Embed Size (px)
Citation preview

Medical & Pharmaceutical Sciences UNIVERSITÉ DE FRANCHE-COMTÉ
YEAR 2017 NO. 17 — 01
Hypocortisolaemia in athletes: focus on causes and risks incurred
THESIS
Presented and supported publicly
On Tuesday, 04 April 2017
To obtain the State Diploma of
DOCTOR OF MEDICINE
BY
Samuel MARAFFI
Born 13 July 1988 in Vesoul (Haute-Saône)
The composition of the jury is as follows:
Chairman: Prof. Gilles DUMOULIN Professor
Thesis director: Dr. Jacky Maillot Doctor
Judges: Prof. Rémi BARDET Professor
Dr. Clément PRATI Dr. Senior Lecturer Hospital
Fabrice MICHEL Practitioner
Dr. Armand MEGRET National Federal Physician
| UFR SMP 19 rue Ambroise Paré — CS 71806 F-25030 Besançon cedex | Tel. +33 (0)3 63 08 22 00 | Fax +33 (0)3 81 66 56 83
| http://medecine-pharmatie.univ-fcomte.fr

Page | 2
Director of Studies
Prof. Xavier BERTRAND Deputy Director Prof. Laurence NICOD Director of Studies Ms. Florence PRETOT
UNIVERSITÉ DE FRANCHE-COMTÉ
U. F.R. OF MEDICAL & PHARMACEUTICAL SCIENCES OF BESANCON
DIRECTOR
MEDICAL ASSESSORS
DEAN OF PHARMACY
PHARMACY ASSESSOR
Prof. Thierry MOULIN
Prof. Gilles CAPELLIER
Prof. Catherine CHIROUZE
Prof. Marie-France SERONDE
Prof. Jean-Paul FEUGEAS
ADMINISTRATIVE SUPERVISOR
UNIVERSITY PROFESSORS – HOSPITAL PRACTITIONERS
Mr. Olivier
Mr. Frédéric
Mr. François
Ms. Yvette
Ms. Alessandra
Mr. Hugues
Mr. Christophe
Mr. Hatem
Mr. Jean-Luc
Mr. Gilras
Mr. Joan-Marc
Ms. Catherine
Mr. Sidney
Mr. Jean-Luc
Ms. Cécile
Mr. Alain
Mr. Jean-Charles
Mr. Siamak
Mr. Benoît
Mr. Eric
Mr. Bruno
Mr. Eric
Mr. Bernard
Mr. Thibaut
Mr. Vincent
Mr. Didier
Mr. Gilles
Mr. Dominique
Mr. Jean-Paul
Mr. Patrick
Mr. Emmanuel
ADOTEVI
AUBER
AUBIN
BERNARD
BIONDI
BITTARD
BORG
BOULANDOU
BRESSON
CAPELLIER
CHALOPIN
CHIROUZEC
CHOCRON
CHOPARD
COURIVAUD
CZORNY
DALPHIN
DAVANI
DE BILLY
DECONINCK
DEGANO
DELABROUSSE
DELBOSC
DESMETTRE
Di MARTINO
DUCLOUX
DUMOULIN
FELLMANN
FEUGEAS
GARBUIO
HAFFEN
IMMUNOLOGY
PAEDIATRIC SURGERY
DERMATO-VENEREOLOGY
CARDIOLOGY
RADIOLOGY AND MEDICAL IMAGING
UROLOGY
ONCOLOGY
BIOPHYSICS AND NUCLEAR MEDICINE
DEVELOPMENTAL AND REPRODUCTIVE BIOLOGY AND MEDICINE
INTENSIVE CARE
NEPHROLOGY
INFECTIOUS DISEASES
THORACIC AND CARDIOVASCULAR SURGERY
LEGAL MEDICINE AND HEALTH CARE LAW
NEPHROLOGY
NEUROSURGERY
PNEUMONOLOGY
CLINCAL PHARMACOLOGY
PAEDIATRIC SURGERY
HAEMATOLOGY
PSYCHOLOGY
RADIOLOGY AND MEDICAL IMAGING
OPHTHALMOLOGY
EMERGENCY MEDICINE
HEPATOLOGY
NEPHROLOGY
PHYSIOLOGY
CYTOLOGY AND HISTOLOGY
BIOCHEMISTRY AND MOLECULAR BIOLOGY
ORTHOPAEDIC AND TRAUMA SURGERY
ADULT PSYCHIATRY
MEDICINE

Page | 3
HERBEIN
HEYD
HOCQUET
HUMBERT
KLEINCLAUSS
MAGY-BERTRAND
MAUNY
MENEVEAU
MEYER
MILLON
MONNET
MOUGIN
MOULIN
NEZELOF
OBERT
PARRATTE
PAUCHO
PILI-FLOURY
PIVOT
PLESIAT
PRETET
RAMANAH
REGNARD
RIETHMULLER
RINCKENBACH
ROUX
SALEH
SAMAIN
SCHIELE
SECHTER
SERONDE
TATU
TAVERNIER
THEVENOT
THINES
THIRIEZ
TIBERGHIEN
TOUSSIROT
TRACQUI
VALMARY-DEGANO
VANDEL
VAN MALDERGEM
VIEUX
VUILLIER
WENDLING
WESTEEL-KAULEK
Mr. Georges
Mr. Bruno
Mr. Didier
Mr. Philippe
Mr. François
Mrs. Nadine
Mr. Frédéric
Mr. Nicolas
Mr. Christophe
Ms. Laurence
Ms. Elisabet
Ms. Christiane
Mr. Thierry
Ms. Sylvie
Mr. Laurent
Mr. Bernard
Mr. Julien
Mr. Sébastien
Mr. Xavier
Mr. Patrick
Mr. Jean-Luc
Mr. Rajeev
Mr. Jacques
Mr. Didier
Mr. Simon
Mr. Christophe
Mr. Maher
Mr. Emmanuel
Mr. François
Mr. Daniel
Ms. Marie-France
Mr. Laurent
Mr. Laurent
Mr. Thierry
Mr. Laurent
Mr. Gérard
Mr. Pierre
Mr. Eric
Mr. Antoine
Ms. Séverine
Mr. Pierre
Mr. Lionel
Ms. Rachel
Mr. Fabrice
Mr. Daniel
Ms. Virginie
VIROLOGY
GENERAL SURGERY
HOSPITAL HYGIENE
DERMATO-VENEREOLOGY
UROLOGY
INTERNAL MEDICINE
BIOSTATISTICS, MEDICAL INFORMATICS AND
COMMUNICATIONS TECHNOLOGY
CARDIOLOGY
MAXILLOFACIAL SURGERY AND STOMATOLOGY
PARASITOLOGY AND MYCOLOGY
EPIDEMIOLOGY, HEALTH ECONOMICS AND PREVENTION
CELLULAR BIOLOGY
NEUROLOGY
PAEDOPSYCHIATRY
ORTHOPAEDIC AND TRAUMA SURGERY
ANATOMY
PLASTIC, RECONSTRUCTIVE AND COSMETIC SURGERY
ANAESTHESIOLOGY - INTENSIVE CARE
ONCOLOGY
BACTERIOLOGY - VIROLOGY
CELLULAR BIOLOGY
GYNAECOLOGY - OBSTETRICS
PHYSIOLOGY
GYNAECOLOGY - OBSTETRICS
VASCULAR SURGERY
DEVELOPMENTAL AND REPRODUCTIVE BIOLOGY AND MEDICINE
OPHTHALMOLOGY
ANAESTHESIOLOGY - INTENSIVE CARE
CARDIOLOGY
ADULT PSYCHIATRY
CARDIOLOGY
ANATOMY
OTORHINOLARYNGOLOGY
HEPATOLOGY
NEUROSURGERY
PAEDIATRICS
THERAPEUTIC
IMMUNOLOGY
LEGAL MEDICINE AND HEALTH CARE LAW
PATHOLOGICAL ANATOMY AND CYTOLOGY
ADULT PSYCHIATRY
GENETICS
PAEDIATRICS
ANATOMY
RHEUMATOLOGY
PNEUMONOLOGY

Page | 4
PROFESSORS EMERITUS
Mr. Paul BIZOUARD PAEDOPSYCHIATRY
Mr. Jean-François BOSSET RADIOTHERAPY
Mr. Jean-Claude CHOBAUT ENT
Mr. Robert MAILLET GYNAECOLOGY - OBSTETRICS
Mr. Georges MANTION GENERAL SURGERY
Mr. Yves TROPET PLASTIC, RECONSTRUCTIVE AND COSMETIC SURGERY
Ms. Dominique VUITTON THERAPEUTIC
SENIOR UNIVERSITY LECTURERS – HOSPITAL PRACTITIONERS
Ms.
Mr.
Mr.
Mr.
Mr.
Clotilde
Sebastien
Jamal
AMlOT
AUBRY
BAMOULID
CYTOLOGY AND HISTOLOGY
RADIOLOGY AND MEDICAL IMAGING
IMMUNOLOGY
Ms. Anne-Pauline BELLANGER PARASITOLOGY
Ms. Djamila BENNABI ADULT PSYCHIATRY
Mr. Sophie BOROT ENDOCRINOLOGY, DIABETES AND METABOLIC DISEASES
Ms. Malika BOUHADDI PHYSIOLOGY
Mr. Alain COAQUETTE VIROLOGY
Ms. Elsa CURTIT ONCOLOGY
Mr. Benoît CYPRIANI BIOCHEMISTRY AND MOLECULAR BIOLOGY
Mr. Pierre DECAVEL PHYSICAL MEDICINE AND REHABILITATION
Ms. Katy JEANNOT BACTERIOLOGY - VIROLOGY
Mr. Daniel LEPAGE ANATOMY
Mr. Eloi MAGNIN NEUROLOGY
Ms. Elisabeth MEDEIROS NEUROLOGY
Mr. Christian MOUSSARD BIOCHEMISTRY AND MOLECULAR BIOLOGY
Mr. Patrice MURET CLINICAL PHARMACOLOGY
Mr. Fabien PELLETIER DERMATO-VENEREOLOGY
Mr. Gaël PITON INTENSIVE CARE
Ms. Anaïs POTRON BACTERIOLOGY - VIROLOGY
Mr. Clément PRATI RHEUMATOLOGY
Mr. Antoine THIERY-VUILLEMIN ONCOLOGY
Mr. Jean-Pierre WOLF-BERTHELAY PHYSIOLOGY
ASSOCIATE TEACHERS
Mr. Régis AUBRY Associate Professor THERAPEUTICS
Mr. Rémi BARDET Associate Professor GENERAL MEDICINE
Mr. François DUMEL Associate Professor GENERAL MEDICINE
Mr. Jean-Michel PERROT Associate Professor GENERAL MEDICINE
Mr. Benoit DINET Associate Senior Lecturer GENERAL MEDICINE
Mr. Pascal JORDAN Associate Senior Lecturer GENERAL MEDICINE
Mr. Thierry LEPETZ Associate Senior Lecturer GENERAL MEDICINE
Mr. José-Philippe MORENO Associate Senior Lecturer GENERAL MEDICINE

Page | 5
PHARMACY
Mr. Xavier BERTRAND MICROBIOLOGY- INFECTIOUS DISEASES
Mr. Franck BONETTAIN BIOSTATISTICS
Ms. Céline DEMOUGEOT PHARMACOLOGY
Ms. Francine GARNACHE-OTTOU HAEMATOLOGY
Ms. Corine GIRARD-THERNIER PHARMACOGNOSY
Mr. Frédéric GRENOUILLET PARASITOLOGY - MYCOLOGY
Mr. Yves GUILLAUME ANALYTICAL CHEMISTRY
Mr. Samuel LIMAT CLINICAL PHARMACY
Mr. Dominique MEILLET PARASITOLOGY - MYCOLOGY
Ms. Laurence NICOD CELLULAR BIOLOGY
Mr. Bernard REFOUVELET ORGANIC AND THERAPEUTIC CHEMISTRY
Ms. Lysiane RICHERT TOXICOLOGY
Mr. Philippe SAAS IMMUNOLOGY
Ms. Estelle SEILLES IMMUNOLOGY
PROFESSORS EMERITUS
Mr. Alain BERTHELOT PHYSIOLOGY
Ms. Françoise BÉVALOT PHARMACOGNOSY
Ms. Mariette MERICER BIOMATHEMATICS AND BIOSTATISTICS
SENIOR LECTURERS
Ms. Claire ANDRE ANALYTICAL CHEMISTRY
Ms. Aurélie BAGUET BIOCHEMISTRY
Mr. Arnaud BEDUNEAU GALENICAL PHARMACY
Mr. Laurent BERMONT BIOCHEMISTRY
Mr. Oleg BLAGOSKLONOV BIOPHYSICS AND MEDICAL IMAGING
Ms. Oxana BLAGOSKLONOV GENETICS
Mr. Eric CAVALLI PHYSICAL AND MINERAL CHEMISTRY
Mr. Jean-Patric DASPET BIOPHYSICS
Ms. Sylvie DEVAUX PHYSIOLOGY
Mr. Yann GODET IMMUNOLOGY
Mr. Lhassane ISMAILI ORGANIC CHEMISTRY
Ms. Isabelle LASCOMBE BIOCHEMISTRY / ISIFC
Ms. Carole MIGUET ALFONSI TOXICOLOGY
Mr. Johnny MORETTO PHYSIOLOGY
Mr. Frédéric MUYARD PHARMACOGNOSY
Ms. Virginie NERICH CLINICAL PHARMACY
Mr. Yann PELEQUER GALENICAL PHARMACY
Mr. Marc PUDLO THERAPEUTIC CHEMISTRY
Ms. Nathalie RUDE BIOMATHEMATICS AND BIOSTATISTICS
Ms. Perle TOTOSON PHARMACOLOGY
OTHER TEACHERS
Ms. Lucie BERNARD ENGLISH TEACHING FELLOW
Ms. Mylène COSTER ENGLISH PAST
Mr. Alain DEVEVEY SENIOR LECTURER IN PSYCHOLOGY
Ms. Clemence POROT ASSOCIATE SENIOR LECTURER IN BIOPHYSICS
Ms. Florence VAN LANDUYT PAST CLINICAL PHARMACY - DISPENSARY

Page | 6
ACKNOWLEDGMENTS
To Professor Dumoulin, Chairman of the Jury For your availability, your interest, and our constructive exchanges. For your advice and criticisms which guided my thoughts throughout my work.
To Dr. Maillot, the Thesis Director For your guidance, help, orientation and seeing in me the capability to perform this work.
For your availability, kindness and listening during these many exchanges. For all the professional and personal enrichment I have acquired at your side. Thank you for your confidence and especially for your support during the many hours spent re-reading my work.
To Dr. Mégret, For your telephone availability, your involvement, your advice and your help during the most difficult times.
To the members of the Jury, For doing me the honour of being a member of my Jury, and for your interest in my work.

Page | 7
To Professor Duclos, For helping me in my research, giving me your point of view and your expertise in sports endocrinology.
To my hospital internship teachers, For having helped me to find my vocation, and taking the time to teach me an exciting and complex profession.
To my general medicine internship teachers, Dr. Bordet, Dr. Jordan, Dr. Royer and Dr. Sylvain, For their help and coaching. For teaching me everything that theory cannot describe, and what
cannot be dictated in the lecture hall. For those unforgettable moments in my professional and private life. For making me understand what medicine and its human values are. For having simply made me grow with you.
To my many co-interns: Pia, Charlotte, Nicolas, Mika, Simon, Frank, Eva, Marc, Claire, Regula and Marine,
For those many shared moments, those crazy laughs and difficult duties.
To the paramedical teams of the emergency services (Vesoul HC), Rheumatology (Minjoz UHC, Besançon), Paediatrics and Gynaecology (Vesoul CH), Geriatrics (Vesoul CH)
For your sympathy, welcome and generosity. For all those unforgettable department meals. In you, I have discovered people with great hearts, dedication and great humanity. All of these encounters during my internship will continue to have a place in my heart.

Page | 8
To my parents, For their love and their eternal support, in the good times as well in the bad. The culmination of
this work and these years of study is the result of your help. You have given me a magnificent model of hard work, courage, perseverance and generosity. I am indebted for this education and this love that makes me proud. I love you.
To my grandparents, For your love since my youngest age. For your help, and your confidence. For having transmitted
to me the true values of life. You are the example that love is timeless. To Granny Marguerite for all those little moments that were so important, for your sense of sharing and love. To Grandpa and Granny Chico and Quina for your eternal love of simple things, and for your entire life lived with courage, hard work, merit and sharing.
To you Grandpa, A special thought for you Grandpa Louis, who would have loved to see this work accomplished
and those years come to fruition. For the humility, generosity, perfectionism, kindness, modesty and devotion you conveyed. All these values shared since my earliest years are today the firm and nostalgic foundations of my future. Know that I have always followed your example humbly. I miss you.
To Tony, my brother, For his encouragement, his support and all the shared moments in our common passions. For all
those childhood memories that are forever present in my heart. But also for having transmitted his iliotibial band syndrome, encouraging me in my errands, and reconciling me with raclette and Nutella. You only have one brother. You will remain the person who counts the most for me. I love you, brother.
To my friends, Mika and Marie-Astrid, Stéphanie, Claire, Marc, Eva and David, Dimitri and Floriane. For all those convivial meals, failed barbecues, those post-prandial board games whose rules
always escape me, those evenings, those weekends... in short, because you have always been there. I love you.
To my sporting friends, For all those human adventures spent together, at the races and outside. To Aurore, Sebastien,
Alexandra, Alexandre for this magnificent Tour of Haute-Saone that will remain one of the most beautiful human and sports adventures of my life. To Aurore, Sebastien and their cafetière for their generosity and kindness. To all my sporting friends who share the same philosophy of our sport.
To Florence, For all your love, your encouragement and your attention. For the many time-consuming
proofreading sessions. For supporting me in those testing times, and for believing in me. For making me smile in the most difficult moments. For sharing all those moments of life, however insignificant, but so important. For having been simply at my side, and for waiting patiently to finally build our future together. Alone we can move faster, but together we will go further. I love you.
To all those who have made my life what it is today.
Thank you.

Page | 9
HIPPOCRATIC OATH
In the presence of the Teachers of this School, and my dear fellow students, I promise and swear, on behalf of the Supreme Being, to be faithful to the laws of honour and integrity in the practice of Medicine.
I will give my care free of charge to the indigent, and will never demand a salary above my work.
Being allowed inside houses, my eyes will not see what happens there, my tongue will hold the secrets that are confided to me, and my status will not be used to corrupt morality, nor to promote crime.
Being respectful and grateful to my Teachers, I will give to their children the instruction I have received from their parents.
May men grant me their esteem if I am faithful to my promises!
May the scorn and censure of my colleagues be cast upon me if I am found lacking!

Page | 10
“Sport will seek fear to dominate it, fatigue to triumph over it, difficulty to defeat it”
Pierre de Coubertin

Page | 11
TABLE OF CONTENTS
INTRODUCTION Current state of knowledge and problems ......................................................................... page 13
PART 1: PHYSIOPATHOLOGY OF THE CORTICOTROPIC AXIS AND SPECIFIC FEATURES OF EXERTION 1. Anatomy and Physiology
o Central: Hypothalamus and pituitary ................................................................... page 17 o Peripheral: Adrenal glands and glucocorticoids .................................................... page 19
2. Glucocorticoids and their effects ................................................................................... page 24 3. Effects of corticosteroids on performance ..................................................................... page 26 4. Exploration of corticotropic function
o Static ...................................................................................................................... page 28 o Dynamic ................................................................................................................. page 29
5. Special case of salivary cortisol ....................................................................................... page 29 6. Adrenal insufficiency and general pathology ................................................................. page 36 7. Corticotropic axis and physical activity
o Intensity, duration and training ............................................................................ page 37 o Recovery ................................................................................................................ page 39 o Food and hydration .............................................................................................. page 39 o Recovery disorder: fatigue syndrome and over-training ...................................... page 40 o Age ........................................................................................................................ page 42 o Other factors ......................................................................................................... page 42
8. Risks incurred by athletes in hypocortisolaemia during physical activity o Acute adrenal insufficiency ................................................................................... page 44 o Chronic adrenal insufficiency ................................................................................ page 44 o Adverse effects of corticosteroids ........................................................................ page 45
PART 2: LITERATURE REVIEW: HYPOCORTISOLAEMIA AND EXOGENOUS GLUCOCORTICOIDS
1. Introduction .......................................................................................................... page 47 2. Materials and methods .......................................................................................... page 48 3. Search: Exogenous glucocorticoids and hypocortisolaemia
o Inhaled corticosteroids .......................................................................................... page 49 o Intramuscular, intradermal and subcutaneous corticosteroids ........................... page 61 o Peri- and intraarticular corticosteroids ................................................................. page 62 o Dermocorticoids ................................................................................................... page 65 o Intranasal corticosteroids ..................................................................................... page 70 o Corticosteroids in eyedrops .................................................................................. page 73
4. Conclusion and discussion ..................................................................................... page 75
PART 3: OBSERVATIONAL STUDY: Hypocortisolaemias screened in the context of biological surveillance implemented by the French Cycling Federation (FFC) and the prevalence of corticosteroid intake
1. Introduction .......................................................................................................... page 77 2. Materials and method ............................................................................................ page 78 3. Results .................................................................................................................. page 78 4. Conclusion and discussion ..................................................................................... page 80
GENERAL CONCLUSION, DISCUSSION AND PROSPECTS ............................................................. page 81
BIBLIOGRAPHY ....................................................................................................................... page 83
ANNEXES List of figures and tables .................................................................................................... page 95

Page | 12
LIST OF ABBREVIATIONS
ACTH Adrenocorticotrophin ADH Antidiuretic Hormone NSAID Non-steroidal anti-inflammatory(ies) WADA World Anti-Doping Agency AMPD Medical Office for Doping Prevention mRNA Messenger ribonucleic acid TUE Therapeutic Use Exemption AVP Arginine Vasopressin COBP Chronic Obstructive BronchoPneumopathy Ca Calcium CBG Cortisol Binding Protein CRH Corticotropin-Releasing Hormone ICS Inhaled Corticosteroid(s) INCS Intranasal Corticosteroid(s) CTC Corticosteroid(s) Dal Dalton INN International Nonproprietary Name Desoxi Desoximetasone Dex(a) Dexamethasone DHEA Dehydroepiandrosterone DHEAS Dehydroepiandrosterone Sulfate DNA Desoxyribonucleic acid SD Standard Deviation AE Adverse Effect EPO Erythropoietin FDA Food and Drug Association
FFC Federation Française de Cyclisme FSH Follicle-Stimulating Hormone GH Growth Hormone GHIH Growth Hormone-Inhibiting Hormone (Somatostatin) GHRH Growth Hormone-Releasing Hormone (Somatoliberin) GI Gastrointestinal GnRH Gonadotropin-releasing hormone
HPA Hypothalamic—Pituitary—Adrenal HSP Heat Shock Proteins IgE Immunoglobulin E IL1 Interleukin 1 IL2 Interleukin 2 IL6 Interleukin 6 INF Interferon IRBMS Institute for Research on Well-Being in Sports Medicine and Health Care OG Olympic Games LC-MSH/MS Liquid Chromatography Mass
Spectrometry LH Luteinising Hormone AMS Acute Mountain Sickness MeSH Medical Subject Headings MPCC Mouvement Pour un Cyclisme Crédible (Credible Cycling Movement) MSH Melanocyte Stimulating Hormone OR Over-reaching

Page | 13
Exercise physiology data
Concentric contraction
Eccentric contraction
Isometric contraction
Ergogenic
Endurance exercise
Resistance exercise
ORL OT TNF- a TSH
TRH UCI VO2 max PPV NPV WADA
Otorhinolaryngology Over-training Tumor Necrosis Factor Alpha Thyreostimulin
Thyrotropin-releasing hormone International Cyclists’ Union Maximum oxygen consumption (mL/min/kg) Positive Predictive Value Negative Predictive Value World Anti-doping Agency
Muscular contraction of the muscle or muscle group by shortening Muscular contraction of the muscle or muscle group by stretching Muscular contraction without changes in length Describes a substance that is likely to improve athletic performancePhysical exercise whose main source of energy is provided by oxidative glycogenolysis Physical exercise whose main source of energy is provided by anaerobic routes (lactic and alactic).

Page | 14
INTRODUCTION
This paper is the fruit of multidisciplinary reflection and questions within the Movement for Credible Cycling (MPCC) and the French Cycling Federation (FFC). The initial idea is to focus on hypocortisolaemia in cyclists (and more broadly in athletes) from an aetiological viewpoint, but in particular in terms of prevention, risks and behaviour.
In the context of high-level sports practice, the screening of biological adrenal insufficiency expressed as hypocortisolaemia is performed in the context of the usual tests of the national and international anti-doping bodies.
The principal identified factor that induces hypocortisolaemia is the use of exogenous glucocorticoids (Courtney, McAllister et al. 2000; Duclos, Guinot et al. 2007 (1)).
A survey conducted by the FFC in 2002 revealed corticosteroid use among 85 of 538 cyclists, or 15.8%. Among cyclists with hypocortisolaemia, this rate was 92%. In 2010, Ana Senard-Ojero (2), in a 7-year retrospective study (2002 to 2008) of data from the Midi-Pyrénées doping prevention clinic, found glucocorticoid use in 9 of 35 cases, i.e. in second place among substances declared to be prohibited.
Arnaud M. in 2010 (4), in an observational study in ultra-trainers of the Diagonale des fous (note: ultra-endurance race in the mountains on the island of Réunion between 70 and 160km), reports that:
- 22.95% of the 1,691 athletes reported being treated with anti-asthmatic background therapy, - 4.91% reported using corticosteroids in the preparatory phase, - 0.78% reported using them during the race.
According to the World Anti-Doping Code, oral, intravenous, intramuscular and rectal glucocorticoids are on the prohibited list as banned substances in competition. (Annex 1). Other routes of administration are not subject to prohibition of use in sports practice. The World Anti-Doping Agency (WADA) admits Therapeutic Use Exemptions (TUEs) for prohibited glucocorticoids, and the International Cycling Union (UCI) applies the WADA rules.
In connection with the FFC, among other things, the MPCC performs a screening of athletes with hypocortisolaemia. Well beyond the anti-doping regulatory framework, the MPCC is part of a more focused effort to monitor the health of athletes and for prevention. To do this, monitoring of the plasma cortisol level is performed in cyclists and a practical code of conduct adapted to the risks involved has been put in place.
The implications of this screening are multiple, inducing an immediate temporary suspension for aetiological investigation:
- Anti-doping control with potential disciplinary sanction (automatic suspension, etc.). - Medical management determining the fitness and subsequent sporting risk, integrated into a
more general framework of health monitoring of athletes.
The discovery of hypocortisolaemia in cyclists has been the subject of recommendations concerning the conduct to be followed, on the advice of experts (3) (Annex 2). (Experts: Prof. Duclos M., Prof. Le Bouc Y., Dr. Guinot M., Prof. Bonifazi M., Dr. Ownby J.G., Prof. Brismar K.)

Page | 15
Corticosteroid administration declared at the time of sampling
Administration of corticosteroids not declared
Plasma cortisol level lower than 6 67 pg/L (184 nmol/L) (mean -2 SD)
Very high probability of adrenal insufficiency Contraindication in sporting practice
Urgent notification in endocrinology environment
High probability of adrenal insufficiency Contraindication in sporting practice Urgent notification in endocrinology environment
Plasma cortisol level between 67 and 160 µg/L. (184-500 nmol/L, mean -2 SD and mean +1 SD)
Attending physician’s checking in co-prescription with the federal physician in 10 days in relation to the day of sampling (sampling to be done in the network).
If there is value persistence in this range, seek urgent advice of an endocrinologist
Normal value If osteocalcin low to high (strong presumption of corticosteroid therapy), verification in a period of 10 days compared to the day of sampling, by the attending physician in co-prescription with the federal physician (sampling to be done in the network)
Plasma cortisol level 5 180 µg/L (mean + 1 SD)
Normal adrenal function Normal adrenal function
Table 1- Conduct to be followed in hypocortisolaemia, Medical Expert Committee 2004, validated by the National Medical Committee of the French Cycling Federation on 22 October 2010 (3).
The French experts Prof. Duclos M., Prof. Le Bout Y., and Dr. Guinot M., were questioned by the FFC on this subject. Their answers are below (Annex 7):
Regarding screening of the impact of the use of glucocorticoids on adrenal function “The data from the scientific literature clearly shows that, whatever the mode of administration of a glucocorticoid (…), there is systemic passage which may cause a decrease in the physiological secretion of cortisol by the adrenal glands, (…). This effect is probably proportional to the administered dose (...), but there are probably individual susceptibilities explaining severe cases of adrenal function in low systemic passages.
The demonstration of the partial or total blockage of cortisol secretion (adrenal insufficiency) is ideally based on a pharmacological stimulation test of the hypothalamic-pituitary-adrenal axis. For practical reasons, it is not possible to perform this type of test in competitions in asymptomatic subjects. Therefore, the simple quantitative analysis of plasma cortisol in the morning, when its concentration is physiologically highest, makes it possible to detect the most fundamental biological adrenal insufficiencies, even if it does not make it possible to screen all of them. (...). ”
Regarding the health risks linked to adrenal insufficiency “The demonstration of a plasma cortisol concentration below the standards of the kit used by the laboratory reflects a biological adrenal insufficiency. This is the consequence in athletes of the administration of a synthetic glucocorticoid, whatever its mode of administration (...). This biological situation corresponds to a situation where the body is unable to respond adequately to severe stress (anaesthesia for surgery, bacterial infection, haemorrhagic shock, major trauma). Indeed, these situations require that the adrenal glands must secrete an increased amount of cortisol, (...). Thus, when this response is deficient (acute adrenal insufficiency), the prognosis can be life-threatening, even in an a priori healthy subject. The few studies that have identified these cases show a high morbidity rate or even mortality (...). ”

Page | 16
Regarding medical decisions for athletes: “(...) an athlete with a biological adrenal insufficiency runs a risk of life-threatening cardiovascular or metabolic stress, even if this is rare. Cycling (...) is a sport with a high trauma risk, with the possibility of haemorrhagic fracture or requiring surgery; therefore, it seems relevant that the French Cycling Federation’s regulation provides medical solutions to reduce the risk of acute adrenal insufficiency. ” Other international experts have also answered these questions (Prof. Bonifazi M., Dr. Ownby J.G., Prof. Brismar K.). Their responses are along the same lines (Annex 7).
In addition to this data, the discovery of hypocortisolaemia in athletes raises several questions which constitute the focus of our paper:
Can physical activity in itself induce hypocortisolaemia? Is there a medical risk for an athlete with hypocortisolaemia to compete in the event of an
accident or stress?
What is the influence of exogenous glucocorticoids on the plasma cortisol level?
To better understand these problems, we will briefly discuss, in the first chapter, the anatomy, physiology, and physiopathology of the corticotropic axis. This chapter also covers:
salivary cortisol and its validity in the screening of adrenal insufficiency, the specific details of the corticotropic axis under exertion, the risks incurred by athletes in hypocortisolaemia during physical exertion.
The second part, which forms the central part of our work, aims to take stock of the influence of glucocorticoids on the corticotropic axis through a review of the literature, according to the different routes of administration.
Finally, we will illustrate our work in a third part by means of an observational study of the prevalence of corticosteroid therapy in cyclists screened in hypocortisolaemia via the MPCC database.

Page | 17
1. Anatomy and physiology of the corticotropic axis
1. Central: Hypothalamus and pituitary
The body’s most important neuroendocrine interface is the hypothalamus.
The hypothalamus (from the Greek ono, hypo = beneath and OciAapoc, thalamos = chamber, cavity) is a structure of the central nervous system located in the anteroinferior face of the encephalon, in the median and inferior part of the base and the lateral parts of the 3rd cerebral ventricle.
Through neurosecretory cells, the hypothalamus synthesises and secretes peptides and amines called “hypothalamic-pituitary hormones” that induce the synthesis and secretion of hormones by the pituitary, via the pituitary stem containing the non-myelinated axons of these cells.
The neurons with endocrine activities of the hypothalamus are divided histologically into 2 parts: The magnocellular system in relation to the neurohypophysis. The parvocellular system in relation to the anterior pituitary. The latter system secretes activator
or inhibitor hypophysiotropic neuropeptides that regulate the anterior pituitary. o CRH (corticotropin-releasing hormone) o GnRH (gonadotropin-releasing hormone) o Dopamine o GHIH (growth hormone-inhibiting hormone) or somatostatin o GHRH or somatoliberin o TRH (thyrotropin-releasing hormone) o Vasopressin or antidiuretic hormone (ADH) o Oxytocin
In addition to its role in co-ordinating endocrine functions, the hypothalamus allows thermoregulation, regulation of homoeostasis of the internal environment, appetite and the peripheral nervous system, as well as sexual functions, behaviour and affect.
The pituitary gland (hypophysis) is an ovoid endocrine gland located in the hypophyseal fossa, a true cavity on the supero-posterior part of the median part of the sphenoid bone.
The pituitary gland is composed of several embryologically different lobes The anterior pituitary (adenohypophysis): in an anterior location, The posterior pituitary (neurohypophysis): in a posterior location, The intermediate pituitary: developed in certain animal species, in the foetal period, and in the
state of cystic remnants in adults.
PART 1: PHYSIOLOGY AND PHYSIOPATHOLOGY OF THE
CORTICOTROPIC AXIS ON EXERTION

Page | 18
Nuclei N. of the hypothalamus
Optical chiasma
1st network of papillary muscles
ANTERIOR PITUITARY
Hypophyseal
portal vein
2nd network of capillaries
Hypothalamic neurons
Pituitary stem
POSTERIOR PITUITARY
Artery
Anterior pituitary hormones
Posterior pituitary
hormones .
Figure 1- The hypothalamic-pituitary system (4).
Anterior pituitary hormones
Hypothalamic neurohormones
The anterior pituitary comprises several different cell types, the role of which is the secretion of different hormones, grouped with their peripheral actions into axes.
- Growth hormone (GH) and the somatotropic axis, prolactin and the lactotropic axis, - Follicle-stimulating hormone (FSH) and the gonadotropic axis, - Luteinising hormone (LH) and the gonadotropic axis, - Thyreostimulin (TSH) and the thyreotropic axis, - Melanostimulin (MSH) and endorphins, - Adrenocorticotropic hormone (ACTH).
The posterior pituitary is derived embryologically from the hypothalamus. The axons it contains excrete, in the form of neurosecretions,
- vasopressin or antidiuretic hormone (ADH), - oxytocin.
The central part of the corticotropic axis is then detailed with: - At the hypothalamic level: secretion of CRH, - At the pituitary level: CRH induces a stimulation of the secretion of ACTH by
the anterior pituitary.
Note: other molecules have an accessory stimulatory role (intestinal vasoactive peptide, angiotensin II, catecholamines, etc.) or inhibitory (atrial natriuretic factor, etc.) on the secretion of ACTH.
Vein

Page | 19
Capsule
Cortex _
Medulla
Adrenal glands
2. Peripheral: Adrenal glands and corticosteroids
a. Adrenal glands
The peripheral organs of the corticotropic axis are the adrenal glands.
At the anatomical level, this is an asymmetric twin organ located on the anterosupero-internal pole of the 2 kidneys, in the fat capsule, in the retroperitoneal zone. The right adrenal has a classic shape of a “gendarme’s hat” and the left is like an “inverted comma”.
They are vascularised by: At the arterial level:
o Superior adrenal artery (from the diaphragmatic artery), o Median adrenal artery (from the aorta, inconsistent, in particular on the right), o Inferior adrenal artery (from the renal artery).
These arteries become capsular, and then become organised into a subcapsular, cortical then medullary network.
On the venous level: drainage by the central medullary vein, flowing into the adrenal vein in the
direction of the inferior vena cava on the right and left renal vein.
Figure 2 - Anatomy of the adrenal glands (5).
Histologically, the adrenal glands are composed of 2 concentric embryologically different zones. The adrenal cortex (mesodermal embryological origin) in peripheral location, The adrenal medulla secreting catecholamines (norepinephrine and epinephrine) (embryological
origin of the neural crest) in the central location.
The adrenal cortex has 3 histological tissues which are actors in the corticotropic axis. From the periphery to the central medullary part, the following are described:
– The zona glomerulata, where the cells synthesise mineralocorticoids (aldosterone), The zona fasciculata, where the cells synthesise glucocorticoids, The zona reticularis, where the cells also synthesise glucocorticoids and male and female sexual
steroids.

Page | 20
FACTORS ACTING
ON THE GLAND
—} Capsule
—} Zona glomerulosa
Zona fasciculata
- Zona reticularis
Medulla
I, 9
11-desaxycodicosierone
Corticosterone
11-deoxycorticosterone TESTOSTERONE
Angiotensin and ACTH
ACTH
ACTH
Androgens
Glucocorticoids
Androgens (dehydroepaindrosterone and androstenedione)
Glucocorticoids (cortisol and cortisone)
Mineralocortocoids (aldosterone)
HORMONES SECRETED Zona glomerulosa
Zona fasciculata
Capillaries
Zona reticularis
Cortico-adrenal
Figure 3 - Histology of the adrenal cortex (6).
b. Corticosteroids
The synthesis precursor of all the following molecules is cholesterol.
Long regarded as independent, the secretions of mineralocorticoids and glucocorticoids are closely linked. For example, cells in the zona glomerulosa have been shown to have ACTH receptors (Liakos et al., 1998 (7)).
Principal synthesis routes of adrenal cortex hormones in humans
Cholesterol
Pregnenolone
Progesterone
17α-hydraxypregnenolone Dehydroplandrosterone
17α-hydroxyprogesterone Androstenedione
CORTISOL
Oestradiol
18-Hydroxycorticosterane
ALDOSTERONE
Figure 4 - Diagram of adrenal cortex biochemistry (8).
11-desoxycortisol

Page | 21
Figure 5 - Molecular presentation of different glucocorticoids (9).
The mineralocorticoids secreted by the zona glomerulosa of the adrenal cortex have an effect on the hydro-electrolyte balance of the body and the regulation of blood pressure via their receptors on the distal renal tubules.
There are 2 mineralocorticoids: Aldosterone (95%), a component of the renin-angiotensin-aldosterone system, 11-deoxycorticosterone (5%).
Endogenous glucocorticoids are mainly produced by the zona fasciculata and zona reticularis of the adrenal cortex. The principal endogenous glucocorticoids are:
Cortisol or hydrocortisone (95%), Cortisone (5%), which is biologically inactive.
Figure 6 - Biochemistry of glucocorticoids (10).
Figure 6 - Glucocorticoid biochemistry (10).
As illustrated in the above figures, synthetic glucocorticoids are therefore derived from cortisol by the addition of OH, carbon or fluorine radicals (Corticoids and corticosteroid therapy, Richard D., Senon J.L., Roblot P (5)).
Cortisol Cortisone Methylprednisolone Dexamethasone
Prednisolone Prednisone Triamcinolone Fludrocortisone
Hydroxylation in
position 11
cortisone
Hydroxylation in
position 11
Addition of fluorine
in position 9 α
hydrocortisone
(or cortisol) triamcinolone
betamethasone
dexamethasone
prednisone prednisone
Double bond 1-2 Double bond 1-2
methylprednisolone
Methylation in
position 6α

Page | 22
Acrophase 0832h
(0759h – 0905h)
Nadir 0018h
(2339h — 0058h)
MESOR: 5.2 mcg/dL (4.7 — 5.7)
Co
rtis
ol
(mcg
/dL
)
Factors influencing cortisol secretion:
Circadian and seasonal rhythms
The blood secretion of cortisol is not stable, but follows a circadian variation (waking - sleeping rhythm). The origin of this circadian rhythm is multiple. We find:
the role of the suprachiasmatic nuclei at the supra-pituitary level, the role of the sympathetic nervous system and its action on the adrenal cortex, the role of “clock genes”, which are true peripheral clocks.
As shown in the following figure, the plasma cortisol level is higher in the morning (maximum between 8 and 9 a.m.). This period is called the acrophase. It then decreases, reaching its minimum (nadir) in the middle of the night.
Clock time
Figure 1: Circadian variation in the secretion of cortisol (11).
This secretion cycle is in phase contrast with that of melatonin (the hormone secreted by the pineal gland and modulated by light and darkness). The latter reduces (in vivo) the response of cortisol to ATCH. It is likely that the secretion of nocturnal melatonin induces the collapse of the plasma cortisol level.
22 23 24 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21

Page | 23
Figure 2 - Circadian variation of plasma cortisol and melatonin levels (12).
Similarly, this daily variation is applicable to pharmacological tests for corticotropic stimulation or inhibition. The response of the plasma cortisol level following an ACTH injection is higher in the morning than in the evening. In addition, cortisol production is more strongly inhibited after injection of exogenous corticosteroids at 4 a.m. in the morning than during the day, with a gradual return.
Therefore, the interpretation of the biological data and the results of the pharmacological tests must take into account the lifestyle of the athlete (jet lag, travel, sleeping periods, etc.), which frequently varies among international athletes.
Psychological aspect Neuropsychological stimulations increase the production of CRF and thus of ACTH.
Age In the elderly, there is a change in the secretion of cortisol: the morning plasma peakcomes earlier, and the feedback loop is usually decreased.
Transport of cortisol: Blood transport in linked form is performed via transporters:
Cortisol-binding globulin (CBG) or transcortin (90%) (specific, high affinity, but low capacity),
Serum albumin (10%) (low specificity, low affinity, but high capacity). Only the free fraction is active. The linked fraction constitutes a reserve. These two forms are balanced.
Three different sessions of 24 h, 2 to 4 weeks apart: 1st session
2nd session
3rd session
Ser
um
Mel
ato
nin
(p
g/m
L)
Ser
um
Co
rtis
ol
(m
mo
l/L
)
Sampling hours

Page | 24
Action of corticosteroids: Via its binding to specific receptors, the ligand-receptor complex acts by gene transactivation (induction of gene expression) or on the contrary by transrepression, causing a phenotypic and genotypic response.
Figure 7 - Mechanism of action of different glucocorticoids according to the National College of Medical Pharmacology (13).
2. Glucocorticoids and their effects
Only a brief outline of the different pharmacological effects of glucocorticoids will be given in this chapter.
These effects are influenced by: The dosage, The mode and route of administration,
Their pharmacokinetics (local and systemic effect), The biological half-life or duration of action (which is corresponds to the duration of inhibition of
the axis corticotropic), The duration of treatment, The field (pathology, age, etc.).
a. Anti-inflammatory action
Glucocorticoids inhibit different stages of the inflammatory process (regardless of origin, post-traumatic, infectious, etc.). They limit vasodilation and vascular permeability, inducing reduction of oedema, pain and erythema. In a second phase, they limit the phagocytosis and degranulation of mast cells. Finally, in the tissue healing phase, they reduce fibroblastic proliferation, protease release and collagen synthesis.
“Immunogenic” domain Ligand
Cytoplasmic
membrane
Cytoplasm
Nuclear membrane
Nucleus
DNA
Transcription Transcription
Protein
Cell
membrane
Cytoplasm
Cell
membrane
Nucleus
Direct transcriptional action: positive or negative effect

Page | 25
Figure 8 - Impact of corticosteroids in the arachidonic cascade (Blanloeil Y., Le Teurnier Y., Demeure D. (14)).
b. Anti-allergic action
In summary, the allergic reaction is marked by the release of a specialised immunoglobulin of the IgE type by the differentiated B-lymphocytes. This IgE will bind to its specific receptors expressed on mast cells and to the polynuclear basophils, inducing the release of mediators (histamine, etc.), thus limiting the previously described inflammatory reaction.
As seen previously, glucocorticoids inhibit the degranulation of mast cells but also inhibit cellular reactions upstream.
c. Immunosuppressive action
Glucocorticoids act in different phases of the immune response. Inhibition of antigen recognition by B-lymphocytes and macrophages, Reduction of the immune amplification phase by blocking the multiplication and activation of
lymphocytes against an antigen, Inhibition of the synthesis of pro-inflammatory interleukins (IL-1, IL-2, IL-6, INF, INF-a), Inhibition of phagocytosis and production of oxygenated free radicals.
d. Bone action
By their direct effects on bone-forming cells (osteoblasts) and indirectly on bone-destroying cells (osteoclasts), glucocorticoids induce bone loss. They decrease the intestinal absorption of calcium and its tubular reabsorption. The calcium balance is therefore negative, with hypercalciuria.
Corticosteroids
Phospholipase A2
Membrane phospholipids
Arachidonic acid
Lipo-oxygenase Cyclo-oxygenase
Leukotrienes Prostaglandins

Page | 26
Osteoporosis
- Apoptosis of osteoblasts
↓ Growth
factors
Glucocorticoids __________________
↓LH and FSH
Testosterone
Oestrogens
↓Ca absorption - Ca elimination
Bone resorption Bone formation
Figure 9 - Bone action of corticosteroids (15).
e. Action on carbohydrate metabolism
Via the activation of hepatic enzymes, glucocorticoids promote the synthesis of glycogen (and thus hepatomuscular storage). In addition, they inhibit the synthesis of insulin and increase that of glucagon, hence their hyperglycaemic effect.
f. Action on protein metabolism
Glucocorticoids reduce protein synthesis by decreasing the muscle incorporation of amino acids and increase their tissue release.
g. Action on lipid metabolism
The latter activate lipolysis and the release of long-chain fatty acids which are used for neoglucogenesis.
3. Effects of corticosteroids on performance
There are principally 5 expected effects in the context of the search process for performance improvement:
Reduction of the fatigue onset threshold and the fight against asthenia, Energetic and ergogenic effect, Potential stem cell stimulation (with EPO), Limitation of inflammation and analgesia, Psychostimulatory effect.
According to Rochcongar P. in 2005, very few well-conducted studies have dealt with this subject.
Kuiper et al. (2008) (16) were interested in the ergogenic effects. Endurance athletes were administered inhaled corticosteroids for 4 weeks at 800 μg budesonide (therapeutic dose) and performed a maximum power test with no ergogenic effects being described.
Osteoprotegetrin Muscular strength
↓ Serum Ca

Page | 27
In the same year, Nordsborg et al. (17) did not find any ergogenic effects for high-intensity exercise, as opposed to exercise of moderate intensity.
Similarly, Soetens et al. (1995) (18) found no significant increase in pedalling duration until exhaustion in professional cyclists following the injection of 1 mg of ACTH. Arlettaz et al. (2006 and 2008) (19) reported no improvement in pedalling time during maximum exercise on an ergocycle until exhaustion in healthy men following 20 mg oral prednisolone. Marquet et al. (1999) (5) found no ergogenic effect following dexamethasone 0.5mg or 4mg versus placebo in a triangular test until exhaustion on the ergocycle. Similarly, a study conducted by the team of Gerard Lac did not demonstrate effects on VO2 max on fatigue after taking dexamethasone in moderately trained subjects.
In contrast to these publications on acute administration, Arlettaz et al., in 2007 (19), showed that short-term administration of prednisolone (60 mg daily for 7 days) significantly improved the performance of healthy men in exercise with an intensity of 70-75% of VO2 max. Collomp et al. (2008) (19) reported a mean increase in pedalling time of 80% in the group taking 60 mg of prednisolone per day for 7 days associated with 2 hours of training per day, compared to the mean increase in pedalling time of 54% for the group without training.
It therefore seems difficult to conclude that a definite ergogenic effect exists. The studies presented above suffer from an exploration of short and intense exertions, and not endurance. The short-term potential ergogenic effects observed are reported in subjects with moderate-intensity physical activity. For higher intensities and longer durations, these ergogenic effects were not clearly demonstrated.
4. Exploration of the corticotropic axis
Figure 10 - Diagrams of the regulation of the corticotropic axis (20).
Stress
Cortisol
Exogenous
corticosteroids
CRH
ACTH
CRH
ACTH
GLUCOCORTICOIDS
HYPOTHALAMUS
PITUITARY
ADRENAL GLAND

Page | 28
The exploration of the corticotropic axis includes: Static explorations, Dynamic explorations.
1. Static explorations
The cortisol concentration is measured in urine (cortisoluria) and in plasma (plasma cortisol level). It is measured by immunoassay (immunometric or competition methods).
a. At the urinary level: cortisoluria
Only 1% of the daily production of cortisol is metabolised and therefore excreted unchanged in the urine. The 24-hour cortisoluria is therefore a measure that more accurately reflects the secretion of cortisol. The sampling is performed over 24 hours. This assay is principally used to look for conditions of hypercortisolaemia.
b. At the plasma level: the plasma cortisol level
Cortisol and the concentration of blood ACTH can be assayed. As we have seen previously, the nycthemeral cycle of the plasma cortisol level requires a precise hourly dosage. It is advisable to adapt this dosage to the lifestyle of the patients (night work, sleep cycle and time differences during trips) and their pathologies.
The plasma cortisol level corresponds to the measurement of the total circulating cortisol (free and linked fraction). The variation of the transport proteins described above can therefore potentially induce abnormal results of the plasma cortisol level without pathology of the corticotropic axis. The most frequent example is the use of an oestro-progestative contraceptive, which increases the level of transcortin and therefore the measured the plasma cortisol level.
In the usual medical setting, the assay is usually performed at 8 p.m. If the sleep-wake rhythm is shifted, it is advisable to perform this assay at an interval of one hour and a half to two hours after waking.
In the sports context, the assay of cortisol must be valid and secured, and anonymised for optimal interpretation. The selected RBML-Biomnis laboratory network uses a chemiluminescence technique on a BECKMAN DxI immunoassay system and provides specific kits.
These explorations make it possible to identify the physiological and pathological mechanisms of the corticotropic axis:
Low cortisol, high ACTH = peripheral adrenal insufficiency, Low cortisol, low ACTH = central corticotropic insufficiency (note that such a table is created
every day at midnight), High cortisol, low ACTH = secretory tumour of the adrenal cortex, High cortisol, high ACTH: interpretation impossible: it may be the simple effect of the stress of
the sampling.
c. In the hair
The advantage of this type of assay lies in the possibility of traceability in taking glucocorticoids and in establishing its retrospective chronological use. During the formation of the hair (anagenic phase), foreign substances can be fixed in the hair matrix and progress cephalofugally according to the growth of the hair. The fixation can occur endogenously or externally (shampoos, lotions, sebum, etc.).

Page | 29
The literature on this subject has made it a reliable and robust method (Russell E. in 2012 (21), Stalder T. in 2012 (22)), although its use is restricted to analysis and long-term interpretation (chronic stress, etc.). This method is used in psychology and psychiatry and does not seem suitable for screening for hypocortisolaemia.
2. Dynamic tests
Overall, these explorations make it possible to precisely state the dysfunction of the corticotropic axis.
At the peripheral level: ACTH stimulation test. This test is indispensable to confirm a case of peripheral adrenal insufficiency. The principle is to administer, intramuscularly or intravenously, a dose of synthetic ATCH 1-24 and evaluate the peripheral response induced by the measurement of the plasma cortisol level.
At the central level: there are different tests to evaluate the response of the hypothalamic-pituitary axis (metopirone test, dexamethasone inhibition tests, CRH tests, etc.) which we will not detail in this paper.
5. Special case of salivary cortisol
We have voluntarily detailed this “static” analysis of cortisol in saliva due to its practical interest in the field of athletics.
The analysis of saliva, as a biological fluid for the assaying of hormones, has become of increasing interest to researchers, in particular to clinicians. This method is used in research in the fields of psychiatry, endocrinology, veterinary medicine and, more recently, sports medicine.
Saliva is produced by the principal salivary glands (parotids, sublingual and submandibular) and accessory salivary glands.
Its different roles are as follows: Protection and hydration of the endobuccal mucosa, Initial phase of digestion: preparation and deglutition (e.g. salivary amylase), Communication: Speech production and language, Indirect involvement in the perception of taste, Immune function due to the presence of antimicrobial proteins and immunoglobulin A,
The daily production is in the range of 500mL to 1,200mL. (70% is of parotid origin, 20% of submandibular origin, 10% remainder.) This secretion varies between periods of fasting and mealtimes and is also subject to a nycthemeral intrinsic rhythm. There are also seasonal, sexual, medication-induced or emotional changes.
The pH of saliva varies between 5.6 and 7.9. The overall composition of saliva is as follows:
Water: principal component, Proteins: 1.5 to 6.4 g/L (principally mucin), Potassium: 8 to 40 mmol/L, Sodium: 5 to 100 mmol/L, Calcium: 1.5 to 2 mmol/L, Phosphate: 5.5 to 14 mmol/L, Chloride: 5 to 70 mmol/L, Hormones,

Page | 30
Microbiota: bacteria, viruses, fungi, …. Food debris,
The mechanism of saliva production is complex. It occurs principally according to two mechanisms. Passive transfer according to the concentration gradient: relates to small lipophilic molecules
such as steroids. In the absence of metabolism or in-situ degradation, the salivary concentration therefore remains very close to the free blood concentration,
Paracellular via the tight junctions relates to smaller, more polar molecules (DHEA sulphate-type conjugated steroids and conjugated oestriol). Their concentration varies according to the salivary flow.
Active transport (insulin).
Figure 11 - Diagram of saliva formation (23).
The saliva concentrations of unconjugated liposoluble steroid hormones such as cortisol thus reflect the plasma concentrations of the same forms not linked to plasma proteins (10%), while hydrophilic conjugated steroids such as dehydroepiandrosterone sulphate are present at a saliva level of less than 1% of their plasma concentration.
It is theoretically known that a poor blood/saliva correlation exists for the rather water-soluble peptide hormones (FSH, LH,
TSH, prolactin).
Conjugations of some steroids (DHEA to DHEAS). Changes during transport (cortisol to cortisone by 110-hydroxysteroid-dehydrogenase-II).
The value of the salivary assay of cortisol lies in the fact that only the free (and therefore biologically active) fraction is excreted in saliva. The salivary assay of cortisol is therefore “theoretically” more representative of the biological activity of the corticotropic axis.
blood
interstitial space
epithelial cells
saliva
Very small (<200 Dal) & polar
Small & hydrophobic (like steroids)
ultrafiltration (flux-dependent!!!)
passive diffusion active transport

Page | 31
Other advantages of this method are: Its non-invasive nature, The operator requires little training or can be the athlete himself (medical supervision is
unnecessary), Suitable for mass use, Reduction of stress induced by the sampling, Repeated approximation of the possible assay, Assay during exertion is easier than a blood or urine assay, No variability in relation to the transport protein (CBG).
The disadvantages of this method are: The variability of the saliva composition, Possible contamination by “non-salivary” substances (bronchial, nasal, blood by oral mucosa
breakage, food, physiological dental components or those related to dental procedures, etc.),
The kinetics between the variations of blood and salivary concentrations, Sampling conditions
Behr GA (24) showed in a publication that the presence of salivary transferrin was an indicator of blood contamination of the saliva. His study identified no changes in salivary cortisol due to oral blood contamination.
Importantly, in 2012, Van der Véen BS (25) found no interference between taking inhaled fluticasone propionate and the measurement of salivary cortisol.
Sampling conditions:
There are several sampling kits specific to each laboratory and their analysis and packaging method. In general, a kit contains a centrifuge tube to hold the sample, a plug, and a Salivette for stimulating salivary secretion.
Although selective sampling of saliva from a salivary gland is possible, either by aspiration or cannulation, the saliva mixture is most commonly used. Salivary stimulation is often used to obtain a sufficient amount of biological fluid for the correct interpretation of the sample. It must be noted that this stimulation is not conceivable if the concentration of the hormone to be assayed varies as a function of the salivary flow (e.g. DHEA sulphate). However, this is not the case for cortisol, which follows a passive transport mechanism in a concentration gradient.
To stimulate salivation, the following are used: The application of citric acid to the tongue, Prior chewing of an inactive Salivette.
The sampling must be performed before brushing teeth (which limits mucous intrusions) outside mealtimes (at least 30 min) (which limits food debris) and before smoking cigarettes.

Page | 32
r Instructions to patient:
- before brushing teeth
- at least 30 min after any
ingestion of food
- mastication around 45 s
- storage at 4OC (but transport
possible to outpatient T)
tube for
centrifugation
plug
cotton
pad
(citric acid)
hanging
container
Saliva sampling using Salivettes
Figure 12 - Example of implementation of salivary cortisol in practice, by the Sarstedt laboratory (26).
Currently, the most widely used sampling systems are: Salivette® (Sarstedt) (Annex 3), Quantisal® (Immunalysis) (Annex 5), (Intercept® (Orasure Technologies) (Annex 4), the Saliva Collection System®.
These systems use a pad to be inserted either under the tongue or against the cheek. This absorbent pad is kept in the mouth for a fixed period (usually 1 to 2 minutes) to become impregnated with saliva and is then transferred to the storage container. After centrifugation, the saliva is recovered. The salivary cortisol concentration is not affected by the material of this pad.
According to the kit, the sample can be transported at room temperature and stored at 4° if necessary. Due to the salivary stability of cortisol, it does not undergo any significant changes associated with the sampling methods. This biological stability of salivary cortisol amounts to at least one week at room temperature.
The long-used analytical technique is the immunoassay due to its simplicity and the low volume of saliva required. However, as the risk of cross-reactions is high (pregnancy, medications, pathologies, etc.), the method has been refined. The current reference method is an ELISA. New biochip or microbead methods must be developed in the future.
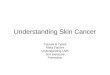
As shown in the following table, for many years, the number of publications on salivary cortisol (either in clinical or research situations) has risen dramatically, indicating a growing interest in this method.

Page | 33
Number of PubMed publications
Figure 3 - Evolution of the number of publications found on PubMed, containing the MeSH “Cortisol” and “Salivary” from 1967 to January 2017.
Logically, with regard to salivary cortisol, the following questions arise: Do variations in cortisol levels induce similar variations in salivary cortisol? If so, within what
timeframe? Is there a significantly acceptable correlation for screening hypocortisolaemia in a salivary
cortisol measurement? In general, is this test reliable?
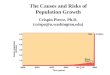
Introduction: As shown in the following figures, salivary cortisol, like the plasma cortisol level, follows a circadian rhythm, with a peak of production a few hours after waking, then decreasing and reaching its minimum in the middle of the night.
Saliv
ary
cort
isol (n
mol/l)
Figure 4 - Circadian variation of salivary cortisol (27).
This data then causes an interpretation of the result according to the time of day and the sleep-wake cycle of athletes, as for the plasma cortisol level. A slightly delayed increase is described in the salivary cortisol peak following corticotropic stimulation, as well as a greater response.
Method: We have performed a literature review, with a description of the research in qualitative narrative form.
Time
saliv
ary
cort
isol in
nm
ol/l (L
C/M
S-M
S)
defection due study 8
hours since awakening
number of
samples

Page | 34
MeSH: Cortisol Salivary, Plasma cortisol Search engines: PubMed, Google Scholar, Cochrane, Med Line Initial number of publications: 492 Number of publications used: 35
The selection includes all publications from 1982 to January 2017 that studied principally or incidentally a possible correlation between the plasma cortisol level and salivary cortisol.
Year Authors Goals Publication type Standard of proof Correlation
2017 El Farahn assay method ? ? yes
2016 Robertson CV CTC and exertion behaviour Trial A yes
2016 Faassen MV Assay method CTC salivary melatonin Analytical study B yes
2016 Araz F Adrenal insufficiency and cirrhosis, inter & CS Analytical study B yes
2016 Steffensen C. Hypercortisolaemia and salivary cortisol Analytical study B low
2016 Bellastella G. CS and plasma cortisol level variation diabetes Observational study C yes
2016 Behr GA Method of blood contamination of saliva ? C yes
2014 Zeitzer LM. Diurnal variation CS and plasma breast cancer Analytical study B yes
2014 Maas C. CS and blood relationship in premature infants Observational study C none
2014 Jung C. Monitoring corticosteroid supplementation insufficiency
Observational study C yes
2013 Bozovic D. CS as a stress marker Observational study C yes
2013 Trifonova ST Use of CS for pulsatile secretion of cortisol Observational study C yes
2013 Qian Zang Salivary cortisol and Cushing syndrome Literature review C yes
2012 Bernabe DG. Plasma cortisol and CS oropharyngeal cancer Observational study C yes
2011 Gatti R. Salivary hormones and physical activity Article C yes
2010 Thomasson R Correlation plasma saliva cortisol exertion Observational study C yes
2010 Sakihara S. Cushing’s syndrome: plasma, urine and CS Article C yes
2009 Shi SR Cushing’s syndrome: CS reliability Observational study C yes
2008 Carroll TY Cushing’s diagnosis Expert opinions C yes
2006 John G. Lewis Focus on salivary cortisol Literature review C yes
2005 Kumar AM. CRH test: CS and plasma Analytical study B yes
2005 Gozansky W. S. Validity of salivary cortisol for dynamic exploration Analytical study A yes
2004 Yates DT Correlation of blood and salivary cortisol after ACTH test
Analytical study A yes
2003 Hill SA. Cortisol and reboxetine Analytical study B yes
2002 Mormon MC. Variation in cortisol metastatic colorectal cancer Observational study C none
1997 Obminski Z. Acceleration effect on corticotropic and gonadotropic axis
Analytical study B yes
1993 Lac G. Correlation of cortisol blood and saliva Analytical study B yes
1992 Lo MS. Clinical application salivary cortisol Article C yes
1991 Galard R Correlation CS and ACTH Depression according to dexa test
Analytical study B yes
1991 Port K Exercise and plasma cortisol level and CS Article C variable
1989 Ben Arey H. Effect of exercise on plasma cortisol level and salivary cortisol
Analytical study B yes
1989 Kirschbaum C. Salivary cortisol and biopsychology Literature review C yes
1988 Kahn JP. Correlation of cortisol blood and saliva Analytical study B yes
1986 Cook N. Utility of dexa test CS and plasma cortisol level Trial B yes
1983 Vining RF salivary hormones Practical implications Article C yes
1982 Peters JR Salivary cortisol and adrenal reserve Article C yes
Table 2 - List of publications used regarding the relationship between salivary cortisol and plasma cortisol level
Results:
Of the 35 publications used, 31 found a correct correlation between the plasma cortisol level and salivary cortisol (i.e. 88%). If only publications with an “A” level of proof are considered, this rate reaches 100% (3 of 3).
El Farahn N (10) in 2017, in the form of a “development of the assay method of plasma, urinary and salivary cortisol levels”, states that “salivary cortisol reflects the variations in the plasma cortisol level and offers an alternative for the measurement of the free fraction of cortisol”.

Page | 35
Indeed, since the start of the work and publications on salivary cortisol, most findings show a reliable link between the plasma cortisol level and salivary cortisol in many situations, despite the different assay methods used. Salivary cortisol is frequently used for the study of stress and activation of the corticotropic axis.
Moreover, although not the subject of our work, the “salivary cortisol” test in the screening of corticotropic hyperactivity (Cushing’s syndrome) has shown good results (sensitivity and specificity). The same observations were made for the dexamethasone inhibition test. However, in clinical practice, we still use a conventional biological confirmation for the management.
The first major remark is: The absence of standardisation for the threshold values according to sex, time of sampling and
assaying (dependent on each sampling method and therefore laboratory).
And the use of different analytical tools.
With regard to hypocortisolaemia, the diagnostic utility is still little known. A limitation of salivary cortisol assays in the study of the adrenal insufficiency is their mediocre sensitivity at very low cortisol levels.
In this context, A. Perogamvros (28) presented a study comparing the results of the assay of salivary cortisol with plasma cortisol following an ACTH stimulation test. He noted a relative increase in salivary cortisol values after adrenal stimulation that were significantly greater and earlier than for plasma cortisol (p<0.0001).
In a discordant case between the result of normal salivary cortisol peaks but abnormal plasma, a CBG deficit was detected. The response peak of cortisol is delayed in saliva compared to plasma.
The team of Zhang Q et al. (29) showed intra-individual stability of salivary cortisol and the cortisol-cortisone ratio. Nunes and Tabarin (12) report that the salivary cortisol assay by liquid chromatography combined with mass spectrometry has a diagnostic performance equivalent to plasma cortisol, or even superior in situations where the CBG concentrations are changed.
Conclusion:
Current publications favour an acceptable correlation between the plasma cortisol level and salivary cortisol, both in the case of circadian variations, as well as following exercise or as a result of an exogenous glucocorticoids intake (for therapeutic purposes or for dynamic tests ).
In clinical research, good validity of this method is noted. The majority of publications agree on this point. This test is already integrated into the diagnosis of Cushing’s syndrome and in specific situations (depressive syndrome, post-traumatic stress syndrome, stress and anxiety, etc.). Salivary cortisol is used as a method of studying the corticotropic axis in many recent works.
On the other hand, the practical use of this assay is still limited by the lack of standardisation of threshold values, according to the type of test and laboratory. Further harmonisation and standardisation work would be useful to be able to use salivary cortisol routinely in screening for hypocortisolaemia in athletes.

Page | 36
6. Adrenal insufficiency and general pathology
In this chapter, we briefly discuss the general pathology of the corticotropic axis inducing hypocortisolaemia in order not to neglect this aspect, even in the context of sporting practice.
Adrenal insufficiency is a rare disease (1/10,000 people). The principal risk is acute adrenal insufficiency during stress, which can occur at any time and is potentially serious.
At the physiopathological level, we then describe, according to the location of the pathology:
Peripheral adrenal insufficiency: decreased adrenal function (hypocortisolaemia) with loss of central negative feedback and thus increased ACTH,
Central adrenal insufficiency: decreased adrenal function (hypocortisolaemia) in association with decreased central stimulation (normal or low ACTH).
a. Aetiologies
Peripheral adrenal insufficiency (Addison’s disease): Autoimmune origin (most common cause), Bilateral adrenal tuberculosis, During HIV infection (opportunistic infection, iatrogenic, etc.), In children: Adrenoleukodystrophy, enzymatic block, Other causes: bilateral adrenalectomy, iatrogenic (ketoconazole, etc.), bilateral lymphoma,
metastases (lung cancer, kidney, ENT, etc.), sarcoidosis, amyloidosis, adrenal thrombosis or ischaemia, etc.
Central adrenal insufficiency (corticotropic insufficiency): Sustained corticosteroid interruption, Hypothalamo-pituitary tumour, Autoimmune hypophysitis, Granulomatosis (sarcoidosis, etc.), Trauma, Pituitary surgery, Radiotherapy, Sheehan syndrome (pituitary necrosis following hypovolaemia),
b. Management
The overall management has 4 principal axes: Replacement therapy (hydrocortisone in combination with fludrocortisone if there is peripheral
adrenal insufficiency),
Aetiological treatment if possible, Therapeutic education (management of replacement therapy, prevention of acute adrenal
insufficiency, etc.), Monitoring of the treatment and adrenal function.
Acute adrenal insufficiency is the most feared complication, which is life-threatening if appropriate treatment is not initiated urgently.
The clinical picture of acute adrenal insufficiency is brutal with signs of extracellular dehydration, neurological signs (consciousness disorder, convulsion, coma), digestive signs (abdominal pain, anorexia, nausea, vomiting etc.), headaches, myalgias.

Page | 37
Biologically, there is haemoconcentration, acute renal function insufficiency, hyponatraemia, hyperkalaemia, hypoglycaemia, etc.
The aetiology can be spontaneous in a context of chronic adrenal insufficiency or come from a decompensation during an intercurrent event (infection, surgical stress, myocardial infarction, anaesthesia, etc.).
The treatment corresponds to the injection of hydrocortisone 100 mg to 200 mg in IV or IM in an attack, followed by maintenance treatment, re-equilibration of hydroelectrolyte disorders, associated with aetiological treatment and stabilisation of the underlying adrenal gland pathology as needed.
7. Corticotropic axis and physical activity
In addition to the previous pathological descriptions and the iatrogenesis studied at the end of this paper, in this chapter we will detail the influence of physical activity on the corticotropic axis.
Physical activity is a generic concept encompassing all the motor situations of a subject from a mechanical, energy and co-ordinative viewpoint. Physiologically, this corresponds to any muscle work increasing the baseline metabolism. There are therefore countless situations involving physical activity. Sport is a subtype of physical activity that includes the concept of competition, regulation and codification of practice as well as training.
In a 2003 epidemiological study during the regulatory follow-up of the FFC, Guinot et al. in 2005 (30) found that out of 1,549 samples, cortisol was higher in elite athletes than in amateurs, suggesting an effect of physical activity on the corticotropic axis.
The problem of this chapter then focuses on the following question: - Can sport and its various components induce hypocortisolaemia?
Is hypocortisolaemia a marker of over-training?
A- Physical exercise: intensity, duration and training
The initiation of the corticotropic axis is a physiological response to exercise and its energetic, metabolic, cardiovascular and neuropsychological needs.
In the course of physical exertion, as with any stress, Duclos M. and Tabarin A. (31) describe an increase in circulating ACTH concentration before an increase in the plasma cortisol level. Chronologically, a stimulation is noted in the secretion of CRH and AVP, thus inducing ACTH production and an increase in the plasma cortisol level. The initial factors that induce this secretion of CRH are varied: effect of catecholamines, decrease in blood glucose, variation of osmolarity and plasma volume, etc.
Intensity: The activation of the corticotropic axis generally occurs from a certain intensity threshold (VO2 max threshold), with an increase in the plasma cortisol level and blood ACTH in relation to VO2 max.
Yoon and Park (32) described a relationship between the increase in the plasma cortisol level in response to exercise and the intensity of this exercise: the more intense the exercise becomes, the more the plasma cortisol level increases. However, this relationship does not seem linear. Hartley et al. (1972) (15) reported a significant increase in the cortisol level from 75% VO2 max.

Page | 38
Navari et al. (1981) find a threshold value of 100% of VO2 max, while Rudolf et al. (1998) speak of a value of 60%, as do Hill et al. in 2008. These disparities are probably linked to the protocols and profiles of different subjects. The result, however, is the concept of a “threshold value”: intensity from which there is a noticeable increase in the plasma cortisol level, probably inherent in each.
Below these threshold values, Hartley et al. (1972) (33) found no increase in the plasma cortisol level for a VO2 max intensity of 42%, as did Jacks et al. (2002) for a value of 44% and Hill et al. (2008) for 40%.
Hill et al. in 2008 were also interested in the influence of exercise intensity on the corticotropic axis. Of their 12 subjects, they found a significant increase in ACTH secretion from a VO2 max intensity of 80%. The increase in ACTH was also described for supra-maximum exertions (above VO2 max) by Buono et al. in 1986 (34), Raastad et al. in 2000 (35) and Minetto et al. in 2007 (36).
It is therefore generally accepted to use 60% VO2 max of the threshold value from which a significant increase in the plasma cortisol levels is observed during exertion (over a period of one hour).
Duration: Contrary to intensity, the literature does not describe a “threshold” for duration. It is evident that these concepts of duration and intensity are linked. Below the threshold of 60% of VO2 max, a “time” effect is observed with a 40% activation of the VO2 max for a duration of at least 90 min. Conversely, at 90% of VO2 max, the corticotropic activation takes only 10 min. Numerous publications have been created on this subject, such as Fournier et al. (37) in 1997, who observed an increase in the plasma cortisol level from 33 km in ultramarathon runners until the end of the course.
Repetition: Similarly, repetitive physical activity induces a decrease:
in the peripheral tissue sensitivity to cortisol stimulation, suggesting an optimisation of the adverse effects linked to a state of hypercortisolaemia,
in the central sensitivity of the corticotropic axis to negative feedback, which could explain the faster response to secondary exercise following a recovery phase.
Training: The publications of Sutton et al. (1978) and Mastorakos et al. (2005) (38) demonstrate a reduction in the corticotropic response to exercise in trained subjects. The same observations were made by Paccotti et al. (2005) (39) (saliva assay), Makras et al. (2005) (40) (urine assay) and Minetto et al. (2007) (36) (plasma and salivary assays) that reported higher levels of cortisol in trained subjects compared to less trained or sedentary subjects during exertion.
At rest, Witter et al. (1996) found early onset of morning circadian ACTH in trained subjects treated compared to sedentary patients without notification of any similar changes in the plasma cortisol levels and cortisoluria. Duclos M. did not report any significant difference in the resting plasma cortisol level in athletes compared to sedentary subjects. The cortisol/free cortisol ratio is unchanged at rest.
On the other hand, a decrease in hypothalamic-pituitary sensitivity (Heuser et al. (41)) with negative feedback in trained subjects has been reported. The increase in the plasma cortisol level induces inhibition of the corticotropic axis. In sedentary subjects, therefore, a new stimulation does not induce a new increase in the plasma cortisol level, by this phenomenon of inhibition.

Page | 39
In trained subjects, a reduction of this feedback was described, with a greater increase in the plasma cortisol level observed in response to new exertion in relation to untrained subjects,
Type of exercise:
Similarly, muscular exercise of the eccentric type requires a larger corticotropic response than concentric exercise.
Chen YM. describes an increase in the plasma cortisol level with greater exertion for kayaking exertion compared to walking.
Kanaley et al. (42) described a variability of the corticotropic response to exercise with a circadian rhythm, with a maximum at midnight and a minimum at 9 a.m.
In 1989, Kraemer et al. (25) studied the effect of 10 weeks of sprint, endurance and mixed training on ATCH secretion. They noted a significant increase in ACTH in all 3 groups.
b- Recovery
According to the Research Institute on Wellness in Health and Sports Medicine (IRBMS), recovery means all the processes implemented to enable the body to regain the integrity of its capacities after physical exertion. It corresponds to the time necessary after physical activity to return to a state compatible with the reproduction of new physical activity.
In repeated exercises, the recovery time between exercise also influences the response of the corticotropic axis to exercise. An increase in the corticotropic response during the following exertion was described during a short recovery period compared to a long recovery period. This state is described as maximum at 120-150 min, with a classic corticotropic response to exertion for longer durations.
In trained subjects, the ability to respond to a second stimulus of corticotropic induction (exertion) is not changed, unlike in untrained subjects.
Luger et al. reported a more rapid return to a “normal” cortisol level in post-exercise in trained subjects than in non-trained subjects. Duclos et al., in 1997 (43), reported the same finding, with a more rapid decrease in post-exercise ATCH in trained subjects compared to sedentary subjects. The return to the normal post-exertion plasma cortisol level depends on the factors described above (duration, intensity, training).
c- Food and hydration
Duclos M. and Tabarin A. describe an increase in the corticotropic response to exercise in a dehydration situation, independently of the external temperature.
The diet increases the secretion of cortisol, in particular a diet rich in proteins. During prolonged exercise, carbohydrate intake limits the increase in the plasma cortisol level (Utter et al. in 1999 (44), Nieman et al. in 1998 (45), Deuster et al. in 1992 (46), Murray et al. in 1991 (47), Davis et al. in 1989).

Page | 40
d- Disorders of recovery and adaptation to exertion: fatigue and over-training syndrome
This corresponds to an objective and/or subjective decrease in physical performance without a reduction in the training load. In summary, this condition results from an imbalance of the “physical activity - recuperation” balance in favour of physical activity and to the detriment of recovery.
In addition to this imbalance, many other aetiological factors are taken into account. (Psychic disorders, food, stress, inflammatory or infectious states, sleep disorders, etc.). These states result from complex mechanisms (biological, neuroendocrine and psychological), incompletely understood at the present time.
Figure 13 - Over-training: aetiologies and clinical-biological signs (48).
There are several states, established in a probable continuum, between simple fatigue and over-training syndrome. Described for the first time since 1923, the definition of over-training syndrome differs according to authors, in particular in the intermediate forms (chronic non-functional fatigue and over-reaching).
Kreider et al. (49) propose the following definitions: Over-reaching (OR): the accumulation of stress induced or not by physical activity leading to a short-term decrease in performance capabilities with physical and/or psychological symptoms and signs. The restoration of the performance capacities takes several days to several weeks.
Over-training (OT): the accumulation of stress induced or not by physical activity leading to a long-term decrease in performance capabilities with physical and/or psychological symptoms and signs. The restoration of the performance capacities takes several weeks to several months.
Imbalance Exercise/recovery
Infection, injury
Stress Sleep deprivation
Nutritional disorders
Biological disruptions
energy reserves
neuroendocrine
haematological
immunological
etc.
Clinical symptoms
fatigue
sleep disorders
mood disorders
appetite disorders
etc.
Reduction in
performance
Over-training

Page | 41
Minor physiological · Positive physiological adaptations without adaptations and minor
change in performance performance
Minimal recovery time improvements ·Minimal recovery
time
Increasing intensity, duration, and frequency of training
Under-training Acute overload
Over-reaching
Optimal physiological and performance adaptations
Recovery in days to weeks
Over-training
Physiological maladaptations and decreased performance
Recovery in weeks to months
Figure 14 - Over-training Syndrome in the Athlete: Current Clinical Practice, Carfagno 2014
Urhausen and Kindermann, as well as Nelson and Jeukendrup (50), describe the following classification: Acute or immediate fatigue (post-exertion): duration 24-36 hours without alteration of
performance. Functional chronic fatigue: decreased performance, with return to baseline in several days or
weeks and then overcompensation. (functional over-reaching, OR). Non-functional chronic fatigue: decreased performance, with return to baseline in several
weeks, but obstructing the overcompensation phenomenon. (non-functional over-reaching, OR). Over-training syndrome: decrease in long-term performance, with return to baseline in several
months. (over-training, OT).
They therefore subdivide OR syndrome into functional and non-functional OR with a quantitative and qualitative barrier.
There is a fine line between chronic non-functional fatigue and over-training syndrome. Over-training syndrome therefore corresponds to the most serious and chronic form of the clinical picture, resulting in a very long recovery time. The fundamental characteristic is the persistence in time of a state of physical, biological, neurobiochemical and endocrine maladaptation.
The clinical presentation is of great semiological complexity. The screening is more complex and a clinical examination alone cannot reveal the pathognomonic signs of over-training. Similarly, there are no biological changes with major specificity for this screening. The use of the term “syndrome” refers to the multiple entity of clinical signs that may be present.
Without going beyond the scope of this work, we will limit ourselves to studying the link between the corticotropic axis and this state of over-training.
An advanced hypothesis would be the existence of multiple central endocrine dysregulation, which in our situation would correspond to an influence of chronic stress. Acute stress has been shown to induce activation of the corticotropic axis and, via the same mechanism, chronic stress could lead to central desensitisation in response to renewed stress.
For a long time, hypocortisolaemia has been described in over-training syndrome. In addition, the “Testosterone/Cortisol” plasma ratio has long been considered an indicator of OT. This ratio decreases according to the intensity and duration of training.
Barron et al. reported decreased secretion of ATCH and cortisol in over-trained subjects (in response to insulin-induced hypoglycaemia) compared to asymptomatic subjects. Urhausen et al., Meeusen et al. (51) make the same observations. There is thus a potential modification of the response and the adaptation of the corticotropic axis to exertion in over-trained subjects.

Page | 42
However, following more recent publications, these findings are far from unanimous. In the special communication “Prevention, Diagnosis, and Treatment of the Over-training Syndrome: Joint Consensus Statement of the European College of Sport Science and the American College of Sports Medicine” (51), a similar “resting cortisol” is described in endurance athletes during the recovery period and in sedentary subjects. The authors agree that a simple measure of the plasma cortisol level in the recovery phase is not a reliable indicator of OT.
The endocrine assays currently performed suffer from extreme variability linked to all factors cited in this chapter. In addition, many publications on the subject that found OT markers rather found markers of excessive stress induced by the exercise that can fit into the context of OR.
Despite the fact that the neuroendocrine system responds to acute or chronic stress, current information shows that a simple baseline measure of the plasma cortisol level cannot distinguish between athletes with good adaptation to a functional OR state from those who will suffer from OT. It would therefore be unlikely that hypocortisolaemia would be a sign of adrenal exhaustion or OT.
e- Age
In ageing adults, the response of the corticotropic axis to resistance training decreases. For aerobic exercise, this activation starts earlier. These characteristics do not differ between trained athletes and untrained subjects.
f- Other factors
Hypoxia and altitude At high altitudes and in hypoxic conditions, the increase in cortisol is greater for prolonged exertion at 85% VO2 max than at average or low altitudes. Park HY. in 2016 (32) observed an increase in the blood concentration of ACTH and cortisol following exercise in 10 girls of average 12.8 years of age on an ergocycle for 60 min in a 3,000 m simulated altitude chamber compared to sea level. He notes in 2014 (52) the accelerating increase in the plasma cortisol level in a group of hikers during a trek around Annapurna with the increase in altitude. These corticotropic changes were not observed in local natives (sherpas) who previously trekked the same route.
Hao K. in 2015 (53) notes that subjects with acute mountain sickness (AMS) have a higher CRH concentration than asymptomatic subjects at the same altitude. Woods Dr. in 2012 (54) found no significant correlation between AMS severity and the cortisol level. He found an increase in the morning baseline plasma cortisol level in subjects at rest at an altitude higher than 5,000 m. Panjwani U. in 2006 (55) describes an increase in the plasma cortisol level following an exposure of one hour at 3,500 m altitude.
Benso A. in 2005 (56) found no significant changes in cortisol concentration and ATCH concentration in 9 climbers who had spent 7 weeks at high altitudes (5,200 m after ascending Mount Everest at 8,848m). Dimai HP. in 2000 (57), Martignoni E. in 1997 (58) and Richalet JP. (59) in 1989 made the same observations.
Apart from other factors related to exercise in the mountains (cold, weather, stress, exertion), the high altitude in itself increases the corticotropic stress and thus the plasma cortisol level, as in any other stress situation.

Page | 43
g- Conclusion
Intense and regular physical activity causes an adaptation of the corticotropic function, which goes in the direction of faster response to new stress and the optimisation of corticotropic function. Even if the hypothesis was mentioned, the over-training syndrome does not appear to lead to adrenal exhaustion, despite the other endocrine and biological changes described in this context. Hypocortisolaemia is not a reliable and discriminating marker of over-training syndrome.
With the discovery of hypocortisolaemia in high-level athletes, the aetiological investigation cannot easily be explained by intense physical activity in itself and other more probable causes must be sought.
6 - Risks incurred by athletes in hypocortisolaemia during physical activity
In addition to the medico-legal and sporting consequences arising from the discovery of hypocortisolaemia whatever its aetiology, the question of the risk incurred by athletes is a crucial medical factor in athletes’ health.
With the risks and undesirable effects of corticosteroids, this issue is the focus of the MPCC’s work in the context of monitoring the health of cyclists.
The problem of this chapter focuses on the following question: What are the risks incurred by athletes in adrenal insufficiency (screened or not) who engage in
physical exertion?
a. Introduction
In the general population in the 1970s, it was recognised that a person with balanced adrenal insufficiency had a life expectancy similar to a healthy person. Recent work (Nunes M.L. in 2008, in the Endocrine Society congress 2008, Reznik Y. in 2014, Elfeleh E. in 2016) call this concept into question and suggest an increase in morbidity and mortality.
The difficulty of this situation lies in the possible presence of athletes in a situation of adrenal insufficiency that is totally asymptomatic following the administration of exogenous glucocorticoids.
b. Pathophysiology
The exogenous administration of glucocorticoids decreases the synthesis and secretion of CRH. The latter induces a decrease in the secretion of ACTH with atrophy of the anterior pituitary cells. The adrenal cortex loses its ability to produce cortisol. This decreased cortisol secretion can take several days, weeks or even months to return to its former level.
In the event of a sudden cessation of corticosteroid therapy or in the event of stress, the risk is acute adrenal insufficiency, which is generally symptomatic.
There are then 3 situations: Decompensation of the adrenal insufficiency in the form of acute adrenal insufficiency,
Decrease in performance induced by chronic adrenal insufficiency, Adverse effects of corticosteroid therapy.

Page | 44
c. Acute adrenal insufficiency
This situation can occur conventionally following the sudden cessation of corticosteroid therapy used in the long term, but more rarely in subjects on balanced corticosteroid therapy who undergo unusual stress as may result from the sporting practices.
It is difficult to estimate the real frequency of acute adrenal insufficiency after corticosteroid therapy, as there is no systematic declaration of this complication at the pharmacovigilance centres and/or there are gross forms. It is likely that its incidence is low, but glucocorticoids are prescribed very frequently in general medicine as in sports medicine.
Acute adrenal insufficiency is life-threatening and can lead to death if the treatment is insufficient or initiated too late. Death may be due to hypotension, cardiac arrhythmia or central impairment.
In concrete terms, this biological situation corresponds to a situation where the body is unable to respond adequately to severe stress (anaesthesia for surgery, bacterial infection, haemorrhagic shock, major trauma, intense exercise). Indeed, these situations require that the adrenal glands secrete an increased quantity of cortisol, an essential hormone for metabolic and cardiovascular adaptations for the survival of the body.
Physical exercise and high-level sports practice may therefore involve additional circumstances which increase the need for cortisol and therefore can compensate for underlying corticotropic insufficiency. As in general pathology, any form of stress may be the triggering factor. In the context of sport, the following situations can be considered stress:
Brutal exposure to changes in temperature and environmental conditions (cold, heat, hypoxia at high altitude, etc.),
Surgical intervention necessary after trauma, Anaesthesia and the post-operative acute phase are 2 situations that increase corticotropic stress,
Isolated or multiple trauma, Hypoglycaemia, increased in case of intense and/or prolonged exertion in endurance sports, for
example. Infections (frequent in high-level athletes).
In rare cases, this acute adrenal insufficiency can occur spontaneously in rapid and important forms (underlying pathology).
d. Chronic adrenal insufficiency
The dysfunction of the corticotropic axis could be at the origin of decrease in performance. According to Duclos M, this state of chronic adrenal insufficiency could impede the multiple endocrine adaptations to stress, in particular catecholamines and neoglucogenesis. The response of catecholamines to prolonged stress is diminished, leading to a reduction in cardiovascular adaptation to exercise (relative hypotension, deviations of heart rate) and a tendency to hypoglycaemia. This clinical picture could lead to symptoms similar to the classic sudden fatigue or ravenous hunger of endurance races.

Page | 45
We note the associated presence of signs of chronic (or slow) adrenal insufficiency described conventionally in general pathology but changing the ability to perform physical exertion:
Physical and psychological asthenia, increased during the day and on exertion, Weight loss and anorexia, with caloric and energy restriction, Nausea, vomiting, abdominal pain and digestive disorders that can impair proper hydration and
nutrition during prolonged exertion. More rarely: thymic disorders (depressive syndrome, emotional lability), dysmenorrhoea in
women.
According to Bonifazi M., whose expert opinion was sought by the FFC on the subject (Annex 7), corticotropic inhibition may also change the body’s response to training and limit the adaptation to workloads necessary to improve performance.
e. Adverse effects of corticosteroids
As hypocortisolaemia principally reflects the use of corticosteroids, the risks incurred are also those of the adverse effects of corticosteroids in the short and long term. As they are not the principal concern of our work, they will simply be quoted below without going into detail.
These adverse effects are: Hydroelectrolytic (hypokalaemia, metabolic alkalosis, hydrosodic retention, etc.), Endocrine (Cushing’s syndrome and hypercorticisms, adrenal insufficiency, hyperglycaemia,
corticosteroid-induced diabetes, etc.), Cardiovascular (arterial hypertension, atrial fibrillation, congestive heart failure, venous
thromboembolic disease, etc.), Muscular (myopathies, muscular atrophy, etc.), Osseous (aseptic osteonecrosis of femoral heads, jaw, cortisonic osteoporosis), Cutaneous (atrophies, ecchymoses, stretch marks, hypertrichoses, delayed healing, purpura,
acne, etc.),
Ophthalmological (posterior cataracts, glaucomas, etc.), Neuropsychological (confusion, depressions, convulsions, euphonies, insomnia, irritability,
excitation, etc.),
Immune-related (immunodepression increasing the risk of viral, bacterial, parasitic or mycotic infections, rare cases of hypersensitivity, etc.),
Gynaecological (dysmenorrhoea, oligomenorrhoea, etc.), Morphological (growth disorder, change of body fat distribution (cushingoid facies), etc.),
Metabolic (hypercholesterolaemia, pancreatitis, etc.).
f. Conclusion
As the MPCC notes: “it is clear, and all physicians agree, that there is a high risk to health for athletes when their cortisol level is abnormally low.” Although chronic adrenal insufficiency is an undeniable factor in under-performance, in particular in endurance, the major risk to the health of athletes is acute adrenal insufficiency, which can unfortunately occur at any time and, of course, even more frequently in the aftermath of major stress, which may be present during physical exertion. The decision to withdraw from competition in the event of hypocortisolaemia is therefore appropriate, if the risk information is clearly explained to athletes. The practice of physical activity, even outside of competition, must be limited and proscribed pending the aetiological investigation and a return to “normal” corticotropic activity.

Page | 46
1- Introduction
The aim of this second part is to detail the precise influence of different glucocorticoids types on the plasma cortisol level according to their route of administration via a literature review.
As described above, the discovery of hypocortisolaemia in athletes must initially give rise to suspicion of adrenal insufficiency of iatrogenic origin.
For information, the following table shows the different corticosteroids detected in urine by the World Anti-Doping Agency (WADA) from 2012 to 2014.
GC 2010 2011 2012 2013 2014
Betamethasone 27 25 30 35 34
Budasonide 111 113 157 135 74
Denozacort 3 1 1
Dexamethasone 8 21 18 18 12
Fluticazone 1 2 1 2
Methylprednisolone 7 16 15 14 14
Prednisone 16 19 60 55 44
Prednisolone 9 19 67 68 56
Prednisone + prednisolone 39 40
Triamcinolone 6 2 1 1 1
Triamcinolone acetonide 7 16 16 12 16
Total GC 234 274 365 330 252
% GC/total infraction 4.2 4.9 8.1 6.3 8.0
GC: glucocorticoid; WADA: World Anti-Doping Agency.
Table 3 - Prevalence of glucocorticoid use according to WADA. From “Glucocorticoid administration in athletes: performance, metabolism and detection”, Collomp K. 2016.
This table illustrates the increase in the proportion of corticosteroids in total contraventions reported by WADA between 2010 (4.2%) and 2014 (8%), led by budesonide and prednisolone.
In 2002, through the results of self-filled questionnaires sent to cyclists, the FFC found that 85 of the 538 athletes surveyed (15.8%) took corticosteroids in the previous 3 months. In addition, 11 of the 12 cyclists with a low plasma cortisol level (92%) used corticosteroids.
Winter S. (60), in a retrospective study of the medical observations of athletes penalised for doping by the AMPD (Antenne Medicale de Prevention du Dopage) of Rhone-Alpes between 2002 and 2012, described that glucocorticoids were in 2nd place among detected substances at 19.3%. In this study, 62.4% of athletes who tested positive for the use of glucocorticoids reported a single therapeutic use of this medication class.
Of the 1,330 TUEs issued by WADA in 2015, 431 were reported for corticosteroids (35%).
PART 2 — LITERATURE REVIEW: HYPOCORTISOLAEMIA AND EXOGENOUS GLUCOCORTICOIDS

Page | 47
All this epidemiological data confirms the frequent use of corticosteroids in sports.
The principal research focus of this chapter is on the influence of exogenous glucocorticoid intake (regardless of the route of administration) on the plasma cortisol level.
2- Materials and methods
To do this, we performed a literature review, with a description of the research in qualitative narrative form, classified according to the different means of use of glucocorticoids. We have not deliberately detailed the oral and intravenous routes, as their influence on the plasma cortisol level is known and has already been described many times.
The bibliographic search was performed with the usual medical and scientific search engines (PubMed, The Cochrane Library, MEDLINE, Google Scholar). Additional data from experts was added to this work and detailed in each chapter.
We have selected the studies with the following inclusion criteria: Age above 3 years, men and women included, Healthy or pathological subjects.
Note: after reflection, we did not include the criterion “physical activity”, due to a low number of publications in athletes.
We limited our selection of publications with the following exclusion criteria: Pre-existing pathology of the corticotropic axis known or discovered during the study, Extreme age (less than 3 years and above 85 years), Concomitant use of corticosteroids by another route of administration.
The publications were selected by reading their abstract. The publications used were reviewed in full.
The keywords used for each search are mentioned in each chapter. A table summarising the publications used in reverse chronological order is annexed to each chapter. It includes the date of publication, principal author, summary of the purpose, type of publication, level of scientific proof and an annotation on the possible influence of glucocorticoid studies on the plasma cortisol level.
As a reminder, the classification of the levels of scientific proof (61):
LEVEL OF SCIENTIFIC PROOF PROVIDED BY THE LITERATURE
RECOMMENDATIONS GRADE
Level 1 Randomised comparative trials of high power – Meta-analysis
of randomised controlled trials - Decision analysis based on
well-conducted trials
A
Established scientific proof
Level 2 Low-power randomised trials - Well-conducted non-randomised
comparison trials - Cohort trials
B
Scientific presumption
Level 3 - Case-control trials
Level 4 - Comparative trials with significant biases - Retrospective trials - Series of cases - Descriptive epidemiological trials (transverse, longitudinal)
C
Low level of scientific proof
Table 4 - Level of scientific proof and recommendations

Page | 48
3- Results
a. Inhaled corticosteroids
Inhaled corticosteroids (ICSs) are anti-inflammatory molecules indicated primarily for the treatment of persistent asthma (mild and moderate) and severe COPD conditions. Since their appearance on the market in the year 1986, the management of these pathologies has been improved.
The prevalence of asthma in the general population is estimated at 7-8% according to trials. In the sports population, there is an increase in this prevalence. In 2000, Weiler et al. evaluated the prevalence of asthma and anti-asthma treatments at the 1998 Winter Olympics. They recorded 21.9% of asthma patients, 18.4% of whom had taken treatments for this pathology. It must be noted that 17.4% used these treatments chronically for a so-called persistent pathology.
In the same publication, this prevalence varies according to the sport. The highest prevalences are found in the Nordic combined, cross-country and so-called short races. The lowest prevalences are found in bobsleigh, luge, biathlon, sledging, curling and ski jumping.
In 1984, the figure of 11.2% was reported. In 1996 (Atlanta Olympic Games), the prevalence reached 16.7%. In 2010, in the GA2LEN study (2008 Olympic Games), the athletes reported having asthma diagnosed by a physician in 17% of cases (versus 7% in the general population) and more often using therapeutics for this pathology (10% versus 4%). The risk of asthma was significantly higher in high-performance athletes than in the general population.
In 2012, the prevalence was 8% for Olympic athletes.
Arnaud M. in 2010, in his observational study in ultra-trainers of the Diagonale des fous, reported 22.95% of athletes who declared themselves as treated by anti-asthmatic background treatment.
Overall, the prevalence of asthma is frequently described as higher in the sports population than in the general population. It is also assumed that, for athletes exposed to cold (winter sports) and water (swimming), the prevalence of asthma is greater. According to Lebar V. (TUE supervisor at AFLD), in 2009, 80% of TUEs related to asthmatic pathology.
The use of ICSs is thus very frequent in the sports environment, as it is in the general population.
In the French national market, many molecules are currently available. The main ones are as follows: Beclomethasone (BECLOJET®, BECLOPHAR®, BECLOSPIN®, BECOTIDE®, MIFLASONE®, QVAR®) Budesonide (PULMICORT®, MIFLONIL®) Ciclesonide (ALVESCO®) Fluticasone (FLIXOTIDE®) Mometasone

Page | 49
Fraction
Oral bioavailability
10-40% deposited in
bronchi
I
Oral cavity & pharynx Lung
Absorption (lung)
Absorption by the stomach
GI tract
Inactivation by
1st hepatic passage
Systemic
AEs
Swallowed fraction
60-90%
General circulation
Liver
Figure 15 - Pharmacokinetics of inhaled corticosterides (63).
The different dosages of these molecules is summarised in the following equivalence table:
Dose Low
Dose Average
Dose Strong
Beclomethasone 3 µm Beclomethasone 1 µg
200-500 µg/day 100-200 µg/day
>500-1,000 µg/day
>200-400 µg/day >1,000 µg/day >400 µg/day
Budesonide 200-400 µg/day 400-400 µg/day >800 µg/day
Fluticasone 100-250 µg/day 250-500 µg/day >500 µg/day
Mometasone 100-200 µg/day >200-400 µg/day >400 µg/day
Ciclesonide 80-160 µg/day >160-320 µg/day >320 µg/day
Table 5 – Inhaled corticosteroids, from the National College of Medical Pharmacology (62).
These molecules can be administered alone or in combination with a long-acting beta-2-mimetic in moderate persistent asthma and severe COPD:
Beclomethasone + formoterol (INNOVAIR®), Fluticasone + salmeterol (SERETIDE®), Budesonide + formoterol (SYMBICORT®).
Pharmacokinetics: There are many different inhalation devices, generally with an active fraction which represents 10 to 40% of the inhaled dose. The ingested fraction thus represents 90 to 60% (Figure 15). This ingested fraction possesses a strong effect on first hepatic passage and therefore its elimination is quasi-complete and its metabolic activity is lower. The systemic passage is considered higher by the inhaled fraction.
At the bronchial level, inhaled corticosteroids act on many cell types (lymphocytes, mast cells, polynuclear eosinophils, smooth muscle cells).

Page | 50
Number of publications
All the molecules used have pharmacokinetic and pharmacodynamic parameters of their own (buccal deposition, stasis time and pulmonary volume, microparticle size).
The goal of ICSs is to approach the maximum bronchial concentration and decrease the plasma concentration responsible for general adverse effects and hypocortisolaemia.
Inhalation devices: Inhalers
o Aerosol dispenser or spray, o Dry powder inhaler (Diskus®, Turbuhaler®, etc.), o Autohaler, doser aerosol triggered by inhalation.
Inhalation chamber
Theoretically, the systemic transition is linked to the: Molecule and its dosage, Duration of treatment, Inhalation device, Method of use of the inhalation device, Particle size, Affinity with corticosteroid receptors, Physicochemical properties (solubility, etc.), and the severity of the underlying pathology.
The following figure summarises the number of publications on the PubMed search engine. It is noted that there has been a great deal of interest in this subject since the mid-1990s.
Figure 5- Evolution of the number of PubMed publications on the influence of ICSs on the plasma cortisol level from 1955 to
January 2017.
Research: We used the publications from January 1990 to February 2017, having as the principal (or accessory) criterion the evaluation of the plasma cortisol level in healthy or sick subjects treated with inhaled corticosteroids.

Page | 51
MeSH: Inhaled corticosteroids, Cortisol, HPA Search engines: PubMed, Google Scholar, Cochrane, Med Line Initial number of publications: 1,200 Number of publications used: 112
Year Authors Goals Publication type
Standard of proof Link
2016 O'Byrne PM Safety and efficacy of fluticasone 100 and 200 µg/d Trial B no
2016 Kowalski ML Corticotropic inhibition following ICSs for asthma Literature review B variable
2015 Cavkaytar O Moderate and elevated ICS dose and corticotropic axis
Observational study C
yes (dose)
2015 Zheng J Efficacy and safety of fluticasone/vilanterol Trial B no
2015 Chen X Pharmacodynamics of Fluticasone/Vilanterol Trial B yes
(dose)
2014 Woodcock A Efficacy and safety of fluticasone 100 and 200 µg/day Trial A no
2014 Oliver A Efficacy and safety of fluticasone Trial A no
2014 O'Byrne PM Fluticasone vs. Fluticasone Vilanterol Trial B no
2013 Muley P Efficacy and safety of fluticasone Literature review B no
2013 Woodcock A Fluticasone furoate vilanterol vs. fluticasone propionate salmeterol
Trial B no
2013 Nakahara N Fluticasone 200, 400 et 800 µg and axis Trial B yes
(dose)
2013 Allen A Fluticasone vilanterol 100 and 200/25 and cortico axis Trial B no
2013 Kosoglou T Mometasone 400, 200 fluticasone placebo Trial B yes
(dose)
2013 Busse WW Safety and efficacy fluticasone vilanterol Trial B yes
2011 Skoner DP Mometasone 100 and 200 µg/d children and axis Trial B no
2011 Woodcock A Fluticasone 1 time/d vs. 2 times/d Trial B yes
(dose)
2010 O’Connor BI Efficacy and safety of ciclesonide 320 and 640 2 times/day Trial A no
2010 Maspero JF Long-term safety of mometasone/formoterol Trial B yes
2010 Santiago AH Acute adrenal insufficiency and fluticasone Case report C yes
2010 Pedersen S Efficacy and safety of Ciclesonide 40, 80 and 160 µg/day Trial A no
2010 Kosoglou T Mometasone 2 x 200 µg/d and 4 x 100 µg/d vs. placebo Trial B no
2010 Skoner DP Mometasone 100, 200 and 400 µg/d Trial B yes
(dose)
2009 Craig T Literature review Ciclesonide Literature review C no
2008 Andrade CR Fluticasone 200 and 300 and cortico axis Trial B no
2008 Wlodarczyk IH Impact of ICSs on cortico axis in asthmatic adults Meta-analysis A
yes (dose)
2008 Kerwin EM Fluticasone/salmeterol 1 time/d vs. 2 times/d Trial B no
2008 Bateman ED Ciclesonide 160 and 640 µg/day Trial B no
2007 Breborowicz A Adrenal function in asthmatic children
Study study C no
2007 Mallol J Budesonide 800 µg/day or 400 µg 2 times/day Trial B no
2006 Dahl R Ciclesonide in the treatment of asthma Article C low
2006 Chereches PP Evaluation of effects of ICSs on morning plasma cortisol level
Study study C yes
2006 Metzer EO Literature review Ciclesonide Literature review C no
2006 Gelfand EW Ciclesonide 40, 80, 160 µg Trial A no
2006 White M Long-term ICS effect on corticotropic axis Analytical study B yes
(dose)
2006 Milinarsky T A Highdose budesonide and cortico axis children asthma Analytical study C yes
(dose)
2005 Szefler S Ciclesonide and corticotropic axis in asthma Trial B no
2005 Rohataqi S Pharmacokinetics of Ciclesonide
Study study C low
2005 Altintas DU ICS long-term effects and corticotropic axis Trial B no
2005 Lipworth BJ Effect ciclesonide and fluticasone on corticotropic axis Trial B yes
2005 Kaur C plasma cortisol level after budesonide beclomethasone high dose Analytical study B no
2005 Chapman KR Ciclesonide 160 µg and 640 µg per day Trial B no
2005 Lee DK Fluticasone and ciclesonide hight dose and corticotropic axis
Trial B variable
2005 Lee DK Fluticasone high dose 2,000 µg per day Analytical study B yes
2004 Fardon TC Fluticasone and mometasone and corticotropic axis Trial B yes
(dose)
2004 Bacharier LB Long-term efficacy of budesonide 400 µg/day Trial B no
2004 Reynolds NA Ciclesonide article C no

Page | 52
2003 Sim D High-dose fluticasone and corticotropic axis Analytical study B yes
2002 Alsaeedi A Literature review effects ICSs and COPD Literature review B yes
2002 Eid N Hypocortisolaemia asthmatic children on fluticasone
Study study C yes
2001 Chen A ICS side-effects in asthmatic children Analytical study B yes
(dose)
2001 Casale TB Comparison flunisolide fluticasone and corticotropic axis Trial A yes
2001 Fireman P Safety and long-term efficacy of beclomethasone Trial B no
2001 Adams N Budesonide variable dose in chronic asthma Literature review B yes
(dose)
2000 Gupta D Beclomethasone low dose and corticotropic axis Analytical study C yes
2000 Mackie AE Relationship fluticasone and plasma cortisol level - cortisoluria
Literature review B yes
2000 Wilson AM Dose response of budesonide in asthmatics Trial B yes
(dose)
2000 Ringdal L Comparison fluticasone budesonide and effect on axis Trial A no
1999 Lipworth BJ ICS literature review and corticotropic axis Literature review B yes
(dose)
1999 Scott MB Safety and efficacy of budesonide in paediatric asthma Trial B no
1999 Kemp JP Budesonide 1 time per day children asthma Trial B no
1999 Derom E Systemic effects fluticasone budesonide Trial B yes
(dose)
1999 Hughes JA Prospective study 1 year high dose ICS Trial B no
1999 Li JT ICS long-term effects and corticotropic axis Trial A yes
1999 Ferguson AC Efficacy and safety of fluticasone and budesonide Trial B no
1999 Baker JW Budesonide 1 time or 2 times per day vs. placebo children asthma
Trial A no
1998 Fitzgerald D Fluticasone 750 µg vs. beclomethasone 1,500 µg for asthma
Trial B yes
(dose)
1998 Shapiro G Budesonide 250/500/1,000 µg/day in paediatric asthma Trial A no
1998 Wilson AM Systemic effects budesonide vs. triamcinolone adults Trial B no
1998 Chrousos GP Corticotropic inhibition and use of ICSs Literature review B yes
(dose)
1998 Wilson AM Morning peak cortisol and fluticasone aldosterone Trial B yes
1998 Shapiro G Efficacy safety budesonide 200 and 400 µg children asthma Trial A no
1998 Aaronson D Budesonide 800 and 1600 µg per day and corticotropic axis Trial B no
1998 Paggiaro PL Fluticasone and COPD Trial A variable
1998 Pauwels RA Fluticasone and beclomethasone in moderate asthma Trial A no
1998 Wilson AM Fluticasone and budesonide in adult asthma Trial B yes
(dose)
1997 Donnelly R Effect of budesonide and fluticasone on corticotropic axis Trial B yes
1997 Grebe SK Beclomethasone and corticotropic axis Analytical study C yes
1997 Wilson AM Dose effect fluticasone and triamcinolone adults asthma Trial B yes
(dose)
1997 Clark D1 Marker corticotropic inhibition in asthmatics Trial B yes
(dose)
1997 Condernill Fluticasone triamcinolone in asthmatics Trial A no
1997 Santen RT Comparison ICSs and oral cortico in COPD Analytical study B yes
1997 Grahnen A Plasma cortisol level fluticasone and budesonide Trial B yes
(dose)
1997 Clark D1 Corticotropic inhibition fluticasone vs. budesonide Trial B yes
(dose)
1996 Clark D1 Corticotropic inhibition fluticasone children asthma Trial B yes
1996 Todd G Growth and corticotropic inhibition in children asthma Article C yes
1996 Boorsma M Systemic effects fluticasone budesonide Trial B yes
1996 Girbino G Beclomethasone in asthma: new system Trial B yes
1996 Hasegawa T Effect high dose beclomethasone asthmatic Trial B yes
(dose)
1996 Clark D1 Corticotropic inhibition budesonide vs. fluticasone Trial B yes
1996 Lonnebo A Systemic effects repeated doses fluticasone budesonide Trial B yes
1995 Volovitz B Diurnal variation plasma cortisol level children budesonide Analytical study C no
1995 Doull I1 Effect of ICSs on cortisol in moderate asthma Trial B yes
1995 Pedersen S Budesonide in moderate to sever asthma Trial B no
1995 Grove A Comparison systemic activity budesonide fluticasone Trial B no
1994 Grahnën A Systemic effects fluticasone 1 dose healthy subjects
Study study C yes
1994 Boe 1 ICSs high dose asthma and systemic effects Trial A yes
1994 Nicolaizik WH Endocrine and pulmonary function ICSs children asthma Trial C yes
1994 Hasegawa T Corticotropic inhibition in asthmatics Trial B yes

Page | 53
1994 Gagnon M Efficacy and safety 1 or 2/d beclomethasone asthma Trial C no
1994 Leblanc P Fluticasone 200 µg/day vs. beclomethasone 400 µg/day for asthma
Trial A no
1994 Francia G Corticotropic axis high dose beclomethasone
Study study C
yes (dose)
1993 Volovitz B Asthma budesonide 100 µg 2/d and corticotropic axis
Study study C no
1993 Fabbri L Fluticasone vs. beclomethasone in moderate asthma Trial A yes
1993 Ninan TK Effects high dose ICSs on corticotropic axis children asthma
Study study C
yes (dose)
1993
Hoffmann-Streb A Adrenal function asthma on fluticasone
Observational study C no
1993 Ribeiro LB Budesonide: efficacy and safety long term children Analytical study B no
1993 Hayashida M Beclomethasone: long-term efficacy children asthma
Observational study C no
1992 Kastunuma T Beclomethasone 300 µg/d children asthma
Observational study C no
1992 Philip M Plasma cortisol level asthmatic children ICS long term Analytical study C yes
(dose)
1991 Brown PH Evaluation of corticotropic function asthma high dose ICS
Observational study C yes
1991 Prahl P Corticotropic inhibition budesonide vs. beclomethasone Trial C variable
1990 Yamaguchi M Effects beclomethasone 800 µg per day Trial B yes
1990 Varsano I Safety after 1 year of budesonide in paediatric asthma
Observational study C no
Table 6 - List of publications used regarding the influence of inhaled corticosteroids on the plasma cortisol level
Results:
The number of publications on the subject is very large, with very different methodologies and levels of proof. The vast majority of these publications relate to a young asthmatic population. There are few publications related to the use of ICSs and physical activity.
According to the National College of Medical Pharmacology, “corticosteroids administered by inhalation cause minor changes in the function of the hypothalamic-pituitary axis. These inhibitory effects exerted on the hypothalamic-pituitary axis relate to all molecules and are dose-dependent. The clinical significance of these biological disorders is not clearly established. Several trials have shown that the probability of occurrence of adrenal insufficiency (…) under inhaled corticosteroids is low, except at high doses. ”
The epidemiostatistic technique of capture-recapture estimated that there were 598 cases of adrenal insufficiency following the use of inhaled corticosteroids in the period 2000 to 2005 in France. This figure is most likely underestimated due to the low specificity of the symptoms of adrenal insufficiency and the low level of screening.
As the table above shows, the data is very heterogeneous, variable in terms of results, methodology, included subjects and levels of proof. To clarify the interpretation of this data, we have chosen to describe these results by categorising the ICSs factors playing a suspicious role in the plasma cortisol level.
Dose and posology:
In 2008, Wlodarczyk JH. (64), in a meta-analysis involving 31 trials, found a reported corticotropic inhibition of low doses of ICSs which increase significantly with an increase in the dosage.
The Bordeaux pharmacology and endocrinology teams were interested in the prevalence and clinical presentation of adrenal insufficiency following inhaled corticosteroid intake. They describe that inhaled corticosteroids at doses greater than 400-500 μg/d in children and 800-1,000 μg/d in adults can induce adrenal insufficiency

Page | 54
In the study by Mortimer, the mean daily doses of inhaled corticosteroids in patients with iatrogenic adrenal insufficiency were 1116 pg/d for beclomethasone dipropionate, 444 pg/d for budesonide and 890 pg/d for fluticasone propionate.
According to Tetu L. (65), the systemic side-effects are therefore exceptional, up to 1,500 WI beclomethasone equivalent in adults and in children up to doses of 400 to 600 pg/d.
Taytard A. in 1999 (updated in 2012) considers that the systemic effects occur after a treatment duration of more than 1 year or at doses exceeding 1,500 pg of beclomethasone equivalent.
Claudia R. De Andrade in 2008 (66) found no effect of inhibition on the corticotropic axis in the use of 200 pg and 300 pg of fluticasone in asthmatic children aged 11 years and less. Oliver A. in 2014 (67) made the same finding in asthmatic children aged 5 to 11 years treated with fluticasone 100 pg per day. However, Schwartz RH. (68), in a literature review on PubMed in 2012 found 92 cases of adrenal insufficiency following the use of inhaled fluticasone in children with asthma, at doses of less than 500 pg per day.
In a pharmacacoepidemiological study of 11,783 paediatricians, endocrinologists, pulmonologists and ICU physicians in France, who received a questionnaire by mail with regard to corticotropic insufficiency in patients treated with inhaled corticosteroids between 2000 and 2005, 70 cases of adrenal insufficiency were reported (of which only 46 were validated by the expert committee). 23 subjects had clinically isolated adrenal insufficiency and 23 had adrenal insufficiency associated with clinical corticosteroid impregnation signs.
The prescribed inhaled corticosteroids were fluticasone, budesonide and beclomethasone and all were consumed at high doses (exceeding 500 pg/d beclomethasone equivalent in children and 1,000 pg/d in adults). A majority of cases of adrenal insufficiency involved fluticasone (7 out of 14 cases in children and 20 out of 30 cases in adults).
In 2012, Milner W. (69), studied the ICS dose and the combination of intranasal corticosteroids as predictive factors of corticotropic axis inhibition in 143 children with asthma.
In 2005, Kaur C. (70), in a publication on 15 asthmatics with a low level of proof, found no change in the plasma cortisol level following 6 weeks of high-dose budesonide and beclomethasone (2,000 pg/d).
Martin RJ. in 2002 (71) attempted to demonstrate a threshold value of 6 inhaled corticosteroids from which corticotropic inhibition was noted (decrease of the area under the plasma cortisol level curve) in steroid-naïve asthmatic subjects. He determined threshold values of flunisolide at 936 pg/d; triamcinolone at 787 pg/d; beclomethasone at 548 pg/d; fluticasone dry powder at 445 pg/d; budesonide at 268 pg/d; and fluticasone at 111 pg/d.

Page | 55
Cortico-inhibitory dose of different inhaled corticosteroids
Budesonide Fluticasone Ciclesonide Beclomethasone Mometasone
Figure 6 - Estimation of corticosteroid threshold dose according to the inhaled corticosteroid used.
Although the definition of the “threshold” value from which corticotropic inhibition occurs is difficult to make, given the many other factors involved, interindividual variability, as well as the very different methodologies of the publications, the above figure summarises the mean data found in our literature review paper for ICSs checks. Beyond these threshold doses, the inhibitory effect is commonly described.
Molecules:
Budesonide: In 2007, Mallol J. (72) found no difference in corticotropic inhibition between the intake of 800 µg per day and 400 μg 2 times per day.
Milinarsky T.A. in 2006 found 3 cases of corticotropic inhibition in 20 children receiving 80 0μg of
budesonide for severe persistent asthma. At the pharmacodynamic level, Lonnebo A. (73) described a frequent inhibition of the corticotropic axis following the taking of budesonide. As summarised in the following figure from his publication, the dosage is a major factor in the level of inhibition.
Dose (µg/day)
Absence of inhibition
Variable inhibition according to literature

Page | 56
Individual predictions Observations
Figure 7 - Evolution of the plasma cortisol level and blood concentration of ACTH according to the dose of budesonide
In 2004, Bacharier LB. (74) did not find corticotropic inhibition following the long-term use of budesonide 400 μg per day for 12 to 36 months in 63 asthmatic children.
Aaronson D. in 1998 (75) did not find any significant corticotropic inhibition with the use of therapeutic doses (800 to 1,600 μg per day) in asthmatic patients. On the other hand, at higher doses (3,200 μg per day), there is significant inhibition of the corticotropic axis.
Fluticasone: Many publications have demonstrated that fluticasone is the ICS that most strongly inhibits the corticotropic axis. O’Byrne PM. (76), in a double-blind, randomised trial in adult and asthmatic adolescents (Phase II and Phase III trial) showed that inhalation of fluticasone at a dose of 100 and 200 μg per day had no influence on the corticotropic axis. The same findings were made by Woodcock A. in 2014 in a double-blind, multicentre trial at the same doses.
In 1999, Lipworth BJ. (77), in a literature review from 1966 to 1998, found a corticotropic inhibition categorised as marked with high doses of ICSs (around 1.5 mg/d and even 0.75 mg/d of fluticasone). He noted a higher level of this adverse effect with fluticasone (compared to beclomethasone, triamcinolone and budesonide).
In a double-blind, randomised trial, Woodcock A. (78) found no difference between fluticasone furoate vilanterol 100/25 μg and fluticasone propionate salmeterol 250/50 μg in terms of the plasma cortisol level.
In the same year, Nakahara N. (79) described an increasing corticotropic inhibition of fluticasone (200 < 400 < 800 μg/d) in healthy subjects.
Observations
Observations
Observations
Individual predictions
Individual predictions
Individual predictions
Population predictions
Population predictions
Population predictions
Placebo
Active
Placebo
Active
Co
rtis
ol
co
nce
ntr
ati
on
s
(nm
ol/
L)
AC
TH
co
nc
en
tra
tio
ns
(pm
ol/
L)
Bu
de
so
nid
e c
on
cen
tra
tio
ns
(µg
/L)
Time (hrs)

Page | 57
In the same way in 2005, Whelan GJ. (80) described a linear relationship between increased blood fluticasone concentration and decreased plasma cortisol level.
In predictive terms, Cavkaytar O. (81) found a threshold of 291 μg/d fluticasone in 2015, from which there would be significant inhibition of the corticotropic axis. Allen A. (82) in 2013 defined this threshold at 200 μg per day.
In 2005, Lee DK. (83) found a significant difference between the use of high-dose fluticasone (2,000 μg per day), causing corticotropic inhibition and high-dose ciclesonide (1,600 μg per day) without any reported influence.
Nevertheless, Eid N. in 2002 (84), in an observational study in children treated with fluticasone chronically, found a 43% decrease in morning cortisol for his group “fluticasone high dose” (880 μg per day or more), but also 17% of abnormal plasma cortisol level in the morning for “fluticasone low dose” (176 μg per day).
Brus R. (85), in 1999, demonstrated in a randomised trial that fluticasone is one of the inhaled corticosteroids that statistically generates the most single-dose corticotropic inhibition. In multiple doses and unlike other ICSs, fluticasone has a more marked inhibitory effect. In the same year, Wales D. (86) described a greater inhibitory effect of fluticasone than budesonide and beclomethasone at a bioequivalent dose. Li JT. (87) found similar results in 1999.
In 1997, Donnelly R. (88) reported that fluticasone is 3.1 times stronger than budesonide in reducing the plasma cortisol level after 8 h. In the same year, Clark DJ. (89) found a more marked corticotropic inhibition with the use of fluticasone compared to budesonide in adults. The explanations given would be the longer binding and greater affinity to the fluticasone receptor, greater tissue retention and longer biological half-life.
In 1996, Boorsma M. (90) estimated the corticotropic inhibition ratio “fluticasone/budesonide” at 3.7/1. This ratio rises to 5.2/1 if the single criterion of the plasma cortisol level at 8:00 a.m. is used. This major systemic action of fluticasone was also noted in a double-blind randomised trial by Clark DJ. in 1996.
Ciclesonide: Ciclesonide is one of the most recent inhaled corticosteroids brought to the market.
In 2016, Kowalski ML. (91) described a more pronounced influence of beclomethasone, followed by fluticasone and budesonide. With regard to ciclesonide, he does not describe inhibition of the corticotropic axis with this molecule.
In a literature review, Kramer S. (1992) found more pronounced corticotropic inhibition (decrease in urinary cortisol at 24 h) for budesonide compared to ciclesonide.
In 2010, O’Connor BJ. (93), in a randomised, double-blind trial of 365 patients, showed no corticotropic inhibition with the use of ciclesonide at 320 μg or 640 μg twice daily for 12 weeks. In the same year, Pedersen S. did not report any effect on the corticotropic axis with the use of ciclesonide at 40 μg, 80 μg or 160 μg, in treated children with asthma. Gelfland EW. reached the same conclusions in 2006.
A literature review performed in 2009 by Craig T. (94) found no corticotropic inhibition described with the use of ciclesonide in children and asthmatic adults. The same work in 2006 by Meltzer EO. (95) reached the same conclusions.
In 2009, Pedersen S. (96) found a reduction in cortisoluria with fluticasone in a randomised, double-blind trial in asthmatic children aged 6 to 11 years, which was not found with ciclesonide after 12 weeks of treatment.

Page | 58
In 2008, Bateman ED. (97), in a 6-month randomised double-blind trial in asthmatic patients, did not find any significant change in the baseline plasma cortisol level with the use of ciclesonide 160 μg/d and 320 μg twice daily over this period. Lipworth BJ. in 2005 (77) made the same observations.
At the pharmacokinetic level, Rohatagi S. in 2003 (98) found a dose of 800 μg per day of ciclesonide to be the threshold value.
Mometasone: In 2013, Kosoglou T. (99) found an inhibition of the corticotropic axis with mometasone formoterol
400/10 μg versus placebo, which was not found with mometasone formoterol 200/10 μg.
In 2005, Chrousos GP. (100), in a randomised, double-blind, 14-day controlled trial, found a significant decrease in the plasma cortisol level with mometasone 400 μg per day compared to 200 μg and 100 μg per day.
In 2011, Skoner DP. (101) found no change in the corticotropic axis following chronic (1 year) administration of mometasone 100 μg and 200 μg per day in asthmatic children aged 4 to 9 years. The same author in 2010 found a reduction of the area under the curve of the plasma cortisol level after 12h for a mometasone dose of 400 μg/d.
Betamethasone: In 1996, Hasegawa T. (102) described a threshold dose of beclomethasone ranging between 800 μg and 1200 μg per day. He notes, however, high interindividual variability. In 1995, Doull IJ. (103) described that a dose of beclomethasone of 400 μg per day significantly decreases the plasma cortisol level. In 1992, Katsunuma T. (104) did not describe any corticotropic inhibition (24h cortisoluria, morning plasma cortisol level and ACTH test) with the use of beclomethasone 300 μg per day for 12 weeks in asthmatic children.
Association of inhaled corticosteroids with other molecules:
In 2015, Chen X. (105) found a decrease in the baseline plasma cortisol level in his study of healthy adults who had a daily combination of fluticasone and vilanterol of 100/25 μg for 7 days. It must be noted that the prevalence of this hypocortisolaemia was increased with the dose increase to 200/25 μg. Zhang J., in a trial in subjects with COPD, did not find any significant inhibition of the corticotropic axis.
Oliver A., in a double-blind randomised trial in asthmatic children aged 5 to 11 years in 2014 (67), found no significant difference in the baseline plasma cortisol level between the daily intake of fluticasone 100 μg and the combination of fluticasone and vilanterol 100/25 μg.
In 2010, Berger WE. (106), in a multicentre randomised trial, found no difference in the plasma cortisol level between budesonide alone 200 μg 2 times daily and the combination of budesonide and formoterol 160/4.5 μg 2 times daily.
In 2009, Bousquet J. (109) described a more marked decrease in the plasma cortisol level following the joint administration of beclomethasone 1,000 μg and formoterol 241.4 μg than with the fixed association of the same molecules of beclomethasone 400 μg.

Page | 59
In 2006, Jenkins C. (110), in a double-blind, randomised trial, found no difference in the plasma cortisol level between the group treated with budesonide/formoterol fixed combination 320/9 μg per day and the group treated with the same molecules but used separately.
Concomitant use of medications interacting with hepatic metabolism, on the other hand, can influence the efficacy, but also the inhibitory effect of the corticotropic axis of ICSs. Mahlad-Guri K. in 2011 (107) found this element, with the simultaneous use of a therapeutic dose of Ritonavir and fluticasone (3 Cushing syndromes and corticotropic inhibitions in the 3 patients studied). Other authors found this association (St Germain RM in 2007 (108), Raaska K. in 2002, etc.)
Duration of treatment: Gupta D. in 2000 (111) found a time factor, with corticotropic inhibition noted in 1 patient of 7 treated with beclomethasone 800 μg per day after 6 months, whereas it is not shown in the group treated with 400 μg per day.
Type of inhaler and material: In 2016, Srichana T. (112) did not describe any difference between the taking of budesonide as dry powder and as a pressurised dose. Similarly, Nair A. in 2011 (113) found no difference in the bioavailability and corticotropic inhibition of fluticasone/salmeterol used in the Aerochamber form (Aerochamber Plus®), Volumatic Spacer® or Autohaler®.
In 2002, Goldberg S. (114) described corticotropic inhibition following budesonide 400 μg per day as dry powder, which was not found with the pressurised inhaler system. In the same year, in a randomised double-blind trial, Tukiainen H. (115) found no significant difference in the plasma cortisol level between the use of budesonide 800 μg per day with the EasyHaler® or Turbuhaler® devices in adult asthmatics.
Thorsson L. in 2001 (116) described, in a pharmacodynamic and pharmacokinetic article, a more pronounced corticotropic inhibition with fluticasone in a pressurised flask than in a dry powder device. In 1999, Trescoli C. (117) found greater systemic effects with the use of beclomethasone in the form of a dry powder compared to an inhalation chamber type inhaler device.
In a standard exposed-non-exposed analytical study, Goldberg S. in 1996 found that ICS-induced corticotropic inhibition was more pronounced with the use of pressurised (spray) systems than with inhalation chambers. The same findings were made by Selroos O. in 1991 (119), Farrer M. in 1990 and Brown PH. in 1990.
Time of administration and chronotherapy: In 2008, Wu K. (120) found that a morning dose of inhaled corticosteroids would have a more pronounced effect on cortisol than an evening dose. On the other hand, Zetterstrom O. (2008) (121) did not report any differences in corticotropic inhibition between a dose of mometasone furoate dry powder 400 μg in the morning or evening. These findings are found by Weinbrenner A. in 2002 (122), with no difference in the plasma cortisol level among users of ciclesonide 800 μg in the morning or evening or 2 times 400 μg. In a trial in 2001, Postma DS. (123) did not find any change in the plasma cortisol level by taking ciclesonide 200 μg in the morning or evening.
Other factors:
As expected, a large individual variability independent of the preceding factors is present and influences
the response of the corticotropic axis to the administration of ICSs.

Page | 60
In 2012, Tsartsali L. (124) noticed genetic changes that led to variable reactions of the corticotropic axis: the polymorphism of the single nucleotides named rs1876828 and rs242941. Their presence in the homozygous state showed a more marked inhibition of the corticotropic axis in asthmatic patients treated with ICSs. This finding may explain the interindividual variability in response to ICSs.
In 2010, Schwindt CD. (125) was concerned with the effect of inhaled fluticasone intake and physical activity. In this study of 11 healthy men between the ages of 18 and 30 years, using fluticasone (440 μg/d) for 2 weeks, followed by exertion on a bicycle, a reduction was described in the plasma cortisol level and the corticotropic response to exertion.
At the pathological level, Daley-Yates PT. in 2000 (126), in a literature review of pharmacokinetics, described more pronounced corticotropic inhibition following fluticasone in healthy subjects than in asthmatics. He gave the hypothesis of bronchoconstriction which impedes the flow of inspiratory air in pathological subjects. Brutsche MH. confirmed this data in 2000 (127), concluding that there was a more marked systemic change in the use of ICSs in healthy subjects than in pathological subjects.
With regard to the repetition of daily doses, Thorsson L. in 1997 (128) found a more marked corticotropic inhibition after repetition of fluticasone in healthy subjects. He issued the aetiological hypothesis of a longer pulmonary half-life and therefore an accumulation with increased systemic passage. Lonnebo A. in 1996 (129) made the same observation with cumulative doses in healthy volunteers.
Conclusion: The risk of hypocrotisolaemia is proportional to the dose used, the duration and also dependent on medication interactions with cytochrome P450-inhibiting substances such as Ritonavir or itraconazole.
At bioequivalent doses, fluticasone appears to be the most inhibitory ICS on the corticotropic axis and ciclesonide is the least inhibitory. The use of a chamber inhalation system seems to limit this inhibition, unlike pressurised systems. The conventional association with long-acting bronchodilators does not seem to affect the corticosteroid inhibitory effect of ICSs. The presence of an inflammatory pulmonary pathology such as asthma seems to decrease the systemic passage in relation to healthy subjects.
b. Intramuscular, intradermal and subcutaneous
The use of these routes of administration is more rare (specialised indications). The intradermal route has been used principally in dermatology since the 1960s. Unfortunately, these routes of administration, in particular subcutaneous, are also used currently for doping purposes in microdoses.
Research:
MeSH: Intramuscular corticosteroids, Intradermal corticosteroids, Subcutaneous corticosteroids, Adrenal axis Search engines: PubMed, Google Scholar, Cochrane, Med Line Initial number of publications: 611 Number of publications used: 7

Page | 61
Year Authors Goals Publication type Standard of proof Influence
2013 Reddy S Corticotropic axis and triamcinolone IM Observational study C yes
2010 Finken J Adrenal insufficiency triamcinolone Case report C yes
2004 Kumar S Cushing syndrome following intradermal CTC Case report C possible
1974 Michael T Intradermal CTC effects on corticotropic axis Observational study C yes
1973 Wachs GN Intradermal effects on the plasma cortisol level Article C yes
1971 Potter RA Intralesional triamcinolone and corticotropic axis Article C yes
1975 Carson TE Long-term administration triamcinolone IM Observational study C yes
Table 7 - List of publications used regarding the influence of intramuscular, intradermal and subcutaneous corticosteroids on the
plasma cortisol level
Results:
There are few publications on the subject. There were 2 reported cases and 3 observational trials on small numbers of subjects. The overall level of proof of the trials used is low (grade C for 100% of the publications used, i.e. 7 out of 7). Almost all of these trials reported significant corticotropic inhibition. 6 publications out of 7 or 85.7%.
With regard to intramuscular injections, Reddy S. in 2013 (130) found marked corticotropic inhibition at 6 and 12 weeks following the injection of triamcinolone as IM in 14 patients having received 2 injections at intervals of 6 and 12 weeks. In 1975, Carson TE. (131) recorded corticotropic inhibition following the chronic administration (5 months to 3 years) of triamcinolone IM in 5 patients throughout the duration of administration and for up to 10 months.
With regard to intradermal injections, in 1974, Michael T. found a more marked corticotropic inhibition with intradermal betamethasone compared to triamcinolone acetonide and diacetate at a bioequivalent dose. In 1973, Wachs GN. (132) made the same observation in his publication, with a more marked inhibitory effect of betamethasone relative to triamcinolone. In 1971, Potter RA. (133) found an inhibition with intralesional triamcinolone used for inflammatory dermal cysts. He described a link with the number of injections and the injected dose.
Conclusion: Regardless of the dose, molecule or route (intramuscular, intradermal or subcutaneous), hypocortisolaemia appears to be systematic in the low number of publications used. There is a progressive dose effect and probably a biological half-life effect.
c. Periarticular and intraarticular
Osteoarticular infiltrations of glucocorticoids are commonly used in orthopaedics, traumatology and sports medicine. Originally described from the 1950s onwards for osteoarthritis of the knee, their use has developed. The infiltrations can be performed in an articular cavity, in which case they are called “intraarticular”. They can be performed in spaces around the joint or a myotendinous or nervous structure, in a bursa, in a sheath, etc. They will then be called “articular PERKs”.
The principal molecules used are classified according to their anti-inflammatory power (evaluated as anti-inflammatory equivalence compared to 5 mg of prednisone) and biological half-life (hence their duration of action).

Page | 62
The different molecules currently marketed and used in France are summarised in the following table:
DCI Non-commercial Presentation
Prednisone equivalent
per vial (mg)
Indications
Art
icu
lar
Per
iart
icu
lar
Epid
ura
l
Hydrocortisone acetate Hydrocortisone 1 ml = 25 mg 5 ml = 125 mg
6.25 31
Yes Yes Yes
Prednisone acetate Hydrocortancyl 1 ml = 25 mg 5 ml = 125 mg
25 125
Yes Yes Yes
Betamethasone (F) Diprostene Celestene chronodose
1 ml = 2 mg 1 ml = 6 mg
45 50
Yes Yes No
Cortivazol Altim 1.5 ml = 3.75 mg 75 Yes Yes Yes
Methylprednisolone acetate Depo-Medrol 2 ml = 40 mg 2 ml = 80 mg
50 100
Yes Yes Yes
Paramethasone acetate Dilar 2 ml = 40 mg 100 Yes Yes No
Dexamethasone acetate (F) Dectancyl 1 ml = 5 mg 3 ml = 15 mg
33 100
Yes Yes Yes
Triamcinolone (F) Hexatrione Kenacort
2 ml = 40 mg 1 ml = 40 mg 2 ml = 80 mg
50 50
100
Yes No No Yes
(F): fluorinated derivative
Table 8 - Epidural, intra- and periarticular corticosteroids (134).
Pharmacokinetics: The intraarticular injection of glucocorticoids induces local anti-inflammatory action at the synovial membrane with increased intraarticular viscosity and hyaluronic acid concentration (Jesser, 1953). In 1970, Dick described a decrease in synovial hyperaemia following intraarticular glucocorticoid injection in the case of synovitis. Other authors have described different local changes (decrease of pro-inflammatory cytokines, certain proteins, leucocytes, etc.).
The action of glucocorticoids is principally in synovial tissue (synoviocytes and pericellular spaces) and the diffusion gradient induces plasma passage.
The local theoretical anti-inflammatory action depends on the concentration, the anti-inflammatory power and the solubility of the product used. The addition of fluorine increases this activity.
Research:
MeSH: Intra-articular corticosteroids, Periarticular corticosteroids, adrenal axis, cortisol Search engines: PubMed, Google Scholar, Cochrane, Med Line Initial number of publications: 413 Number of publications used: 9

Page | 63
Year Authors Goals Publication type Standard of proof Influence
2009 Habib GS Literature review of systemic effects intra infiltrations Literature review B yes
2007 Duclos M Risk of intra- or periarticular adrenal insufficiency Analytical study B yes
2006 Younes M Systemic effects injected corticosteroids Observational study B yes
2005 Mader R Effect articular injection methylprednisolone Trial B yes
2000 Wicki J Acute adrenal insufficiency following articular CTC Case report C yes
1999 Creamer P comparison 3 injectable corticosteroids in PR Observational study C yes
1997 Huppertz HI Corticotropic axis and articular injection CTC children Observational study B yes
1981 Gless KH systemic effect betamethasone intra-articular Observational study B yes
1980 Weiss S Systemic effects articular triamcinolone Observational study C no
Table 9 - List of publications used regarding the influence of intra and periarticular corticosteroids on the plasma cortisol level
Results:
8 of the 9 publications used (88%) show a significant influence of intra-articular or periarticular CTCs on the corticotropic axis.
Figure 16 - Results of publications used on the detection of hypocortisolaemia following the infiltration of corticosteroids (yes:
hypocortisolaemia found, no: hypocortisolaemia not found; variable: non-discriminating results)
In 2007, Duclos M. (1) described in his publication a marked corticotropic inhibition at D2, D7 and D14 following single intravenous or periarticular infiltration of 10 athletes with Cortivazol or betamethasone. Younes M. in 2006 (135) published hypocortisolaemia of D1 to D7 following 3 intra-articular infiltrations in 29 patients. The plasma cortisol level was found to be normal at D21.
In 2005, Mader R. (136) described hypocortisolaemia following an intra-articular injection of methylprednisolone in 48% of patients (12 patients out of 25) 1 day after injection, in 4% after one week and in 4% after 2 weeks.
In the same way, Huppertz HI in 1997 (137) described a transient corticotropic insufficiency between 10 and 30 days in 14 of the 22 patients, following an intra-articular injection of glucocorticoids in children and adolescents with chronic arthritis.
yes
no

Page | 64
In 1981, Gless KH. (138) made the same observation with regard to the plasma concentration and systemic effects of intra-articular betamethasone. He reported an increase in the plasma concentrations of betamethasone 30 min after a subsequently degressive injection and a decrease in the plasma cortisol level between 6 and 24h post-injection for a return to the usual values after 4 days. These changes were more pronounced in subjects with articular effusion.
A literature review performed in 2009 by Habib GS. (139) found that plasma cortisol level decreased to a nadir around 24-48h after intra-articular infiltration of corticosteroids, with recovery in 1 to 4 weeks. This variability takes into account the number of injections, the half-life and the concentration of the corticosteroid used.
Wicki J. in 2000 (140) published a case of a patient with acute adrenal insufficiency following a single intra-articular injection of glucocorticoids.
The only publication used that did not find hypocortisolaemia following infiltration is Weiss S. dating from 1980 (141), who did not find hypocortisolaemia following intra-articular administration of triamcinolone in 10 patients with rheumatoid arthritis.
Conclusion: Compared to inhaled corticosteroids, the number of publications concerned with the influence of intra- or periarticular glucocorticoids is low and so is their level of proof. In addition to this concept, it appears that a large part of these trials relate only to intra-articular infiltrations in the knees and very few relate to other locations.
Nevertheless, the publications used on this subject seems to agree that a single intra-articular infiltration of glucocorticoids can lead to transient hypocortisolaemia that is usually regressive in a few days to a few weeks. In the publications used, this time period is at least 4 days and on average 8 days.
As with other routes of administration, the factors influencing the depth of inhibition of the corticotropic axis, as well as the recovery time, are:
the number of infiltrations, the type of molecule used and its biological half-life, its concentration, the presence of joint inflammation.
It is also reported that a small percentage of patients retain marked inhibition of their corticotropic axis during a longer or shorter period.
d. Dermocorticoids
Since the topical use of hydrocortisone in the 1950s, dermocorticoids have changed the therapeutic management of many dermatological diseases. Currently, there are more than 20 different molecules, sold alone or in combination in over a hundred specialities and classified according to their anti-inflammatory activity.
The following are described: Level IV: very strong anti-inflammatory activity, Level III: strong anti-inflammatory activity, Level II: moderate anti-inflammatory activity, Level I: low anti-inflammatory activity.
Dermocorticoids are usually prescribed in the context of general medicine. Their use is not prohibited by anti-doping agencies.

Page | 65
Activity
Anti-inflammatory
Common name
International
Speciality name Galenic forms Concentration
%
Very strong Clobetasol propionate Dermoval Cream, capillary gel 0.05
Betamethasone
dipropionate
Diprolene Cream, pomade 0.05
Strong Betamethasone valerate Betneval
Betneval lotion
Cream, pomade
Emulsion
0.10
Betamethasone valerate Celestoderm Cream 0.10
Betamethasone
dipropionate
Diprosone Cream, pomade, lotion 0.05
Hydrocortisone aceponate Efficort Hydrophilic cream
Lipophilic cream
0.127
Difluprednate Epitopic 0.05% Cream, gel 0.05
Fluticasone Flixovat Cream
Pomade
0.05
0.005
Desonide Locatop Cream 0.10
Hydrocortisone butyrate Locoid Cream, thick cream, fluid
emulsion, lotion, pomade
0.10
Diflucortolone valerate Nerisone
Nerisone Gras
Cream, pomade
Anhydrous pomade
0.10
Moderate Betamethasone valerate Celestoderm Cream 0.05
Difluprednate Epitopic 0.02% Cream 0.02
Desonide Locapred Cream 0.10
Fluocinolone acetonide Synalar The solution 0.01
Desonide Tridesonit Cream 0.05
Fluocortolone
base+caproate
Ultralan Pomade 0.50
Low Hydrocortisone Aphilan itching Cream 0.50
Hydrocortisone Biacort Cream 0.50
Hydrocortisone Hydracort cream Cream 0.50
Hydrocortisone Dermaspraid itching Cream The solution
0.50
Hydrocortisone Mitocortyl
itching
Cream 0.50
Hydrocortisone Hydrocortisone
Kerapharm
Cream 1
Table 10 - List of dermocorticoids from the National College of Medical Pharmacology (142).
Their indications are multiple: - Inflammatory dermatoses, - Dysimmune dermatoses, - Some tumour lesions. Pharmacokinetics: Cutaneous absorption and systemic passage therefore require crossing the epidermis, dermis and hypodermis. The ratio of dermal absorption of the different topicals is very low in medicine. For dermocorticoids, it is evaluated at 2%.
Skin absorption and penetration are influenced by: - Biochemical characteristics of the molecule and excipients and additives (liposolubility, keratolytics) - Cutaneous permeability (age, skin pathology, cutaneous reservoir effect, etc.), - Skin hydration, - Skin hyperaemia, - Occlusion (by increase in hydration, temperature and duration of contact), - Location (significant skin thickness on the sole and palms and low at the eyelids, forehead and scrotum),
- Application surface, - Quantity and frequency of application.

Page | 66
Research:
MeSH: Topical corticosteroids, Adrenal axis Search engines: PubMed, Google Scholar, Med Line Initial number of publications: 183 Number of publications used: 23
Year Authors Goals Publication type Standard of proof Influence
2014 Bockle BC DermoCTC misuse and adrenal insufficiency Case report C yes
2014 Levin E DermoCTC and adrenal insufficiency Literature review B no
2013 Silver S Calcipotriene + betamethasone and cortico axis Observational study C no
2012 Castela E DermoCTC literature review and corticotropic axis Literature review B yes
2012 Campbell LS Case of adrenal insufficiency in dermoCTC Case report C yes
2011 Kerner M Evaluation of corticotropic axis after dermoCTC Observational study C yes
2011 Nutan DermoCTC and atopic dermatitis Trial C yes
2010 Pileggi FO Clobetasone 0.05% for phimosis and axis Observational study C no
2007 Eichenfield LF Desonide 0.05% and corticotropic axis Observational study C no
2006 Hebert AA Fluticasone lotion and atopic dermatitis Observational study C no
2003 Sobngwi E Betamethasone 0.05% and cortico insufficiency Case report C yes
2000 Ellison JA Cortico axis and atopic dermatitis Observational study C variable
1999 Gilbertson EO Adrenal insufficiency following dermoCTC Case report C yes
1997 Lucky AW Desonide 0.05% Hydro 2.5% and cortico axis Observational study C no
1988 Neumann RA Effects of dermoCTC on endogenous cortisol Trial B yes
1987 Ohman EM Low-dose clobetasol and corticotropic insufficiency Case report C yes
1987 Katz HI DermoCTC level IV and corticotropic insufficiency Trial B yes
1985 Thornfeldt C Alclometasone 0.05% and corticotropic axis in healthy subjects
Observational study C yes
1983 Salde L Systemic effects of 3 dermoCTCs on corticotropic axis
Trial B yes
1982 Herz G Hydrocortisone and corticotropic axis in children Observational study C no
1981 Cornell RC Desoxi and chronic betamethasone and axis Observational study C yes
1980 Marten RH Hydrocortisone and corticotropic axis in children Observational study C no
1976 Munro DD Intensive dermoCTC and corticotropic insufficiency Observational study C yes Table 11 - List of publications used regarding the influence of dermocorticoids on the plasma cortisol level
Results:
With regard to the repercussions on the plasma cortisol level, numerous publications have been released, in particular for atopic dermatitis, which show variable results. The explanation may come from the different methodologies of these publications.
14 publications of the 23 used found corticotropic inhibition (60.8%). For the 3 trials used with the highest level of proof (grade B), this rate rises to 3 out of 3 (100%). These 3 publications relate to the use of level III or IV dermocorticoids.

Page | 67
Figure 17 - Results of publications used on the detection of hypocortisolaemia following the use of dermocorticoids (yes: hypocortisolaemia found, no: hypocortisolaemia not found; variable: non-discriminating
results)
As expected, an influence of dose, duration, application location, occlusion and anti-inflammatory level of dermocorticoids on the occurrence of adverse effects, in particular local effects, is described.
In 2014, Bockle BC. (143) published two cases of adrenal insufficiency and cushingoid clinical syndromes following dermocorticoid misuse (chronic use and frequency of supratherapeutic application).
A literature review by Levin E. in 2014 (144) showed no pathological inhibition of the corticotropic axis in 15 out of 16 publications. The latter study was a supratherapeutic use (2 times the dose of clobetasol for 18 months), with the conclusion that the use of dermocorticoids is not associated with an inhibition of the corticotropic axis at the therapeutic dose.
In 1998, Gilbertson EO. (145) made a similar finding, by publishing 2 cases of severe adrenal insufficiency linked to misuse of dermocorticoids with a high level of anti-inflammatory activity.
In 2013, Silver S. (146) published on the influence of the treatment of psoriasis vulgaris (calcipotriol+betamethasone) for 8 weeks. He described 2 cases of adrenal insufficiency (hypocortisolaemia and ACTH test in favour) in 43 patients, linked to the use on a large cutaneous surface.
In a literature review from 1980 to 2011 in patients with psoriasis, Castela E. in 2012 (147) found that, in the 22 randomised trials used, a transient hypocortisolaemia was noted at the start of treatment in 0 to 25% of cases in 10 publications and up to 48% in other publications. Only 4 showed no influence on the corticotropic axis in chronic use (exceeding 6 months).
Campbell LS. in 2012 (148) reported corticotropic insufficiency following the use of a so-called moderate power dermocorticoid in a patient with exfoliative erythrodermal psoriasis. The hypothesis advanced is the important change of the function of the skin barrier in this pathology, with increased systemic passage.
yes
variable
no

Page | 68
Kerner M. in 2011 (149), in an observational study, made similar observations. The publication included 27 patients using different dermocorticoids once daily for 2 weeks on a skin surface area of at least 10% of the total body surface area. 38% of the patients had adrenal insufficiency. A more advanced age was described in these subjects, a larger area of application as well as the use of dermocorticoids with more marked anti-inflammatory activity.
In 2000, Ellison JA. (150), in his publication on 35 adolescents with atopic dermatitis, described the absence of adrenal insufficiency in those treated with a low to moderate activity dermocorticoid. On the other hand, he observed a temporary inhibition of the corticotropic axis in the use of dermocorticoids with high activity or associated with corticosteroid therapy per os.
In 1998, in a randomised double-blind trial comparing 3 groups of 7 subjects treated for 8 days with different dermocorticoids, Neumann RA. (151) noted no effect on the corticotropic axis in 2 groups treated with dermocorticoids of weak and moderate anti-inflammatory activity and a non-reversible inhibition after 4 days in the last group treated with the dermocorticoid with the strongest anti-inflammatory activity. In the same year, Katz HI. (152), in a randomised double-blind trial in 40 patients, found a temporary inhibition of the corticotropic axis in 8 patients treated with high activity dermocorticoids.
Ohman EM, in 1987 (153), found 3 cases of prolonged adrenal insufficiency following the use of clobetasol at the conventional therapeutic dose in the long term.
In 1981, Cornell RC. (154) found 9 decreases in the plasma cortisol level following a chronic treatment (6 months) with desoximetasone, of which 4 were transient and regressive despite the continuation of treatment, 4 were regressive following the cessation of therapy in 7 days and 1 was persistent.
On the other hand, other highly targeted publications, with short exposure times a low number of subjects, using conventional therapeutic doses, and studying a single molecule and a precise concentration, showed no influence on the corticotropic axis. (Silver S. in 2013 (146), Pileggi FO. in 2010, Eichenfield LF. in 2007, Hebert AA. in 2006, Lucky AW. in 1997, Herz G. in 1982, Marten RH. in 1980)
In 1985, Thornfledt C. (155) found no adrenal insufficiency following the application of 0.05% alclometasone on 80% body surface area per day in healthy subjects with occlusion for 21 days.
Conclusions:
The current and existing literature shows variable results with regard to the influence of dermocorticoids on the plasma cortisol level. This variability can be explained by the heterogeneity of the publications, the subjects studied, the pathologies, the molecules used and the doses.
In some publications, an initial, asymptomatic, regressive hypocortisolaemia is described despite the continuation of the treatment. (This may be due to a restoration of the skin barrier, with consequent limitation of absorption.)
Overall, the long-term use of dermocorticoids on pathological skin, on a large skin area, at a supratherapeutic dose with a high level (IV) and in very young or elderly subjects, appears to increase the risk of hypocortisolaemia. This data is frequently reported in children, but is more controversial in adults.

Page | 69
e. Intranasal corticosteroids (INCs)
The aim of intranasal corticosteroid administration is to achieve a local action by minimising the adverse systemic effects. INCs have been widely used in first-line medicine for many years, in particular in allergic rhinitis.
There are many molecules currently available: Beclometasone (BECLO-RHINO®, BECONASE®, RHINIRE®), Fluticasone (FLIXONASE®, AVAMYS®), Budesonide (RHINOCORT®), Flunisolide (NASALIDE®), Mometasone (NASONEX®), Tixocortol (PIVALONE®), Triamcinolone (NASACORT®).
They are sometimes administered in association with: A vasoconstrictor: Naphazoline+prednisolone (DERINOX®), oxymetazoline+prednisolone
(DETURGYLONE®).
The recognised indications are: Acute allergic rhinitis, acute allergic rhinoconjunctivitis, Chronic inflammatory and allergic rhinitis, Common infectious rhinitis of viral origin, Nasal or nasosinusal polyposis.
Pharmacokinetics:
The systemic bioavailability of INCs varies according to: The dose, The technique and material, The molecule, The duration of use, Age, Probably, the degree of nasal obstruction.
Research:
MeSH: Nasal Spray, Adrenal axis, Cortisol Search engines: PubMed, Google Scholar, Med Line Initial number of publications: 105 Number of publications used: 16
Year Authors Goals Publication type Standard of proof Influence
2015 Martino B J Effect of Dexa spray on the plasma cortisol level and ocular pressure
Observational study C Yes
2014 Georges G Triamcinolone effect on corticotropic axis Randomised trial B Yes
2012 Liang J Nasal prednisolone and corticotropic axis Analytical study C No
2009 Bruni FM Literature review - Intranasal CTC and cortico function Literature review C Variable
2009 Tripathy I Nasal fluticasone and corticotropic axis Observational study C No
2008 Patel D Nasal fluticasone and corticotropic axis Randomised trial B No
2005 Licata AA 2 cases systemic effects nasal CTC Case report C Yes
2004 Kim KT Budesonide spray and corticotropic axis Randomised trial B No
2004 Hermann R Pharmacokinetics Loteprednol and fluticasone Randomised trial B No
2004 Bachert C Nasal fluticasone and triamcinolone and dynamic test Randomised trial B No
2003 Galant SP Nasal fluticasone and corticotropic axis Observational study C No
2001 Dibildox J Safety and efficacy intranasal mometasone Randomised trial B No

Page | 70
1998 Vargas R Nasal fluticasone and corticotropic axis Randomised trial B No
1998 Nayak AS Triamcinolone effect on corticotropic axis Randomised trial B No
1995 Brannan MD Beclomethasone low strong dose and corticotropic axis
Randomised trial B No
1994 Sastre J Adrenal insufficiency and nasal Dexa abuse Case report C Yes
Table 12 - List of publications used regarding the influence of intranasal corticosteroids on the plasma cortisol level
Results:
As shown in Figure 8, the majority of the publications used (50%) used fluticasone as a molecule or a combination of fluticasone with another intranasal corticosteroid.
Figure 8 - prevalence of intranasal corticosteroids (%) used in publications used.
11 out of 16 publications (68.75%) did not find a significant relationship between the use of CTC-based nasal spray and hypocortisolaemia (Figure 18).
Figure 18 - Results of publications used on the detection of hypocortisolaemia following the use of intranasal corticosteroids (yes: hypocortisolaemia found, no: hypocortisolaemia not found; variable: non-discriminating
results)
no
variable
yes

Page | 71
In 2015, Martino BJ. (156) published an article on the influence of intranasal dexamethasone 0.132% on the plasma cortisol level. The 28 patients included were treated chronically (mean 38.3 weeks) for clinical pictures of chronic rhinitis with nasal polyposis. He described hypocortisolaemia in 10 patients.
In a prospective, double-blind study in 2014, George G. described a significant difference in the plasma cortisol level between the use of intranasal triamcinolone and a placebo.
In 2005, Licata (157) reported a case of acute adrenal insufficiency following the administration of intranasal fluticasone. Similarly, in 1994, Sastre J. (158) described a case of adrenal insufficiency following misuse (for 2 years) of dexamethasone in a 55-year-old woman. Note that this patient had a cushingoid clinical syndrome.
A literature review performed in 2009 by Bruni FM. (159) found variable results. He found one publication with an inhibition of the corticotropic axis by budesonide and intranasal fluticasone and one publication with beclomethasone in healthy subjects. On the other hand, he found other publications without significant influence with mometasone, budesonide and fluticasone in children and adults.
In 2009, Tripathy I. (160) did not describe the influence of fluticasone 110 μg once daily on the plasma cortisol level in a population of children aged 2 to 11 with perennial allergic rhinitis.
In a double-blind randomised trial with a higher level of proof, Patel D. in 2008 (161) made the same observations for fluticasone at therapeutic doses in patients aged 12 to 65 versus placebo.
In 2004, Kim KT. (162) did not find hypocortisolaemia after 6 weeks of intranasal budesonide treatment in children aged 2 to 5 with allergic rhinitis. In the same year, Hermann R. (163), in a double-blind, randomised trial comparing fluticasone, Loteprednol at 2 different concentrations and placebo found no changes in blood cortisol after 14 days of treatment. The same observations were made by Bachert C. (164) who tested the corticotropic axis by dynamic ACTH stimulation test following fluticasone and triamcinolone in a nasal spray.
Many other authors did not find hypocortisolaemia following an acute intake of intranasal corticosteroids (Vargas R. in 1998, Nayak AS, etc.).
In 1995, Brannan MD. (165) compared the use of beclomethasone at 336μg and 168μg versus placebo in 64 subjects during 36 days of treatment and did not report hypocortisolaemia for these two doses.
Conclusion:
Despite some recent publications which describe an influence of intranasal corticosteroids on the corticotropic axis, the literature on the subject is more measured. Indeed, there is a significant number of publications (10 out of 16) that find against the existence of hypocortisolaemia at therapeutic doses. Most authors agree on the therapeutic safety of the use of these molecules at therapeutic doses. Hypocortisolaemia is related to misuse in the publications used.

Page | 72
f. Ophthalmic corticosteroids: Eyedrops
From the start of the 1950s, hydrocortisone preparations have been used as eyedrops. There are many presentations of treatments based on corticosteroids administered ophthalmically (solutions, gels, suspensions, etc.) It should be noted that the suspension form requires a preliminary phase of agitation of the product. Nourry H. has shown that this form of administration does not guarantee a homogeneous concentration of glucocorticoids.
We have deliberately not discussed other ophthalmological modes of administration (intraocular, periocular, etc.). Their use is limited to specific indications.
The principal molecules used are: Hydrocortisone, Prednisolone, Dexamethasone, Fluorometholone, Rimexolone, Loteprednol, Medrysone.
These different molecules are distinguished by: Their variable anti-inflammatory action, Their different intracorneal penetration, Their effect on intraocular tension.
The principal indications are: Uveitis, Scleritis and episcleritis, Allergic conjunctivitis, Non-infectious keratitis, Post-operative inflammation.
The principal side-effects are local. The systemic penetration via this path depends on: The concentration of the glucocorticoid, The molecule, The excipients.
As the preparations are very diverse, a great variability in the intraocular passage of corticosteroids has been described. (McGhee CN, 2002 (166))
Research:
MeSH: Cortisol, Drop Eye, HPA, adrenal insufficiency, Cortisol Search engines: PubMed, Google Scholar, Med Line Number of initial publications: 13 Number of publications used: 5
Year Authors Goals Publication type Standard of proof Influence
2012 Sandhu SS Corticotropic insufficiency CTC eyedrops post operative
Observational study C No
2003 Afandi B Cushing syndrome induced CTC eyedrops Case C Yes
1996 Ruters S Plasma cortisol level after dexa eyedrops Observational study C Yes
1983 Baba S Hydro concentration - efficiency and AEs (short duration)
Observational study C No
1976 Krupin T Influence dexa eye on the plasma cortisol level Observational study C Yes Table 13 - List of publications used regarding the influence of intranasal corticosteroids in the form of eyedrops on the plasma cortisol level

Page | 73
Results:
There are very few publications with regard to the influence of ophthalmic corticosteroids on the plasma cortisol level. Their levels of proof are low. 3 out of 6 publications found hypocortisolaemia following the use of corticosteroid-based eyedrops (60%). These are published case reports or observational trials on very low numbers of subjects (<10 patients).
Figure 19 - Results of publications used on the detection of hypocortisolaemia following the use of corticosteroid eyedrops
(yes: hypocortisolaemia found, no: hypocortisolaemia not found; variable: non-discriminating results)
In 1976, Krupin T. (167) described hypocortisolaemia in 50 patients prospectively treated with 1 drop of 0.1% dexamethasone eyedrops in each eye 4 times a day for 6 weeks. He also noted reversibility in the ACTH test and concluded at that time that there was a significant systemic passage with partial iatrogenic adrenal insufficiency.
In a short course, Baba S. in 1983 (168) noted the absence of a change in the plasma cortisol level in his publication, which consisted of comparing the efficacy and the repercussions on the plasma cortisol level of different concentrations of betamethasone eyedrops.
In 1996, Ruters S. also described a biological inhibition of the corticotropic axis (decrease in the plasma cortisol level, salivary and urinary cortisol) following the administration of dexamethasone 0.1% in eyedrops every hour in the post-operative period (cataract by phakoemulsification) in all 13 patients in his sample.
In 2003, Afandi B. (169) reported a case of clinical Cushing’s syndrome induced in a patient on long-term treatment. Hypocortisolaemia as well as weak ACTH have been described.
More recently, in 2012, Sandhu SS. (170) studied the reactivity of the corticotropic axis to dynamic tests in patients treated with a post-keratoplasty topical glucocorticoid. Of the 20 patients included, with a mean treatment of 28.2 months and without other adrenal disease or glucocorticoid intake, the cortisol values were within normal values and the tests did not reveal any adrenal insufficiency in almost all subjects (except for 1). The authors concluded on the absence of significant systemic effects on the adrenal axis of the local topicals in their study.
yes
no

Page | 74
Conclusion:
Given the small number of publications on this subject, it is complicated to conclude in favour of a major systemic effect. Moreover, the methodology of these publications and their level of proof do not allow a significant causal link to be established. Despite this, the chronic use and the increased dose appear to increase systemic passage and the risk of hypocortisolaemia.
In common use at therapeutic doses and over a short period of time, corticosteroid-based eyedrops do not appear to cause hypocortisolaemia.
4- Conclusion and Discussion
At the end of this literature review, there are certain individualised recurring factors of glucocorticoids with significant influence on the plasma cortisol level, which may be predictive:
The type of glucocorticoid, the molecule and its anti-inflammatory activity, Systemic use (per os, IV), The supratherapeutic dose, The long duration of treatment, The cumulative dose, The existence and intensity of the underlying pathology and hence the indication, The presence of a clinical cushingoid syndrome.
ICSs significantly inhibit the corticotropic axis at high doses. At a bioequivalent dose, fluticasone appears to be more inhibitory than ciclesonide. Intramuscular, intradermal or subcutaneous use has a significant systemic action, with transient systemic hypocortisolaemia. The periarticular and intra-articular pathways, whatever the molecule used and its half-life, also significantly inhibit the corticotropic axis, often transiently.
With regard to the use of glucocorticoids by the nasal or ocular routes, apart from rare cases of abusive supratherapeutic uses, hypocortisolaemia is not described.
In the case of dermocorticoids, their chronic use on pathological skin, on a large skin area, at a supratherapeutic dose with a high level (IV) and in very young or elderly subjects, seem to constitute factors that increase the risk of hypocortisolaemia. For the rest, the data is heterogeneous, and does not allow the elimination of the doubt on their total safety with respect to the corticotropic axis.
“Close monitoring, patient education, vigilance with regard to the factors influencing the corticotropic axis, the recognition of patients at risk, the use of the minimum effective dose and the constant questioning of this dose make it possible to reduce the risks of iatrogenic adrenal insufficiency. ” (Ahmet A, 2011).

Page | 75
PART 3: OBSERVATIONAL STUDY Hypocortisolaemias screened in the context of biological
surveillance implemented by the French Cycling Federation and the prevalence of corticosteroid intake
1— Introduction
The MPCC is a movement based on the voluntary work of French and foreign professional cycling teams. This organisation is an association whose goal is to support “clean cycling”, focusing on the concepts of transparency, responsibility and mobilisation of the different actors involved.
In 2016, the MPCC comprised 38% of the World Tour teams, 73% of the pro continental teams, 11% of continental teams and 17% of women’s teams (171).
The MPCC is a major player in the field of the correct use of corticosteroids in cyclists, with numerous internal recommendations based on expert advice (Annex 7). Among the medical actions performed by the MPCC, there is the unexpected determination of the plasma cortisol level during the competitions. The ultimate goal is to protect the health of these athletes in the context of the rider’s health surveillance and prevention.
The subject of hypocortisolaemia is an important area of work and research in the MPCC for the reasons given in the preceding chapters: the potentially doping effect of these molecules, but principally and in particular due to the risk of secondary adrenal insufficiency and its consequences in the case of sports practice.
In addition to the national (AFLD) and international (WADA and UCI) bodies, the MPCC has launched its regular follow-up in 2009, of which the determination of cortisol forms part.
Without entering into the technical provisions (Annex 5), this sampling is performed unexpectedly by approved laboratories, and the results are transmitted to the physician of the MPCC who informs the physician of the team. A pre-analytical self-questionnaire is regularly filled out by the riders during the season (to facilitate interpretation and in particular the possibility of jet lag) (Annex 6).
In practice, in the presence of a plasma cortisol level below the lower limit, a contraindication to the practice of cycling is pronounced with immediate effect. Just as an occupational physician can advise the employer, the physician referring to the MPCC warns the employer of the immediate unfitness of its rider without further details. The rider is only allowed to take part in a later race in the event of the normalisation of the plasma cortisol level (Annex 5).
The purpose of this section is to illustrate the entire hypocortisolaemia problem described in our work, through the collection of observational prevalence data on the use of corticosteroids in cyclists with hypocortisolaemia.

Page | 76
2 — Materials and methods
To do this, we collected data from the FFC biological monitoring questionnaires for professional cyclists screened for hypocortisolaemia in the context of the MPCC for the years 2015 and 2016.
The biological data transmitted by the FFC in this period was thoroughly examined. Hypocortisolaemia was defined as a plasma cortisol level lower than the low value of the laboratory that performed the sampling.
As shown in Annex 6, self-questionnaires are completed by athletes themselves, without the need to mention the molecule, trade name or dose. Only hypocortisolaemic athletes’ self-questionnaires were examined.
The cyclists were screened in the events of the following years 2015 and 2016: Paris Nice®, Circuit de la Sarthe®, Les 4 jours de Dunkerque®, Le Dauphine libere®, Le Tour de France®, L'Eneco Tour®.
We have included data from the 2015 and 2016 French Championships.
3 — Results
From 2009 to 2015, 774 samples were taken by the MPCC, out of 80 teams and 239 riders. (171)
Firstly, among the 590 pre-analytic self-questionnaires available for the year 2015, a non-negligible part found the mention of corticosteroid use, principally by inhalation (5.25%) and the nasal route (1.8%) (Table 14). Obviously, the use of an oestro-progestative or progestative contraceptive is the principal therapy in women. The use of dietary supplements (spirulina 1.6%), iron (3.22%), magnesium (2.71%) and multivitamin medications (2.37%) is significant.
Molecule Number (n=) Percentage (%)
Corticosteroids
General route 6 1.02
Inhaled 31 5.25
Dermocorticoids 6 1.02
Nasal spray 11 1.86
Infiltration 1 0.17
Eyewash 1 0.17
Antihistaminic HI. 9 1.53
Oestrogen-progesterone 36 6.10

Page | 77
Molecule Number (n=) Percentage (%)
Analgesics
Paracetamol 10 1.69
Tramadol 3 0.51
Morphine 1 0.17
NSAIDs 6 1.02
Vitamins
Vitamin C 11 1.86
Multivitamins 14 2.37
Trace elements
Iron 19 3.22
Magnesium 16 2.71
Infectious diseases medicine
Oral antibiotics 3 0.51
Local antibiotics 2 0.34
Antifungals 1 0.17
Decongestants 1 0.17
Antitussives 1 0.17
Mouthwashes 1 0.17
Vasoconstrictor spray 1 0.17
Digestive system
Antispasmodics 2 0.34
Antidiarrhoeals 1 0.17
Anti-emetics 1 0.17
Probiotics 2 0.34
Laxatives 1 0.17
IPP 1 0.17
Antacids 1 0.17
Nutritional supplements
Spirulina 10 1.69
Antioxidant 1 0.17
Citrulline 2 0.34
Protein - Creatinine 4 0.68
Other 4 0.68

Page | 78
Molecule Number (n=) Percentage (%)
Other
Antimalarial 1 0.17
Levothyroxin 2 0.34
Anticoagulant 1 0.17
Biotherapy 2 0.34
Insulin 2 0.34
Homoeopathy 2 0.34 Table 14 - Prevalence of treatments reported by cyclists in the FFC self-questionnaire for the year 2015.
In 2015, two riders experienced hypocortisolaemia. These two riders were both male road cyclists. The first rider was treated by intra-articular infiltration in the days preceding the sampling. The second did not report taking corticosteroids. On the other hand, a jet-lag explanation was
given with regard to the time of sampling.
In 2016, four riders experienced hypocortisolaemia. These 4 riders were both male road cyclists. The first rider used a fixed combination of inhaled corticosteroid and long-acting beta-2-mimetic
(fluticasone/salmeterol, Seretide®) for asthma, but the dose was not reported. The second used a dermocorticoid whose indication, molecule name and dose were not
reported. The third rider was treated by intra-articular infiltration in the days preceding the sampling. The fourth withdrew from the MPCC and we do not have the self-questionnaire data.
In total, over the years 2015 and 2016, among the 6 riders screened with hypocortisolaemia, we found 4 riders out of 6 being treated or having already been treated with corticosteroids (66.6%).
4 — Conclusion and discussion
This prevalence study suffers from many biases: A sampling bias (professional cyclists monitored in the context of the MPCC only, not
representative of athletes in general),
A recall bias (name of the molecule, dose, duration, etc.), The Hawthorne effect (change of the behaviour of cyclists after knowing that they have been
observed and screened), An indication bias (declarations of athletes voluntarily or involuntarily incomplete),
A data bias (some self-questionnaires not found), A bias due to loss of follow-up (withdrawal of a rider with hypocortisolaemia in 2016 from the
follow-up of the MPCC).
Despite this, this data illustrates the significant prevalence of corticosteroid use among MPCC cyclists. Moreover, the vast majority of cyclists screened with hypocortisolaemia are or have been treated with corticosteroids.
A complementary epidemiological study with all MPCC data since 2009 would increase the power and validity of this study.

Page | 79
GENERAL CONCLUSION, DISCUSSION AND PROSPECTS
Our work, although vast and varied in nature, suffers principally from considerable heterogeneity and variability in view of the great diversity of the publications, their methodology and level of proof. The work of synthesising and interpreting the data is therefore very complicated. Despite this, it confirms and complements the recommendations of experts.
Hypocortisolaemia among athletes is a worrying situation which needs to be screened for optimal aetiological and therapeutic management. Besides the legal aspect of the doping context, this hypocortisolaemia leads to the suspicion of a state of adrenal insufficiency posing a major health risk for athletes, which can ultimately lead to an situation of acute adrenal insufficiency. This risk is increased in athletes who perform physical activity despite this corticotropic inhibition. Sport in itself, with its risks of traumatic injury and all the consequences induced, increases the risk of acute adrenal insufficiency. Sporting rest is therefore a significant health and safety decision for athletes, encouraged by all the experts.
It is therefore essential to screen for hypocortisolaemia in athletes using corticosteroids, whether symptomatic or asymptomatic (but with risk factors). The morning plasma cortisol level remains the most reliable screening test, with potential adaptation to the circadian rhythm of athletes, which is often changed or shifted. Publications relating to salivary cortisol are unanimously in favour of the theoretical validity and correct reliability of this test for adrenal insufficiency screening, with the advantages being its non-invasive character and greater representativity of the free and therefore biologically active fraction of cortisol. However, creating uniformity in the values and standardisation of sampling, packaging and transport methods are necessary to popularise this type of sampling.
Physical exercise, in all its forms leads, in a transient or more marked way, to an adaptation of the corticotropic axis. However, physical activity alone does not appear to induce hypocortisolaemia. The syndrome of over-training remains a complex nosological entity, with very heterogeneous publications and corticotropic changes that are not very sensitive and specific to this state, thus making it difficult to clearly establish hypocortisolaemia as a “pathognomonic” biological marker of this syndrome.
It is recognised that the use of exogenous glucocorticoids is the leading cause of the biological discovery of hypocortisolaemia. This action depends principally on the dose, the molecule and the duration of use. Despite the great diversity of publications, inhaled, intramuscular, intradermal and subcutaneous corticosteroids are clearly evident from our literature review as the routes of administration that are most inhibitory of the corticotropic axis (outside of the conventional oral and intravenous routes). For intranasal glucocorticoids, in eyedrops, corticotropic inhibition is very rare, and inherent to abusive supratherapeutic uses, the indication and purpose of which are debatable in practice, with other therapeutic alternatives being available.
For dermocorticoids, the literature is not so clear. The results are heterogeneous. The predictive factors for possible adrenal inhibition are: chronic use on pathological skin, on a large skin area, at a supratherapeutic dose with a high level (IV) and in very young or elderly subjects.
This work refines the previous publications and expert opinions. A major area of study then opens up on the following points:

Page | 80
Firstly, the reflection on the need to continue investigating the effects of corticosteroids on performance, in particular for chronic uses in endurance sports, to continue investigating over-training syndrome and its biological screening, and finally the influence of endurance exercise on the corticotropic axis.
Subsequently, the reflection on the awareness of prescribers, athletes, their entourage and in particular the different sports federations concerning the considerable risk of corticosteroids and the measures to be taken at the healthcare level in treated athletes.
Finally, more broadly, there is the question of the inclusion or extension of inclusion of all corticosteroids in the lists of medicines not authorised in competition and out of competition, given the severity of the adverse effects cited above.

Page | 81
BIBLIOGRAPHY
1. Duclos M, Guinot M, Colsy M, Merle F, Baudot C, Corcuff JB, et al. High risk of adrenal insufficiency after a single articular steroid injection in athletes. Med Sci Sports Exerc. juill 2007;39(7):1036-43.
2. Senard-Ojero A, Durrieu G, Depiesse F, Schmitt L, Riviere D, Montastruc J-L. Consommation de substances interdites chez le sportif : etude a l'Antenne Medicale de Prevention du Dopage de Midi-Pyrenees (AMPD-MP). Therapie. sept 2010;65(5):459-63.
3. COMMISSION MEDICALE - Axe-surrenalien-Cortisolemie.pdf [Internet]. [cited 13 March 2017]. Available at: http://www.ffc.fr/wp-content/uploads/2016/01/Axe-surrenalien-Cortisolemie.pdf?5f5a18
4. Axe hypothalamohypophysaire; axe hypothalamo-hypophysaire; axe hypothalamo-pituitaire; axe hypothalamopituitaire; systeme hypothalamo-hypophysaire; systeme hypothalamohypophysaire; systeme hypothalamo-pituitaire; systeme hypothalamopituitaire [Internet]. [cited 13 March 2017]. Available at: http://lookfordiagnosis.com/mesh_info.php?term=axe+hypothalamohypophysaire&lang=4
5. Adrenal Glands and Stress » Cause Point Correlative Testing - Natural Healing through Nutrition [Internet]. [cited 13 March 2017]. Available at: http://nutritionalmuscletesting.com/index.php?p=2_12
6. Difference between Adrenal Cortex and Adrenal Medulla I Major Differences [Internet]. [cited 13 March 2017]. Available at: http://www.majordifferences.com/2014/04/difference-between-adrenal-cortex-and.htmli*.WMbnqDhMC8A
7. Liakos P, Chambaz EM, Feige JJ, Defaye G. Expression of ACTH receptors (MC2-R and MC5-R) in the glomerulosa and the fasciculata-reticularis zones of bovine adrenal cortex. Endocr Res. nov 1998;24(3-4):427-32.
8. No Title [Internet]. [cited 13 March 2017]. Available at: http://tgenade.freeshell.org/thesis/thesisx.htm
9. Glucocorticoids [Internet]. [cited 13 March 2017]. Available at: http://www.lookfordiagnosis.com/mesh_info.php?term=Glucocorticoids&lang=1
10. Low cortisol high IGF I raised cortisol raised CPK I I cortisol and urine colour' [Internet]. [cited 13 March 2017]. Available at: http://www.stephaniespees.com/deed-reducing-levels-of-cortisol/
11. Debono M, Ghobadi C, Rostami-Hodjegan A, Huatan H, Campbell MJ, Newell-Price J, et al. Modified-release hydrocortisone to provide circadian cortisol profiles. J Clin Endocrinol Metab. May 2009;94(5):1548-54.
12. Snapshot [Internet]. [cited 13 March 2017]. Available at: http://www.academie-medecine.fr/publication100036371/
13. Corticoides locaux [Internet]. [cited 13 March 2017]. Available at: http://pharmacomedicale.org/medicaments/par-specialites/item/corticoides-locaux
14. [cited 13 March 2017]. Available at: http://jpmiss2.free.fr/Divers/SFAR_2008/ca96/html/ca96_028/96_28.htm

Page | 82
15. La pseudo polyarthrite rhizomelique - PDF [Internet]. [cited 13 March 2017]. Available at: http://docplayer.fr/12507074-La-pseudo-polyarthrite-rhizomelique.html
16. Kuipers H, Van’t Hullenaar G a. C, Pluim BM, Overbeek SE, De Hon O, Van Breda EJ, et al. Four
weeks’ corticosteroid inhalation does not augment maximal power output in endurance
athletes. Br J Sports Med. Nov 2008;42(11):868-71.
17. Nordsborg N, Ovesen J, Thomassen M, Zangenberg M, Jons C, laia FM, et al. Effect of
dexamethasone on skeletal muscle Na+,K+ pump subunit specific expression and K+ homeostasis during exercise in humans. J Physiol. 1 March 2008;586(5):1447-59.
18. Soetens E, De Meirleir K, Hueting JE. No influence of ACTH on maximal performance.
Psychopharmacology (Berl). Apr 1995;118(3):260-6.
19. Collomp K, Arlettaz A, Buisson C, Lecoq A-M, Mongongu C. Glucocorticoid administration
in athletes: Performance, metabolism and detection. Steroids. Nov 2016;115:193-202.
20. Snapshot [Internet]. [cited 13 March 2017]. Available at: https://fr.wikipedia.org/w/index.php?title=Hormone_corticotrope&oldid=134439834
21. Russell E, Koren G, Rieder M, Van Uum S. Hair cortisol as a biological marker of chronic stress: current status, future directions and unanswered questions.
Psychoneuroendocrinology. May 2012;37(5):589-601.
22. Miller R, Stalder T, Jarczok M, Almeida DM, Badrick E, Bartels M, et al. The CIRCORT database:
Reference ranges and seasonal changes in diurnal salivary cortisol derived from a meta-dataset comprised of 15 field studies. Psychoneuroendocrinology. nov 2016;73:16-23.
23. Medical Physiology/Gastrointestinal Physiology/Secretions - Wikibooks, open books for an open world [Internet]. [cited 13 March 2017]. Available at: https://en.wikibooks.org/wiki/Medical_Physiology/Gastrointestinal_Physiology/Secretions
24. Behr GA, Patel JP, Coote M, Moreira JCF, Gelain DP, Steiner M, et al. A statistical method to calculate blood contamination in the measurement of salivary hormones in healthy women. Clin Biochem. 16 Dec 2016;
25. van der Veen BS, Appelhof M, de Vries TW. Inhaled fluticasone propionate does not influence salivary cortisol when measured with tandem mass spectrometry. J Pediatr Endocrinol Metab JPEM. 2012;25(11-12):1217-9.
26. Saliva/Esputo - Sarstedt [Internet]. [cited 13 March 2017]. Available at: https://www.sarstedt.com/es/productos/diagnostico/salivaesputo/
27. Haussmann MF, Vleck CM, Farrar ES. A laboratory exercise to illustrate increased salivary cortisol in response to three stressful conditions using competitive ELISA. Adv Physiol Educ. 1 Jan 2007;31(1):110-5.
28. Perogamvros I, Keevil BG, Ray DW, Trainer PJ. Salivary cortisone is a potential biomarker for
serum free cortisol. J Clin Endocrinol Metab. Nov 2010;95(11):4951-8.
29. Zhang Q, Chen Z, Chen S, Xu Y, Deng H. Intraindividual stability of cortisol and cortisone and
the ratio of cortisol to cortisone in saliva, urine and hair. Steroids. Feb 2017;118:61-7.
30. Guinot M, Duclos M, Souberbielle J-C, Megret A, Le Bouc Y. Intérêts du Dosage du Cortisol Plasmatique Chez Des Cyclistes Elite. Rev Francoph Lab. 1 Sep 2005;2005(375):29-36.

Page | 83
31. Duclos M. Sollicitation de l'axe corticotrope aprés l'exercice musculaire chez le sportif entrainé [Thèse]. [1970-2013, France]: Universite de Bordeaux II; 1994.
32. Park H-Y, Nam S-S, Tanaka H, Lee D-J. Hemodynamic, Hematological, and Hormonal Responses to
Submaximal Exercise in Normobaric Hypoxia in Pubescent Girls. Pediatr Exerc Sci. weft 2016;28(3):417-22.
33. Hartley LH, Mason JW, Hogan RP, Jones LG, Kotchen TA, Mougey EH, et al. Multiple hormonal responses to prolonged exercise in relation to physical training. J Appl Physiol. nov 1972;33(5):607-10.
34. Buono MJ, Yeager JE, Hodgdon JA. Plasma adrenocorticotropin and cortisol responses to brief
high-intensity exercise in humans. J Appl Physiol Bethesda Md 1985. Oct 1986;61(4):1337-9.
35. Raastad T, Bjoro T, Hallén J. Hormonal responses to high- and moderate-intensity strength exercise. Eur J Appl Physiol. May 2000;82(1-2):121-8.
36. Minetto MA, Lanfranco F, Baldi M, Termine A, Kuipers H, Ghigo E, et al. Corticotroph axis
sensitivity after exercise: comparison between elite athletes and sedentary subjects. J Endocrinol Invest. Mar 2007;30(3):215-23.
37. Fournier PE, Stalder J, Mermillod B, Chantraine A. Effects of a 110 kilometers ultra-marathon race
on plasma hormone levels. Int J Sports Med. May 1997;18(4):252-6.
38. Mastorakos G, Pavlatou M. Exercise as a stress model and the interplay between the hypothalamus-pituitary-adrenal and the hypothalamus-pituitary-thyroid axes. Horm Metab Res Horm Stoffwechselforschung Horm Metab. Sep 2005;37(9):577-84.
39. Paccotti P, Minetto M, Terzolo M, Ventura M, Ganzit GP, Borrione P, et al. Effects of high-
intensity isokinetic exercise on salivary cortisol in athletes with different training schedules: relationships to serum cortisol and lactate. Int J Sports Med. Nov 2005;26(9):747-55.
40. Makras P, Koukoulis GN, Bourikas G, Papatheodorou G, Bedevis K, Menounos P, et al. Effect of 4 weeks of basic military training on peripheral blood leucocytes and urinary excretion of catecholamines and cortisol. J Sports Sci. weft 2005;23(8):825-34.
41. Heuser I, Deuschle M, Weber B, Stalla GK, Holsboer F. Increased activity of the hypothalamus-pituitary-adrenal system after treatment with the mineralocorticoid receptor antagonist spironolactone. Psychoneuroendocrinology. Jul 2000;25(5):513-8.
42. Kanaley JA, Weltman JY, Pieper KS, Weltman A, Hartman ML. Cortisol and growth hormone
responses to exercise at different times of day. J Clin Endocrinol Metab. Jun 2001;86(6):2881-9.
43. Duclos M. Facteurs limitants de l'anabolisme en phase de récupération de l'exercice musculaire intense et prolongé [Thèse Doctorat]. [Bordeaux, France]: sn; 1997.
44. Utter AC, Kang J, Robertson RJ, Nieman DC, Chaloupka EC, Suminski RR, et al. Effect of carbohydrate ingestion on ratings of perceived exertion during a marathon. Med Sci Sports Exerc. Nov 2002;34(11):1779-84.
45. Nieman DC. Influence of carbohydrate on the immune response to intensive, prolonged exercise.
Exerc Immunol Rev. 1998;4:64-76.
46. Deuster PA, Singh A, Hofmann A, Moses FM, Chrousos GC. Hormonal responses to ingesting
water or a carbohydrate beverage during a 2 h run. Med Sci Sports Exerc. Jan 1992;24(1):72-9.

Page | 84
47. Murray R, Paul GL, Seifert JG, Eddy DE. Responses to varying rates of carbohydrate ingestion during exercise. Med Sci Sports Exerc. Jun 1991;23(6):713-8.
48. doc-875.gif (Image GIF, 415 x 294 pixels) [Internet]. [cited 13 March 2017]. Available at: http://www.msport.net/newSite/IMG/doc-875.gif
49. Greenwood M. Aspects of Over-training. In: Antonio J, RD DK, Stout JR, Greenwood M, Willoughby DS, Haff GG, Eds. Essentials of Sports Nutrition and Supplements [Internet]. Humana Press; 2008 [cited 13 March 2017]. p. 121-42. Available at: http://link.springer.com/chapter/10.1007/978-1-59745-302-8_6
50. Halson SL, Jeukendrup AE. Does Over-training Exist? Sports Med. 1 Dec 2004;34(14):967-81.
51. Meeusen R, Duclos M, Foster C, Fry A, Gleeson M, Nieman D, et al. Prevention, diagnosis, and treatment of the over-training syndrome: joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med Sci Sports Exerc. Jan 2013;45(1):186-205.
52. Park JY, Hwang TK, Park HK, Ahn RS. Differences in cardiovascular and hypothalamic-pituitary-adrenal axis functions between high-altitude visitors and natives during a trek on the Annapurna circuit. Neuroendocrinology. 2014;99(2):130-8.
53. Hao K, Kong F-P, Gao Y-Q, Tang J-W, Chen J, Evans AM, et al. Inactivation of corticotropin-
releasing hormone-induced insulinotropic role by high-altitude hypoxia. Diabetes. Mar
2015;64(3):785-95.
54. Woods DR, Davison A, Stacey M, Smith C, Hooper T, Neely D, et al. The cortisol response to hypobaric hypoxia at rest and post-exercise. Horm Metab Res Horm Stoffwechselforschung Horm Metab. Apr 2012;44(4):302-5.
55. Panjwani U, Thakur L, Anand JP, Malhotra AS, Banerjee PK. Effect of simulated ascent to 3500
meter on neuro-endocrine functions. Indian J Physiol Pharmacol. Sep 2006;50(3):250 -6.
56. Benso A, Broglio F, Aimaretti G, Lucatello B, Lanfranco F, Ghigo E, et al. Endocrine and metabolic
responses to extreme altitude and physical exercise in climbers. Eur J Endocrinol. Dec 2007;157(6):733 -40.
57. Dimai HP, Ramschak-Schwarzer S, Leb G. [Altitude hypoxia: effects on selected endocrinological
parameters]. Wien Med Wochenschr 1946. 2000;150(8-9):178-81.
58. Martignoni E, Appenzeller O, Nappi RE, Sances G, Costa A, Nappi G. The effects of physical
exercise at high altitude on adrenocortical function in humans. Funct Neurol. Dec 1997;12(6):339
-44.
59. Richalet JP, Rutgers V, Bouchet P, Rymer JC, Kéromès A, Duval-Arnould G, et al. Diurnal variations of acute mountain sickness, colour vision, and plasma cortisol and ACTH at high altitude. Aviat Space Environ Med. fevr 1989;60(2):105-11.
60. Winter S. Évaluation de l’entretien médical réalisé par les sportifs sanctionnes pour dopage : expérience de l’Antenne médicale de prévention du dopage Rhône-Alpes de 2002 a 2012. 15 Mar 2013;64.
61. Site du French Paradox [Internet]. [cited 01 March 2017]. Available at: http://controverses.mines-paristech.fr/public/promo10/promo1O_G12/synthese/preuve.html

Page | 85
62. Corticosteroids: Corticoides inhales [Internet]. [cited 13 March 2017]. Available at: http://www.pharmacomedicale.org/medicaments/par-specialites/item/42
63. Corticosteroids: Corticoïdes inhalés [Internet]. [cited 13 March 2017]. Available at:
http://pharmacomedicale.org/medicaments/par-specialites/item/42
64. Wlodarczyk JH, Gibson PG, Caeser M. Impact of inhaled corticosteroids on cortisol suppression in adults with asthma: a quantitative review. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. Jan 2008;100(1):23-30.
65. Inhaled corticosteroids: - 090611111550.pdf [Internet]. [cited 01 March 2017]. Available at: http://www.dufmcepp.ups-tIse.fr/app_scom/scom_fichier/repertoire/090611111550.pdf
66. Andrade CR de, Camargos PAM, Ibiapina C da C, Lasmar LM de LBF. Basal cortisol in asthmatics on two different doses of fluticasone propionate. J Pediatr (Rio J). Aug 2008;84(4):373-6.
67. Oliver A, VanBuren S, Allen A, Hamilton M, Tombs L, Inamdar A, et al. Tolerability of fluticasone
furoate/vilanterol combination therapy in children aged 5 to 11 years with persistent asthma.
Clin Ther. 1 Jun 2014;36(6):928-939.e1.
68. Moderate dose inhaled corticosteroid-induced symptomatic adrenal suppression: case report and review of the literature. - PubMed - NCBI [Internet]. [cited 01 March 2017]. Available at: https://www.ncbi.nlm.nih.gov/pubmed/23043135
69. Milner EW, Lombard C, Galal U, Hough S, Irusen E, Weinberg E. Hypothalamic-pituitary-adrenal
axis suppression in asthmatic children on inhaled and nasal corticosteroids--more common
than expected? J Pediatr Endocrinol Metab JPEM. 2011;24(7-8):529-34.
70. Kaur C, Barisal SK, Chhabra SK. Study on serum and urinary cortisol levels of asthmatic patients after treatment with high dose inhaled beclomethasone dipropionate or budesonide. Indian J Chest Dis Allied Sci. Jun 2005;47(2):89-95.
71. Martin RJ, Szefler SJ, Chinchilli VM, Kraft M, Dolovich M, Boushey HA, et al. Systemic effect comparisons of six inhaled corticosteroid preparations. Am J Respir Crit Care Med. 15 May 2002;165(10):1377-83.
72. Mallol J, Aguirre V. Once versus twice daily budesonide metered-dose inhaler in children with
mild to moderate asthma: effect on symptoms and bronchial responsiveness. Allergol Immunopathol (Madr). Feb 2007;35(1):25-31.
73. PubMed entry [Internet]. [cite 17 Feb 2017]. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9248762
74. Bacharier LB, Raissy HH, Wilson L, McWilliams B, Strunk RC, Kelly HW. Long-term effect of budesonide on hypothalamic-pituitary-adrenal axis function in children with mild to moderate asthma. Pediatrics. Jun 2004;113(6):1693-9.
75. Aaronson D, Kaiser H, Dockhorn R, Findlay S, Korenblat P, Thorsson L, et al. Effects of budesonide by means of the Turbuhaler on the hypothalmic-pituitary-adrenal axis in asthmatic subjects: a dose-response study. J Allergy Clin Immunol. Mar 1998;101(3):312-9.
76. O'Byrne PM, Bleecker ER, Bateman ED, Busse WW, Woodcock A, Forth R, et al. Once-daily fluticasone furoate alone or combined with vilanterol in persistent asthma. Eur Respir J. Mar 2014;43(3):773-82.

Page | 86
77. Lipworth BJ, Kaliner MA, LaForce CF, Baker JW, Kaiser HB, Amin D, et al. Effect of ciclesonide and fluticasone on hypothalamic-pituitary-adrenal axis function in adults with mild-to-moderate persistent asthma. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. Apr 2005;94(4):465-72.
78. Woodcock A, Lötvall J, Busse WW, Bateman ED, Stone S, Ellsworth A, et al. Efficacy and safety of fluticasone furoate 100 µg and 200 µg once daily in the treatment of moderate-severe asthma in adults and adolescents: a 24-week randomised study. BMC Pulm Med. 9 Jul 2014;14:113.
79. Nakahara N, Wakamatsu A, Kempsford R, Allen A, Yamada M, Nohda S, et al. The safety, pharmacokinetics and pharmacodynamics of a combination of fluticasone furoate and vilanterol in healthy Japanese subjects. Int J Clin Pharmacol Ther. Aug 2013;51(8):660-71.
80. Whelan GJ, Blumer JL, Martin RJ, Szefler SJ, Asthma Clinical Research Network and the Pediatric Pharmacology Research Unit Network. Fluticasone propionate plasma concentration and systemic effect: effect of delivery device and duration of administration. J Allergy Clin Immunol. Sep 2005;116(3):525-30.
81. Cavkaytar O, Vuralli D, Arik Yilmaz E, Buyuktiryaki B, Soyer O, Sahiner UM, et al. Evidence of hypothalamic-pituitary-adrenal axis suppression during moderate-to-high-dose inhaled corticosteroid use. EurJ Pediatr. Nov 2015;174(11):1421-31.
82. Allen A, Schenkenberger I, Trivedi R, Cole J, Hicks W, Gul N, et al. Inhaled fluticasone furoate/vilanterol does not affect hypothalamic-pituitary-adrenal axis function in adolescent and adult asthma: randomised, double-blind, placebo-controlled study. Clin Respir J. Oct 2013;7(4):397-406.
83. Lee DKC, Fardon TC, Bates CE, Haggart K, McFarlane LC, Lipworth BJ. Airway and systemic effects
of hydrofluoroalkane formulations of high-dose ciclesonide and fluticasone in moderate
persistent asthma. Chest. Mar 2005;127(3):851-60.
84. Eid N, Morton R, Olds B, Clark P, Sheikh S, Looney S. Decreased morning serum cortisol levels in children with asthma treated with inhaled fluticasone propionate. Pediatrics. Feb 2002;109(2):217-21.
85. Brus R. Effects of high-dose inhaled corticosteroids on plasma cortisol concentrations in healthy adults. Arch Intern Med. 13 Sep 1999;159(16):1903-8.
86. Wales D, Makker H, Kane J, McDowell P, O’Driscoll BR. Systemic bioavailability and potency of
high-dose inhaled corticosteroids: a comparison of four inhaler devices and three drugs in healthy adult volunteers. Chest. May 1999;115(5):1278-84.
87. Li JT, Ford LB, Chervinsky P, Weisberg SC, Kellerman DJ, Faulkner KG, et al. Fluticasone propionate powder and lack of clinically significant effects on hypothalamic-pituitary-adrenal axis and bone mineral density over 2 years in adults with mild asthma. J Allergy Clin Immunol. Jun
1999;103 (6):1062-8.
88. Donnelly R, Williams KM, Baker AB, Badcock CA, Day RO, Seale JP. Effects of budesonide and fluticasone on 24-hour plasma cortisol. A dose-response study. Am J Respir Crit Care Med. Dec 1997;156(6):1746-51.
89. Clark DJ, Lipworth BJ. Adrenal suppression with chronic dosing of fluticasone propionate
compared with budesonide in adult asthmatic patients. Thorax. Jan 1997;52(1):55-8.
90. Boorsma M, Andersson N, Larsson P, Ullman A. Assessment of the relative systemic potency of inhaled fluticasone and budesonide. Eur Respir J. Jul 1996;9(7):1427-32.

Page | 87
91. Kowalski ML, Wojciechowski P, Dziewonska M, Rys P. Adrenal suppression by inhaled corticosteroids in patients with asthma: A systematic review and quantitative analysis. Allergy Asthma Proc. Feb 2016;37(1):9-17.
92. Kramer S, Rottier BL, Scholten RJPM, Boluyt N. Ciclesonide versus other inhaled corticosteroids for chronic asthma in children. Cochrane Database Syst Rev. 28 Feb 2013;(2):CD010352.
93. O’Connor BJ, Kilfeather S, Cheung D, Kale H, Blagden MD, Schlosser N, et al. Efficacy and safety of ciclesonide in patients with severe asthma: a 12-week, double-blind, randomized, parallel-group study with long-term (1-year) follow-up. Expert Opin Pharmacother. Dec 2010;11(17):2791-803.
94. Craig T. The safety profile of ciclesonide in the treatment of persistent asthma. Allergy Asthma
Proc. Jun 2009;30(3):315-24.
95. Meltzer EO, Derendorf H. The systemic safety of inhaled corticosteroid therapy: a focus on ciclesonide. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. Aug 2006;97(2):149-57.
96. Pedersen S, Engelstatter R, Weber H-J, Hirsch S, Barkai L, Emeryk A, et al. Efficacy and safety of ciclesonide once daily and fluticasone propionate twice daily in children with asthma. Pulm Pharmacol Ther. Jun 2009;22(3):214-20.
97. Bateman ED, Linnhof AE, Homik L, Freudensprung U, Smau L, Engelstatter R. Comparison of twice-daily inhaled ciclesonide and fluticasone propionate in patients with moderate-to-severe persistent asthma. Pulm Pharmacol Ther. 2008;21(2):264-75.
98. Rohatagi S, Arya V, Zech K, Nave R, Hochhaus G, Jensen BK, et al. Population pharmacokinetics
and pharmacodynamics of ciclesonide. J Clin Pharmacol. Apr 2003;43(4):365-78.
99. Kosoglou T, Hubbell J, Cutler DL, Johnson-Levonas AO, Xu D, Kantesaria BS, et al. Hypothalamic-pituitary-adrenal axis effects of mometasone furoate/formoterol fumarate vs. fluticasone propionate/salmeterol administered through metered-dose inhaler. Chest. Dec 2013;144(6):1795 -802.
100. Chrousos GP, Ghaly L, Shedden A, Lezzoni DG, Harris AG. Effects of mometasone furoate dry
powder inhaler and beclomethasone dipropionate hydrofluoroalkane and chlorofluorocarbon on the hypothalamic-pituitary-adrenal axis in asthmatic subjects. Chest. Jul 2005;128(1):70-7.
101. Skoner DP, Gentile DA, Angelini B. Effect of therapeutic doses of mometasone furoate on cortisol
levels in children with mild asthma. Allergy Asthma Proc. Feb 2010;31(1):10-9.
102. Hasegawa T, Ishihara K, Fujii H, Hajiro T, Watanabe I, Nishimura T, et al. Influence of high dose
inhaled steroids on hypothalamo-pituitary-adrenal axis function in Japanese patients with asthma: a comparison over the course of time. Intern Med Tokyo Jpn. May 1996;35(5):362-6.
103. Doull IJ, Freezer NJ, Holgate ST. Growth of prepubertal children with mild asthma treated with inhaled beclomethasone dipropionate. Am J Respir Crit Care Med. Jun 1995;151(6):1715-9.
104. Katsunuma T, Akasawa A, Iikura Y. Adrenal function of children with bronchial asthma treated with beclomethasone dipropionate. Ann Allergy. Dec 1992;69(6):529-32.
105. Chen X, Zheng X, Jiang J, Hu P, Wu K, Zhuang L, et al. Pharmacodynamics and pharmacokinetics of fluticasone furoate/vilanterol in healthy Chinese subjects. Pharmacotherapy. Jun 2015;35(6):586 -99.

Page | 88
106. Berger WE, Leflein JG, Geller DE, Parasuraman B, Miller CJ, O’Brien CD, et al. The safety and clinical benefit of budesonide/formoterol pressurized metered-dose inhaler versus budesonide alone in children. Allergy Asthma Proc. Feb 2010;31(1):26-39.
107. Mahlab-Guri K, Asher I, Gradstein S, Zung A, Radian-Sade S, Elbirt D, et al. Inhaled
fluticasone causes iatrogenic Cushing’s syndrome in patients treated with Ritonavir. J Asthma Off J Assoc Care Asthma. Oct 2011;48(8):860-3.
108. St Germain RM, Yigit S, Wells L, Girotto JE, Giratto JE, Salazar JC. Cushing syndrome and severe adrenal suppression caused by fluticasone and protease inhibitor combination in an HIV-infected adolescent. AIDS Patient Care STDs. Jun 2007;21(6):373-7.
109. Bousquet J, Poli G, Acerbi D, Monno R, Ramael S, Nollevaux F. Systemic exposure and implications for lung deposition with an extra-fine hydrofluoroalkane beclometasone dipropionate/formoterol fixed combination. Clin Pharmacokinet. 2009;48(6):347-58.
110. Jenkins C, Kolarikova R, Kuna P, Caillaud D, Sanchis J, Popp W, et al. Efficacy and safety of high-dose budesonide/formoterol (Symbicort) compared with budesonide administered either concomitantly with formoterol or alone in patients with persistent symptomatic asthma. Respirol Carlton Vic. May 2006;11(3):276-86.
111. Gupta D, Behera D, Lalrinmawia H, Dash RJ. Hypothalamo-pituitary-adrenal axis function in
asthmatics taking low dose inhaled beclomethasone dipropionate. J Assoc Physicians India. Jul
2000;48(7):682-4.
112. Srichana T, Juthong S, Thawithong E, Supaiboonpipat S, Soorapan S. Clinical equivalence of budesonide dry powder inhaler and pressurized metered dose inhaler. Clin Respir J. Jan 2016;10(1):74-82.
113. Nair A, McKinlay L, Williamson P, Short P, Burns P, Lipworth BJ. Comparative lung bioavailability of fluticasone/salmeterol via a breath-actuated spacer and conventional plastic spacers. Eur J
Clin Pharmacol. Apr 2011;67(4):355-63.
114. Goldberg S, Einot T, Algur N, Schwartz S, Greenberg AC, Picard E, et al. Adrenal suppression in asthmatic children receiving low-dose inhaled budesonide: comparison between dry powder inhaler and pressurized metered-dose inhaler attached to a spacer. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. Dec 2002;89(6):566-71.
115. Tukiainen H, Rytilä P, Hämäläinen KM, Silvasti MSL, Keski-Karhu J, Finnish Study Group. Safety, tolerability and acceptability of two dry powder inhalers in the administration of budesonide in steroid-treated asthmatic patients. Respir Med. Apr 2002;96(4):221-9.
116. Thorsson L, Edsbacker S, Källén A, Löfdahl CG. Pharmacokinetics and systemic activity of fluticasone via Diskus and pMDI, and of budesonide via Turbuhaler. Br J Clin Pharmacol. Nov 2001;52(5):529-38.
117. Trescoli C, Ward MJ. Systemic activity of inhaled and swallowed beclomethasone
dipropionate and the effect of different inhaler devices. Postgrad Med J. Nov
1998;74(877):675-7.
118. Goldberg S, Algur N, Levi M, Brukheimer E, Hirsch HJ, Branski D, et al. Adrenal suppression among asthmatic children receiving chronic therapy with inhaled corticosteroid with and without spacer device. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. Mar 1996;76(3):234-8.

Page | 89
119. Selroos O, Halme M. Effect of a volumatic spacer and mouth rinsing on systemic absorption of inhaled corticosteroids from a metered dose inhaler and dry powder inhaler. Thorax. Dec 1991;46(12):891-4.
120. Wu K, Goyal N, Stark JG, Hochhaus G. Evaluation of the administration time effect on the cumulative cortisol suppression and cumulative lymphocytes suppression for once-daily inhaled corticosteroids: a population modeling/simulation approach. J Clin Pharmacol. Sep 2008;48(9):1069 -80.
121. Zetterström O, Dahl R, Lindqvist A, Olsson P. Comparable morning versus evening administration
of once-daily mometasone furoate dry powder inhaler. Respir Med. Oct 2008;102(10):1406-11.
122. Weinbrenner A, Hüneke D, Zschiesche M, Engel G, Timmer W, Steinijans VW, et al. Circadian rhythm of serum cortisol after repeated inhalation of the new topical steroid ciclesonide. J Clin Endocrinol Metab. May 2002;87(5):2160-3.
123. Postma DS, Sevette C, Martinat Y, Schlosser N, Aumann J, Kafé H. Treatment of asthma by the inhaled corticosteroid ciclesonide given either in the morning or evening. Eur Respir J. Jun 2001;17(6):1083 -8.
124. Tsartsali L, Papadopoulos M, Lagona E, Papadimitriou A, Kanaka-Gantenbein C, Louizou E, et al. Association of hypothalamic-pituitary-adrenal axis-related polymorphisms with stress in asthmatic children on inhaled corticosteroids. Neuroimmunomodulation. 2012;19(2):88-95.
125. Schwindt CD, Zaldivar F, Eliakim A, Shin H-W, Leu S-Y, Cooper DM. Inhaled fluticasone and the hormonal and inflammatory response to brief exercise. Med Sci Sports Exerc. Oct 2010;42(10):1802-8.
126. Daley-Yates PT, Tournant J, Kunka RL. Comparison of the systemic availability of fluticasone propionate in healthy volunteers and patients with asthma. Clin Pharmacokinet. 2000;39 Suppl
1:39-45.
127. Brutsche MH, Brutsche IC, Munawar M, Langley SJ, Masterson CM, Daley-Yates PT, et al. Comparison of pharmacokinetics and systemic effects of inhaled fluticasone propionate in patients with asthma and healthy volunteers: a randomised crossover study. Lancet Lond Engl. 12 Aug 2000;356(9229):556-61.
128. Thorsson L, Dahlström K, Edsbäcker S, Källeé A, Paulson J, Wirén JE. Pharmacokinetics and systemic effects of inhaled fluticasone propionate in healthy subjects. Br J Clin Pharmacol. Feb 1997;43(2):155-61.
129. Lonnebo A, Grahnen A, Jansson B, Brundin RM, Ling-Andersson A, Eckernäs SA. An assessment of the systemic effects of single and repeated doses of inhaled fluticasone propionate and inhaled budesonide in healthy volunteers. EurJ Clin Pharmacol. 1996;49(6):459-63.
130. Reddy S, Ananthakrishnan S, Garg A. A prospective observational study evaluating hypothalamic-
pituitary-adrenal axis alteration and efficacy of intramuscular triamcinolone acetonide for steroid-responsive dermatologic disease. J Am Acad Dermatol. Aug 2013;69(2):226-31.
131. Carson TE, Daane TA, Weinstein RL. Long-term intramuscular administration of triamcinolone acetonide. Effect on the hypothalamic-pituitary-adrenal axis. Arch Dermatol. Dec 1975;111(12):1585-7.
132. Wachs GN. Letter: The effect of intracutaneous glucocorticoids on plasma cortisol levels. Br J
Dermatol. Dec 1973;89(6):647-8.

Page | 90
133. Potter RA. Intralesional triamcinolone and adrenal suppression in acne vulgaris. J Invest Dermatol. Dec 1971;57(6):364-70.
134. principaux corticoïdes utilisables par voie locale et indications [Internet]. [cited 13 March 2017]. Available at: http://www.rhumato.info/fiches-pratiques2/152-corticoides/1828-principaux-corticoides-utilisables-par-voie-locale-et-indications
135. Younes M, Neffati F, Touzi M, Hassen-Zrour S, Fendri Y, Béjia I, et al. Systemic effects of epidural and intra-articular glucocorticoid injections in diabetic and non-diabetic patients. Joint Bone Spine. Oct 2007;74(5):472-6.
136. Mader R, Lavi I, Luboshitzky R. Evaluation of the pituitary-adrenal axis function following
single intraarticular injection of methylprednisolone. Arthritis Rheum. Mar 2005;52(3):924-8.
137. Huppertz HI, Pfüller H. Transient suppression of endogenous cortisol production after intraarticular steroid therapy for chronic arthritis in children. J Rheumatol. Sep 1997;24(9):18337.
138. Gless KH, Klee HR, Vecsei P, Weber M, Haack D, Lichtwald K. [Plasma concentration and systemic effect of betamethasone after intra-articular injection (author's transl)]. Dtsch Med Wochenschr 1946. 29 May 1981;106(22):704 -7.
139. Habib GS. Systemic effects of intra-articular corticosteroids. Clin Rheumatol. Jul 2009;28(7):74956.
140. Wicki J, Droz M, Cirafici L, Vallotton MB. Acute adrenal crisis in a patient treated
with intraarticular steroid therapy. J Rheumatol. Feb 2000;27(2):510-1.
141. Weiss S, Fischel B, Kisch ES. Systemic effects of intra-articular steroid preparations. Ann
Rheum Dis. weft 1980;39(4):413-4.
142. Corticoïdes locaux [Internet]. [cited 13 March 2017]. Available at: http://pharmacomedicale.org/medicaments/par-specialites/item/corticoides-locaux
143. Bockle BC, Jara D, Nindl W, Aberer W, Sepp NT. Adrenal insufficiency as a result of long-
term misuse of topical corticosteroids. Dermatol Basel Switz. 2014;228(4):289-93.
144. Levin E, Gupta R, Butler D, Chiang C, Koo JYM. Topical steroid risk analysis: differentiating between physiologic and pathologic adrenal suppression. J Dermatol Treat. Dec 2014;25(6):501 - 6.
145. Gilbertson EO, Spellman MC, Piacquadio DJ, Mulford MI. Super potent topical corticosteroid
use associated with adrenal suppression: Clinical considerations. J Am Acad Dermatol. Feb
1998;38(2, Supplement):318-21.
146. Silver S, Tuppal R, Gupta AK, Clonier F, Olesen M, Leeder R, et al. Effect of calcipotriene plus betamethasone dipropionate topical suspension on the hypothalamic-pituitary-adrenal axis and calcium homeostasis in subjects with extensive psoriasis vulgaris: an open, non-controlled, 8-week trial. J Drugs Dermatol JDD. Aug 2013;12(8):882-7.
147. Castela E, Archier E, Devaux S, Gallini A, Aractingi S, Cribier B, et al. Topical corticosteroids in plaque psoriasis: a systematic review of risk of adrenal axis suppression and skin atrophy. J Eur Acad Dermatol Venereol JEADV. May 2012;26 Suppl 3:47-51.

Page | 91
148. Campbell LS, Chevalier M, Levy RA, Rhodes A. Hypothalamic-pituitary-adrenal axis suppression related to topical glucocorticoid therapy in a child with psoriatic exfoliative erythroderma. Pediatr Dermatol. Feb 2012;29(1):101-4.
149. Kerner M, Shay A, Ziv M, Rozenman D, Luboshitzky R. Evaluation of the pituitary-adrenal axis
function in patients on topical steroid therapy. J Am Acad Dermatol. 1 Jul 2011;65(1):215-6.
150. Ellison JA, Patel L, Ray DW, David TJ, Clayton PE. Hypothalamic-pituitary-adrenal function and
glucocorticoid sensitivity in atopic dermatitis. Pediatrics. Apr 2000;105(4 Pt 1):794-9.
151. Neumann RA, Schmidt JB, Spona J. [Effect of topical glucocorticoids on endogenous cortisol production]. Z Hautkr. 15 Apr 1988;63(4):302-8.
152. Katz HI, Hien NT, Prawer SE, Mastbaum LI, Mooney JJ, Samson CR. Superpotent topical steroid treatment of psoriasis vulgaris--clinical efficacy and adrenal function. J Am Acad Dermatol. Apr 1987;16(4):804-11.
153. Ohman EM, Rogers S, Meenan FO, McKenna TJ. Adrenal suppression following low-dose topical
clobetasol propionate. J R Soc Med. Jul 1987;80(7):422-4.
154. Cornell RC, Stoughton RB. Six-month controlled study of effect of desoximetasone and
betamethasone 17-valerate on the pituitary-adrenal axis. Br J Dermatol. Jul 1981;105(1):91-5.
155. Thornfeldt C, Cornell RC, Stoughton RB. The effect of alclometasone dipropionate cream 0.05%
on the hypothalamic-pituitary-adrenal axis of normal volunteers. J Int Med Res. 1985;13(5):27680.
156. Martino BJ, Church CA, Seiberling KA. Effect of intranasal dexamethasone on endogenous cortisol
level and intraocular pressure. Int Forum Allergy Rhinol. Jul 2015;5(7):605-9.
157. Licata AA. Systemic effects of fluticasone nasal spray: report of 2 cases. Endocr Pract Off J Am
Coll Endocrinol Am Assoc Clin Endocrinol. Jun 2005;11(3):194-6.
158. Sastre J, Déez JJ, López Guzmán A, Iglesias P, Martínez I, Gómez-Pan A. [Self-induced Cushing’s syndrome due to dexamethasone abuse in nasal spray: clinical and biochemical study]. An Med Interna Madr Spain 1984. Apr 1994;11(4):181-4.
159. Bruni FM, De Luca G, Venturoli V, Boner AL. Intranasal corticosteroids and adrenal suppression.
Neuroimmunomodulation. 2009;16(5):353-62.
160. Tripathy I, Levy A, Ratner P, Clements D, Wu W, Philpot E. HPA axis safety of fluticasone furoate
nasal spray once daily in children with perennial allergic rhinitis. Pediatr Allergy Immunol Off Publ Eur Soc Pediatr Allergy Immunol. May 2009;20(3):287-94.
161. Patel D, Ratner P, Clements D, Wu W, Faris M, Philpot E. Lack of effect on adult and adolescent hypothalamic-pituitary-adrenal axis function with use of fluticasone furoate nasal spray. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. May 2008;100(5):490-6.
162. Kim KT, Rabinovitch N, Uryniak T, Simpson B, O'Dowd L, Casty F. Effect of budesonide aqueous nasal spray on hypothalamic-pituitary-adrenal axis function in children with allergic rhinitis. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. Jul 2004;93(1):61-7.
163. Hermann R, Locher M, Siebert-Weigel M, LaVallee N, Derendorf H, Hochhaus G. Intranasal loteprednol etabonate in healthy male subjects: pharmacokinetics and effects on endogenous cortisol. J Clin Pharmacol. May 2004;44(5):510-9.

Page | 92
164. Bachert C, Lukat KF, Lange B. Effect of intranasal fluticasone propionate and triamcinolone acetonide on basal and dynamic measures of hypothalamic-pituitary-adrenal-axis activity in healthy volunteers. Clin Exp Allergy J Br Soc Allergy Clin Immunol. Jan 2004;34(1):85-90.
165. Brannan MD, Herron JM, Reidenberg P, Affrime MB. Lack of hypothalamic-pituitary-adrenal axis suppression with once-daily or twice-daily beclomethasone dipropionate aqueous nasal spray administered to patients with allergic rhinitis. Clin Ther. Aug 1995;17(4):637-47.
166. McGhee CNJ, Dean S, Danesh-Meyer H. Locally administered ocular corticosteroids: benefits
and risks. Drug Saf. 2002;25(1):33-55.
167. Krupin T, Mandell Al, Podos SM, Becker B. Topical corticosteroid therapy and pituitary-
adrenal function. Arch Ophthalmol Chic III 1960. Jun 1976;94(6):919-20.
168. Baba S, Mishima H, Okimoto M, Miyachi Y. Plasma steroid levels and clinical effects after
topical application of betamethasone. Graefes Arch Clin Exp Ophthalmol Albrecht Von Graefes Arch Klin Exp Ophthalmo1.1983;220(5):209-14.
169. Afandi B, Toumeh MS, Saadi HF. Cushing's syndrome caused by unsupervised use of ocular glucocorticoids. Endocr Pract Off J Am Coll Endocrinol Am Assoc Clin Endocrinol. Dec 2003;9(6):526-9.
170. Sandhu SS, Smith JM, Doherty M, James A, Figueiredo FC. Do topical ophthalmic
corticosteroids suppress the hypothalamic-pituitary-adrenal axis in post-penetrating keratoplasty patients? Eye Lond Engl. May 2012;26(5):699-702.
171. MPCC - Mouvement Pour un Cyclisme Credible [Internet]. [cited 02 March 2017]. Available at: http://www.mpcc.fr/index.php/fr/

Page | 93
Decrees, orders, circulars GENERAL TEXTS
MINISTRY OF FOREIGN AFFAIRS
AND INTERNATIONAL DEVELOPMENT
Decree No. 2016-1923 of 19 December 2016 issuing the amendment to Annex I to the International Convention against Doping in Sport, adopted in Paris on 29 November 2016 (1)
NOR: MAEJ1634743D
The President of the Republic,
On the report of the First Minister of Foreign Affairs and International Development,
In view of the Constitution, in particular Articles 52 to 55 thereof;
In view of Decree No. 53-192 of 14 March 1953, as amended, relating to the ratification and publication of
international commitments entered into by France,
In view of Decree No. 2007-503 of 2 April 2007 on the publication of the International Convention against Doping in
Sport (together two annexes), adopted in Paris on 19 October 2005:
In view of Decree No. 2009-93 of 26 June 2009 on the publication of the amendment to the Annex to the Anti-
Doping Convention adopted on 13 November 2008 in Strasbourg, and to Annex 1 to the International Convention
against Doping in Sport, adopted in Paris on 17 November 2008;
In view of Decree No. 2010-134 of 10 February 2010 on the publication of the amendment to the Annex to the Anti-
Doping Convention adopted on 18 November 2009 in Strasbourg, and to Annex 1 to the International Convention
against Doping in Sport, adopted in Paris on 28 October 2009;
In view of Decree No. 2010-1578 of 16 December 2010 on the publication of the amendment to the Annex to the
Anti-Doping Convention adopted on 08 and 09 November 2009 in Strasbourg, and to Annex 1 to the International
Convention against Doping in Sport, adopted in Paris on 17 November 2010;
In view of Decree No. 2011-1947 of 23 December 2011 on the publication of the amendment to the Annex to the
Anti-Doping Convention adopted on 07 November 2011 in Strasbourg, and to Annex 1 to the International Convention
against Doping in Sport, adopted in Paris on 14 November 2011;
In view of Decree No. 2012-1426 of 19 December 2012 on the publication of the amendment to the Annex to the
Anti-Doping Convention adopted on 13 November 2012 in Paris, and to Annex 1 to the International Convention
against Doping in Sport, adopted in Paris on 12 November 2012;
In view of Decree No. 2013-1286 of 27 December 2013 on the publication of the amendment to the Annex to the
Anti-Doping Convention adopted on 14 November 2013 in Strasbourg, and to Annex 1 to the International Convention
against Doping in Sport, adopted in Paris on 11 November 2013;
In view of Decree No. 2014-1005 of 4 September 2014 publishing the 2014 list of substances and methods prohibited
in sport (version 2, adopted on 1 July 2014);
Decree No. 2014-1556 of 22 December 2014 issuing the amendment to Annex I to the International Convention
against Doping in Sport, adopted in Paris on 17 November 2014;
Decree No. 2015-1684 of 16 December 2015 issuing the amendment to Annex I to the International Convention
against Doping in Sport, adopted in Paris on 06 November 2015;
Decrees as follows:
Art. 1. - The amendment to Annex I to the International Convention against Doping in Sport, adopted in Paris on 29
November 2016, will be published in the Official Journal of the French Republic.
Art. 2. – The Prime Minister and the Minister for Foreign Affairs and International Development are responsible, in
their respective spheres, for the execution of this decree, which is to be published in the Official Journal of the French
Republic.
Drawn up on 14 December 2016. FRANÇOIS HOLLANDE
By the President of the Republic:
30 December 2016 OFFICIAL JOURNAL OF THE REPUBLIC OF FRANCE Text 18 of 223
ANNEX
Annex 1- List of prohibitions according to the Sports Code, updated December 2016

Page | 94
The Prime Minister, BERNARD CAZENEUVE
The Minister of Foreign Affairs and International Development, JEAN-MARC AYRAULT
(1) Entry into force: 1 January 2011
AMENDMENT
TO ANNEX I TO THE INTERNATIONAL CONVENTION AGAINST DOPING IN SPORT, ADOPTED IN PARIS ON 29 NOVEMBER 2016
WORLD ANTI-DOPING CODE
LIST OF PROHIBITIONS 2017 – INTERNATIONAL STANDARD
Entry into force on 1 January 2017
The official roster of the Prohibited List will be kept up to date by WADA and published in English and French.
The English version will be authoritative in case of discrepancy between the two versions.
According to Article 4.2.2 of the World Anti-Doping Code, Prohibited Substances must be deemed to be
“specified substances” except for substances in Classes S1, S2, S4.4, S4.5, S6.a and the prohibited methods M1, M2
and M3.
PERMANENTLY PROHIBITED SUBSTANCES AND METHODS (WITHIN AND OUTSIDE OF COMPETITION)
PROHIBITED SUBSTANCES
S0. NON-APPROVED SUBSTANCES
Any pharmacological substance not included in a section of the below list that is not currently approved for therapeutic use in humans by a government health regulatory authority (e.g. medicines in preclinical or clinical development or that are no longer available, customised medicines, substances approved only for veterinary use) is prohibited at all times.
S1. ANABOLIC AGENTS
Anabolic agents are prohibited.
1. Anabolic androgenic steroids (AAS)
a. Exogenous AAS*, including:
1-androstenediol (5α.-androst-1.-ene-3β,17β-diol);
1- androstenedione (5α.-androst-1.-ene-3,17-dione);
1-testosterone (17β-hydroxy-5α-androst-l-ene-3-one)
4-hydroxytestosterone (4,17β-dihydroxyandrost-4-ene-3-one);
balandiol (estr-4-ene-3 β,17β-diol);
bolasterone;
calusterone;
clostebol;
danazol ([1,2]oxazolo[4’,5’:2,3]pregna-4-ene-20yn-17α-ol);
dehydrochlormethyltestosterone (4-chloro-17β-hydroxy-17α-methylandrosta-1,4-diene-3-one);
deoxymethyltestosterone (17α-methyl-5α-androst-2-ene-17β-ol);
drostanolone;
ethylestrenol (19-norpregna-4-ene-17α-ol);
fluoxymesterone;
formebolone;
furazabol (17α-methyl[1,2,5]oxadiazolo[3’,4’:2,3]-5α-androstane-17β-ol);
gestrinone;
mestanolone;
mesterolone;
methandienone (17β-hydroxy-17α-methylandrosta-1,4-diene-3-one);
30 December 2016 OFFICIAL JOURNAL OF THE REPUBLIC OF FRANCE Text 18 of 223

Page | 95
metenolone;
methandriol;
methasterone (17β-hydroxy-2α,17α-dimethyl-5α-androstane-3-one);
methyldienolone (17β-hydroxy-17α-methylestra-4,9-diene-3-one);
methyl-1-testosterone (17β-hydroxy-17α-methyl-5α-androst-1-ene-3-one);
methylnortestosterone (17β-hydroxy-17α-methylestr-4-en-3-one);
methyltestosterone;
metribolone (methyltrienolone, 17β-hydroxy-17α-methylestra-4,9,11-triene-3-one);
mibolerone;
norboletone;
norclostebol;
norethandrolone;
oxabolone;
oxandrolone;
oxymesterone;
oxymethelone;
prostanozol (17β-[(tetrahydropyrane-2-yl)oxy]-1’Hpyrazolo[3,4 :2,3]-5 α-androstane;
quinbolone;
stanozolol;
stenbolone;
tetrahydrogestrinone (17-hydroxy-18 α-homo-19-nor-17 α a-pregna-4,9,11-triene-3-one);
trenbolone (17β-hydroxyestr-4,9,11-triene-3-one);
And other substances with a similar chemical structure or similar biological effect(s).
b. Androghenic AAS** by exogenous administration:
19-norandrostenediol (estr-4-ene-3,7-diol);
19-norandrostenedione (estr-4-ene-3,7-dione);
boldenone;
boldione (androsta-1,4-diene-3,17-dione);
dihydrotestosterone (17β-hydroxy-5 α-androstan-3-one);
nandrolone (19-nortestosterone);
parasterone (dehydroepiandrosterone, DHEA, 3β-hydroxyandrost-5-ene-17-one)
testosterone;
and the following metabolites and isomers, including but not limited to:
3β-hydroxy-5α-androstan-17-one;
5α-androst-2-ene-17-one;
5α-androstane-3α,17α-diol;
5α-androstane-3α,17α-diol;
5α-androstane-3α,17α-diol;
5α-androstane-3α,17α-diol;
5β-androstane-3α,17α-diol;
7α-hydroxy-DHEA;
7β-hydroxy-DHEA;
4-androstenediol (androst-4-ene-3 β ,17 β-diol);
5-androstenedione (androst-5-ene-3,17-dione);
7-keto-DHEA;
19-norandrosterone;
19-noretiocholanone;
androst-4-ene-3α,17α-diol;
androst-4-ene-3α,17β-diol;
androst-4-ene-3α,17β-diol;
androst-5-ene-3α,17β-diol;
androst-5-ene-3α,17β-diol;
androst-5-ene-3β,17α-diol;
androsterone;
epi-dihydrotestosterone;
30 December 2016 OFFICIAL JOURNAL OF THE REPUBLIC OF FRANCE Text 18 of 223

Page | 96
epitestosterone;
etiocholanolone.
2. Other anabolic agents;
Including but not limited to:
Clenbuterol, selective modulators of androgen receptors (SARMs, e.g. andarine and ostarine), tibolone,
zeranol and zilpaterol.
For the purposes of this document:
<exogenous> means a substance that cannot ordinarily be produced naturally by the human body.
<exogenous> means a substance that cannot ordinarily be produced naturally by the human body.
S2. PEPTIDE HORMONES, GROWTH FACTORS, RELATED AND MIMETIC SUBSTANCES
The following substances, and other substances with similar chemical structure or similar biological effect(s),
are prohibited:
I. Agonists of the erythropoietin receptor:
1.1 Erythropoietin-stimulating agents (ESAs), e.g. darbepoetin (dEPO);
erythropoietin (EPO);
EPO-Fc;
GATA inhibitors, e.g. K-11706;
inhibitors of growth factor-β (TGF-β), e.g. sotatercept, luspatercept;
methoxy polyethylene glycol-epoetin beta (CERA);
peptides mimetic of EPO (EMP); e.g. CNTO 530 and peginesatide;
1.2. Non-(141-erythropoietic agonists of the EPO receptor, e.g.
ARA-290 ;
Asialo-EPO;
Carbamylated EPO;
2. Stabilisers of factors inducible by hypoxia (HIF), e.g. cobalt, molidustat and roxadustat (FG-4592); and
HIF activators, e.g. xenon and argon;
3. Chorionic gonadotrophin (CG) and luteinising hormone (LH) and their release factors, e.g. buserelin,
gonadorelin and leuprorelin, prohibited in male athletes only;
4. Corticotropins and their releasing agents, e.g. corticorelin;
5. Growth hormone (GHS) and its release factors including: growth hormone releasing hormone (GHRH)
and its analogues, e.g. CJC-1295, sermorelin and tesamorelin+growth hormone secretagogues (GHS), e.g.
ghreline and mimetic ghrelin, e.g. anamoelin and ipamorelin; growth hormone releasing peptides (GHRPs),
e.g. alexamoreline, GHRP-6, hecareline and pralmorelin (GHRP-2)
Additional prohibited growth factors:
Platelet-derived growth factor (PDGF); vascular endothelial growth factor
(VEGF); insulin-like growth factor-1 (IGF-1) and analogues thereof; hepatocyte growth factor (HGF);
fibroblastic growth factors. (FGF); mechanical growth factors (MGF) as well as any other influencing factor in
tendons or ligaments, protein synthesis/degradation, vascularisation, the use of energy, regenerative capacity
or change of fibre type.
S3. BETA-2 AGONISTS
All beta-2 selective and non-selective agonists, including all their optical isomers, are prohibited.
These include, without limitation:
Fenoterol; formoterol; igenamine; indacaterol; olodaterol; reproterol; salbutamol; salmeterol; terbutaline;
vilanterol.
Except for:
- inhaled salbutamol: maximum 1600 microgrammes per 24 hours, not exceeding 800 microgrammes per 12
hours;
- inhaled formoterol: maximum delivered dose of 54 microgrammes per 24 hours;
- inhaled salmeterol: maximum delivered dose of 200 microgrammes per 24 hours.
The presence of salbutamol in urine at a concentration exceeding 1,000 ng/mL or formoterol at a concentration
exceeding 40 ng/mL serum is presumed not to be intentional therapeutic use, and a concentration exceeding 40 ng/mL
must be presumed not to be intentional therapeutic use and will be considered an abnormal analysis result (AAR), unless the athlete proves, by a controlled
30 December 2016 OFFICIAL JOURNAL OF THE REPUBLIC OF FRANCE Text 18 of 223

Page | 97
pharmacokinetic study, that this abnormal result is indeed the consequence of using a therapeutic dose (by inhalation)
up to the maximum dose indicated above.
S4. HORMONAL AND METABOLIC MODULATORS
The following hormones and hormone modulators are prohibited:
1. Aromatase inhibitors, including but not limited to:
4-androstene-3,617-trione (6-oxo);
aminoglutethimide;
anastrozole;
androsta-1,4,6-triene-3,17-dione (androstatrienedione);
androsta-3,5-diene-7,17-dione (arimistane);
exemestane;
formestane;
letrozole;
testolactone.
2. Selective estrogen receptor modulators (SERMs), including but not limited to:
Ralexirene;
tamoxifen;
toremifen;
3. Other anti-estrogenic substances, including but not limited to:
Clonilfeme;
cyclofenil;
fulvestrant.
4. Agents which modify the function(s) of myostatin, including, but not limited to: myostatin inhibitors.
5. Metabolic modulators:
5.1PAM P(AMPK)-activated protein kinase activators, e.g. AlCAR and agonists of the peroxisome
proliferative 6 receptor agonist (PI’R6), e.g. GW 1516;
5.2 Insulins and mimetics of insulin;
5.3 Meldonium;
5.4 Trimetazidine.
S5. DIURETICS AND MASKING AGENTS
The following diuretics and masking agents are prohibited, as well as other substances possessing a similar
chemical structure or similar biological effect(s).
Including but not limited to:
- Desmopressin; probenecid; plasma substitutes, e.g. glycerol and intravenous administration of albumin,
dextran, hydroxyethyl starch and mannitol.
- Acetazolamide; amiloride; bumetanide; canrenone; chlortalidone; etacrynic acid; furosemide;
indapamide; metolazone; spironolactone; thiazides; e.g. bendroflumethiazide, chlorothiazide, and
hydrochlorothiazide; triamterene and vaptans, e.g. tolvaptan.
Except for:
- drospitenome; pamabrome and the ophthalmic administration of carbonic anhydrase inhibitors
(e.g. clorzolamide, brinzolamide,
- the local administration of felypressin in dental anaesthesia
The detection in the athletes’ sample, either continuously or in competition, if applicable, of any of the
following substances being subject to a threshold level: formoterol, salbutamol, cathine, ephedrine,
methylephedrine and pseudoephedrine, in conjunction with a diuretic or masking agent, will be considered an
abnormal analysis result (AAR). Unless athletes have a therapeutic use exemption (TUE) approved for this
substance, in addition to that obtained for the diuretic or masking agent.
PROHIBITED METHODS
M1. MANIPULATION OF BLOOD OR BLOOD COMPONENTS
30 December 2016 OFFICIAL JOURNAL OF THE REPUBLIC OF FRANCE Text 18 of 223

Page | 98
The following are prohibited:
1. The administration or reintroduction of any amount of autologous, allogeneic (homologous) or heterologous blood
or red blood cells of any origin into the circulatory system.
2. The artificial improvement of the consumption, transport or release of oxygen.
Including but not limited to:
Perfluorochemical products; efaproxiral (RSR113); and modified haemoglobin products, e.g. haemoglobin-based
blood substitutes and cross-linked haemoglobin products, but excluding oxygen supplementation by inhalation.
3. Any intravascular manipulation of blood or blood component(s) by physical or chemical methods.
M2. CHEMICAL AND PHYSICAL MANIPULATION
The following are prohibited;
1. Falsification or attempted falsification, in order to change the integrity and validity of the samples collected during
the doping control.
These include, without limitation:
The substitution and/or alteration of urine, e.g. proteases.
2. Intravenous infusions and/or injections of more than 50 mL per 6-hour period, except those legitimately received in
hospital admissions, procedures or clinical examinations.
M3. GENETIC DOPING
The following, having the potential to improve sporting performance, are prohibited:
1. Transfers of nucleic acid polymer or analogues of nucleic acid polymers;
2. The use of normal or genetically modified cells;
SUBSTANCES AND METHODS PROHIBITED IN COMPETITION
In addition to the categories S0 to S5 and M1 to M3 defined above, the following categories are prohibited in
competition:
PROHIBITED SUBSTANCES
S6. STIMULANTS
All stimulants, including all their practical isomers, e.g. d- and l- if appropriate, are prohibited.
Stimulants include:
a. Non-specified stimulants:
adrafinlil;
amfepramone;
amphetamine;
amphetaminil;
amiphenazole;
benfluorex;
benzylpiperazine;
bromantane;
clobenzorex;
cocaine;
cropropamide;
crotetamide;
fencamine;
fenethylline;
fenfluramine;
fenproporex;
fonturacetam [4-phenylpiracetam (carphedon)];
furenorex;
lisdexamfetamine;
mefenorex;
mephentermine;
30 December 2016 OFFICIAL JOURNAL OF THE REPUBLIC OF FRANCE Text 18 of 223

Page | 99
mesocarb;
methamphetamine (d-);
p-methylamphetamine;
modafinil; norfenfluramine;
phendimetrazine; phenterimine;
prenylamine;
prolintane; A stimulant that is not expressly named in this section is a specified substance.
b. Specified stimulants (examples):
4-methylhexan-2-amine (methylhexaneamine); benzgletamine;
cathine;
cathinone and its analogues, e.g. mephedrone, methedrone and a-pyrrolodlinovalerophenone;
dimethylamphetamine;
ephedrine;
epinephrine;
etamivan;
ethylamphetamine;
ethylephrine;
famprofazone;
fenbutrazate;
fencamfamine;
heptaminol;
hydroxyamphetamine (parahydroxyamphetamine);
isometheptene;
levnetamfetamine;
meclofenoxate;
methylenedioxymethamphetamine;
methylephedrine;
methylphenidate;
nicethamide;
norfenefrine;
octopamine;
oxilofrine (methylsynephrine);
pemoline;
pentetrazine;
phenethylamine and its derivatives;
phenmetrazine;
phenpromethamine;
propylhexedrine;
pseuodoephedrine;
selegiline;
sinutramine;
strychnine;
tenamfetamine (methylenedioxyamphetamine);
tuaminoheptane;
And other substances with a similar chemical structure or similar biological effect(s).
Except for: - clonidine - imidazole derivatives for topical/ophthalmic application and the stimulants included in the 2017 Monitoring Programme
* Bupropion, caffeine, nicotine, phenylephrine, phenylpropanolamine, pripadrol and synephrine: These substances are included in the 2017 Monitoring Programme and are not considered to be prohibited substances.
**Cathine: prohibited when its concentration in urine exceeds 5 microgrammes per millilitre.
***Ephedrine and methylephedrine: prohibited when their respective concentrations in urine exceed 10 microgrammes per millilit
30 December 2016 OFFICIAL JOURNAL OF THE REPUBLIC OF FRANCE Text 18 of 223

Page | 100
****Epinephrine (adrenaline): this is not prohibited for local use, e.g. nasal or ophthalmological or CO-administered
with local anaesthetics.
**** Pseudoephedrine: prohibited when its concentration in urine exceeds 150 microgrammes per millilitre.
S7. NARCOTICS
Prohibited:
buprenorphine;
dextromonimide;
diamorphine (heroin);
fentanyl and its derivatives;
hydromorphone;
methadone;
morphine;
nicomorphine;
oxycodone;
oxymorphone;
pentazocine;
pethidine.
S8. CANNABINOIDS Prohibited:
natural tetrahydrocannabinol (THC), e.g. cannabis, hashish and marijuana, or synthetics;
- Cannabimimetics, e.g. “Spice”, JWII-OIX, JWH-073» III -210.
S9. GLUCOCORTICOIDS
All glucocorticoids are prohibited when administered orally, intravenously, intramuscularly or rectally.
SUBSTANCES PROHIBITED IN CERTAIN SPORTS
P1. ALCOHOL
Alcohol (ethanol) is prohibited in competition only in the following sports. The detection will be performed by
ethylometry and/or blood analysis. The violation threshold is equivalent to an alcohol concentration of 0.10 g/L.
- Aeronautics (FAI);
- Automobile (FIA);
- Motorboating (UIM);
- Archery (WA).
P2. BETA-BLOCKERS
Beta-blockers are prohibited in competition only in the following sports and also prohibited outside of competition if
indicated.
- Automobile (FIA);
- Billiards (all disciplines) (WCBS);
- Darts (WDF);
- Golf (IGF);
- Skiing (IFS) for ski jumping, freestyle/halfpipe jumping and halfpipe/big air snowboarding;
- Underwater sports (CMAS) for dynamic apnoea with or without fins, free immersion apnoea,
constant weight apnea with or without fins, variable weight apnoea, Jump Blue apnoea, static apnoea,
underwater hunting and target shooting.
- Shooting (ISSF); IPC)*:
- Archery (WA)*.
* Also prohibited outside of competition
These include, without limitation:
acebutolol;
alprenolol;
atenolol;
betaxolol;
bisoprolol;
30 December 2016 OFFICIAL JOURNAL OF THE REPUBLIC OF FRANCE Text 18 of 223

Page | 101
bunolol;
carteolol;
carvedilol; celiprolol;
esmolol;
labetalol;
levobunolol;
metipranolol;
metoprolol;
nadolol;
oxprenolol;
pindolol;
propranolol;
sotalol;
timolol.
30 December 2016 OFFICIAL JOURNAL OF THE REPUBLIC OF FRANCE Text 18 of 223

Page | 102
Annex 2 – Decision-making algorithm in cases of hypocortisolaemia
Medical information to inform the decisions of the CAUT
ADRENAL INSUFFICIENCY
AI suspected
Severe pathology Less severe pathology
AI diagnosed/emerge
ncy care card - AI
AI undiagnosed response to
treatment
Blood sampling
Hydrocortisone, 100 mg, IV or
prednisone, 20 mg, IV
Evaluation of ACTH and pituitary function (e.g.
thyroid, gonads);
cerebral MRI
Disease history, clinical
examination
Basal cortisol
< 3.2 μg/dL 3.2-18 μg/dL > 18 μg/dL > 18 μg/dL 10-18 μg/dL < 10 μg/dL
Provocation test
Provocation test
Basal cortisol Yes
No
Absence of
AI
Cortisol >18 μg/dL Cortisol <18 μg/dL
Other
explanations? Cortisol <18 μg/dL Cortisol >18 μg/dL
Postponement of glucocorticoid therapy;
absence of AI history
Normal ACTH, cortisol
and DHEA-S levels Administration of hydrocortisone
for an additional 4 weeks
Initiation of hydrocortisone treatment at a triple dose;
early reduction to maintenance
dose
Other endocrine function tests (e.g. Synacthen,
ACTH, renin, intermediate steroid)
Secondary AI Low levels of ACTH and
renin
High levels of ACTH and renin
Primary AI
Absence of
antibodies Presence of
antibodies
Autoimmune
adrenalitis
Polyglandular
syndrome? Tomodensitometry
Very long-chain fatty acids
Special analyses (e.g.
intermediate steroids)
AI = adrenal insufficiency © WADA - World Anti-Doping Programme Version 3.1
April 2012

Page | 103
SaIivette - Instructions for use
The patient removes the swab from the Salivette (see
Figs. 1 and 2 ) …
… and replaces the stopper (see Fig. 5)
Centrifugation for 2 minutes at 1,000 x g yields a clear
saliva sample in the concical tube (see. Fig. 6)
… and places the swab in the mouth and chews it for
about 45 seconds to stimulate salivation (see Fig. 3)
Now the patient returns the swab with the absorbed
saliva to the Salivette (see fig. 4) …
l
Particles and mucus strands are collected in the specially
designed extended tip of the Salivette tube (see Fig. 7)
The closed insert containing the swab is then hygienically
disposed. The saliva recovered can now be used for
analysis (see Fig. 8)
IMMUNALYSIS
Annex 3 - Salivette® device for determining salivary cortisol
Insert pad into mouth

Page | 104
Annex 4 - Intercept devices for determining salivary cortisol
ORASURE... INTERCEPT
Intercept Oral Fluid Collection Device

Page | 105
Annex 5 - General information on the organisation of blood sampling by the MPCC and FCC for
2017 events
Determination of the plasma cortisol level
General information Organisation of blood sampling during 2017 events
- During the unexpected monitoring of the plasma cortisol level in competition, the blood samples are
taken by the biologists of the mandated laboratory,which is a member of the RBMI, approved by FFC/UCI.
- The samples are collected at the hotels of each GS at the earliest at 6.30 a.m. and at the latest at 9.00 a.m.
- It is not necessary to have fasted.
- The samples are taken by the laboratory itself under the conditions required by law. The collectors will
bring with them a mission letter signed by Dr. Armand MEGRET.
- The riders must:
o Present their licence to the sampler
o Provide the completed information sheet
-
- There is only one accredited laboratory per sampling day.
- The laboratory is different from the day and place of the race. All mandated laboratories are members of
the RBML and fulfil the same obligations of French law.
- On the day of sampling, the same machine will be used to perform the assay of the plasma cortisol level for
all riders.
- The results are transmitted in full by the expert physician (Dr. Armand MEGRET) on the same day to the
team physicians who transmits them to the riders.
- There is no standard lower threshold number. This depends on the machine and kit used.
Regardless of the machine used, it must be in conformity with the rules validated by the
accreditation and meets the legal obligations. In each case, the machine used must be specified as
well as the numbers of the lower and upper normal limits.
- There is no media communication. The assigned physician transmits the results of the riders only to the
physician of the team concerned.
- The chairman of the MPCC is informed if there is a contraindication and without specifying a number.
However, since only one parameter is measured, non-departure may in fact be related to this examination.
- Taking inhaled corticosteroids cannot prevent the contraindication decision. The fact that the
plasma cortisol level is low is the reason for the medical contraindication (biological adrenal
insufficiency with risk of decompensation) even if there is legal and justified taking of
corticosteroids.
- In the case of the plasma cortisol level being below normal (i.e. below the lower limit of the machine
which performed the examination), the rider will be told to take rest. The rider will not be allowed to
start of the next stage. The return to competition will occur after at least 8 days of rest, after
normalisation of the plasma cortisol level.
This operation is under the sole authority of Dr. Armand MEGRET, the national federal physician of the
French Cycling Federation, for samples taken in France,
The same provision (abnormally low plasma cortisol level at rest) is also valid for the biological
tests performed by the UCI.
This is a health surveillance measure. This is not an anti-doping control.
Possible situation:
Unannounced anti-doping tests may be initiated by the UCI/WADA and performed on the same morning
as those of the MPCC.
The UCI/WADA sampling is given priority. In this case, contact Dr. Armand MEGRET (+33 6 07 63 02 22)
to determine the appropriate course of action.
It must be avoided that two samples are taken from the same rider on the same day.
Organisation of sampling for plasma cortisol level determination 2017

Page | 106
Annex 6 - Pre-analytical questionnaire
MPCC Sampling for plasma cortisol level - 2017
Pre-analytical information sheet
- Name of rider:
- Forename:
- Licence number:
Team name:
Name of accompanying person:
Jet lag
Pro medications:
o Names:
.
.
.
o Route of administration (pomade, eyedrops, inhalation, tablet, injection)
.
o Posology
Place of sampling:
Sampling date:
Sampling time:
Name of laboratory:
Name of sampler:
Date and signature of rider:
Date and signature of sampler:

Page | 107
Annex 7 - Expert advice on dealing with biological adrenal insufficiency
Conduct in the case of biological adrenal insufficiency
FFC MPCC LNC
Prof. Martine DUCLOS, Prof. Yves LE BOUC & Dr. Michel GUINOT - France
Prof. Martine Duclos
University Professor, Hospital Practitioner. Endocrinologist,
Professor of Physiology (University of Auvergne), Head of Department: Department of Sports Medicine
and Functional Explorations, UHC G. Montpied, Clermont-Ferrand
Member of the Medical Committee of the French National Olympic and Sports Committee, French Anti-
Doping Agency: member of the Foresight Committee, member of the Pre-targeting Committee,
member of the list committee WADA AFLD AFSSAPS:
Update on the “Use of glucocorticoids in athletes with traumatic, allergic, infectious or cutaneous
pathologies: state of affairs and measures to be taken”, validated by the National Marketing
Authorisation Committee on 10 April 2008 (collective expert appraisal).
Prof. Yves Le Bouc
University Professor, Hospital Practitioner. Endocrinologist, Paediatrician, Professor of Physiology (Paris
IV) Head of Department: Endocrine Functional Exploration Laboratory, Hôpital Armand Trousseau,
APHP
Director of team 4 “IGF System” at the St-Antoine research centre, INSERM Unit 938 Chairman of the
Scientific Orientation Council of the French Anti-Doping Agency
Corresponding member of the French Academy of Medicine.
Dr. Michel Guinot
Rheumatologist and Physiologist, Hospital Practitioner at UHC of Grenoble
Head of the Medical Doping Prevention Unit, Rhône Alpes Medical Unit Sports & Pathologies, Clinic for
Physiology, Sleep, Exercise - Locomotion, Rehabilitation Physiology Centre.
To
Dr. Armand MEGRET
Fédération Française de Cyclisme
5, rue de Rome
93560 ROSNY SOUS BOIS
20 September 2013
Dear National Federation physician, dear colleague.
You have requested our expertise on the importance of regulatory plasma cortisol measurement in competitors
for the screening of the consequences of the use of glucocorticoids on adrenal function, the health risks to
which athletes could be exposed and the medical decisions that can be recommended when biological adrenal
insufficiency is found.

Page | 108
Conduct in the case of biological adrenal insufficiency FFC MPCC LNC
Regarding screening of the impact of the use of glucocorticoids on adrenal function
The data from the scientific literature clearly shows that, whatever the mode of administration of a glucocorticoid (by general or local route), there is systemic passage which may cause a decrease in the physiological secretion of cortisol by the adrenal glands, essentially by a hypothalamic and pituitary reverse-inhibition mechanism. This effect is probably proportional to the administered dose of the glucocorticoid, but there are probably individual susceptibilities explaining severe cases of adrenal function in low systemic passages.
The demonstration of the partial or total blockage of cortisol secretion (adrenal insufficiency) is ideally based on a pharmacological stimulation test of the hypothalamic-pituitary-adrenal axis. For practical reasons, it is not possible to perform this type of test in competitions in asymptomatic subjects. Therefore, the simple quantitative analysis of plasma cortisol in the morning, when its concentration is physiologically highest, makes it possible to detect the most fundamental biological adrenal insufficiencies, even if it does not make it possible to screen all of them.
1 2 3 De plus, le chiffre retenu comme anormalement bas est en dessous des bornes
inférieures du laboratoire (moyenne moins 2 déviations standards).
With regard to the sampling conditions, in particular the time of sampling, it is important to specify that cortisol is naturally secreted in a circadian rhythm. Thus, its plasma concentration also varies according to a sleep-waking rhythm. It will be lowest in the early night and maximum on waking. The interpretation of cortisol must therefore take into account the sleeping rhythm of the subject, since the rate of secretion can be reversed in athletes who work at night or who have experienced jet lag. Ideally, the measurement of plasma cortisol should be at the time when it has its highest value. Thus, the sampling times recommended
7 by the regulation of your federation seem well suited to athletes who usually
have a “standard” sleep-waking rhythm.
Regarding the health risks linked to adrenal insufficiency:
The demonstration of a plasma cortisol concentration below the standards of the kit used by the laboratory reflects a biological adrenal insufficiency. This is the consequence in athletes of the administration of a synthetic glucocorticoid, whatever its mode of administration, and regardless of how it was obtained (presence or absence of a medical prescription)
4.
This biological situation corresponds to a situation where the body is unable to respond adequately to severe stress (anaesthesia for surgery, bacterial infection, haemorrhagic shock, major trauma). Indeed, these situations require that the adrenal glands secrete an increased quantity of cortisol, an essential hormone for metabolic and cardiovascular adaptations for the survival of the body.
1 Numbers based on data from the literature are detailed in the guidelines of the medical regulations of the FFC 2 6.30 to 9.00 a.m. 3 There are other causes of adrenal insufficiency, the incidence of which is low, generally occurring in a known pathological context

Page | 109
Prof. Martine Duclos Prof. Yves Le Bouc
Dr. Michel Guinot
Conduct in the case of biological adrenal insufficiency FFC MPCC LNC
Thus, when this response is deficient (acute adrenal insufficiency), the prognosis can be life-threatening, even
in an a priori healthy subject. The few studies that have identified these cases show a high morbidity rate or
even mortality.
It is difficult to estimate the real frequency of acute adrenal insufficiency after corticosteroid therapy, as there
is no systematic declaration of this complication at the pharmacovigilance centres and/or there are gross forms. It is likely that its incidence is low, but glucocorticoids are prescribed very frequently in general
medicine as in sports medicine.
Regarding medical decisions for athletes:
As stated above, an athlete with a biological adrenal insufficiency runs a risk of life-threatening cardiovascular
or metabolic stress, even if this is rare.
Cycling, in particular in road races, is a sport with a high trauma risk, with the possibility of haemorrhagic
fracture or requiring surgery; therefore, it seems relevant that the French Cycling Federation’s regulation
provides medical solutions to reduce the risk of acute adrenal insufficiency.
Thus, the establishment of the dose of cortisol before the start of competitions or during the medical follow-up
seems well adapted to identifying the subjects at risk.
The systematic declaration of recent glucocorticoid treatments by riders or their entourage also seems to be
desirable. We note that when general corticosteroid therapy or by infiltration is prescribed, it corresponds to a
state of health which requires a rest from sporting practice to allow healing.
Finally, the decision to declare a contraindication by the federal physician is one of the possibilities even if other solutions can be proposed in competitions where medical assistance is provided.
We hope to have fulfilled your expectations.
Yours sincerely,
4 It is possible that malaise in the course of exertion sometimes leads to unexplained underperformance or abandonment that may be manifestations of gross adrenal insufficiency.

Page | 110
PROF. MARCO BONIFAZI PHYSIOLOGY ASSOCIATE UNIVERSITÀ DEGLI STUDI Dl SIENA SPECIALIST IN SPORTS MEDICINE VIALE VITTORIO EMANUELE II, 28 53100 SIENA Sienna, 21 August 2015, Dear Dr. Megret, I have read the documents you have sent me with great interest. I must say that I fully share your viewpoint with regard to the risks of provoking an inhibition of the hypothalamic-pituitary-adrenal axis following the ingestion of exogenous corticosteroids for whatever reason. The report of the French colleagues, Professors Martine Duclos and Yves Le Bouc and Dr. Michel Guinot, is perfectly correct in this respect. I would also like to point out that such an inhibition, even if modest and without any risk to athletes’ health, can change the systemic response to stressors caused by training and thus limit the adaptation to the workloads necessary to improve performance. Therefore, in addition to being aware of the risks, athletes and coaches must also be aware that their exertions during training can be impaired by the ingestion of exogenous corticosteroids. Consequently, in all cases, their intake must be considered only when absolutely necessary, and the intensity of training must be reduced for an appropriate length of time adapted to the duration of the therapy. It is necessary to identify reference values using statistical criteria to protect the health of athletes, by prohibiting them from participating in competitions in the event of the detection of abnormally low cortisol levels.

Page | 111
Conduct in the case of biological adrenal insufficiency FFC MPCC LNC
Annex 1 to the extract from the Federal Medical Regulations of the French Cycling Federation, on page 12, indicates the reference values for cortisol in plasma in samples collected on an empty stomach between 7:30 a.m. and 9:00 a.m. The mean cortisol value was 147 ± 40 pg/L (400 ± 109 nmol/L). The mean value minus 2 standard deviations gives a cortisol value of 67 pg/L, below which the risk of adrenal insufficiency is high and is therefore a contraindication due to the agonistic activity. At the same time, the data in the scientific literature indicates normal adrenocortical function in cyclists ranging from 180 to 226 pg/L which, in my opinion, is a fairly narrow range. In this regard, and since this is not explicitly described in the document, I would like to know whether the reference values you indicate come from cyclists and, if so, under what training conditions. I am pleased to inform you that, in 2009 and 2010, the Italian Cycling Federation collected blood samples subjected to cortisol analysis from more than 300 cyclists participating in the GiroBio. In order to obtain the optimal reference values, samples were collected before, during and after the end of the race. The GiroBio is a race reserved for the category of cyclists under 27 years and it has similar validity to the amateur Tour of Italy, being divided into nine stages (one time trial) over 10 days. During the entire race, according to the innovative organisation and management model used for this race, all riders slept in similar accommodation, received an identical diet (around 5,700 kcal per day per cyclist), standardised medical care and food supplements between
meals, according to the health and safety rules established by Italian law. In conclusion, the same medical team monitored all cyclists. To be allowed to participate, cyclists and team members must be committed to respecting the organisational model of the race, any violation of the rules of the race being penalised by disqualification of cyclists and/or the team. It could be possible to compare the cortisol values obtained from the samples collected by the Italian Cycling Federation under the responsibility of Dr. Luigi Simonetto to those in your possession so as to better define the benchmark values for well-trained elite cyclists for a stage race. If you deem it appropriate, we could exchange the results of the samples analysed for cortisol over the years, with strict observance of the confidentiality and data processing requirements, with the aim of improving the measures to protect the health of cyclists. I look forward to your reply. Best regards,
Marco Bonifazi

Page | 112
Conduct in the case of biological adrenal insufficiency FFC MPCC LNC
Dr. Jonathan G. OWNBY USA
English version
Dr. Jonathan G. OWNBY, MD
Specialist in endocrinology, diabetes and metabolism
On Wed. Apr 1. 2015 at 12:55 PM, Jonathan OWNBY wrote:
1 * / What is the impact of the use of glucocorticoids in the passage in the blood?
1 performed a literature review and there is evidence that short burst of glucocorticoids can improve athletic
performance thus it could be used for performance enhancement.
2 * / is there an acute medical risk and therefore risk of serious accident or stress?
There is true and serious risk if glucocorticoids are used even in the short term as athletes would need to cycle
on and off of the steroid and this could lead to partial or complete adrenal insufficiency (Al). This is a serious
medical condition and is potentially life threatening as glucocorticoids act like cortisol, which is your bodies
stress hormone. When someone takes exogenous glucocorticoids, this suppresses the adrenal gland from
making glucocorticoids. A lack of cortisol could lead to hyponatremia (low sodium and potentially altered mental
status), severe nausea/vomiting, and the inability to deal with medical or physical stress which may in turn lead
to death. Long term, continued use will also lead to weakened bones, thus a crash could lead to fracture.
3 * / action to take is a contraindication for the practice of sport?
The recommendation to only check an AM cortisol is lacking. The article provided is correct in that cortisol is
released in a circadian rhythm with higher values in the morning and a decline does occur during the day but there are caveats. Studies of shift workers show that circadian rhythms reverse in persons working all night and
sleeping during the day. This would correlate to a pro athlete just arriving in a county 12 time zones from their
home (this also leads to jet lag). An athlete who has arrived for a race a few days prior to a race may not have
a circadian rhythm consistent with an 8* 9AM local time lab draw and it may take weeks for their rhythm to
completely adjust (this would lead to a false positive per French recommendations). Furthermore, some
glucocorticoids cross react with the cortisol assay thus someone could be abusing prednisone or hydrocortisone
and their AM cortisol could be normal or even elevated instead of being low. I would suggest that if a screening
test comes back abnormally high or low that a serum synthetic glucocorticoid screen be performed as this
would detect any common synthetic glucocorticoid use. It may take some time for this lab to result, so it could be stated that an athlete abusing glucocorticoids is responsible for any events that lead to injury due to use and
if a synthetic screen returns positive, the athlete is disqualified.
Dr. Jonathan G. OWNBY USA
French version
Dr. Jonathan G. OWNBY
Spécialiste endocrinologie, diabète et métabolisme Atlanta
Le mercredi 1er avril 2015 à 12:55, Jonathan OWNBY a écrit :
1 * / Quelle est l’incidence des glucocorticoïdes, en termes de passage dans le sang ?

Page | 113
Conduite a tenir devant une insuffisance surrénalienne biologique
FFC MPCC LNC
J’ai effectué une revue de la littérature qui apporte la démonstration que l’administration aigu de
glucocorticoïdes peut améliorer la performance athlétique. Ils peuvent donc utilisés a des fins ergogénes.
2* /Existe-t-il un risque médical aigu, et donc un risque d’accident grave ou de stress ?
Le risque de l’utilisation des glucocorticoïdes est réel et sérieux, meme sur une courte période. Quand les
cyclistes doivent faire un effort: (pendant ou apres l’administration de glucocorticoïdes), cela peut entrainer
une insuffisance surrénale partielle ou totale. Cette affection est grave et potentiellement mortelle car l’action
des glucocorticoïdes est analogue a celle du cortisol, l’hormone du stress synthetisée par l’organisme.
Lorsqu’une personne prend des glucocorticoïdes exogenes, ceux-ci bloquent la production de l’ACT-I
hypophysaire, régulateur stimulateur des glucocorticoïdes par les glandes surrénales. Le manque de cortisol
peut alors provoquer une hyponatrémie (faible taux de sodium et risque d’altération de l’état psychique), des
nausées/vomissements severes et l’incapacité de faire face au stress médical ou physique, ce qui peut
entrainer le déces. En outre, l’utilisation prolongée affecte le tissu osseux, ce qui augmente le risque de
fracture en cas de chute.
3 / La conduite a tenir est-elle la contre-indication lors de la pratique sportive ?
La recommandation de ne controler le cortisol que le matin est insuffisante. L’article fourni a raison sur le fait
que le cortisol est secreté selon un rythme circadien, c’est-a-dire que son taux est plus elevé le matin et
diminue progressivememt au cours de la journée. Toutefois, des mises en garde sont nécessaires. Les études
menées sur des personnes travaillant en équipe de quart montrent que le rythme circadien s’inverse chez les
travailleurs de nuit qui dorment durant la journée. Ce profil serait observe chez un sportif professionnel qui
arriverait dans un endroit eloigné de son domicile de 12 fuseaux horaires c’est ce qui conduit au décalage
horaire (“jet lag”). Cependant, un sportif arrivant quelques jours avant une course, n’a pas eu le temps
d’avoir un rythme circadien qui correspond a l’horaire local du prélevement de 8-9 h du matin. En effet,
l’ajustement de son rythme peut prendre plusieurs semaines (ce qui entrainerait un faux positif au regard des
recommandations françaises). En outre, certains glucocorticoïdes ont des reactions croisées avec le kit de
dosage du cortisol, de sorte qu’une personne abusant de prednisone ou d’hydrocortisone (cortisol exogene)
pourrait avoir un taux de cortisol matinal normal ou élevé alors qu’il devrait etre bas. Je suggérais, si un test
de depistage donne un résulat anormalement elevé ou bas, de réaliser la recherche de glucocorticoïdes de
synthese sur un échantillon de sérum. Les résultats de cet examen étant un peu longs a obtenir, il pourrait
etre établi qu’un athlete ayant une consommation abusive de glucocorticoides soit responsable de tout
évenement entrainant des blessures en raison de cette consommation et si le résultat du dépistage est positif,
l’athlete serait alors disqualifié

Page | 114
Conduite a tenir devant une insuffisance surrénalienne biologique FFC MPCC LNC
Prof. Kerstin BRISMIAR Swedish
French
Vidarebefordrat brev :
Fran: Kerstin Brismar <[email protected]
Datum: 6 november 2015 15:54:16 CET
Till: ‘Lykka Tarnrn’ <[email protected]>
Amnia: RE: VB: expert endocrinologie et sport
Hej Lykke,
Har kornmer mitt forsok till star pa fragorna:
1) What is the impact of the use of glucocorticoids (passage into blood)?
A peak of cortisol may improve performance, but the intake of exogenous glucocorticoids blocks the secretion
of cortisol stimulated by endogenous ACTH, which means that, after a prolonged period of use, endogenous
corticosteroid inhibition occurs and is likely to be harmful to health. The restoration of normal cortisol production
may take several days or even several weeks in the case of the long-term use of exogenous
glucocorticosteroids.
Glucocorticosteroids circulate in plasma through the use of cortisol-binding globulin (CBG). In case of low CBG,
the total plasma cortisol level may appear to be falsely low, whereas free cortisol can be normal. Exogenous
glucocorticoids can lead to low and elevated levels of cortisol in the plasma, depending on the medication
taken.
2) Is there an acute medical risk and therefore a risk of a severe accident or stress?
The acute risk associated with stopping glucocorticoid therapy depends on the length of treatment. Long-term
treatment may induce adrenal insufficiency, so glucocorticoid insufficiency in this situation may lead to
hypotension, hypoglycaemia and induce acute adrenal insufficiency, in particular after muscular exertion that
can lead to a life-threatening risk. High concentrations of glucocorticoids can cause electrolyte imbalance,
hyperglycaemia, muscle weakness and high blood pressure.
3) Is the appropriate measure to be taken to contraindicate sporting practice?
In Sweden, we recommend an additional examination of the corticotropic axis if the morning blood cortisol level
after fasting is lower than 200 nmol/L. I would recommend avoiding sporting practice before the additional
examination has been performed. I agree with Dr. Jonathan Ownby that, if the screening test indicates a low or
high level of cortisol, the search for synthetic glucocorticoid intake must be performed on the serum. This can
be quite lengthy, and therefore, to accelerate this search, it is possible to measure other parameters of adrenal
function in serum, such as electrolytes (potassium (K) and sodium (Na)), aldosterone and DHEA sulphate as
well as ACTH.
Kind regards,
Kerstin Brismar
Trevlig helg halsar Kerstin
Kerstin Brismar, Ph.D.
Professor in Diabetes Research
Karolinska Institute
Department of Molecular Medicine and Surgery
RGIf Luit Research Center or Diabetes and Endocrinology
Karolinska University Hospital, Solna, L1;00.
171 76 Stockholm

Page | 115
AUTHORISATION TO PRINT
*******
Thesis to obtain the State Diploma of Doctor of Medicine
Presented by: Samuel MARAFFI
Born on: 13 July 1998 in: Vesoul
With the title:
Hypocortisolaemia in athletes: focus on causes and risks incurred
Read. Read and approved,
Besançon, 14/03/2017 Besançon, 11 Mar 2017
The Chairman of the Thesis Jury,
The Director of UFR SMP,
Prof. Thierry MOULIN
Medical Biology Laboratory PC BIO
Dr. G. DUMOULIN PU-PH
MEDICAL BIOCHEMISTRY CHRU de Besançon – 2 boulevard
Fleming 25030 Besançon cedex
Tel. 03 70 63 21 11 E-MAIL: [email protected]
Note: The Director of UFR SMP cannot be held responsible for the ideas and remarks defended in this thesis.
UFR SMP 19 rue Ambroise Paré F-25030 Besançon cedex – Tel. +33 (0)3 63 08 22 00 – Fax +33 (0)3 81 66 56 83
http://medecine-pharmacie.univ.fcomte.fr
Medical & Pharmaceutical Sciences UNIVERSITÉ DE FRANCHE-COMTÉ

Page | 116
SUMMARY
Surname - Forename: MARAFFI Samuel
Thesis defended on: Tuesday, 04 April 2017
Thesis title:
Hypocortisolaemia in athletes: focus on causes and risks incurred
Summary:
Hypocortisolaemia in athletes, a sign of adrenal insufficiency, constitutes a major health problem. Many
international experts agree that the practice of sport and its potentials risks (falls, trauma, etc.) represent
an additional risk of entering acute adrenal insufficiency. Screening for it is therefore of primary
importance. Salivary cortisol is a practical and reliable method, but it needs to be standardised and
analysed. Physical activity or over-training do not appear to lead to hypocortisolaemia. The use of
exogenous glucocorticoids is the leading cause of hypocortisolaemia. As illustrated by the data of the
French Cycling Federation, this literature review finds a notable influence of inhaled intra- or periarticular,
intramuscular, intradermal, and subcutaneous corticosteroids on adrenal function, which is more variable
for dermocorticoids, and is limited for intranasal corticosteroids and eyedrops. This data therefore
encourages great caution in use, and a greater consideration of the risks to athletes of corticosteroids,
which have potentially serious consequences for health in the case of corticotropic insufficiency.
Keywords: hypocortisolaemia, corticotropic axis, sport, exogenous glucocorticoids
I UFR SMP 19 rue Ambroise Paré F-25030 Besançon cedex I Tel. +33 (0)3 63 08 22 00 I Fax +33 (0)3 81 66 56 83 I http://medecine-pharmacie.univ-fcomte.fr
Medical & Pharmaceutical Sciences UNIVERSITÉ DE FRANCHE-COMTÉ