Embed Size (px)
Citation preview

Thorax (1974), 29, 713.
Hypertrophic cardiomyopathy and hyperthyroidism:a report of three cases
C. SYMONS, P. J. RICHARDSON,and 0. FEIZI
Department of Cardiology, Royal Free Hospital, London NW3 2QG
Symons, C., Richardson, P. J., and Feizi, 0. (1974). Thorax, 29, 713-719. Hypertrophiccardiomyopathy and hyperthyroidism. The combination of hypertrophic cardiomyopathyand hyperthyroidism gives rise to a complex clinical picture as some of the symptoms
and signs may be common to both conditions. The presentation and investigation ofthree patients are reported. In one patient there was evidence of progression from thehypertrophic obstructive phase to that associated with loss of outflow tract obstruction.The echocardiogram was especially useful in assessing the presence or absence ofhypertrophic disease in the thyrotoxic subject. It is suggested that the long continuedhigh-output circulatory state in clinically undetected hyperthyroidism may prove to
be a stimulus for unrestrained cardiac muscle hypertrophy.
Three patients are described, each of whom, atone time, had evidence of both hypertrophic car-diomyopathy and hyperthyroidism. Although theassociation of the two conditions may be fortu-itous, the combination has not previously beenreported, and the symptoms and signs pose prob-lems in diagnosis which merit discussion. Inaddition, the extra work-load inherent in themaintenance of the hyperkinetic circulation inthyrotoxicosis might have some bearing on theaetiology of hypertrophic cardiomyopathy. Abnor-mal echocardiograms were recorded in each, andthis technique proved a useful and simple methodof screening these thyrotoxic patients when car-diomyopathy was suspected and prior to moredetailed investigation by cardiac catheterizationand angiography.
CASE REPORTS
PATIENT 1. A 38-year-old woman was referred to thecardiac clinic in 1958 because of a murmur. This hadbeen noted by the general practitioner in 1956 buthad not previously been commented upon at earlierroutine examinations. Clinically an anxious womanof average build, the only physical abnormality wasa grade 3/4 mid-to-late apical systolic murmur whichceased before the second sound. The blood pressurewas 130/80 mmHg. The chest radiograph was normal.The electrocardiogram revealed sinus rhythm, frontalplane QRS axis -15°, a small Q in aVF, PR interval0-12 sec. In 1959 she had attacks of paroxysmal supra-
ventricular tachycardia, and a year later chest painand shortness of breath on exertion occurred. In1961 the electrocardiogram showed a pre-excitationtype B pattern, PR interval 0-08 sec, frontal planeQRS axis +10° (repeated records remained almostidentical henceforward). There was no alteration inthe physical signs in the cardiovascular system buthyperthyroidism was suspected because of undueanxiety, tachycardia, and a small midline thyroidnodule. However, relevant investigations were negative(BMR 9%, 1'I thyroid uptake 25% at 4 hours and50% at 48 hours).The patient was followed up routinely and in 1968
typical thyrotoxicosis developed, thyroid enlargementbecoming more obvious, although there were no eyesigns. The diagnosis was confirmed with thyroid func-tion studies (protein-bound iodine 9-5 and 11 2 ,ug/100 ml, 13'I thyroid uptake 68 % at 4 hours). A subtotalthyroidectomy was performed and histology showeda multinodular goitre with areas of epithelial hyper-plasia and absorption of colloid.The patient improved but the following year
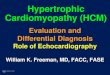
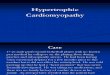
developed palpitations and attacks of paroxysmalnocturnal dyspnoea, necessitating full cardiac investi-gation. The chest radiograph revealed left ventricularenlargement, the electrocardiogram was unaltered,and an echocardiogram was abnormal (Fig. 1), show-ing a prominent forward systolic displacement of theanterior mitral valve leaflet together with a reduceddiastolic closure rate and evidence of a thickenedseptum. At cardiac catheterization the left ventricularpressure was 240/20 mmHg and there was an intra-ventricular systolic gradient of 140 mmHg; there was
713
copyright. on N
ovember 13, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.29.6.713 on 1 N
ovember 1974. D
ownloaded from

C. Symons, P. J. Richardson, and 0. Feizi
1
FIG. 1. PATIENT 1. Echocardiogram showing abnor-mal systolic forward displacement (arrowed) of theanterior mitral valve leaflet (AM), prominent inter-ventricular septal echoes (IVS), and closure of mitralvalve during mid-diastole (E,F).
no systolic gradient across the aortic valve. A leftventricular angiocardiogram showed obliteration ofthe distal part of the left ventricular cavity withsevere septal hypertrophy and mitral incompetence.
Despite medical treatment the patient deteriorated,cardiac surgery was considered, and eventually aresection of muscle from the left ventricular outflowtract was performed. At operation there was markedthickening of the left ventricular wall with additionalhypertrophy of the whole of the septum as far as
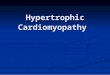
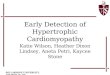
the aortic valve. There was no localized stenosis andno abnormality of the mitral valve. The patient dieda few hours after operation. A myocardial musclebiopsy taken at operation revealed classical changesof hypertrophic obstructive cardiomyopathy (Fig. 2).Necropsy showed that there was no coronary arterydisease, no intrinsic mitral leaflet abnormality, andno cardiac infarct. The small coronary vessels were
normal; no microscopic examination of the con-
ducting tissue was made.
PATIENT 2. In March 1969 a woman aged 53 was
admitted with acute left ventricular failure consideredto be due to non-rheumatic mitral incompetence.There was no previous relevant history of cardiacdisease; pernicious anaemia had been diagnosed in1956, for which regular B12 injections were given.The protein-bound iodine was raised, 8-9 ug/l00 ml,
but no further investigations were carried out. InAugust 1969 she complained of weight loss, anxiety,orthopnoea, and palpitation and expressed a pre-ference for cold weather. Examination revealed a thinanxious woman with a palpable thyroid gland, handtremor, and palmar erythema; tachycardia waspresent. There were no eye signs. The pulse was offull volume with a rapid upstroke, the blood pressurewas 120/80 mmHg, there was evidence of left ventri-cular hypertrophy, and a grade 3/4 late apical systolicmurmur was audible. The chest radiograph was nor-mal but the electrocardiogram showed evidence ofmoderate left ventricular hypertrophy, frontal planeQRS axis of 00. Thyroid function tests confirmedthyrotoxicosis (protein-bound iodine 9-6 ,ug/100 ml,T3 resin uptake 121%, thyroxine iodine raised,'"I thyroid uptake 56% at 4 hours and 54% at 48hours).The patient improved with carbimazole but as the
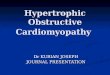
murmur remained loud detailed cardiac investigationwas carried out. The echocardiogram (Fig. 3) showeda small forward systolic displacement of the anteriormitral valve leaflet with a normal diastolic closurerate. There was evidence of gross septal hypertrophy.At catheterangiography the left ventricular pressurewas 160/14 mmHg, there was septal and papillarymuscle hypertrophy, and a moderate degree of mitralregurgitation completed the picture of hypertrophiccardiomyopathy (Fig. 4). When the patient becameeuthyroid repeat angiography and echocardiographyshowed no changes in the features of hypertrophiccardiomyopathy, although the electrocardiogram hadbecome normal.The patient had improved after 18 months of
medical treatment but when this was stopped relapseoccurred and radio-iodine was administered. To dateher general condition is good, although the murmur isstill loud and the systolic forward displacement of themitral valve is still evident in the echocardiogram.
PATIENT 3. In 1956, thyrotoxicosis was diagnosed ina 32-year-old woman who was treated with carbi-mazole and thyroid extract for four years. An electro-cardiogram had shown occasional sino-atrial blockand established second-degree atrioventricular blockwith Wenckebach phenomenon. The chest radiographshowed cardiac enlargement. She responded well tothe antithyroid treatment, but in 1966, while inHolland, a saddle embolism occurred during an epi-sode of atrial fibrillation, and bilateral femoral arterialembolectomy was performed. Postoperatively thepatient had a thyrotoxic crisis. Treatment with car-bimazole was re-instituted and improvement was rapid.It was thought that an apical mid-to-late systolic mur-mur was due to rheumatic mitral disease but in retro-spect the accompanying carotid arterial trace (Fig. 5)appeared identical with that frequently recorded inhypertrophic obstructive cardiomyopathy. The patientwas first seen at the Royal Free Hospital in 1968 whenher general condition indicated an euthyroid statewith exophthalmos. No cardiac murmurs or abnormal
714
copyright. on N
ovember 13, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.29.6.713 on 1 N
ovember 1974. D
ownloaded from

Hypertrophic cardiomyopathy and hyperthyroidism: a report of three cases
FIG. 2. PATIENT 1. Left ventricular muscle showing characteristic changes of hypertrophic cardiomyopathy, viz, directionaldisorganization ofmuscle fibres, increase of connective tissue, and 'short appearing' fibres. H and E cryostat section x 120.
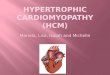
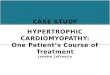
sounds were audible or recorded phonocardiographi-cally. Atrial fibrillation was present, blood pressurewas 130/80 mmHg, and the electrocardiogramshowed evidence of moderate left ventricular hyper-trophy. Carbimazole treatment was stopped but thefollowing year thyrotoxicosis recurred. Radio-iodinetherapy was given and the thyroid condition againimproved, but in 1969 increasing dyspnoea, especiallynocturnally, and an abnormal echocardiogramsuggested the diagnosis of cardiomyopathy. Theechocardiogram (Fig. 6) showed a fast diastolic closurerate of the anterior mitral valve leaflet with a second-ary re-opening during mid-diastole; movement of theposterior ventricular wall and septum was reduced.No forward systolic displacement of the mitral valvewas evident. Right heart catheterization revealed anindirect mean left atrial pressure of 24 mmHg, risingto 32 mmHg after exercise. The pulmonary arterypressure was 53/20 with a mean of 36 mmHg. Theleft heart was not catheterized. In view of the de-terioration in the patient's condition exploratorycardiac surgery was carried out. No valvar diseasewas present but limited examination by palpationthrough the mitral valve revealed marked thickening
of the left ventricular muscle with increased cavitysize. A biopsy was taken near the cardiac apex, andthis showed gross hyperplasia of the muscle fibreswith marked dystrophic changes. There was a con-siderable degree of fibrosis and elastosis, and someincrease in glycogen in the perinuclear areas (Fig. 7).Two days after operation the patient developed aright hemiplegia, presumably due to thromboembol-ism. Convalescence was slow. Carbimazole was con-tinued and there have been no further episodes ofleft ventricular failure (possibly related to the markedrestriction of physical activity). Currently the physicalfindings, the electrocardiogram, and the echocardio-gram are unchanged.
DISCUSSION
In the three cases described the exact relationshipof thyroid overactivity to the time of onset ofhypertrophic disease is difficult to assess. Certainlytwo patients had thyrotoxicosis, one at the sametime as the cardiomyopathy was present (patient
715
copyright. on N
ovember 13, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.29.6.713 on 1 N
ovember 1974. D
ownloaded from

C. Symons, P. J. Richardson, and 0. Feizi
1!)
FIG. 5. PATIENT 3. External carotid pulse tracingshowing rapid upstroke, sudden collapse, and sharptidal wave. There is a mid-to-late systolic murmur.
FIG. 3. PATIENT 2. Mitral valve echocardiogramshowing a small forward displacement during systole(arrowed) of the anterior valve leaflet (AM), inter-ventricular septum (IVS), and closure of the mitralvalve during mid-diastole (E,F).
FIG. 4. PATIENT 2. Single frame from left ventri-cular cine-angiogram (right anterior oblique) showingtypical features of hypertrophic cardiomyopathy (seetext).
FIG. 6. PATIENT 3. Echocardiogram of mitral valveindicating a rapid diastolic closure rate (E,F) and thesecondary diastolic re-opening (arrowed) of theanterior mitral valve leaflet (AM).
1" 1, 1. :..
imm" .-.Wo-i 1- ro.,
716
copyright. on N
ovember 13, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.29.6.713 on 1 N
ovember 1974. D
ownloaded from

Hypertrophic cardiomyopathy and hyperthyroidism: a report of three cases
I LA*
&~ ~ ~ ~ ~ ~~l
FIG. 7. PATIENT 3. Left ventricular muscle biopsy showing gross hyperplasia of muscle fibres (up to 60ju diameter) withincrease of connective tissue. H and E cryostat section x 300.
2) and the other preceding the diagnosis of car-diac disease (patient 3). However, in patient 1 acardiac murmur had been audible for many yearsbefore the definitive diagnosis of hypertrophiccardiomyopathy was made, and during the timethis patient attended the cardiac clinic underlyingthyrotoxicosis had been suspected as a cause ofthe cardiac lesion eight years before hyperthyroid-ism was actually confirmed.
It is possible that each might have suffered fromoccult hyperthyroidism for a prolonged length oftime prior to obvious heart disease, as it is knownthat thyroid overactivity may not be manifestclinically, particularly in older subjects, until itspresentation as a cardiac disorder (Symons,Richardson, and Wood, 1971). Self-limitingperiods of thyrotoxicosis have also been observed(McLarty, Alexander, Harden, and Robertson,1971) and a repeated search for this condition maywell prove rewarding in patients with hypertrophiccardiomyopathy when thyroid function is initiallynormal.The clinical diagnosis of hypertrophic cardio-
myopathy in the presence of hyperthyroidism isdifficult to make since many of the physical signsare common to both diseases, viz, rapid upstrokepulse, mild hypertension, left ventricular type ofcardiac impulse, and a systolic murmur at the leftsternal edge. The murmur differs in timing in thetwo conditions and may be a useful diagnosticpoint of differentiation; in thyrotoxicosis thetypical murmur is in early systole (Ueda et al.,1963) while in hypertrophic cardiomyopathy themurmur occurs later in systole (Goodwin, 1970).Although in one of our three cases no murmur orabnormal sound was either heard or recordedfrom 1968 onwards, it would seem reasonable tosuspect the presence of hypertrophic cardiomyo-pathy in addition to hyperthyroidism, should amid or late systolic murmur persist after theeuthyroid state is attained. Dysrhythmias com-monly occur in both conditions, e.g., multipleventricular ecoptic beats and atrial fibrillation,and although pre-excitation has been recorded inthyrotoxicosis (Sanghvi and Banerjee, 1961), itis not possible to state if either hypertrophic car-
717
copyright. on N
ovember 13, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.29.6.713 on 1 N
ovember 1974. D
ownloaded from

C. Symons, P. J. Richardson, and 0. Feizi
diomyopathy or thyrotoxicosis was the cause ofthis abnormality in our first patient.We have found echocardiography especially in-
formative in screening patients with thyrotoxicosisas it is frequently impossible or undesirable to per-form invasive investigations in these highlyanxious subjects if hypertrophic myocardial diseaseis suspected. The characteristic abnormal forwarddisplacement of the anterior mitral valve leaflet(Pridie and Turnbull, 1968; Shah, Gramiak, andKramer, 1969) was demonstrated in patients 1 and2 where there was also evidence of septal hyper-trophy. The former also had a reduced diastolicclosure rate of the mitral valve. The abnormalitiesin the third patient were different. The diastolicclosure rate of the anterior mitral valve leaflet wasfast but, in addition, there was secondary re-opening in mid-diastole. One explanation for thiswould be a rapid reversal of the pressure gradientbetween the left atrium and left ventricle becauseof the high left atrial pressure and a poorly com-pliant left ventricular muscle. In this patient therewas also a notable absence of a systolic openingmovement of the mitral valve, suggesting pro-gression in the natural history of hypertrophiccardiomyopathy, from the truly hypertrophic statesuggested by the phonocardiogram and indirectcarotid pressure recording of 1966 to the currentclinical condition with some of the features of thephase described by Goodwin (1970) where thereis a spontaneous loss of outflow tract obstructionfrom impairment of systolic contractile function.
Thyrotoxicosis has been known to cause cardiachypertrophy as shown by necropsy studies, butno contemporary data exist to compare thesechanges with the features of hypertrophic diseaseas described by Goodwin (1970) and Goodwin andOakley (1972). A search of the literature for de-tailed and unequivocal descriptions of necropsyfindings in patients who have died after and withlong-standing thyrotoxicosis indicates that impres-sive and abnormal left ventricular hypertrophymay occur, in keeping with the modern conceptof hypertrophic myocardial disease. Symmers(1918) described six such patients, one of whom hestated had papillary muscle hypertrophy (andshown by photograph), and Loos (1929) also re-ported a similar case with gross left ventricularhypertrophy and a cartilage-like thickening of thepapillary muscles.The cardiac muscle biopsies which we have
obtained showed the typical features of hyper-trophic cardiomyopathy (Olsen, 1973) on lightmicroscopy, histochemistry, and electron micro-scopy in one instance. In patient 3 the changes
were not specific for this condition, showing evi-dence only of muscle hypertrophy and fibrosis,although the area examined was not from themost favourable site. Muscle hypertrophy couldresult directly from the effects of increased levelsof circulating thyroid hormones and their ana-logues (Symons, Olsen, and Hawkey, 1974), alsofrom the secondary effect of tachycardia andaugmented cardiac output. The long-continuedhigh output state, conceivably clinically unde-tected for many years, may prove to be a stimulusfor unrestrained muscle hypertrophy, if someunderlying myocardial fault is present. A general-ized muscle disorder may be present in bothhyperthyroidism and hypertrophic cardiomyo-pathy, for it is of interest that the electromyo-gram shows diffuse abnormalities in the formercondition, and changes have also been recorded involuntary muscle in subjects with hypertrophiccardiomyopathy (Meerschwam, 1969). We do notbelieve there is enough evidence to postulate anautoimmune basis for the myocardial abnormal-ities. Thyroid antibodies were negative in ourpatients, and in two cases where this test wasperformed we have not found any cardiac muscleantibodies.Both hyperthyroidism and hypertrophic cardio-
myopathy have a familial association, but none ofthe three patients we have described had relativeswho had any unusual forms of cardiac disorder.
We are grateful to Mr. Lance Bromley, F.R.C.S.,Dr. Simon Rees, Professor Everson Pearse, and MissSusan van Noorden for their help with these cases.
REFERENCES
Goodwin, J. F. (1970). Congestive and hypertrophiccardiomyopathies. Lancet, 1, 731.and Oakley, C. M. (1972). The cardiomyopathies.British Heart Journal, 34, 545.
Loos, F. (1929). Kasuistischer Beitrag zur Frage derHerzveranderungen bei Morbus Basedowii. Zeit-schrift fur Kreislaufforschung, 21, 641.
McLarty, D. G., Alexander, W. D., Harden, R. McG.,and Robertson, J. W. K. (1971). Self-limitingepisodes of recurrent thyrotoxicosis. Lancet, 1, 6.
Meerschwam, I. S. (1969). Hypertrophic ObstructiveCardiomyopathy, a Clinical Study, p. 134. Ex-cerpta Medical Foundation, Amsterdam.
Olsen, E. G. J. (1973). The Pathology of the Heart.Intercontinental Medical Book Corporation, NewYork.
Pridie, R. B. and Turnbull, T. A. (1968). The aeti-ology of mitral valve dysfunction as revealed byultrasonics. In Proceedings of the 5th EuropeanCongress of Cardiology, Athens, September1968, pp. 263-272.
718
copyright. on N
ovember 13, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.29.6.713 on 1 N
ovember 1974. D
ownloaded from

Hypertrophic cardiomyopathy and hyperthyroidism: a report of three cases
Sanghvi, L. M. and Banerjee, K. (1961). Wolff-Parkinson-White syndrome associated with thyro-toxicosis. American Journal of Cardiology, 8, 431.
Shah, P. M., Gramiak, R., and Kramer, D. H. (1969).Ultrasound localization of left ventricular outflowobstruction in hypertrophic obstructive cardio-myopathy. Circulation, 40, 3.
Symmers, D. (1918). The relationship of the so-calledidiopathic cardiopathy to exophthalmic goitre.Archives of Internal Medicine, 21, 337.
Symons, C., Olsen, E. G. J., and Hawkey, C. M.(1974). Production of cardiac hypertrophy bytriiodothyroacetic acid (triac). Submitted forpublication.
Richardson, P. J., and Wood, J. B. (1971).Unusual presentation of thyrocardiac disease.Lancet, 2, 1163.
Ueda, H., Uozumi, Z., Watanabe, H. Kobayashi, T.,Kawai, N., Matuura, T., and Iwase, T. (1963).Phonocardiographic study of hyperthyroidism.Japanese Heart Journal, 4, 509.
Requests for reprints to: Dr. C. Symons, Departmentof Cardiology, Royal Free Hospital, Pond Street,London NW3 2QG.
719
copyright. on N
ovember 13, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.29.6.713 on 1 N
ovember 1974. D
ownloaded from