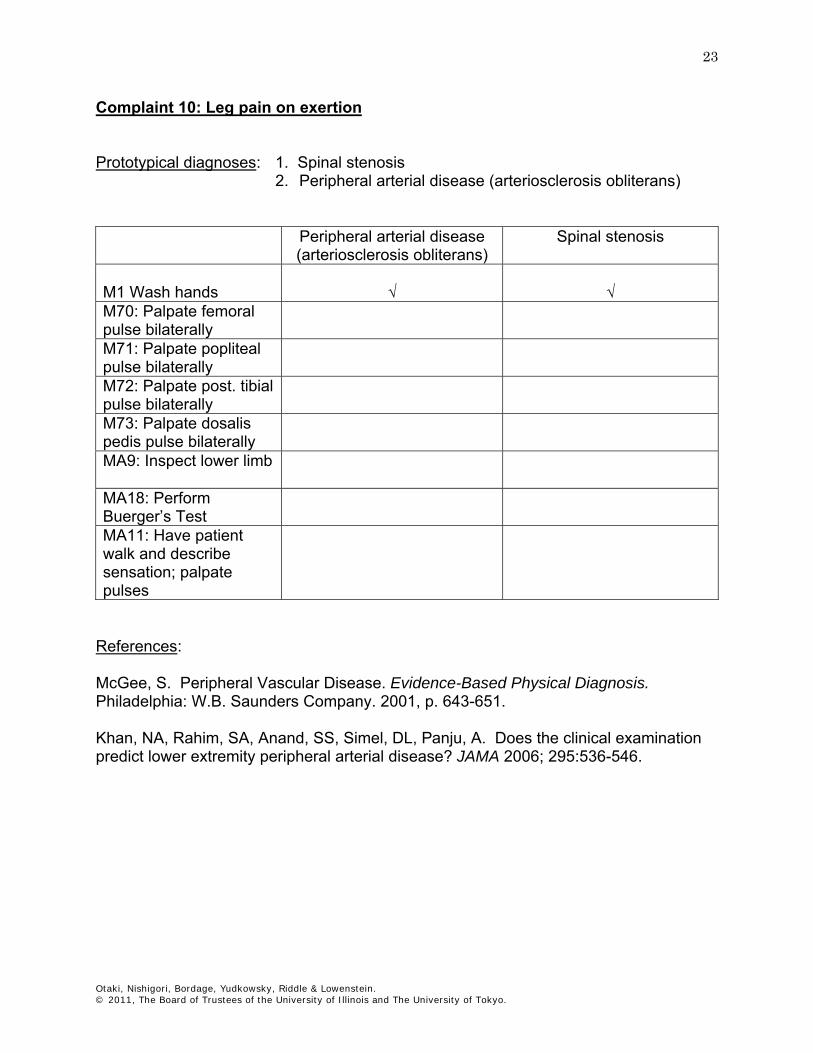
Complaint 10: Leg pain on exertion Prototypical diagnoses: 1. Spinal stenosis
2. Peripheral arterial disease (arteriosclerosis obliterans) Peripheral arterial disease
(arteriosclerosis obliterans) Spinal stenosis
M1 Wash hands
√
√
M70: Palpate femoral pulse bilaterally
M71: Palpate popliteal pulse bilaterally
M72: Palpate post. tibial pulse bilaterally
M73: Palpate dosalis pedis pulse bilaterally
MA9: Inspect lower limb
MA18: Perform Buerger’s Test
MA11: Have patient walk and describe sensation; palpate pulses
References: McGee, S. Peripheral Vascular Disease. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 643-651. Khan, NA, Rahim, SA, Anand, SS, Simel, DL, Panju, A. Does the clinical examination predict lower extremity peripheral arterial disease? JAMA 2006; 295:536-546.
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
24
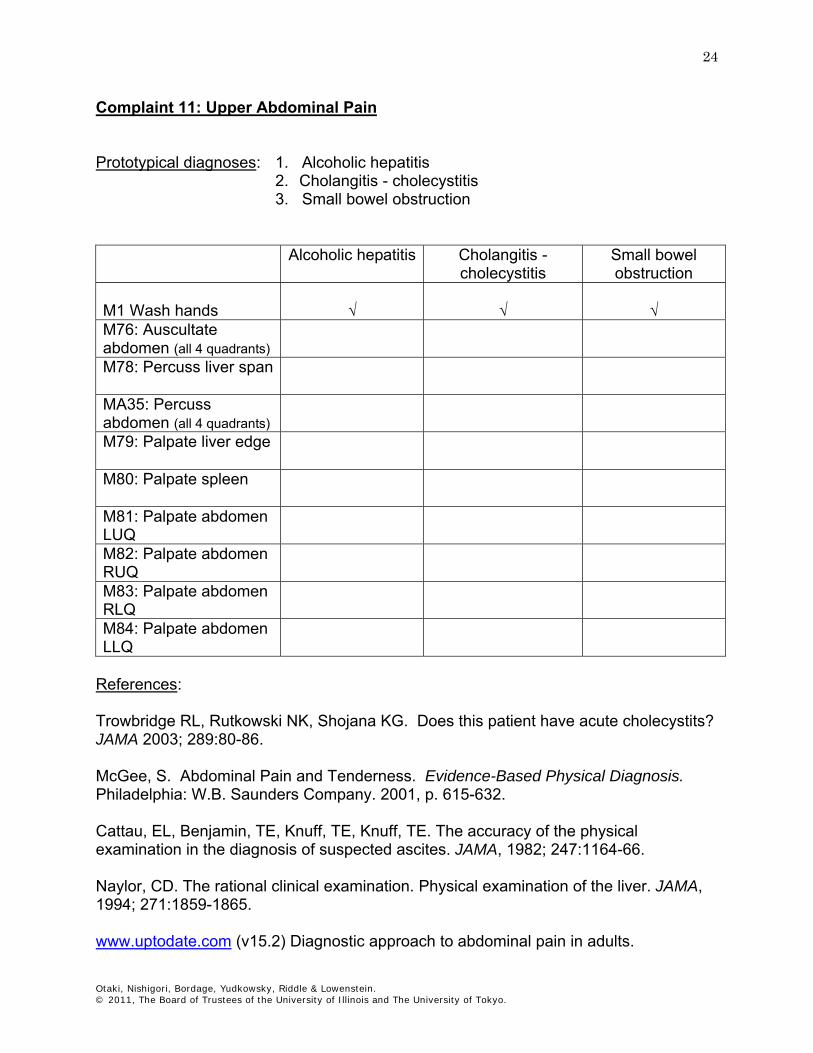
Complaint 11: Upper Abdominal Pain Prototypical diagnoses: 1. Alcoholic hepatitis
2. Cholangitis - cholecystitis 3. Small bowel obstruction
Alcoholic hepatitis Cholangitis -
cholecystitis Small bowel obstruction
M1 Wash hands
√
√
√
M76: Auscultate abdomen (all 4 quadrants)
M78: Percuss liver span
MA35: Percuss abdomen (all 4 quadrants)
M79: Palpate liver edge
M80: Palpate spleen
M81: Palpate abdomen LUQ
M82: Palpate abdomen RUQ
M83: Palpate abdomen RLQ
M84: Palpate abdomen LLQ
References: Trowbridge RL, Rutkowski NK, Shojana KG. Does this patient have acute cholecystits? JAMA 2003; 289:80-86. McGee, S. Abdominal Pain and Tenderness. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 615-632. Cattau, EL, Benjamin, TE, Knuff, TE, Knuff, TE. The accuracy of the physical examination in the diagnosis of suspected ascites. JAMA, 1982; 247:1164-66. Naylor, CD. The rational clinical examination. Physical examination of the liver. JAMA, 1994; 271:1859-1865. www.uptodate.com (v15.2) Diagnostic approach to abdominal pain in adults.

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
25
Complaint 12: Lower Abdominal Pain Prototypical diagnoses: 1. Appendicitis
2. Colitis 3. Ectopic pregnancy 4. Pyelonephritis
Appendicitis Colitis Ectopic
pregnancy Pyelonephritis
M1 Wash hands
√
√
√
√
M76: Ausculate abdomen (all 4 quadrants)
M81: Palpate abdomen LUQ
M82: Palpate abdomen RUQ
M83: Palpate abdomen RLQ
M84: Palpate abdomen LLQ
M111: Perform kidney punch bilat.
MA6: Assess for rebound tenderness
MA14: Assess for psoas sign
MA33: Perform pelvic exam
MA34: Palpate suprapubic area
MA28: Perform rectal exam
MA35: Percuss abdomen (all 4 quadrants)
References: McGee, S. Abdominal Pain and Tenderness. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 615-632. Wagner, JM. Does this patient have appendicitis? JAMA, 1996; 276:1589-1594. www.uptodate.com (v15.2) Diagnostic approach to abdominal pain in adults.
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
26
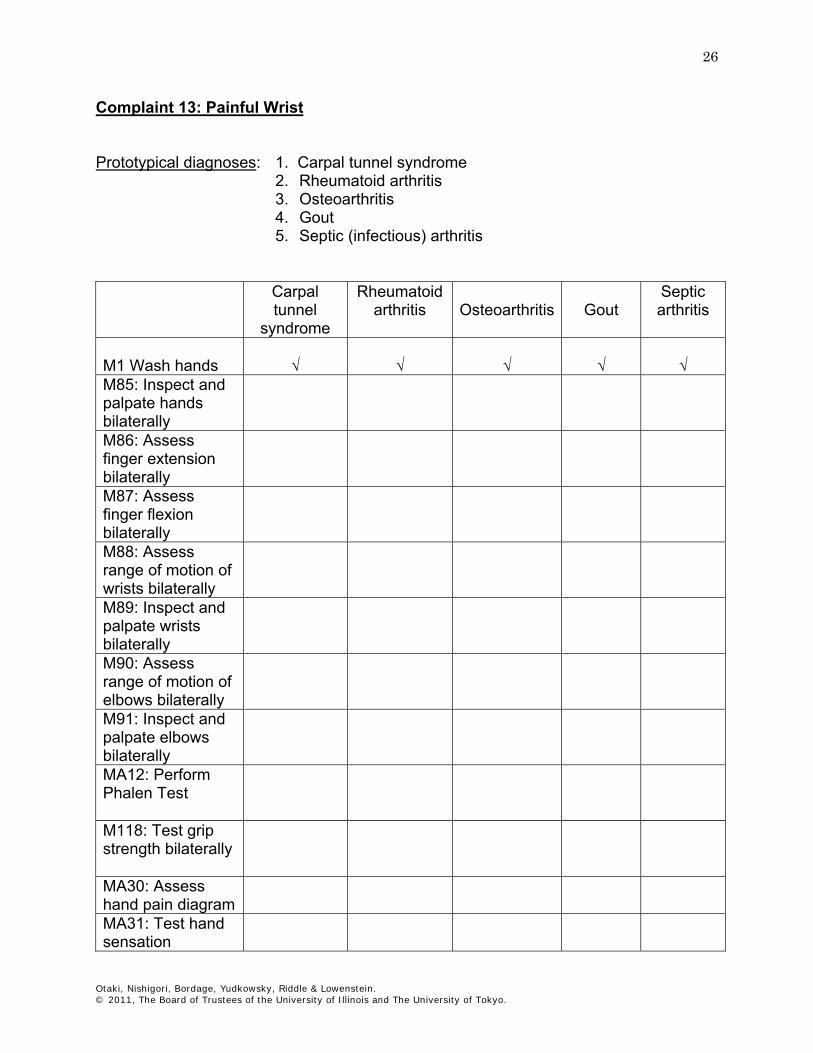
Complaint 13: Painful Wrist Prototypical diagnoses: 1. Carpal tunnel syndrome
2. Rheumatoid arthritis 3. Osteoarthritis 4. Gout 5. Septic (infectious) arthritis
Carpal
tunnel syndrome
Rheumatoid arthritis
Osteoarthritis
Gout
Septic arthritis
M1 Wash hands
√
√
√
√
√
M85: Inspect and palpate hands bilaterally
M86: Assess finger extension bilaterally
M87: Assess finger flexion bilaterally
M88: Assess range of motion of wrists bilaterally
M89: Inspect and palpate wrists bilaterally
M90: Assess range of motion of elbows bilaterally
M91: Inspect and palpate elbows bilaterally
MA12: Perform Phalen Test
M118: Test grip strength bilaterally
MA30: Assess hand pain diagram
MA31: Test hand sensation

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
27
References: D’Arcy CA, McGee S. Does this patient have carpal tunnel syndrome? JAMA 2000; 283:3110-3117. McGee, S. Peripheral Nerve Injury: Diagnosis of Carpal Tunnel Syndrome. Evidence-Based Physical Diagnosis, Philadelphia: W.B. Saunders Company. 2001, p. 803-804. www.uptodate.com (v15.2) Evaluation of the patient with wrist pain

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
28
Complaint 14: Painful Shoulder Prototypical diagnoses: 1. Adhesive capsulitis (frozen shoulder)
2. Bicipital tendonitis 3. Rotator cuff tendonitis 4. Referred pain
Adhesive
capsulitis (frozen shoulder)
Bicipital tendonitis
Rotator cuff tendonitis
Referred pain
M1 Wash hands
√
√
√
√
MA10: Have patient point out location of pain
M92: Assess shoulder flexion (empty can test)
M93: Assess shoulder internal rotation
M94: Assess shoulder external rotation
M103: Assess neck flexion
M104: Assess neck extension
M105: Assess rotation of neck bilaterally
M106: Assess lateral bending of neck bilat.
MA1: Palpate shoulder (top, lateral, anterior) bilaterally
MA15: Assess active shoulder abduction
MA16: Assess passive shoulder abduction
References: Woodward, T.W. & Best, T.M. The painful shoulder: part I. clinical evaluation. Am Fam Phys, 2000; 61:3079-88. www.uptodate.com (v15.2) Evaluation of the patient with shoulder complaints

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
29
Complaint 15: Sore Knee Prototypical diagnoses: 1. Cruciate ligament injury
2. Meniscus injury 3. Osteoarthritis 4. Gout
Cruciate
ligament injury
Meniscus injury
Osteoarthritis
Gout
M1 Wash hands
√
√
√
√
M95: Inspect and palpate knees bilat.
M96: Assess range of motion of knee bilat.
MA3: Perform McMurray test
MA4: Perform drawer Test
References: Solomon DH, Simel DL, Bates DW, Katz JN, Schaffer JL. Does this patient have a torn meniscus or ligament of the knee? Value of the physical examination. JAMA 2001; 286: 1610-1620. www.uptodate.com (v15.2) Evaluation of the adult patient with knee pain.

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
30
Complaint 16: Painful Hip Prototypical diagnoses: 1. Osteoarthritis 2. Trochanteric bursitis Osteoarthritis Trochanteric bursitis M1 Wash hands
√
√
MA10: Have patient point out location of pain
M97: Assess hip flexion bilaterally
M98: Assess external & internal hip rotation bilaterally
References: www.uptodate.com (v15.2) Evaluation of the adult with hip pain.

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
31
Complaint 17: Painful Ankle Prototypical diagnoses: 1. Ankle fracture
2. Gout 3. Septic (infectious) arthritis 4. Second-degree ankle sprain
Ankle fracture Gout Septic
(infectious) arthritis
Second-degree ankle
sprain
M1 Wash hands
√
√
√
√
MA10: Have patient point out location of pain
M99: Inspect and palpate ankle bilaterally
MA20: Palpate both ankles bilaterally
M100: Assess range of motion of ankle bilaterally
M101: Inspect mid foot and toes bilat.
M102: Inspect plantar surface bilaterally
M113: Observe gait while patient walks
MA21: Take temperature
References: Wolfe, MW, Uhl, TL, Mattacola, CG, McCluskey, LC. Management of ankle sprains. Am Fam Phys, 2001; 63:93-104. www.guidelines.gov 2006. National Guideline Clearinghouse. Ankle Sprain http://www.ncemi.org/cgi-ncemi/edecision.pl?TheCommand=Load&NewFile=ottawaankle_criteria&BlankTop=1 http://www.ohri.ca/programs/clinical_epidemiology/OHDEC/ankle_rule/flash_ankle_rule.htm (1999) Loeb Health Research Institute at the Ottawa Hospital
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
32
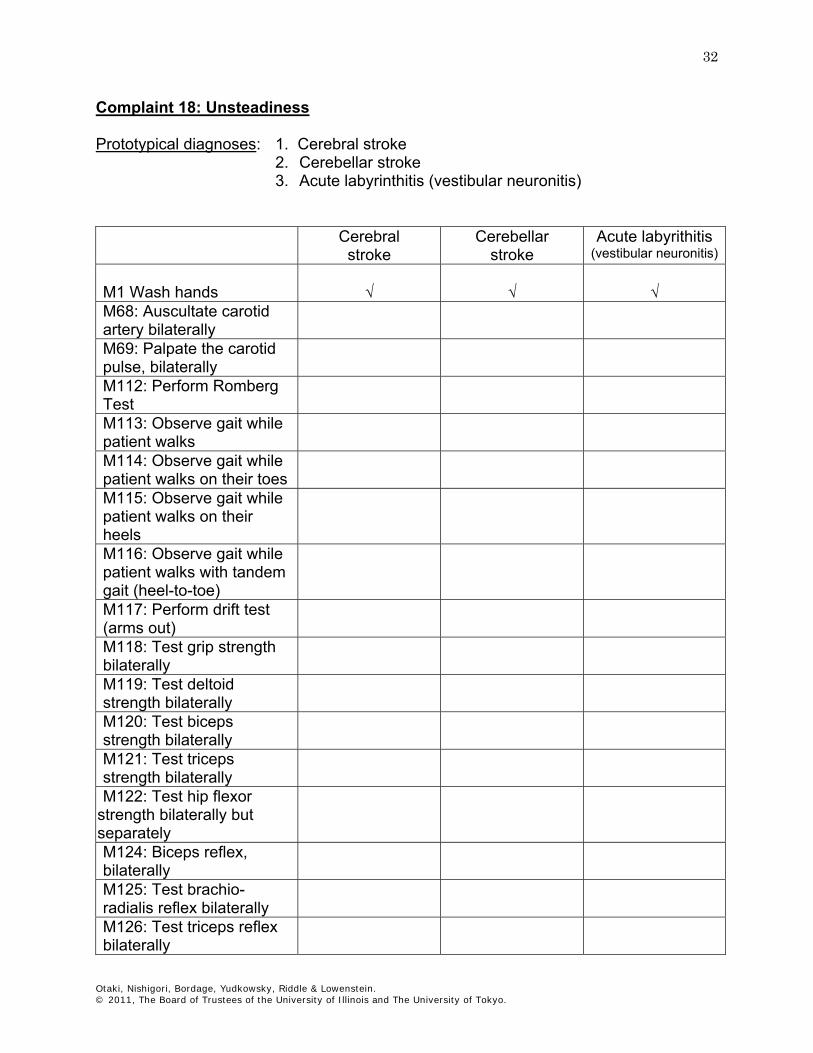
Complaint 18: Unsteadiness Prototypical diagnoses: 1. Cerebral stroke
2. Cerebellar stroke 3. Acute labyrinthitis (vestibular neuronitis)
Cerebral
stroke Cerebellar
stroke Acute labyrithitis
(vestibular neuronitis)
M1 Wash hands
√
√
√
M68: Auscultate carotid artery bilaterally
M69: Palpate the carotid pulse, bilaterally
M112: Perform Romberg Test
M113: Observe gait while patient walks
M114: Observe gait while patient walks on their toes
M115: Observe gait while patient walks on their heels
M116: Observe gait while patient walks with tandem gait (heel-to-toe)
M117: Perform drift test (arms out)
M118: Test grip strength bilaterally
M119: Test deltoid strength bilaterally
M120: Test biceps strength bilaterally
M121: Test triceps strength bilaterally
M122: Test hip flexor strength bilaterally but separately
M124: Biceps reflex, bilaterally
M125: Test brachio-radialis reflex bilaterally
M126: Test triceps reflex bilaterally

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
33
Cerebral stroke
Cerebellar stroke
Acute labyrithitis (vestibular neuronitis)
M127: Test patellar reflex bilaterally
M128: Test Achilles reflex bilaterally
M129: Perform Babinski Test bilaterally
M130: Test finger-to-nose coordination bilat.
M132: Test sharp & dull on fore arms & palms
M133: Test sharp & dull on thighs, shins & feet
M134: Test sharp & dull on trunk
M136: Test position sense bilaterally
M138: Test vibratory sense bilaterally
MA22: Perform Dix-Hallpike maneuver
MA23: Assess hip extension bilaterally
MA24: Assess knee flexion bilaterally
MA25: Assess knee extension bilaterally
MA26: Assess foot dorsiflexion bilaterally
MA27: Assess plantar flexion bilaterally
References: McGee, S. Approach to Weakness. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 733-747. McGee, S. Coordination and Cerebellar Testing. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 816-824. McGee, S. Stance and Gait,. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 63-64. Goldstein LB, Somel DL. Is this patient having a stroke? JAMA 2005; 293:2391-2402.

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
34
Complaint 19: Back Pain Prototypical diagnoses: 1. Herniated disk L4-5
2. Muscle strain 3. Compression fracture
Herniated
disk L4-5 Muscle strain Compression
fracture M1 Wash hands √ √ √ MA8: Palpate spine
M108: Assess thoraco-lumbar lateral flexion
M109: Assess lumbar flexion
M110: Assess lumbar extension
M122: Assess hip flexor bilat. but separately
M123: Test lower leg muscles strength bilat.
M127: Test patellar reflex bilaterally
M128: Test Achilles (ankle) reflex bilaterally
M133: Test sharp & dull on thighs, shins & feet
MA7: Assess straight leg raise
References: Deyo RA, Rainville J, Kent DL. What can the history and physical examination tell us about lower back pain? JAMA 1992; 268:760-765. Mazanec, DJ. Back Pain Syndromes. In Black, ER, Bordley, DR, Tape, TG, Panzer, RJ. (eds.) Diagnostic Strategies for Common Medical Problems, 2nd Edition. Philadelphia: American College of Physicians-American Society of Internal Medicine. 1999, p. 401-407. McGee, S. Nerve Roots, Plexi, and Peripheral Nerves. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders Company. 2001, p. 803-810. Speed, C. Low Back Pain, BMJ. 2004; 328:1119-21. www.uptodate.com (v15.2) Approach to the diagnosis and evaluation of low back pain in adults.

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
35
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
36
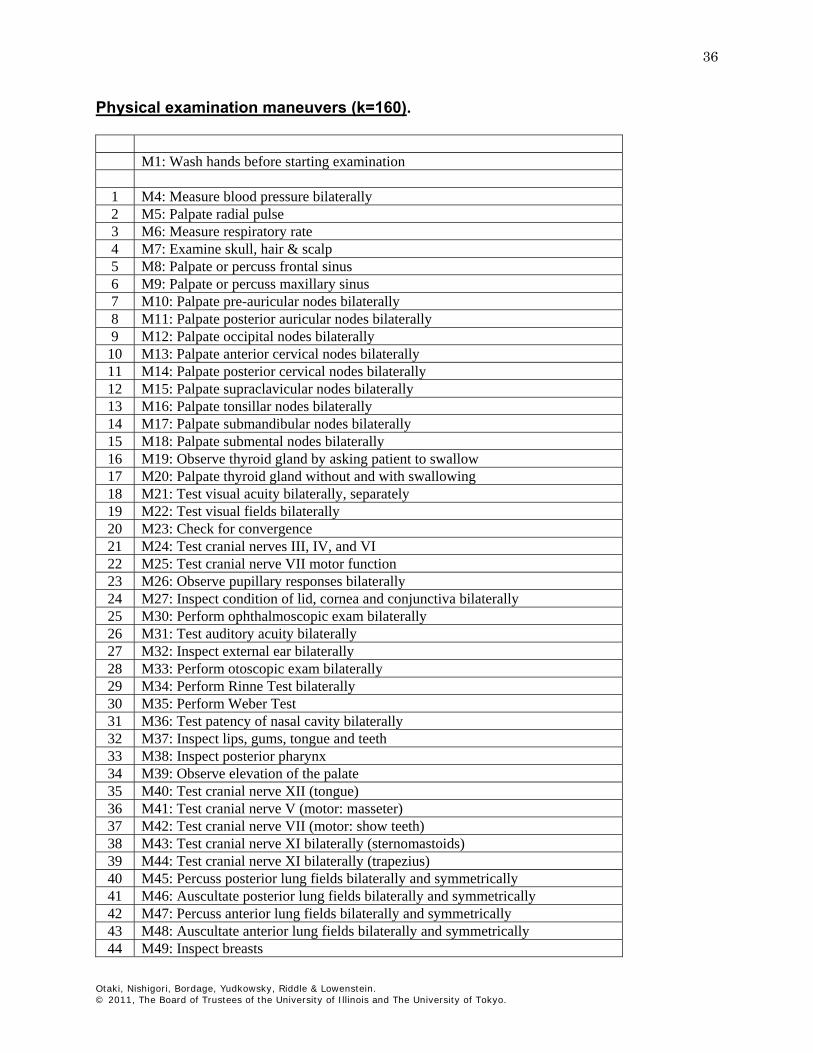
Physical examination maneuvers (k=160).
M1: Wash hands before starting examination
1 M4: Measure blood pressure bilaterally 2 M5: Palpate radial pulse 3 M6: Measure respiratory rate 4 M7: Examine skull, hair & scalp 5 M8: Palpate or percuss frontal sinus 6 M9: Palpate or percuss maxillary sinus 7 M10: Palpate pre-auricular nodes bilaterally 8 M11: Palpate posterior auricular nodes bilaterally 9 M12: Palpate occipital nodes bilaterally
10 M13: Palpate anterior cervical nodes bilaterally 11 M14: Palpate posterior cervical nodes bilaterally 12 M15: Palpate supraclavicular nodes bilaterally 13 M16: Palpate tonsillar nodes bilaterally 14 M17: Palpate submandibular nodes bilaterally 15 M18: Palpate submental nodes bilaterally 16 M19: Observe thyroid gland by asking patient to swallow 17 M20: Palpate thyroid gland without and with swallowing 18 M21: Test visual acuity bilaterally, separately 19 M22: Test visual fields bilaterally 20 M23: Check for convergence 21 M24: Test cranial nerves III, IV, and VI 22 M25: Test cranial nerve VII motor function 23 M26: Observe pupillary responses bilaterally 24 M27: Inspect condition of lid, cornea and conjunctiva bilaterally 25 M30: Perform ophthalmoscopic exam bilaterally 26 M31: Test auditory acuity bilaterally 27 M32: Inspect external ear bilaterally 28 M33: Perform otoscopic exam bilaterally 29 M34: Perform Rinne Test bilaterally 30 M35: Perform Weber Test 31 M36: Test patency of nasal cavity bilaterally 32 M37: Inspect lips, gums, tongue and teeth 33 M38: Inspect posterior pharynx 34 M39: Observe elevation of the palate 35 M40: Test cranial nerve XII (tongue) 36 M41: Test cranial nerve V (motor: masseter) 37 M42: Test cranial nerve VII (motor: show teeth) 38 M43: Test cranial nerve XI bilaterally (sternomastoids) 39 M44: Test cranial nerve XI bilaterally (trapezius) 40 M45: Percuss posterior lung fields bilaterally and symmetrically 41 M46: Auscultate posterior lung fields bilaterally and symmetrically 42 M47: Percuss anterior lung fields bilaterally and symmetrically 43 M48: Auscultate anterior lung fields bilaterally and symmetrically 44 M49: Inspect breasts

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
37
45 M50: Inspect breasts while patient raises arms outstretched above head 46 M51: Inspect breasts while patient holds hands against hips 47 M52: Palpate axillary nodes (ant., post., prox. humerus, axil.) bilat. 48 M53: Inspect breasts while patient raises ipsilateral arm above head 49 M54: Palpate breasts bilaterally 50 M55: Check for jugular venous distention 51 M56: Palpate aortic area 52 M57: Palpate pulmonic area 53 M58: Palpate tricuspid area 54 M59: Palpate mitral area 55 M60: Auscultate aortic area (diaphragm) 56 M61: Auscultate pulmonic area (diaphragm) 57 M62: Auscultate tricuspid area (diaphragm) 58 M63: Auscultate mitral area (diaphragm) 59 M64: Auscultate aortic area (bell) 60 M65: Auscultate pulmonic area (bell) 61 M66: Auscultate tricuspid area (bell) 62 M67: Auscultate mitral area (bell) 63 M68: Auscultate carotid artery bilaterally 64 M69: Palpate carotid artery bilaterally 65 M70: Palpate femoral pulse bilaterally 66 M71: Palpate popliteal pulse bilaterally 67 M72: Palpate posterior tibial pulse bilaterally 68 M73: Palpate dosalis pedis pulse bilaterally 69 M76: Auscultate abdomen, all 4 quadrants 70 M78: Percuss liver span 71 M79: Palpate liver edge 72 M80: Palpate spleen 73 M81: Palpate abdomen LUQ 74 M82: Palpate abdomen RUQ 75 M83: Palpate abdomen RLQ 76 M84: Palpate abdomen LLQ 77 M85: Inspect and palpate hands bilaterally 78 M86: Assess finger extension bilaterally 79 M87: Assess finger flexion bilaterally 80 M88: Assess range of motion of wrists bilaterally 81 M89: Inspect and palpate wrists bilaterally 82 M90: Assess range of motion of elbows bilaterally 83 M91: Inspect and palpate elbows bilaterally 84 M92: Assess shoulder flexion (empty can test) 85 M93: Assess shoulder internal rotation 86 M94: Assess shoulder external rotation 87 M95: Inspect and palpate knees bilaterally 88 M96: Assess range of motion of knees bilaterally 89 M97: Assess hip flexion bilaterally 90 M98: Assess external & internal hip rotation bilaterally 91 M99: Inspect and palpate ankle bilaterally (swelling, redness) 92 M100: Assess range of motion of ankle bilaterally 93 M101: Inspect mid foot and toes bilaterally
Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
38
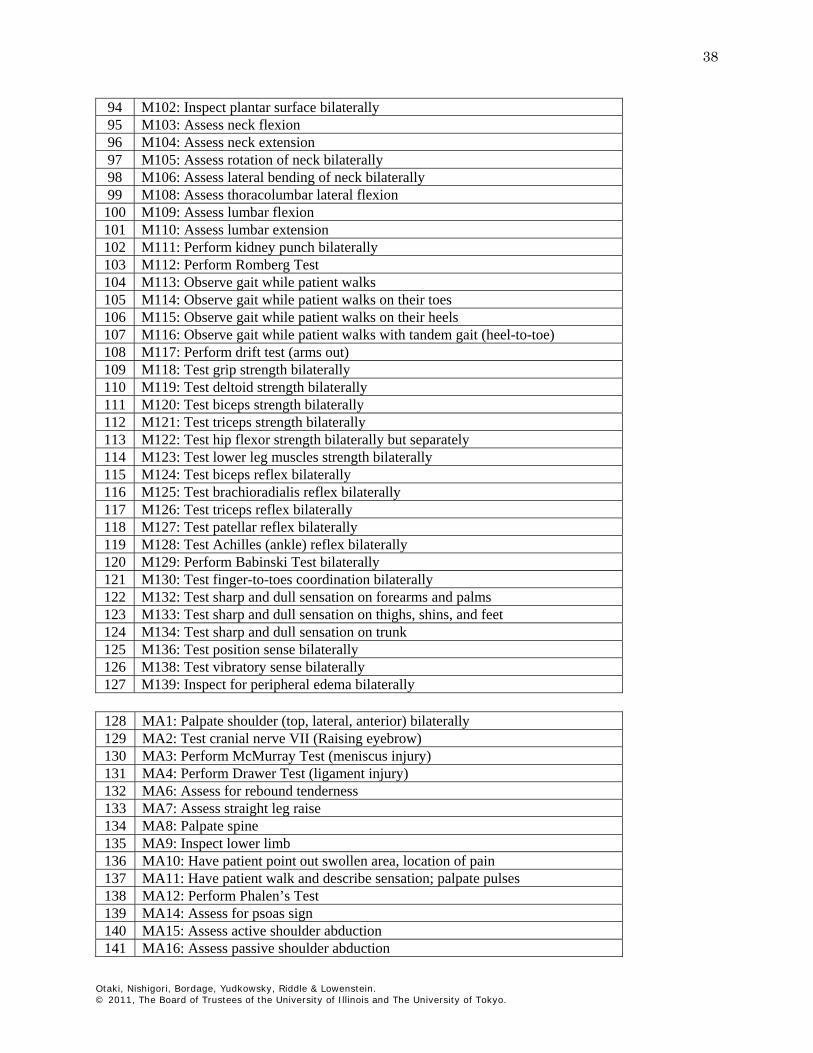
94 M102: Inspect plantar surface bilaterally 95 M103: Assess neck flexion 96 M104: Assess neck extension 97 M105: Assess rotation of neck bilaterally 98 M106: Assess lateral bending of neck bilaterally 99 M108: Assess thoracolumbar lateral flexion
100 M109: Assess lumbar flexion 101 M110: Assess lumbar extension 102 M111: Perform kidney punch bilaterally 103 M112: Perform Romberg Test 104 M113: Observe gait while patient walks 105 M114: Observe gait while patient walks on their toes 106 M115: Observe gait while patient walks on their heels 107 M116: Observe gait while patient walks with tandem gait (heel-to-toe) 108 M117: Perform drift test (arms out) 109 M118: Test grip strength bilaterally 110 M119: Test deltoid strength bilaterally 111 M120: Test biceps strength bilaterally 112 M121: Test triceps strength bilaterally 113 M122: Test hip flexor strength bilaterally but separately 114 M123: Test lower leg muscles strength bilaterally 115 M124: Test biceps reflex bilaterally 116 M125: Test brachioradialis reflex bilaterally 117 M126: Test triceps reflex bilaterally 118 M127: Test patellar reflex bilaterally 119 M128: Test Achilles (ankle) reflex bilaterally 120 M129: Perform Babinski Test bilaterally 121 M130: Test finger-to-toes coordination bilaterally 122 M132: Test sharp and dull sensation on forearms and palms 123 M133: Test sharp and dull sensation on thighs, shins, and feet 124 M134: Test sharp and dull sensation on trunk 125 M136: Test position sense bilaterally 126 M138: Test vibratory sense bilaterally 127 M139: Inspect for peripheral edema bilaterally
128 MA1: Palpate shoulder (top, lateral, anterior) bilaterally 129 MA2: Test cranial nerve VII (Raising eyebrow) 130 MA3: Perform McMurray Test (meniscus injury) 131 MA4: Perform Drawer Test (ligament injury) 132 MA6: Assess for rebound tenderness 133 MA7: Assess straight leg raise 134 MA8: Palpate spine 135 MA9: Inspect lower limb 136 MA10: Have patient point out swollen area, location of pain 137 MA11: Have patient walk and describe sensation; palpate pulses 138 MA12: Perform Phalen’s Test 139 MA14: Assess for psoas sign 140 MA15: Assess active shoulder abduction 141 MA16: Assess passive shoulder abduction

Otaki, Nishigori, Bordage, Yudkowsky, Riddle & Lowenstein. © 2011, The Board of Trustees of the University of Illinois and The University of Tokyo.
39
142 MA17: Inspect internal nose with speculum 143 MA18: Perform Buerger’s Test 144 MA19: Inspect the face 145 MA20: Palpate ankle bilaterally 146 MA21: Take temperature 147 MA22: Perform Dix-Hallpike maneuver 148 MA23: Assess hip extension bilaterally 149 MA24: Assess knee flexion bilaterally 150 MA25: Assess knee extension bilaterally 151 MA26: Assess foot dorsiflexion bilaterally 152 MA27: Assess plantar flexion bilaterally 153 MA28: Perform rectal exam 154 MA29: Test cranial nerve V (sensory) 155 MA30: Assess hand pain diagram 156 MA31: Test hand sensation 157 MA32: Palpate maxillary tooth bilaterally 158 MA33: Perform pelvic exam 159 MA34: Palpate suprapubic area 160 MA35: Percuss abdomen, all 4 quadrants