Embed Size (px)
Citation preview

11/23/2013
1
The Case of J.W.
§ 0925: Paramedic radio call
§ 50 y/o male “lives on sidewalk”; found down by passersby. GCS 4-6-4; Ox2. Doesn’t know how he ended up on the ground. Laceration above left eye, repetitive questioning; exam otherwise normal
§ VS in field: 170/96 100 16
§ Brought to hospital as a Tier I trauma
The Case of J.W.
§ 0945: ED arrival – Primary Survey
§ C spine immobilized
§ ABCs normal
§When patient unclothed, nurse notes patient feels warm to touch
§ Rest of primary survey normal
The Case of J.W.
§ 0945: ED arrival – Secondary Survey§ VS: 186/93 134 34 100%
§ Superficial laceration over left eye
§ PERRL 2 1 bilaterally
§ Neuro: Repetitive questioning. Unable to give medical history other than “anxiety and depression on some psych meds”
§ Denies illicit drug use; positive EtOH use
The Case of J.W.
§ 0945: ED arrival – Secondary Survey§ VS: 186/93 134 34 100%
§ Tempadot not working
§ Superficial laceration over left eye
§ PERRL 2 1 bilaterally
§ Neuro: Repetitive questioning. Unable to give medical history other than “anxiety and depression on some psych meds”
§ Denies illicit drug use; positive EtOH use
The Case of J.W.
§ ED Course
§ Trauma team in ED putting patient on the monitor to go to CT
§ Is he stable enough to go?
§ But wait… there’s more…
§ Rectal temperature comes back at 41.7C
The Case of J.W.
§ Is this patient just a trauma patient?
§ What are the general categories of what might be wrong with this patient?
§ General categories – “TIME”
§ T = Toxic
§ I = Infectious
§ M = Metabolic (including withdrawal)
§ E = Environmental

11/23/2013
2
What do you think is wrong with this patient?
1. Serotonin syndrome
2. Anticholinergic syndrome
3. Heat stroke
4. Neuroleptic malignant syndrome
5. Meningitis / encephalitis
6. Other
The Case of J.W.
§ ED Course
§ IV NS 1 liter – room temperature
§ Ice packs to groin and axillae
§ IVF placed on ice for later infusion
§ Moist towels applied to forehead
§ Request made for fan / misters
The Case of J.W.
§ ED Course§ After CT, the patient returns to ED and is
placed on cooling blanket
§ 1020 (35 minutes after arrival)§ Temp 41.1 180/82 133 30 100% NRB
§ Triple lumen foley from OR
§ IVF: 1L cooled NS
§ Bladder continuously irrigated with cooled fluids
The Case of J.W.
§ ED Course
§ Portable CXR: Cardiomegaly
§ Pelvis: Negative
§ EKG obtained
§ Labs sent
§ Head and C spine CT: Negative
The Case of J.W.
§ 1040 (55 minutes after arrival)
§ 40.3 145/76 127 27 99% FM
§ Patient now oriented to name/place/month
§ “I feel very bad”
§ Meds: Seroquel, elavil
§ Cooling measures (except fans/mist) continued
The Case of J.W.
§ 1100 (1 hr, 5 minutes after arrival)§ 40.1 143/77 121 26 98%
§ Labs§ CBC: 13.8 / 14.6 / 42.7 / 287 (normal)
§ Chem 7: 138 / 3.9 / 106 / 20 / 15 / 1.4 / 127
§ LFT’s: 1.2 / 38 / 22 / 83
§ Coags: WNL
§UA: 8 RBC, o/w WNL
§ Tox, including ASA, EtOH, APAP: Negative
§ CK-MB: 0.9 Troponin: 0.15 Total CK: 205
§ Blood cultures pending

11/23/2013
3
The Case of J.W.
§ 1145 (2 hours after arrival)
§ A, O x 4
§ “I don’t remember what happened. I have been drinking a lot (last drink day prior), and I was trying to get to a friend’s home, woke up here. I take all my meds and I am only recently living on the street.”
The Case of J.W.
§ 1230
§ 38.4
§ Cooling measures stopped
§ Temp remained 100-101
§ 1320
§ Transported to ICU
The Case of J.W.
§ So… what’s wrong with J.W.?
§ Differential Diagnosis…
§ Serotonin syndrome?
§ Neuroleptic malignant syndrome?
§ Heat stroke?
§ Anticholinergic syndrome?
§ Meningitis / encephalitis?
§ Other?
Neuroleptic Malignant Syndrome
Neuroleptic Malignant Syndrome
§ A relatively rare, easily overlooked, high mortality syndrome with limited treatment options
§ A “diagnosis of exclusion”
§ “Requires High Clinical Suspicion”
NMS: Incidence and Mortality
§ Incidence of 0.01-0.02% of pts on antipsychotics
§ 2000 cases/year
§ Mortality 10-20% (previously 80%)§ Change in mortality from § Change in types of meds
§Newer definitions of NMS
§ Better supportive care

11/23/2013
4
NMS: Classic Presentation
§ Classic Tetrad
§ Altered Mental Status
§ Muscular Rigidity
§ Fever
§ Autonomic Instability
NMS: Clinical History
§ Drug Exposure:
§ Typical high potency antipsychotics (haloperidol)
§ Atypical neuroleptics (risperidone, olanzapine, clozapine)
§ Antiemetics (metochlopromide, promethazine)
§ No definite time or dose relationship
§ DSM IV: “within last month”
NMS: Clinical History
§ Higher incidence with other co-morbid conditions:
§ Substance Abuse
§ Trauma
§ Dehydration
§ Acute Medical Illness
§ Data is derived primarily from case reports as well as retrospective analysis
NMS: Pathogenesis
§ Overall theory: Central dopamine receptor blockade
§ Dopamine antagonism in frontal lobes leads to Altered Mental Status
§ Dopamine antagonism of hypothalamus leads to Fever
§ Unclear mechanism that causes disruption of sympathetic system leads to labile HR and BP Dysautonomia
§ Interference in the nigrostriatal dopamine pathways causes (Parkinsonian like) Rigidity and tremor
NMS: Rigidity
§ Historically muscle rigidity is one of the defining features of NMS
§ Contributes to the hypermetabolism, hyperthermia, and rhabdo§ Alternate theory: interference in peripheral mitochondrial
function that leads to rigidity
NMS: Lab Findings
§ Non-specific
§ Total CK > 1000
§WBC > 10K
§ Mildly elevated LDH, LFTs
§ Renal Insufficiency (secondary to rhabdo)
§ CSF with mildly elevated protein
§ Low serum iron

11/23/2013
5
NMS: Diagnostic Criteria
§ DSM-IV: § Recent administration of antipsychotic
§ Elevated Temp (> 40C)
§ Muscle Rigidity
§ At least 2 other signs/symptoms or lab findings c/w NMS
§ Bottom Line: Dx should be considered when 2 of 4 in tetrad present in setting of patient on appropriate agent
§ Most references support that all 4 generally present over the course of 1-3 days
NMS: TREATMENT
§ ABCs
§ Stop the Offending Agent! (and don’t give other potentially offending agents)
§ Aggressive cooling measures
§ Fluid resuscitation
§ Supportive care
§ Benzodiazepines for agitation
NMS: Role of Dantrolene
§ Dantrolene
§ Direct skeletal muscle relaxant
§ Blocks release of calcium from sarcoplasmic reticulum
§ Decreases myocyte metabolism
§ Rationale
§ Reduces heat production
§ Decreases muscle rigidity (and its complications)
§ “It works in malignant hyperthermia”
NMS: Dantrolene
§ Numerous case reports of use, with mixed results
§ One meta-analysis (based on retrospective studies
and case reports) showed improvement in 80% cases
§ Dose: 10mg/kg per day§ Caution in pts on calcium channel blockers
(theoretically can lead to cardiovascular collapse)
NMS: Treatment
§ Bromocriptine§ Dopamine agonist to counteract central
blockade
§ Max: 40mg/day
§ Amantadine§ Dopamine agonist and anticholinergic agent
§ Max 400mg/day
§ ECT (electroconvulsive therapy)
NMS: Treatment
§ There are no clinical trials for NMS
§ One animal model showed dantrolene reduced temps, CK levels, and rigidity
§ Several retrospective analyses
§ Suggest patients on dantrolene +/- bromocriptine had faster recovery (if survived) – 9 days vs 12 days
§ Of note
§ In most reports, therapy initiated between 24-48 hours of presentation

11/23/2013
6
NMS: New Developments
§ Azumolene
§ More water soluble than dantrolene
§ Requires less time to prepare
§ Dantrolene in newer preparations
Currently not available for clinical use
NMS: Dx and Tx… Incorporated
§ Woodbury Stages § Incorporates severity of disease with
treatment§ Stages I, II and III (Mild to Moderate NMS)§ Supportive care +/- benzodiazepines
§ Stage IV (Moderate NMS)§ All four features present (at some point)
§ Benzodiazepines, bromocriptine
§ Stage V (Severe NMS)§ Tetrad with higher temp
§ Benzos, dantrolene, bromocriptine, consider ECT
NMS: Prognosis
§ Most resolve within 2 weeks, without long term sequelae
§ Poorer prognosis in those with high peak and/or long duration of hyperthermia
NMS: Potential Pitfalls
§ Overlooking the AMS in a “psych pt”
§ Delay in obtaining rectal temp
§ Use of physical restraints§ Isometric contractions leads increased
metabolism, worsening rhabdo and hyperthermia
§ Use of high potency antipsychotics to “calm” the patient
Serotonin Syndrome
SEROTONIN SYNDROME
§ Triad of:
§Altered mental status
§Autonomic instability
§Neuromuscular abnormalities§ In the setting of a recent initiation or dosage
change of an offending agent
§ Reactions range from barely perceptible to life threatening

11/23/2013
7
SS: Incidence
§ Widespread and increasing usage of SSRIs
§ High frequency of mild reactions
§ Approximately 7000 toxic reactions/year
§ 100 deaths/year
SS: Clinical Presentation
§ Classically
§ AMS§ Agitated delirium, restless, anxious, hypervigilence
§ Autonomic instability§ Hyperthermia, tachycardia, HTN, shivering
§ Neuromuscular abnormalities§ Clonus, hyperreflexia, tremor, repetitive movements, rigidity
§ GI§ Nausea, vomiting, abdominal pain
SS: Implicated Drugs
§ SSRIs
§ MAOIs
§ TCAs
§ Drugs of Abuse: Cocaine, ecstasy, marijuana (?)
§ Analgesics: demerol, fentanyl
§ Antiemetics
§ OTC: Cough meds, herbal products, St John’s Wort
§ Triptans
§ Bromocriptine
SS: Pathophysiology
§ Serotonin works centrally
§ Modulates attention, behavior, thermoregulation
§ High concentration of serotonergic neurons in the raphe nuclei in the brainstem
§ Overstimulation à anxious, agitated, tachycardic, clonus, hyperreflexia
§ Peripheral receptors in GI tract: N/V/D
SS: Physical Exam
§ Clonus is most defining feature
§ Spontaneous or inducible
§ Ocular clonus (horizontal)
§ Shivering
§ Hyperreflexia
§ Diaphoresis, nausea
SS: Laboratory Evaluation
§ Like NMS, no confirmatory tests
§ Non-specific
§ Elevated WBC
§ Elevated CK
§ Evidence of rhabdomyolysis
§ ARDS
§ DIC

11/23/2013
8
SS: Diagnostic Criteria
§ Hunter Criteria Decision Rules
(84% Sensitivity; 97% Specificity)
§ Serotonergic agent plus 1 of following:
§ Spontaneous clonus
§ Inducible clonus plus agitation
§ Ocular clonus plus agitation
§ Clonus plus hyperthermia
SS: Diagnostic Criteria
§ Sternbach’s Criteria:§ No new neuroleptics or change in neuroleptic dose
§ Other etiologies have been excluded (infxn, tox)
§ New serotonergic agent or dosage change plus 3 of the following:§ AMS
§ Hyperreflexia
§ Hyperthermia
§ Diarrhea
§ Clonus
§ Shivering
SS: Treatment
§ ABCs
§ Discontinue offending agent
§ Supportive care
§ Benzodiazepines for agitation
§ Avoid physical restraints
§ Consider paralysis with non-depolarizing agent
SS: Cyproheptadine
§ Cyproheptadine is serotonin antagonist (works centrally and peripherally)
§ Case reports describe successful treatment of serotonin syndrome
§ An animal model shows that an initial dose (12mg) blocked 85-95% of serotonin receptors§ 8mg NG, then 4mg Q2H; Max 32mg/day
Clinical Course and Prognosis
§ Serotonin Syndrome generally presents within 6-24H of exposure to offending agent
§ Resolves within 24H
§ Mortality is relatively low <1%
NMS vs Serotonin Syndome
NMS
§ Dopamine antagonism
§ Slower onset
§ Longer course
§ Hyperthermia and rigidity
§ TX: Supportive, Bromocriptine, Dantrolene
Serotonin Syndrome
§ Serotonin agonists
§ Acute onset
§ Short clinical course
§ Clonus and hyperreflexia
§ TX: Supportive, Cyproheptadine

11/23/2013
9
NMS vs Serotonin Syndome
NMS
§ Dopamine antagonism
§ Slower onset
§ Longer course
§ Hyperthermia and rigidity
§ TX: Supportive, BZDs, Bromocriptine, Dantrolene
Serotonin Syndrome
§ Serotonin agonists
§ Acute onset
§ Short clinical course
§ Clonus and hyperreflexia
§ TX: Supportive, BZDs, Cyproheptadine
Heat Stroke
HEAT ILLNESSThe Syndromes
§ Minor Syndromes§ Heat edema
§ Heat tetany
§ Heat syncope
§ Heat cramps
§ Major Syndromes§ Heat exhaustion
§ Heat stroke
HEAT STROKEGeneral Information
§ Characterized by combination of ...
§ Hyperthermia
§ Altered mental status
§ Least common form of heat illness
§ A true medical emergency
§ Can be fatal if unrecognized / untreated
HEAT STROKE General Information
§ Caused by overwhelming of thermoregulatory ability of body
§ Mortality / morbidity determined by degree and duration of elevated temperature
§ Aggressive cooling critical
HEAT STROKEPathophysiology
§ At temperature of 42 C
§ Oxidative phosphorylation uncouples
§ Enzymes dysfunction
§ Proteins denature
11/23/2013
10
HEAT STROKEPathophysiology
§ Effects
§ Increasing hyperthermia
§ Membrane fluid leaks
§ Widespread necrosis
§Especially vasculature, liver, neural tissue
HEAT STROKEHistory
§HPI§ Onset precipitous in 80%
§ Prodrome in 20%§Weakness, vomiting, headache
§ Exposure to elevated ambient temperatures
§ Excessive exercise
HEAT STROKE History
§ PMH
§ Medical illnesses
§ Medications
§ Drug use
HEAT STROKEPhysical Examination
§ Vital Signs
§ Increased temperature
§Can be over 41 C, but may be less
§ Increased HR
§Up to 200 BPM
§ Low or normal BP
§Wide pulse pressure often found
§ Increased RR
HEAT STROKEPhysical Examination
§ Altered mental status
§ Sine qua non for making diagnosis
§ Rest of exam often nonfocal
HEAT STROKEClassic Heat Stroke (CHS)
§ During period of sustained high ambient temperature
§ Due to compromised homeostasis
§ Patients at risk§ Elderly, especially poor socioeconomic group
§ Debilitated patients
§ Psychotic patients
§ Very young patients

11/23/2013
11
HEAT STROKEClassic Heat Stroke (CHS)
§ Clinical findings
§ Altered mental status
§ Hyperthermia
§ Hot, dry, flushed skin
HEAT STROKEExertional Heat Stroke (EHS)
§ Young, healthy people§ Often athletes, military recruits
§ Exertion overwhelms thermoregulation
§ Clinical§ Confused, combative, comatose
§ 50% sweating, often profusely
§ Mild to moderate volume depletion
§ Complications common and serious
HEAT STROKEEvaluation
§ SMA-7
§ CBC
§ PT / PTT, Fibrinogen, FSP
§ ABG
§ CPK
§ LFT’s
§ U/A; consider urine electrolytes, osmolality
§ CXR
§ Head CT if indicated
§ Consider LP, tox screen, blood cultures
HEAT STROKEDifferential Diagnosis
§ Infections
§ CVA
§ Toxins (esp. anticholinergic drugs)
§ Neuroleptic malignant syndrome
§ Serotonin syndrome
§ Prolonged status epilepticus
§ Endocrine disorders
§ Malignant hyperthermia
HEAT STROKECNS Involvement
§ Common early in illness
§ Delirium, coma most common
§ Focality rare
§ Seizures in 25-40%
§ Often occur during cooling stage
§ Tends to resolve with cooling
§ May have residual deficits
HEAT STROKECardiovascular Involvement
§ Tachycardia - up to 200 bpm
§ Mild hypotension common
§ EKG§ ST depression
§ T wave inversion
§ QT prolongation
§ IVCD’s
§ Dysrhythmias rare
§ May hemorrhage into the myocardium
11/23/2013
12
HEAT STROKEHematologic Involvement
§ DIC common in severe heat stroke
§ EHS >>> CHS
§ Common cause of death in these patients
§ Due to endothelial damage
§ Leukocytosis common
HEAT STROKEGastrointestinal Involvement
§ Hepatic damage almost universally seen
§ Multifactorial
§ Splanchnic vasoconstriction
§Hyperthermia
§ LDH, transaminases elevate within 24 hours
§ Peak at 48-72 hrs
§ AST > 1000 poor prognostic sign
HEAT STROKEGastrointestinal Involvement
§ Jaundice may be seen day 2-3
§ Hypoglycemia seen in 30% of EHS patients
§ Diarrhea common
HEAT STROKERenal Involvement
§ Myoglobinuria common in EHS
§ Rhabdomyolysis
§ EHS >>> CHS
§ Hyperuricemia common in EHS
HEAT STROKERenal Involvement
§ Oliguric renal failure
§ CHS 5%, EHS 25-30%
§ Multifactorial§ Splanchnic vasoconstriction
§Hyperthermia
§Hypovolemia
§ Rhabdomyolysis
§DIC
HEAT STROKEElectrolytes / Acid-Base
§ Hypokalemia common (EHS >> CHS)
§ Hyperkalemia seen if renal failure
§ Respiratory alkalosis (CHS >> EHS)
§ Metabolic acidosis (EHS >> CHS)
11/23/2013
13
HEAT STROKETreatment
§ If in doubt.....treat for heat stroke
§ ABC’s = “ABCC” in heat stroke
§ Airway
§ Breathing
§ Circulation
§ Cooling
HEAT STROKETreatment
§ If in doubt.....treat for heat stroke
§ ABC’s = “ABCC” in heat stroke
§ Cooling
§ Airway
§ Breathing
§ Circulation
HEAT STROKEAirway / Breathing
§ All patients should receive supplemental oxygen
§ Intubation?
§ Unable to protect airway
§ Inadequate oxygenation / ventilation
§ Consider in all heat stroke patients
HEAT STROKECirculation
§ IV access in all patients
§ Fluids
§ Rarely need large amounts
§ 1-2 liters NS over 2-4 hours
§ Watch for pulmonary edema, ARDS
§ Hypotension
§ Usually responds to cooling, IVF
§ If need pressors, avoid norepinephrine
§ Foley to monitor urine output
HEAT STROKECooling
§ Cornerstone of therapy
§ Goal: Rapid cooling to 39 C§ Aim for a decrease of 0.1-0.2 C/min
§ Initiate cooling measures immediately§ Remove clothes
§ Ice to groin, armpits, neck
§ Wet sheet on patient or spray mist on naked patient
§ Circulation of air
HEAT STROKECooling
§ Check temperature every 5 minutes
§ Temperature monitoring method
§ Oral unreliable
§ Rectal or bladder probe
§Most commonly used method
§May lag behind core temperature by 5-10 minutes

11/23/2013
14
HEAT STROKECooling
§ Temperature monitoring
§ Tympanic membrane
§Not proven accurate in hyperthermic patients
§ Esophageal thermometry
§Most accurate way to measure temperature
§Often not available in ED
HEAT STROKECooling Measures
§ Immersion technique
§ Evaporative techniques
§ Ice
§ Iced gastric lavage
§ Iced peritoneal lavage
§ Cool air ventilation
§ Cooled IV fluid
HEAT STROKEImmersion Techniques
§ Rapid temperature reduction (0.25 C/min)§ Ice slush, cool water§ Drawbacks§ Cumbersome, impractical,
not readily available§ May cause shivering (increases temp)§ Causes vasoconstriction - “Human thermos bottle”§ Overcooling in 33%
§ Not proven consistently more effective than evaporative techniques
HEAT STROKEEvaporative Techniques
§ Cooling rates of 0.1 - 0.2 C/min
§ Spray tepid water on naked patient
§ Use fans to circulate air
§ Universally available
§ Easy to use
HEAT STROKEIce Packs
§ In armpits, groin, neck
§ May use as an adjunct
§ Watch for shivering
HEAT STROKEIced Gastric Lavage
§ Cooling rates up to 0.15 C/min
§ A very useful adjunct
§ Minimally invasive
§ Takes times to cool fluid
§ Put NS bags in ice on patient arrival or on EMS contact
11/23/2013
15
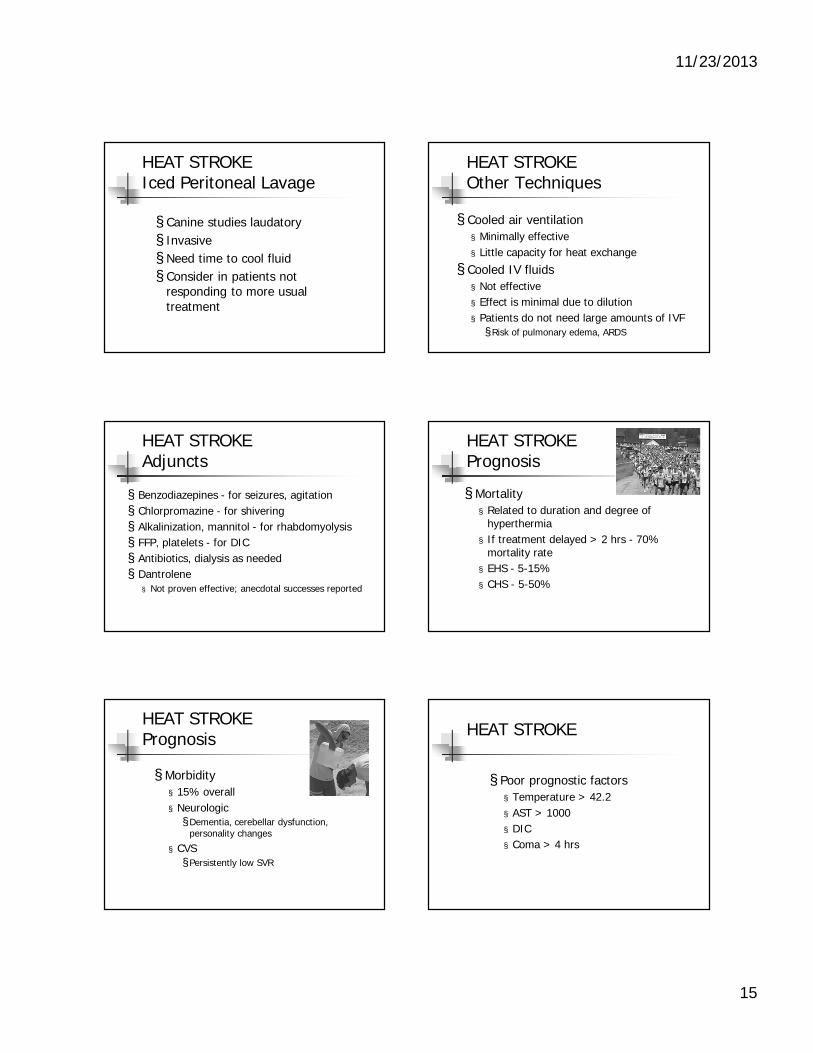
HEAT STROKEIced Peritoneal Lavage
§ Canine studies laudatory
§ Invasive
§ Need time to cool fluid
§ Consider in patients not responding to more usual treatment
HEAT STROKEOther Techniques
§ Cooled air ventilation
§ Minimally effective
§ Little capacity for heat exchange
§ Cooled IV fluids
§ Not effective
§ Effect is minimal due to dilution
§ Patients do not need large amounts of IVF
§ Risk of pulmonary edema, ARDS
HEAT STROKEAdjuncts
§ Benzodiazepines - for seizures, agitation
§ Chlorpromazine - for shivering
§ Alkalinization, mannitol - for rhabdomyolysis
§ FFP, platelets - for DIC
§ Antibiotics, dialysis as needed
§ Dantrolene
§ Not proven effective; anecdotal successes reported
HEAT STROKEPrognosis
§ Mortality
§ Related to duration and degree of hyperthermia
§ If treatment delayed > 2 hrs - 70%mortality rate
§ EHS - 5-15%
§ CHS - 5-50%
HEAT STROKEPrognosis
§ Morbidity
§ 15% overall
§ Neurologic§Dementia, cerebellar dysfunction,
personality changes
§ CVS
§ Persistently low SVR
HEAT STROKE
§ Poor prognostic factors
§ Temperature > 42.2
§ AST > 1000
§ DIC
§ Coma > 4 hrs

11/23/2013
16
CHS vs. EHS: A comparison
CLASSIC EXERTIONALMechanism Impaired heat loss Excess heat gain
Age group Elderly Younger
Health status Chronically ill Healthy
Activity level Sedentary Strenuous
Drugs Multiple Usually none
Sweating Usually absent Often present
Lactic acidosis Usually absent Common; marked
Rhabdomyolysis Unusual Common, severe
Acute renal failure < 5% 25-30%
DIC None or mild Marked
CPK elevation Mild Marked
Hypoglycemia Uncommon Common
Anticholinergic Syndrome
Anticholinergic Syndrome
§ Caused by intentional or inadvertent overdose of anticholinergic agent
§ Antihistamines, psych meds most often implicated
§ Herbal remedies, mushroom ingestion may also cause syndrome
Anticholinergic Syndrome
§ Blind as a Bat (dilated pupils)
§ Dry as a Bone (unable to sweat)
§ Red as a Beet (flushing)
§ Mad as a Hatter (CNS anticholinergic)
§ Hot as a Hare (fever)
Anticholinergic Syndrome
§ Physical Findings§ Elevated temperature
§ Tachycardia
§ Elevated blood pressure
§ Dilated pupils
§ Dry skin
§ Absent bowel sounds
§ Altered mental status
§ Urinary retention
Anticholinergic Syndrome
§ Treatment§ Gastric decontamination controversial§Usually NOT indicated
§ Consider activated charcoal
§ Cooling measures as needed
§ Treat seizures as usual
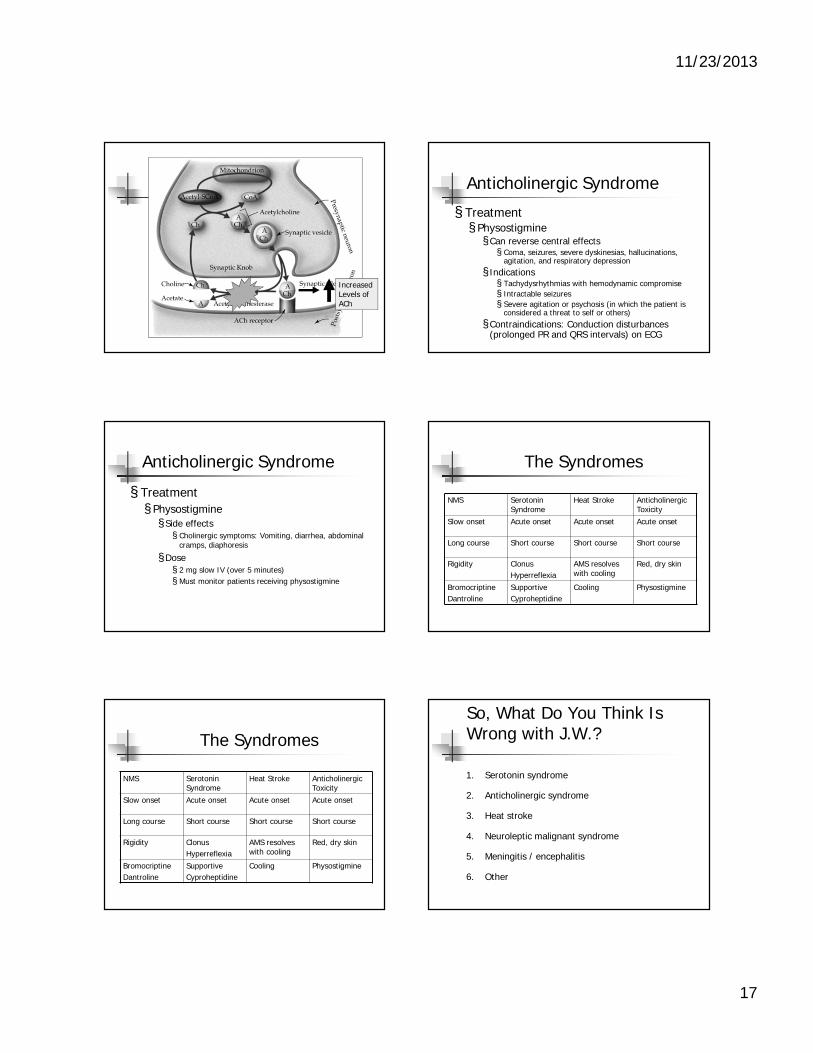
§ Physostigmine§ Inhibits acetylcholinesterase§ Increases acetylcholine levels
11/23/2013
17
Increased Levels ofACh
Anticholinergic Syndrome
§ Treatment§ Physostigmine§ Can reverse central effects § Coma, seizures, severe dyskinesias, hallucinations,
agitation, and respiratory depression
§ Indications§ Tachydysrhythmias with hemodynamic compromise
§ Intractable seizures
§ Severe agitation or psychosis (in which the patient is considered a threat to self or others)
§ Contraindications: Conduction disturbances (prolonged PR and QRS intervals) on ECG
Anticholinergic Syndrome
§ Treatment
§ Physostigmine
§ Side effects§ Cholinergic symptoms: Vomiting, diarrhea, abdominal
cramps, diaphoresis
§Dose§ 2 mg slow IV (over 5 minutes)
§ Must monitor patients receiving physostigmine
The Syndromes
NMS Serotonin Syndrome
Heat Stroke Anticholinergic Toxicity
Slow onset Acute onset Acute onset Acute onset
Long course Short course Short course Short course
Rigidity Clonus
Hyperreflexia
AMS resolves with cooling
Red, dry skin
Bromocriptine
Dantroline
Supportive
Cyproheptidine
Cooling Physostigmine
The Syndromes
NMS Serotonin Syndrome
Heat Stroke Anticholinergic Toxicity
Slow onset Acute onset Acute onset Acute onset
Long course Short course Short course Short course
Rigidity Clonus
Hyperreflexia
AMS resolves with cooling
Red, dry skin
Bromocriptine
Dantroline
Supportive
Cyproheptidine
Cooling Physostigmine
So, What Do You Think Is Wrong with J.W.?
1. Serotonin syndrome
2. Anticholinergic syndrome
3. Heat stroke
4. Neuroleptic malignant syndrome
5. Meningitis / encephalitis
6. Other

11/23/2013
18
So, What Do You Think Is Wrong with J.W.?
1. Serotonin syndrome
2. Anticholinergic syndrome
3. Heat stroke
4. Neuroleptic malignant syndrome
5. Meningitis / encephalitis
6. Other
The Case of J.W. (cont)
§ 1530: In 5E ICU
§ Pulm Fellow note
§ 50 y/o male, homeless, heavy EtOH, on seroquel and paxil. A, O x 4 but somnolent. Exam normal except “generalized weakness likely due to effort. Serotonin syndrome, NMS less likely given exam; encephalitis less likely due to mental status improvement.”
The Case of J.W. (cont)
§ Overnight
§ Patient remains afebrile
§ Normotensive, HR 110, RR 28, 93-96% 2L NC
§ Overnight labs WNL; Cr down to 1.1
§ Troponin trending downward
§ EKG without acute changes
The Case of J.W. (cont)
§ Overnight
§ Patient became agitated and delirious
§ Required ativan, haldol, benadryl§ “For EtOH withdrawal and insomnia”
The Case of J.W. (cont)
§ Day 2: 0830 (23 hours after arrival)§ Spikes to 39.3
§ 180/125 120 28 95%
§ Altered, disoriented, rambling
§ Placed in restraints
§ Bilateral rales noted on exam
§ “Likely CHF; AMS, HTN, tachycardia due to withdrawal”§ Rx: Ativan and Lasix
The Case of J.W. (cont)
§ Day 2: 1000 (24.5 hours after arrival)
§ Event note
§ Patient more tachypneic; desaturating
§ CXR: Cardiomegaly
§ “Likely CHF”
§Given 20 mg IV lasix; no improvement
§ Intubated (impending respiratory failure)§ Used etomidate and rocuronium
11/23/2013
19
The Case of J.W. (cont)
§ Day 2: 1000
§ Post-intubation BP 240/150
§Nitroglycerin drip initiated
§ Stat echo ordered
§ 1400
§Hypotensive to 72/22, HR 118
§NTG drip stopped; levophed drip started
The Case of J.W. (cont)
§ Day 2
§ Emergent echo
§ EF 25%; anterior wall thinned; small effusion
§ Impression: Likely late MI; febrile illness with sepsis
§ Recommended IV Abx; add dopamine as needed
The Case of J.W. (cont)
§ Day 2: 2000 (35 hours after arrival)§Ward call§ Temp 41.6 BP 60/40
§ Swan: SVR 400, CO 5, CI 2.2, PCWP 14
§ Cooling measures started
§ Levophed, dopamine drips; vasopressin added§ 90/50
§ Decadron, ceftriaxone, flagyl, azithromycin
The Case of J.W. (cont)
§ Day 3
§ Labs
§WBC 19.1 Platelets 62
§ Cr 1.8
§ LFTs: 2.0 / 71 / 56 / 66
§ CPK: 1736
§ CK-MB: 15.7
§ Trop: 1.9
The Case of J.W. (cont)
§ Day 3 am
§ MICU attending note
§ Increasing rigidity and decreased mental status
§Will LP for meningitis
§ Continue abx; add ceftazidime and acyclovir
§ Consider dantrolene; consult anesthesia
§Get psych consult
Now what do you think is wrong with this patient?
1. Serotonin syndrome
2. Anticholinergic syndrome
3. Heat stroke
4. Neuroleptic malignant syndrome
5. Meningitis / encephalitis
6. Other

11/23/2013
20
Now what do you think is wrong with this patient?
1. Serotonin syndrome
2. Anticholinergic syndrome
3. Heat stroke
4. Neuroleptic malignant syndrome
5. Meningitis / encephalitis
6. Other (alcohol withdrawal?)
NMS: Diagnostic Criteria
§ DSM-IV: § Recent administration of antipsychotic
§ Elevated Temp (> 40C)
§ Muscle Rigidity
§ At least 2 other signs/symptoms or lab findings c/w NMS
The Case of J.W. (cont)
§ Day 3 pm
§ Psych consult
§History of alcoholism and psychosis
§ Reported OP meds seroquel and wellbutrin
§ Increased temp and rigidity today
§ Consider NMS; recommend dantrolene 2-3 mg/kg IV Q 6 hr and bromocriptine 2.5-10 mg tid
§Dantrolene 250 mg IV Q6H and bromocriptine 5 mg tid started
The Case of J.W. (cont)
§ Day 4 am
§ Temp 42.2
§ Hypotensive on 3 pressors
§ Unresponsive off sedation > 24 hours
§ Made DNR by MICU attending
§ Patient asystolic and pronounced at 1115; 4 days after presentation
The Case of J.W. (cont)
§ Take-Home Points
§ Remember differential of febrile patients includes diagnoses other than infections
§ Extreme hyperthermia?
§ Toxic, metabolic, environmental > infectious
§ Know diagnostic criteria for the other hyperthermia-associated syndromes
§ Cooling measures critical if heat stroke suspected
References
§ Adnet, P, Lestavel, P, Krivosic-Horber, R. Neuroleptic Malignant Syndrome. Br J Anaest 2000; 85:129.
§ Bopyer, Shannon. The Serotonin Syndrome. NEJM 2005; 352:11.
§ Carbone, JR. The neuroleptic malignant and serotonin syndromes. Emerg Med Clin North Am 2000; 18:317.
§ Dunklet, EJC et al. The Hunter serotonin toxicity criteria: simple and accurate diagnostic decision rules. QJM 2003; 96:635.
§ Kent, Kristen. Serotonin Syndrome. UpToDate 2007.
§ Krause, T, et al. Dantrolene—a review of it pharmacology, therapeutic use and new developments. Anaesthesia 2004; 59: 364.
§ Sternback, H. The Serotonin Syndrome. Am J Psychiatry 1991; 148:705.
§ Wijdicks, Eelco. Neuroleptic Malignant Syndrome. UpToDate 2007.




![Employment Law Update - Handout.ppt · Microsoft PowerPoint - Employment Law Update - Handout.ppt [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/600d67b141a89f494f575053/employment-law-update-microsoft-powerpoint-employment-law-update-handoutppt.jpg)

![Immunosuppressant Medications Final - Handout.ppt. 2000;47:291-298 DMARDs ... Microsoft PowerPoint - Immunosuppressant Medications Final - Handout.ppt [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/5afd1d6e7f8b9a444f8d00a7/immunosuppressant-medications-final-200047291-298-dmards-microsoft-powerpoint.jpg)




















![Malignant hyperthermia [final]](https://img.pdfslide.us/doc/110x75/58ceb1b71a28abb2218b5123/malignant-hyperthermia-final.jpg)