Embed Size (px)
Citation preview

[↓Na+]Busting Myths and de-Mist-ifying its
Assessment & Management
Peter LoewenB.Sc.(Pharm), ACPR, Pharm.D., FCSHP
Faculty of Pharmaceutical SciencesThe University of British Columbia
Lower Mainland Pharmacy Services
COI Disclosure[↓Na+]
By the end of the session, and upon further learning and reflection participants should be able to: 1. Correctly use the terms “hypovolemia” and
“dehydration”.2. Demonstrate an APPROACH to evaluating [↓Na+] in a
patient and its potential cause.3. Describe drug-related causes of [↓Na+] and treatment
approaches tuned to the cause.4. Diagnose or rule out SIADH and implement a
treatment approach if detected.
OBJECTIVES [↓Na+]
www.peterloewen.com/made

Patterson JH. Hospital Pharmacy 2011;46:S3–S10.
[↓Na+]is COMMON
has CLINICAL CONSEQUENCES
mortality, CNS, hip fracture, heart failureeconomic impacts
[↓Na+]
Zilberberg MD et al. Curr Med Res Opin 2008;24:1601–8Upadhyay A, et al. Am J Med 2006;119:S30–5Waikar SS, et al. Am J Med 2009;122:857–65Wald R, et al. Arch. Intern. Med. 2010;170:294
Patterson JH. Hospital Pharmacy 2011;46:S3–S10.
[↓Na+] and Heart Failure[↓Na+]
2/3 1/3
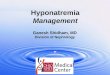
Intracellular fluid (ICF) Extracellular fluid (ECF)
intra
vasc
ular
wat
er
interstitial water
3/4 1/4
cell
mem
bran
e
H2O H2O
Na+
Total body water (TBW) = 0.6* x total body weight *More precisely: 0.45 for elderly female, 0.5 for non-elderly female or elderly male, 0.6 for non-elderly male.
Where’s your water?
Intracellular osmolality must be maintained for cells to function. Plasma osmolality will be sacrificed in either direction to achieve this.
H2O freely crosses cell membranes. Na+ doesn’t. Intracellular osmoles are mostly large proteins that don’t move.

DRUG THERAPY
[↓Na+] CASEKP is a 77 y/o M brought to ED from home because of increasing lethargy and confusion over the past 48 hours. He has had diarrhea for the past 4 days subsequent to a course of cefuroxime for mild CAP, and has been receiving HCTZ 25 mg/d for one year for ISH.
PMH: HTN. CAP.
O/E: Oriented x 3. 100/60 supine, 75/45 standing. HR 65 supine, 80 standing. Postural dizziness. JVP <2cm ASA.
[↓Na+]
↑ hypernatremia
(↓ ICF) ↓
hyponatremia
(↑ ICF)
Serum [Na+] �135-145 mmol/L
Assess the ICF
↑ hypernatremia
(↓ ICF) ↓
hyponatremia
(↑ ICF)
Serum [Na+] �135-145 mmol/L
Assess the ICF
assess the ECF
[↓Na+]

assess the ECF[↓Na+] assess the ECF[↓Na+]
CASE [↓Na+]KP is a 77 y/o M brought to ED from home because of increasing lethargy and confusion over the past 48 hours. He has had diarrhea for the past 4 days subsequent to a course of cefuroxime for mild CAP, and has been receiving HCTZ 25 mg/d for one year for ISH.
PMH: HTN. CAP.
O/E: Oriented x 3. 100/60 supine, 75/45 standing. HR 65 supine, 80 standing. Postural dizziness. JVP <2cm ASA.
[↓Na+]

[↓Na+]
Zarychanski R, et al. JAMA 2013;309:678–88.
In hypovolemic [↓Na+], is the Na+ in the NS raising your patient’s
serum [Na+]?
[↓Na+]
ADH[↓Na+]
ICF ECF
IV
H2O goes in Intracellular
tonicity decreases
Need to maintain “normal”
intracellular tonicity
H2O moves [Na+] ↓
How does excess ICF cause hyponatremia?

ICF ECF
How does loss of ICF cause hypernatremia?
H2O leaves [loop diuretics,
fever] Intracellular
tonicity increases
Need to maintain “normal”
intracellular tonicity
H2O moves [Na+] ↑
IV
How much water should you drink?
[↓Na+]
How much water should you drink?
[↓Na+]What makes you
thirsty?
[↓Na+]

SITUATION
“Hey, pharmacist, I’ve got a patient here with a serum Na of 122 and they’re on [insert any drug name that starts with “c”]. I think they’ve probably got SIADH. Fix it, please.”
[↓Na+] assess the ECF
Does my patient have SIADH?
[↓Na+] in a non-hypovolemic patient...[↓Na+]
Holm EA, et al. South. Med. J. 2009;102:380–4.

CASERQ is a 67 y/o white M admitted from home for general malaise and increasing confusion for one week.
PMH: Carcinoma of the bronchus (surgical resection and radiation therapy) 4 months ago; Mild HTN x 5 y (metoprolol 100 mg po bid);Depression (diagnosed 4 months ago and treated with fluoxetine 50 mg/d)
O/E: Moderately obese, disoriented white male. BP 150/85 supine, 145/85 standing. HR 70 supine, 75 standing. Temp 36.8C, Wt. 100 kg, JVP 3 cm ASA.
[↓Na+] Managing SIADH[↓Na+]1. Identify & remove cause 2. H2O restriction (<1000 or <500 ml/d)3. Furosemide4. Salt liberalization (eg, >10g/d) 5. Fludrocortisone
6. Lithium / Demeclocycline / Tolvaptan
Managing SIADH[↓Na+]EVEREST
QUESTSALT 1 & 2
EVEREST. JAMA 2007;297:1319–31QUEST. Cardiovasc Drugs Ther 2011;25 Suppl 1:S33–45
SALT 1 & 2. NEJM 2006;355:2099–112
[↓Na+]
Dinicolantonio JJ, et al. Heart 2013; (10.1136/heartjnl-2012-302337)
6 RCTs (N=2747) comparing low-Na diets (1.8 g/day) with normal Na diets (2.8 g/d) in patients with systolic HF
HF readmission 1.83 (1.62-2.06)Mortality 1.95 (1.66-2.29)Sudden death 1.72 (1.21-2.44)HF death 2.23 (1.77-2.81)

Putting it all together...
[↓Na+] CASEID: 74 year old M admitted 1 week ago for failure to thrive. On admission his [Na+] was 128. Today it’s 133.
PMH: HTN, chronic angina, MI 5 years ago.
MPTA: ramipril 5mg, ASA 81mg/d, metoprolol 100mg bid, atorvastatin 80mg/d.
[↓Na+]
COURSE: He got some volume in ED, ramipril was continued, and today is [Na] is 133. Someone sometime in the intervening days wondered whether he had SIADH and ordered urine electrolytes: Na+ was 14, UOsm was 512.
“Can ramipril cause hyponatremia?
[↓Na+]
Peter LoewenB.Sc.(Pharm), ACPR, Pharm.D., FCSHP
Faculty of Pharmaceutical SciencesThe University of British Columbia
Lower Mainland Pharmacy Services
Busting Myths and de-Mist-ifying its Assessment & Management