-
8/2/2019 Hypoglycaemia Final
1/31
NEONATAL HYPOGLYCAEMIA
-
8/2/2019 Hypoglycaemia Final
2/31
DEFINITION
Glucose delivery or availability is inadequate tomeet glucose
demand.
KarlsenK.TheSTABLEProgram.STABLEProgram, Utah. 2001.
< 2.6mmol/L in term and preterm infants Peads protocol
50 110 mg/dl (2.75 6.05 mmol/L) (Karlsen, 2006)
> 40 mg/dl (2.2 mmol/L)(Verklan & Walden, 2004)
> 30 term (1.65mmol/L)
> 20 preterm (1.10 mmol/L)(Kenner & Lott, 2004)
> 45 mg/dl (2.47mmol/L)(Cowett, R. as cited by
Barnes-Powell,2007)
-
8/2/2019 Hypoglycaemia Final
3/31
Hypoglycemia is the most common metabolic
problem in neonates.
1.3-3 per 1000 live births emed
-
8/2/2019 Hypoglycaemia Final
4/31
Clinical features
Jittery and irritabilityApnoea and cyanosis
Hypotonia
Poor feedingConvulsions
Asymptomatic
-
8/2/2019 Hypoglycaemia Final
5/31
Why is it a problem
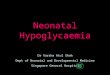
Glucose is the primary fuel for the brain.
The brain needs a steady supply of glucose to
function normally.
Glucose is the fetuss only
source of carbohydrate.
Fig. 1 Bilateral occipital lesions typical of
neonatal hypoglycemic brain injury
-
8/2/2019 Hypoglycaemia Final
6/31
Compared with adults, infants have a higher
brain to body weight ratio, resulting in higher
glucose demand in relation to glucose
production capacity.
Cerebral glucose
utilization accounts for90% of the neonates
glucose consumption
-
8/2/2019 Hypoglycaemia Final
7/31
Karlsen, 2006
Preparation for Birth
Fetal plasma glucose is 60 80% of the
maternal glucose level.
The fetus stores glucose in the form of
glycogen (liver, heart, lung, and skeletal
muscle).
Most of the glycogen is made and stored in
the last month of the 3rd trimester.
-
8/2/2019 Hypoglycaemia Final
8/31
Haney, 2005
Preparation for Birth
The fetus has limited ability to convert
glycogen to glucose and must rely upon
placental transfer of glucose to meet energy
needs.
When the infant is born, the cord is cut and
so is the major supply of glucose!
-
8/2/2019 Hypoglycaemia Final
9/31
Haney, 2005
Preparation for Birth
The transition from fetus to newborn creates
a significant energy drain on the newborn.
The newborn is now required to meet
increased metabolic demands while changing
the energy source from a placenta-supplied
source to an external food source.
-
8/2/2019 Hypoglycaemia Final
10/31
Whos at Risk? What could be the
cause?
3 basic mechanisms
Limited glycogen stores
Hyperinsulinism
Diminished glucose production
-
8/2/2019 Hypoglycaemia Final
11/31
Limited Glycogen store/supply
Prematurity
Perinatal stress/distress
SGA
Disorders of Glycogen metabolism Glucose 6-phosphatase def
Amylo-1,6 glucosidase def
Phosphorylase def limit either glycogen metabolism or glucose
release resulting
in excess glycogen stores,hepatomegaly and
hypoglycemia-inherited primarily as autosomal recessive
-
8/2/2019 Hypoglycaemia Final
12/31
Hyperinsulinism
Infant of Diabetic mother
Beckwith Wiedemann Syndrome
Maternal Drug Effects on neonatal glucose
metabolism Chlorpromazine & benzothiazides
Propanolol
Terbutaline
Inappropriate intrapartum maternal glucoseadministration
-
8/2/2019 Hypoglycaemia Final
13/31
Diminished Glucose Production
SGA
Decreased glycogen stores and impaired
gluconeogenesis
Inborn error of metabolism
Aminoacidopathies (amino acids involved in
gluconeogenesis)
-
8/2/2019 Hypoglycaemia Final
14/31
Others
Hypothermia, Sepsis, Perinatal asphyxia
Normal glycogen stores but inadequate to meetincrease energy
demand
Cortisol and Growth hormone deficiencies Secondary to effects on
hepatic glycogenolysis and
gluconeogenesis
Polycythemia
Direct result of increased glucose consumption by thered cell
massas well as secondary to effects on theintestinal absorption of
substrates.
-
8/2/2019 Hypoglycaemia Final
15/31
High Risk Infants
Infants of diabetic mothers
Small for gestational age
Preterm infants
Macrosomic infants wt > 4.0 kg
Sick babies including
Perinatal asphysia
Sepsis Hypothermia
Polycythaemia
-
8/2/2019 Hypoglycaemia Final
16/31
Management
Prevention and early detection
Identification of babies as risk
Immediate feeding
Supplement feeding until breastfeeding
astablished
Regular glucometer monitoring
-
8/2/2019 Hypoglycaemia Final
17/31
If blood sugar levels < 2.6 mmol/l or
symptomatic
Iv bolus D10% at 2-3 ml / kg
D10% drip at 60-90ml/kg/day
-
8/2/2019 Hypoglycaemia Final
18/31
Glucose monitoring should be done hourly
until reflo stable >2.6mmol/l for 2 readings
Then 2 hourly x 2
Then 4 6 hourly
-
8/2/2019 Hypoglycaemia Final
19/31
Glucose requirement
Glucose requirement (mg/kg/min) for IV Drip% dextrose x rate
(ml/hour)
weight (kg) x 6
Glucose requirement (mg/kg/min) for formulafeeds
(g of glucose per day) x 1000Wt x 24 x 60
Total glucose requirements target 6 to 8 mg/kg/min
formula feeding = 7.5 gm in 100 ml
glucose in (g) per day
= total feeding (ml) x 7.5
100
-
8/2/2019 Hypoglycaemia Final
20/31
Importance of glucose load
Numerical measurement of a current regime
Maintain a similar glucose load if
hypoglycaemia is controlled with a particular
IV dextrose regime
Allow calculations of a mix formula feeding and IV
dextrose.
Step up glucose delivery if persistenthypoglyceamic
-
8/2/2019 Hypoglycaemia Final
21/31
IV glucagon 30 100 mcg/ kg over 20 mins
or
IM glucagon 100 mcg/kg (maximum 3 doses
Should not be used in SGA patients where liver
stores are reduced
-
8/2/2019 Hypoglycaemia Final
22/31
Investigations
RBS
FBC
Urine ketone
Se cortisol
Growth hormone
Insulin level
VBG
Review cord tsh
-
8/2/2019 Hypoglycaemia Final
23/31
Failure to find large ketones with
hypoglycemia suggests that fat is not being
metabolized from adipose tissue
(hyperinsulinism) or that fat cannot be usedfor ketone body
formation (enzymatic defects
in fatty acid oxidation)
-
8/2/2019 Hypoglycaemia Final
24/31
Neonates with symptomatic
hyperinsulinemic hypoglycemia generate
inappropriately low serum cortisol
counterregulatory hormonal responses
-
8/2/2019 Hypoglycaemia Final
25/31
B/O N Delivered at
EMLSCS in view of macrosomia
Apgar score 9/10
Suctions clear BW 4.55 kg
Mother BG A +ve
HIV/VDRL NR
Antenatally Type 2 diabetes
HbA1c 7.0%
Total insulin usage 40 units per day
-
8/2/2019 Hypoglycaemia Final
26/31
No risk of sepsis
No prematurity
No pprom
No chorioamionitis
No maternal pyrexia
-
8/2/2019 Hypoglycaemia Final
27/31
Admitted at 4 hours of life in view of infant of
diabetic mother for observation
Reflo at 4 hours of life 2.9mmol/L
Was started on feeding 80cc/kg/day
Repeated reflo post feeding was 2.7mmol/L
-
8/2/2019 Hypoglycaemia Final
28/31
On exmination
Hypotonia
Jittery on provocation
No cyanosis No seizure
No apnoea
No rapid breathing No hepatospleenomegaly
No macroglosia
-
8/2/2019 Hypoglycaemia Final
29/31
Plan
1. IV D10% 10 cc slow bolus
2. IV D 10% 9.5 ml / hour
total fluid 50 ml/kg/day
3. Total feeding 30ml / 3 hourly
total fluid 50 ml/kg/day
4. IM glucagon 0.2 mg stat
-
8/2/2019 Hypoglycaemia Final
30/31
5. If persistant hypoglycaemia
-
8/2/2019 Hypoglycaemia Final
31/31
6. If still hypoglycaemic, to increase concentration to12.5%IV
D12.5% 11.5 ml/hour = 5.3feeding 35ml/3 hourly = 3.2
total glucose load = 8.5 mg/kg/min7. If still persistent, to
increase concentration to 15%and start glucagon infusion
10mcg/kg/hourIV D15% 11.5 ml/hour = 6.3feeding 35ml/3 hourly =
3.2
total glucose load = 9.5 mg/kg/min