Embed Size (px)
Citation preview

Hyperleptinemia: Implications on the Inflammatory Stateand Vascular Protection in Obese Adolescents Submittedto an Interdisciplinary Therapy
Priscila L. Sanches,1 Marco T. de Mello,1,2,3 Natália Elias,3 Francisco A. H. Fonseca,4
Raquel M. S. Campos,1 June Carnier,1 Aline de Piano,1 Deborah C. L. Masquio,1
Patrícia L. Silva,1 Lila M. Oyama,5 Flavia C. Corgosinho,1 Cláudia M. O. Nascimento,1,5
Lian Tock,8 Carolina Ackel D’Elia,1 Sergio Tufik,2,3 and Ana R. Dâmaso1,6,7,9,10
Abstract—The low-grade systemic inflammation seen in obesity may affect the actions of someadipose tissue-derived adipokines that are involved in the regulation of vascular function. We soughtto verify whether hyperleptinemia may influence the inflammatory and atherogenic responses in obeseadolescents undergoing interdisciplinary therapy. Thirty-four obese adolescents underwent interdis-ciplinary therapy for 1 year. Subjects were considered hyperleptinemic if they had baseline values ofleptin above 20 ng/mL for boys and 24 ng/mL for girls. Both groups showed an improvement in bodycomposition and a reduction in carotid intima-media thickness. However, only subjects in the non-hyperleptinemic group showed an increase in adiponectin concentration after therapy. Moreover,leptin concentration was positively correlated with adiponectin and inversely correlated with PAI-1 inthis group. Hyperleptinemic state may impair the attenuation of inflammation in obese adolescentsundergoing interdisciplinary therapy, particularly by impeding the increase in adiponectin concen-tration, which is directly involved in vascular protection.
KEY WORDS: hyperleptinemia; adiponectin; obesity; vascular protection; interdisciplinary therapy.
INTRODUCTION
An increase in adipose tissue mass can lead to analteration in the production of systemic regulators ofchronic inflammation, which can then directly or indirectlyaffect vascular tissue [1]. Leptin is an adipocyte-derivedhormone that in physiological conditions exhibits func-tions related to the regulation of energy balance andcardiovascular health [2–4]. However, hyperleptinemia,common in obesity, is associated with insulin resistanceand disorders related to endothelial dysfunction,suggesting an overall decrease in sensitivity to leptin [3–5].
A recent study demonstrated that leptin and plasmin-ogen activator inhibitor type-1 (PAI-1) concentrations aredirectly associated, and adiponectin concentration is in-versely associated, with metabolic syndrome (MetS) amongadolescents, suggesting that these adipokinesmay be used asbiomarkers to predict MetS in this population [6].
1 Post-graduate Program of Nutrition, Universidade Federal de SãoPaulo, São Paulo, Brazil
2 Psychobiology Department, Universidade Federal de São Paulo, SãoPaulo, Brazil
3 Association Found of Incentive to Research, Universidade Federal deSão Paulo, São Paulo, Brazil
4 Cardiology Division, Department of Medicine, Universidade Federalde São Paulo, São Paulo, Brazil
5 Physiology Department, Universidade Federal de São Paulo, SãoPaulo, Brazil
6 Post-graduate Program of Interdisciplinary Health Sciences, Santos,Brazil
7 Biosciences Department, Universidade Federal de São Paulo, SãoPaulo, Brazil
8 Universidade Federal de São Paulo, São Paulo, Brazil9 Rua Prof. Francisco de Castro, 93–Vila Clementino, São Paulo, SP,Brazil 04020-050
10 To whom correspondence should be addressed at Rua Prof. Franciscode Castro, 93–Vila Clementino, São Paulo, SP, Brazil 04020-050. E-mail: [email protected]
0360-3997/14/0100-0035/0 # 2013 Springer Science+Business Media New York
Inflammation, Vol. 37, No. 1, February 2014 (# 2013)DOI: 10.1007/s10753-013-9709-9
35

Moreover, adiponectin, an adipose tissue-specificfactor that improves insulin sensitivity and inhibitsvascular inflammation, is paradoxically reduced in obe-sity [7]. Studies with obese adolescents have shown thatexpression of this anti-inflammatory adipokine is nega-tively correlated with leptin concentrations and withcarotid intima-media thickness (cIMT), a traditionalmarker of subclinical atherosclerosis [5, 8–10].
Although it is well established in the literature thatobesity is associated with higher leptin concentrations,lower levels of adiponectin, and with atherosclerosis [1, 4,11], the influence of hyperleptinemia on inflammatoryand atherogenic responses in obese adolescents undergo-ing long-term interdisciplinary therapy has not beenexamined. Some findings suggest that high leptin con-centrations accelerate the atherosclerotic process whileother studies show a protective role for leptin inatherosclerosis [2, 12, 13].
Therefore, the aim of this study was to verifywhether higher baseline leptin concentrations, reflectinga state of hyperleptinemia, may influence the inflamma-tory and atherogenic responses in obese adolescentsundergoing long-term interdisciplinary therapy. We hy-pothesized that higher baseline leptin concentrationswould negatively affect the outcomes of this therapy.
MATERIALS AND METHODS
Study Subjects
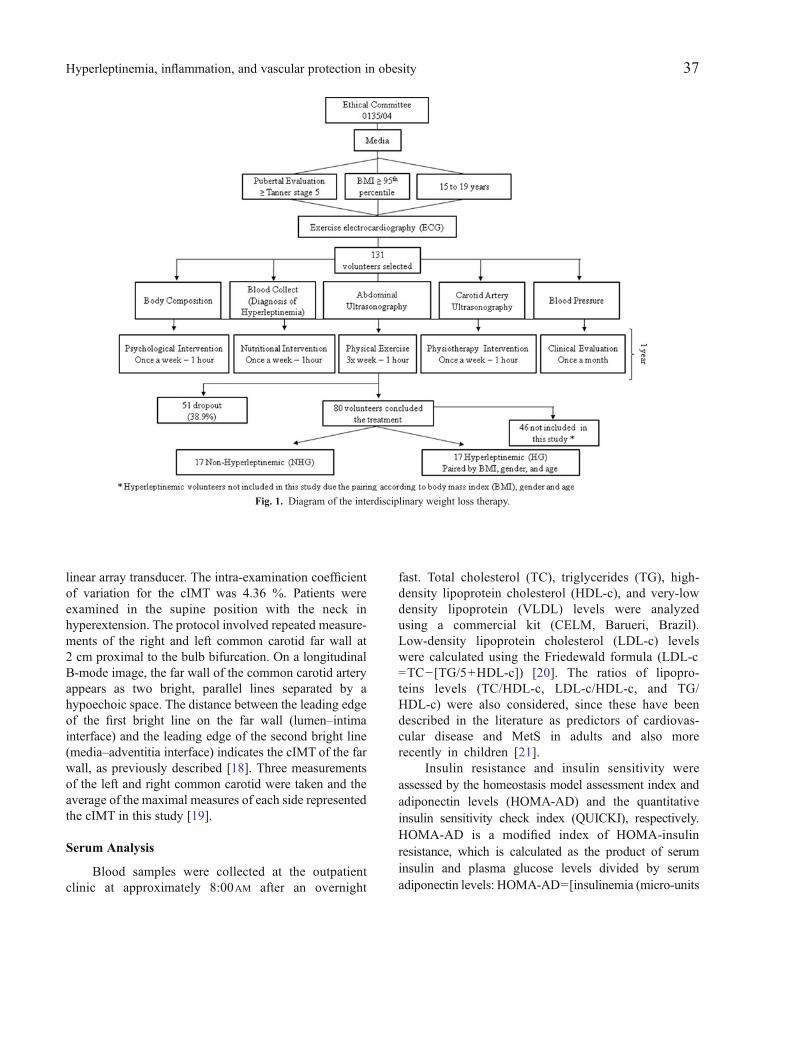
A total of 131 post-pubescent [14] obese adolescentsof both genders were recruited for interdisciplinaryweight loss therapy for a course of 1 year. However, ofthese 131 participants, 51 (38.9 %) dropped out of thestudy before the completion of therapy. Of the 80volunteers who completed the treatment, 17 (eight boysand nine girls) had physiological concentrations of leptinat baseline and were included in the study, while 63volunteers exhibited high leptin concentrations(hyperleptinemia) at baseline. Of these 63 participants,17 were included in the study; they were paired by bodymass index (BMI), gender, and age with the control group(Fig. 1). To meet the inclusion criteria for participation inthis weight loss therapy, subjects had to be post-pubescentadolescents presenting with obesity who were healthyenough to perform physical activity and who were willingand able to participate in the program for 1 year. Theexclusion criteria included factors such as an identifiedgenetic disease, chronic alcohol consumption, previous
use of drugs such as glucocorticoids and psychotropics,and pregnancy. All participants were from 15 to 19 yearsof age and presented with obesity, i.e., a BMI≥ the 95thpercentile, as defined by the Centers for Disease Controland Prevention [15].
Subjects were considered hyperleptinemic if theyexhibited baseline leptin values above 20 ng/mL for boysand 24 ng/mL for girls, based on reference values cited byGutin et al. [16]. Informed parental consent and theadolescents’ assent to participate as a volunteer in aweight loss therapy program were obtained. This studywas conducted in accordance with the principles of theHelsinki Declaration and was formally approved by theEthics Committee of the Federal University of São Paulo(Number: 0135/04) and registered at clinicaltrials.gov(NCT01358773).
Anthropometric Measurements and BodyComposition
Volunteers were weighedwhile wearing light clothingand barefoot, on a Filizola scale to the nearest 0.1 kg.Height was measured to the nearest 0.5 cm with a wall-mounted stadiometer (Sanny, model ES 2030). BMI wascalculated as body weight divided by height squared (wt/ht2). Body composition was measured by air displacementplethysmography in a BOD POD body compositionsystem (version 1.69; Life Measurement Instruments,Concord, CA).
Measurements of Visceral and Subcutaneous Fat
All abdominal ultrasonography procedures and mea-surements of visceral and subcutaneous fat were performedby the same blinded diagnostic imaging specialist using a3.5 MHz multifrequency transducer (broad band), beforeand after intervention. This procedure allowed a reductionin the risk margin for misclassification. The intra-exami-nation coefficient of variation for ultrasonography was0.8 %. Ultrasonography measurements of visceral andsubcutaneous fat were taken in according to methodologypreviously described [17].
Measurements of Carotid Artery Intima-MediaThickness
The cIMT was measured by the same experiencedradiologist, who was blinded to the participants’ labora-tory values and risk factor levels, before and afterintervention using high-resolution ultrasound equipment(Logic 5 and Logic 7, General Electric) with a 7–14 MHz
36 Sanches, de Mello, Elias, Fonseca, Campos, et al.
linear array transducer. The intra-examination coefficientof variation for the cIMT was 4.36 %. Patients wereexamined in the supine position with the neck inhyperextension. The protocol involved repeated measure-ments of the right and left common carotid far wall at2 cm proximal to the bulb bifurcation. On a longitudinalB-mode image, the far wall of the common carotid arteryappears as two bright, parallel lines separated by ahypoechoic space. The distance between the leading edgeof the first bright line on the far wall (lumen–intimainterface) and the leading edge of the second bright line(media–adventitia interface) indicates the cIMT of the farwall, as previously described [18]. Three measurementsof the left and right common carotid were taken and theaverage of the maximal measures of each side representedthe cIMT in this study [19].
Serum Analysis
Blood samples were collected at the outpatientclinic at approximately 8:00AM after an overnight
fast. Total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-c), and very-lowdensity lipoprotein (VLDL) levels were analyzedusing a commercial kit (CELM, Barueri, Brazil).Low-density lipoprotein cholesterol (LDL-c) levelswere calculated using the Friedewald formula (LDL-c=TC− [TG/5+HDL-c]) [20]. The ratios of lipopro-teins levels (TC/HDL-c, LDL-c/HDL-c, and TG/HDL-c) were also considered, since these have beendescribed in the literature as predictors of cardiovas-cular disease and MetS in adults and also morerecently in children [21].
Insulin resistance and insulin sensitivity wereassessed by the homeostasis model assessment index andadiponectin levels (HOMA-AD) and the quantitativeinsulin sensitivity check index (QUICKI), respectively.HOMA-AD is a modified index of HOMA-insulinresistance, which is calculated as the product of seruminsulin and plasma glucose levels divided by serumadiponectin levels: HOMA-AD=[insulinemia (micro-units
Fig. 1. Diagram of the interdisciplinary weight loss therapy.
37Hyperleptinemia, inflammation, and vascular protection in obesity

per liter)×glycemia (millimoles per liter)]/adiponectinemia(micrograms per milliliter) [22]. QUICKIwas calculated as1/(log I+log fasting blood glucose). The coefficient ofvariation for the insulin test was 3.3 %.
The leptin, adiponectin, and PAI-1 concentrationswere measured using a commercially available enzyme-linked immunosorbent assay kit from R&D Systems(Minneapolis, USA), according to the manufacturer’sinstructions.
Blood Pressure
Blood pressure (BP) was measured on the right armusing a mercury-gravity manometer with proper cuff size,with the volunteers in the seated position [10, 23].Hypertension was determined by reference values of BPpercentiles for gender, according to age and heightpercentile [24]. Mean blood pressure (MBP) was calcu-lated as DBP+[(SBP−DBP)/3].
Research Design
The interdisciplinary weight loss program includedclinical, nutritional, psychological physiotherapy andcombined exercise training (aerobic plus resistancetraining). All measurements were performed before andafter 1 year of intervention (Fig. 1).
Clinical Therapy
Obese adolescents visited the endocrinologistmonthly for the assessment of health and clinicalparameters. Medical treatment and follow-up were basedon an initial patient and family history, physical exami-nation, and intervention in any health problems that thepatient developed over the course of the therapy.
Nutritional Therapy
Energy intake was set at the levels recommended bythe dietary reference intake for subjects with low levels ofphysical activity of the same age and gender [25]. Once aweek, adolescents received dietetics lessons covering thetopics related to a healthy eating pattern. All patientsreceived individual nutritional consultation during theintervention program. At the beginning of the study and at12 months into the program, a 3-day dietary record wascollected. Because most obese people under-report theirfood consumption, each adolescent was asked to recordtheir diet with help from their parents. The degree ofunder-reporting may still be substantial; however, this is a
validated method for the assessment of dietary consump-tion [17]. These dietary data were transferred to acomputer by the same dietician, and the nutrientcomposition was analyzed by a PC program devel-oped at the Federal University of São Paulo–PaulistaMedicine School (Nutwin software, for Windows,version 1.5, 2002).
Psychological Therapy
Psychological therapy treatment plans wereestablished based on validated questionnaires taking intoaccount some of the psychological problems caused byobesity, as outlined in the literature. These includeddepression, eating disorders, anxiety, decreased self-esteem, and body-image disorders. Interdisciplinarytherapy consisted of weekly 1-h group sessions. Individ-ualized psychological therapy was recommended whenserious problems were found.
Exercise Protocol
The combined exercise-training program wasperformed three times per week and included 30 min ofaerobic training plus 30 min of resistance training persession. The subjects were instructed to reverse the orderof the exercises (aerobic and resistance) at each trainingsession.
The aerobic training consisted of running on amotor-driven treadmill (Life Fitness–Model TR9700HR) at a cardiac frequency intensity representingventilatory threshold 1 (±4 bpm), according to the resultsof an initial oxygen uptake test for aerobic exercises. Theexercise program was based on guidelines from theAmerican College of Sports Medicine (ACSM), 2009[26].
Resistance training was also designed based onACSM recommendations. Exercises targeted each of themain muscle groups. After an introductory period(2 weeks for adaptation to training to learn the move-ment), the load of training was adjusted, and each 8-weekvolume and intensity were adjusted inversely, decreasingthe number of repetitions from 15–20 to 10–12 and 6–8respectively, for three sets. All sessions were rigorouslysupervised by an experienced physiologist.
Physiotherapy
The subjects participated in an intervention with twophysical therapists once per week. The themes of theseinterventions were global postural reeducation, isostretching,
38 Sanches, de Mello, Elias, Fonseca, Campos, et al.

diaphragmatic breathing, hydrotherapy, balance, andstretching. Individual consultations were also performed ifthe patient had any injuries. The interventions wereconducted in a room next to the gym, suitable for this typeof intervention.
Statistical Analysis
Statistical analyses were performed usingSTATISTICA (version 7.0 for Windows). The Gaussiandistribution of variables (including Δ values) wereverified using the Kolmogorov–Smirnov test. Variableswith a normal distribution were expressed as mean(standard deviation (SD)), while variables that did nothave a normal distribution were expressed as median(quartile range) in a descriptive table. The HOMA-ADand leptin/adiponectin ratio were log-transformed fortests of statistical significance, since these variables didnot have a normal distribution.
Comparisons between measurements before andafter intervention were performed using the pairedStudent’s t test. Independent Student’s t and Mann-Whitney U tests were performed to compare the magni-tude of change (Δ) between groups. Spearman andPearson’s correlation coefficients were calculated toassess possible relationships between normal and non-normally distributed variables, respectively. Significancewas set as p<0.05.
RESULTS
There was a significant reduction of cIMT [mean(SD)] in both groups [from 0.41 (0.07) to 0.36 (0.04)(millimeters) and from 0.41 (0.04) to 0.35 (0.04)(millimeters) in the non-hyperleptinemic (NHL) andhyperleptinemic (HL) groups, respectively] after theinterdisciplinary intervention. Both groups also showedsignificant improvements in body composition (totalbody mass, BMI, body fat (kilograms), and visceral fat),as demonstrated in Table 1, as well as significantdecreases in lipoprotein ratios (CT/HDL-c and LDL-HDL-c) and some indices of glucose metabolism (insulinconcentration and HOMA-AD) (Table 2). A statisticalanalysis by gender indicated similar outcomes betweenboys and girls of both groups. Therefore, we have noreason to suspect that the data presented in this study isgender-dependent.
Non-hyperleptinemic Group
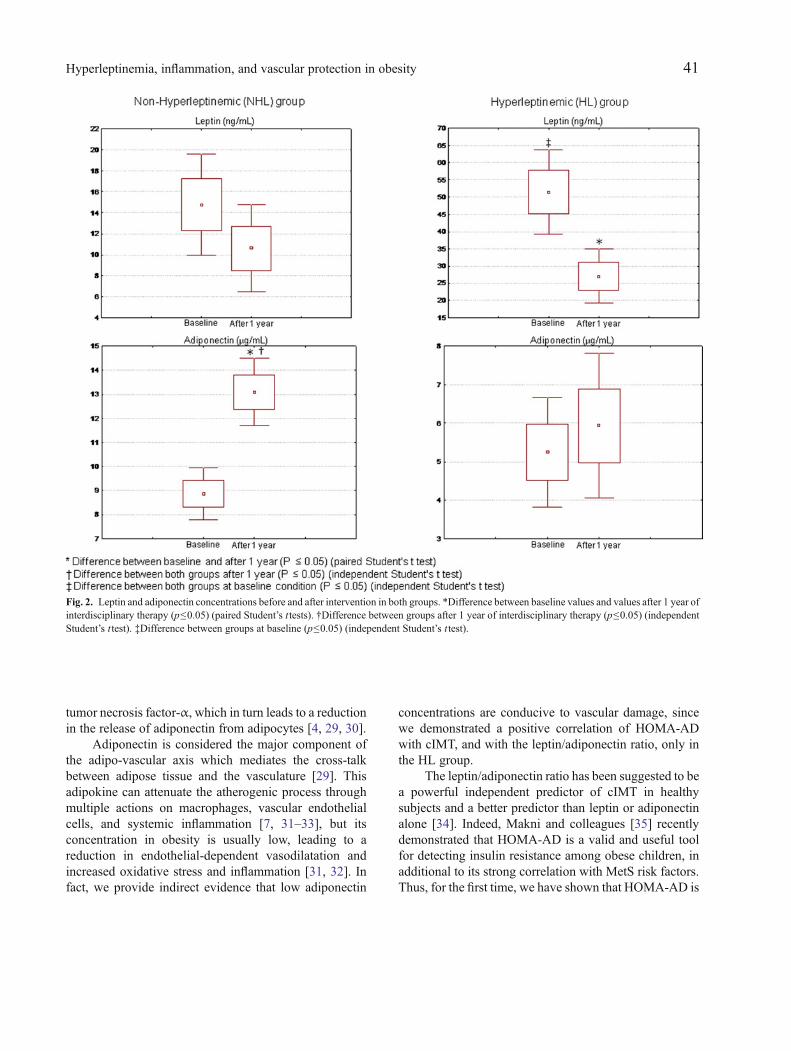
Only the NHL group showed significant increases inadiponectin concentrations after the interdisciplinaryintervention (Fig. 2). At the end of therapy, the concen-tration of this hormone was significantly higher (Fig. 2)whereas the HOMA-AD values were significantly lower(Table 2) in this group compared with the HL group.
Physiological leptin concentrations were positivelycorrelated with serum adiponectin (r=0.63, p<0.05) andnegatively correlated with PAI-1 concentrations (r=−0.51, p<0.05) and with HOMA-AD (r=−0.50, p<0.05).
Hyperleptinemic Group
At baseline, leptin concentrations were significantlyhigher in the HL group than in the NHL group, and onlythe HL group showed significant reductions of thishormone after therapy (Fig. 2). However, even with thesignificant decrease in the leptin/adiponectin ratio seen inthe HL group, these subjects still had higher valuescompared with the NHL group both before and afterintervention (Table 2). The HOMA-AD values werepositively correlated with cIMT (r=0.64, p<0.05) andwith the leptin/adiponectin ratio (r=0.65, p<0.05) atbaseline, and these higher values were maintained at theend of therapy when compared with the NHL group(Table 2). In the HL group only, the change in PAI-1concentration (ΔPAI-1) was positively correlated with thechange in cIMT (ΔcIMT) (r=0.60; p<0.05).
DISCUSSION
Programs that attempt to modify lifestyle have beenthe mainstay of controlling obesity in children andadolescents and have proved to be effective in reducingtraditional and novel risk factors of atherosclerosis,including insulin resistance, inflammatory markers, andatherogenic lipid profiles [10, 27, 28]. In agreement withthese findings, the long-term interdisciplinary therapyproposed in this study contributed to significant reduc-tions in total body mass, BMI, body fat mass, visceral fat,insulin concentration, HOMA-AD, TC/HDL-c, LDL/HDL-c, and cIMT in both groups. All these ameliorationsare important to control obesity and subclinical athero-sclerotic processes.
Nevertheless, the most important finding of thisstudy was that only subjects in the NHL group showed anincrease in adiponectin concentration after therapy, whichwas maintained at significantly higher levels after
39Hyperleptinemia, inflammation, and vascular protection in obesity

interdisciplinary therapy, when compared with the HLgroup. These outcomes suggest that a hyperleptinemicstate impairs the attenuation of inflammation and thusleads to a decrease in vascular protection in obeseadolescents. The molecular theory that supports this
finding is the fact that multiple immune cells express theleptin receptor (Ob-Rb) and thus may be modulated bythis hormone. Therefore, a hyperleptinemic state leads toan inflammatory milieu that induces the secretion ofproinflammatory cytokines such as interleukin-6 and
Table 1. Body Composition of Both Groups Before and After Long-Term Interdisciplinary Therapy
Non-hyperleptinemic (NHL) n=17 Hyperleptinemic (HL) n=17
Baseline After 1 year Δ Baseline After 1 year Δ
Age (years) 18 (2) 17 (1)Total body mass (kg) 97.01 (13.49) 87.21 (14.50)* −13.06 (8.76) 99.54 (16.25) 86.76 (12.08)* −10.32 (6.86)Body mass index (kg/m2) 34.61 (3.99) 29.95 (4.89)* −4.68 (2.86) 34.77 (4.15) 30.36 (4.30)* −3.99 (2.49)Fat body mass (kg) 38.46 (16.67) 27.34 (11.02)* −14.66 (8.32) 44.81 (11.37) 30.20 (10.34)* −12.99 (5.86)Lean body mass (kg) 55.61 (7.44) 60.97 (8.90) 3.28 (5.83) 54.71 (7.77) 56.60 (7.64) 2.74 (3.17)Visceral fat (cm) 3.83 (3.79) 2.19 (0.75)* −2.14 (0.60) 4.22 (1.47) 2.77 (0.92)* −1.33 (1.33)Subcutaneous fat (cm) 3.58 (0.70) 2.63 (0.75) −0.70 (0.59) 3.77 (0.73) 2.99 (0.75)* −0.73 (0.90)
Data are presented as mean (SD)*p≤0.05, difference between baseline and after 1 year (paired Student’s ttest)
Table 2. Glucose Metabolism, Lipid Profile, Inflammation, and Carotid Intima-Media Thickness for Both Groups before and After Long-Term Inter-disciplinary Therapy
Non-hyperleptinemic (NHL) n=17 Hyperleptinemic (HL) n=17
Baseline After 1 year Δ Baseline After 1 year Δ
Insulin (mU/L) 16.68 (6.19) 7.51 (2.23)* −10.00 (6.81) 15.72 (6.51) 11.66 (5.93)* −3.93 (5.00)Glucose (mg/dL) 89 (6) 82 (4)* −11 (6) 91 (7) 89 (6) −2 (7)HOMA-AD 9.06
[5.43–11.94]2.72[2.0–3.29]*
−5.86[−14.95–−5.38]
12.01[7.74–29.11]
10.69[3.57–20.60]*†
−5.60 [−11.28–−0.78]
QUICKI 0.32 (0.02) 0.36 (0.02)* 0.05 (0.02) 0.32 (0.02) 0.34 (0.03) 0.02 (0.03)Total cholesterol(mg/dL)
179 (25) 163 (40) −21 (35) 167 (31) 164 (31) −4 (15)
HDL-c (mg/dL) 42 (9) 38 (8) 1 (6) 41 (9) 46 (9)* 5 (6)LDL-c (mg/dL) 117 (25) 103 (29)* −23 (25) 106 (28) 100 (28) −7 (14)VLDL (mg/dL) 19 (6) 22 (9) 1 (10) 20 (9) 18 (10) −2 (7)Triglycerides(mg/dL)
98 (30) 109 (44) 4 (48) 101 (45) 91 (48) −12 (37)
TC/HDL-c ratio 4.45 (1.14) 4.29 (0.79)* −0.75 (0.80) 4.28 (1.39) 3.75 (1.06)* −0.59 (0.58)LDL-c/HDL-c ratio 2.95 (0.97) 2.72 (0.66)* −0.74 (0.59) 2.74 (1.12) 2.33 (0.92)* −0.45 (0.57)TG/HDL-c ratio 2.51 (1.09) 2.84 (0.98) −0.09 (1.18) 2.70 (1.61) 2.09 (1.24) −0.68 (0.93)MBP (mmHg) 94 (10) 88 (6) −7 (9) 92 (9) 86 (6) −6 (10)Leptin/adiponectin ratio 1.64
[2.09–1.02]0.67[0.33–1.31]
−0.64[−1.20–−0.25]
12.45[3.97–17.01]‡
3.49[2.43–8.59]*†
−5.08 [−12.59–−3.08]
PAI-1 (ng/mL) 17.91 (8.77) 16.12 (10.25) −0.47 (6.72) 11.41 (8.02) 7.40 (8.04) −4.77 (6.77)hs CRP (ng/mL) 0.28 (0.27) 0.16 (0.24) −0.13 (0.28) 0.19 (0.14) 0.22 (0.21) 0.03 (0.26)cIMT(mm) 0.41 (0.07) 0.36 (0.04)* −0.06 (0.08) 0.41 (0.04) 0.35 (0.04)* −0.06 (0.05)
HOMA-AD homeostasis model assessment of adiponectin index, QUICKI quantitative insulin sensitivity check index, HDL-c High-density lipoprotein-cholesterol, LDL-c low-density lipoprotein-cholesterol, VLDL very-low-density lipoprotein, MBP mean blood pressure, PAI-1 plasminogen activatorinhibitor 1, hs CRP high-sensitivity c-reactive protein, cIMT carotid intima-media thickness. Reference values (13): total cholesterol<150; LDL-c<100;HDL-c≥45; triglycerides<100 (milligrams per deciliter). Data are presented as mean (SD) or median [quartile range]*p≤0.05, difference between baseline values and values after 1 year of interdisciplinary therapy (paired Student’s t tests)† p≤0.05, difference between groups after 1 year of interdisciplinary therapy (independent Student’s t test)‡ p≤0.05, difference between groups at baseline (independent Student’s t test)
40 Sanches, de Mello, Elias, Fonseca, Campos, et al.
tumor necrosis factor-α, which in turn leads to a reductionin the release of adiponectin from adipocytes [4, 29, 30].
Adiponectin is considered the major component ofthe adipo-vascular axis which mediates the cross-talkbetween adipose tissue and the vasculature [29]. Thisadipokine can attenuate the atherogenic process throughmultiple actions on macrophages, vascular endothelialcells, and systemic inflammation [7, 31–33], but itsconcentration in obesity is usually low, leading to areduction in endothelial-dependent vasodilatation andincreased oxidative stress and inflammation [31, 32]. Infact, we provide indirect evidence that low adiponectin
concentrations are conducive to vascular damage, sincewe demonstrated a positive correlation of HOMA-ADwith cIMT, and with the leptin/adiponectin ratio, only inthe HL group.
The leptin/adiponectin ratio has been suggested to bea powerful independent predictor of cIMT in healthysubjects and a better predictor than leptin or adiponectinalone [34]. Indeed, Makni and colleagues [35] recentlydemonstrated that HOMA-AD is a valid and useful toolfor detecting insulin resistance among obese children, inadditional to its strong correlation with MetS risk factors.Thus, for the first time, we have shown that HOMA-AD is
Fig. 2. Leptin and adiponectin concentrations before and after intervention in both groups. *Difference between baseline values and values after 1 year ofinterdisciplinary therapy (p≤0.05) (paired Student’s t tests). †Difference between groups after 1 year of interdisciplinary therapy (p≤0.05) (independentStudent’s t test). ‡Difference between groups at baseline (p≤0.05) (independent Student’s t test).
41Hyperleptinemia, inflammation, and vascular protection in obesity

positively correlated with markers of subclinical athero-sclerosis in hyperleptinemic obese adolescents.
Adiponectin also improves insulin sensitivitythrough its actions on liver and skeletal muscle, whichindirectly contributes to vascular protection [31, 36]. Inthis study, we observed that the HL group had higherHOMA-AD values (a marker of insulin resistance) aftertherapy compared with the NHL group. These resultsreinforce the positive association between adiponectinand insulin sensitivity, and suggest that the productionand function of adiponectin in insulin sensitivity may belimited by the higher leptin concentrations in obeseadolescents. A cohort study should be performed toconfirm this finding.
In addition, previous studies have shown thatleptin can increase the expression of PAI-1 in humancoronary artery endothelial cells [37], which is inline with the positive correlation between leptin andPAI-1 concentrations seen in the present study. PAI-1plays an important role in the development andprogression of atherosclerosis [38, 39], and our studyhas revealed that changes in this prothrombotic factorare positively correlated with changes in cIMT in theHL group.
Taken together, our results suggest that, in obeseadolescents, the influence of interdisciplinary weight losstherapy on the inflammatory response and vascularprotection is negatively influenced by hyperleptinemia,mediated by low concentrations of adiponectin.
We acknowledge certain limitations of our research.The sample size was small due to the high drop-out rateoften seen in long-term studies and, in particular, instudies with adolescent populations, where study recruit-ment and compliance with treatment is more difficult andthe success of treatment depends at least partly on theparticipation of the parents and/or guardians. Furtherinvestigation including a control group and long-termfollow-up are needed. In addition, in general, subjectswith high levels of leptin appeared to have roughlyidentical “recoveries” following substantial weight loss,which could suggest that baseline leptin is not aparticularly useful predictor of the disease risks associat-ed with obesity. However, the strength of our study wasthat, although both groups had significantly reduced thetotal body mass, fat body mass, visceral fat, amongother markers, the impairment in the inflammatoryresponse was specific to the hyperleptinemic group.Additional experimental studies will be necessary toinvestigate the mechanisms involved in our clinicalfindings.
In conclusion, our results suggest that a hyperleptinemicstate may impair the attenuation of inflammation in obeseadolescents undergoing interdisciplinary therapy, particularlyby impeding the increase in adiponectin concentration, whichis directly involved in the vascular protection againstatherosclerosis.
It is important to highlight the relevance of investi-gating leptin concentrations in obese adolescents undergo-ing to weight loss programs, since a hyperleptinemic stateseems to impair the effects of interdisciplinary therapy.
ACKNOWLEDGMENTS
We would like to thank the patients that participatedof the study.
Grants. This study was supported in part by researchgrants from: AFIP; FAPESP 2008/53069-0; FAPESP 2011/50356-0, FAPESP 2011/50414-0; FAPESP (CEPID/Sleep#9814303-3 S.T); CNPq; CAPES (AUX-PE-PNPD 2566/2011); CEPE, FADA, and UNIFESP.
Disclosures. No conflicts of interest are reported by theauthor(s).
REFERENCES
1. Zhang, H., J. Cui, and C. Zhang. 2010. Emerging role of adipokinesas mediators in atherosclerosis. World Journal of Cardiology 2(11):370–376.
2. Bełtowski, J. 2012. Leptin and the regulation of endothelial functionin physiological and pathological conditions. Clinical and Experi-mental Pharmacology and Physiology 39(2): 168–178.
3. Mantzoros, C.S., F. Magkos, M. Brinkoetter, E. Sienkiewicz, T.A.Dardeno, S.Y. Kim, O.P. Hamnvik, and A. Koniaris. 2011. Leptin inhuman physiology and pathophysiology. American Journal ofPhysiology, Endocrinology and Metabolism 301(4): E567–E584.
4. Martin, S.S., A. Qasim, and M.P. Reilly. 2008. Leptin resistance: apossible interface of inflammation and metabolism in obesity-relatedcardiovascular disease. Journal of the American College ofCardiology 52(15): 1201–1210.
5. Dâmaso, A.R., A. de Piano, P.L. Sanches, F. Corgosinho, L. Tock,L.M. Oyama, L. Tock, C.M. do Nascimento, S. Tufik, and M.T. deMello. 2011. Hyperleptinemia in obese adolescents deregulatesneuropeptides during weight loss. Peptides 32(7): 1384–1391.
6. González,M., BibiloniM. DelMar, A. Pons, I. Llompart, and J.A. Tur.2012. Inflammatory markers and metabolic syndrome among adoles-cents. European Journal of Clinical Nutrition 66(10): 1141–1145.
7. Matsuzawa, Y. 2005. Adiponectin: identification, physiology andclinical relevance in metabolic and vascular disease. AtherosclerosisSupplements 6(2): 7–14.
42 Sanches, de Mello, Elias, Fonseca, Campos, et al.

8. Beauloye, V., F. Zech, H.T. Tran, P. Clapuyt, M. Maes, and S.M.Brichard. 2007. Determinants of early atherosclerosis in obesechildren and adolescents. Journal of Clinical Endocrinology andMetabolism 92: 3025–3032.
9. Corgosinho, F.C., A. de Piano, P.L. Sanches, R.M. Campos, P.L.Silva, J. Carnier, L.M. Oyama, L. Tock, S. Tufik, M.T. de Mello, andA.R. Dâmaso. 2012. The role of PAI-1 and adiponectin on theinflammatory state and energy balance in obese adolescents withmetabolic syndrome. Inflammation 35(3): 944–951.
10. de Lima, Sanches P., M.T. de Mello, N. Elias, F.A. Fonseca, A. dePiano, J. Carnier, L.M. Oyama, L. Tock, S. Tufik, and A.R. Dâmaso.2011. Improvement in HOMA-IR is an independent predictor ofreduced carotid intima-media thickness in obese adolescentsparticipating in an interdisciplinary weight-loss program. Hyperten-sion Research 34(2): 232–238.
11. Korda, M., R. Kubant, S. Patton, and T. Malinski. 2008. Leptin-induced endothelial dysfunction in obesity. American Journal ofPhysiology-Heart and Circulatory Physiology 295(4): 1514–1521.
12. Brennan, A.M., T.Y. Li, I. Kelesidis, A. Gavrila, F.B. Hu, and C.S.Mantzoros. 2007. Circulating leptin levels are not associated withcardiovascular morbidity and mortality in women with diabetes: aprospective cohort study. Diabetologia 50: 1178–1185.
13. Matarese, G., C. Mantzoros, and A. La Cava. 2007. Leptin andadipocytokines: bridging the gap between immunity and atheroscle-rosis. Current Pharmaceutical Design 13: 3676–3680.
14. Tanner, J.M., and R.H. Whitehouse. 1976. Clinical longitudinalstandards for height, weight, weight velocity and stages of puberty.Archives of Disease in Childhood 51: 170–179.
15. Centers for Disease Control and Prevention. Hyattsville: NationalCenter for Health Statistics. (Updates on 11 January 2007; accessedon 15 August 2011). Prevalence ofoverweight among children andadolescents: United States 1999–2002. http://www.cdc.gov/nchs/products/pubs/pubd/hestats/overwght99.htm.
16. Gutin, B., L. Ramsey, P. Barbeau, W. Cannady, M. Ferguson, M.Litaker, and S. Owens. 1999. Plasma leptin concentrations in obesechildren: changes during 4-mo periods with and without physicaltraining. American Journal of Clinical Nutrition 69: 388–394.
17. de Piano, A., W.L. Prado, D.A. Caranti, K.O. Siqueira, S.G. Stella,M. Lofrano, L. Tock, D.M. Cristofalo, H. Lederman, S. Tufik, M.T.de Mello, and A.R. Dâmaso. 2007. Metabolic and nutritional profileof obese adolescents with nonalcoholic fatty liver disease. Journal ofPediatric Gastroenterology and Nutrition 44: 446–452.
18. Guardamagna, O., F. Abello, P. Saracco, V. Baracco, E. Rolfo, andM. Pirro. 2009. Endothelial activation, inflammation and prematureatherosclerosis in children with familial dyslipidemia. Atheroscle-rosis 207: 471–475.
19. Rabago Rodriguez, R., R.A. Gómez-Díaz, J. Tanus Haj, F.J. AvelarGarnica, E. Ramirez Soriano, E. Nishimura Meguro, C.A. Aguilar-Salinas, and N.H. Wacher. 2007. Carotid intima-media thickness inpediatric type 1 diabetic patients. Diabetes Care 30: 2599–2602.
20. Friedewald, W., R. Levy, and D. Friderickson. 1972. Estimation ofthe concentration of low density protein cholesterol in plasma,without use of the preparative ultracentrifuge. Clinical Chemistry18: 449–515.
21. Quijada, Z., M. Paoli, Y. Zerpa, N. Camacho, R. Cichetti, V.Villarroel, G. Arata-Bellabarba, and R. Lanes. 2008. The triglycer-ide/HDL-cholesterol ratio as a marker of cardiovascular risk inobese children; association with traditional and emergent riskfactors. Pediatric Diabetes 9: 464–471.
22. Matsuhisa, M., Y. Yamasaki, M. Emoto, M. Shimabukuro, T.Funahashi, and Y. Matsuzawa. 2007. A novel index of insulinresistance determined from the homeostasis model assessment indexand adiponectin levels in Japanese subjects. Diabetes Research andClinical Practice 77: 151–154.
23. Chobanian, A.V., G.L. Bakris, H.R. Black, W.C. Cushman, L.A.Green, J.L. Izzo Jr., D.W. Jones, B.J. Materson, S. Oparil, J.T.
Wright Jr., E.J. Roccella, and National Heart, Lung, and BloodInstitute Joint National Committee on Prevention, Detection,Evaluation, and Treatment of High Blood Pressure; National HighBlood Pressure Education Program Coordinating Committee. 2003.The seventh report of the joint national committee on prevention,detection, evaluation, and treatment of high blood pressure: the JNC7 report. Journal of the American Medical Association 289(19):2560–2572.
24. Giuliano, I.C.B., B. Caramelli, L. Pellanda, B. Duncan, S. Mattos, andF.A.H. Fonseca. 2006. I Guideline for preventing atherosclerosis inchildhood and adolescence. International Atherosclerosis 1: 1–30..
25. NRC. 2001. Dietary reference intake: applications in dietaryassessment. Washington, DC: National Academic Press.
26. Donnelly, J.E., S.N. Blair, J.M. Jakicic, M.M. Manore, J.W. Rankin,and B.K. Smith. 2009. Appropriate physical activity interventionstrategies for weight loss and prevention of weight regain for adults.Medicine & Science in Sports & Exercise 41: 459–471.
27. Kelishadi, R., M. Hashemi, N. Mohammadifard, S. Asgary, and N.Khavarian. 2008. Association of changes in oxidative andproinflammatory states with changes in vascular function after alifestyle modification trial among obese children.Clinical Chemistry54(1): 147–153.
28. Monzavi, R., D. Dreimane, M.E. Geffner, S. Braun, B. Conrad, M.Klier, and F.R. Kaufman. 2006. Improvement in risk factors formetabolic syndrome and insulin resistance in overweight youth whoare treated with lifestyle intervention. Pediatrics 117: e1111–e1118.
29. Matarese, G., S. Moschos, and C.H. Mantzoros. 2005. Leptin inimmunology. Journal of Immunology 173: 3137–3142..
30. Zhao, Y., R. Sun, L. You, C. Gao, and Z. Tian. 2003. Expression ofleptin receptor and response to leptin stimulation of human naturalkiller cell lines. Biochemical and Biophysical Research Communi-cations 300(2): 247–252.
31. Li, F.Y., K.K. Cheng, K.S. Lam, P.M. Vanhoutte, and A. Xu.2011. Cross-talk between adipose tissue and vasculature: roleof adiponectin. Acta Physiologica (Oxford, England) 203(1):167–180.
32. Ohashi, K., N. Ouchi, and Y. Matsuzawa. 2012. Anti-inflammatoryand anti-atherogenic properties of adiponectin. Biochimie 94(10):2137–2142.
33. Ouchi, N., and K.Walsh. 2007. Adiponectin as an anti-inflammatoryfactor. Clinica Chimica Acta 380(1–2): 24–30.
34. Norata, G.D., S. Raselli, L. Grigore, K. Garlaschelli, E. Dozio, P.Magni, and A.L. Catapano. 2007. Leptin: adiponectin ratio is anindependent predictor of intima media thickness of the commoncarotid artery. Stroke 38: 2844–2846.
35. Makni, E., W. Moalla, G. Lac, C. Aouichaoui, D. Cannon, M.Elloumi, and Z. Tabka. 2012. The Homeostasis ModelAssessment-adiponectin (HOMA-AD) is the most sensitivepredictor of insulin resistance in obese children. Annalesd’endocrinologie 73(1): 26–33..
36. Dullaart, R.P., R. de Vries, A. Van Tol, andW.J. Sluiter. 2007. Lowerplasma adiponectin is a marker of increased intima-media thicknessassociated with type 2 diabetes mellitus and with male gender.European Journal of Endocrinology 156: 387–394.
37. Singh, P., T.E. Peterson, K.R. Barber, F.S. Kuniyoshi, A. Jensen, M.Hoffmann, A.S. Shamsuzzaman, and V.K. Somers. 2010. Leptinupregulates the expression of plasminogen activator inhibitor-1 inhuman vascular endothelial cells. Biochemical and BiophysicalResearch Communications 392(1): 47–52.
38. Lijnen, H.R. 2005. Pleiotropic functions of plasminogenactivator inhibitor-1. Journal of Thrombosis and Haemostasis3(1): 35–45.
39. Scotece, M., J. Conde, R. Gómez, V. López, J. Pino, A. González, F.Lago, J.J. Gómez-Reino, and O. Gualillo. 2012. Role of adipokinesin atherosclerosis: interferences with cardiovascular complicationsin rheumatic diseases. Mediators of Inflammation 125458.
43Hyperleptinemia, inflammation, and vascular protection in obesity










![Let's Move [Read-Only] - WV Early Childhood · Childhood Obesity Facts • 17% or 12.7 million children and adolescents aged 2-19 years are obese in the United States • Obesity](https://img.pdfslide.us/doc/110x75/601e3ade4f60ba26054b8417/lets-move-read-only-wv-early-childhood-obesity-facts-a-17-or-127-million.jpg)

















