Embed Size (px)
Citation preview

Hyperkalemia
Muhamed Al Rohani, MDConsultant nephrologist
Asoc. Professor, UST and USTHIn-charge of nephrology deviation in Dibba hospital

Case Study:A 72-year-old man presents to his family physician for follow-up of hypertension, reporting fatigue and generalized weakness.
Medical history: peptic ulcer disease,
type 2 diabetes mellitus
chronic kidney disease. eGFR is 30 mL/min / 1.73 m2. Medications: metformin, lansoprazole, acetylsalicylic acid, hydrochlorothiazide and ramipril, 2 weeks earlier its dose was increased.
Lab. Work: s. K level is 6.7 mmol/L from a nonhemolyzed sample. He was referred ED urgently. The patient is hemodynamically stable, with BP 124/70 mm Hg, HR 80 beats/min (regular).
Repeat testing shows a. s. K level of 6.9 mmol/L, and ECG shows sinus rhythm with peaked T waves, prolonged PR interval (240 milliseconds) and a narrow QRS interval.
This patient requires urgent treatment of hyperkalemia. What therapeutic options are available, and what is the evidence supporting their use?

Definition• Normal levels: 3.5 – 5.0 mmol/L. • Prevalence in general population 2 – 3% • The prevalence in advanced CKD (eGFR < 15) 40 – 50% of pts, as
results of compensation failure • Hyperkalemia = plasma K+ concentration > 5.0mmol/L
5.5-6.0 mEq/L – Mild 6.1-7.0 mEq/L – Moderate ≥7.0 mEq/L – Severe

Hyperkalemia as a clinical challenge:
Patients with HF, CKD, DM-DNUse od RAASi cardio-renal protection
Limitation of use and titration for maximal benefits Use of K-spiring agents Limited tools to manage the hyperkalemia
Diet (compliance of patient)Sodium polystyrene sulfonate (colon necrosis, taste)Loop diuretics
Increase in hospital admission


Causes of Hyperkalemia:Potassium excessive cellular release from cells or transcellular shifts:
• DM or hyperglycemia. Hyporeninemic hypoaldostronism • Increase in take meanly in renal failure • Intravascular hemolysis• Tumor Lysis Syndrome• Rhabdomyolysis• Non-gap metabolic acidosis• Severe Digitalis toxicity
Decreased renal loss: • Renal failure• Decreased K+ secretionImpaired Na+ reabsorptionadrenal insufficiency (Addison dis)hyporeninemic hypoaldosteronismdrugs: ACEi, NSAIDS, heparin, K+-sparing diuretics, BB and others
distal type 4 RTAEnhanced Cl- reabsorptionCyclosporineGordon’s syndrome

Causes Pseudohyperkalemia Movement of K out of cells during or after blood
drawingHemolysis Fist clenching (local exercise effect)Leukocytosis WBC > 70,000Thrombocytosis Platelets > 1000,000Increase RBC fragility
Hereditary spherocytosis: RBC membrane abnormality
Acanthocytosis Dx: plasma (unclotted) vs. serum (clotted)

Drugs known to induce hyperkalemia Drug – inducing transmembrane K movement
Non selective BBDigoxin intoxicationIntravenous catonic amino acids Mannitol Suxamethonium
Decrease Na/K-ATPase pump activity and renin releaseInhibition of Na/K ATPase pumpIncrease in EC K shiftsHyperosmolality with increase of EC K shifts Prolonged depolarization of cell membrane
Drugs that affect aldosterone secretionACE inhibitors
ARBsDirect renin inhibitors NSAIDs and COX-2 inhibitorsCalcineurin inhibitors
Blockade of Ang II synthesis / decrease aldosterone secretion Impaired delivery of Na to the distal nephronDecrease aldosterone formation in RAAS Decrease aldosterone formation in RAAS Decrease of PG-mediated renin release, renal BF, and GFRDecrease aldosterone synthesis and Na/K-ATPase pump activity
Drugs cause tubular resistance to aldosterone:Aldosterone antagonistsK-sparing diuretics Trimethoprim, pentamidine
Blockage of mineralcorticoid receptors Blockade of luminal Na channels Blockade of luminal Na channels
K-containing agents Salt-substitutes Penicillin G, stored blood products
K sources

Co-existing diseases affecting the level of PotassiumDietary modifications for CKD:
Increase dietary K intakeHerbal supplements (alfalfa, noni, dandelion)K-rich heart healthy diets
Metabolic acidosis:Shifting K from intracellular to extracellular compartment
Anemia requiring blood transfusionKidney transplantation:
Calcineurin inhibitorsRenal tubular acidosis
AKI:Rapid decline in GFR Catabolic status
Diabetes Mellitus Hyperglycemia shifting water from the cellsHyporeninemic hypoaldostronism unable in tubular K secretion
Cardiovascular disease:Requiring drugs contribute to hyperkalemia
Advanced stages of heart failure Drop in renal perfusion

Clinical Presentation:
Level > 7 mmol/L significant hemodynamic neurologic consequences.
Level exceeding 8.5 mmol/L respiratory paralysis or cardiac arrest or sudden death
Symptoms:Asymptomatic, nonspecific Weakness fatigueNausea and vomiting Paresthesia (tingling or pricking)Frank muscle paralysis or SOB Palpitation or chest pain

Figure 1
Kidney International Supplements 2016 6, 16-19DOI: (10.1016/j.kisu.2016.01.003) Copyright © 2016 International Society of Nephrology Terms and Conditions

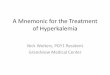
The ECG change related to Potassium level
Early ECG changes: At a S.K level of 5.5-6.5 mEq/L, includes:
Tall, peaked T waves with a narrow base, best seen in precordial leads
Shortened QT interval ST-segment depression
At level of 6.5-8.0 mEq/L:Peaked T waves Prolonged PR interval Decreased or disappearing P wave Widening of the QRS Amplified R wave
At level > 8.0 mEq/L :Absence of P wave Progressive QRS widening Intraventricular/fascicular/bundle branch blocks
The progressively widened QRS eventually merges with the T wave, forming a sine wave pattern. Ventricular fibrillation or asystole follows.

Electrocardiogram demonstrating severe hyperkalemia on admission before treatment.

Arrhythmias in patients with severe hyperkalaemia illustrating bradycardia with wide QRS [K+ 9.6 mmol/L] (a), sine wave with pause [K+ 9.3 mmol/L] (b) and sine wave without pause [K+ 8.4 mmol/L] (c) and ventricular tachycardia [K+ 9.1 mmol/L] (d). - See more at: http://www.renal.org/guidelines/joint-guidelines/treatment-of-acute-hyperkalaemia-in-adults#Figure01

Electrocardiogram after correction of the hyperkalemia.
Taha Ayach et al. Clin Kidney J 2014;7:49-52
© The Author 2013. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. For permissions, please email: [email protected].

• Differential Diagnoses Acute Tubular Necrosis Congenital Adrenal Hyperp
lasia Digitalis Toxicity Electrical Burn Injuries Head Trauma Hypocalcemia Metabolic Acidosis Rhabdomyolysis Thermal Burns Tumor Lysis Syndrome
Diagnosis: ECG monitoring s. K already you haveAdd dialysis renal profile and CBCs. Glucose s. Ca, s, PhosUrinary K, Na and osmolality
If urine K above 40 mEq/L suggests intact renal excretory mechanisms, implying that high intake or failure of cell uptake.
level below 20 mEq/L suggests impaired renal excretion
ABG CK, urine myoglobin Estimation of GFR

KEY RECOMMENDATIONS FOR PRACTICE AFP
Clinical recommendationEvidence rating
Patients with hyperkalemia who have electrocardiographic (ECG) changes, a rapid rate of rise of serum potassium, decreased renal function, or significant acidosis should be urgently treated.
C
Patients with hyperkalemia and characteristic ECG changes should be given intravenous calcium gluconate.
C
Acutely lower potassium by giving intravenous insulin with glucose, a beta2 agonist by nebulizer, or both.
C
Total body potassium should usually be lowered with sodium polystyrene sulfonate (Kayexalate).
C

• Calcium chloride: (6.8 mmol),Local cell necrosis • Calcium gluconate (2.26 mmol)• Effect within minutes • Repeat from 5 – 10 min• IV calcium can cause bradycardia, observe in 2nd dose.• Duration of action of IV Ca 30-60 min concern in prolonged hyperkaliemia
Protect heart
• IV glucose and insulin infusion:• 10 U of regular insulin and 50 mL of dextrose 50% in water. • The onset of action is within 20-30 minutes, • The duration 2 to 6 h.• Close monitoring K and blood sugar 2 hourly (AKI and CKD and insulin) or 6 h in
others and ECG monitoring • Salbutamol: reduce s. K level by 0.5-1.5 mEq/L. • beneficial in patients with renal failure or fluid overload. • action is 30 minutes; • duration of action is 4-6 h• Sodium Bicarbonate: when there is acidosis
Shifting K into IC compartment
• Loop diuretics • Furosemide • Bumetanide • Sodium Polystyrene Sulfonate action after 2 – 6 h.
Remove Potassium from body

Treatment Mechanism Time to onset of action Duration of action
Calcium Gluconate Antagonises cardiac membrane excitability
Immediate 5 min
Insulin Actrapid with glucose
Increase IC uptake pf K via Na – K ATP pump
Within 15 min 60 min
Nebulised Salbutamol Increase IC uptake of K via Na-k ATP pump
Variable 30 – 90 min 1 – 3 h
Sodium Bicarbonate Promotes IC uptake of K by correcting acidosis
After 60 min Unknown
Calcium Resonium Exchange Na for K in the intestine 2 – 6 h Unknown
Treatment of acute hyperkalemia ( Nottingham university hospitals)

Medication Dosage Onset Length of effect Mechanism of action CautionsCalcium gluconate 10 to 20 mL of 10%
solution IV over 2-3 min
Immediate 30 minutes Protects myocardium from toxic effects of calcium.
Can worsen digoxin toxicity
Insulin Regular insulin 10 u. IV with 50 mL of 50% glucose
15 to 30 minutes
2-6 hours Shifts s. K out of the vascular space and into the cells;
Consider 5% D at 100 mL/h to prevent hypoglycemia
Albuterol (Ventolin)Nebulized
10 to 20 mg over 10 min.
15 to 30 minutes
2-3 hours Shifts s. K into the cells, May cause a brief initial rise in serum potassium
Furosemide (Lasix) 20 to 40 mg IV, 15 minutes to one hour
4 hours Increases renal excretion of potassium
Only effective if adequate renal response to loop diuretic
Sodium polystyrene sulfonate (Kayexalate)
Oral: 50 g in 30 mL of sorbitol solution Rectal: 50 g in a retention enema
1-2 h (rectal route is faster)
4 – 6 hours Removes potassium from the gut in exchange for sodium
bowel necrosis. sodium retention
Medications Used in Acute Treatment of Hyperkalemia by AFP

Figure 1
Kidney International 2016 89, 546-554DOI: (10.1016/j.kint.2015.11.018)
To regimens of insulin in therapy of hyperkalemiaRisk of hyperglycemia after an hours Adding 50% Dextrose.

Figure 3
Kidney International 2016 89, 546-554DOI: (10.1016/j.kint.2015.11.018)
Plasma potassium concentration during and after dialysis.Modified, with permission, from Figure 3 in Blumberg A, Roser HW, Zehnder C, Muller-Brand J. Plasma potassium in patients with terminal
renal failure during and after haemodialysis; relationship with dialytic potassium removal and total body potassium. Nephrol Dial Transplant. 1997;12:1629–1634.93
Hemodialysis effect on levels of Potassium Pre and Post dialysis

Chronic Management
Avoid: NSAIDs including COX-2 inhibitors Herbal remedies K containing salt
Prescribe: Low K diet Thiazide or loop diuretics
Correct metabolic acidosis Start low dose ACEi or ARBs
Sodium polystyrene sulfonate (Kayexalate) Oral and rectal Colonic necrosis
eGFR: < 30 mL/min/1.73m2Impaired renal secretion and excretionHyporeninemic hypoaldostronic (RTA) AKICKD late stages
Close monitoring of s. K
Management of chronic Hyperkalemia



Proposals for standardized management1. No treatment, other than kayexalate, for K 5.1 – 6 unless medical condition strongly
predicts the value will continue to increase. Examples: acute oliguric renal failure, tumor lysis syndrome. Do repeat and f/u on potassium level.
2. Policy that for any K+ > 6.0, order ECG. Consider stat repeat K+ if concern pseudohyperkalemia
3. For persistent K+ > 5.1, order telemetry4. Policy if K+ <6.5 and no ECG changes present, treat with kayexalate and repeat K+ level
and ECG in 4-6 hours. No need other interventions.5. Policy if K+ < 6.5 and ECG changes present, administer CaGluconate, Insulin/Glucose,
Nebulizer Rx, and Kayexalate. Consider consult ICU team.6. Policy if K+ > 6.4, regardless of presence of ECG changes, administer CaGluc,
Insulin/Glucose, Nebulizer Rx, and Kayexalate. Repeat ECG and K+ level in 1 hour. Consider consult ICU team.


















![Treatment of Hyperkalemia [Read-Only]](https://img.pdfslide.us/doc/110x75/62e53ff26c7a3007180b6201/treatment-of-hyperkalemia-read-only.jpg)








