Embed Size (px)
Citation preview

Hypernatremia is often an unanticipated complication in critically ill cats.It can be life-threatening in intensive-care patients with inadequate waterintake, renal failure, head injury, respiratory disease, infection, hormoneimbalances, or osmotic diuresis from diabetes mellitus or drug therapy.Through rapid loss of intracellular water, hypernatremia acutely and pri-marily affects the central nervous system, resulting in lethargy, seizures,coma, or death.This article reviews the pathophysiology of hypernatremiain critically ill cats.
ABSTRACT:
Hypernatremia in Critically Ill Cats:Pathophysiology*
Kristen Temo, DVMElke Rudloff, DVM, DACVECCMarla Lichtenberger, DVM, DACVECCRebecca Kirby, DVM, DACVIM, DACVECC Animal Emergency CenterGlendale, Wisconsin
*A companion article onevaluation and treatment
appears on p. 434.
HYPERNATREMIA INCRITICALLY ILL CATS
An In-Depth Look:
Article #1
CE
ife-threatening hypernatremia can develop in patients affected by vastly dif-ferent pathophysiologic processes (see box on page 423). Excessive sodiumintake or loss of sodium-free water, the primary reasons for serum sodium ele-
vations, can result either from the pathology of the underlying disease or from ther-apy. The end results of acute hypernatremia are rapid transcellular fluid shifts andbrain dysfunction. These complications may cause neurologic changes ranging frommild depression in mentation to fatal intracranial hemorrhage and cellular death,depending on the rate and level of sodium increase and the presence of concurrentcardiovascular, renal, and neurologic disease. Therefore, profound alteration in acat’s mentation or level of consciousness warrants immediate evaluation of theserum electrolyte level to detect an elevated serum sodium concentration (values>155 mEq/L merit close monitoring, and clinical signs of hypernatremia are oftennoted when sodium levels become >160 mEq/L). Although the incidence of acutehypernatremia in cats is poorly described, we have observed the syndrome in criti-cally ill cats.
Email comments/questions to
fax 800-556-3288, or log on to
www.VetLearn.com
L
COMPENDIUM 422 June 2004

NORMAL SODIUM HOMEOSTASISFunction
Sodium, the most abundant electrolyte in extracellularfluid, plays a major role in determining the osmolaritya
of fluids within each fluid compartment (i.e., intravas-
cular, interstitial, intracellular) within the body. In addi-tion to sodium, glucose and blood urea nitrogen (BUN)contribute to osmolarity in the following way:
Osmolarity = 2(Sodium) + (Glucose ÷ 18) + (BUN ÷ 2.8)
Water moves passively across all compartment mem-branes in volumes controlled by the osmolarity of thefluid compartments.
Sodium passively moves across the capillary mem-brane, and its concentration rapidly equilibrates betweenthe interstitial and plasma fluid compartments. In con-trast, sodium must be activelytransported into and out of thecell. Transcellular sodium gradientis the normal physiologic propertythat controls water content withina cell (Figure 1).
Like sodium, glucose passesfreely across the intravascularmembrane but not the cell mem-brane. Its contribution to watershifts can become significant whenthe serum glucose concentrationrises above the renal threshold(approximate mean threshold:>200 mg/dl in dogs and >290
mg/dl in cats),1 such as in patients with diabetes melli-tus. BUN, however, is freely permeable across all mem-branes. It is an “ineffective” osmole because it freelypasses across the capillary and cell membranes andequilibrates. Normal cats reportedly maintain their
plasma sodium concentration and plasma osmolarity(pOsm) within narrow limits (sodium: 145 to 155mEq/L; pOsm: 308 to 335 mOsm/L).2
Water RegulationPlasma sodium concentration is actually a reflection of
plasma water content. When the plasma water contentincreases, the plasma sodium is diluted, and the milli-equivalents per liter value decreases. Alternatively, whenthe plasma water content decreases, the sodium concen-tration increases. Water is lost continuously throughevaporation from the respiratory tract and cellular metab-
June 2004 COMPENDIUM
Hypernatremia in Critically Ill Cats: Pathophysiology 423CE
aOsmolarity is the number of osmolesper liter of solution (e.g., plasma);osmolality is the number of osmolesper kilogram of solvent. Becauseosmoles in the body are dissolved inwater (which has a density of 1),osmolar concentrations can be ex-pressed as Osm/L of water, and eachosmole is equivalent to osmolarity.
When Regulatory Mechanisms Are Normal
Reduced water intakeInaccessibility to waterOropharyngeal diseaseNauseaAltered mentationInsensible water lossesHyperthermiaHyperventilationRespiratory disorders (e.g., upper
respiratory tract infection, pneumonia)FeverBurnsGastrointestinal diseaseOsmotic diuresisHyperglycemiaUremiaExcessive sodium intakeMannitol administrationHypertonic sodium fluid administrationSodium bicarbonate administrationSodium phosphate enemas
Causes of Hypernatremia
Acute hypernatremia can occur in critically ill cats that haveinadequate water intake, osmotic diuresis, head injury, infection,
respiratory disease, hormonal imbalances, or renal disease.
When Regulatory Mechanisms Are Abnormal
Central diabetes insipidus resulting from:Congenital pituitary malformationPituitary neoplasiaHead injuryMeningoencephalitis
Nephrogenic diabetes insipidus resultingfrom:
Congenital causePyelonephritisHypokalemiaHypercalcemiaCirculating Escherichia coli endotoxinsDrug therapy (e.g., lithium, colchicine,
gentamicin, amphotericin B,methoxyflurane, vinca alkaloids)

Antidiuretic HormoneAntidiuretic hormone (ADH) release is
stimulated by reduced cardiac output, nau-sea, and, most important, increased plasmaosmolality.3,4 ADH, the most potent regu-lator of body water content, is releasedwhen an osmotic gradient developsbetween the cerebral vessel and thesupraoptic and paraventricular nuclei in thehypothalamus (Figure 2). As little as a 2%increase in plasma osmolality above theosmotic threshold (280 mOsm/kg water inhumans) increases measurements of circu-lating ADH within minutes.5 ADH is anarteriole constrictor throughout the bodyand increases arterial pressure and cardiacoutput. This response is less important thanthe renal response to ADH, which issolute-free water reabsorption.
Thirst MechanismIncreased pOsm also results in increased
water intake via activation of the thirstcenter. Hyperosmolar fluid bathing thethirst center located near the supraopticand preoptic nuclei in the anteroventralregion of the third ventricle in the brain isa potent stimulator of thirst.3,6 Reducedbaroreceptor stretch caused by hypo-volemia and hypotension also results instimulating the thirst center. Finally, hypo-volemia-induced release of renal angio-tensin II directly stimulates the subfornicalorgan in the diencephalon, which stimu-lates neural areas associated with the thirstresponse.4,6,7
Increased water intake, coupled withADH-mediated water reabsorption,results in a diluted plasma sodium concen-tration and decreased osmolarity. A con-scious individual with unrestricted accessto water can maintain pOsm under mostconditions.
MECHANISMS OF HYPERNATREMIAStimulation of thirst and water reabsorption from the
renal collecting ducts should normally maintain sodiumand water balance within an acceptable range. Urinespecific gravity (USG) and urine osmolality (uOsm)
olism (called sensible water loss) and in normal productionof body fluids (e.g., urine, feces, mucus). Hormonal andrenal mechanisms maintain water and sodium balance byregulating renal water excretion and reabsorption,whereas thirst mechanisms influence water intake.
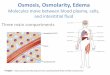
Figure 1. Effect of increased intravascular sodium concentration on thebrain. When sodium concentration increases in vessels, intravascular osmolarityincreases.Through the process of osmosis, water moves across the cell through theinterstitial space and into the vessel following the transcellular and transendothelialosmolar gradient.The result is increased intravascular volume and decreased interstitialand intracellular volume. Neurologic complications arise from rapid water loss in braincells and hemorrhage of intracerebral vessels. (Illustration by Barbara Harmon)
COMPENDIUM June 2004
Hypernatremia in Critically Ill Cats: Pathophysiology424 CE
Na+ H2ONucleus

COMPENDIUM June 2004
Hypernatremia in Critically Ill Cats: Pathophysiology426 CE
Figure 2. Normal ADH release and effect. Increases in pOsm result in an osmotic gradient in the brain, with shrinking of thesupraoptic and paraventricular nuclei in the hypothalamus.An action potential is initiated along the nerve cells of the supraoptico-hypophyseal tract to the posterior pituitary. Depolarization at the nerve endings results in release of secretory granules containingADH into the bloodstream. Circulating ADH binds to V2 receptors on the basolateral aspect of the collecting duct in the nephron.Through adenylate cyclase, aquaporin-2 channels open in the collecting tubules, permitting solute-free water reabsorption as sodiumis excreted in concentrated urine. Renal water reabsorption dilutes the plasma sodium, maintaining normal plasma concentration.(Illustration by Barbara Harmon)
Na+
H2O
Increase in pOsm
Shrinking of nucleiin hypothalamus
Release of ADH
Solute-free waterreabsorbed
Aquaporin-2 channels open
ADH binds toV2 receptors in collecting duct
Na+ excreted inconcentrated urine

reflect concentrated urine during dehydration and waterdeprivation. When normal thirst and ADH regulatorymechanisms fail to meet rapid changes in plasmasodium and water concentrations or the mechanismsbecome impaired because of disease, hypernatremia andtranscellular fluid shifts occur.
Normal Regulatory MechanismsSodium and water regulatory mechanisms may not be
adequate during water deprivation when there is ongo-ing water loss in excess of sodium or when sodiumintake exceeds water intake (see box on page 423). Catsmay become water deprived if they are denied access to
water; have an illness or problem causing immobility; orfail to drink as a result of oropharyngeal disease, nausea,or altered mentation. Hypodipsic hypernatremia due totransient hypopituitarism in a hydrocephalic cat has alsobeen reported.8
Administering isotonic sodium–containing fluids(e.g., 0.9% saline, lactated Ringer’s solution, Nor-mosol-R [Abbott Laboratories], Plasmalyte-A [Bax-ter]) for extracellular volume replacement should notresult in hypernatremia if normal sodium regulatorymechanisms are functioning.9 However, if a cat losesmore water than expected (because of tachypnea, diar-rhea, or osmotic diuresis) or fails to take in water,
COMPENDIUM June 2004
Hypernatremia in Critically Ill Cats: Pathophysiology428 CE
Figure 3. Causes of hypernatremia. Various types of injury to the central osmoreceptors, hypothalamus, supraopticohypophysealtract, or posterior pituitary (see box on page 423) can cause reduced ADH production/secretion and subsequent central diabetesinsipidus. Familial or acquired nephrogenic diabetes insipidus results in lack of renal ADH receptor responsiveness.The results are thesame: dilute urine, hypernatremia, and elevated pOsm when compensatory water intake is inadequate. (Illustration by Barbara Harmon)
H2O
ADH
Na+
Brain injury
Primary/secondarynephrogenic diabetes
ADH receptor responsiveness
Dilute urine
ADH
Þ
Þ

posterior pituitary and altered ADH synthesis and se-cretion can result in acute sodium imbalances18 (Figure3). Impaired water intake may also contribute to hyper-natremia in patients with these injuries. Recovery of theinjured hypothalamic–pituitary tract may take days toyears or may not occur at all.
Nephrogenic Diabetes InsipidusThe presence of primary (familial) or secondary
(acquired) nephrogenic diabetes insipidus is character-ized by lack of response to ADH by renal receptors. Pri-
June 2004 COMPENDIUM
Hypernatremia in Critically Ill Cats: Pathophysiology 429CE
Figure 4. Compensatory response of brain cells tohypernatremia. A high serum sodium concentration causeswater to leave brain cells, resulting in initial brain cell shrinkage.With time, the brain generates idiogenic osmoles and equilibratesthe intracellular and extracellular osmolarity, reestablishing theintracellular water concentration. (Illustration by Barbara Harmon)
plasma sodium concentration can increase despitenormal regulatory responses. Problems such as renaldisease, encephalitis, and head trauma can lead toabnormalities within the sodium–water regulatorymechanism.
Abnormal Regulatory MechanismsInadequate water reabsorption from the renal collect-
ing ducts results in loss of sodium-free water, significanthypernatremia, and elevated pOsm when compensatorywater intake is either impaired or prevented. Regulatorymechanism abnormalities leading to this life-threaten-ing complication include inadequate ADH productionor release from the neurohypophysis or posterior pitu-itary (central diabetes insipidus), failure of the renal col-lecting duct cell to recognize and respond to ADH(nephrogenic diabetes insipidus), or a combination ofboth (see box on page 423 and Figure 3). If this happensin a cat, clinical dehydration or hypotension can beexpected to occur along with urine dilution (i.e., USG<1.023 and uOsm <800 mOsm/kg water).1
Central Diabetes InsipidusIn dogs, hypernatremia has been associated with
meningoencephalitis,10 pituitary malformation, and headinjury.1 Although reports of hypernatremia in cats arerare,8,11,12 we have treated four cats that developed dete-riorating neurologic signs concurrent with hyperna-tremia 2 to 13 days following head injury.
In humans, encephalitis, vascular disorders, neoplasia,and head injury can directly affect ADH production and
release from the hypothalamic–pituitary axis, resultingin hypernatremia.6,13,14 Approximately 10% of humanswith diabetes insipidus have suffered blunt or penetrat-ing cranial trauma.15 In humans, hypernatremia is re-portedly a rare but often fatal complication of severehead trauma when anoxic encephalopathy, skull frac-tures, and cranial nerve dysfunction have occurred.16–18
In addition, hypernatremia has reportedly been a conse-quence of minor head trauma.15
Within hours to days, injury to the central osmore-ceptors, hypothalamus, supraopticohypophyseal tract, or
Acute hypernatremia is usually associated with a solute-freewater deficit and hyperosmolality.
H2O
Idiogenicosmoles
Na+

mary nephrogenic diabetes insipidus has not beenreported in cats.1
Secondary nephrogenic diabetes insipidus results fromdisruption of the corticomedullary osmotic gradient orinhibition of ADH action by the kidneys18 (Figure 3).Disruption of the corticomedullary osmotic gradient
can occur in the presence of infection, hypokalemia, orhypercalcemia. Endotoxins produced by Escherichia colimay produce renal V2 receptor resistance to ADH andcan be seen as a result of pyelonephritis and pyometra.Hypercalcemia damages ADH receptors in the tubules,and hypokalemia can decrease renal responsiveness toADH.1,18 Certain drug therapies have also reportedlycaused partial impairment of renal concentrating abilitythrough partial inhibition of ADH receptors.7
CONSEQUENCES OF ACUTEHYPERNATREMIA
In humans, the rate and degree that pOsm increasesdetermine the severity of the resulting clinical signs.9,19,20
Slowly progressive increases in pOsm caused by hyper-natremia may result in no signs. Acute hypernatremiacauses rapid fluid shifts from the intracellular to extra-cellular compartment (Figure 1). Clinical signs ofhypernatremia primarily involve the central nervous sys-tem.9,18,20 Neurologic signs range from lethargy andweakness to twitching, seizures, coma, and death.18,19
Brain cells respond to hypernatremia and cell shrink-age by increasing intracellular osmolarity to make itequal to pOsm. In rabbits and rats, experimentallyadministered intraperitoneal and IV hypertonic salinesolution result in a process of accommodation in braincells.6,19,21 Extracellular hypernatremia initially promoteswater loss from brain cells. Within 30 minutes, sodiumand potassium ion concentrations increase in brain cells.Within hours to days, the idiogenic osmole (aminoacids, glutamine, and inositol) concentration increases,reestablishing transcellular osmotic gradient and intra-cellular water content21 (Figure 4).
Few reports pertain to symptomatic hypernatremia incats. Mortality rates of more than 70% have been re-ported in adult humans when serum sodium levelsacutely increased over 160 mEq/L in less than 24
hours.22 We have observed hypernatremia as a severecomplication of diabetes mellitus, chronic respiratorydisease with upper airway discharge, and head trauma incats. When hypernatremia occurred in association withdiabetes mellitus or respiratory disease, treatment,including careful manipulation of fluid balance, was
usually successful; development of hypernatremia is pre-sumably slowly progressive in these cases. When acutehypernatremia occurred in four cats with head injury(sodium concentration: 171 to 209 mEq/L), concurrentneurologic deterioration developed. Three of the catswere humanely euthanized because of continued neuro-logic deterioration, and one recovered after 10 weeks ofsupportive care.
REFERENCES1. Feldman EC, Nelson RW: Canine and Feline Endocrinology and Reproduction,
ed 2. Philadelphia, WB Saunders, 1996.
2. Manning AM: Electrolyte disorders. Vet Clin North Am Small Anim Pract31(6):1289–1317, 2001.
3. Guyton AC, Hall JE: Regulation of extracellular fluid osmolarity and sodiumconcentration, in Guyton AC, Hall JE (eds): Textbook of Medical Physiology,ed 9. Philadelphia, WB Saunders, 1996, pp 349–365.
4. Ganong W: Central regulation of visceral function, in Ganong W (ed):Review of Medical Physiology, ed 14. San Mateo, CA, Appleton and Lange,1989, pp 191–211.
5. Robertson GL, Aycinena P, Zerbe RL: Neurogenic disorders of osmoregula-tion. Am J Med 72:339–353, 1982.
6. Palevsky PM: Hypernatremia. Semin Nephrology 18(1):20–30, 1998.
7. Blevins LS, Wand GS: Diabetes insipidus. Crit Care Med 20(1):69–79,1992.
8. Dow SW, Fettman MJ, LeCouteur RA, Allen TA: Hypodipsic hyperna-tremia and associated myopathy in a hydrocephalic cat with transient hypopi-tuitarism. JAVMA 191(2):217–221, 1987.
9. Rose BD, Post T: Clinical Physiology of Acid–Base and Electrolyte Disorders, ed5. New York, McGraw-Hill, 2001.
10. Mackay BM, Curtis N: Adipsia and hypernatremia in a dog with focalhypothalamic granulomatous meningoencephalitis. Aust Vet J 77(1):14–17,1999.
11. Kraus KH: The use of desmopressin in diagnosis and treatment of diabetesinsipidus in cats. Compend Contin Educ Pract Vet (9)7:752–758, 1987.
12. Burnie AG, Dunn JK: A case of central diabetes insipidus in the cat: Diagno-sis and treatment. J Small Anim Pract 23:237, 1982.
13. Ober KP: Diabetes insipidus. Crit Care Clin 7(1):109–125, 1991.
14. Bacic A, Gluncic V, Gluncic I: Disturbances in plasma sodium in patientswith war head injuries. Military Medicine 164(3): 214–217, 1999.
15. Kern KB, Meislin HW: Diabetes insipidus: Occurrence after minor headtrauma. J Trauma 24(1):69–72, 1984.
COMPENDIUM June 2004
Hypernatremia in Critically Ill Cats: Pathophysiology432 CE
Acute hypernatremia can rapidly result in loss of intracellularwater and neurologic alterations.

16. Notman D, Mortek M, Moses AM: Permanent diabetes insipidus followinghead trauma: Observations on ten patients and an approach to diagnosis. JTrauma 20(7):599–602, 1980.
17. Takaku A, Tatoian JA, LaDow CS, Diamond MC: Permanent posttraumaticdiabetes insipidus. J Oral Surg 33:548–551, 1975.
18. Geheb MA: Clinical approach to the hyperosmolar patient. Crit Care Clin5:797–815, 1987.
19. Gullans SR, Verbalis JG: Control of brain volume during hyperosmolar andhypoosmolar conditions. Annu Rev Med 44:289–301, 1993.
20. Ayus JC, Armstrong DL, Arieff AI: Effects of hypernatremia in the centralnervous system and its therapy in rats and rabbits. J Physiol 492:243–255,1996.
21. Lien YHH, Shapiro JI, Chan L: Effects of hypernatremia on organic brainosmoles. J Clin Invest 85:1427–1435, 1990.
22. Mandal AK, Saklayen MG, Hillman NM, Markert RJ: Predictive factors forhigh mortality in hypernatremic patients. Am J Emerg Med 15(2):130–132,1997.
1. What is the most abundant electrolyte in extra-cellular fluid and the major determinant ofpOsm?a. potassiumb. sodiumc. chlorided. magnesium
2. Which hormone is released during even minorincreases in pOsm?a. epinephrineb. glucagonc. ADHd. insulin
3. Administering which fluid may result in hyperna-tremia?a. 0.9% salineb. lactated Ringer’s solutionc. Normosol-Rd. hypertonic saline
June 2004 COMPENDIUM
Hypernatremia in Critically Ill Cats: Pathophysiology 433CE
ARTICLE #1 CE TEST This article qualifies for 1.5 contact hours of continuingeducation credit from the Auburn University College ofVeterinary Medicine. Subscribers who wish to apply thiscredit to fulfill state relicensure requirements should consulttheir respective state authorities regarding the applicabilityof this program.To participate, fill out the test form insertedat the end of this issue. To take CE tests online and get real-time scores, log on to www.VetLearn.com.
CE
4. Which condition can result in hypernatremiathrough renal osmotic diuresis and free waterloss?a. diabetes mellitusb. diabetes insipidusc. head traumad. pneumonia
5. Why does hypernatremia occur in patients withcentral diabetes insipidus?a. The kidneys are not responsive to ADH, resulting in
renal free water loss in excess of solute.b. There is minimal to no circulating ADH to allow
solute-free water resorption in the kidneys, andwater is lost in excess of solute.
c. More sodium is reabsorbed by the kidneys.d. Excessive aldosterone is released, resulting in
sodium gain.
6. Clinical signs of acute hypernatremia primarilyaffect the _______________ system.a. gastrointestinalb. cardiopulmonaryc. musculoskeletald. central nervous
7. The brain responds to chronic hypernatremia by a. producing idiogenic osmoles.b. becoming hyperplastic.c. releasing calcium.d. shrinking.
8. Hypernatremia can occur as a complication of a. diabetes mellitus.b. renal failure.c. diabetes insipidus.d. all of the above
9. Acute hypernatremia leads to neurologic dys-function because ita. alters potassium levels.b. causes rapid fluid shifts from the intracellular to
extracellular compartment.c. inhibits the sodium–potassium pump.d. causes hypocalcemia.
10. E. coli may cause nephrogenic diabetes insipidus bya. directly binding to ADH molecules.b. causing hypercalcemia.c. producing endotoxins that cause V2 receptor resis-
tance to ADH.d. altering BUN levels, thereby causing renal medullary
washout.