Embed Size (px)
Citation preview

1
Hyphema & Treatment RegimentHyphema & Treatment Regiment
Strict bed rest for at least 4 daysStrict bed rest for at least 4 days
Head elevated at 30 degreesHead elevated at 30 degrees
Pred Forte QIDPred Forte QID
CycloplegicCycloplegic
Mild analgesicMild analgesic
AmicarAmicar——forms clots fasterforms clots faster
Antiemetic may be neededAntiemetic may be needed
Manage elevated IOPManage elevated IOP’’ss–– b-blockers, alpha- b-blockers, alpha-agonistsagonists
Hyphema DoHyphema Do’’s and Dons and Don’’tsts
DonDon’’t perform gonioscopy initiallyt perform gonioscopy initially
Do take pressures by Do take pressures by applanationapplanation
-expect low immediately after the-expect low immediately after the
injury injury
-IOP remains low until CB regains-IOP remains low until CB regains
function, uveitis sets in or function, uveitis sets in or
secondary bleed secondary bleed
-can be a very difficult glaucoma to-can be a very difficult glaucoma to
manage manage
Never take pressures by digital Never take pressures by digital applanationapplanation
Do not perform scleral depression Do not perform scleral depression
Hyphema: DoHyphema: Do’’s and Dons and Don’’tsts
No aspirin useNo aspirin use
Do quantitate the amount of theDo quantitate the amount of thehyphemahyphema
Do see patient on a daily basis untilDo see patient on a daily basis untilresolutionresolution
Do inform patients to returnDo inform patients to returnimmediately for reevaluation if thereimmediately for reevaluation if thereis sudden pain or decreased visionis sudden pain or decreased vision
Do not patchDo not patch
Rebleed HyphemasRebleed Hyphemas
Tend to be much worse than primaryTend to be much worse than primary
bleedsbleeds
Viscous cycleViscous cycle
Consider the risk factors of bloodConsider the risk factors of blood
disordersdisorders
HEY!! What about ourHEY!! What about our
friend the Retina??friend the Retina??
Posterior Segment DamagePosterior Segment Damage
Results from impact over the scleraResults from impact over the sclera
or shock wavesor shock waves

2
Posterior Segment DamagePosterior Segment Damage
Macular edemaMacular edema
Commotio retinaeCommotio retinae
Choroidal rupturesChoroidal ruptures
Evulsion of theEvulsion of theoptic nerveoptic nerve
Retinal tearsRetinal tears
Retinal dialysisRetinal dialysis
VitreousVitreoushemorrhagehemorrhage
Flashes and FloatersFlashes and Floaters
FlashesFlashes
HistoryHistory
–– What do they look like? Sparkles, flashWhat do they look like? Sparkles, flash
bulb, streaks?bulb, streaks?
–– When do you notice them most?When do you notice them most?
Evening, anytime, before onset of HA?Evening, anytime, before onset of HA?
–– Do you see floaters? Any change in sizeDo you see floaters? Any change in size
or number?or number?
–– Previous history of retinal tear or break?Previous history of retinal tear or break?
FloatersFloaters
HistoryHistory
–– New onset? How many? Which eye?New onset? How many? Which eye?
Describe them. Flashes? Any change inDescribe them. Flashes? Any change in
vision?vision?
Differential DiagnosisDifferential Diagnosis
Acute PVDAcute PVD
Acute retinal breakAcute retinal break
Ocular migraineOcular migraine
Posterior or Intermediate uveitisPosterior or Intermediate uveitis

3
Acute PVDAcute PVD
May have associated vitreousMay have associated vitreous
hemorrhage or disc hemorrhagehemorrhage or disc hemorrhage
Symptoms Symptoms Floaters, Floaters, ““cobwebscobwebs””,,
blurred vision, move with eyeblurred vision, move with eyemovementsmovements
Documented scleral depressionDocumented scleral depression
SchafferSchaffer’’s signs sign
Follow up DFE in 4-6 weeksFollow up DFE in 4-6 weeks
4
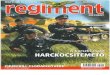
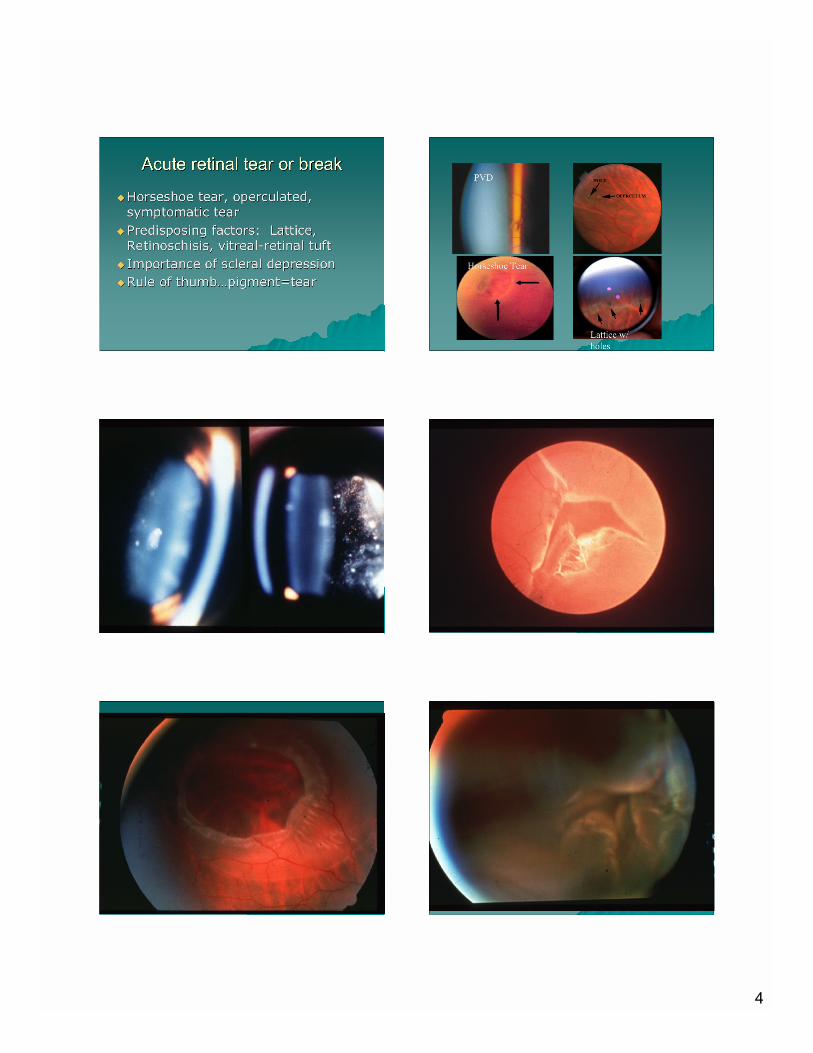
Acute retinal tear or breakAcute retinal tear or break
Horseshoe tear, operculated,Horseshoe tear, operculated,
symptomatic tearsymptomatic tear
Predisposing factors: Lattice,Predisposing factors: Lattice,
Retinoschisis, vitreal-retinal tuftRetinoschisis, vitreal-retinal tuft
Importance of scleral depressionImportance of scleral depression
Rule of thumbRule of thumb……pigment=tearpigment=tear
PVD
Horseshoe Tear
Lattice w/
holes

5
Ocular migraineOcular migraine
Usually last 15-30 minutes, mostly femaleUsually last 15-30 minutes, mostly female
(60-70%)(60-70%)
Transient swirls, colors, wavesTransient swirls, colors, waves
Throbbing head pain, nausea, photophobiaThrobbing head pain, nausea, photophobia
Termed a classic migraine when HATermed a classic migraine when HA
followsfollows
Triggers: caffeine, chocolate, red wine,Triggers: caffeine, chocolate, red wine,
birth control, menopause, hormones,birth control, menopause, hormones,
fatigue, stress, refractive errorfatigue, stress, refractive error