Embed Size (px)
Citation preview
Hypertension Controversies:
SPRINTing to New Goals
Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland Clinic
Disclosures
• Lauren Wolfe and Diana Isaacs have nothing to
disclose.
Objectives
• Compare and contrast published guidelines for the
treatment of patients with hypertension.
• Evaluate the literature utilized to determine guideline
recommendations.
• Discuss the implications of the SPRINT trial in
establishing blood pressure goals for different patient
populations.
• Design a patient centered therapy plan based on
published guidelines and clinical trials.
AL is a 65 year old African American male. AL’s in-office BP today is 148/88mmHg and same on repeat. One month ago, AL’s BP was 146/88mmHg.
• PMH: Sleep apnea, allergic rhinitis
• Meds: Loratadine 10mg po daily
• No known drug allergies/ADR’s
• Height: 5’11” 225lbs, BMI=31.4
• Family history: mother with type 2 diabetes
• Social history: non-smoker, frequently eats out at restaurants, adds salt to food
Patient Case
• What is AL’s BP goal?
• How would you treat AL’s BP?
• How would your treatment plan differ if AL had diabetes? CAD?
• Would the goal BP change if AL was over 80 years old?
Questions to Think About
Definition/Epidemiology
• HTN defined: BP≥140/90mm Hg on repeated exam
• About 1/3 of adults have HTN
– Most common condition seen in primary care
• Close relationship with high BP and risk of MI, stroke,
renal failure and death
• Events lowest at BP=115/75 mmHg
– CV and stroke events double for each increase of 20/10mmHg
in SBP/DBP
Weber MA, et al. J Clin Hypertens. 2014 Jan;16(1):14-26.
James PA, et al. JAMA. 2014;311(5):507-520.
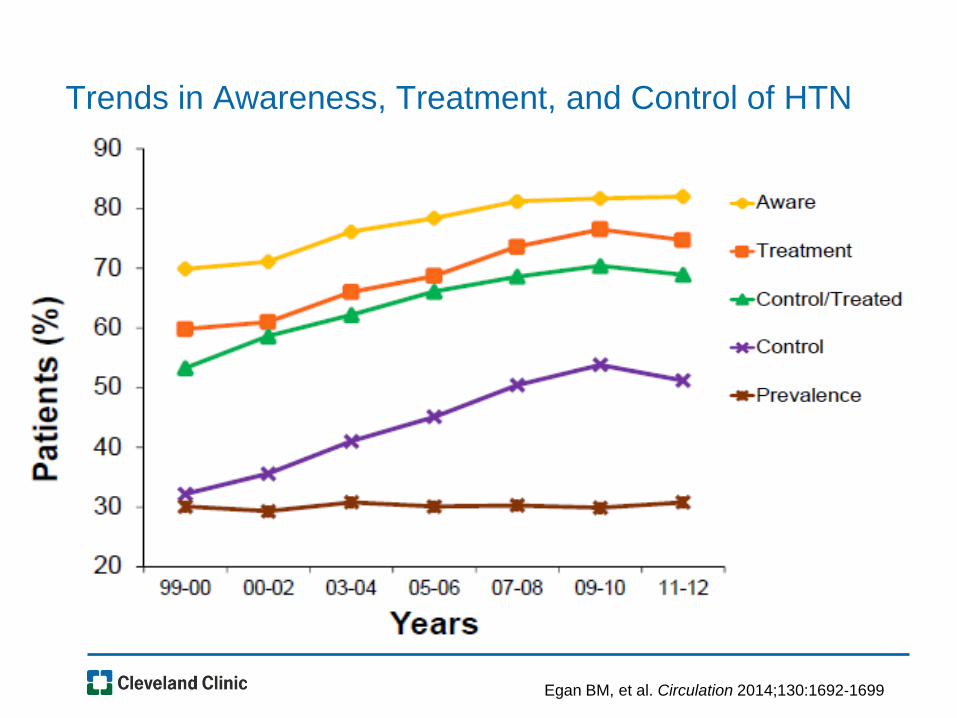
Trends in Awareness, Treatment, and Control of HTN
Egan BM, et al. Circulation 2014;130:1692‐1699
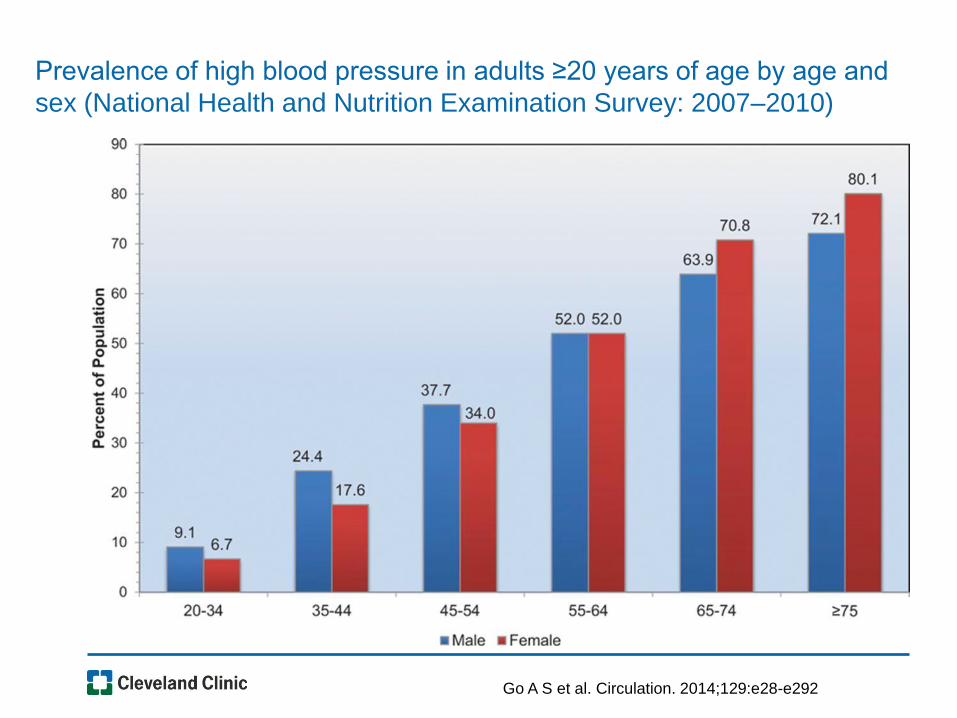
Go A S et al. Circulation. 2014;129:e28-e292
Prevalence of high blood pressure in adults ≥20 years of age by age and
sex (National Health and Nutrition Examination Survey: 2007–2010)
Joint National Committee (JNC7) Guidelines
-Published in 2003
We anxiously waited for JNC8, but the years
kept passing…
And then all of a
sudden!
A Flood of HTN Guidelines
• Kidney Disease: Improving Global Outcomes (KDIGO)-2012
• European Society of Cardiology/European Society of Hypertension(ESC/ESH)-2013
• American College of Cardiology/American Heart Association/Centers for Disease Control (ACC/AHA/CDC) Scientific Advisory-2013
• 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults-2013 (“JNC8”)
• American Society of Hypertension/International Society of Hypertension (ASH/ISH)-2013
• AHA/ACC/ASH Treatment of Hypertension and Coronary Artery Disease-2015
• Canadian Hypertension Educational Program (CHEP)-2016
• American Diabetes Association (ADA) Standards of Care-2017
• American College of Physicians/American Association of Family Physicians (ACP/AAFP) Pharmacologic Treatment of Hypertension in Adults Aged ≥ 60 Ann Intern Med-2017
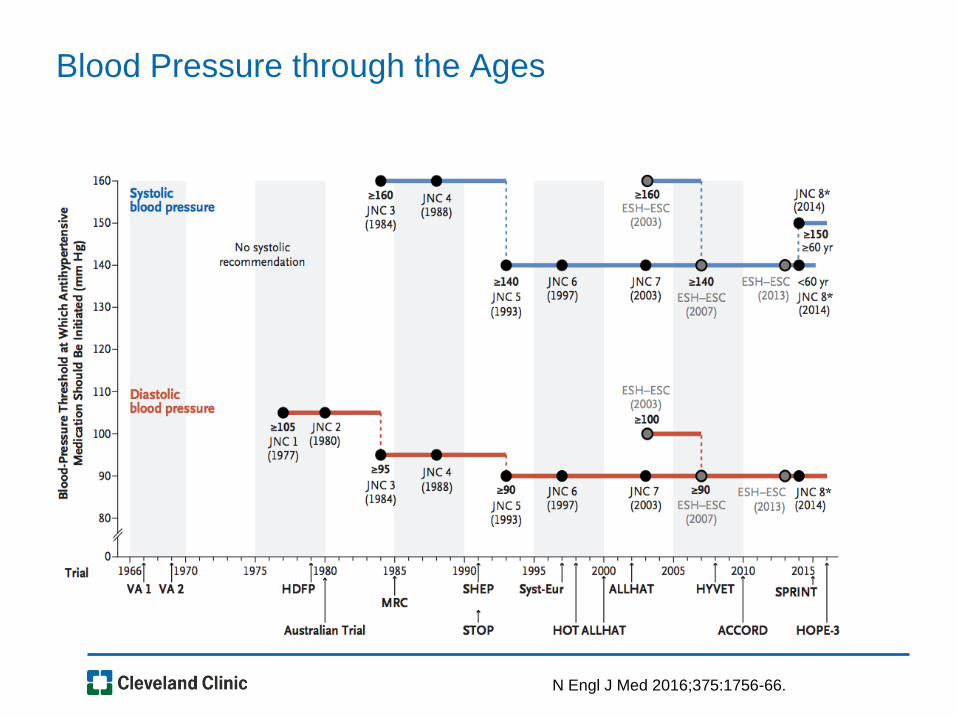
Blood Pressure through the Ages
N Engl J Med 2016;375:1756-66.
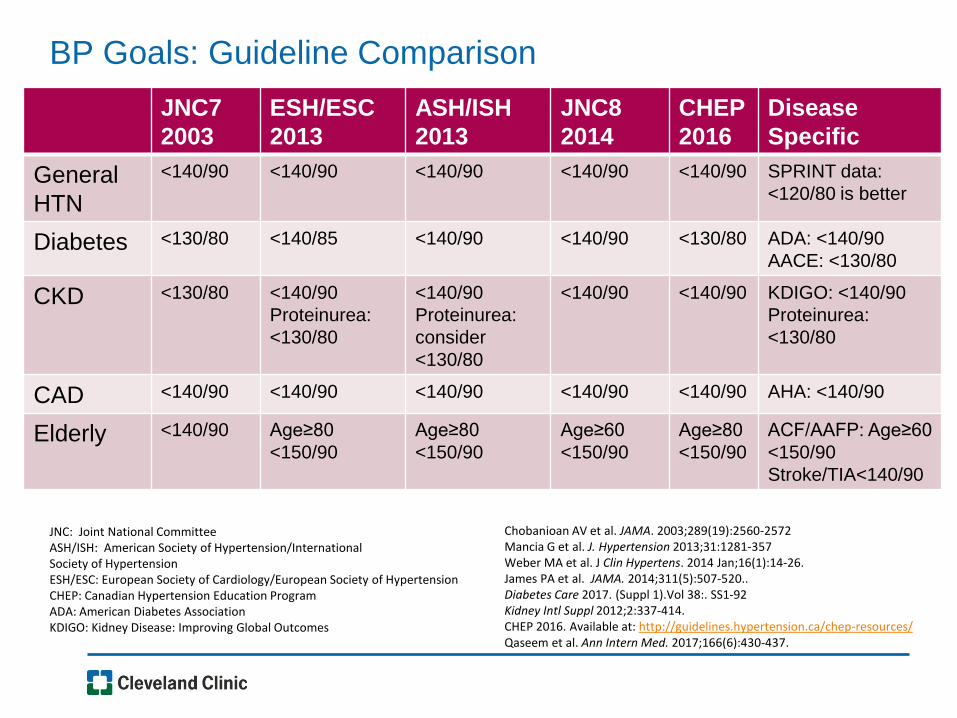
BP Goals: Guideline Comparison
JNC7
2003
ESH/ESC
2013
ASH/ISH
2013
JNC8
2014
CHEP
2016
Disease
Specific
General
HTN
<140/90 <140/90
<140/90 <140/90
<140/90 SPRINT data:
<120/80 is better
Diabetes <130/80 <140/85 <140/90 <140/90
<130/80 ADA: <140/90
AACE: <130/80
CKD <130/80 <140/90
Proteinurea:
<130/80
<140/90
Proteinurea:
consider
<130/80
<140/90
<140/90 KDIGO: <140/90
Proteinurea:
<130/80
CAD <140/90 <140/90 <140/90 <140/90 <140/90 AHA: <140/90
Elderly <140/90 Age≥80
<150/90
Age≥80
<150/90
Age≥60
<150/90
Age≥80
<150/90
ACF/AAFP: Age≥60
<150/90
Stroke/TIA<140/90
Chobanioan AV et al. JAMA. 2003;289(19):2560-2572 Mancia G et al. J. Hypertension 2013;31:1281-357 Weber MA et al. J Clin Hypertens. 2014 Jan;16(1):14-26. James PA et al. JAMA. 2014;311(5):507-520.. Diabetes Care 2017. (Suppl 1).Vol 38:. SS1-92 Kidney Intl Suppl 2012;2:337-414. CHEP 2016. Available at: http://guidelines.hypertension.ca/chep-resources/ Qaseem et al. Ann Intern Med. 2017;166(6):430-437.
JNC: Joint National Committee ASH/ISH: American Society of Hypertension/International Society of Hypertension ESH/ESC: European Society of Cardiology/European Society of Hypertension CHEP: Canadian Hypertension Education Program ADA: American Diabetes Association KDIGO: Kidney Disease: Improving Global Outcomes
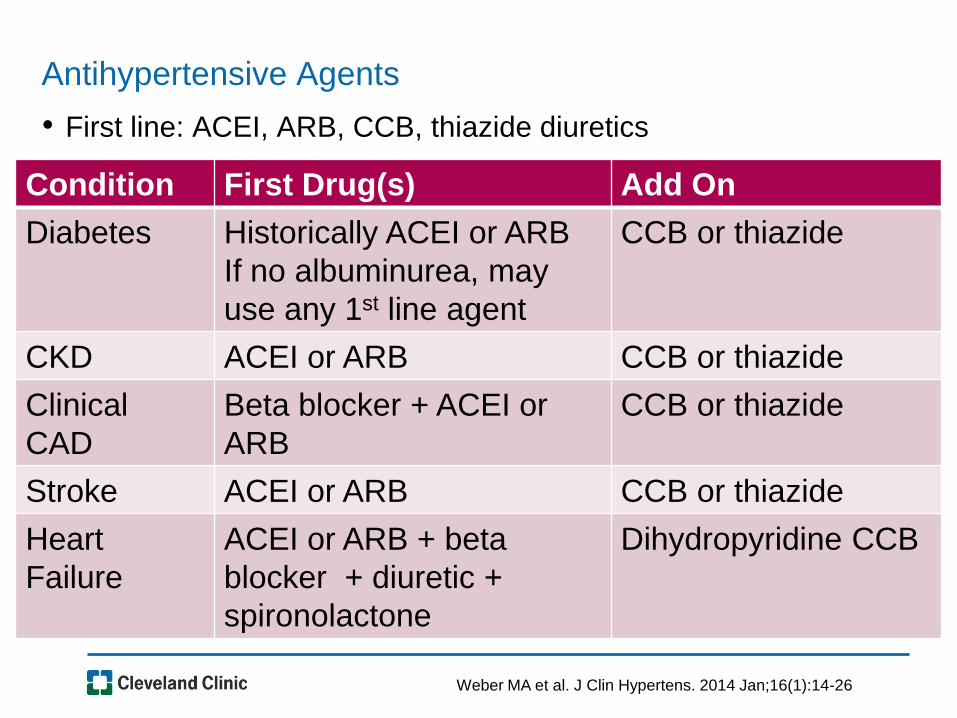
Antihypertensive Agents
• First line: ACEI, ARB, CCB, thiazide diuretics
Condition First Drug(s) Add On
Diabetes Historically ACEI or ARB
If no albuminurea, may
use any 1st line agent
CCB or thiazide
CKD ACEI or ARB CCB or thiazide
Clinical
CAD
Beta blocker + ACEI or
ARB
CCB or thiazide
Stroke ACEI or ARB CCB or thiazide
Heart
Failure
ACEI or ARB + beta
blocker + diuretic +
spironolactone
Dihydropyridine CCB
Weber MA et al. J Clin Hypertens. 2014 Jan;16(1):14-26
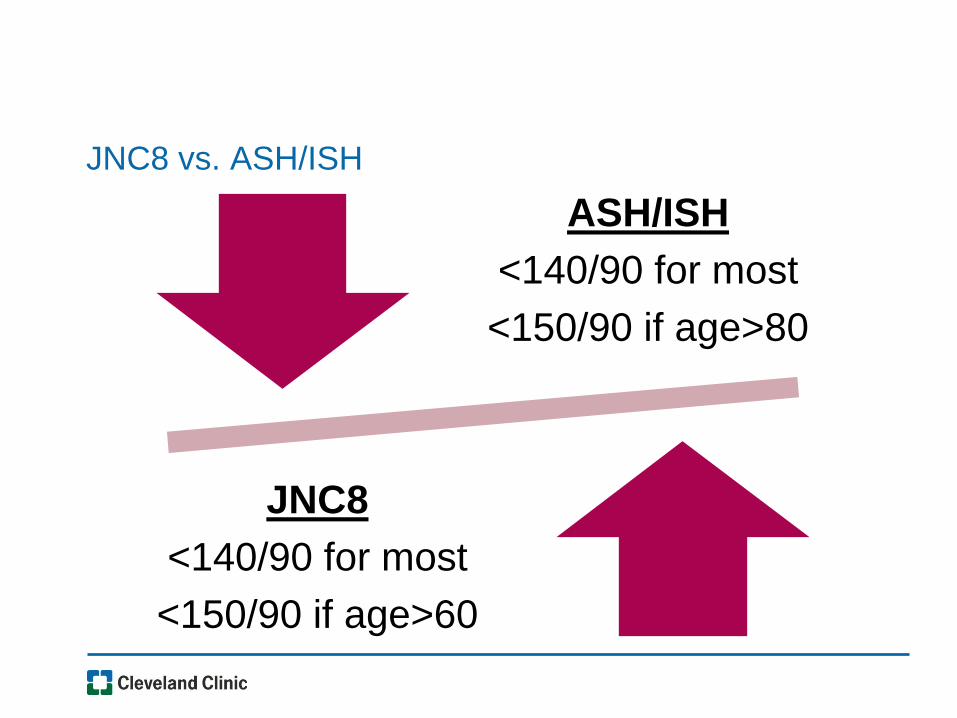
JNC8 vs. ASH/ISH
ASH/ISH
<140/90 for most
<150/90 if age>80
JNC8
<140/90 for most
<150/90 if age>60
JNC8: A Unanimous Consensus?
• Agreement on all but 1 recommendation
– SBP from 140 to 150 mm Hg in persons aged 60 years or older without DM or CKD
• “The majority embraced the view that in the absence of definitive evidence, increasing the SBP goal was the optimum approach”
• The minority “concluded that the evidence for increasing a BP target in high-risk populations should be at least as strong as the evidence required to decrease the recommended BP target”
– BP goal should be <140/90 in patients <80 and <150/90 in patients ≥80
Ann Intern Med, 2014;160:499-503.
Definition of Elderly
• Merriam-Webster: “being past middle age”
• Most countries have accepted the age of 65 years as
the definition of 'elderly’
• Lack of United Nations standard numerical criterion,
however agreed cutoff is ≥ 60 years of age
• By 2050,1/5 people will be ≥ 60 years of age
World Health Organization. http://www.who.int/healthinfo/survey/ageingdefnolder/en/. Accessed 2017 April 4.
Merriam-Webster . https://www.merriam-webster.com/dictionary/elderly. Accessed 2017 April 4.
Hypertension in the Elderly
• Systolic blood pressure (SBP) increases steadily with age
– Diastolic BP (DBP) increases until age 55, then declines
• Importance of BP as a cardiovascular risk has been
demonstrated to shift from DBP to SBP with advancing age
• Isolated systolic hypertension
– Most common form by age 50
– Increased risk of target organ damage and adverse health outcomes
– Treatment associated with reduced risk for dementia, stroke, MI, and CHF
Circulation. 2011;124:e175.
How Low is Too Low?
• Consistent relationship between degree of BP
elevation and risk of CVD and stroke
– Treating to lower target levels may not result in fewer CV events
–J-shaped association: CV risk at both low and high BP
– Overaggressive treatment can lead to organ hypoperfusion
• Excessive BP lowering may impair quality of life
– Orthostatic hypotension more common and associated with
increased CV risk and fall risk
– In the U.S., almost 40% of people age 60 years and older take
at least 5 medications
Clinical Interventions in Aging 2013:8;1505-1517. Circulation. 2011;124:e175.
Brocklehurst’s Textbook of Geriatric Medicine. 2010:880-885.
Literature Behind JNC8
SHEP Syst-Eur JATOS
VALISH HYVET CARDIO-
SIS
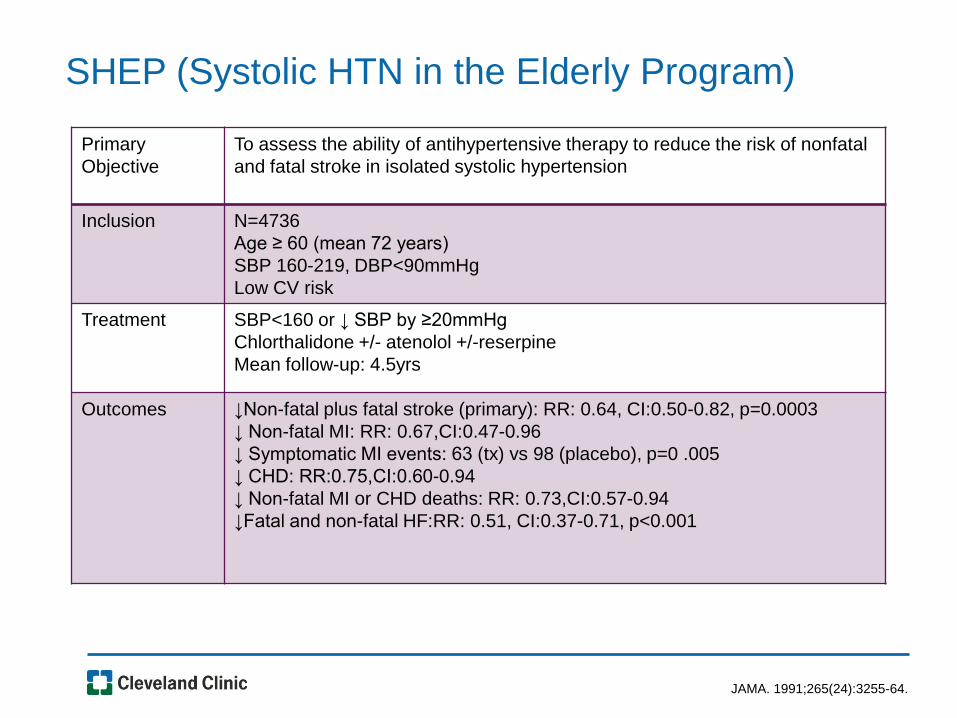
JAMA. 1991;265(24):3255-64.
Primary
Objective
To assess the ability of antihypertensive therapy to reduce the risk of nonfatal
and fatal stroke in isolated systolic hypertension
Inclusion N=4736
Age ≥ 60 (mean 72 years)
SBP 160-219, DBP<90mmHg
Low CV risk
Treatment SBP<160 or ↓ SBP by ≥20mmHg
Chlorthalidone +/- atenolol +/-reserpine
Mean follow-up: 4.5yrs
Outcomes ↓Non-fatal plus fatal stroke (primary): RR: 0.64, CI:0.50-0.82, p=0.0003
↓ Non-fatal MI: RR: 0.67,CI:0.47-0.96
↓ Symptomatic MI events: 63 (tx) vs 98 (placebo), p=0 .005
↓ CHD: RR:0.75,CI:0.60-0.94
↓ Non-fatal MI or CHD deaths: RR: 0.73,CI:0.57-0.94
↓Fatal and non-fatal HF:RR: 0.51, CI:0.37-0.71, p<0.001
SHEP (Systolic HTN in the Elderly Program)
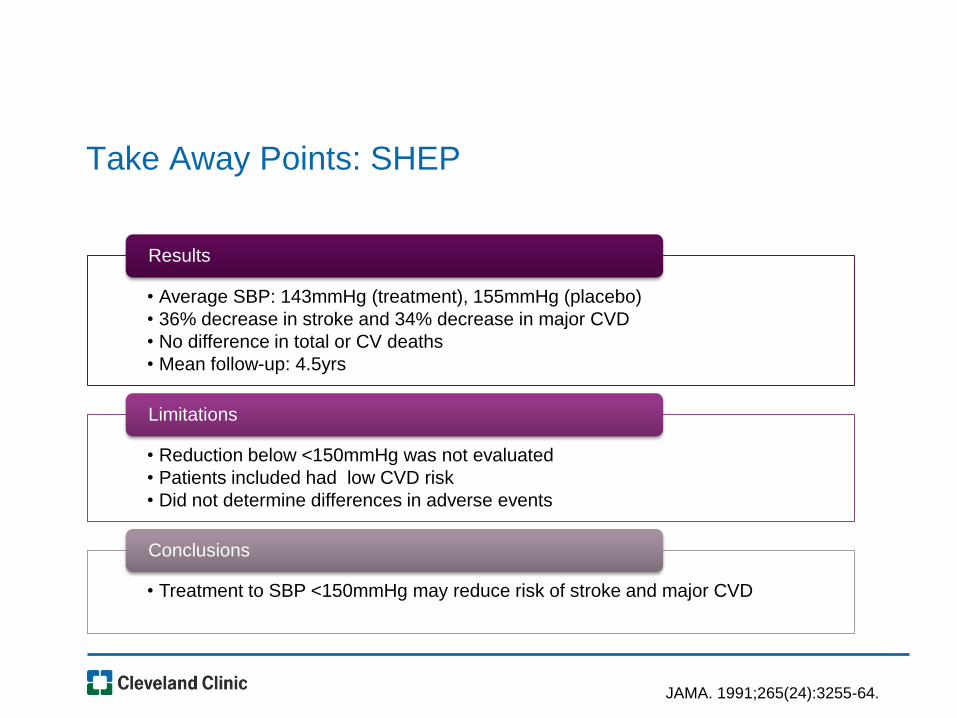
Take Away Points: SHEP
• Average SBP: 143mmHg (treatment), 155mmHg (placebo)
• 36% decrease in stroke and 34% decrease in major CVD
• No difference in total or CV deaths
• Mean follow-up: 4.5yrs
Results
• Reduction below <150mmHg was not evaluated
• Patients included had low CVD risk
• Did not determine differences in adverse events
Limitations
• Treatment to SBP <150mmHg may reduce risk of stroke and major CVD
Conclusions
JAMA. 1991;265(24):3255-64.
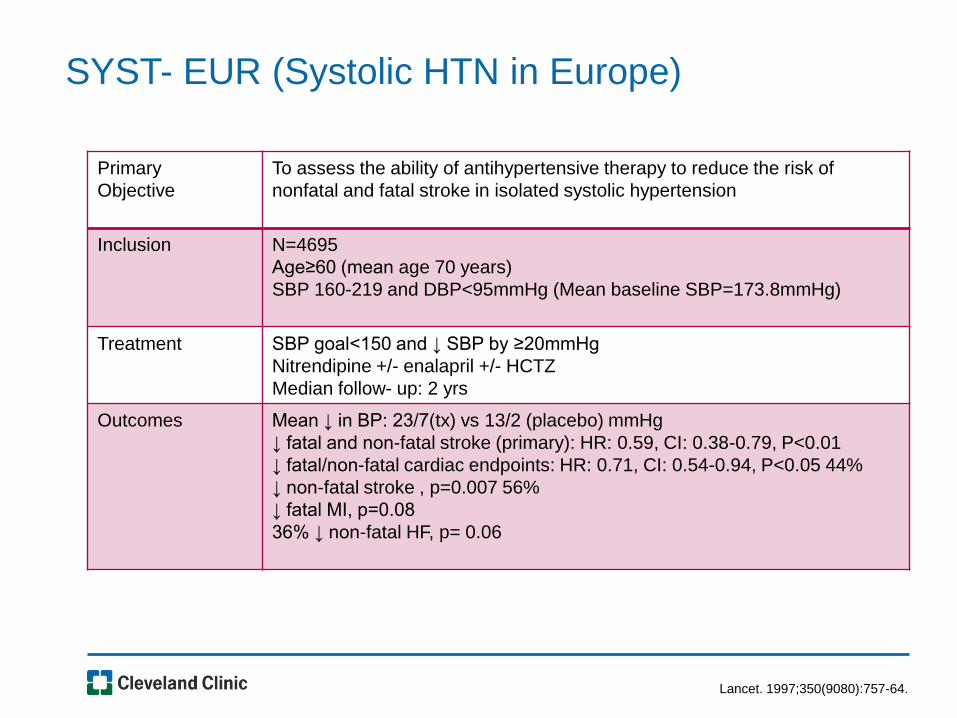
Lancet. 1997;350(9080):757-64.
Primary
Objective
To assess the ability of antihypertensive therapy to reduce the risk of
nonfatal and fatal stroke in isolated systolic hypertension
Inclusion N=4695
Age≥60 (mean age 70 years)
SBP 160-219 and DBP<95mmHg (Mean baseline SBP=173.8mmHg)
Treatment SBP goal<150 and ↓ SBP by ≥20mmHg
Nitrendipine +/- enalapril +/- HCTZ
Median follow- up: 2 yrs
Outcomes Mean ↓ in BP: 23/7(tx) vs 13/2 (placebo) mmHg
↓ fatal and non-fatal stroke (primary): HR: 0.59, CI: 0.38-0.79, P<0.01
↓ fatal/non-fatal cardiac endpoints: HR: 0.71, CI: 0.54-0.94, P<0.05 44%
↓ non-fatal stroke , p=0.007 56%
↓ fatal MI, p=0.08
36% ↓ non-fatal HF, p= 0.06
SYST- EUR (Systolic HTN in Europe)
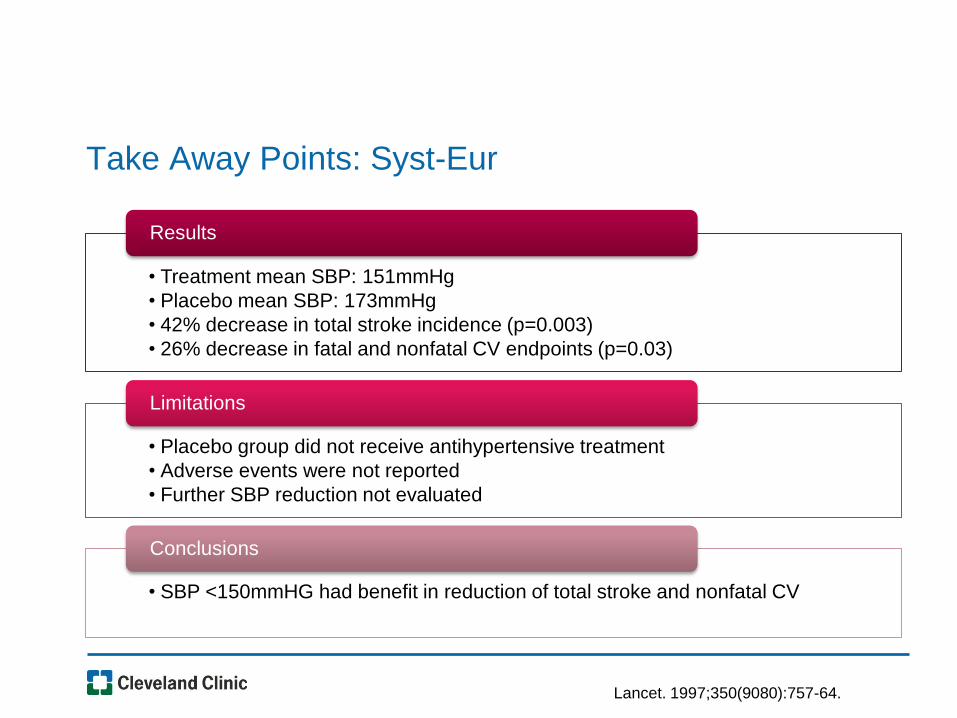
Take Away Points: Syst-Eur
• Treatment mean SBP: 151mmHg
• Placebo mean SBP: 173mmHg
• 42% decrease in total stroke incidence (p=0.003)
• 26% decrease in fatal and nonfatal CV endpoints (p=0.03)
Results
• Placebo group did not receive antihypertensive treatment
• Adverse events were not reported
• Further SBP reduction not evaluated
Limitations
• SBP <150mmHG had benefit in reduction of total stroke and nonfatal CV
Conclusions
Lancet. 1997;350(9080):757-64.
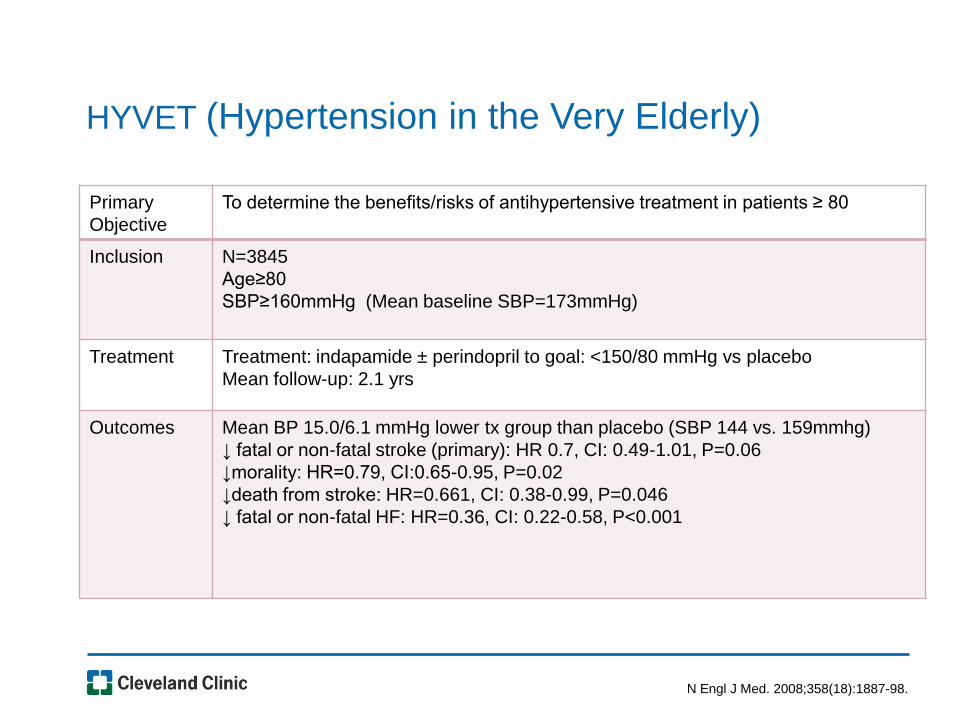
N Engl J Med. 2008;358(18):1887-98.
Primary
Objective
To determine the benefits/risks of antihypertensive treatment in patients ≥ 80
Inclusion N=3845
Age≥80
SBP≥160mmHg (Mean baseline SBP=173mmHg)
Treatment Treatment: indapamide ± perindopril to goal: <150/80 mmHg vs placebo
Mean follow-up: 2.1 yrs
Outcomes Mean BP 15.0/6.1 mmHg lower tx group than placebo (SBP 144 vs. 159mmhg)
↓ fatal or non-fatal stroke (primary): HR 0.7, CI: 0.49-1.01, P=0.06
↓morality: HR=0.79, CI:0.65-0.95, P=0.02
↓death from stroke: HR=0.661, CI: 0.38-0.99, P=0.046
↓ fatal or non-fatal HF: HR=0.36, CI: 0.22-0.58, P<0.001
HYVET (Hypertension in the Very Elderly)
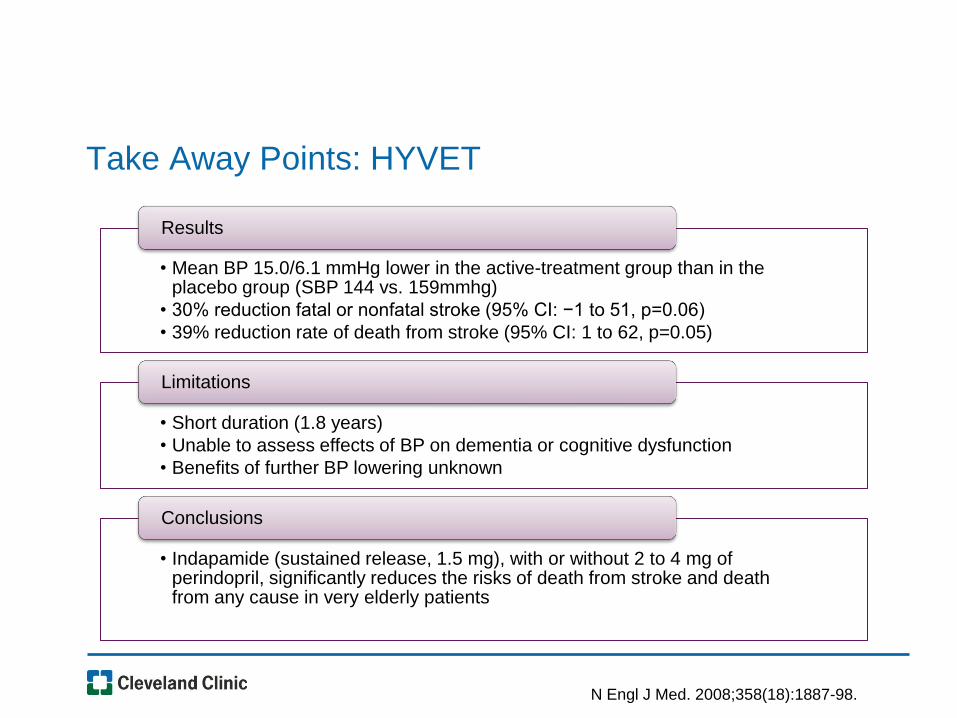
Take Away Points: HYVET
• Mean BP 15.0/6.1 mmHg lower in the active-treatment group than in the placebo group (SBP 144 vs. 159mmhg)
• 30% reduction fatal or nonfatal stroke (95% CI: −1 to 51, p=0.06)
• 39% reduction rate of death from stroke (95% CI: 1 to 62, p=0.05)
Results
• Short duration (1.8 years)
• Unable to assess effects of BP on dementia or cognitive dysfunction
• Benefits of further BP lowering unknown
Limitations
• Indapamide (sustained release, 1.5 mg), with or without 2 to 4 mg of perindopril, significantly reduces the risks of death from stroke and death from any cause in very elderly patients
Conclusions
N Engl J Med. 2008;358(18):1887-98.
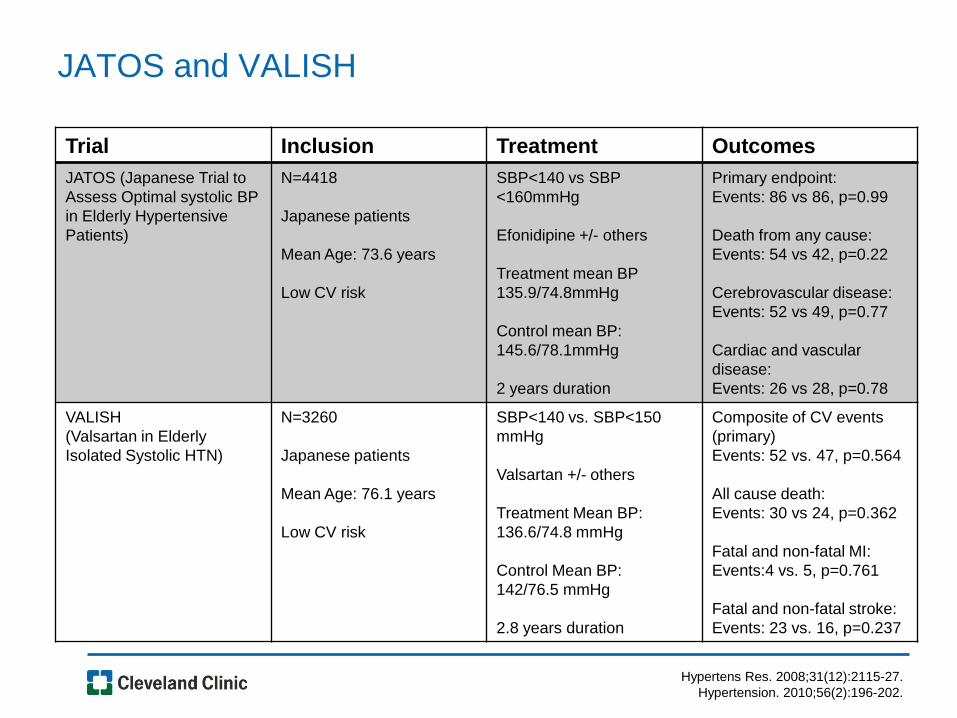
Hypertens Res. 2008;31(12):2115-27.
Hypertension. 2010;56(2):196-202.
Trial Inclusion Treatment Outcomes
JATOS (Japanese Trial to
Assess Optimal systolic BP
in Elderly Hypertensive
Patients)
N=4418
Japanese patients
Mean Age: 73.6 years
Low CV risk
SBP<140 vs SBP
<160mmHg
Efonidipine +/- others
Treatment mean BP
135.9/74.8mmHg
Control mean BP:
145.6/78.1mmHg
2 years duration
Primary endpoint:
Events: 86 vs 86, p=0.99
Death from any cause:
Events: 54 vs 42, p=0.22
Cerebrovascular disease:
Events: 52 vs 49, p=0.77
Cardiac and vascular
disease:
Events: 26 vs 28, p=0.78
VALISH
(Valsartan in Elderly
Isolated Systolic HTN)
N=3260
Japanese patients
Mean Age: 76.1 years
Low CV risk
SBP<140 vs. SBP<150
mmHg
Valsartan +/- others
Treatment Mean BP:
136.6/74.8 mmHg
Control Mean BP:
142/76.5 mmHg
2.8 years duration
Composite of CV events
(primary)
Events: 52 vs. 47, p=0.564
All cause death:
Events: 30 vs 24, p=0.362
Fatal and non-fatal MI:
Events:4 vs. 5, p=0.761
Fatal and non-fatal stroke:
Events: 23 vs. 16, p=0.237
JATOS and VALISH
Take Away Points: JATOS and VALISH
Hypertens Res. 2008;31(12):2115-27.
Hypertension. 2010;56(2):196-202.
• Short study durations
• Did not achieve power
• Lack of generalizability of patient population
Limitations
• Did not show a difference in primary endpoints including cerebrovascular disease, cardiac and vascular disease, or renal failure
Conclusions
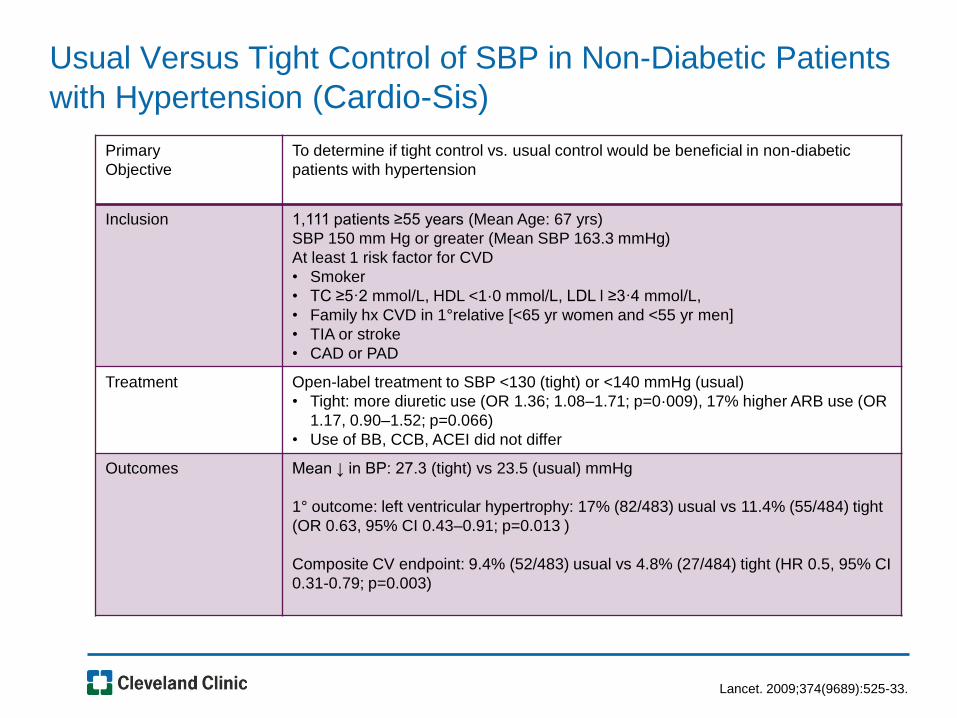
Usual Versus Tight Control of SBP in Non-Diabetic Patients
with Hypertension (Cardio-Sis)
Lancet. 2009;374(9689):525-33.
Primary
Objective
To determine if tight control vs. usual control would be beneficial in non-diabetic
patients with hypertension
Inclusion 1,111 patients ≥55 years (Mean Age: 67 yrs)
SBP 150 mm Hg or greater (Mean SBP 163.3 mmHg)
At least 1 risk factor for CVD
• Smoker
• TC ≥5·2 mmol/L, HDL <1·0 mmol/L, LDL l ≥3·4 mmol/L,
• Family hx CVD in 1°relative [<65 yr women and <55 yr men]
• TIA or stroke
• CAD or PAD
Treatment Open-label treatment to SBP <130 (tight) or <140 mmHg (usual)
• Tight: more diuretic use (OR 1.36; 1.08–1.71; p=0·009), 17% higher ARB use (OR
1.17, 0.90–1.52; p=0.066)
• Use of BB, CCB, ACEI did not differ
Outcomes Mean ↓ in BP: 27.3 (tight) vs 23.5 (usual) mmHg
1° outcome: left ventricular hypertrophy: 17% (82/483) usual vs 11.4% (55/484) tight
(OR 0.63, 95% CI 0.43–0.91; p=0.013 )
Composite CV endpoint: 9.4% (52/483) usual vs 4.8% (27/484) tight (HR 0.5, 95% CI
0.31-0.79; p=0.003)
Take Away Points: Cardio-Sis
• Tight Mean BP: 131.9/77.4mmHg
• Standard Mean BP: 135.6/75mmHg
• 37% decrease in left ventricular hypertrophy
• 50% decrease composite endpoint
Results
• Open-label design
• 2 year duration
• Caucasian patients only
• Both groups reached BP <140/90
Limitations
• Primary endpoint improvement with lower BP
Conclusions
Lancet. 2009;374(9689):525-33.
Literature Not Referenced by JNC8
FEVER SPS3
INVEST SPRINT
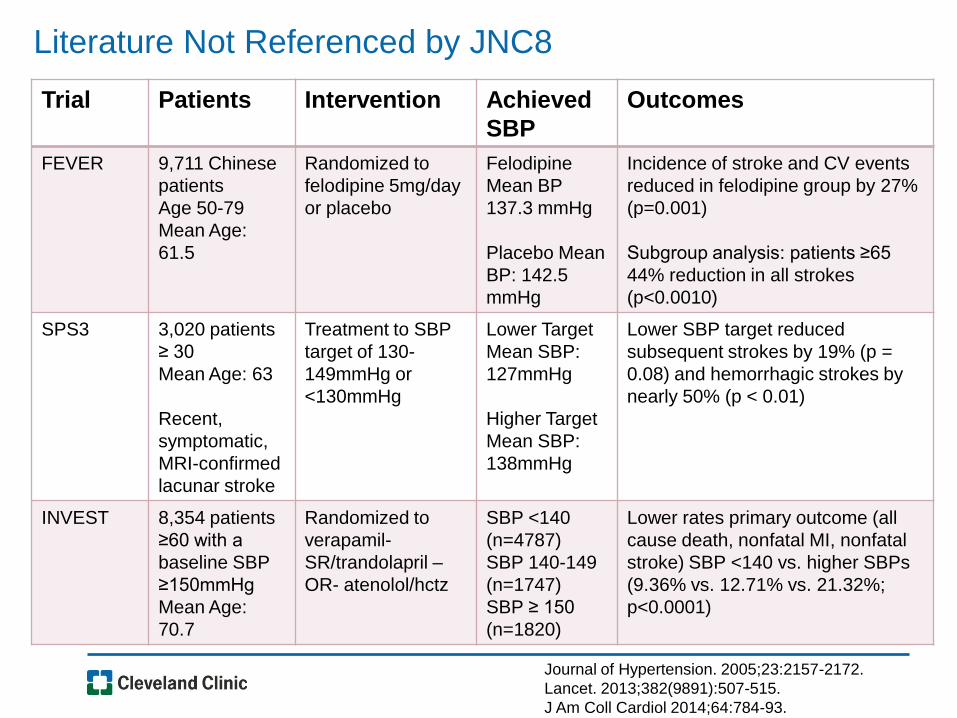
Literature Not Referenced by JNC8
Journal of Hypertension. 2005;23:2157-2172.
Lancet. 2013;382(9891):507-515.
J Am Coll Cardiol 2014;64:784-93.
Trial Patients Intervention Achieved
SBP
Outcomes
FEVER 9,711 Chinese
patients
Age 50-79
Mean Age:
61.5
Randomized to
felodipine 5mg/day
or placebo
Felodipine
Mean BP
137.3 mmHg
Placebo Mean
BP: 142.5
mmHg
Incidence of stroke and CV events
reduced in felodipine group by 27%
(p=0.001)
Subgroup analysis: patients ≥65
44% reduction in all strokes
(p<0.0010)
SPS3 3,020 patients
≥ 30
Mean Age: 63
Recent,
symptomatic,
MRI-confirmed
lacunar stroke
Treatment to SBP
target of 130-
149mmHg or
<130mmHg
Lower Target
Mean SBP:
127mmHg
Higher Target
Mean SBP:
138mmHg
Lower SBP target reduced
subsequent strokes by 19% (p =
0.08) and hemorrhagic strokes by
nearly 50% (p < 0.01)
INVEST 8,354 patients
≥60 with a
baseline SBP
≥150mmHg
Mean Age:
70.7
Randomized to
verapamil-
SR/trandolapril –
OR- atenolol/hctz
SBP <140
(n=4787)
SBP 140-149
(n=1747)
SBP ≥ 150
(n=1820)
Lower rates primary outcome (all
cause death, nonfatal MI, nonfatal
stroke) SBP <140 vs. higher SBPs
(9.36% vs. 12.71% vs. 21.32%;
p<0.0001)
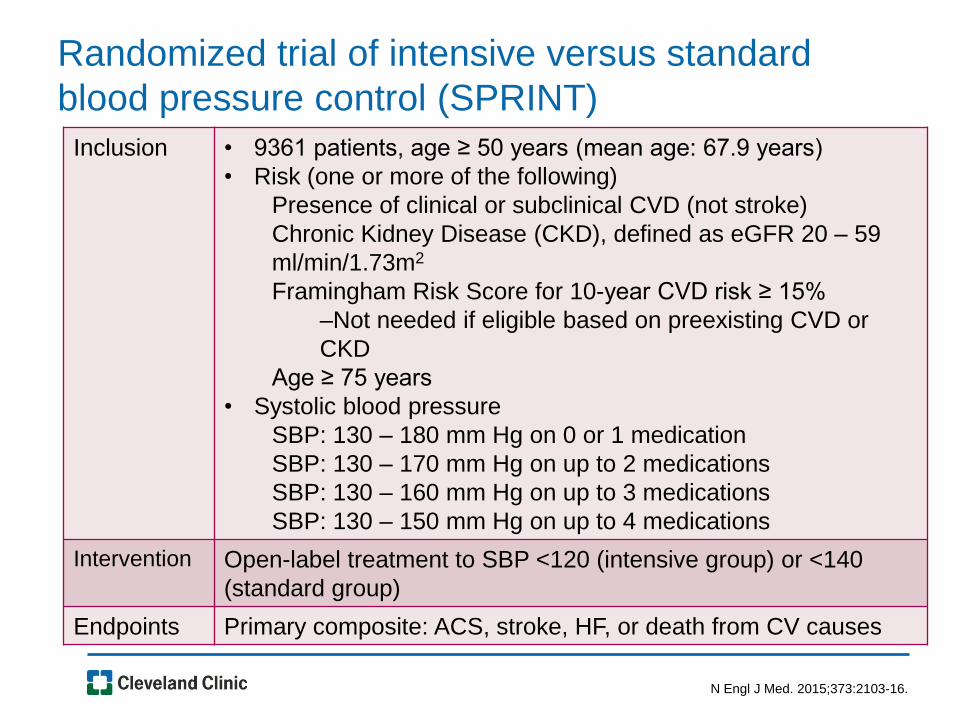
Randomized trial of intensive versus standard
blood pressure control (SPRINT)
N Engl J Med. 2015;373:2103-16.
Inclusion • 9361 patients, age ≥ 50 years (mean age: 67.9 years)
• Risk (one or more of the following)
Presence of clinical or subclinical CVD (not stroke)
Chronic Kidney Disease (CKD), defined as eGFR 20 – 59
ml/min/1.73m2
Framingham Risk Score for 10-year CVD risk ≥ 15%
–Not needed if eligible based on preexisting CVD or
CKD
Age ≥ 75 years
• Systolic blood pressure
SBP: 130 – 180 mm Hg on 0 or 1 medication
SBP: 130 – 170 mm Hg on up to 2 medications
SBP: 130 – 160 mm Hg on up to 3 medications
SBP: 130 – 150 mm Hg on up to 4 medications
Intervention Open-label treatment to SBP <120 (intensive group) or <140
(standard group)
Endpoints Primary composite: ACS, stroke, HF, or death from CV causes
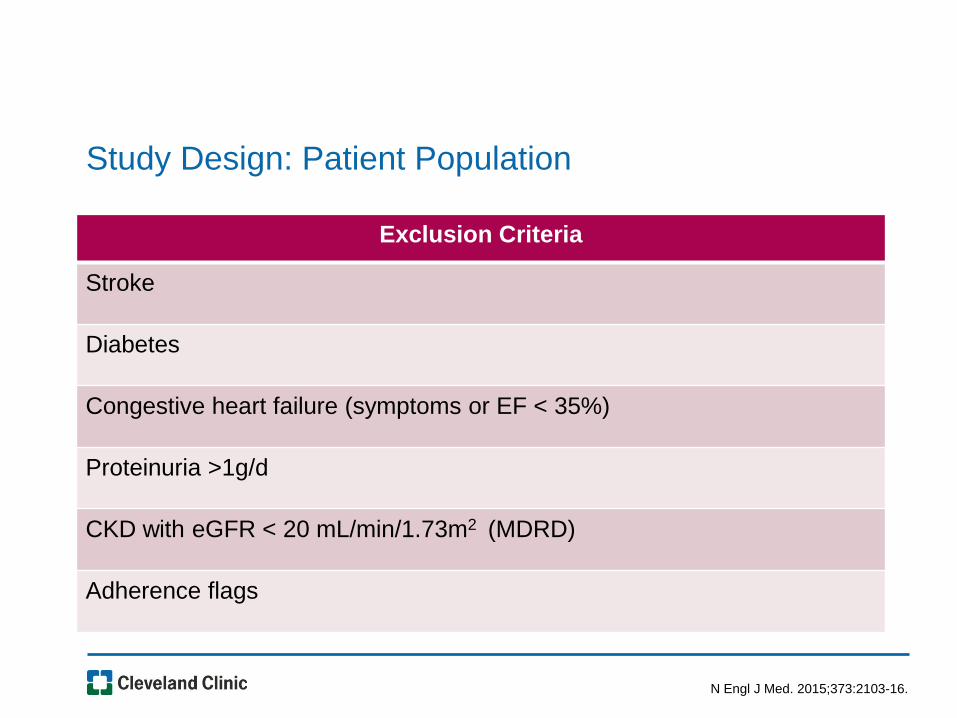
Study Design: Patient Population
N Engl J Med. 2015;373:2103-16.
Exclusion Criteria
Stroke
Diabetes
Congestive heart failure (symptoms or EF < 35%)
Proteinuria >1g/d
CKD with eGFR < 20 mL/min/1.73m2 (MDRD)
Adherence flags
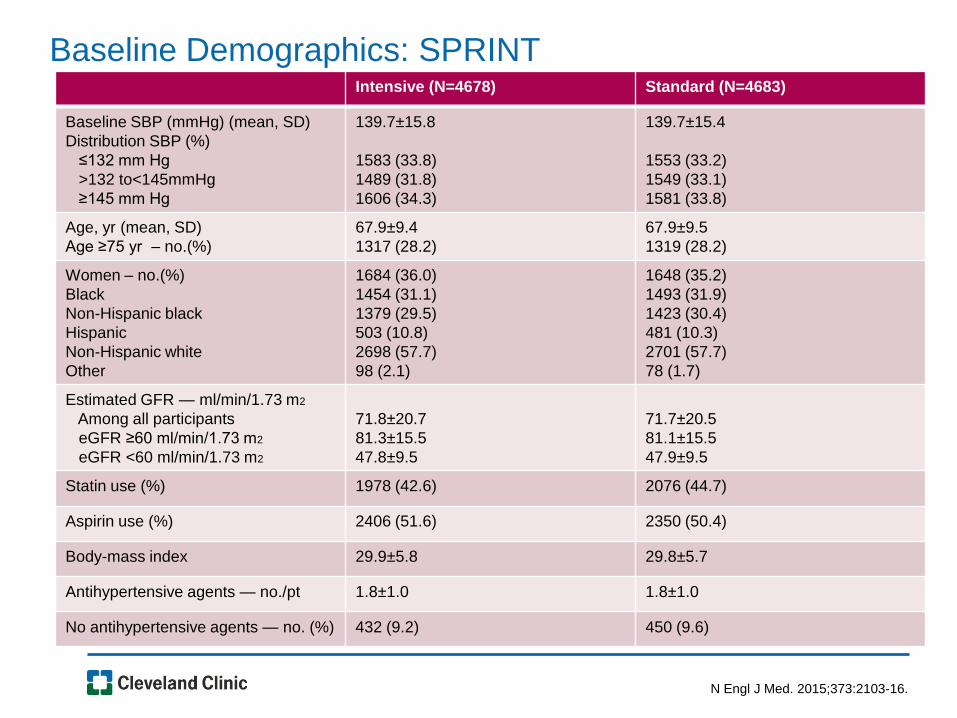
Baseline Demographics: SPRINT
N Engl J Med. 2015;373:2103-16.
Intensive (N=4678) Standard (N=4683)
Baseline SBP (mmHg) (mean, SD)
Distribution SBP (%)
≤132 mm Hg
>132 to<145mmHg
≥145 mm Hg
139.7±15.8
1583 (33.8)
1489 (31.8)
1606 (34.3)
139.7±15.4
1553 (33.2)
1549 (33.1)
1581 (33.8)
Age, yr (mean, SD)
Age ≥75 yr – no.(%)
67.9±9.4
1317 (28.2)
67.9±9.5
1319 (28.2)
Women – no.(%)
Black
Non-Hispanic black
Hispanic
Non-Hispanic white
Other
1684 (36.0)
1454 (31.1)
1379 (29.5)
503 (10.8)
2698 (57.7)
98 (2.1)
1648 (35.2)
1493 (31.9)
1423 (30.4)
481 (10.3)
2701 (57.7)
78 (1.7)
Estimated GFR — ml/min/1.73 m2
Among all participants
eGFR ≥60 ml/min/1.73 m2
eGFR <60 ml/min/1.73 m2
71.8±20.7
81.3±15.5
47.8±9.5
71.7±20.5
81.1±15.5
47.9±9.5
Statin use (%) 1978 (42.6) 2076 (44.7)
Aspirin use (%) 2406 (51.6) 2350 (50.4)
Body-mass index 29.9±5.8 29.8±5.7
Antihypertensive agents — no./pt 1.8±1.0 1.8±1.0
No antihypertensive agents — no. (%) 432 (9.2) 450 (9.6)
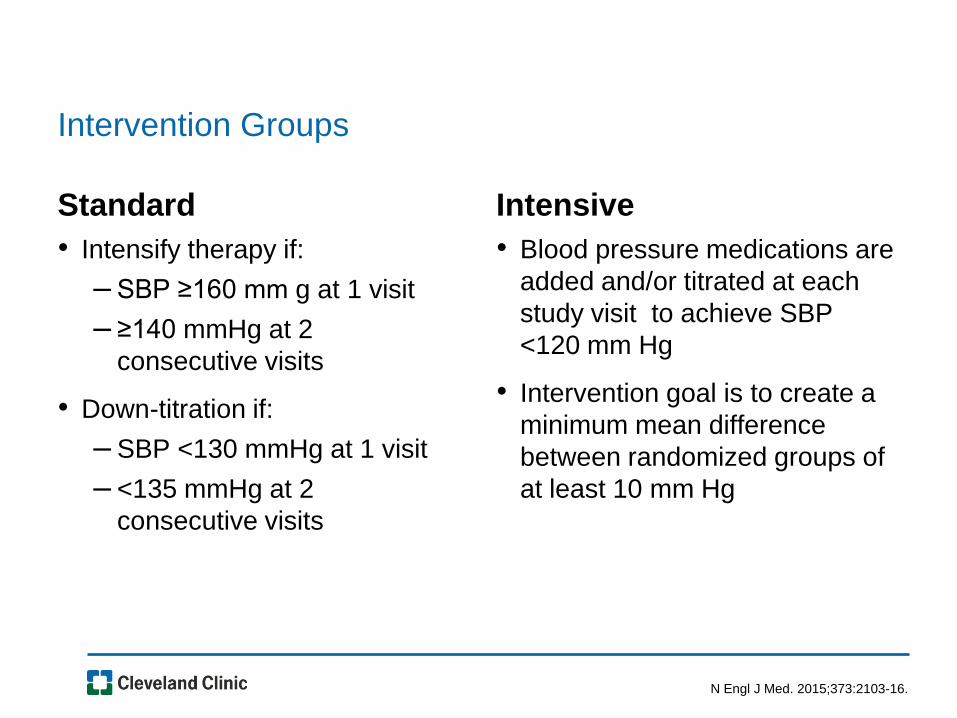
Intervention Groups
Standard
• Intensify therapy if:
– SBP ≥160 mm g at 1 visit
– ≥140 mmHg at 2
consecutive visits
• Down-titration if:
– SBP <130 mmHg at 1 visit
– <135 mmHg at 2
consecutive visits
Intensive
• Blood pressure medications are
added and/or titrated at each
study visit to achieve SBP
<120 mm Hg
• Intervention goal is to create a
minimum mean difference
between randomized groups of
at least 10 mm Hg
N Engl J Med. 2015;373:2103-16.
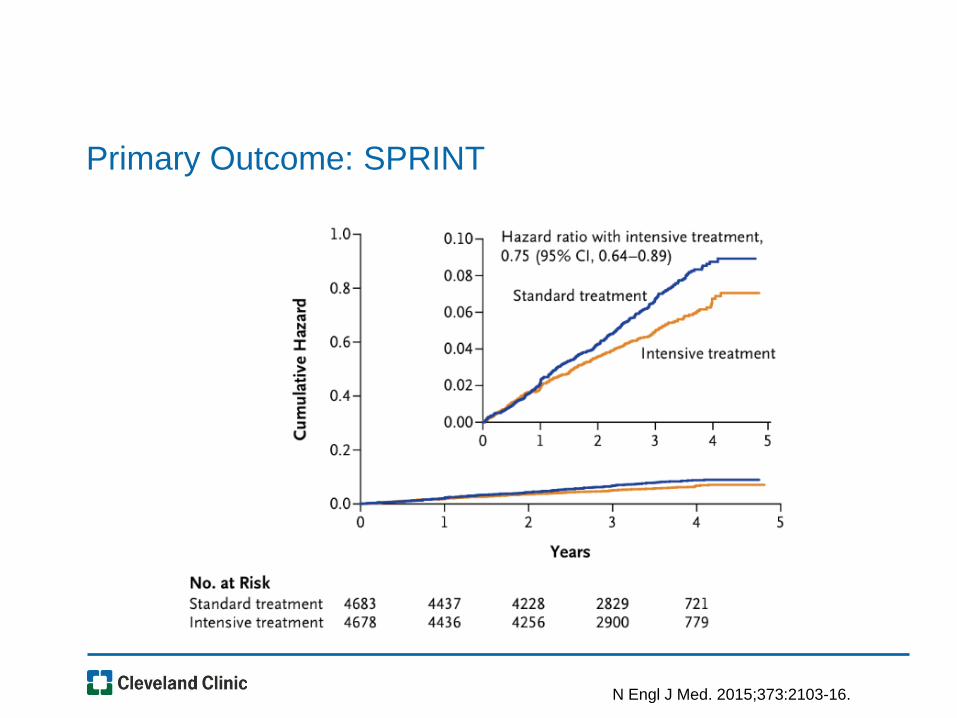
Primary Outcome: SPRINT
N Engl J Med. 2015;373:2103-16.
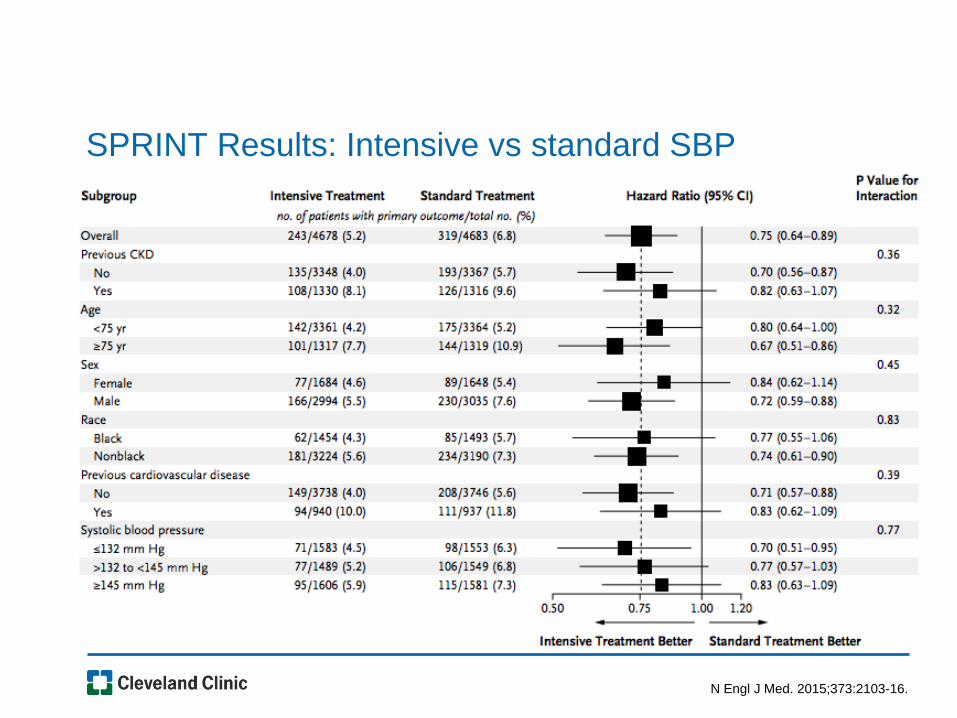
SPRINT Results: Intensive vs standard SBP
N Engl J Med. 2015;373:2103-16.
Take Away Points: SPRINT
• Mean SBP 121.5mmHg (intensive) vs. 134.6mmHg (standard) at 3.26 years
• 25% decrease in primary outcomes in lower SBP group
• NNT to prevent one primary outcome event: 61; death any cause: 90
• No difference: serious adverse event, injurious falls, bradycardia, orthostatic hypotension with dizziness
in hypotension, syncope, electrolyte abnormality, AKI/ARF in intensive treatment group (NNH of 71, 91,100, and 56 respectively)
Results
• Exclusion of patients with prior stroke and patients residing in nursing homes or assisted-living facilities
• Early cessation of trial
• Baseline use of statin 43%, aspirin 51%
• Open label
• Difficult to replicate BP monitoring techniques
Limitations
N Engl J Med. 2015;373:2103-16.
Practical Application: SPRINT
• Treatment to SBP <140mmHg
– Only achieved in 50% of population
• Treatment to SBP <120mmHg
– Required ~1 additional medication
– Achieved in less than half of strict treatment group
– More demanding, time-consuming, and costly in practice
• SPRINT-MIND
• SPRINT-SENIOR
SPRINT-Senior
• Pre-specified subgroup for analysis
• Objective: evaluate effects of intensive vs standard SBP
in patients ≥ 75 yr with HTN but without DM
– 815 participants (30.9%) were classified as frail and 1456 (55.2%)
as less fit
– Exclusion criteria: dementia, expected survival <3 years, SBP
<110mmHg after 1 min standing, unintentional weight loss >10%
6 months prior, nursing home residents
• Outcomes:
– Primary: composite of MI, ACS not resulting in MI, nonfatal stroke,
nonfatal acute decompensated HF, death from CV causes
JAMA. 2016;315(24):2673-82.
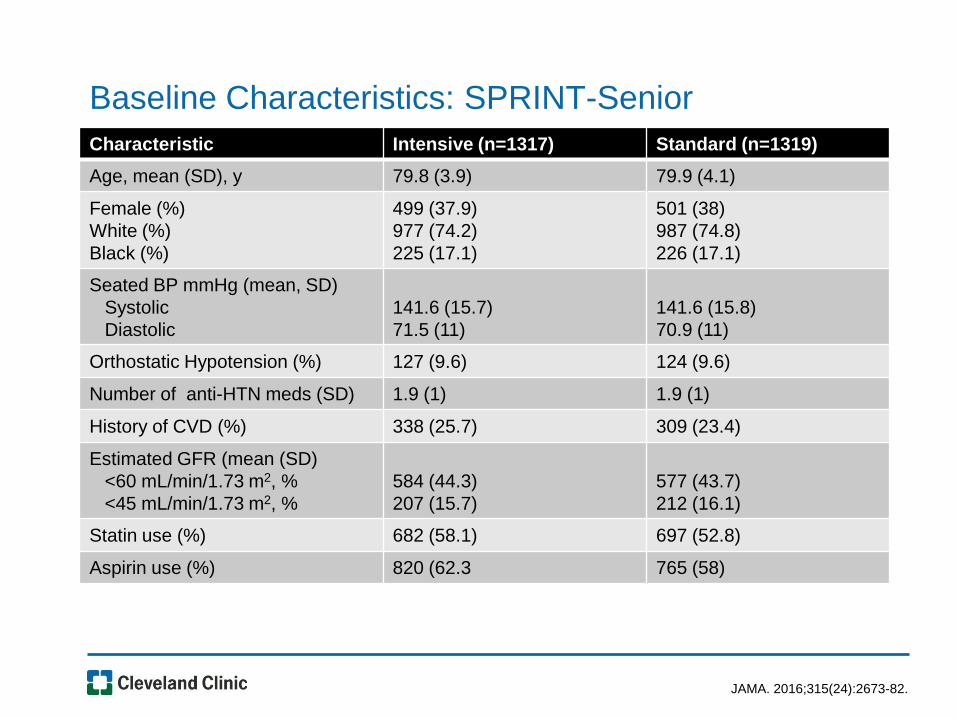
Baseline Characteristics: SPRINT-Senior
JAMA. 2016;315(24):2673-82.
Characteristic Intensive (n=1317) Standard (n=1319)
Age, mean (SD), y 79.8 (3.9) 79.9 (4.1)
Female (%)
White (%)
Black (%)
499 (37.9)
977 (74.2)
225 (17.1)
501 (38)
987 (74.8)
226 (17.1)
Seated BP mmHg (mean, SD)
Systolic
Diastolic
141.6 (15.7)
71.5 (11)
141.6 (15.8)
70.9 (11)
Orthostatic Hypotension (%) 127 (9.6) 124 (9.6)
Number of anti-HTN meds (SD) 1.9 (1) 1.9 (1)
History of CVD (%) 338 (25.7) 309 (23.4)
Estimated GFR (mean (SD)
<60 mL/min/1.73 m2, %
<45 mL/min/1.73 m2, %
584 (44.3)
207 (15.7)
577 (43.7)
212 (16.1)
Statin use (%) 682 (58.1) 697 (52.8)
Aspirin use (%) 820 (62.3 765 (58)
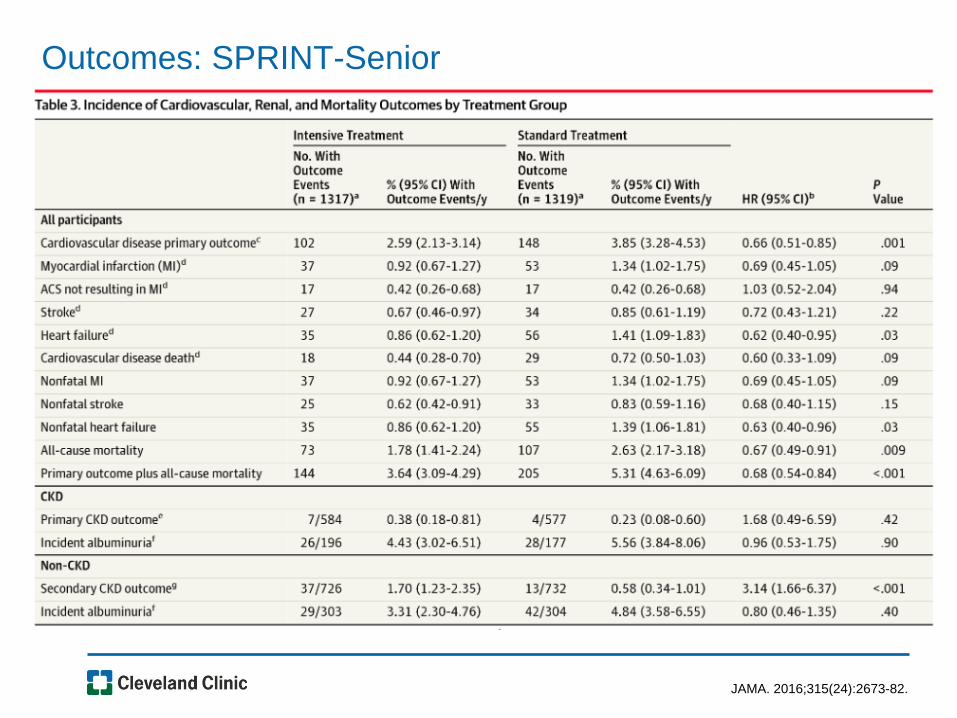
Outcomes: SPRINT-Senior
JAMA. 2016;315(24):2673-82.
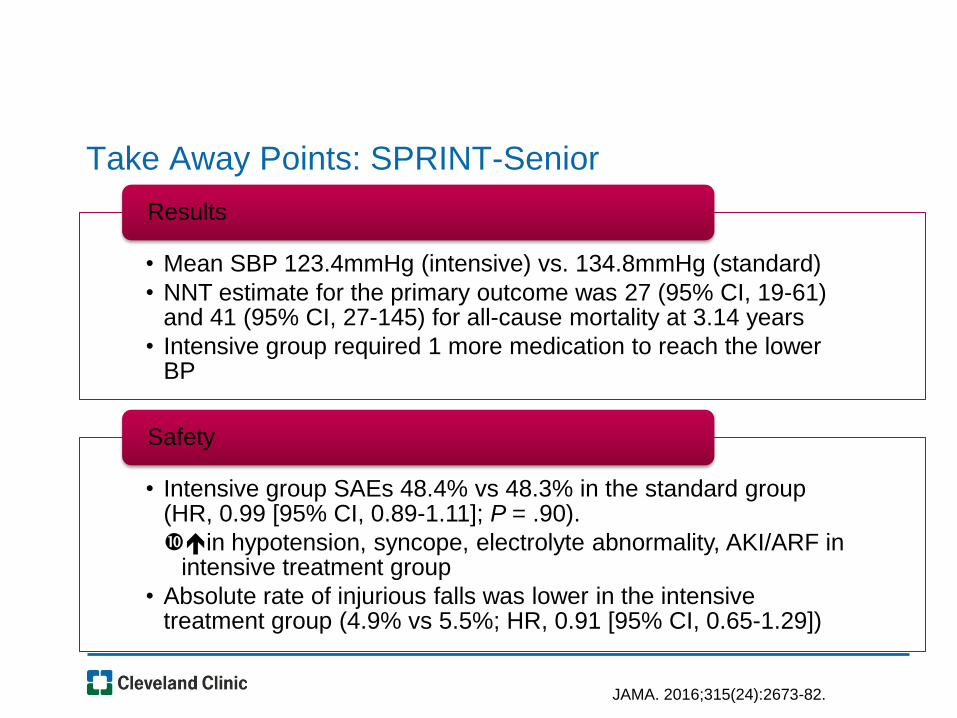
Take Away Points: SPRINT-Senior
• Mean SBP 123.4mmHg (intensive) vs. 134.8mmHg (standard)
• NNT estimate for the primary outcome was 27 (95% CI, 19-61) and 41 (95% CI, 27-145) for all-cause mortality at 3.14 years
• Intensive group required 1 more medication to reach the lower BP
Results
• Intensive group SAEs 48.4% vs 48.3% in the standard group (HR, 0.99 [95% CI, 0.89-1.11]; P = .90).
in hypotension, syncope, electrolyte abnormality, AKI/ARF in intensive treatment group
• Absolute rate of injurious falls was lower in the intensive treatment group (4.9% vs 5.5%; HR, 0.91 [95% CI, 0.65-1.29])
Safety
JAMA. 2016;315(24):2673-82.
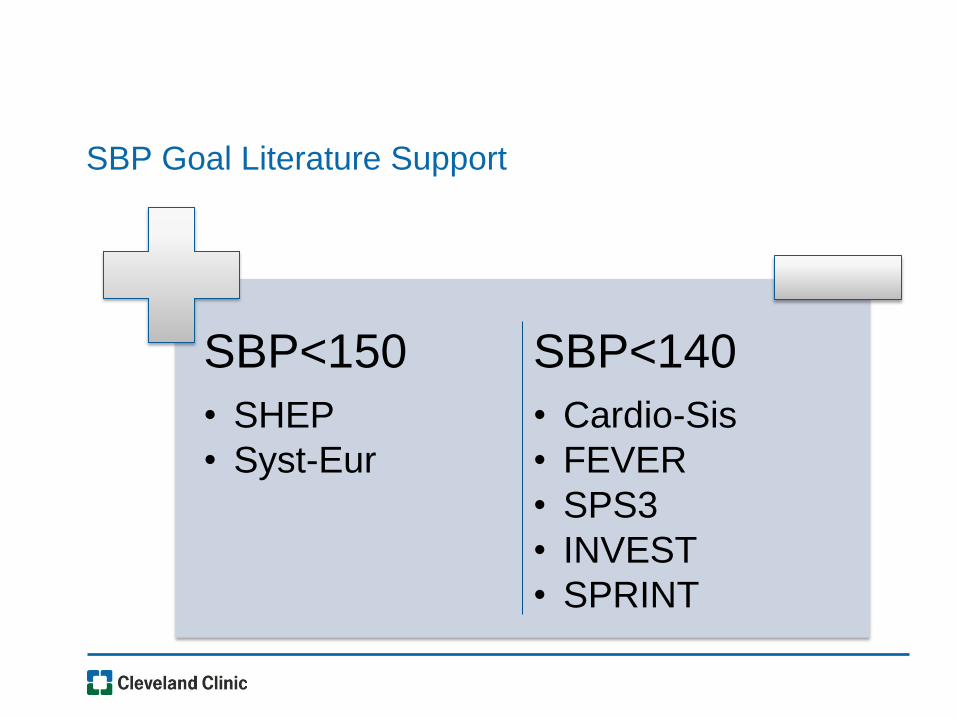
SBP Goal Literature Support
SBP<150
• SHEP
• Syst-Eur
SBP<140
• Cardio-Sis
• FEVER
• SPS3
• INVEST
• SPRINT
BP Goals in Diabetes
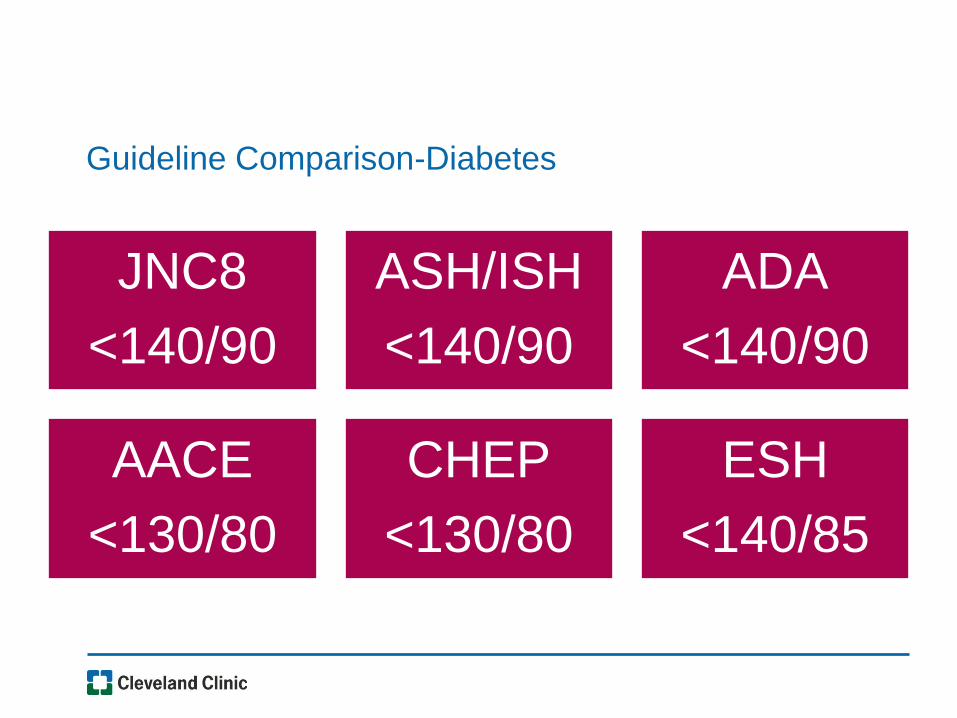
Guideline Comparison-Diabetes
JNC8
<140/90
ASH/ISH
<140/90
ADA
<140/90
AACE
<130/80
CHEP
<130/80
ESH
<140/85
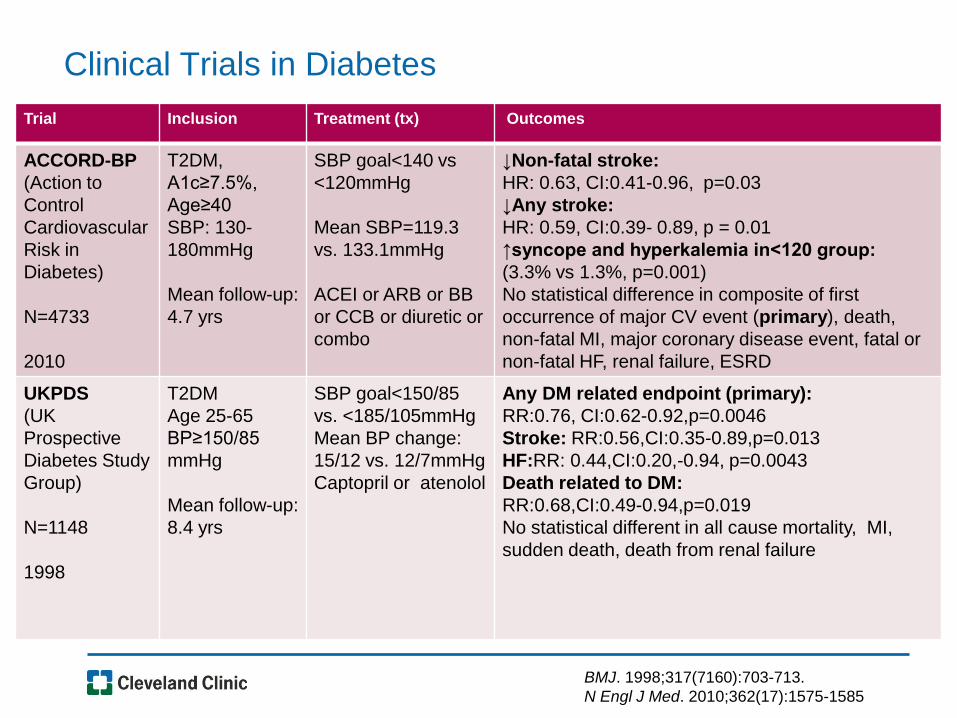
Clinical Trials in Diabetes
Trial Inclusion Treatment (tx) Outcomes
ACCORD-BP
(Action to
Control
Cardiovascular
Risk in
Diabetes)
N=4733
2010
T2DM,
A1c≥7.5%,
Age≥40
SBP: 130-
180mmHg
Mean follow-up:
4.7 yrs
SBP goal<140 vs
<120mmHg
Mean SBP=119.3
vs. 133.1mmHg
ACEI or ARB or BB
or CCB or diuretic or
combo
↓Non-fatal stroke:
HR: 0.63, CI:0.41-0.96, p=0.03
↓Any stroke:
HR: 0.59, CI:0.39- 0.89, p = 0.01
↑syncope and hyperkalemia in<120 group:
(3.3% vs 1.3%, p=0.001)
No statistical difference in composite of first
occurrence of major CV event (primary), death,
non-fatal MI, major coronary disease event, fatal or
non-fatal HF, renal failure, ESRD
UKPDS
(UK
Prospective
Diabetes Study
Group)
N=1148
1998
T2DM
Age 25-65
BP≥150/85
mmHg
Mean follow-up:
8.4 yrs
SBP goal<150/85
vs. <185/105mmHg
Mean BP change:
15/12 vs. 12/7mmHg
Captopril or atenolol
Any DM related endpoint (primary):
RR:0.76, CI:0.62-0.92,p=0.0046
Stroke: RR:0.56,CI:0.35-0.89,p=0.013
HF:RR: 0.44,CI:0.20,-0.94, p=0.0043
Death related to DM:
RR:0.68,CI:0.49-0.94,p=0.019
No statistical different in all cause mortality, MI,
sudden death, death from renal failure
BMJ. 1998;317(7160):703-713.
N Engl J Med. 2010;362(17):1575-1585
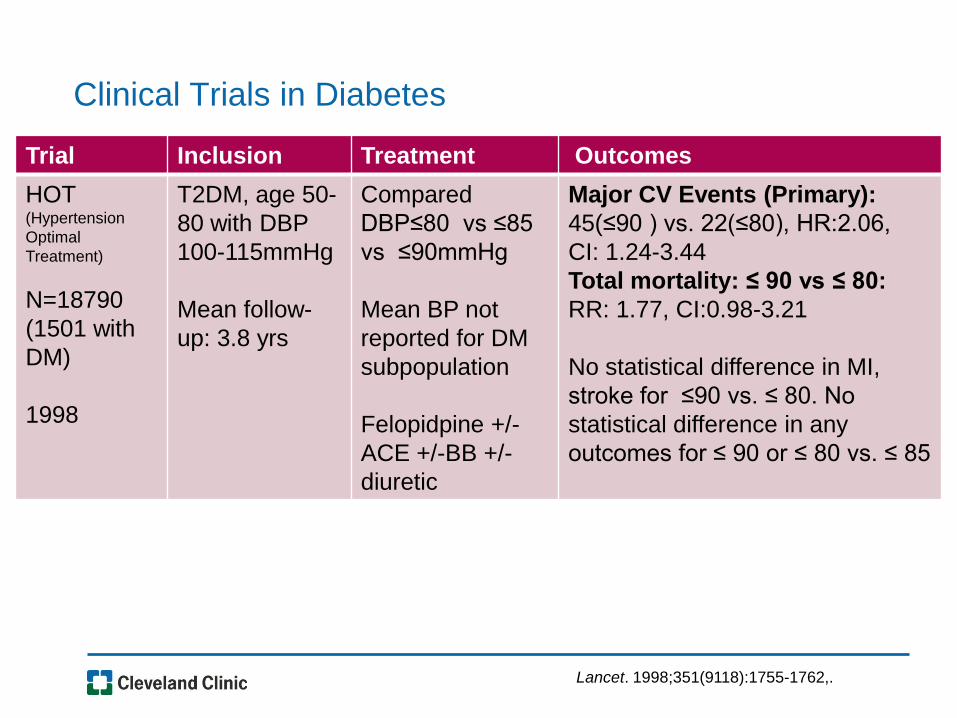
Clinical Trials in Diabetes
Trial Inclusion Treatment Outcomes
HOT (Hypertension
Optimal
Treatment)
N=18790
(1501 with
DM)
1998
T2DM, age 50-
80 with DBP
100-115mmHg
Mean follow-
up: 3.8 yrs
Compared
DBP≤80 vs ≤85
vs ≤90mmHg
Mean BP not
reported for DM
subpopulation
Felopidpine +/-
ACE +/-BB +/-
diuretic
Major CV Events (Primary):
45(≤90 ) vs. 22(≤80), HR:2.06,
CI: 1.24-3.44
Total mortality: ≤ 90 vs ≤ 80:
RR: 1.77, CI:0.98-3.21
No statistical difference in MI,
stroke for ≤90 vs. ≤ 80. No
statistical difference in any
outcomes for ≤ 90 or ≤ 80 vs. ≤ 85
Lancet. 1998;351(9118):1755-1762,.
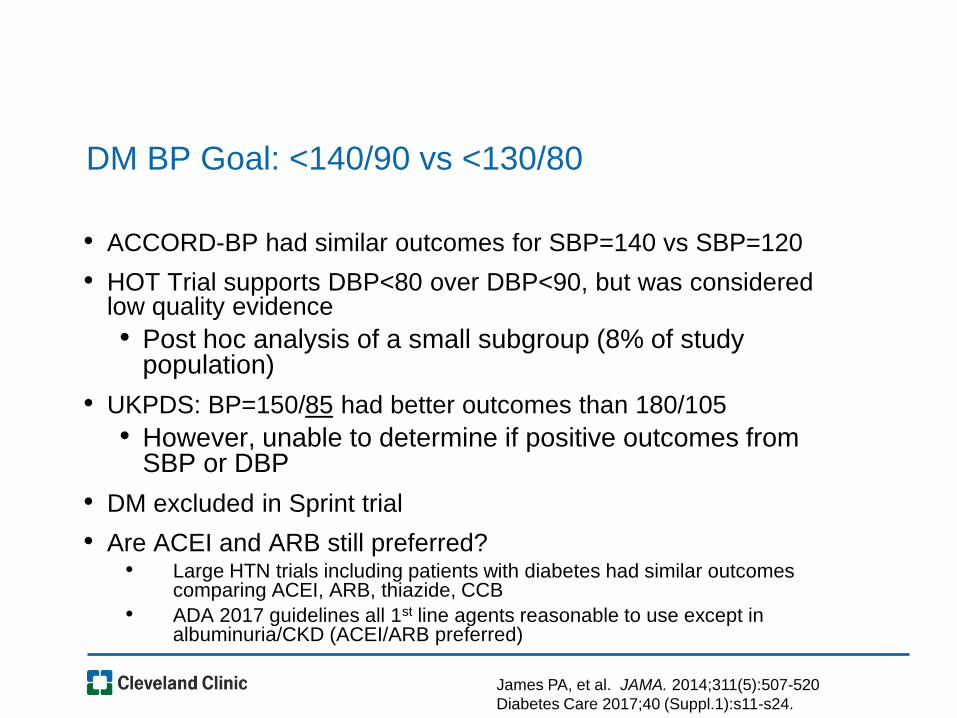
DM BP Goal: <140/90 vs <130/80
• ACCORD-BP had similar outcomes for SBP=140 vs SBP=120
• HOT Trial supports DBP<80 over DBP<90, but was considered low quality evidence
• Post hoc analysis of a small subgroup (8% of study population)
• UKPDS: BP=150/85 had better outcomes than 180/105
• However, unable to determine if positive outcomes from SBP or DBP
• DM excluded in Sprint trial
• Are ACEI and ARB still preferred? • Large HTN trials including patients with diabetes had similar outcomes
comparing ACEI, ARB, thiazide, CCB
• ADA 2017 guidelines all 1st line agents reasonable to use except in albuminuria/CKD (ACEI/ARB preferred)
James PA, et al. JAMA. 2014;311(5):507-520
Diabetes Care 2017;40 (Suppl.1):s11-s24.
BP Goals in CAD
Most guidelines recommend <140/90 with no
separate category for CAD
SPRINT vs. ACCORD-BP
ACCORD-BP
• N=4733, 34% with a previous CV event
• BP<120/80, lower stroke rate
SPRINT
• Better outcomes with BP<120/80 vs <140/80 in high risk patients
CAD/BP Goal Comparisons
• Prospective, observational study (N=22,672)
– 45 countries represented
– Patients with Stable CAD + HN
– Median f/u: 5.0 years
• Primary Outcome: CV death, MI, stroke
• BP>140/80-worse outcomes
• SBP<120 = increased risk
– Adjusted HR 1.56, 95% CI 1·36–1·81
• DBP<70
– DBP 60-69: adjusted HR 1.41 95% CI 1.24–1.61
– DBP <60: adjusted HR 2.01 95% CI 1·.50–2.70
Vidal‐Petiot E, et al. Lancet. 2016 Aug 26..
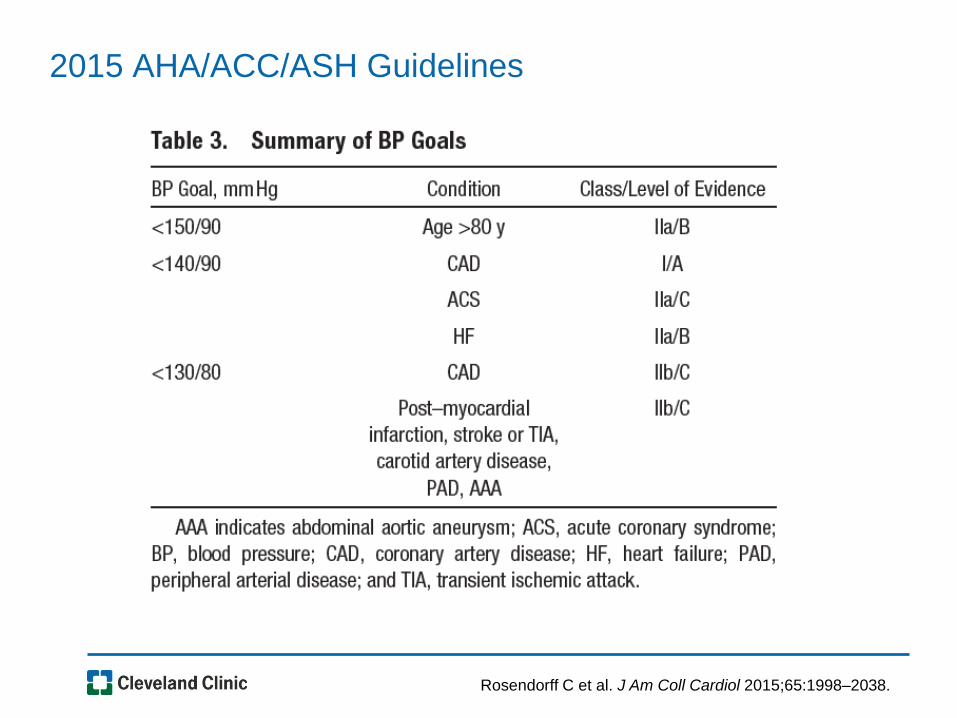
2015 AHA/ACC/ASH Guidelines
Rosendorff C et al. J Am Coll Cardiol 2015;65:1998–2038.
Back to the Case
AL is a 65 year old African American male. AL’s in-office BP today is 148/88mmHg and same on repeat. One month ago, AL’s BP was 146/88mmHg.
• PMH: Sleep apnea, allergic rhinitis
• Meds: Loratadine 10mg po daily
• No known drug allergies/ADR’s
• Height: 5’11” 225lbs, BMI=31.4
• Family history: mother with type 2 diabetes
• Social history: non-smoker, frequently eats out at restaurants, adds salt to food
What is AL’s BP Goal?
A. <150/90
B. <140/90
C. <130/80
D. <120/80
AL is now 70 and he developed diabetes. Current BP is
136/80 and now he’s on HCTZ 25mg daily and metformin
1000mg BID. Which of the following is the best plan?
A1C=6.9%. CMP is wnl. Neg albuminurea
A. Continue current therapy
B. Add lisinopril 10mg daily
C. Add amlodipine 5mg daily
D. Add lisinopril 10mg daily and amlodipine 5mg daily
Two years later (age 72) he developed CAD and had an MI
3 months ago. Current meds: metoprolol succinate,
furosemide, metformin, sitagliptin, lisinopril, ASA. Current
BP is 132/74. What is the most appropriate BP goal?
A. <150/90
B. <140/90
C. <130/80
D. <120/80
What should his BP goal be in 10 years? (Age=82?)
In Summary
• Guidelines differ on optimal BP goals but agree <140/90 is a good
starting point for most
• Thiazides, CCB, ACE-inhibitors, ARB’s are 1st line agents
• SPRINT provides evidence that lower BP may benefit some patients
• Keep in mind SPRINT trial exclusion criteria and overall limitations
• Guidelines provide a general framework, but always consider the
individual patient