Embed Size (px)
Citation preview
http://lup.sagepub.com/Lupus
http://lup.sagepub.com/content/13/1/60The online version of this article can be found at:
DOI: 10.1191/0961203304lu465cr
2004 13: 60LupusE Elinav, M Korem, Y Ofran, A Migdal, V Doviner, N Hiler, S Aamar and M Bursztyn
Hyperplastic gastropathy as a presenting manifestation of systemic lupus erythematosus
Published by:
http://www.sagepublications.com
can be found at:LupusAdditional services and information for
http://lup.sagepub.com/cgi/alertsEmail Alerts:
http://lup.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://lup.sagepub.com/content/13/1/60.refs.htmlCitations:
What is This?
- Jan 1, 2004Version of Record >>
by guest on August 3, 2014lup.sagepub.comDownloaded from by guest on August 3, 2014lup.sagepub.comDownloaded from
CASE REPORT
Hyperplastic gastropathy as a presenting manifestation ofsystemic lupus erythematosus
E Elinav1, M Korem1, Y Ofran1, A Migdal2, V Doviner3, N Hiler4, S Aamar1 and M Bursztyn1¤1Department of Medicine, Hadassah University Hospital, Mount Scopus Campus, Jerusalem, Israel; 2Department of Gastroenterology,
Hadassah University Hospital, Ein-Kerem Campus, Jerusalem, Israel; 3Department of Pathology, Hadassah University Hospital,Mount Scopus Campus, Jerusalem, Israel; and 4Department of Radiology, Hadassah University Hospital, Mount Scopus Campus, Jerusalem, Israel
A patient is described who had severe hyperplastic gastropathy as the presenting manifestation ofsystemic lupus erythematosus (SLE). Aggressive immunosuppressive therapy with systemiccorticosteroids and immunoglobulins resulted in complete remission of lupus, and a prompt clinicaland radiological regression of hyperplastic gastropathy. Hyperplastic gastropathy is an uncommongastric illness, which is usually idiopathic but rarely is associated with Helicobacter pylori infection,cytomegalovirusinfection or lymphocytic gastritis. Three previous case reports have noted a responseof idiopathic hyperplastic gastropathy to systemic corticosteroid treatment, yet none of the presentedpatients had a systemic in� ammatory disease.The presented case is the � rst in the medical literature inwhich hyperplastic gastropathy is directly linked to the development of clinical and laboratorymanifestations of SLE. We suggest that hyperplastic gastropathy be added to the list of raregastrointestinalmanifestationsof SLE, and that autoimmune disease be considereda possible cause ofhyperplastic gastropathy. As such, any patient with symptomatic idiopathic hyperplastic gastropathyaccompanied by other evidence of systemic in� ammation should be considered for SLE evaluationand immunosuppressive treatment. Lupus (2004) 13, 60–63.
Key words: antiphospholipid syndrome; hyperplastic gastropathy; Menetrier; systemic lupuserythematosous
Case report
A 25-year old Caucasian female was admitted for anevaluation of two weeks of nausea, low-grade fever anddiffuse epigastric pain described as intense (9 on a 1 to10 visual scale), nonradiating, and unaffected by eatingor changing of posture. The patient noted no urinarysymptoms, jaundice, vaginal discharge or shortness ofbreath. Empiric treatment with antacids and oralranitidine was ineffective.
Past medical history was signi� cant for the anti-phospholipid syndrome, diagnosed a year earlier. It � rstmanifested as a second trimester abortion, high titre ofantiphospholipid antibodies and mild thrombocyto-penia. Five months later she experienced pre-eclampsiaand the HELLP syndrome during the 21st week of hersecond pregnancy, which necessitated its urgent
interruption. At that time she showed no evidence ofany of the currently recognized hypercoagulabledisorders other than the high titres of antiphospholipidantibodies and did not ful� ll any of the clinical orlaboratory criteria for systemic lupus erythematosus(SLE) or any other autoimmune disorders. She wasstarted on treatment with enoxaparin, with noadditional symptoms noted until her current admission.She did not use any other prescribed, over the counter ornatural medications, or abuse illicit drugs or alcohol.
On admission the patient appeared ill, with normalblood pressure, temperature and arterial oxygensaturation, but with a tachycardia of 100 beats perminute. Physical examination was notable for pallor, amildly distended abdomen, marked tenderness at theepigastric region and a palpable spleen; the rest of theexamination was unremarkable.
The patient’s laboratory results at admission aresummarized in Table 1. Of note is the pancytopeniawith negative haemagglutinin test and morphologicallynormal blood smears, the prolonged partial prothrom-bin time, which normalized after the addition of excessphospholipid, and the severe hypoalbuminemia. Chest
¤Correspondence: Dr Michael Bursztyn, Associate Professor of Medicine,Hypertension Unit, Department of Medicine, Hadassah UniversityHospital, Mount Scopus, PO Box 24035, Jerusalem 91240, Israel.E-mail: [email protected] 14 April 2003; accepted 19 June 2003
Lup us (2004) 13, 60– 63
www.lupus-journal.com
# Arnold2004 10.1191/0961203304lu465cr
by guest on August 3, 2014lup.sagepub.comDownloaded from

X-ray, electrocardiography and echocardiography wereunremarkable. Microscopic examination of the urinarysediment was normal, and there was no proteinuria.
Blood, urine, sputum and faecal cultures for bacteria,mycobacterium, fungi and parasites were repeatedlysterile. Faecal ELISA assays for Clostridium dif� ciletoxin were negative. Serology was negative forinfection with Ebstein-Bar virus, cytomegalo virus,syphilis, brucella, rickettsia, the human immunode� -ciency virus and hepatitis A, B and C viruses.
Serum ferritin, iron, B12 and folic acid were normal.Bone marrow biopsy showed a normal tricellular lineage,with no evidence of chromosomal translocations ormonoclonal immunoglobulin gene rearrangement.Transvaginal ultrasonography was unremarkable.
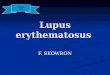
Abdominal ultrasonography was normal. AbdominalCT angiography demonstrated a normal-looking, non-distended small and large bowel and patent mesentericvessels with no evidence of abdominal lymphadeno-pathy, but revealed a mildly enlarged spleen and mark-edly thickened gastric folds, particularly along the lessercurvature and antrum of the stomach (Figure 1).
Autoimmune serology was positive for anti-nuclearantibodies (4/4), antiphospholipid antibodies, anti-b2-microglobulin and anti-dsDNA antibodies (1:84).Cytoplasmatic and perinuclear anti-neutrophiliccytoplasmatic antibodies, cryoglobulins and rheuma-toid factor were negative. No paraprotein was found inthe patient’s serum or urine.
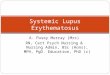
Upper gastrointestinal barium swallow and passageseries demonstrated severely hypertrophic gastric foldsat the antrum and distal portion of the body of thestomach, highly suggestive of hyperplastic gastropathy(Figure 2). The gastric fundus was intact.
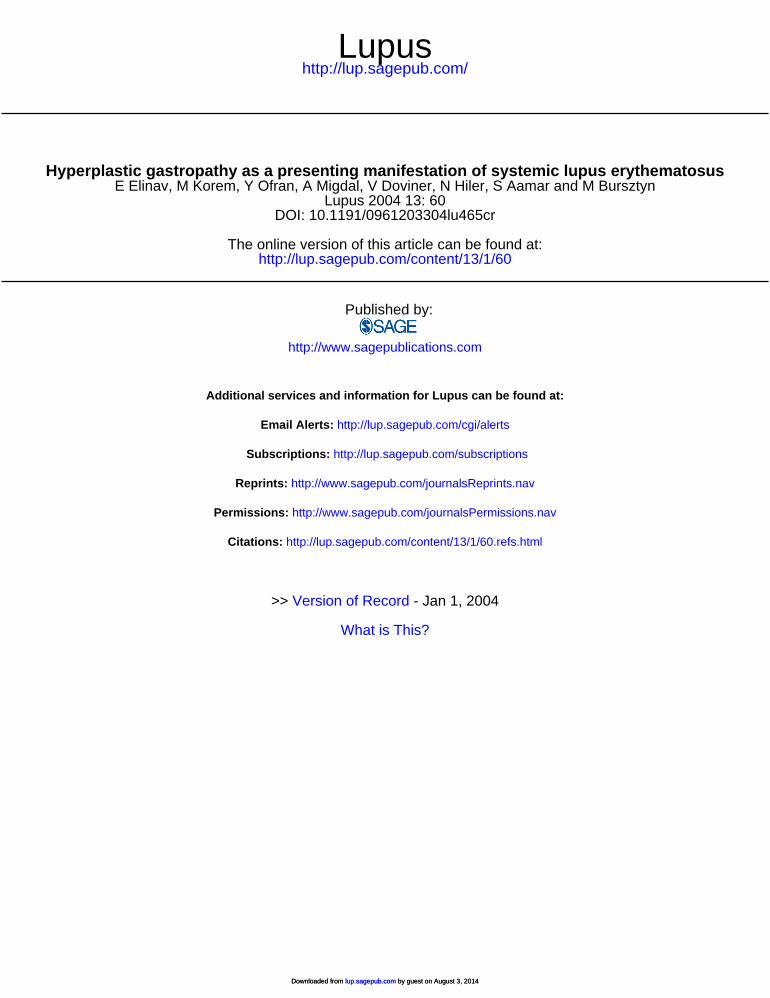
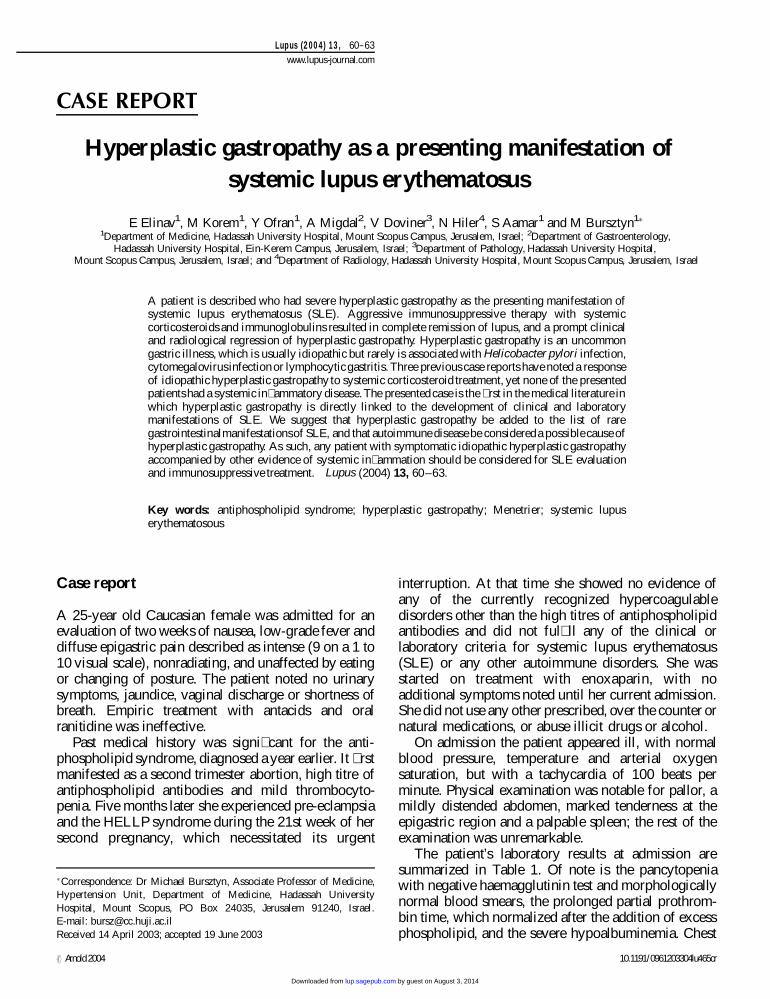
Endoscopy revealed a diffuse in� ltrative mucosalprocess, extending throughout the gastric body andantrum, accompanied by markedly thickened anddistorted, but not in� amed, gastric rugae. No evidenceof gastritis or gastric ulcer was noted. Five gastricbiopsies, including a snare biopsy, revealed extensivegastric pit hyperplasia and cystic dilatation, withfoveolar cell hyperplasia, highly compatible withhyperplastic gastropathy (Figure 3). Very few Helico-bacter pylori bacteria were noted, and there was nopathological evidence of gastritis, vasculitis or mucosalischaemia. Duodenal biopsy was normal.
During the patient’s hospitalization she sufferedagonizing epigastric pain, necessitating the adminis-tration of escalating doses of narcotics (up to 150mgtransdermal fentanyl daily plus occasional extra
Figure 2 A barium meal showing coarse and thickened gastricfolds along the antrum and lesser curvature (arrows).
Table 1 Laboratory results
VariableDay ofadmission
Two monthsafter discharge
ESR (mm/hr) 80 30White cells (mm6) 2900 7600Differential count (%)
Neutrophils 60 73Lymphocytes 32 17Monocytes 6 7Eosinophils 1 0
Hgb (gram%) 9 9.4Platelets (mm6) 60000 288000INR 1.4 2.9 (warfarin)PTT 199 70Urea (mmol/L) 1.8 3.6Creatinine (mmol/L) 86 71Protein (g/L) 64 72
Albumin 23 40Globulin 41 32
ESR, erythrocyte sedimentation rate;INR, international normalized ratio;PTT, partial prothrombin time.
Figure 1 Computed tomography of the upper abdomen, with IVcontrast injection, demonstrating markedly thickened antral wall(arrow). Note also enlargement of the spleen.
H yperpl astic gastropathy and SLEE Elinav et al.
61
Lupus
by guest on August 3, 2014lup.sagepub.comDownloaded from
intravenous doses of fentanyl). Triple therapy forH. pylori with clarythromycin, metronidazole andomeprazole resulted in no improvement.
On the second week of hospitalization the patientdeveloped a bilateral malar rash, an intense right-sidedpleuritic chest pain, accompanied with a small amountof right pleural effusion. Electrocardiography, echocar-diography, chest radiography and spiral CT scanshowed no evidence of a pulmonary in� ltrate,pulmonary thromboembolism or pericarditis. Arepeated 24-hour urine collection and sedimentexamination showed proteinuria of 500mg per dayand numerous red and white cell casts.
At that point it was clear that the patient hadnew onset SLE consisting of pleuritis, nephritis,pancytopenia and positive serology and hyperplasticgastropathy, possibly related to her lupus exacerbation.
Treatment with intravenous hydrocortisone (600mgdaily) and immunoglobulins (30g daily for � ve days)was begun. The nausea and epigastric pain subsidedwithin two days. Within a week she reacheddeffervescence and noted a complete resolution of herchest pain. She was rapidly weaned off the high-
dose narcotic treatment and oral corticosteroids werestarted (prednisone, 60mg daily). Her urinary sedimentand blood counts normalized within a few more days,while her albumin levels normalized after two months(Table 1).
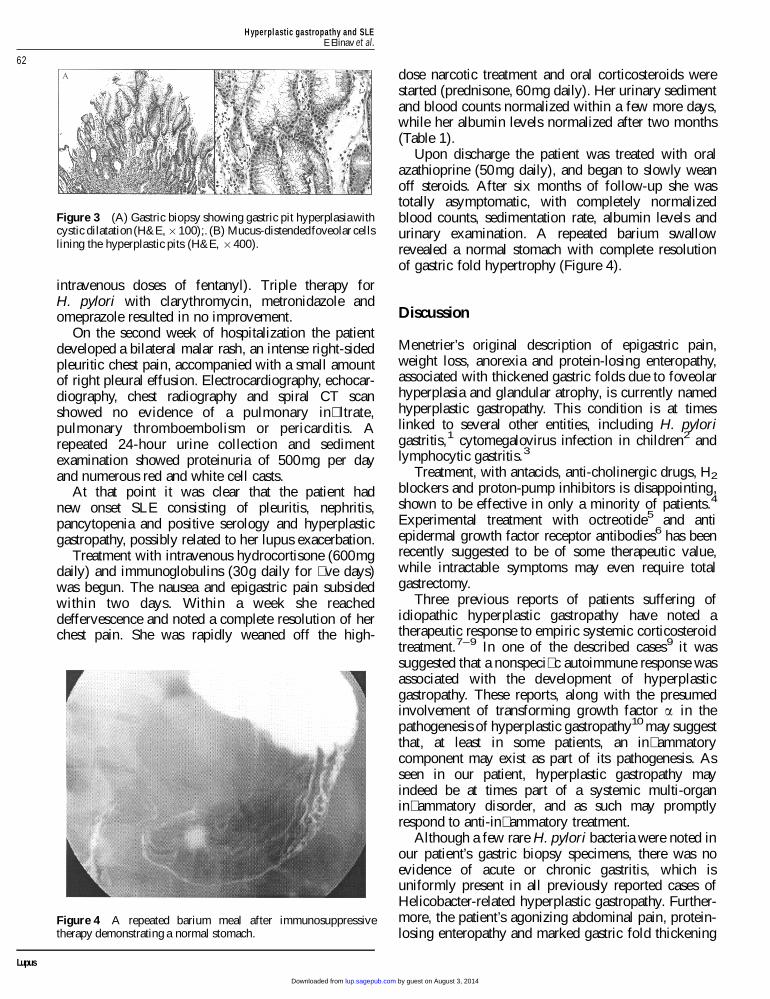
Upon discharge the patient was treated with oralazathioprine (50mg daily), and began to slowly weanoff steroids. After six months of follow-up she wastotally asymptomatic, with completely normalizedblood counts, sedimentation rate, albumin levels andurinary examination. A repeated barium swallowrevealed a normal stomach with complete resolutionof gastric fold hypertrophy (Figure 4).
Discussion
Menetrier’s original description of epigastric pain,weight loss, anorexia and protein-losing enteropathy,associated with thickened gastric folds due to foveolarhyperplasia and glandular atrophy, is currently namedhyperplastic gastropathy. This condition is at timeslinked to several other entities, including H. pylorigastritis,1 cytomegalovirus infection in children2 andlymphocytic gastritis.3
Treatment, with antacids, anti-cholinergic drugs, H2
blockers and proton-pump inhibitors is disappointing,shown to be effective in only a minority of patients.4
Experimental treatment with octreotide5 and antiepidermal growth factor receptor antibodies6 has beenrecently suggested to be of some therapeutic value,while intractable symptoms may even require totalgastrectomy.
Three previous reports of patients suffering ofidiopathic hyperplastic gastropathy have noted atherapeutic response to empiric systemic corticosteroidtreatment.7–9 In one of the described cases9 it wassuggested that a nonspeci� c autoimmune response wasassociated with the development of hyperplasticgastropathy. These reports, along with the presumedinvolvement of transforming growth factor a in thepathogenesis of hyperplastic gastropathy10 may suggestthat, at least in some patients, an in� ammatorycomponent may exist as part of its pathogenesis. Asseen in our patient, hyperplastic gastropathy mayindeed be at times part of a systemic multi-organin� ammatory disorder, and as such may promptlyrespond to anti-in� ammatory treatment.
Although a few rare H. pylori bacteria were noted inour patient’s gastric biopsy specimens, there was noevidence of acute or chronic gastritis, which isuniformly present in all previously reported cases ofHelicobacter-related hyperplastic gastropathy. Further-more, the patient’s agonizing abdominal pain, protein-losing enteropathy and marked gastric fold thickening
Figure 4 A repeated barium meal after immunosuppressivetherapy demonstrating a normal stomach.
Figure 3 (A) Gastric biopsy showing gastric pit hyperplasiawithcystic dilatation (H&E, £100);. (B) Mucus-distendedfoveolar cellslining the hyperplastic pits (H&E, £400).
H yperpl astic gastropathy and SLEE Elinav et al.
62
Lupus
by guest on August 3, 2014lup.sagepub.comDownloaded from

did not improve after H. pylori eradication, whiledramatically improving days after the institution ofhigh-dose steroid therapy directed at SLE.
In conclusion, we suggest that hyperplastic gastro-pathy be added to the list of rare gastrointestinalmanifestations of SLE, and that autoimmune disease beconsidered as a possible cause of hyperplasticgastropathy. As such, any patient with symptomaticidiopathic hyperplastic gastropathy accompanied byother evidence of systemic in� ammation should beconsidered for SLE evaluation. Treatment of hyper-plastic gastropathy in such a patient, as in othersystemic manifestations of lupus, may includecorticosteroids or intravenous immunoglobulin.
References
1 Stolte M, Batz CH, Eidt S. Giant fold gastritis a special form ofHelicobacter-pylori associated gastritis. Z Gastroenterol 1993; 31: 289.
2 Sferra TJ, Pawel BR, Qualman SJ et al. Menetrier disease of childhood.Role of cytomegalovirus and transforming growth factor alpha. J Pediatr1996; 128: 213.
3 Perardi S, Todros L, Musso A, David E, Repici A, Rizzetto M.Lymphocytic gastritis and protein-losing gastropathy. Dig Liver Dis2000; 32(5): 422–425.
4 Berry EM, Ben-Dov Y, Freund U. Spontaneous remission of protein-losing gastropathy associated with Menetrier’s disease. A plea forconservative management. Arch Intern Med 1980; 140: 99.
5 Yeaton P, Frierson HF. Octreotide reduces enteral protein losses inMenetrier’s disease. Am J Gastroenterol 1993; 88: 95.
6 Burdick JS, Chung E, Tanner G et al. Treatment of Menetrier’s diseasewith a monoclonal antibody against the epidermal growth factorreceptor. N Engl J Med 2000; 343: 1697.
7 Molino M, Macchiarella MR, Novara V. Menetrier disease of the child:a case report. Radiol Med 2001; 102(3): 184–185.
8 Winney RJ, Gilnour HM, Matthews JD. Prednisolone in gianthypertrophic gastritis (Menetrier’s disease). Am J Dig Dis 1976; 21(4):337–339.
9 Aoki T, Noma N, Takajo I et al. Protein-losing gastropathy associatedwith autoimmune disease: successful treatment with prednisolone.J Gastroenterol 2002; 37(3): 204–209.
10 Dempsey PJ, Goldenring JR, Soroka CJ et al. Possible role oftransforming growth factor alpha in the pathogenesis of Menetrier’sdisease: supportive evidence from humans and transgenic mice.Gastroenterology 1992; 103: 1950.
H yperpl astic gastropathy and SLEE Elinav et al.
63
Lupus
by guest on August 3, 2014lup.sagepub.comDownloaded from