Embed Size (px)
Citation preview

1. Introduction
2. What is the best method to
estimate cardiovascular risk?
3. Evaluation of total
cardiovascular risk: practical
implications
4. When should treatment of
high BP be initiated?
5. What is the optimal goal BP in
subjects with cardiovascular
disease?
6. What is the optimal choice of
antihypertensive drug?
7. Treatment strategies in
special conditions
8. How should concomitant risk
factors be treated?
9. Conclusions
10. Expert opinion
Review
Hypertension 2010: what was newfor the cardiologist?Zbigniew Gaciong† & Bartosz Symonides†Medical University of Warsaw, Department of Internal Medicine, Hypertension and Vascular
Diseases, Poland
Importance of the field: Despite extensive clinical research, still there is some
uncertainty regarding management of hypertension, in particular initial and
goal blood pressure levels and selection of optimal pharmacotherapy, as
well as concomitant medications, to reduce other risk factors.
Areas covered in this review: An overview of recent findings from major clin-
ical trials in hypertension (until July 2010), along with a reappraisal of the
European Society of Hypertension 2009 guidelines.
What the reader will gain: Practical overview of the management of hyper-
tension, including threshold and goal blood pressure in specific situations,
choice of antihypertensive medications and indications for treatment of
concomitant risk factors.
Take home message: Primary benefits of antihypertensive therapy are medi-
ated by blood pressure reduction and the majority of patients will require
at least two drugs, with the preference of fixed-dose combinations for
effective blood pressure control.
Keywords: antihypertensive therapy, goal blood pressure, guidelines, hypertension,
renal artery stenosis
Expert Opin. Pharmacother. (2010) 11(16):2579-2597
1. Introduction
In October 2009, The European Society of Hypertension (ESH) released a docu-ment [1] that critically reviewed previous hypertension guidelines published just2 years earlier [2]. In the current paper -- appropriately named Reappraisal -- theauthors critically evaluate both contemporary and older evidence from clinical trialsto question certain statements from previous guidelines as well as endorse some rec-ommendations. This update included data from five major clinical trials publishedwithin the last 2 years addressing:
- The benefit of blood pressure (BP) lowering in patients with type 2 diabetesmellitus (ADVANCE) [3]
- The role of angiotensin receptor blocker (ARB) treatment with or without anACE inhibitor in patients at very high cardiovascular risk (ONTARGET,TRANSCEND) [4,5]
- Antihypertensive treatment in the very elderly (HYVET) [6]
- The use of combination therapy in hypertension (ACCOMPLISH) [7].
However, since the publication of Reappraisal, results of new important clinicaltrials have been presented that may influence current recommendations regarding:
- Goal blood pressure in non-diabetic (Cardio-Sis) and diabetic patients(ACCORD) [8,9]
- The role of renin-angiotensin system (RAS) inhibition in diabetes prevention(NAVIGATOR) [10]
10.1517/14656566.2010.513972 © 2010 Informa UK, Ltd. ISSN 1465-6566 2579All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

- The value of renal artery stenting for atheroscleroticstenosis (ASTRAL) [11]
- Concomitant treatment with low-dose aspirin(AAAT) [12].
Also, important new meta-analyses have determined thequantitative efficacy of different classes of antihypertensivedrugs in prevention of major clinical complications [13], riskof new-onset diabetes [14,15], incidence of episodes ofatrial fibrillation [16] or effect on BP lowering, alone or incombination [17,18].In the present survey, these new data will be presented with
an attempt to offer a practical recommendations for
cardiologists taking care of their hypertensive patients. In par-ticular, BP management in terms of treatment initiation,blood pressure goals, choice of antihypertensive drugs, andindications for pharmacotherapy of associated risk factorswill be discussed. Special emphasis will be placed on certainhigh-risk groups such as the elderly, diabetics, and patientswith a history of cardiovascular incidents.
2. What is the best method to estimatecardiovascular risk?
Assessment of total cardiovascular risk dictates the decisionabout treatment initiation, intensity and goals. The finalestimate is based on the presence of risk factors, subclinicalorgan damage, history of atherosclerotic complications andconcomitant states like diabetes or chronic kidney disease.
Current expert opinion emphasizes the role of testing forsubclinical evidence of cardiovascular disease [1,2]. Any modal-ity that can be used to detect asymptomatic target organ dam-age should be applied, from simple (EGFR, echocardiography[ECG], albumin urinary excretion) to more sophisticated,requiring special skills and equipment (echocardiography,pulse wave velocity or central arterial pressure measurements).Recent data show that certain new parameters obtained fromwidely available test have predictive power for future fatal andnonfatal events. For example, left ventricle mass (LVM) maybe more accurately estimated with a Novacode equation thatis based on both voltage and strain pattern criteria. In the pro-spective study including 7495 adults, this estimate was anindependent and significant predictor of 10-year cardiovascu-lar mortality [19]. Also, simple parameters like amplitude ofR-wave in lead aVL shows very good correlation with cardio-vascular risk and detects left ventricular hypertrophy with asensitivity similar to that of established ECG criteria like Cor-nell product [20]. Still, among relatively available methods,ECG remains the most accurate, with significant predictivevalue. In the prospective PAMELA (Pressioni Arteriose Moni-torate E Loro Associazioni) study, increase of LVM by 10%,even within normal range, was associated with an increasedrisk [21].
This is advised to examine for early vascular changes asincreased intima-media thickness (IMT) in carotid artery,and indirect indices of arteriosclerosis like carotid-femoralpulse wave velocity (PWV) or augmentation index, reflectingcentral BP. Data from recent studies show that in apopulation without significant cardiovascular disease, anyabnormalities in these parameters are harbingers of worseprognosis [22-24].
Despite the fact that different measures of arterial stiffnessand wave reflection have been considered as markers ofcardiovascular risk, there is only one analysis that comparesprognostic utility of those parameters in prospective,community-based study. In the Framingham Heart Study,2232 disease-free participants were observed for a median of7.8 years after measurement of markers of arterial stiffness
Article highlights.
. It appears reasonable to start blood pressure loweringtherapy in stage 1 hypertensive patients at low/moderate risk after a suitable period with life-stylemodification. Treatment may be initiated immediately insubjects with high risk or grade 2 or 3 hypertension.
. SBP should be lowered below 140 mm Hg and DBPbelow 90 mm Hg in all hypertensive patients. Previouslyuntreated very old patients (>80 years) should starttreatment with SBP at least 160 mm Hg with goal BPbelow 150 mm Hg. In subjects with isolated systolicblood pressure, caution should be taken not to lowerDBP below 65 mm Hg.
. There is no clinical trial evidence that diabetic subjectswould obtain additional benefit from reduction in SBPbelow 130 mm Hg. However, in subjects with diabeticnephropathy benefits of treatment were observedregardless initial BP level. In patients with advanceatherosclerotic artery disease progressive lowering ofSBP below mm Hg and DBP below 75 mm Hg may beassociated with an increased incidence of cardiovascularincidents.
. The 2007 ESC/ESH guidelines conclusion that diuretics,ACE inhibitors, ARBs, CCB, and beta-blockers can all beused for initiation of antihypertensive therapy can thusbe confirmed. Most hypertensive patients will need atleast 2 different drugs to achieve satisfactory BP control,and fixed-dose combinations seems to facilitate reachingBP target. Among different possible combinations RASinhibition and CCB seem to offer better metabolicprofile and more effective organ protection whilecombined use of ACE inhibitors with ARBs or diureticswith beta-blockers should be avoided due to increasedrisk of renal complications or new-onset diabetes,respectively.
. Treatment of associated risk factors with anti-plateletagents or statins for primary prevention should be basedon estimated risk/benefit ratio. Diabetes or subclinicalatherosclerosis without any clinical atheroscleroticcomplications cannot be considered as compellingindications for anti-platelet therapy.
This box summarizes key points contained in the article.
Hypertension 2010: what was new for the cardiologist?
2580 Expert Opin. Pharmacother. (2010) 11(16)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

(PWV), wave reflection (augmentation index, carotid brachialpressure amplification) and central pulse pressure. Using mul-tiple variable models adjusted for concomitant risk factorsonly higher aortic stiffness assessed by PWV improved predic-tion of future cardiovascular events, independently of stan-dard risk factors like age, gender, smoking, hypertension,diabetes, and lipids [25].
The 2007 ESH/ESC guidelines included urinary albuminand EGFR as measures of subclinical kidney damage associ-ated with cardiovascular risk [2]. In a recent meta-analysis,standardized data for all-cause and cardiovascular mortalitywere pooled from studies enrolling at least 1000 participantsfor whom baseline measurement were available for EGFRand urine albumin excretion. Urine albumin-to-creatinineratio (ACR) was measured in 14 studies including a total of105,872 participants (730,577 person-years), and urineprotein was measured by dipstick in seven studies enrollinga total of 1,128,310 subjects (4,732,110 person-years). Riskfor mortality was unrelated to an EGFR between 75 and105 ml/min/1.73 m2 and increased at lower EGFRs. Adjustedhazard ratios (HR) for all-cause mortality versus an EGFR of95 ml/min/1.73 m2 were 1.18 (95% CI, 1.05 -- 1.32) for anEGFR of 60 ml/min/1.73 m2, 1.57 (95% CI, 1.39 -- 1.78)for an EGFR of 45 ml/min/1.73 m2, and 3.14 (95% CI,2.39 -- 4.13) for an EGFR of 15 ml/min/1.73 m2. On thelog--log scale, ACR was linearly associated with the risk formortality without threshold effects. Adjusted HRs for all-cause mortality versus an ACR of 0.6 mg/mmol were1.20 (95% CI, 1.15 -- 1.26) for an ACR of 1.1 mg/mmol,1.63 (95% CI, 1.50 -- 1.77) for an ACR of 3.4 mg/mmol,and 2.22 (95% CI, 1.97 -- 2.51) for an ACR of 33.9 mg/mmol. ACR and EGFR were multiplicatively associatedwith the risk for mortality, and there was no evidence forinteraction. Results were similar for cardiovascular mortalityand in studies with dipstick measurements of urine protein.As stated by the authors of the study, ‘EGFR less than60 ml/min/1.73 m2 and ACR 1.1 mg/mmol (10 mg/g) ormore are independent predictors of mortality risk in thegeneral population’ [26].
For GFR calculation, authors used the Modification ofDiet in Renal Disease Study (MDRD) equation, which wasderived from primarily white subjects (mean age of 51 ±12.7 years) who had non-diabetic kidney disease, with meanGFR of 40 ml/min/1.73 m2. Like other common formulasutilized to estimate the GFR, they are less accurate in certainpopulations. These include individuals with normal GFR,children, elderly patients, specific ethnic groups, pregnantwomen, and those with unusual muscle mass, body habitus,and weight (e.g., morbid obesity, amputees).
The CKD-EPI equation (The Chronic Kidney DiseaseEpidemiology Collaboration) was developed to provide amore accurate estimate of GFR among individuals with nor-mal or only mildly reduced GFR (> 60 ml/min/1.73 m2),using data pooled from 10 studies and validated against dataderived from 16 additional studies, in which the gold
standard was direct measurement of GFR using external filtra-tion markers [27]. CKD-EPI uses the same variables (serumcreatinine level, age, gender, and race) as the MDRD equa-tion. In the validation studies, the CKD-EPI equation wasas accurate as the MDRD study equation among individualswith estimated GFR < 60 ml/min/1.73 m2 and substantiallymore accurate among those with higher GFRs. When bothequations were used to estimate GFR in > 16,000 NHANESparticipants, GFR estimates by CKD-EPI were higher thanestimates obtained using the MDRD Study equation amongindividuals with a measured GFR > 30 ml/min/1.73 m2. Asa result, the overall prevalence of CKD was lower when theCKD-EPI equation was used to define the population withchronic kidney diseases (13.0 vs 11.5%). A possible limitationof the CKD-EPI equation is that it was developed usingsample populations that included few elderly and non-whiteindividuals, as well as people selected for or against havingkidney disease.
In the recent study, EGFR calculated based on CKD-EPIand MDRD equations was correlated with cardiovascular epi-sodes in the 13,905 middle-age subjects followed by a medianof 16.9 years participating in a prospective cohort study, theAtherosclerosis Risk in Communities (ARIC) Study [28].The CKD-EPI equation better categorized individuals withrespect to long-term clinical risk compared with the MDRDstudy equation, suggesting improved clinical usefulness inthis middle-aged population.
In the algorithm for global cardiovascular risk estimationused in current guidelines, the presence of metabolic syn-drome places a hypertensive subject in the group with highor very high added risk. It is assumed that clustering ofabdominal obesity, elevated glucose, abnormal lipids, and ele-vated BP are associated with an increased risk of coronaryheart disease, greater than that conferred by its constituentcomponents. In 2005, the American Diabetes Association(ADA) and the European Association for the Study of Diabe-tes (EASD) published a joint statement raising questionsabout whether the components of the metabolic syndromecan be classified as a true ‘syndrome’ [29]. The critical weak-ness of the idea of metabolic syndrome is that treatment ofthe syndrome is no different from treatment for each of itscomponents. Other arguments raised include imprecise defi-nition due to lack of a consistent evidence base for settingthe thresholds for the various components in the definitions.Also, pathogenesis of metabolic syndrome seems to be unclearand insulin resistance may not underlie all disturbances.Within the metabolic syndrome, there are various phenotypesrequiring a different treatment approach. In some studiesthe cardiovascular risk associated with the metabolic syn-drome has not been shown to be greater than the sum of itsindividual components [30].
To investigate this issue, Mente and colleagues analyzeddata from the INTERHEART study, a case-control study ofincident acute myocardial infarction (MI) that involved12,297 cases and 14,606 controls from 52 countries. They
Gaciong & Symonides
Expert Opin. Pharmacother. (2010) 11(16) 2581
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

classified the study participants using the World HealthOrganization (WHO) and International Diabetes Federation(IDF) criteria for metabolic syndrome, and their risks forMI were compared with the individual metabolic-syndromecomponent factors. Results showed that metabolic syndromewas associated with a two to three times increased risk ofMI, but the same risk was conferred by having either hyper-tension or diabetes alone [31]. Authors found the continuousrelationship between values of parameters included in the def-inition of metabolic syndrome and risk of acute MI. This cor-relation was also observed for subthreshold values -- that is,levels higher than normal but below the levels that define dia-betes, hypertension, low HDL or abdominal obesity. Aggrega-tion of risk factors with values below their threshold wasassociated with a significantly greater risk of MI, comparedwith having component factors with normal values (odds ratio1.5), but lower than the risk conferred by an aggregation ofrisk factors with values above the threshold points. In theirpaper, the investigators conclude: ‘These findings of a dose--response relationship between risk-factor severity and MIrisk suggest that a standard definition of metabolic syndromeloses information when continuous variables are converted tocategorical variables and provide support for calls to replacethe categorical definition of metabolic syndrome with a scor-ing system that may involve each risk factor being assigned aweight based on its level and a regression formula developedto estimate risk’. Therefore the advice remains to treat indi-vidual risk factors when present, and to prescribe therapeuticlifestyle changes and weight management for obese patientswith multiple risk factors.Experimental and clinical evidence have established inflam-
matory processes as important contributors to atherogenesis,as well as to the vulnerability of an atherosclerotic lesion to rup-ture or erosion. The most extensively studied biomarker ofinflammation in cardiovascular diseases is C-reactive protein(CRP), for which standardized high-sensitivity assays (hs-CRP) are widely available. In apparently healthy subjects, hs-CRP level is continuously related to the risk of cardiovascularcomplications (including sudden cardiac death, MI, ischemicstroke, atrial fibrillation, and heart failure) as well as develop-ment of hypertension and diabetes mellitus. In patients withestablished atherosclerotic vascular disease, the predictive valueof CRP for disease severity and prognosis has been studied indifferent populations including patients after acute coro-nary syndrome, revascularization procedures, cerebrovasculardisease, heart failure, atrial fibrillation and intermittentclaudication, and recipients of cardiac allograft [32].The observations that statin therapy reduces serum CRP
and that serum CRP is correlated with cardiovascular riskraises the possibility that the risk reduction with statin therapymay be attributed, at least in part, to anti-inflammatoryeffects. In a literature review of 13 controlled trials, statinsreduced CRP levels by 13 -- 50% compared with placebo;there was no advantage of one statin over another in fivestudies making direct comparisons, and more intensive statin
therapy was associated with a modestly greater reduction inCRP [33].
The 2007 European guidelines have emphasized the prog-nostic value of treatment-induced modifications of subclinicalorgan damage. Analysis of data from the LIFE (LosartanIntervention For Endpoint Reduction in Hypertension) studyshows that changes in ECG signs of left ventricular hypertro-phy (LVH), left atrial diameter and left ventricular geometryas well as albumin excretion correlated with incident cardio-vascular event rate [34,35]. These findings were confirmed byrecent data from the ADVANCE (Action in Diabetes andVascular disease; Preterax and Diamicron-MR ControlledEvaluation) trial which included 11,140 patients withtype 2 diabetes randomly treated with a fixed combinationof perindopril--indapamide or placebo, regardless of their ini-tial BP level. The level of albumin excretion correlated withrenal and cardiovascular risk, not only at entry but alsoaccording to on-treatment values. A protective effect of pro-teinuria reduction was independent of the concomitant valuesof EGFR [36].
3. Evaluation of total cardiovascular risk:practical implications
The 2007 ESH/ESC guidelines recommend that differentorgans be searched for damage, because of the evidence thatmultiple organ damage (in the kidney and the heart) carriesa worse prognosis than when limited to a single organ.However, as it discussed below, the presence of subclinicalorgan damage does not mandate earlier initiation of antihy-pertensive treatment (i.e., with high normal BP). Treat-ment-induced improvement of LVH and increased urinaryprotein excretion are associated with a reduced incidence ofcardiovascular events [37], thereby giving physician andpatients an insight on whether the applied treatment isoffering organ protection.
New technology offers better measures to assess subclinicalorgan damage. For example, MRI allows detection of silentcerebrovascular lesions, which are even more prevalent thancardiac and renal subclinical damage. And, as one studyshows, white-matter lesions may develop in the absence ofother signs of organ damage [38]. However, new methods arecostly; and, more importantly, their effect on the strategy ofantihypertensive treatment has not been established. Availabledata, like the recently published INTERSTROKE study, con-firm that ‘old’ or ‘classical’ risk factors describe at least 90% ofmodifiable cardiovascular risk [39].
4. When should treatment of high BP beinitiated?
The ESH/ESC 2007 guidelines introduced the concept of dif-ferent goal thresholds for pharmacotherapy based on globalcardiovascular risk [2]. Subjects with high risk (those withdiabetes, chronic kidney disease or atherosclerotic disease)
Hypertension 2010: what was new for the cardiologist?
2582 Expert Opin. Pharmacother. (2010) 11(16)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

should receive antihypertensive drugs when high normal bloodpressure (‡ 130/85 mmHg) is recognized. For other patientgroups, including the elderly, recommendations are to initiatetreatment where BP is persistently ‡ 140/90 mmHg. How-ever, evidence for these guidelines comes mainly from obser-vational data, post hoc analysis of outcome trials and theeffects of BP lowering on subclinical damage. Moreover, inthe majority of trials the initial BP pressure values were diffi-cult to determine because subjects were recruited while receiv-ing antihypertensive drugs at baseline. Frequently, subjectsfrom so-called ‘low-risk groups’ had symptoms of subclinicalorgan damage, which increases their risk category. Also, nor-mal BP was differently defined and, in the ‘normotensive’arm of the ABCD (Appropriate Blood Pressure Controlin Diabetes) trial, included diabetic patients with SBP< 160 mmHg [40]. In the ADVANCE trial, the significant ben-efit of antihypertensive treatment was observed in diabeticswith initial SBP values ‡ 140 mmHg, but not in those withlower values [3]. Similar objections can be raised regarding theclinical trials which included patients with coronary heart dis-ease (INVEST, HOPE) or previous cerebrovascular incident(PROGRESS) [41-43].
In the most recent Cardio-Sis trial (see below), whichincluded patients without diabetes and known signs of sub-clinical organ damage, there was a requirement that systolicBP at baseline should be ‡ 150 mmHg and subjects had tobe treated for 12 weeks and present with at least one risk fac-tor [8]. Therefore, the substantial number of patients in theCardio-Sis study might actually belong to at least a moderaterisk category. Also, there is no single trial on elderly hyperten-sive patients that recruited patients with a SBP in the grade1 hypertension range (< 160 mmHg).
The goal of BP-lowering treatment is to prevent organ dam-age, and it should be administered immediately hypertension isdiagnosed. In patients with high BP, there are no data fromclinical trials on treatment benefits; however, the therapy post-poned the development of stage 1 hypertension in prehyperten-sive subjects (TROPHY [Trial of Preventing Hypertension],PHARAO [Prevention of Hypertension with the ACE-inhibitor Ramipril in Patients with High-normal BloodPressure]) [44,45]. In the ongoing TIResiAS trial, young (aged18 -- 40 years) prehypertensive persons are temporarily treatedwith ACE inhibitors or placebo for 1 year and their BP valuesand LVMwill be estimated 2 years after cessation of therapy [46].For diabetic subjects at risk presenting with microalbuminuriaor proteinuria, early treatment based on RAS inhibition is stillrecommended [1].
5. What is the optimal goal BP in subjectswith cardiovascular disease?
The ESH/ESC 2007 guidelines recommended lowering BPto < 140/90 mmHg in the general population and to< 130/80 mmHg in subjects with high or very highcardiovascular risk [2]. As it reviewed in Reappraisal, in the
majority of analyzed trials the suggested goal pressure has notbeen reached in the prevailing group of patients [1]. Moreover,in only a few small trials (ABCD, SANDS [Stop Atherosclero-sis in Native Diabetics Study]) were SBP values < 130 mmHgactually achieved, and they were associated with questionableclinical benefit, mostly related to surrogate end points [40,47].Similar results were found in trials that included patients witha history of coronary heart disease or cerebrovascular incidentwith no further risk reduction when BP was lowered to< 130 mmHg [48-52]. According to a review based only ondata from randomized controlled trials, there is no evidencethat lowering BP to targets < 140 -- 160/90 -- 100 mmHg isbeneficial to any hypertensive patient in terms of reducing mor-bidity and mortality. The only evidence in favor of currentlyrecommended BP goals is for diastolic blood pressure(DBP) £ 90 -- 100 mmHg, but there is no additional reductionin morbidity or mortality in lowering it to £ 85 mmHg.
The ACCORD (Action to Control Cardiovascular Risk inDiabetes) BP trial addressed the possible role of more aggres-sive BP lowering [9]. A total of 4733 diabetic patients wererandomized, in a non-blinded fashion, to an intensiveBP-lowering regimen with a target systolic BP goal of< 120 mmHg -- with patients on average taking 3.5 anti-hypertensives -- or standard BP lowering, where the goalwas < 140 mmHg. The primary composite outcome was non-fatal MI, nonfatal stroke, or death from cardiovascular causes,and the mean follow-up was 4.7 years. After 1 year, the meansystolic pressure (SBP) was 119.3 mmHg in the intensiveBP-lowering group and 133.5 mmHg in the standard group.There was no significant difference in the primary end pointbetween the groups. There was also no difference betweenthe groups in terms of prespecified secondary end points,which included the primary outcome plus revascularizationor nonfatal heart failure; major coronary disease events; andfatal or nonfatal heart failure. The significant difference instroke between the intensive and standard BP-loweringarms was noted, yet stroke was relatively uncommon, and89 patients had to be treated for 5 years to prevent onestroke. Subjects assigned to the intensive-therapy groupwere more likely to experience adverse events due to anti-hypertensive therapy (3.3, vs 1.3% in the standard-therapygroup; p < 0.001).
In another recently published trial, Cardio-Sis, a total of1111 non-diabetic individuals aged ‡ 55 years withSBP ‡ 150 mmHg were randomly assigned to a targetSBP < 140 mmHg (usual control) or < 130 mmHg. All trialparticipants had been taking antihypertensive medicationfor ‡ 12 weeks and had at least one additional risk factor, asdefined by ESH/ESC hypertension management guidelines [8].The usual-control group reached a mean BP of 135.6/78.7mmHg and the tight-control group reached a mean of131.9/77.4 mmHg. Throughout the study, use of antihyper-tensive drugs increased equally in both groups, although useof diuretics and ARBs was more frequent in the tight-controlgroup. By the end of the study, 17.0% of the usual-control
Gaciong & Symonides
Expert Opin. Pharmacother. (2010) 11(16) 2583
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

group had ECG-documented LVH, the primary end point ofthe trial, compared with only 11.4% of the tight-control group(p = 0.013). A composite cardiovascular end point occurred in9.4% of patients in the usual-control group versus 4.8% in thetight control group (p = 0.003). Among the components ofthe composite end point, rates of new-onset atrial fibrillationand coronary revascularization were significantly lower in thetight-control group than the usual-control group (1.8 vs3.8%, p = 0.044; and 0.9 vs 2.7%, p = 0.032, respectively).Adverse events were rare, generally mild, and did not differsignificantly between the two groups.The Cardio-Sis trial was not double-blind and there were
few clinical events due to the small sample size, yet its resultssuggest potential benefits for tight BP control beyondcurrently recommended levels in selected groups of patients.In many trials (VALUE, ONTARGET, PROGRESS,
INVEST, ADVANCE, TNT), post hoc analysis has been per-formed to evaluate the relationship between achieved BP andcardiovascular incidents. Data from these studies show a pro-gressive reduction in cardiovascular events with progressivelowering of SBP down to around 120 mmHg and DBPdown to about 75 mmHg. However, it should be emphasizedthat within the lower ranges of BP the observed benefit wassmaller than expected based on the difference in mmHg [53,54].These findings do not apply to nephroprotection in dia-
betic subjects. In ADVANCE trial, administration of fixedperindopril--indapamide combination resulted in reducedrisk of renal end point as the SBP achieved during treatmentdecreased to values about 110 mmHg regardless of initialBP level [36].Also, the issue of ‘the J-curve phenomenon’ reappeared
due to post hoc analyses of the results of trials on high-riskpatients. For example, a secondary analysis of the INVEST trial(The International Verapamil-Trandolapril Study) of > 22,000patients demonstrated a a strong J-shaped relationship betweenDBP and adverse outcomes (death, nonfatal MI or nonfatalstroke). In this study, however, more patients with a mean fol-low-up DBP < 70 mmHg had a history of MI and heart failurethan those with higher diastolic pressures (> 40 vs < 30%, and10 vs 5%, respectively). The J-shaped relationship wasmarkedly attenuated in multivariate analyses adjusted for MI,heart failure, and risk factors for cardiovascular disease, suggest-ing that the J-shaped relationship is partly related to underlyingcoronary artery disease [50].Previous randomized trials with placebo control have shown a
similar J-curve in both treated and placebo groups and for non-cardiovascular as well as cardiovascularmortality, suggesting thatpatients with lower DBPs are at higher risk independent ofantihypertensive therapy. The J-curve for MI and DBP hasbeen found in VALUE, TNT, ONTARGET, SYST-EUR,INSIGHT,HOT,ACTION, PROVE-IT, and other large, pro-spective, randomized trials. In most of these, the J-curve for cor-onary events and DBP was more pronounced in patients withmanifest coronary artery disease (CAD) than in patients withoutCAD. It is possible that patients with CAD do worse at these
lower pressures because much coronary filling occurs dur-ing diastole; alternatively, low DBPs may be a reflection ofunderlying severe vascular disease, or other chronic illness.This hypothesis is supported by results of the ROADMAP study(Olmesartan and Diabetes Microalbuminuria Prevention), pre-sented during the ESH meeting in Oslo in June 2010, whichshow a lower incidence of new-onset nephropathy in diabeticsubjects receiving olmesartan as compared to placebo. A slightexcess of cardiovascular deaths was noted in the ARB-treatedgroup, but only in patients with pre-existing atheroscleroticcomplications and SBP < 120 mmHg.
The current reappraisal of the ESH/ESC guidelines statesthat there is sufficient evidence to recommend that SBP belowered to < 140 mmHg and DBP < 90 mmHg in all hyper-tensive patients, regardless of their cardiovascular risk. How-ever, the benefits of lowering SBP to < 140 mmHg were nottested in clinical trials in the elderly.
Lowering SBP to < 130 mmHg may provide benefit in sub-jects with uncomplicated hypertension, but patients withadvanced atherosclerotic artery disease may be exposed tohigher risk with SBP/DBP values < 120/75 mmHg (J-curvephenomenon). However, the J-curve is probably explainedby poor health associated with lower BPs rather than anadverse effect of antihypertensive therapy. More aggressiveBP lowering slows the rate of progression of chronic renal dis-ease in patients with daily urinary proteinuria > 1 g, as well asin diabetics at risk of nephropathy [55].
6. What is the optimal choice ofantihypertensive drug?
The main benefits of antihypertensive therapy are due tolowering BP itself and are largely independent of the class ofdrugs used. The 2007 ESH/ESC hypertension guidelines listedfive classes of drugs considered appropriate as first-line therapy:
- Diuretics- ACE inhibitors- Calcium channel blockers (CCBs)- ARBs- Beta-blockers.
The choice of a particular medication is based on concom-itant diseases and risk factors that constitute indications orcontraindications for specific classes of antihypertensive drugs.The list is compelling, and relative indications has notchanged substantially. A number of major new trials and addi-tional retrospective analyses have since added important evi-dence in favor of the protective effects of ACE inhibitors,ARBs, and CCBs alone or in combination.
6.1 Beta-blockersThe use of beta-blockers in hypertension remains controver-sial [56], yet clinical trial evidence as well as meta-analysesshow that beta-blockers have relative advantages and
Hypertension 2010: what was new for the cardiologist?
2584 Expert Opin. Pharmacother. (2010) 11(16)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

inconveniences. The largest meta-analysis ever performed,which included 147 randomized trials, showed only lowerefficacy of beta-blockers (17 vs 29% reduction with otherclasses of antihypertensive drugs) in preventing stroke, nodifference in preventing coronary events and heart failure,and a higher efficacy than other drugs in patients withrecent acute coronary incidence [13]. Compared with otheragents -- particularly ACE inhibitors or ARBs -- beta-blockersare less efficient in reduction of LVH, increased intima-media thickness, arterial stiffness and central pressure.They also have well-known adverse metabolic effects, partic-ularly in combination with diuretics, and recent meta-analysis reported an increased risk of new-onset diabetesby 33% as compared to placebo or other classes of anti-hypertensive drugs [14]. However, it should be noted thatbeta-blockers do not constitute a homogenous class and‘vasodilating’ agents (carvedilol, nebivolol, celiprolol) maynot share negative properties with older agents. Carvedilolshows a better metabolic profile than metoprolol bothin terms of risk of new-onset diabetes and control ofestablished disease (COMET, GEMINI studies) -- [57,58].Nebivolol reduces central arterial pressure and improvesendothelial dysfunction as well as its use is associated withlower risk of erectile dysfunction [59]. Both drugs showbenefit in clinical outcomes in patients with heartfailure [60,61].
6.2 DiureticsAmerican guidelines (JNC-7) recognize thiazide diuretics asthe first choice in therapy of uncomplicated hypertension [62].However, the evidence base for thiazide diuretics refers to datafrom trials done in the 1980s and 1990s, when the dose ofdiuretics used was about four times greater than that nowused. Some hypertension experts draw attention to the factthat there are no data showing that 12.5 -- 25 mg of hydro-chlorothiazide (HCTZ) reduces heart attack and stroke ordeath [63]. All other trials that have shown improvements inoutcomes with diuretics have employed drugs other thanHCTZ, like chlorthalidone in SHEP and ALLHAT, andindapamide in PROGRESS, ADVANCE and HYVET.Comparisons based on 24-h ambulatory blood pressure(ABP) monitoring show that thiazide-like diuretics (chlortha-lidone and indapamide) are about 1.5 -- 2.0 times morepotent and have a much longer duration of action thanHCTZ, with a similar effect on serum potassium levels [17].In the ACCOMPLISH (Avoiding Cardiovascular Eventsin Combination Therapy in Patients Living with SystolicHypertension) trial, combination of HCTZ with an ACEinhibitor was less effective in prevention of cardiovascularcomplications than the same ACE inhibitor with a CCB [7].Also, replacement of HCTZ with a CCB in combinationwith ARB reverses glucose intolerance in subjects withmetabolic syndrome (The Study of Trandolapril/VerapamilSR and Insulin Resistance -- Long-Term Extension Trial,STAR-LET) [64].
6.3 ACE inhibitors and angiotensin receptor
antagonistsDebate is ongoing as to whether ACE inhibitors can be substi-tuted with ARBs. In the TRANSCEND (Telmisartan Ran-domized Assessment Study in ACE-I Intolerant Subjectswith Cardiovascular Disease) study, in subjects with high car-diovascular risk and intolerant of ACE inhibitors, treatmentwith telmisartan resulted in only a small and nonsignificantreduction in cardiovascular events as compared to placebo [5].Similar findings were reported in the PROFESS (PreventionRegimen for Effectively avoiding Second Strokes) trial, whichevaluated efficacy of telmisartan in secondary prevention ofcerebrovascular events [65]. Yet results of the very largeONTARGET trial have shown that telmisartan was not statis-tically inferior to ramipril in the effect on cardiovascular endpoints [4]. The results of this study question the credibilityof a different meta-analysis that suggested lower efficacy ofARBs in preventing MI, as well as claims that ACE inhibitorsare inferior to sartans in preventing strokes [66,67]. In theONTARGET trial, > 60% of patients recruited to the studyhad a history of coronary heart disease and the rates of MIand stroke were similar in both treatment groups.
Meta-analysis also suggested reduced risk of new-onsetdiabetes with treatment based on RAS blockade [15]. In partic-ular, telmisartan has repeatedly been shown to activatePPAR-g receptors, resulting in a favorable metabolic profileand anti-diabetogenic potential [68]. However, in theONTARGET trial there was no difference in diabetes riskin patients treated with telmisartan or ramipril; also ramiprilonly slightly improved glucose tolerance as compared to pla-cebo in the DREAM (Diabetes Reduction Assessment withRamipril and Rosiglitazone Medication) study [69]. Recentlypublished data from NAVIGATOR (Nateglinide and Valsar-tan in Impaired Glucose Tolerance Outcomes Research) trialshow reduced by 14% relative risk of new-onset diabetes inpatients with glucose intolerance receiving valsartan [10]. Yetimprovement in metabolic profile in valsartan-treated subjectswas not associated with reduction in cardiovascular risk.
In the CHARM (Candesartan in Heart Failure -- Assess-ment of Mortality and Morbidity) study, which includedpatients with heart failure treated with candesartan, a signifi-cant excess of fatal cancers was observed; but investigatorsconcluded that this finding was probably due to chance [70].New cancer data available for 61,950 patients from five trials,with most patients (85.7%) receiving telmisartan as the studydrug, were used for meta-analysis to assess the incidence ofnew cancer. In the meta-analysis, patients randomly assignedto receive ARBs had a significantly increased risk of new can-cer occurrence, compared with those in the control groups(7.2 vs 6.0%; risk ratio [RR] 1.08; p = 0.016). When analysiswas limited to trials where cancer was a prespecified endpoint, the RR was 1.11 (p = 0.001). Among the malignanciesexamined -- lung, breast, and prostate -- only new lung canceroccurrence was significantly higher in those randomlyassigned to ARBs than in control subjects (0.9 vs 0.7%; RR
Gaciong & Symonides
Expert Opin. Pharmacother. (2010) 11(16) 2585
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

1.25; p = 0.01). There was no significant difference in cancerdeaths observed in the meta-analysis between those whotook ARBs and control subjects (1.8 vs 1.6%; RR 1.07;p = 0.183) [71].The mechanism of potential association between ARBs and
lung cancer risk remains speculative. In animal models, block-ade of the angiotensin receptor type 1 and direct stimulationof angiotensin receptors type 2 -- both of which are affectedby ARBs -- are capable of stimulating tumor angiogenesis.But the relevance of these observations in human malignancyis largely unknown. Also, it is difficult to explain differencesin cancer incidence over a very short period of observation,while development of lung cancer usually takes about 10 years.The observed risk is small and can be compared to that of pas-sive smoking, but the results of meta-analysis should still beconsidered hypothesis-generating and more studies in thisarea are needed. In their meta-analysis, the authors omittedmany trials that contain cancer data. Only adding cancer casesfrom the VALUE trial abolishes the association between ARBsand cancer risk [72].
6.4 Calcium antagonists (CaCB)Recent meta-analyses suggest that CaCB offer better protec-tion against stroke but are less efficient in preventing heartfailure [13]. However, when BP difference was considered,the efficacy of CaCB in preventing heart failure was onlyslightly lower than other antihypertensive agents (19 vs24%). CaCB show a neutral metabolic profile and they maybe used in combination with other drugs, in particular RASblockade (discussed below). At the moment, this group hasbeen completely cleared from the suspicion of causing anexcess of coronary complications.
6.5 Combination therapyNumerous data from clinical trials demonstrate that BPcontrol requires administration of at least two drugs in mostpatients. A meta-analysis of 42 different studies with> 11,000 patients has shown that adding another antihyper-tensive drug is five times more effective than doubling thedose of existing drug [17]. Combination therapy may offera synergism not only in lowering BP but also in organprotection. This notion is confirmed by data from various tri-als (ASCOT BPLA, STAR, ACCOMPLISH, ADVANCE)that used defined combinations of BP-lowering drugs.The 2007 guidelines strongly favored combination therapy,
which most hypertensive patients needs to achieve their BPgoal. Combinations as an initial therapy were particularlyrecommended in patients with high cardiovascular risk or/andthose who need reduction of BP by > 20/10 mmHg of SBP/DBP values, respectively. The guidelines stated that combina-tion should be based on a complementary mechanism of actionthat delivers additional BP reduction and/or minimizes individ-ual side effects. Any combination that fulfils these criteriacould be used; however, trial data suggest important clinicaldifferences between specific combinations.
The 2009 update provides practical information aboutadvantages and disadvantages of specific two-drug combina-tions. Combination of thiazide (or thiazide-like diuretic)with RAS blockade is among the most frequently used in clin-ical practice. Fixed-dose perindopril--indapamide combina-tion was used in ADVANCE -- the largest-ever study oftreatments for type 2 diabetes mellitus which included popu-lation of 11,140 patients, mean age 66 years, with at least oneadditional risk factor for cardiovascular disease who were ran-domized to combination or placebo [3]. ConcomitantBP-lowering therapy (including ARBs and ACE inhibitors),except thiazide diuretics, was allowed at the discretion ofthe treating physician. Over a mean follow-up duration of4.3 years, average BP in the active treatment group was134.7/74.8 mmHg compared with 140.3/77.0 mmHg inthe placebo group. The primary end point of the study, acomposite of major macrovascular (death from cardiovasculardisease, nonfatal stroke or nonfatal MI) and microvascular(new or worsening renal or diabetic eye disease) events, wasreduced by 9% with active treatment versus placebo (hazardratio [HR] 0.91, 95% CI 0.83 -- 1.00, p = 0.041). The relativerisk of death from cardiovascular disease was reduced by 18%(HR 0.82, p = 0.027) and all-cause mortality by 14% (HR0.86, p = 0.025) in the active treatment arm, with significantreductions also seen with active treatment in total coronaryevents (14%) and total renal events (21%). Indapamide, towhich perindopril was added if the target BP of 150/80 wasnot reached, was used in the HYVET trial, which randomizedpeople aged > 80 and with sustained systolic blood pressure> 160 mmHg. Over a follow-up of only 2 years, active treat-ment as compared to placebo resulted in a significant 21%reduction of total and cardiovascular (21%) mortality. Riskof stroke was also significantly reduced, by 30%; new heartfailure by 64%. Serious adverse events were much more fre-quent with placebo (448 vs 358 instances) than with activetreatment [6]!
However, the presence of diuretic in combination mayincrease a probability of development of diabetes in popula-tion with high metabolic risk. In the STAR trial, patientswith glucose intolerance treated with losartan/HCTZ combi-nation showed higher incidence of new-onset diabetes ascompared to those receiving trandolapril/verapamil (T/V11.0 vs L/H 26.6%; p = 0.002) [73]. In the continuation ofthe trial (STARLET), patients on losartan/HCTZ switchedto trandolapril/verapamil combination, which resulted inimprovement of serum glucose concentration and insulinvalues [64].
Combination of ACE inhibitor or ARB with CCB offersnot only better metabolic profile, but also fully additive BPreduction; more importantly, it has been shown to providethe most efficient protection against target organ damage. Inthe ASCOT-BPLA (Anglo-Scandinavian Cardiac OutcomesTrial -- Blood Pressure-lowering Arm) trial, treatment withamlodipine--perindopril combination was more effective inlowering BP and cardiovascular events than combination of
Hypertension 2010: what was new for the cardiologist?
2586 Expert Opin. Pharmacother. (2010) 11(16)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

a beta-blocker with a thiazide [74]. In the EUROPA (EuropeanTrial on Reduction of Cardiac Events with Perindopril in Sta-ble Coronary Artery Disease) trial, patients with stable coro-nary heart disease who received perindopril experienced20% relative risk reduction of a composite cardiovascularend point of cardiovascular death, nonfatal MI, and resusci-tated cardiac arrest as compared to placebo-treated controls.At baseline, 32% of the EUROPA population were receivingCCB and post hoc analysis shows a significant clinical benefit(46% reduction in total mortality) compared with patientswho were not treated with CCB along with ACE inhibitor.Altogether, these data suggest a potential synergism and clin-ically important interaction between ACE inhibitors andCCB [75].
The ACCOMPLISH study was the first clinical outcometrial to compare different fixed-dose combinations. Over11,000 hypertensive patients with elevated cardiovascularrisk were randomized to receive an ACE inhibitor (benazepril)plus a calcium channel blocker (amlodipine or HCTZ). Thetrial was prematurely stopped after 36 months because thebenazepril--amlodipine combination was superior to the bena-zepril--HCTZ combination in reducing all cardiovascular fataland nonfatal events except for heart failure [7]. Further analysishas shown that the ACE inhibitor/CCB combination slowsprogression of chronic kidney disease to a greater extentthan ACE inhibitor/HCTZ [76].
It has been suggested that double RAS blockade with anARB plus an ACE inhibitor is useful in patients with renaldisease in whom proteinuria is insufficiently reduced withan ARB or ACE inhibitor alone. Evidence that this combina-tion is protective in renal outcomes came from the COOPER-ATE (Combination Treatment of Angiotensin-II ReceptorBlocker and Angiotensin-Converting-Enzyme Inhibitor inNon-Diabetic Renal Disease) trial including subjects withchronic kidney disease, but the credibility of this study wascalled into question and it was eventually retracted by thepublisher [77]. In hypertensive subjects, as observed in theONTARGET study, ARB/ACE inhibitor combination hasbeen associated with worsening of renal outcomes [4]. Thus,the direct evidence of the advantages of dual RAS blockadefor nephro/cardiovascular protection remains limited, whereasit is often associated with an increase in side effects like hyper-kalemia or decline in GFR. ACE/ARB combinations producelittle additional BP reduction compared with monotherapywith either agent alone, and in the ONTARGET study theACE inhibitor/ARB combination was less effective in preven-tion of cardiovascular end points. Therefore, for treatment ofhypertension this combination is not recommended. Yet therole of double blockade in subjects with established glomerul-opathy with substantial proteinuria is uncertain. In the ongo-ing VA-NEPHRON-D trial, the effect of ACE inhibitor/ARBcombination versus standard treatment with ARB on the pro-gression of kidney disease in individuals with type 2 diabetesand overt nephropathy is being evaluated; the study will becompleted in 2013.
The combination of a calcium antagonist with a diuretic isaccepted in the reappraisal of current guidelines, despite lackof synergistic effect in BP lowering. This combination wasused in the FEVER (Felodipine Event Reduction), ELSA(European Lacidipine Study on Atherosclerosis) and VALUEtrials with some clinical benefits [78-80]. In a population-based case-control study, patients treated with diuretics withCCB had a higher risk of MI than subjects receiving adiuretic/beta-blocker combination [81]. These findings suggestavoiding these combinations if possible.
6.6 Fixed-dose combinationsGuidelines recommend using fixed-dose combinations of twodrugs when initial monotherapy has failed and another drug isneeded to control BP, or as the first step in subjects requiringsubstantial BP reduction due to either high initial values orcardiovascular risk. Fixed-dose combinations, by reducingthe number of medications, facilitates adherence to therapy.A study using pharmacy records found that adherence wasinversely related to the number of medications and drops dra-matically with increasing number of doses taken per day from71% with once-daily dosing to 31% with four daily doses ofantihypertensive medications [82].
Employing low-dose fixed-combination therapies, asopposed to the usual treatment guidelines, which are com-plex, allows for better BP control. This was clearly demon-strated in the Canadian STITCH (Simplified TreatmentIntervention to Control Hypertension) trial, where a simplealgorithm was used consisting of four steps: initial use ofa low dose of diuretic/ACE inhibitor or diuretic/ARBfixed-dose combination; up-titration of combination therapyto the highest dose; addition of a calcium-channel blockerand up-titration; and addition of a non--first-line antihyper-tensive agent [83]. Family physician practices were asked toenroll patients with uncontrolled hypertension and employeither the STITCH algorithm (18 practices) or the usualCanadian guidelines (27 practices), then assess the proportionof patients treated to target BP after 6 months (< 140/90mmHg for those without diabetes mellitus, < 130/80 mmHgfor those with diabetes). The proportion achieving BP targetwas significantly higher in the intervention group (64.76 vs52.7%; p = 0.026), and multivariate analysis showed thatassignment to the simple-algorithm arm increased the chanceof reaching BP target by 20% (p = 0.028).
Rational drug combinations may improve overall tolerabil-ity of the treatment when side effects associated with a partic-ular agent are neutralized by pharmacological properties ofanother drug. An example is the use of low-dose combinationof ACE inhibitor and dihydropyridine CCB in a patient whoexperienced edema at a higher CCB dose [84].
Wald and Law described the concept of the single ‘polypill’that should contain different medications (triple antihyperten-sive combination, statin, aspirin and folic acid) for primary orsecondary prevention of heart disease [85].The Indian PolycapStudy (TIPS), tested ‘Polycap�’, a new capsule version of the
Gaciong & Symonides
Expert Opin. Pharmacother. (2010) 11(16) 2587
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

polypill containing low doses of five generic drugs: b-blocker(atenolol 50 mg), a diuretic (HCTZ 12.5 mg), an ACE inhib-itor (ramipril 5 mg), a statin (simvastatin 20 mg), and aspirin(100 mg). Each component in the formulation of Polycapshowed efficacy similar to the effects of each alone. Also, the tol-erability of the Polycap was similar to that of other treatments,with no evidence of increasing intolerability with increasingnumber of active components in a single capsule [86].The ‘red heart pill’ is another polypill combination (ACE
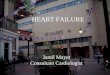
inhibitor, diuretic, aspirin and simvastatin) being tested inpatients at moderate risk of cardiovascular disease in the Pro-gram to Improve Life and Longevity (PILL) pilot study and inthe Improving Adherence using Combination Therapy(IMPACT) trial. Results of a three-drug polypill containingaspirin, a statin, and an ACE inhibitor for secondary preven-tion in patients who have had a MI will be available in 2010.Nevertheless, the limited efficacy of aspirin and statins inprimary prophylaxis (see Section 8) questions the originalpolypill concept, and multiple drug combinations may be rec-ommended only for secondary prevention in high-risk sub-jects. Possible combination for initiation of antihypertensivetherapy are presented in Figure 1.
7. Treatment strategies in special conditions
7.1 ElderlyPublication of the results of HYVET trial (Hypertension inthe Very Elderly Trial) provided much needed informationof the effect of BP lowering in the very elderly. In the HYVETstudy, patients aged ‡ 80 years in whom entry SBPwas ‡ 160 mmHg (average 173 mmHg) were randomizedto receive either placebo or active treatment, consisting ofindapamide (1.5 mg daily) and the eventual addition of theACE inhibitor perindopril (2 and 4 mg daily) with the targetto attain a SBP value < 150 mmHg. The trial was stoppedafter < 2 years because of evident clinical benefits, includingreduction in stroke (30%), congestive heart failure (64%),and major cardiovascular events, and all-cause death (21%)in the active treatment group as compared to placebo. Thetherapy was very well tolerated, with a similar number ofadverse effects in both treatment and placebo arms [6].It is uncertain whether the HYVET results can be trans-
lated into a population of the same age, but with the morewidespread vascular damage that clinicians often see. Resultsin sicker populations may be better because of a higher eventrate and a potentially higher absolute benefit, but may also beworse because risks may be less dependent on BP.The Reappraisal of the ESH/ESC guidelines raises an issue
of lack of evidence of benefits of antihypertensive therapy inelderly people with grade 1 hypertension (SBP 140 -- 159mmHg) as well as when on-treatment SBP values were low-ered to < 140 mmHg. Secondary analysis of available datafrom trials in subjects with isolated systolic hypertensionshows an increased risk when DBP values are loweredto < 65 mmHg [87].
Thus, the current guidelines recommend the same treatmentalgorithm in elderly and younger patients. Treatment should becontinued or initiated when subjects turn 80, with initialmonotherapy with thiazide (or thiazide-like) diuretic.
7.2 Diabetes and coronary heart diseaseThe treatment strategy regarding the threshold and goal ofBP, as well as selection of antihypertensive drugs, werediscussed earlier.
7.3 Atrial fibrillationPost hoc analyses of data from heart failure and hypertensiontrials show a lower incidence of episodes of atrial fibrillation inpatients receiving RAS blockade. Therefore, the 2009 ESH/ESC guidelines recommended ARBs or ACE inhibitors inpatients at high risk of recurrent atrial fibrillation. It washypothesized that RAS blockade inhibits atrial structural andelectrical remodeling, which was directly shown in studieson animal models of atrial fibrillation. In a recent meta-anal-ysis of 23 randomized controlled trials including87,048 patients, RAS inhibition reduced the odds for atrialfibrillation by 33% overall, with greater effect in subjectsreceiving antiarrhythmic drugs [16]. These data were not con-firmed in specific trials (Candesartan in the Prevention ofRelapsing Atrial Fibrillation -- CAPRAF, Gruppo Italianoper lo Studio della Sopravvivenza nell’Infarto Miocardico --Atrial Fibrillation -- GISSI-AF), which were designed to assessthe effect of ARBs on incidence of recurrent episodes of atrialfibrillation [88,89].
7.4 Stroke and transient ischemic attackPatients with a history of cerebrovascular incident are consid-ered a population at high risk who warrant an early andintensive antihypertensive therapy. Nevertheless, there are insuf-ficient data to recommend initiation of therapy with high nor-mal BP. Also post hoc analysis of data from the PROGRESS(Perindopril Protection against Recurrent Stroke Study) trialsuggests that lowering SBP to < 130 mmHg is not associatedwith further reduction of the risk of future incidents [54].
Another unresolved issue is optimal BP managementduring the acute phase of stroke. The relevant clinical trialshave yet to be completed. Also, the belief in neuroprotectiveactivity of RAS inhibition has not been confirmed inclinical trials. The PRoFESS trial (Prevention Regimen forEffectively Avoiding Second Strokes) randomly assigned20,332 patients with non-cardioembolic ischemic stroke toreceive either telmisartan (80 mg daily) or placebo [65]. Approx-imately three-quarters of patients had a prior history of hyper-tension, and the average BP was 144/84 mmHg in both groupsat baseline. At an average follow-up of 2.5 years, there was nodifference between the telmisartan and placebo groups in theprimary outcome of recurrent stroke, or in secondary outcomesincluding major cardiovascular events. This finding is similar tothe lack or benefit with perindopril monotherapy in thePROGRESS trial, in which benefit was seen only in patients
Hypertension 2010: what was new for the cardiologist?
2588 Expert Opin. Pharmacother. (2010) 11(16)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

treated with perindopril plus indapamide, which producedsubstantially greater BP reduction [43].
7.5 Atherosclerotic renovascular diseaseRenovascular hypertension, mostly due to atherosclerosis, isconsidered the second most common cause of secondaryhypertension, with a prevalence of approximately 2% of adulthypertensives evaluated in specialized centers [90]. With theuse of low-profile stents, atherosclerotic renal artery stenosiscan be successfully treated in about 100% of cases with reste-nosis in the range of 0 -- 23%, depending on the diameter ofthe renal artery [91]. Yet the treatment of patients with athero-sclerotic renal hypertension is a controversial issue due to thelimited number of large-scale long-term outcome trialscomparing different therapeutic approaches, as well as thedifficulty to predict BP response to renal revascularizationprocedures in individual patients [92].
Until the year 2009, data from only three randomized, rel-atively small studies comparing percutaneous angioplasty withmedical treatment alone were available [93-95]. In the year2009, two randomized trials addressing the issue of percuta-neous revascularization in patients with atheroscleroticrenovascular disease (STAR and ASTRAL) were published.
The STAR trial (Stent Placement and Blood Pressure andLipid-lowering for the Prevention of Progression of RenalDysfunction Caused by Atherosclerotic Ostial Stenosis ofthe Renal Artery) was performed in 10 centers and enrolled140 patients with ostial renal artery stenosis > 50% [96]. Otherinclusion criteria were BP controlled to < 140/90 mmHgon stable medication 1 month before the study, if
possible without ACE inhibitors, and creatinine clearance of15 -- 80 ml/min. Exclusion criteria were: renal size < 8 cm,renal artery diameter < 4 mm, estimated creatinineclearance < 15 ml/min/1.73 m2, diabetes mellitus with pro-teinuria (3 g/d), and malignant hypertension. Patients wererandomized for stent placement and medical treatment(64 patients) or medical therapy alone (76 patients), whichincluded all classes of antihypertensive drugs along withmandatory atorvastatin and low-dose aspirin.
Only 46 of the 64 patients assigned for stenting eventuallyunderwent the procedure, and they did not differ fromcontrol group in BP control, renal function and rate of cardio-vascular complications. Serious complications occurred in thestent group, including two procedure-related deaths. Theauthors concluded that stent placement with medical treat-ment has no clear effect on progression of impairedrenal function and leads to a small number of significantprocedure-related complications.
Similar conclusions come from ASTRAL (The Angiographyand Stenting for Renal Artery Lesions), another multicentertrial that randomized 806 patients with atherosclerotic renaldisease either to undergo percutaneous revascularization inaddition to receiving medical therapy or to receive medicaltherapy alone. Inclusion criteria were substantial anatomicalatherosclerotic stenosis in at least one renal artery suitable forendovascular revascularization and lack of physician’s beliefthat the patient would definitely have a worthwhile clinicalbenefit from revascularization. During the median follow-up of 34 months, the decline in renal function over time wasslightly slower in the revascularization group, but the
Thiazide/thiazide-likediuretics
ACE inhibitors
Calcium antagonists
Angiotensinreceptor blockersβ-blockers
LIFE, VALUE
ASCOTACCOMPLISH
ADVANCEPROGRESS
HYVET
ONTARGET
ASCOT
ELSAVALUEFEVER
Figure 1. Possible combinations between basic classes of BP-lowering drugs for initiation of antihypertensive therapy. The
preferred combinations are represented as solid lines, combinations that should be avoided with double lines, and the dotted
line indicates combination of questionable benefit. Acronyms of trials where these combinations were tested are noted.
Gaciong & Symonides
Expert Opin. Pharmacother. (2010) 11(16) 2589
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

difference was not statistically significant (p = 0.06). There wasno significant difference in SBP between the studied groups.The decrease in DBP was smaller in the revascularization groupthan in the medical-therapy group, and the slope for DBPdiverged at the rate of 0.61 mmHg per year (p = 0.03).Post hoc analysis of BP control and the rate of decline of
GFR in the subgroup with severe stenosis, bilateral or narrow-ing of the one existing kidney show advantage of revasculari-zation over medical treatment alone. Serious associatedcomplications in the revascularization group were observedin 23 patients, including two deaths and three amputationsof toes or limbs [11].The results of STAR and ASTRAL, despite their obvious
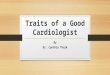
limitations, suggest a conservative approach in the treatmentof atherosclerotic renovascular disease; yet they do not ruleout the possibility that, in selected patients with such classicalindications as flashing pulmonary edema or acute renalfailure, renal artery stenting may be effective. These trialsalso do not provide a clear answer as to whether percuta-neous intervention may be a valuable method of loweringBP in drug-resistant hypertension. The ongoing CORAL(Cardiovascular Outcomes in Renal Atherosclerotic Lesions)study may provide a more definite answer to that query.However, it is worth mentioning, that our meta-analysisof five randomized studies carried out to date, includingSTAR and ASTRAL, revealed significantly lower SBP in theintervention group than in the medically treated group,with a mean weighted difference of only -3.11 mmHg(95% CI -6.15, -0.07; p = 0.04) (Table 1) [96].
8. How should concomitant risk factors betreated?
Reappraisal stated that benefits observed in statin trials withhypertensive patients like ASCOT- LLA endorse their rolein primary prevention, and recommends to initiate this treat-ment in subjects with moderate cardiovascular risk (~ 15%cardiovascular events in 10 years). This statement is mostlybased on data from the JUPITER (Justification for the Useof Statins in Primary Prevention: An Intervention Trial Eval-uating Rosuvastatin) trial in which 17,802 healthy men(aged ‡ 50 years) and women (aged ‡ 60 years) with a low-density lipoprotein cholesterol (LDL-C) level < 130 mg/dl(3.4 mmol/l) and a CRP level ‡ 2.0 mg/l were randomlyassigned to treatment with 20 mg of rosuvastatin daily orplacebo. The trial was stopped early after a median follow-upof 1.9 years because the first major cardiovascular event (non-fatal MI, nonfatal stroke, hospitalization for unstable angina,arterial revascularization procedure, confirmed death fromcardiovascular causes) was lower in patients treated with rosu-vastatin (0.77 vs 1.36 events per 100 person-years; HR 0.56;95% CI, 0.46 -- 0.69), as was the risk of all-cause mortality(1.00 versus 1.25 deaths per 100 person-years; HR 0.80;95% CI, 0.67 -- 0.97) [97]. Achieved hsCRP concentrationswere predictive of event rates irrespective of the lipid end
point used, including the apolipoprotein B to apolipoproteinAI ratio. These data suggest that inclusion of inflammatorymarkers may allow better estimation of cardiovascular risk,yet current guidelines as well as their reappraisal do notrecommend measurement of hs-CRP level.
The clinical relevance of the JUPITER study has been ques-tioned by some researchers who have raised serious objectionsto the trial methodology. Premature termination excluded thepossibility of assessing treatment efficacy over longer periodsand may have exaggerated possible benefit. Furthermore,data show a major discrepancy between significant reductionof nonfatal stroke and myocardial infarction, but no effecton mortality from these two conditions. Also, cardiovascularmortality was unexpectedly lower as compared with totalmortality as well as rate of fatal MI [98]. Also, a recent meta-analysis of 11 randomized controlled trials involving 65,229high-risk participants did not find evidence for the benefiton statin therapy on total mortality in primary prevention [99].In the lipid arm of the ACCORD trial, addition of fenofi-brate to statin did not improve clinical outcome except indiabetic subjects with low high-density lipoprotein choles-terol (HDL-C) (< 34 mg/dl) and hypertriglyceridemia(> 204 mg/dl) [100]. Yet many experts advise administrationof statins in hypertensive subjects with type 2 diabetes andno coronary heart disease, regardless of initial cholesterol level,with the target values for LDL-C < 100 mg/dl (reviewedin [101]).
Current clinical practice strongly recommends low-doseacetylsalicylic acid for secondary prevention in patientswith previous cardiovascular atherosclerotic complications.Findings from secondary prevention trials invariably showoverall benefit over the risk of serious adverse events, partic-ularly intracranial bleeds. Yet the data from primary preven-tion trials are less consistent. A large meta-analysis that alsoincluded six primary prevention trials with 95,000 low-risk individuals the net benefit to be small and associatedwith significant risk of major gastrointestinal and extracra-nial bleeds [102]. Even in patients with asymptomatic athero-sclerosis (Aspirin for Asymptomatic Atherosclerosis -- AAATstudy), also associated with diabetes (Prevention and Pro-gression of Arterial Disease and Diabetes -- POPADAD),low-dose aspirin did not change the rate of cardiovascularcomplications and mortality [12,103]. Therefore, cautionshould be exercised in this group of patients whenaspirin is prescribed, in particular in patients at high risk ofbleeding [104].
9. Conclusions
Management of the hypertensive patient is guided by totalcardiovascular risk, which includes assessment of BP leveland concomitant risk factors with a special emphasis on sub-clinical organ damage and associated diseases. Despite exten-sive research, new indices like intima-media thickness andparameters of arterial stiffness do not improve estimation
Hypertension 2010: what was new for the cardiologist?
2590 Expert Opin. Pharmacother. (2010) 11(16)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

Table
1.Meta-analysisoftheeffect
ofrenalartery
interventionsonSBPco
ntrol.
Studyorsu
bgroup
Angioplasty/stenting
Medicaltreatm
ent
Meandifference
Meandifference
Mean
SD
Total
Mean
SD
Total
Weight
IV,Random,95%
CI
IV,Random,95%
CI
ASTRAL2009
146
25
332
149
25
350
65.5%
-3.00[-6.75,0.75]
Favo
urs
expe
rimen
tal
-20
-10
1020
0Fa
vour
s co
ntro
l
Bax2009
151
23
50
155
26
60
11.0%
-4.00[-13.16,5.16]
Jaarsveld
2000
169
28
55
176
30
50
7.4%
-7.00[-18.13,4.13]
Plouin
1998
140
15
23
141
15
25
12.8%
-1.00[-9.49,7.49]
Websterbilateral1998
166
38
12
177
22
15
1.6%
-11.00[-35.21,13.21]
Websterunilateral1998
170
29
11
163
27
11
1.7%
7.00[-16.42,30.42]
Total(95%
CI)
483
511
100.0%
-3.11[-6.15,-0.07]
Heterogeneity:
Tau2=0.00;Chi2=1.87;df=5(p
=0.87);I2=0%
.
Test
foroveralleffect:Z=2.01(p
=0.04).
Gaciong & Symonides
Expert Opin. Pharmacother. (2010) 11(16) 2591
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

of cardiovascular risk and are not recommended for routineclinical practice. The Reappraisal of current ESH/ESCguidelines, as well as data from more recent research, endorsethe current recommendation to reduce SBP to < 140 mmHg(and DBP to < 90 mmHg) in patients with grade 1 or2 hypertension and low or moderate total cardiovascularrisk, although they point out that there is still no trial evi-dence for whether this should be done in elderly patients.Furthermore, there is also no solid scientific evidence to sup-port lowering BP to < 130/80 mmHg in high-risk patientswith diabetes mellitus or a history of cardiovascular disease.Effective BP control requires multiple drugs with comple-
mentary mechanisms of action, and the time needed to achievegoal BP can affect clinical outcomes. Combining RAS inhibi-tors with CCB may offer effective BP reduction with possibilityof better organ protection. In subjects without clinically evidentatherosclerotic arterial disease, anti-platelet therapy does notoffer significant cardiovascular benefit over the risk of bleedingcomplications. More interest should be directed to issues ofbetter compliance with chronic antihypertensive therapy andpractical implications of guidelines for public health.
10. Expert opinion
Despite continuously accumulating data, many decisions onhypertension management must be taken without the supportof evidence from appropriate clinical trials. We still do notknow the best strategy for dealing with patients with stage1 hypertension, and there is uncertainty about whether sub-jects with BP in the range 140 -- 1499/90 -- 99 mmHg wouldbenefit from antihypertensive treatment.Also, available data from clinical trials do not prove that
lowering BP to < 130 mmHg in high-risk groups translatesinto additional benefit. The Systolic Blood Pressure Interven-tion Trial (SPRINT), funded by the US National Institutesof Health, which will test the effects of tight control ofSBP to < 120 mmHg compared with usual controlto < 140 mmHg on prevention of cardiovascular disease inapproximately 7500 subjects. Participants in SPRINT willbe aged ‡ 55 years, with SPB ‡ 130 mmHg and at least oneadditional risk factor. People with diabetes mellitus or whohave had a stroke will be excluded from SPRINT becausethey were the target groups of other trials (ACCORD,Secondary Prevention of Small Subcortical StrokesTrial -- SPS3) that are testing a lower BP goal.Most major clinical trials have included a direct comparison
of different treatment regimens. However, overall conclusionsbased on the results and large-scale meta-analyses do not indi-cate the absolute winner. Basic drug classes (diuretics, ACEinhibitors, ARBs, calcium antagonists and beta-blockers) canall be considered suitable for both initiation and maintenance
of hypertension. Choice of antihypertensive drugs should bebased on clinical setting. Because most hypertensive patientsrequire multiple drug therapy to control their BP, treatmentwith a fixed-dose combination may offer a valuable optionfor more effective BP reduction and better patient compliance.Results of landmark clinical trials support that combinationscomprised of a RAAS blocker with either a diuretic or CCBshould be considered first-line therapy for patients unlikely toachieve BP goals on a single drug. Based on these findings, cal-cium antagonists may be preferred over diuretics as the initialchoice for dual therapy in most patients, due to lower risk ofdiabetes and possibly better organ protection.
Only one new antihypertensive drug -- aliskiren, an orallyactive renin inhibitor -- has been introduced recently toclinical practice; but many new molecules are currentlyunder investigation, including NO donors, vasopressinantagonists, neutral endopeptidase inhibitors, AT2 angioten-sin receptor agonists, antagonists of endothelin receptors,dual inhibitors of the angiotensin II receptor and neprilysin.Encouraging results from first attempts of treatment of resis-tant hypertension with catheter-mediated ablation of renalsympathetic nerves and data from the ongoing controlledSymplicity HTN-1 trial will be released by the end of 2010.
It is assumed that lowering BP by any means will reduceincidence of cardiovascular events. Given the practical diffi-culty of maintaining long-term BP reductions with lifestylemodification, it would be valuable to test whether the lifestyleapproach in grade 1 hypertensive subjects may affect at leastsubclinical target organ damage.
Finally, guidelines should reconcile scientific evidence withclinical practice and reality of health care. The results of themodeling study based on demographical data from Norwayshow that to provide medical services according to currentESH/ESC 2007 guidelines, the number of primary care physi-cians in the population studied should be at least doubled, whichcreates an unbearable burden on the healthcare system [105].
Other ways of improving BP control in society may be effec-tive, as demonstrated recently in England where rates of BPcontrol in treated patients had increased to > 50% in menand women. These latest improvements are attributed, at leastin part, to the introduction in 2004 of a pay-for-performancesystem that rewards general practitioners financially for achiev-ing certain clinical targets, including lowering BP levels toSBP < 150 mmHg and DBP to < 90 mmHg [106].
Declaration of interest
Z Gaciong has received research grants and consultancy/speaking honoraria from Servier, Sanofi-Aventis, Pfizer,ADAMED, KRKA and Novartis. B Symonides has noconflict of interest to declare.
Hypertension 2010: what was new for the cardiologist?
2592 Expert Opin. Pharmacother. (2010) 11(16)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. Mancia G, Laurent S, Agabiti-Rosei E,
et al. Reappraisal of European guidelines
on hypertension management:
a European Society of Hypertension
Task Force document. J Hypertens
2009;27:2121-58.. Detailed reappraisal of the evidence
underlying 2007 guidelines; integrates
current research and indicates which
recommendations are based on solid
scientific evidence and which on
judgment and tradition.
2. Mancia G, De Backer G, Dominiczak A,
et al. 2007 Guidelines for the
management of arterial hypertension: the
task force for the management of arterial
hypertension of the European Society of
Hypertension (ESH) and of the
European Society of Cardiology (ESC).
J Hypertens 2007;25:1105-87
3. ADVANCE Collaborative Group.
Effects of a fixed combination of
perindopril and indapamide on
macrovascular and microvascular
outcomes in patients with type 2
diabetes mellitus (the ADVANCE
trial): a randomized controlled trial.
Lancet 2007;370:829-40. First clinical trial to demonstrate the
benefits of blood pressure reduction on
both microvascular and macrovascular
events in both hypertensive and
normotensive patients with
type 2 diabetes mellitus.
4. The ONTARGET Investigators.
Telmisartan, ramipril, or both in
patients at high risk for vascular events.
N Engl J Med 2008;358:1547-59. Findings from this trial demonstrate
that telmisartan is an effective and safe
alternative to ramipril, but that
combination therapy with an ACE
inhibitor plus an ARB should not
be used.
5. Telmisartan Randomized Assessment
Study in ACE intolerant subjects with
cardiovascular Disease (TRANSCEND)
Investigators. Effects of the
angiotensin-receptor blocker telmisartan
on cardiovascular events in high-risk
patients intolerant to
angiotensin-converting enzyme inhibitors:
a randomized controlled trial. Lancet
2008;372:1174-83
6. Beckett NS, Peters R, Fletcher AE,
et al.; HYVET Study Group. Treatment
of hypertension in patients 80 years of
age or older. N Engl J Med
2008;358:1887-98. HYVET study provided important
clinical trial data to support the
benefit of treating elevated blood
pressure for persons in their 80s.
7. Jamerson K, Weber MA, Bakris GL,
et al.; ACCOMPLISH Trial
Investigators. Benazepril plus amlodipine
or hydrochlorothiazide for hypertension
in high-risk patients. N Engl J Med
2008;359:2417-28. The only large clinical trial with
different fixed-dose combinations.
8. Verdecchia P, Staessen JA, Angeli F,
et al. Usual versus tight control of
systolic blood pressure in non-diabetic
patients with hypertension (Cardio-Sis):
an open-label randomised trial. Lancet
2009;374:525-33
9. ACCORD Study Group, Cushman WC,
Evans GW, et al. Effects of intensive
blood-pressure control in type 2 diabetes
mellitus. N Engl J Med
2010;362:1575-85
10. NAVIGATOR Study Group,
McMurray JJ, Holman RR, et al.
Effect of valsartan on the incidence
of diabetes and cardiovascular events.
N Engl J Med 2010;362:1477-90. Treatment with valsartan reduced the
risk of new-onset diabetes in subjects
with glucose intolerance but did not
affect the cardiovascular risk.
11. ASTRAL Investigators. Revascularization
versus medical therapy for renal-artery
stenosis. N Engl J Med
2009;361:1953-62. The largest controlled study did not
show the benefits of revascularization
of atherosclerotic renal stenosis, but
the noticeable danger of adverse
side effects.
12. Fowkes FG, Price JF, Stewart MC, et al.
Aspirin for prevention of cardiovascular
events in a general population screened
for a Low Ankle Brachial Index
A Randomized Controlled Trial. JAMA
2010;303:841-8
13. Law MR, Morris JK, Wald NJ. Use of
blood pressure lowering drugs in the
prevention of cardiovascular disease:
meta-analysis of 147 randomised trials
in the context of expectations from
prospective epidemiological studies.
BMJ 2009;338:b1665.. Data from this largest meta-analysis
did not show any significant
difference in clinical efficacy
between major classes of
antihypertensive agents.
14. Bangalore S, Parkar S, Grossman E,
Messerli FH. A meta-analysis of
94,492 patients with hypertension
treated with beta blockers to determine
the risk of new-onset diabetes mellitus.
Am J Cardiol 2007;100:1254-62
15. Andraws R, Brown DL. Effect of
inhibition of the renin-angiotensin
system on development of
type 2 diabetes mellitus (meta-analysis
of randomized trials). Am J Cardiol
2007;99:1006-12
16. Schneider MP, Hua TA, Bohm M,
et al. Prevention of atrial fibrillation
by renin-angiotensin system inhibition
a meta-analysis. J Am Coll Cardiol
2010;55:2299-307
17. Baguet JP, Robitail S, Boyer L, et al.
A meta-analytical approach to the
efficacy of antihypertensive drugs in
reducing blood pressure. Am J
Cardiovasc Drugs 2005;5:131-40
18. Wald DS, Law M, Morris JK, et al.
Combination therapy versus
monotherapy in reducing blood
pressure: meta-analysis on
11,000 participants from 42 trials.
Am J Med 2009;122:290-300. Data from this meta-analysis show
that addition of another
anti-hypertensive drug is five times
more potent than doubling the
dose of existing drug.
19. Havranek EP, Froshaug DB,
Emserman CD, et al. Left ventricular
hypertrophy and cardiovascular
mortality by race and ethnicity.
Am J Med 2008;121:870-5
20. Verdecchia P, Angeli F, Cavallini C,
et al. The voltage of R wave in lead
aVL improves risk stratification in
hypertensive patients without ECG left
ventricular hypertrophy. J Hypertens
2009;27:1697-704
21. Bombelli M, Facchetti R, Carugo S,
et al. Left ventricular hypertrophy
increases cardiovascular risk
independently of in- and out-of office
Gaciong & Symonides
Expert Opin. Pharmacother. (2010) 11(16) 2593
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

blood pressure values. J Hypertens
2009;27:2458-64
22. Zanchetti A, Hennig M, Hollweck R,
et al. Baseline values but not treatment
induced changes in carotid intima media
thickness predict incident cardiovascular
events in treated hypertensives. Findings
in the ELSA. Circulation
2009;120:1084-90
23. Inoue M, Maeda R, Kawakami H, et al.
Aortic pulse wave velocity predicts
cardiovascular mortality in middle-aged
and elderly Japanese men. Circ J
2009;73:549-53
24. Jankowski P, Kawecka-Jaszcz K,
Czarnecka D, et al. Aortic blood pressure
and survival study group. Pulsatile but
not steady component of blood pressure
predicts cardiovascular events in coronary
patients. Hypertension 2008;51:848-55
25. Mitchell GF, Hwang SJ, Vasan RS, et al.
Arterial stiffness and cardiovascular
events: the Framingham Heart Study.
Circulation 2010;121:505-11
26. Chronic Kidney Disease Prognosis
Consortium, Matsushita K,
van der Velde M, et al. Association of
estimated glomerular filtration rate and
albuminuria with all-cause and
cardiovascular mortality in general
population cohorts: a collaborative
meta-analysis. Lancet 2010;375:2073-81
27. Levey AS, Stevens LA, Schmid CH,
et al. A new equation to estimate
glomerular filtration rate.
Ann Intern Med 2009;150:604-12. A new, more precise algorithm
for EGFR.
28. Matsushita K, Selvin E, Bash LD, et al.
Risk implications of the new CKD
Epidemiology Collaboration (CKD-EPI)
equation compared with the MDRD
Study equation for estimated GFR: the
Atherosclerosis Risk in Communities
(ARIC) Study. Am J Kidney Dis
2010;55:648-59
29. Kahn R, Buse J, Ferrannini E, et al.
The metabolic syndrome: time for a
critical appraisal: joint statement from
the American Diabetes Association and
the European Association for the Study
of Diabetes. Diabetes Care
2005;28:2289-304
30. Sundstrom J, Vallhagen E, Riserus U,
et al. Risk associated with the metabolic
syndrome versus the sum of its individual
components. Diabetes Care
2006;29:1673-4
31. Mente A, Yusuf S, Islam S, et al.
Metabolic syndrome and risk of acute
myocardial infarction. A case-control
study of 26 903 subjects from
52 countries. J Am Coll Cardiol
2010;55:2390-8
32. Libby P, Ridker PM, Hansson GK.
Leducq Transatlantic Network on
atherothrombosis. Inflammation in
atherosclerosis: from pathophysiology
to practice. J Am Coll Cardiol
2009;54:2129-38
33. Genser B, Grammer TB, Stojakovic T,
et al. Effect of HMG CoA reductase
inhibitors on low-density lipoprotein
cholesterol and C-reactive protein:
systematic review and meta-analysis. Int J
Clin Pharmacol Ther 2008;46:497-510
34. Okin PM, Devereux RB, Jern S, et al.
Regression of electrocardiographic left
ventricular hypertrophy during
antihypertensive treatment and the
prediction of major cardiovascular events.
JAMA 2004;292:2343-9
35. Ibsen H, Olsen MH, Wachtell K, et al.
Reduction in albuminuria translates to
reduction in cardiovascular events in
hypertensive patients with left ventricular
hypertrophy and diabetes. J Nephrol
2008;21:566-9
36. de Galan BE, Perkovic V, Ninomiya T,
et al. Lowering blood pressure reduces
renal events in type 2 diabetes. J Am
Soc Nephrol 2009;20:883-92
37. Verdecchia P, Angeli F, Borgioni C,
et al. Changes in cardiovascular risk by
reduction of left ventricular mass in
hypertension: a meta-analysis.
Am J Hypertens 2003;16(11 Pt 1):895-9
38. Kearney-Schwartz A, Rossignol P,
Bracard S, et al. Vascular structure and
function is correlated to cognitive
performance and white matter
hyperintensities in older hypertensive
patients with subjective memory
complaints. Stroke 2009;40:1229-36
39. O’Donnell MJ, Xavier D, Liu L, et al.
Risk factors for ischemic and
intracerebral haemorrhagic stroke in
22 countries (the INTERSTROKE
study): a case-control study. Lancet
2010;DOI:10.1016/S0140-6736(10)
60834-3.. Similar to myocardial infarction,
stroke risk can be ascribed to
well-known and easily assessed
risk factors.
40. Schrier RW, Estacio RO, Esler A, et al.
Effects of aggressive blood pressure
control in normotensive type 2 diabetic
patients on albuminuria, retinopathy and
strokes. Kidney Int 2002;61:1086-97
41. Pepine CJ, Handberg EM,
Cooper-DeHoff RM, et al. A calcium
antagonist vs a non-calcium antagonist
hypertension treatment strategy for
patients with coronary artery disease.
The International Verapamil-Trandolapril
Study (INVEST): a randomized
controlled
trial. JAMA 2003;290:2805-16
42. Yusuf S, Sleight P, Pogue J,
et al. Effects of an
angiotensin-converting-enzyme
inhibitor, ramipril, on cardiovascular
events in high-risk patients. The Heart
Outcomes Prevention Evaluation Study
Investigators. N Engl J Med
2000;342:145-53
43. PROGRESS Collaborative Group.
Randomised trial of a perindopril-based
blood-pressure-lowering regimen among
6,105 individuals with previous stroke
or transient ischaemic attack. Lancet
2001;358:1033-41
44. Julius S, Nesbitt SD, Egan BM, et al.
Feasibility of treating prehypertension
with an angiotensin-receptor blocker.
N Engl J Med 2006;354:1685-97
45. Luders S, Schrader J, Berger J, et al.
The PHARAO study: prevention of
hypertension with the
angiotensin-converting enzyme inhibitor
ramipril in patients with high-normal
blood pressure: a prospective,
randomized, controlled prevention trial
of the German Hypertension League.
J Hypertens 2008;26:1487-96
46. van den Bogaard B, Baumann M,
van Weert HC, et al. Study on the
temporary treatment of high normal
blood pressure for the prevention of
hypertension and hypertensive organ
damage: the TIResiAS-study.
Ned Tijdschr Geneeskd
2007;151:1800-2
47. Howard BV, Roman MJ, Devereux RB,
et al. Effect of lower targets for blood
pressure and LDL cholesterol on
atherosclerosis in diabetes: the SANDS
randomized trial. JAMA
2008;299:1678-89
48. Mancia G, Messerli F, Bakris G, et al.
Blood pressure control and improved
cardiovascular outcomes in the
Hypertension 2010: what was new for the cardiologist?
2594 Expert Opin. Pharmacother. (2010) 11(16)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

International Verapamil SR-Trandolapril
Study. Hypertension 2007;50:299-305
49. Messerli FH, Mancia G, Conti CR, et al.
Dogma disputed: can aggressively
lowering blood pressure in hypertensive
patients with coronary artery disease be
dangerous? Ann Intern Med
2006;144:884-93
50. Mancia G, Messerli F, Bakris G, et al.
Blood pressure control and improved
cardiovascular outcomes in the
International Verapamil SR-Trandolapril
Study. Hypertension 2007;50:299-305
51. Sleight P, Redon J, Verdecchia P, et al.
Prognostic value of blood pressure in
patients with high vascular risk in the
ongoing telmisartan alone and in
combination with Ramipril Global
Endpoint Trial study. J Hypertens
2009;27:1360-9
52. Redon J, Sleight P, Mancia G, et al.
Safety and efficacy of aggressive blood
pressure lowering among patients with
diabetes: subgroup analyses from the
ONTARGET trial. J Hypertens
2009;27(Suppl 4):S16
53. Zanchetti A, Mancia G, Black HR,
et al. Facts and fallacies of blood
pressure control in recent trials:
implications in the management of
patients with hypertension.
J Hypertens
2009;27:946-7
54. Zanchetti A, Grassi G, Mancia G.
When should antihypertensive drug
treatment be initiated and to what
levels should systolic blood pressure be
lowered? A critical reappraisal.
J Hypertens 2009;27:923-34.. Extensive discussion of trials data to
document lack of scientific evidence
for recommended thresholds and goal
values for blood pressure.
55. K/DOQI Clinical Practice Guidelines on
Hypertension and Antihypertensive
Agents in Chronic Kidney Disease. Am J
Kidney Dis 2004;43:(5 Suppl 1):S1-290
56. Bielecka-Dabrowa A, Aronow WS,
Rysz J, Banach M. Current place of
beta-blockers in the treatment of
hypertension. Curr Vasc Pharmacol
2010. [Epub ahead of print]
57. Poole-Wilson PA, Swedberg K,
Cleland JG, et al. Carvedilol Or
Metoprolol European Trial Investigators.
Comparison of carvedilol and metoprolol
on clinical outcomes in patients with
chronic heart failure in the Carvedilol Or
Metoprolol European Trial (COMET):
randomised controlled trial. Lancet
2003;362:7-13
58. Bakris GL, Fonseca V, Katholi RE,
et al. Metabolic effects of carvedilol vs
metoprolol in patients with
type 2 diabetes mellitus and
hypertension: a randomized controlled
trial. JAMA 2004;292:2227-36
59. Munzel T, Gori T. Nebivolol: the
somewhat-different beta-adrenergic
receptor blocker. J Am Coll Cardiol
2009;54:1491-9
60. van Veldhuisen DJ, Cohen-Solal A,
Bohm M, et al. Beta-blockade with
nebivolol in elderly heart failure patients
with impaired and preserved left
ventricular ejection fraction: data from
SENIORS (Study of Effects of Nebivolol
Intervention on Outcomes and
Rehospitalization in Seniors With Heart
Failure). J Am Coll Cardiol
2009;53:2150-8
61. Cleland JG. Beta-blockers for heart
failure: why, which, when, and where.
Med Clin North Am 2003;87:339-71
62. Chobanian AV, Bakris GL, Black HR,
et al. The seventh report of the joint
national committee on prevention,
detection, evaluation, and treatment of
high blood pressure: the JNC 7 report.
JAMA 2003;289:2560-72.. The most popular US guidelines,
endorsed by the National Institutes
of Health.
63. Kaplan NM. The choice of thiazide
diuretics: why chlorthalidone may replace
hydrochlorothiazide. Hypertension
2009;54:951-3. This review by a hypertension expert
points out that most clinical data
speaks for thiazide-like diuretics and
not hydrochlorothiazide.
64. Bakris G, Molitch M, Zhou Q, et al.
Reversal of diuretic-associated impaired
glucose tolerance and new-onset diabetes:
results of the STAR-LET study.
J Cardiometab Syndr 2008;3:18-25
65. Yusuf S, Diener HC, Sacco RL, et al.
Telmisartan to prevent recurrent stroke
and cardiovascular events. N Engl J Med
2008;359:1225-37
66. Strauss MH, Hall AS. Angiotensin
receptor blockers may increase risk of
myocardial infarction: unraveling the
ARB-MI paradox. Circulation
2006;114:838-54
67. Fournier A, Messerli FH, Achard JM,
Fernandez L. Cerebroprotection mediated
by angiotensin II: a hypothesis supported
by recent randomized clinical trials. J Am
Coll Cardiol 2004;43:1343-7
68. Janke J, Schupp M, Engeli S, et al.
Angiotensin type 1 receptor antagonists
induce human in-vitro adipogenesis
through peroxisome proliferator-activated
receptor-gamma activation. J Hypertens
2006;24:1809-16
69. Hanley AJ, Zinman B, Sheridan P,
et al. Effect of Rosiglitazone and
Ramipril on {beta}-cell function in
people with impaired glucose tolerance
or impaired fasting glucose: the
DREAM trial. Diabetes Care
2010;33:608-13
70. Solomon SD, Wang D, Finn P, et al.
Effect of candesartan on cause-specific
mortality in heart failure patients: the
Candesartan in Heart failure Assessment
of Reduction in Mortality and
morbidity (CHARM) program.
Circulation 2004;110:2180-3
71. Sipahi I, Debanne SM, Rowland DY,
et al. Angiotensin-receptor blockade
and risk of cancer: meta-analysis
of randomised controlled trials.
Lancet Oncol
2010;DOI:10.1016/S1470-2045(10)
70106-6
72. Julius S, Kjeldsen SE, Weber MA.
Angiotensin-receptor blockade and
the risk of cancer. Omission of VALUE
trial data invalidates conclusions
[letter to the editor].
Not yet published
73. Bakris G, Molitch M, Hewkin A,
et al. Differences in glucose tolerance
between fixed-dose antihypertensive
drug combinations in people with
metabolic syndrome. Diabetes Care
2006;29:2592-7
74. Dahlof B, Sever PS, Poulter NR,
et al. Prevention of cardiovascular
events with an antihypertensive
regimen of amlodipine adding
perindopril as required versus
atenolol adding bendroflumethiazide
as required, in the Anglo-Scandinavian
Cardiac Outcomes Trial-Blood Pressure
Lowering Arm (ASCOT-BPLA):
a multicentre randomized controlled
trial. Lancet 2005;366:895-906
75. Bertrand ME, Ferrari R, Remme WJ,
et al. Clinical synergy of perindopril
and calcium-channel blocker in the
Gaciong & Symonides
Expert Opin. Pharmacother. (2010) 11(16) 2595
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

prevention of cardiac events and
mortality in patients with coronary
artery disease. Post hoc analysis of the
EUROPA study. Am Heart J
2010;159:795-802
76. Bakris GL, Sarafidis PA, Weir MR,
et al. Renal outcomes with different
fixed-dose combination therapies in
patients with hypertension at high risk
for cardiovascular events
(ACCOMPLISH): a prespecified
secondary analysis of a randomised
controlled trial. Lancet
2010;375:1173-81
77. Retraction -- Combination treatment
of angiotensin-II receptor blocker and
angiotensin-converting-enzyme inhibitor
in non-diabetic renal disease
(COOPERATE): a randomised
controlled trial. Lancet 2009;374:1226
78. Liu L, Zhang Y, Liu G, et al. The
Felodipine Event Reduction (FEVER)
Study: a randomized long-term
placebo-controlled trial in Chinese
hypertensive patients. J Hypertens
2005;23:2157-72
79. Zanchetti A, Bond MG, Hennig M,
et al. Calcium antagonist lacidipine
slows down progression of asymptomatic
carotid atherosclerosis: principal results
of the European Lacidipine Study on
Atherosclerosis (ELSA) -- a randomized,
double-blind, long-term trial. Circulation
2002;106:2422-7
80. Julius S, Kjeldsen SE, Weber M, et al.
Outcomes in hypertensive patients at
high cardiovascular risk treated with
regimens based on valsartan or
amlodipine: the VALUE randomised
trial. Lancet 2004;363:2022-31
81. Boger-Megiddo I, Heckbert SR,
Weiss NS, et al. Myocardial infarction
and stroke associated with diuretic
based two drug antihypertensive
regimens: population based case-control
study. BMJ 2010;340:c103
82. Bangalore S, Kamalakkannan G,
Parkar S, et al. Fixed-dose combinations
improve medication compliance:
a meta-analysis. Am J Med
2007;120:713-19
83. Feldman RD, Zou GY,
Vandervoort MK, et al. A simplified
approach to the treatment of
uncomplicated hypertension: a cluster
randomized, controlled trial.
Hypertension 2009;53:646-53
84. Gradman AH, Acevedo C. Evolving
strategies for the use of combination
therapy in hypertension.
Curr Hypertens Rep 2002;4:343-9
85. Wald NJ, Law MR. A strategy to reduce
cardiovascular disease by more than 80%.
BMJ 2003;326:1419-24
86. The Indian Polycap Study (TIPS).
Effects of a polypill (Polycap) on risk
factors in middle-aged individuals
without cardiovascular disease (TIPS):
a phase II, double-blind, randomised
trial. Lancet 2009;373:1341-51
87. Somes GW, Pahor M, Shorr RI, et al.
The role of diastolic blood pressure
when treating isolated systolic
hypertension. Arch Intern Med
1999;159:2004-9
88. Tveit A, Grundvold I, Olufsen M, et al.
Candesartan in the prevention of
relapsing atrial fibrillation. Int J Cardiol
2007;120:85-91
89. GISSI-AF Investigators. Valsartan for
prevention of recurrent atrial fibrillation.
N Engl J Med 2009;360:1606-17
90. Zeller T. Renal artery stenosis:
epidemiology, clinical manifestation,
and percutaneous endovascular therapy.
J Interv Cardiol 2005;18:497-506
91. Textor SC. Current approaches to
renovascular hypertension. Med Clin
North Am 2009;93:717-32
92. Ives NJ, Wheatley K, Stowe RL, et al.
Continuing uncertainty about the value
of percutaneous revascularization in
atherosclerotic renovascular disease:
a meta-analysis of randomized trials.
Nephrol Dial Transplant
2003;18:298-304
93. Plouin PF, Chatellier G, Darne B,
Raynaud A. Blood pressure outcome
of angioplasty in atherosclerotic renal
artery stenosis: a randomized trial. Essai
Multicentrique Medicaments vs
Angioplastie (EMMA) Study Group.
Hypertension 1998;31:823-9
94. van Jaarsveld BC, Krijnen P,
Pieterman H, et al. The effect of balloon
angioplasty on hypertension in
atherosclerotic renal-artery stenosis.
Dutch Renal Artery Stenosis Intervention
Cooperative Study Group. N Engl
J Med 2000;342:1007-14
95. Bax L, Woittiez AJ, Kouwenberg HJ,
et al. Stent placement in patients with
atherosclerotic renal artery stenosis and
impaired renal function: a randomized
trial. Ann Intern Med
2009;150:840-8:W150-1
96. Symonides B, Gaciong Z. The effect
of percutaneous revascularization of
atherosclerotic renal artery stenosis
on blood pressure. A meta-analysis of
randomized trials. J Hypertens
2010;28(Suppl A):E510
97. Ridker PM, Danielson E, Fonseca FA,
et al. Rosuvastatin to prevent vascular
events in men and women with
elevated C-reactive protein. N Eng
J Med 2008;359:2195-207
98. de Lorgeril M, Salen P, Abramson J,
et al. Cholesterol lowering, cardiovascular
diseases, and the rosuvastatin-JUPITER
controversy: a critical reappraisal.
Arch Intern Med 2010;170:1032-6
99. Ray KK, Seshasai SR, Erqou S, et al.
Statins and all-cause mortality in
high-risk primary prevention:
a meta-analysis of 11 randomized
controlled trials involving
65,229 participants. Arch Intern Med
2010;170:s1024-31
100. ACCORD Study Group, Ginsberg HN,
Elam MB, et al. Effects of combination
lipid therapy in type 2 diabetes mellitus.
N Engl J Med 2010;362:1563-74
101. Banach M, Mikhailidis DP, Kjeldsen SE,
Rysz J. Time for new indications for
statins? Med Sci Monit 2009;15:MS1-5
102. Antithrombotic Trialists’ (ATT)
Collaboration, Baigent C, Blackwell L,
et al. Aspirin in the primary and
secondary prevention of vascular disease:
collaborative meta-analysis of individual
participant data from randomised trials.
Lancet 2009;373:1849-60
103. Belch J, MacCuish A, Campbell I, et al.
The prevention of progression of arterial
disease and diabetes (POPADAD) trial:
factorial randomised placebo controlled
trial of aspirin and antioxidants in
patients with diabetes and asymptomatic
peripheral arterial disease. BMJ
2008;337:a1840
104. Pignone M, Alberts MJ, Colwell JA,
et al. Aspirin for primary prevention
of cardiovascular events in people with
diabetes. A position statement of the
American Diabetes Association, a
scientific statement of American Heart
Association, and an expert consensus
document of the American College of
Cardiology Foundation. Circulation
2010;121:2878-86
Hypertension 2010: what was new for the cardiologist?
2596 Expert Opin. Pharmacother. (2010) 11(16)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.

105. Petursson H, Getz L, Sigurdsson JA,
Hetlevik I. Current European guidelines
for management of arterial hypertension:
are they adequate for use in primary
care? Modelling study based on the
Norwegian HUNT 2 population.
BMC Fam Pract 2009;10:70
106. Falaschetti E, Chaudhury M, Mindell J,
Poulter N. Continued improvement in
hypertension management in England:
results from the Health Survey for
England 2006. Hypertension
2009;53:480-6
AffiliationZbigniew Gaciong† MD PhD &
Bartosz Symonides MD PhD†Author for correspondence
The Medical University of Warsaw,
Department of Internal Medicine,
Hypertension and Vascular Diseases,
1a Banacha Street,
02-097 Warsaw, Poland
Tel: +48 22 599 2828; Fax: +48 22 599 2828;
E-mail: [email protected]
Gaciong & Symonides
Expert Opin. Pharmacother. (2010) 11(16) 2597
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 0
8/25
/14
For
pers
onal
use
onl
y.