Embed Size (px)
Citation preview
Hypertension
Presented by:
Maha Islami
Pharm.D.candidateSupervised by:
Prof.Osama M .IbrahimProfessor of clinical pharmacy
1
outlines• Definition .• Classification .• Etiology .• Complication .• Diagnosis .• Treatment .
2
What is blood pressure? • Arterial BP = co x PVR • co = HR x SV (blood out flow after-load
systolic BP) .• pVR resistance of arterioles resistance to
blood flow pre-load diastolic BP.
3
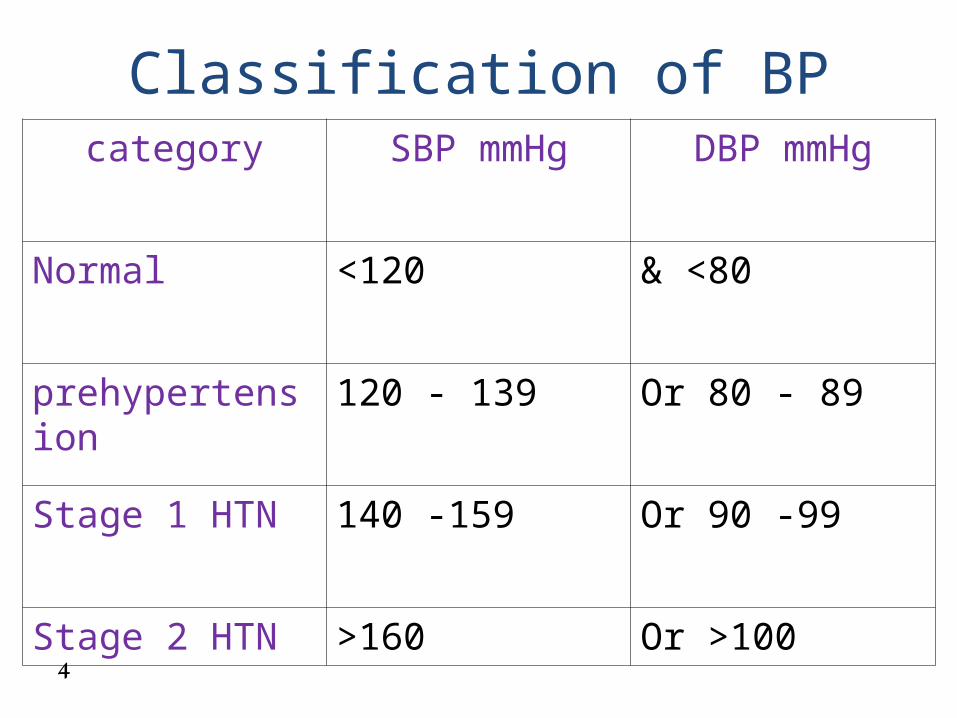
Classification of BPcategory SBP mmHg DBP mmHg
Normal <120 & <80
prehypertension 120 - 139 Or 80 - 89
Stage 1 HTN 140 -159 Or 90 -99
Stage 2 HTN >160 Or >1004

Isolated systolic HTN
• a systolic BP of > 140 mm Hg and diastolic BP < 90 mm Hg and staged .
• Ex : BP 170/82 mmHg is stage 2 isolated systolic HTN.
• Treatment : chlorthalidone .
5
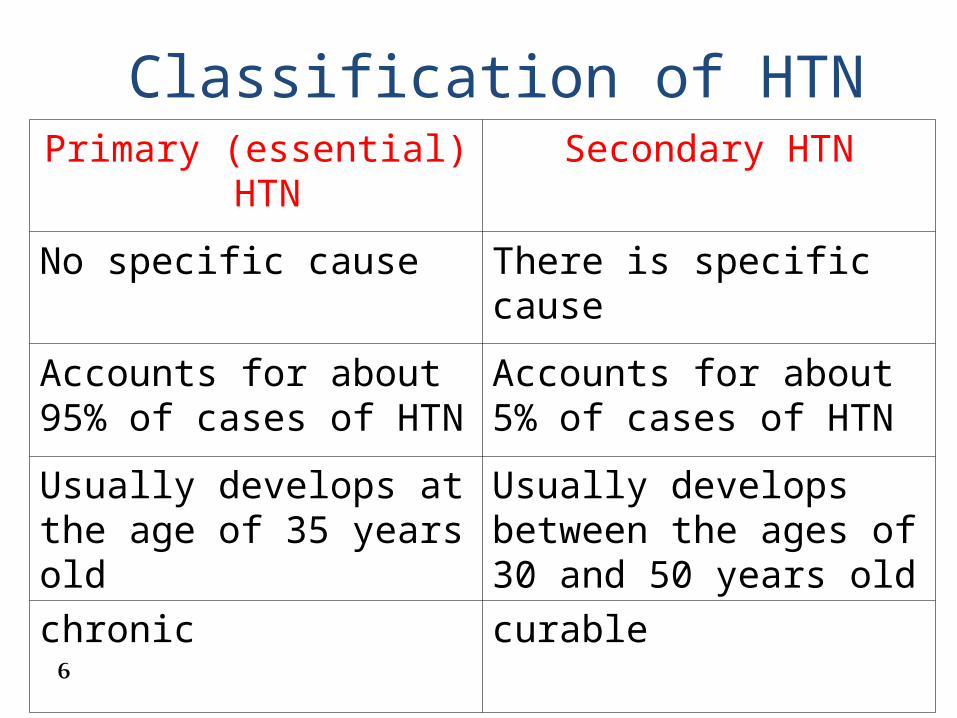
Classification of HTN Primary (essential) HTN Secondary HTN
No specific cause There is specific cause
Accounts for about 95% of cases of HTN
Accounts for about 5% of cases of HTN
Usually develops at the age of 35 years old
Usually develops between the ages of 30 and 50 years old
chronic curable6
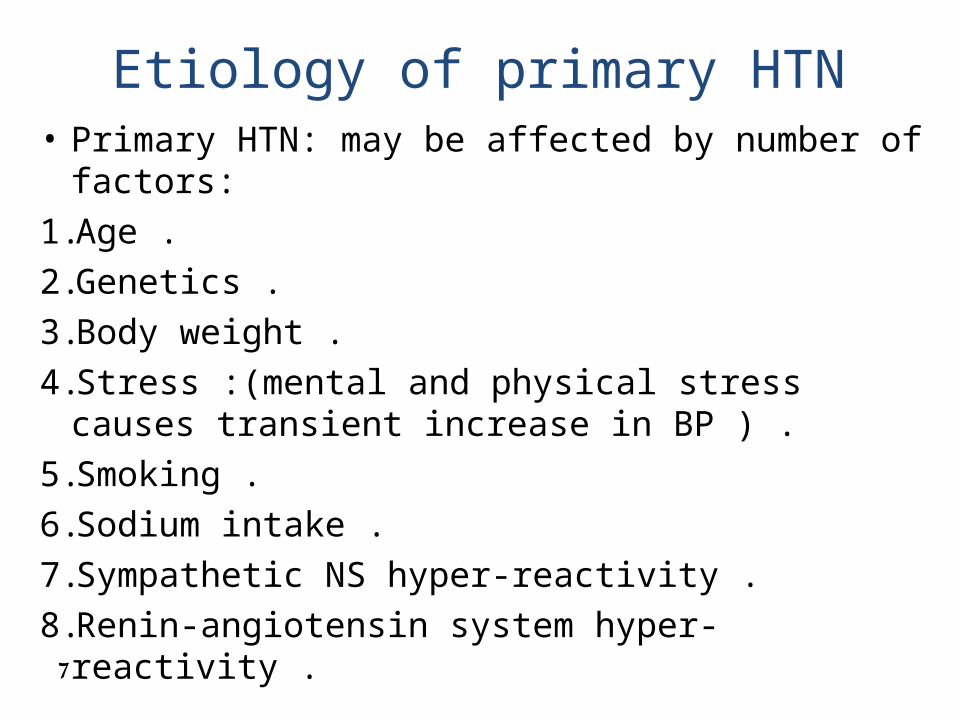
Etiology of primary HTN• Primary HTN: may be affected by number of factors:1. Age .2. Genetics .3. Body weight .4. Stress :(mental and physical stress causes transient
increase in BP ) .5. Smoking .6. Sodium intake .7. Sympathetic NS hyper-reactivity .8. Renin-angiotensin system hyper-reactivity .
7

Etiology of secondary HTN1) Renal diseases:a) Renal artery stenosis.b) Pyelonephritis.c) Polycystic kidneys.2) Endocrinal disease:a) Cushing‘s disease.b) Pheochromocytoma.c) Conn‘s disease.d) Hyperthyrodism.
8
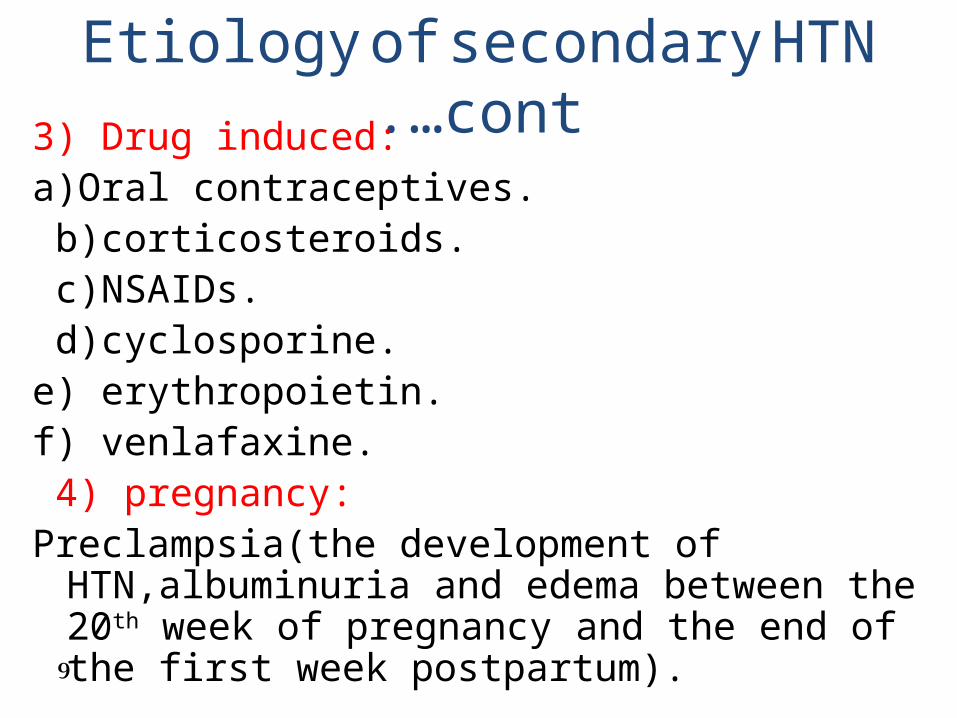
Etiology of secondary HTN cont.…3) Drug induced:a)Oral contraceptives. b)corticosteroids. c)NSAIDs. d)cyclosporine.e) erythropoietin.f) venlafaxine. 4) pregnancy:Preclampsia(the development of HTN,albuminuria and
edema between the 20th week of pregnancy and the end of the first week postpartum).
9
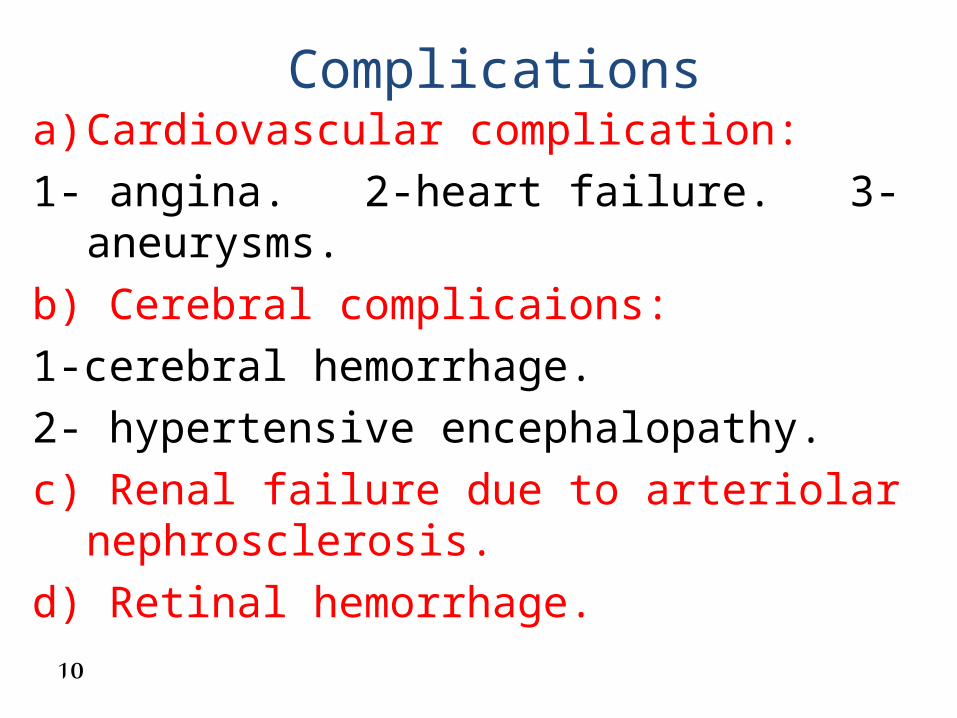
Complications a) Cardiovascular complication:1- angina. 2-heart failure. 3-aneurysms.b) Cerebral complicaions:1-cerebral hemorrhage. 2- hypertensive encephalopathy.c) Renal failure due to arteriolar nephrosclerosis.d) Retinal hemorrhage.
10

Diagnostic studies• 1-urin analysis:a) Increase Urinary excretion of catecholamines or its
metabolites (VMA) confirms pheochromocytoma.b) Presence of hematuria , proteinuria and casts suggests
primary renal disease.• 2- blood analysis:a) Increase BUN and creatinine suggest renal disease.b) Hypokalemia suggests primary hyperaldosteronism or
cushing‘s syndrome.c) Increase serum cortisol confirms cushing‘s syndrome.
11
Diagnostic studies cont.…
• 3- ECG: may reveal left ventricular hypertrophy or
ischemia .• 4- CT scane or MRI: may be done to confirm the diagnosis of
secondary or complicated HTN .
12
Treatment • BP GOAL <140/90 mm Hg . <130/80 mm Hg if DM or renal disease.• More than 2/3 of hypertensive patients can‘t be
controlled on one drug and will require 2 or more agents from different classes.
13
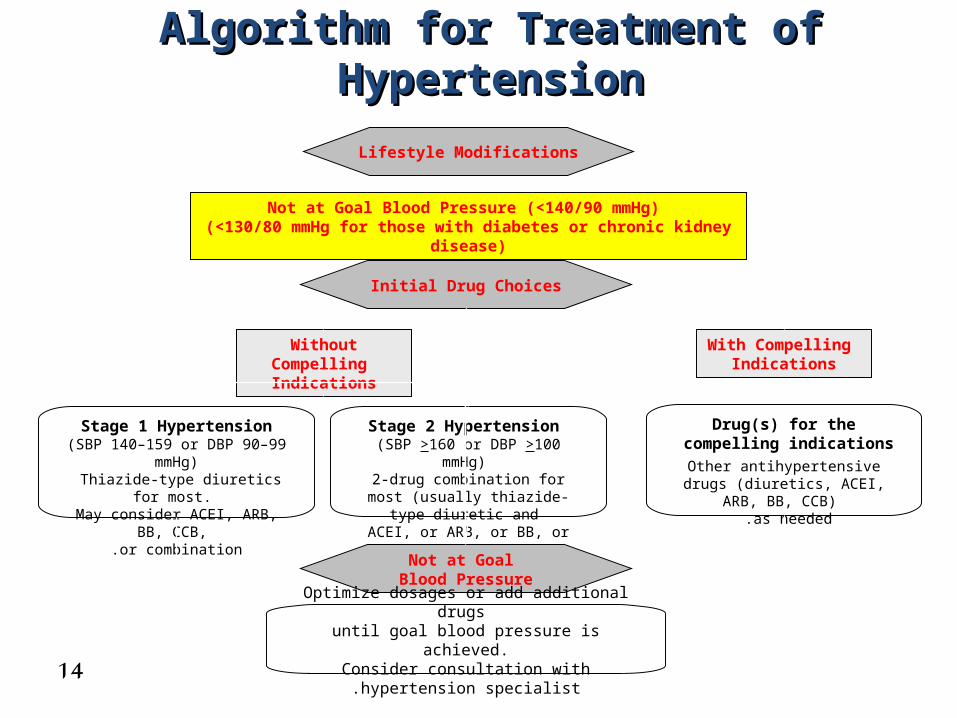
Algorithm for Treatment of HypertensionAlgorithm for Treatment of Hypertension
Not at Goal Blood Pressure (<140/90 mmHg) (<130/80 mmHg for those with diabetes or chronic kidney disease)
Initial Drug Choices
Drug(s) for the compelling indications
Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB)
as needed .
With Compelling Indications
Lifestyle Modifications
Stage 2 Hypertension (SBP >160 or DBP >100 mmHg)
2-drug combination for most (usually thiazide-type diuretic and
ACEI, or ARB, or BB, or CCB)
Stage 1 Hypertension(SBP 140–159 or DBP 90–99
mmHg) Thiazide-type diuretics for most.
May consider ACEI, ARB, BB, CCB,
or combination.
Without Compelling Indications
Not at Goal Blood Pressure
Optimize dosages or add additional drugs until goal blood pressure is achieved.
Consider consultation with hypertension specialist.
14
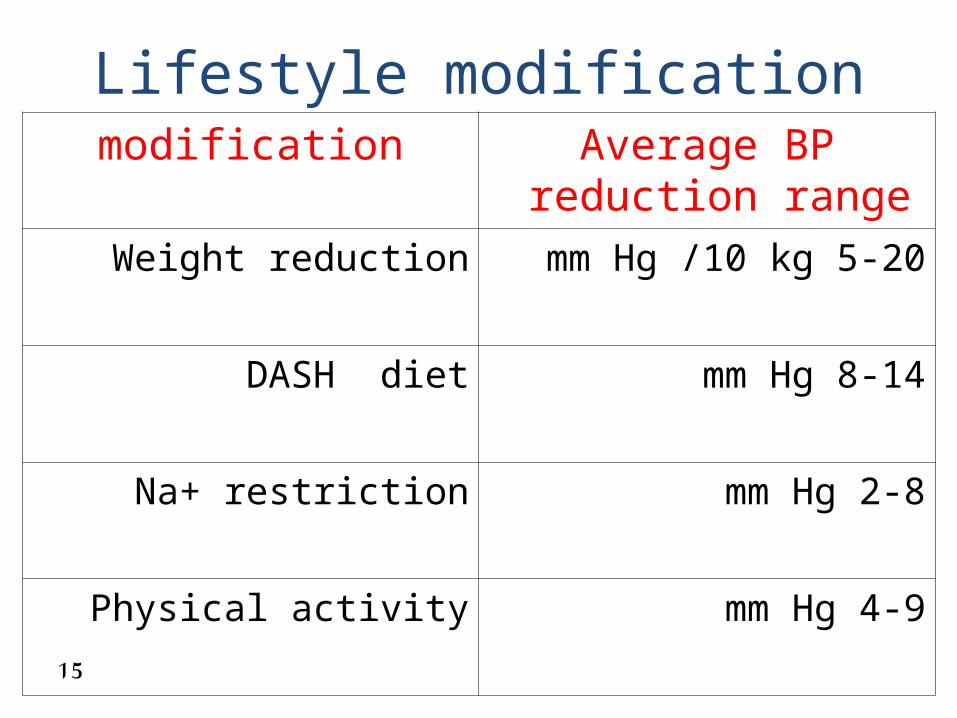
Lifestyle modificationmodification Average BP reduction
range
Weight reduction 5-20 mm Hg /10 kg
DASH diet 8-14 mm Hg
Na+ restriction 2-8 mm Hg
Physical activity 4-9 mm Hg
15
Ischemic heart disease• BBs are DOC due to ↓ HR ( ↓ of MO2).• If BBs are contraindicated such as high degree AV blook ,
sick sinus syndrome give CCB .• Treatment include smoking cessation , ttt DM , Lipid
lowering , antiplatlets , wt reduction.• If BP is not controlled with BB alone, add CCB
(dihydropyridine is preferred for combination ) DHP CCB ↓ total peripheral resistance but NDHP CCB will also ↓ HR more if added to BB sever bradycardia or heart blook may occur.
• If BP is still not controlled on BB & CCB , add nitrate.
16
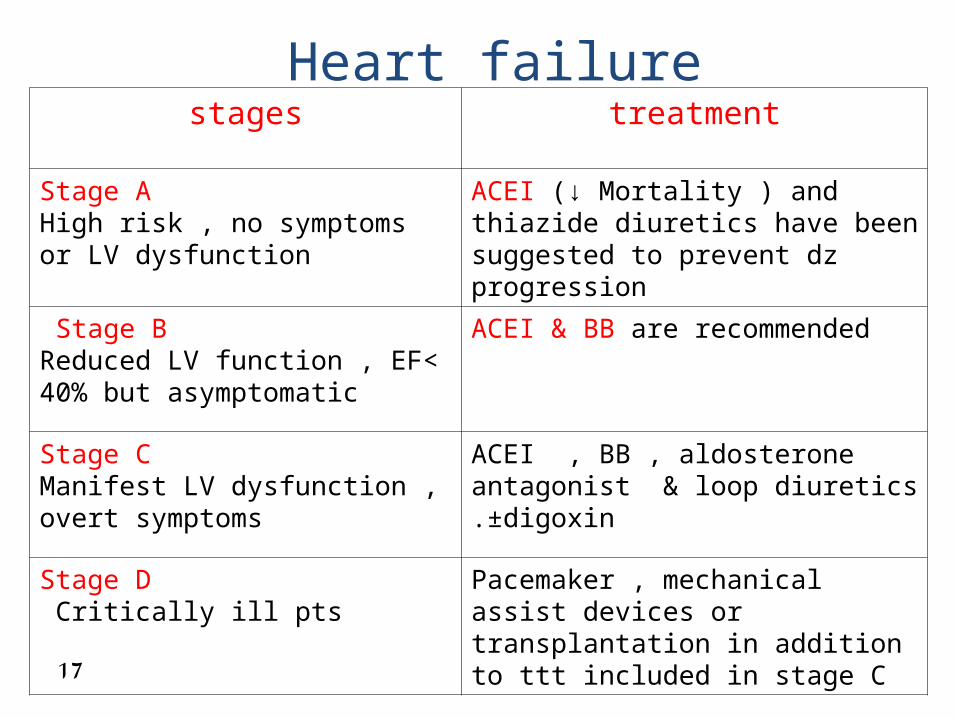
Heart failure stages treatment
Stage AHigh risk , no symptoms or LV dysfunction
ACEI (↓ Mortality ) and thiazide diuretics have been suggested to prevent dz progression
Stage B Reduced LV function , EF< 40% but asymptomatic
ACEI & BB are recommended
Stage CManifest LV dysfunction , overt symptoms
ACEI , BB , aldosterone antagonist & loop diuretics ±digoxin.
Stage DCritically ill pts
Pacemaker , mechanical assist devices or transplantation in addition to ttt included in stage C
17
Diabetes /HTN• The coexistence of HTN in diabetes is particularly
pernicious b/c of the strong linkage of the two condition with all ( CVD , Stroke , renal dz ,and retinopathy).
• American Diabetics Association(ADA) state that BP goal in DM is 130/80 mm Hg or lower.
• Treatment: many agent are used (ACEI , BB , CCB , Diuretics)difficult to specify one b/c most diabetic pts require 2 or more drugs.
• ACEI is important component to control BP in diabetic pts can be used alone or combined with other agents esp.diuretic.
18
.... Diabetes /HTN cont• The ADA has recommended ACEI for diabetics
pts >55 years at high risk for CVD and BBs for those with known CAD.
• The ADA recommended both ACEI and ARB for use in type 2 diabetic pts with CKD b/c these agents delay the deterioration in GFR and worsening of albuminuria.
19

Chronic kidney disease • Many studies found that ACEI or ARB are more
effective in slowing progression of CKD.• Goal BP : <130/80 mm Hg .• ACEI+diuretic (loop is better) or ARB +loop diuretic. central alpha -2 agonists as clonidine appear to
the safest in dialysis population.Transdermal clonidine up to 1.2 mg/day as
monotherapy in one short term study was successful .
20
stroke• The management of BP during an acute stroke remain
controversial b/c BP is high immediately post –stroke period as a compensatory physiologic response to improve cerebral perfusion . If you reduce BP may lead to neurologic deterioration .
• American Stroke Association has a guideline SBP>220 mm Hg or DBP >120-140 mmHg ↓ BP by approx 10-15 % and monitor for neurologic deterioration.
• If DBP>140 mm Hg give IV nitropusid carefully to ↓ BP by 10-15% .
• BP affect the use of thrombolytic agents in ischemic stroke .SBP>185mm Hg or DBP>110 mm Hg is contraindication to use tPA within first 3h of attack, should ↓BP first to prevent intracerebral bleeding.
21
Black people
• HTN is more common , more severe , develop at earlier age .
• The pathogenesis of HTN in different racial subgroups may be due to contribution factors such as salt , stress , cv reactivity , hormonal system and socioeconomic condition .
• CCB or thiazide is effective in these people.
22
Left ventricular hypertrophy• Most antihypertensive agents produces LVH
regression .• New trend : the most consistent reduction in LV mass was
achieved with ACEI. the intermediate benefits with diuretics and CCB . the least reduction with BB .Significant LV mass reduction was also achieved
with Losartan .23

HTN in older people
• With age SBP continue to rise , DBP rises until age of 55 then it decreases due to central arterial stiffness.(ISH).
• Increase in age ------- postural hypotension .• Geriatric > 65 yo the preferred agent is CCB .
24
Orthostatic hypotension• Present when there is a supine to standing BP
↓> 20 mm Hg systolic or > 10 mm Hg diastolic.• Causes:Sever volume depletion , baroreflex dysfunction ,
autonomic insufficiency. venodilator such as alpha blockers , alpha-beta
blockers , and nitrates may further aggravate orthostatic hypotension .
25

Urinary Outflow Obstruction (BPH)
• Use alpha 1 blockers such as terazosin , doxazosin , or prazosin .
• They indirectly dilate prostatic and urinary sphincter smooth muscle and also lower BP .
Precautions : 1- first dose phenmenon (a syncopal epiaode occur
30-90 min of the first dose .2- palpitation & sweating to minimize this effect the
first dose should be limited to 1 mg of each agent & given at bedtime.
26
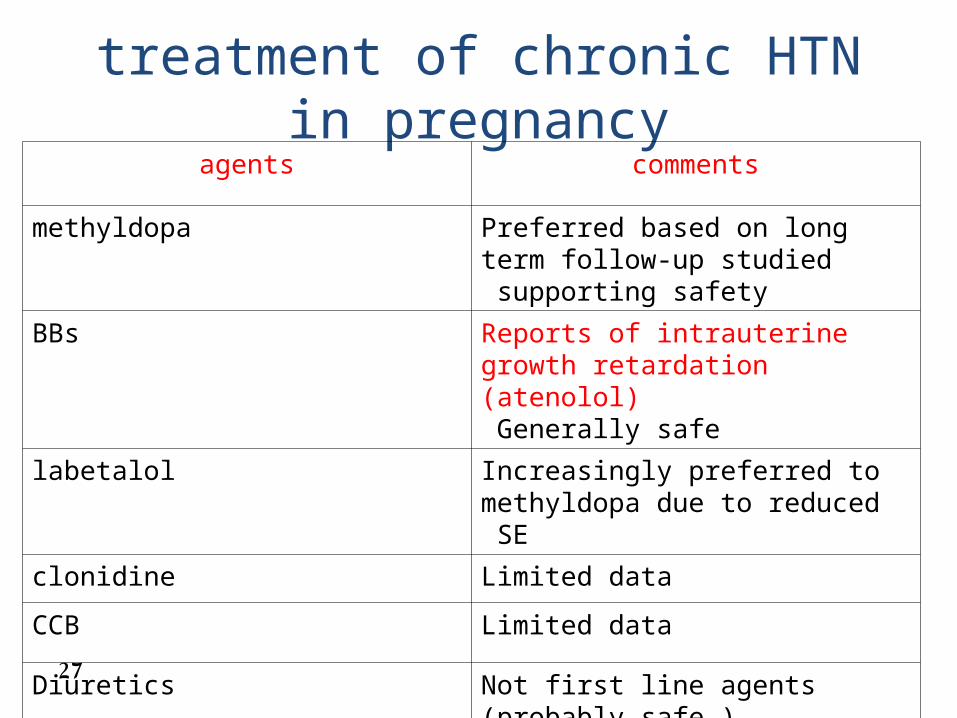
treatment of chronic HTN in pregnancy
agents comments
methyldopa Preferred based on long term follow-up studied supporting safety
BBs Reports of intrauterine growth retardation (atenolol)Generally safe
labetalol Increasingly preferred to methyldopa due to reduced SE
clonidine Limited data
CCB Limited data
Diuretics Not first line agents (probably safe )
ACEIs , ARBs Contraindicated (reported fetal toxicity and death)27
HTN during lactation• All antihypertensive agents are excreted into human
milk.• In mother with stage 1 HTN who wish to breast feed for
a few months , it might be prudent to withhold antihypertensive with close monitoring of BP .resume drug after d/c of breast feeding .
• No short term SE have been reported from exposure to methyldopa .
• Propranolol & Labetalol are preferred if BB is indicated .• Avoided ACEI & ARB .• Diuretic may ↓ milk volume .
28

Renal transplantation• HTN is a relatively common occurence in organ
transplantation.• In kidney allograft HTN prevalence approx 65%.• Mechanism: vasoconstriction and long term vascular structural
changes caused by chronic immunosuppressive such as cyclosporine , Tacrolimus and corticosteroid .
the high risk of graft occlusion and CV events has suggested that BP should be lowered to 130/80 mm Hg or less.
No particular class is superior , combination agent is necessary.
Monitor K and Src particularly when ACEI or ARB are used.
29
Renal transplantation cont.…• In practice : I see CCB is effective in HTN in
transplant.• National kidney foundation Guidelines : most transplant centers use dihydropyridine CCB for
initial therapy , since these agents dilate the afferent arteriole, therapy ameliorating vasoconstricton afferent arteriole induced by calcineurin inhibitors (cyclosporin and tacrolimus).
a recent randomized study comparing nifedipine and lisinopril demonstrated improved kidney outcomes (lower creatinine and improved GFR at 2 years ) with use of nifedipine.
30
Hypertensive emergency• Characterized by sever elevation in BP >180/120
mm Hg complicated by evidence of impending or progressive target organ damage .
• Target organ damage :a)Heart : LVH , angina or MI , HF .b)Brain : stroke or TIA , retinopathy .c) Kidney : GFR , chronic kidney disease.• Pts must be admitted to ICU for BP monitoring
and administration IV antihypertensive agent .
31
Hypertensive emergency cont.…• Initial goal is to reduce BP no more than 25%
within minutes to 1 hr, then if stable, to 160/110 mm Hg within the next 2-6 hrs(avoid excessive fall in BP ---to avoid precipitation of renal , cerebral or coronary ischemia. If the pts tolerated this BP and clinically stable , further gradual reduction toward a normal BP within the next 24-48 hrs .
32

Parental drugs for treatment of hypertensive emerenciesDrug Dose Onset of action Special indication
vasodilators Most use Caution with high ICP or azotemia
Na nitroprusside o.25-10 µg/kg/min as IV infusion
immediate
nitroglycerin 5-100 µg/min as IV infusion
2-5 min Coronary ischemia
Hydralazine hydrochloride
10-20 mg IV 10-40 mg IM
10-20 min IV 20-30 min IM
eclampsia
Adrenergic inhibitor
Labetalol hydrochloride
20-80 mg IV bolus every 10 min 0.5-2 mg/min IV infusion
5-10 min Most use except acute HF
Esmolol hydrochloride
250-500 µ/kg/min IV bolus then 50-100 µg/kg min by infusion
1-2 min Aortic dissection, Perioperative
phentolamine 5-15 mg IV bolus 1-2 min Catecholamine excess33
33
Hypertensive urgency • Severe elevation of BP without target organ
damage . E.g., upper level of stage 2 HTN with severe headache , SOB , epistaxis or severe anxiety.
• Either non compliant or inadequately treatment .• Treatment : oral , short acting agents such as captopril ,
labetalol , or clonidine followed by several hrs of observation at ED. If stable , reinstitute previous medications , combination .
34

Diuretics 1 – K sparing diuretics :• weak when used alone , combined with Thiaz/ loop
to prevent ↓ K .• Avoided in ARF .2-thiaz diuretics:• initial therapy is more effective than loop .• Efficacy @ Cr CL > 30 ml/min .• Low dose 12.5 mg HCTZ , not > 50 mg .3- loop diuretics:• Indicated : loss of THIAZ effect & Cr CL < 30 ml/min.• Expensive than THIAZ.
35
BBsThree pharmacodynamic diffrences :1- cardioselectivity =affinity for B1 than B2
(Atenolol , metoprolol , bisoprolol & acebutolol) dose dependent phenomenon , effect is lost at higher doses .
2- intrinsic sympathomimetic activity (ISA)= these agents release catecholamines to maintains normal basal sympathetic tone . Not safer to use in HF , sinus bradycardia . (acebutolol , carteolol , penbutolol , pindolol ) .
36

BBs cont.…3- membrane-stabilizing action (MSA) =(or quinidine
like effect ) on cardiac cell if large enough doses are given (antidysrhythmic effect ) ,the dose exceeds that used in HTN.
• all BBs share this property .• Only (propranolol , sotolol , acebutolol ) indicated
for arrythmias.• Precautions : no BB is totally safe in pts with bronchospasm . abrupt cessation may produce unstable angina , MI ,
taper dose over 14 days before d/c the drug .37

conclusion• HTN is not a disease but an important risk factor
for CV and cerebrovascular disease.• Education of the pt is necessary on longterm
importance of treatment and lifestyle changes.• There is no ideal antihypertensive drug that
reduces BP without causing SE .• It is imortant to match the antihypertensive to
the patient‘s other coexisting disease states to gain the most benefit .
38
references• Daniel H.cooper. The Washington Manual Of
Medical Therapeutics. Lippincolt Williams and Wilkins , Baltimore , MD . 32nd ED , 2008 ;chapter 4 , page ; 72-91 .
• http://www.emedicinehealth.com/high_blood_pressure/article_em.htm.
Richard A Helms PharmD, BCNSP; David J Quan PharmD. Text Book of Therapeutics. Disease and Drug Management. LWW,
8th Edition ( 2005 ), Chapter 20, hypertension pg : 565 - 485.
39
























![Jihad'e Islami [Urdu]](https://img.pdfslide.us/doc/110x75/577cd86d1a28ab9e78a12842/jihade-islami-urdu.jpg)


