Embed Size (px)
Citation preview

Hyperbaric Oxygen Therapy &
Oxygen Toxicity
Module IIICRC 431
Special Procedures
HBO OUTLINE
• Definitions• History• Altitude/descent• Gas laws• Physiological effects of HBO
Hyperbaric Oxygen Therapy
• Therapeutic oxygen at pressures greater than 1 atm
• Unit expressing HBO pressure = ata• Ata = atmospheric pressure absolute• 1 ata = 1 atmosphere (atm), or 760
mm Hg• HBO general pressure range = 2 to 3
ata

Hyperbaric Oxygen Therapy
• Pressure:Pressure = Force/Area
• Force:Force = mass x
acceleration
Remember: MIP, not NIF!!!

Hyperbaric Oxygen Therapy
• Ambient pressure = surrounding pressure on land, or under water.
• Atmospheric pressure = surrounding pressure caused by the weight of air.
• Water pressure = surrounding pressure caused by weight of water.

Hyperbaric Oxygen Therapy
• Barometric pressure = measure of atmospheric pressure
• Barometric pressure = atmospheric pressure
• When one is surrounded by air: atmospheric pressure = ambient pressure = barometric pressure
Hyperbaric Oxygen Therapy
• Absolute pressure: referenced against a perfect vacuum:
gauge pressure + atmospheric pressure.• Gauge pressure: referenced against
ambient air pressure: absolute pressure - atmospheric
pressure
Hyperbaric Oxygen Therapy
• When surrounded by water: ambient pressure = water
pressure
• CAUTION!!! Don’t confuse: atmospheric pressure & “atmosphere” (atm) used as a unit.

Hyperbaric Oxygen Therapy
• Atmospheric pressure can be ANY value:1 atm (sea level); 760 mm Hg½ atm (8,000 ft elevation); 380 mm Hg3 atm (hyperbaric chamber); 2,280 mm Hg
Hyperbaric Oxygen Therapy
ABSOLUTE PRESSURE vs. GAUGE PRESSURE
• 33 ft sea water = 1 atm• Gauges set sea level pressure at 0 mm
Hg• At 33 ft depth, gauge indicates 1 atm• Absolute pressure = 2 atm
Hyperbaric Oxygen Therapy
• First sealed chamber called Domicilium built in 1662
• Chamber held compressed air (21% O2)
• Treated various ailments: scurvy, arthritis, inflammation, rickets
• Likely too little compression to benefit patients

Hyperbaric Oxygen Therapy
• Beddoes is known as the “Father of Respiratory Therapy”
• Thomas Beddoes founded the “Pneumatic Institute in Bristol,” England 1780
• Patients inhaled different gases to treat their diseases
• Pneumatic laboratory enriched with O2 treated chronic conditions

Hyperbaric Oxygen Therapy
• J. Priestly discovered O2 in England 1776; called “dephlogisticated air.”
• Antoinne Lavoisier of France shares O2 discovery; named oxygen
• Father of English poet Thomas Lovell Beddoes

Hyperbaric Oxygen Therapy
GAS LAWSAir under hyperbaric conditions obeys
the same gas laws as air at sea level.
Boyle’s law (1627 – 1691)Dalton’s law (1766 – 1844)Henry’s law (1774 – 1790)
Hyperbaric Oxygen Therapy
Boyle’s law
• When mass & T are K, V & P inverse
K = V x P• If P increases, V decreases, & vice
versa

Hyperbaric Oxygen Therapy

Hyperbaric Oxygen Therapy
Boyle’s law
• During HBO, D in lungs increases.• Deep scuba diving: D of air
increases, & breathing becomes more difficult.
Hyperbaric Oxygen Therapy
Dalton’s law
• PT = pressure exerted by gas equals the sum of all the Pgas of the constituent gases.
PT = P1 + P2 + P3 + . . . Pn

Hyperbaric Oxygen Therapy
Dalton’s law To calculate the partial pressure of a gas in
a mixture of gases:Pgas = Fgas (PT – PH2O)
EXAMPLES:150 mm Hg = 0.21(760 mm Hg – 47 mm Hg)160 mm Hg = 0.21(760 mm Hg – 0 mm Hg)
Hyperbaric Oxygen TherapyDalton’s law
TRUE or FALSEThe sum of the partial pressures of all the gases in a gas mixture can never exceed the total pressure of the gas mixture.
? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ?
Hyperbaric Oxygen Therapy
Dalton’s law
TRUE!!!
Hyperbaric Oxygen TherapyDalton’s law
TRUE or FALSEAs air pressure increases (hyperbarism) or decreases (altitude), the partial pressures exerted by the constituent gases increases or decreases, as well.
???????????????????????????????????????
Hyperbaric Oxygen Therapy
Dalton’s law
TRUE!!!
Hyperbaric Oxygen Therapy
Dalton’s law TRUE or FALSE
When room air is compressed in a hyperbaric chamber, the percentage of the individual gases in the mixture is the same.
???????????????????????????????????????

Dalton’s law
TRUE!!!
Hyperbaric Oxygen Therapy
Hyperbaric Oxygen TherapyDalton’s law• Lower partial pressures at altitude reflect
presence of less O2 & N2 molecules per volume compared to sea level.
• Summit at Mt. Everest (29,000 ft): 21% O2, 78% N2, 1% other
• # of O2 & N2 molecules per volume of air only 1/3 that at sea level.
• PO2 & PN2 only 1/3 that at sea level
Hyperbaric Oxygen Therapy
Henry’s lawAmount of gas that dissolves in a liquid at a given temperature is a function of the partial pressure of the gas in contact with the liquid, and the solubility of the gas in that particular liquid.
Hyperbaric Oxygen Therapy
Henry’s law
SIMPLIFIED: As the partial pressure of a gas above the surface of a liquid increases, more of that gas will dissolve into that liquid.

Hyperbaric Oxygen Therapy
Henry’s & Dalton’s laws
When ambient pressure decreases (altitude), the partial pressures of O2 & N2 in the body fall, and fewer O2 & N2 molecules dissolve into the blood.

Hyperbaric Oxygen Therapy
Henry’s & Dalton’s laws
When ambient pressure increases (hyperbarism), the partial pressures of O2 & N2 in the body increase, and more O2 & N2 molecules dissolve into the plasma.

Hyperbaric Oxygen Therapy
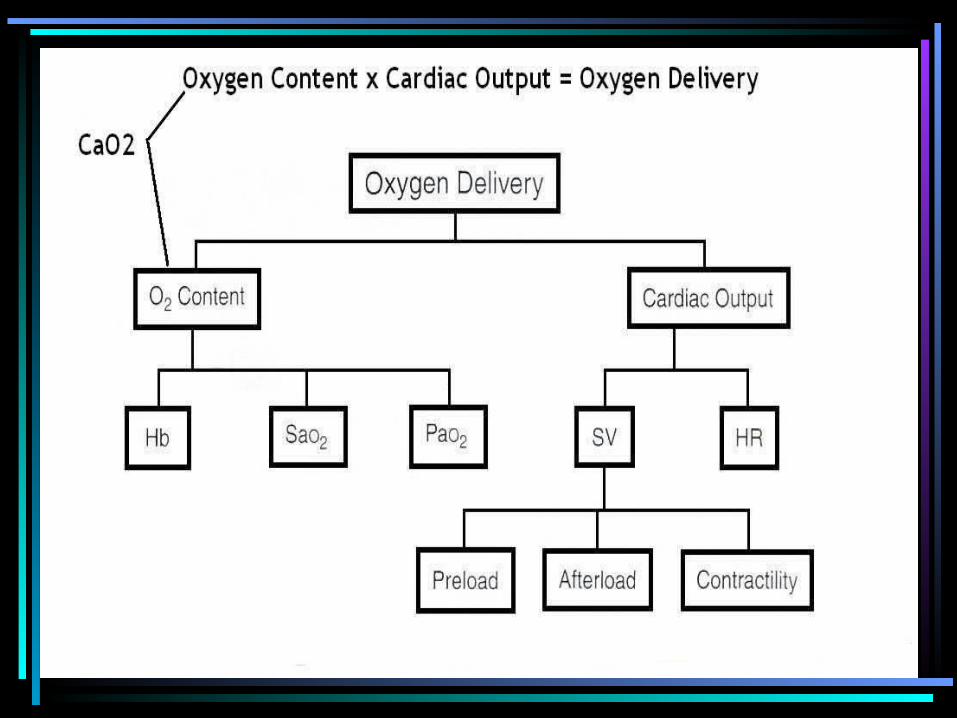
Physiological Effects• Hyperoxygenation
– Increases volume of O2 in plasma
– 10 to 13 x greater than normal
– Elevated O2 levels purge toxins & CO from the body

Hyperbaric Oxygen Therapy
Physiological Effects• Hyperoxygenation
– At sea level while breathing room air plasma O2 concentration is 0.3 vol%
100 mm Hg x 0.003 vol%/mm Hg = 0.3 vol%
Hyperbaric Oxygen Therapy
Physiological Effects• HyperoxygenationAlveolar Air Equation:
PAO2 = FIO2(PB – PH2O) – PaCO2 (FIO2 + [1.00 – FIO2 ÷ R])

Hyperbaric Oxygen Therapy
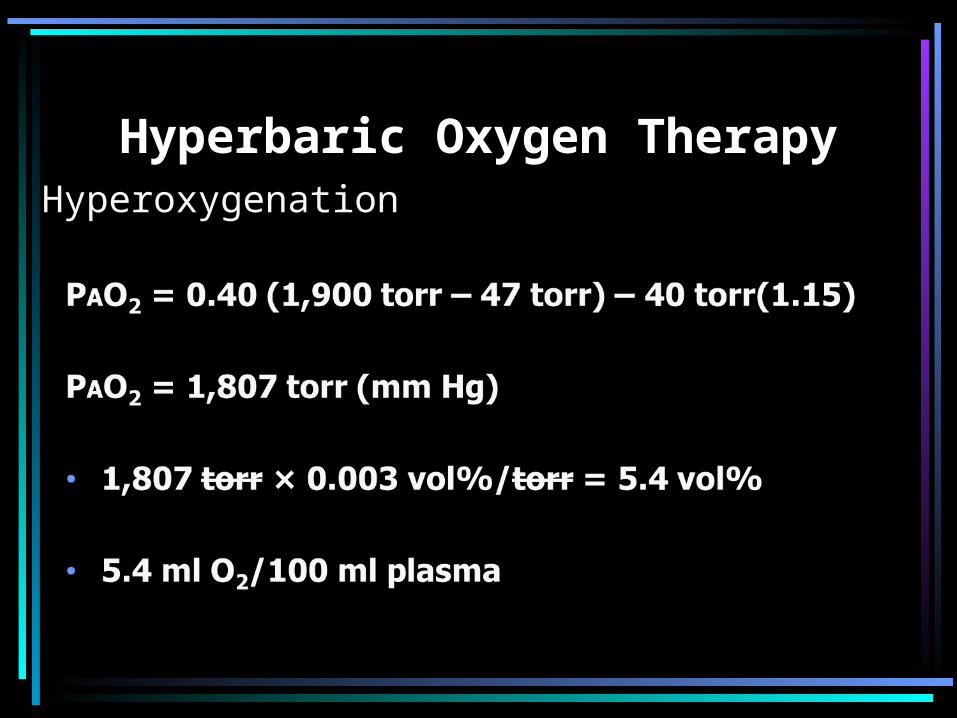
Physiological Effects• Hyperoxygenation
HBO patient breathing FIO2 0.40 @ 2.5 atm
PAO2 = 0.40(1,900 mm Hg – 47 mm Hg) –
40 mm Hg(0.40+ [1.00 + 0.40/0.8])
Hyperbaric Oxygen TherapyHyperoxygenation

Hyperbaric Oxygen Therapy
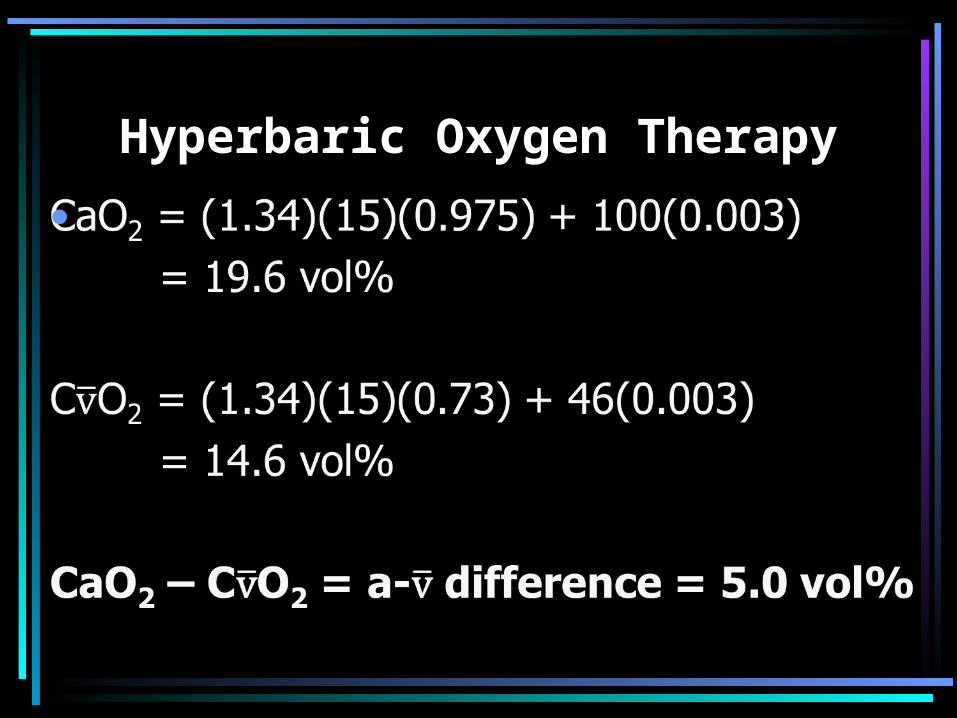
Normal a-v difference = 5.0 vol%
Arterial Blood
PaO2 100 mm Hg SaO2 97.5%
[Hb] 15 g%
Hyperbaric Oxygen Therapy
Hyperbaric Oxygen Therapy
Physiological Effects• Hyperoxygenation
– HBO increases dissolved oxygen in the plasma

Hyperbaric Oxygen Therapy
Physiological Effects• Direct Pressure
– Shrinks gas bubbles (Boyle’s law) to expedite reabsorption of gases
– Good for decompression sickness (DCS – aka: “the bends”)
– Good for air/gas embolism

Hyperbaric Oxygen Therapy
Physiological Effects• Vasoconstriction
– Reduces blood flow
– No significant reduction in tissue O2nation
– Benefits crushing type injuries– Benefits thermal burns
– O2 directly enters interstitial fluid promoting healing
Hyperbaric Oxygen Therapy
Physiological Effects• Bactericidal/Bacteriostatic
– Halts spread of toxins– Enhances killing of bacteria– Stimulates production of neutrophils
Hyperbaric Oxygen Therapy
Physiological Effects• Angiogenesis/Neovascularization
– Promote growth of new blood vessels– Promote collagen formation to
support new blood vessels
Hyperbaric Oxygen Therapy
• Atmospheric pressure caused by weight of gas molecules in contact with earth’s surface
• Atmospheric pressure exerted on a surface of water
• Pressure decreases with altitude• Denver, CO at 5,280 ft elevation; 1 atm = 630 mm Hg
Hyperbaric Oxygen Therapy• Water more dense than air• 33 ft sea water = 1 atm (760 torr)• Pressure at any depth = hydrostatic
pressures + atm pressure• Depth of 33 ft of H2O = 2 atm, or 2 ata• At 33 ft H2O, 2,112 lbs over each ft2 of
body (33 ft x 64 lbs/ft3 = 2,112 lbs/ft2)• 66 ft H2O = 3 ata
Hyperbaric Oxygen Therapy
• Indications – CHRONIC– Nonhealing wounds– Refractory osteomyelitis– Radiation necrosis
www.uhms.org/indications/indications.htm
Hyperbaric Oxygen Therapy
• Hazards– Fire: 50 deaths worldwide in 20 years
(1997)• Most common FATAL complication• Only 100% cotton fabrics in chambers• No alcohol/petroleum products• No sprays, makeup, deodorant
– Barotrauma• Ear/sinus trauma• Tympanic membrane rupture• pneumothorax

Hyperbaric Oxygen Therapy
• Hazards– O2 Toxicity
•CNS toxicity (twitching, seizures, convulsions)
•Pulmonary toxicity (leaky A/C membrane)
– Other•Sudden decompression•Reversible visual changes•Claustrophobia
Hyperbaric Oxygen Therapy
• Hyperbaric Chambers– Monoplace transparent Plexiglas
cylinder– One patient– No mask– No electric equipment inside– 100% oxygen– Less expensive than multi-place

Hyperbaric Oxygen Therapy
Hyperbaric Oxygen Therapy
Hyperbaric Oxygen Therapy
multiplacehyperchamber.jpg
• Multi-place chambers– large tanks able to accommodate 2 – 14
people– achieve pressures up to 6 atm– have a chamber lock entry system that allows
medical personnel to pass through without altering the pressure of the inner chamber
– allows patients to be directly cared for by staff– filled with compressed air; patients breathe
100% oxygen through facemask, head hood, or endotracheal tube.

Hyperbaric Oxygen Therapy
img_header.jpg
multiplacehyperchamber.jpg
Hyperbaric Oxygen Therapy
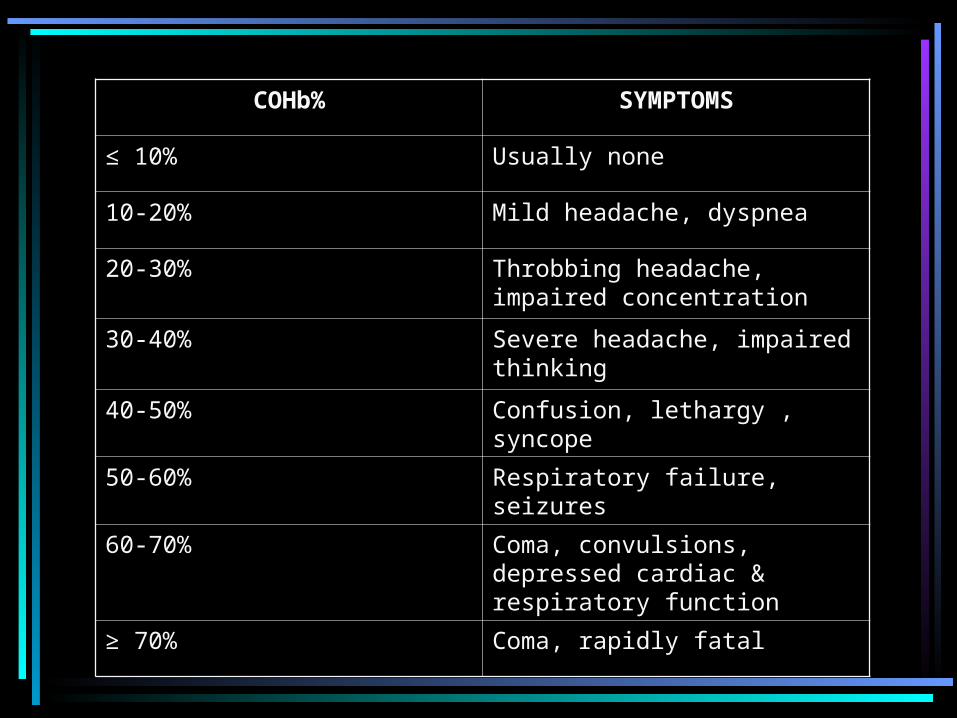
COHb% SYMPTOMS
≤ 10% Usually none
10-20% Mild headache, dyspnea
20-30% Throbbing headache, impaired concentration
30-40% Severe headache, impaired thinking
40-50% Confusion, lethargy , syncope
50-60% Respiratory failure, seizures
60-70% Coma, convulsions, depressed cardiac & respiratory function
≥ 70% Coma, rapidly fatal
Oxygen Toxicity
Oxygen Toxicity
Joseph Priestley said in 1775, “. . . it [oxygen] might be peculiarly
salutary to the lungs in certain morbid cases . . .” and “. . . oxygen might burn the candle of life too quickly, and too soon exhaust the animal powers within. . . .”
Oxygen Toxicity
• Present overview of biochemical processes involved in normal cellular utilization of oxygen.
• Discuss implications of the processes in the context of hyperoxia.
• Explain biochemical role of antioxidants.• Describe the pathophysiological aspects
of pulmonary oxygen toxicity.
Oxygen Toxicity
• Oxidation: loss of electrons
• Reduction: gain of electrons
• Dismutation: same molecular species is oxidized and reduced, and two different products (species) are formed.
Oxidatione–, e–, e–
e–, e–, e–, e–, e–, e–
Reductione–, e–, e–
Dismutation
Oxidatione–, e–, e–
e–, e–, e–, e–, e–, e–
e–, e–, e–
Reduction
Loss of electrons Gain of electrons
Leo the lion goes gerrr!
Oxygen Toxicity
• Atmosphere• Lungs• A-C membrane
• Dissolved in plasma as PaO2 (Henry’s law of Solubility)
• Chemically & reversibly bound to Hb• Mitochondria & electron transport
chain
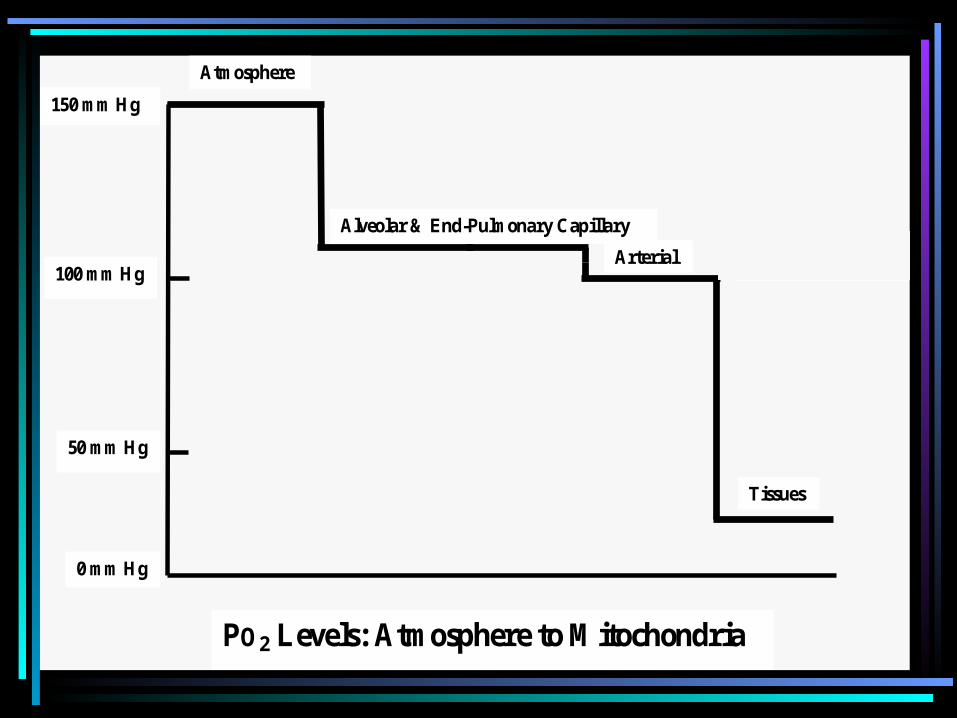
Atmosphere
Alveolar & End-Pulmonary Capillary Diffusion Gradient Arterial
Tissues
150 mm Hg
100 mm Hg
50 mm Hg
0 mm Hg
PO2 Levels: Atmosphere to Mitochondria
Oxygen Toxicity
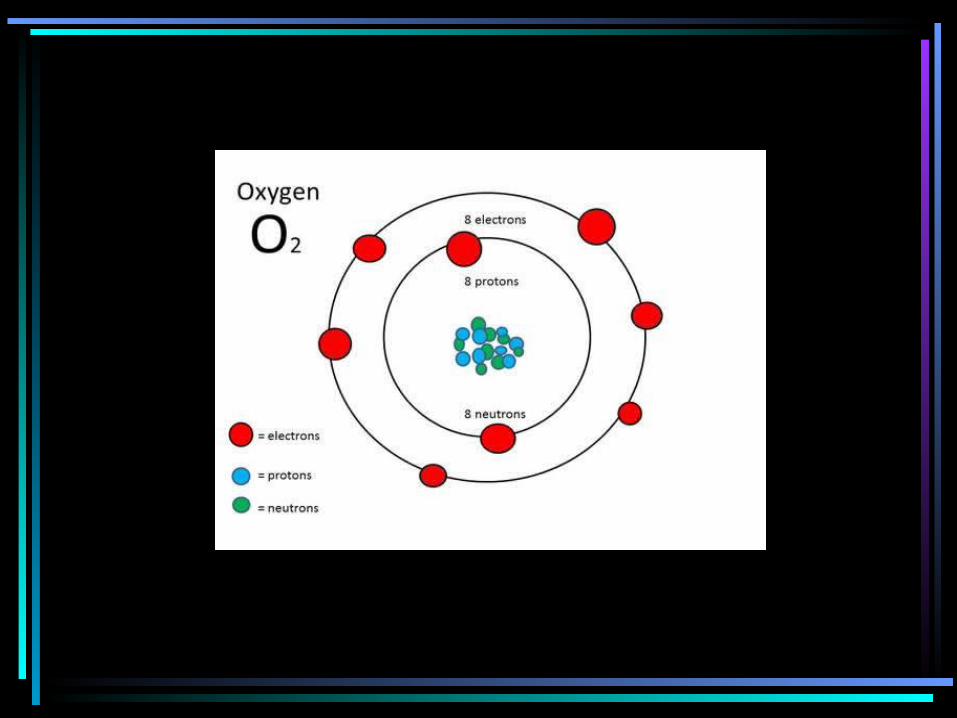
• Oxygen atom– 8 electrons (e-)– 2 e- in 1s orbital– 2 e- in 2s orbital
– 4 e- in 2p orbitals (px, py, pz)• 2 e- are paired • 2 e- are unpaired spin in same direction
causing paramagnetism
e

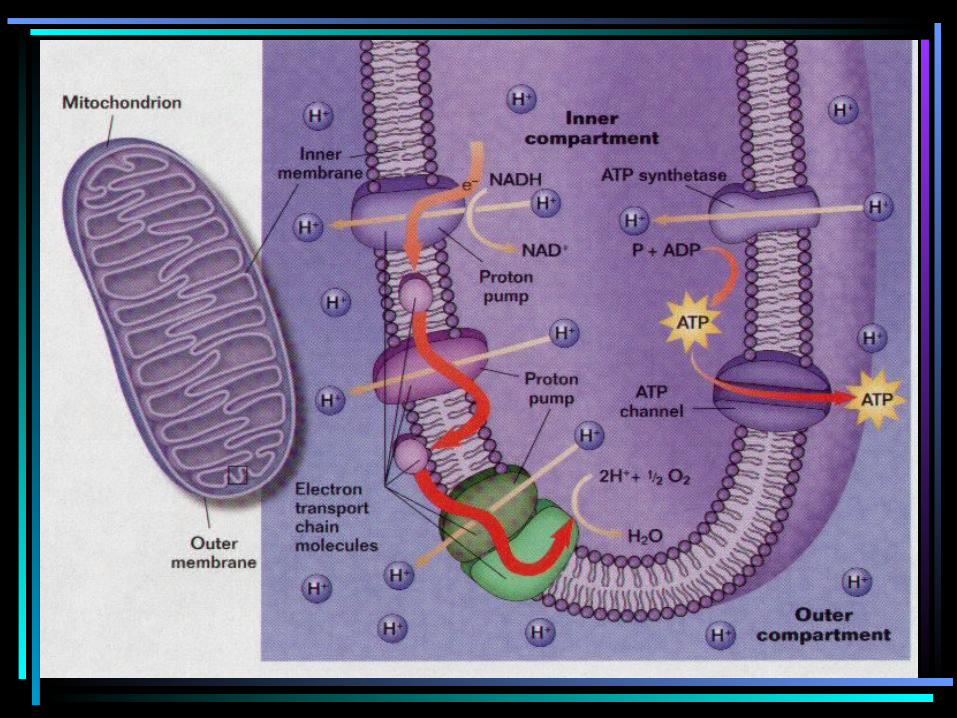
Mitochondrion
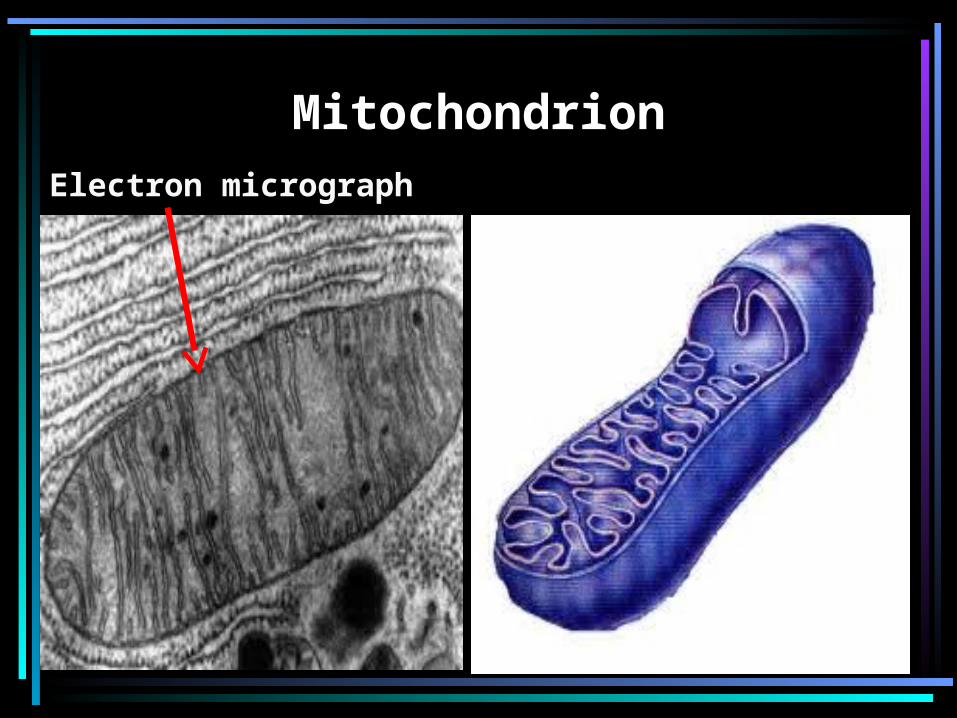
MitochondrionElectron micrograph
Electron Transport Chain• http://www.youtube.com/watch?
v=xbJ0nbzt5Kw&feature=related• http://www.youtube.com/watch?
v=ajZajFrCjtA&feature=related• http://www.youtube.com/watch?
v=RvqR4pExHX8&feature=related• http://www.youtube.com/watch?
v=eizHVQfeMwo&feature=related• http://www.youtube.com/watch?
v=XI8m6o0gXDY
• Single electron transfers occurs 4 times/O2 molecule)
• O2 undergoes 4 separate univalent reductions
• 1 e- at a time added to O2
• O2 gains 1 e- at a time
• Reduction of O2 molecule = 2 H2O
Mitochondrion: Electron Transport Chain
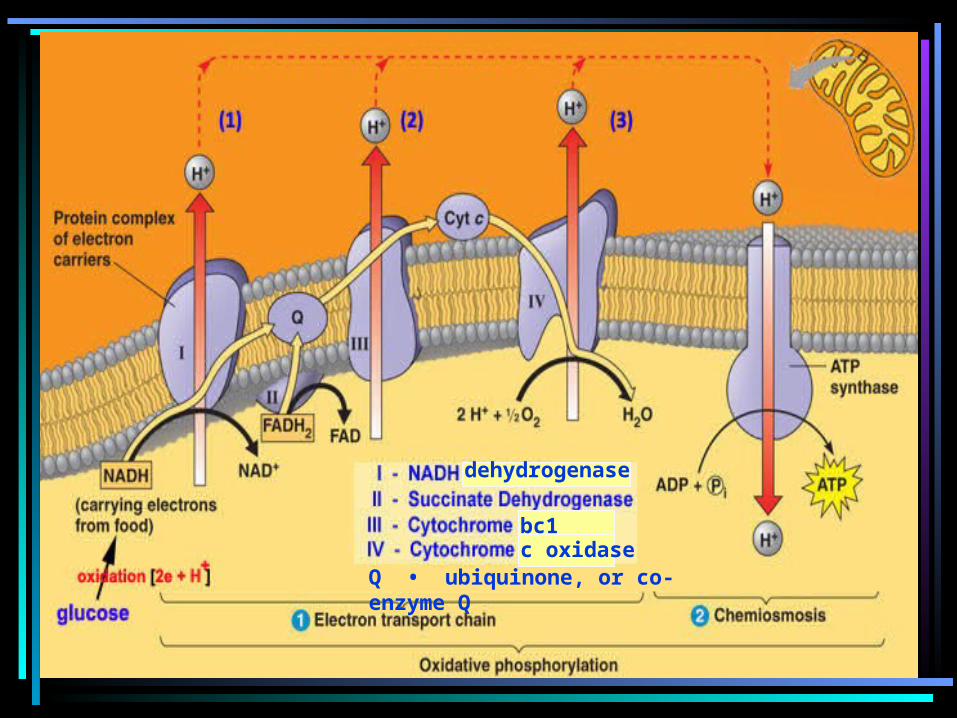
bc1c oxidase
Q • ubiquinone, or co-enzyme Q
dehydrogenase

Mitochondrion: Electron Transport Chain
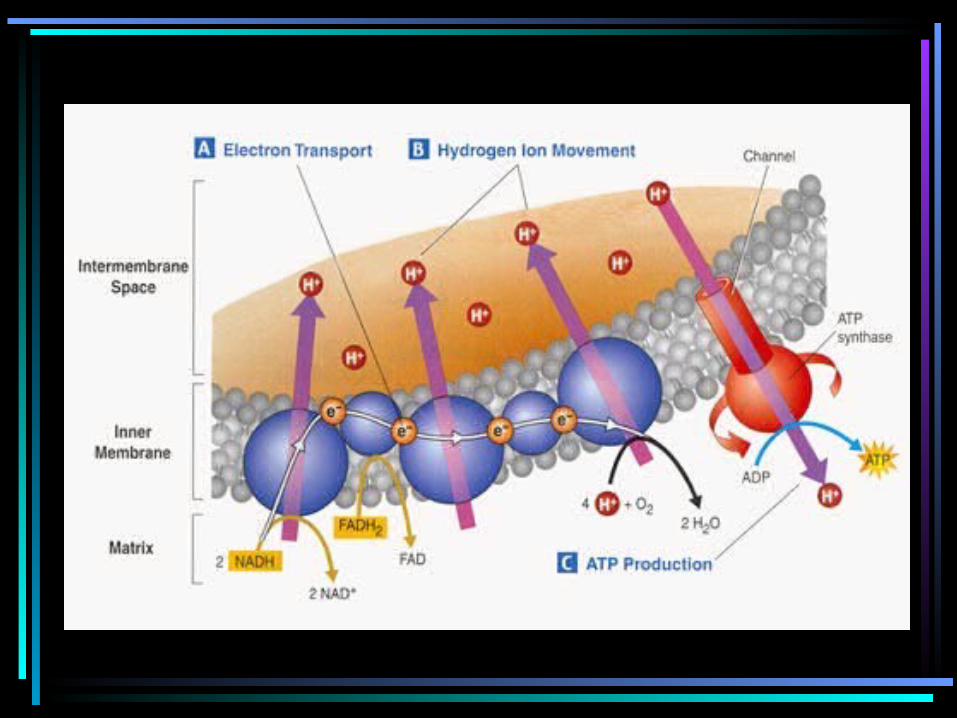
• e- brought to ETC from Kreb’s Cycleby electron carriers– NADH
– FADH2
– http://bcs.whfreeman.com/thelifewire/content/chp07/0702001.html
• Overall reaction:O2 + 4H+ + 4e- 2 H2O

Cytotoxic Metabolites of Oxygen
• O-2• (superoxide anion)
• H2O2 (hydrogen peroxide)
• OH• (hydroxyl radical)
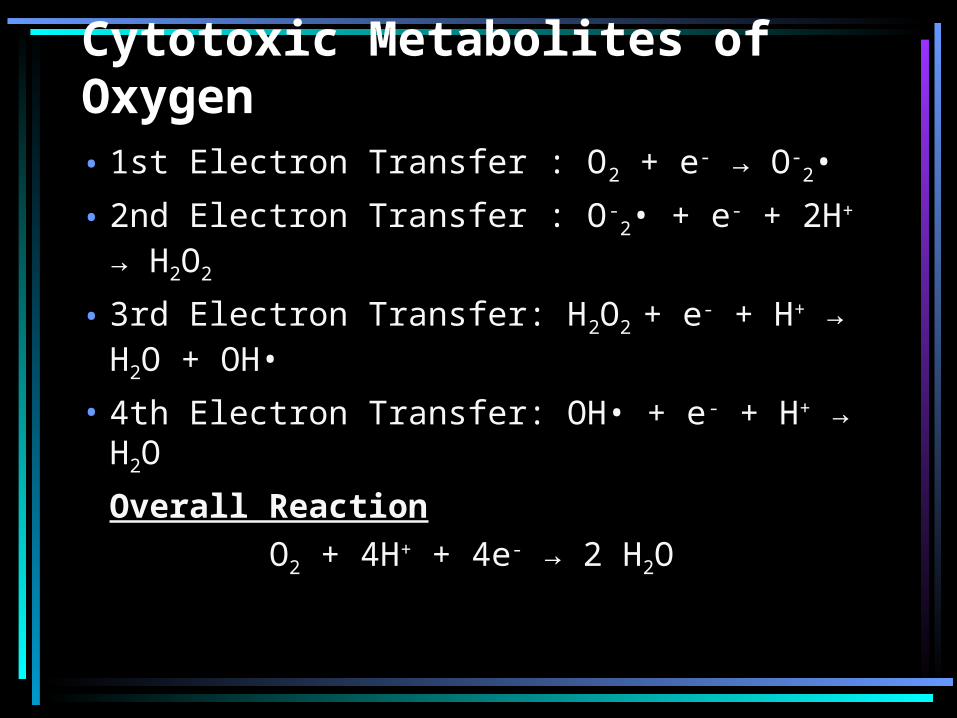
Cytotoxic Metabolites of Oxygen• 1st Electron Transfer : O2 + e- → O-
2•
• 2nd Electron Transfer : O-2• + e- + 2H+ →
H2O2
• 3rd Electron Transfer: H2O2 + e- + H+ → H2O + OH•
• 4th Electron Transfer: OH• + e- + H+ → H2O
Overall Reaction O2 + 4H+ + 4e- → 2 H2O
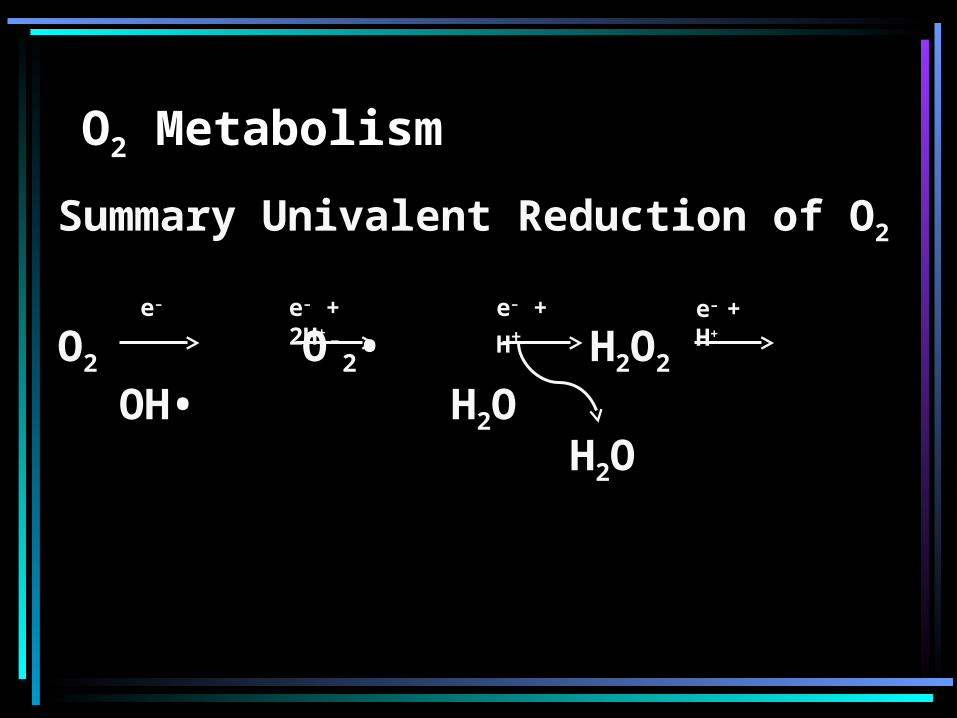
O2 Metabolism
Summary Univalent Reduction of O2
O2 O-2• H2O2 OH• H2O
e– e– + 2H+e– + H+ e– + H+
H2O
Free Radicals
• form during chemical RXN between atoms when one product contains unpaired electron in outermost shell
• extremely unstable state• highly reactive with other
molecules to achieve stable state• ROS includes free radicals
Free Radicals
• During oxygen metabolism, natural by-products often possess unpaired valence shell electrons
• O12• (singlet O2) and OH• contain
unpaired electrons in their outermost shells
• highly unstable, reactive, & can be cytotoxic
Endogenous Antioxidant Defense Mechanisms • ROS & free radicals can
compromise the integrity of cell membranes
• cytotoxic effects of ROS & free radicals can occur
• Normally, they do not • Aging?
Endogenous Antioxidant Defense Mechanisms • Counteract potentially harmful
effects of the oxygen metabolites generated during aerobic respiration
• ROS & free radicals cytotoxic– Large quantities– Defense mechanisms
lacking/compromised
Endogenous Antioxidant Defense Mechanisms
• Oxidative stress• Double-edged sword
– Essential for life: PMNs– Potentially lethal & damaging: amount
• PMNs release O-2• & proteolytic enzymes
to wage war with invading microbes• Destroy cell wall of microbes• Antioxidant defense mechanisms
protective

Oxidative Damage
Destruction of Normal Tissue• Immunocompromised (e.g., AIDS)• Frequent pulmonary infections
(e.g., CF, COPD)• Granulomatous disease (e.g., CGD)
Enyzymatic Antioxidant Defense Mechanisms
• Superoxide dismutase (SOD): breaks down 2 O-
2• species to H2O2 & O2
• Catalase: breaks down H2O2 to H2O & O2
• Glutathione peroxidase: breaks down H2O2 to H2O & R-OHs
Non-Enyzymatic Antioxidant Defense Mechanisms
• Vitamin E (alpha tocopherol): membrane-bound & stops free radical reactions
• Vitamin C (ascorbic acid): membrane-bound & stops free radical reactions
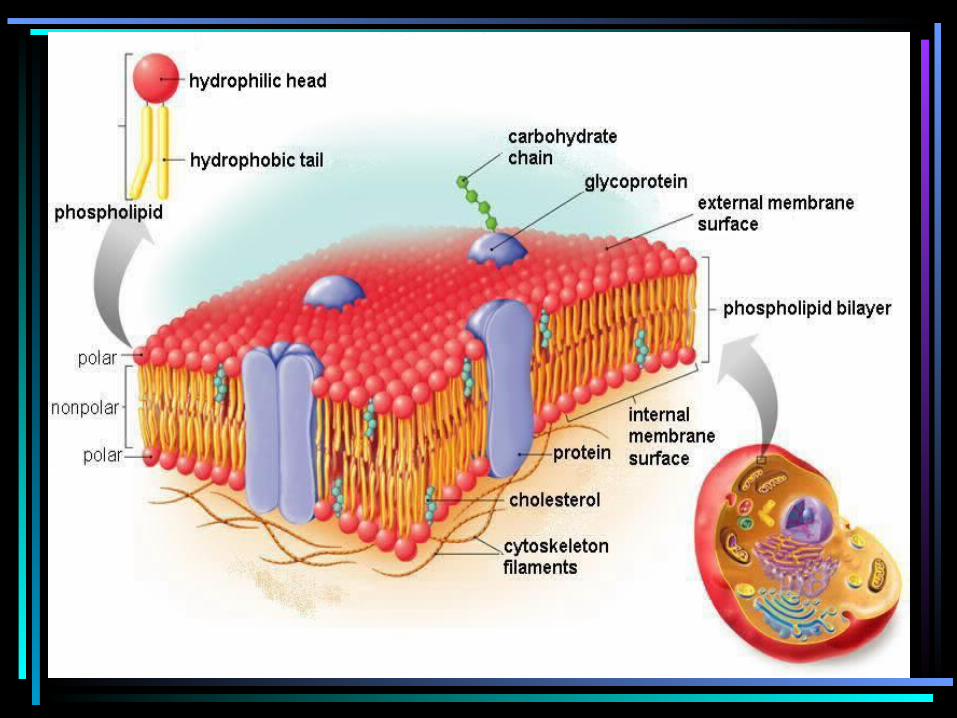
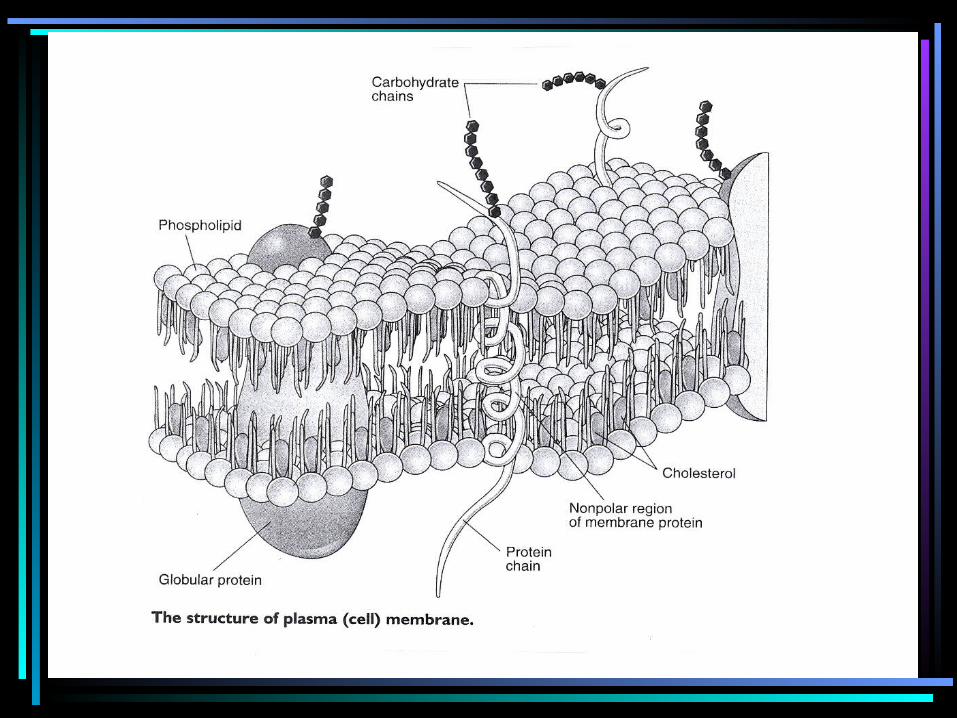
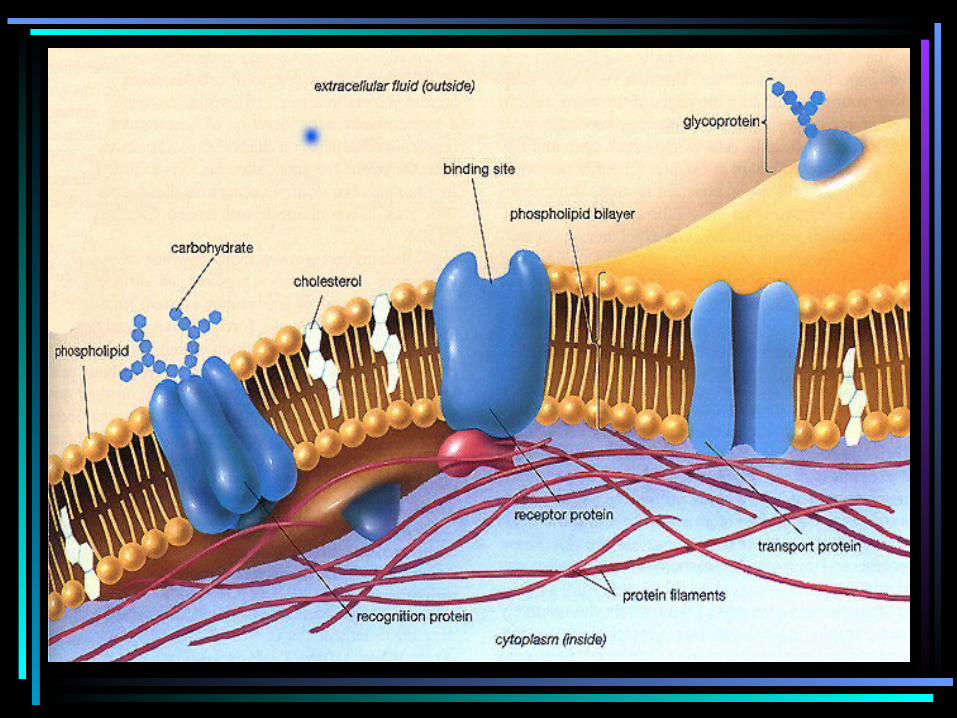
Pulmonary O2 Toxicity
• Disruption of A/C membrane: unsaturated fatty acids along phospholipid bilayer are targets
• Exudation of fluid• Alveolar fibrosis
Animations & Information• http://plantandsoil.unl.edu/
croptechnology2005/pages/animationOut.cgi?anim_name=lipid_peroxidation.swf
• http://www.medmotion.com/html/hydroxyl.html
• http://www.cyberlipid.org/perox/oxid0002.htm#3
• http://www.youtube.com/watch?v=GItnvCzV618