Embed Size (px)
Citation preview
8/13/2019 Hydrosalpinx
http://slidepdf.com/reader/full/hydrosalpinx 1/3
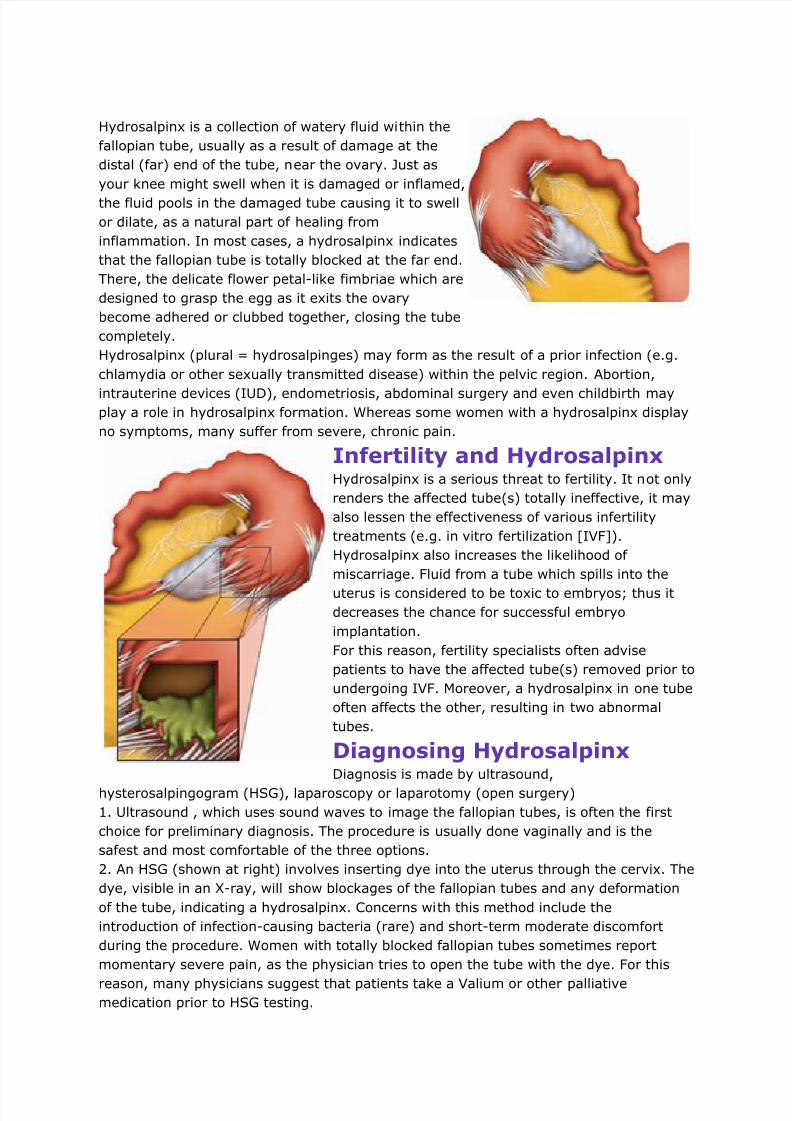
Hydrosalpinx is a collection of watery fluid within the
fallopian tube, usually as a result of damage at the
distal (far) end of the tube, near the ovary. Just as
your knee might swell when it is damaged or inflamed,
the fluid pools in the damaged tube causing it to swell
or dilate, as a natural part of healing from
inflammation. In most cases, a hydrosalpinx indicates
that the fallopian tube is totally blocked at the far end.
There, the delicate flower petal-like fimbriae which are
designed to grasp the egg as it exits the ovary
become adhered or clubbed together, closing the tube
completely.
Hydrosalpinx (plural = hydrosalpinges) may form as the result of a prior infection (e.g.
chlamydia or other sexually transmitted disease) within the pelvic region. Abortion,
intrauterine devices (IUD), endometriosis, abdominal surgery and even childbirth mayplay a role in hydrosalpinx formation. Whereas some women with a hydrosalpinx display
no symptoms, many suffer from severe, chronic pain.
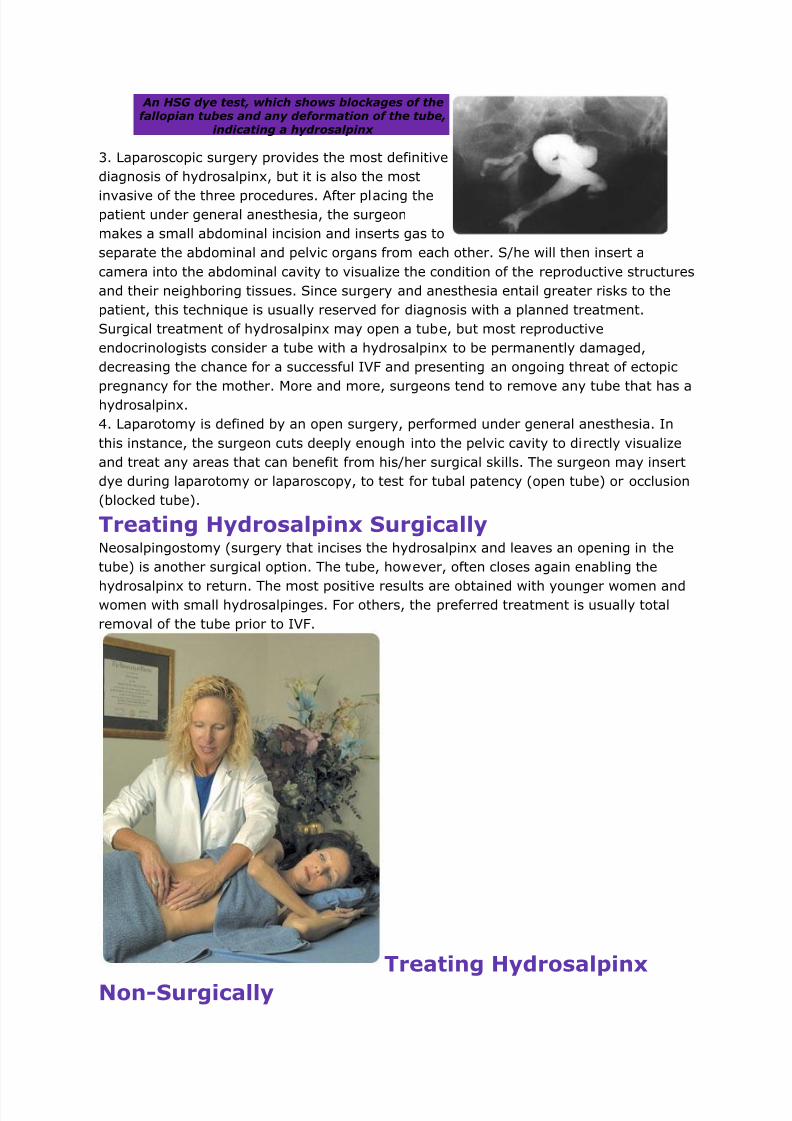
Infertility and HydrosalpinxHydrosalpinx is a serious threat to fertility. It not only
renders the affected tube(s) totally ineffective, it may
also lessen the effectiveness of various infertility
treatments (e.g. in vitro fertilization [IVF]).
Hydrosalpinx also increases the likelihood of
miscarriage. Fluid from a tube which spills into the
uterus is considered to be toxic to embryos; thus it
decreases the chance for successful embryo
implantation.
For this reason, fertility specialists often advise
patients to have the affected tube(s) removed prior to
undergoing IVF. Moreover, a hydrosalpinx in one tube
often affects the other, resulting in two abnormal
tubes.
Diagnosing HydrosalpinxDiagnosis is made by ultrasound,
hysterosalpingogram (HSG), laparoscopy or laparotomy (open surgery)
1. Ultrasound , which uses sound waves to image the fallopian tubes, is often the first
choice for preliminary diagnosis. The procedure is usually done vaginally and is the
safest and most comfortable of the three options.
2. An HSG (shown at right) involves inserting dye into the uterus through the cervix. The
dye, visible in an X-ray, will show blockages of the fallopian tubes and any deformation
of the tube, indicating a hydrosalpinx. Concerns with this method include the
introduction of infection-causing bacteria (rare) and short-term moderate discomfort
during the procedure. Women with totally blocked fallopian tubes sometimes report
momentary severe pain, as the physician tries to open the tube with the dye. For this
reason, many physicians suggest that patients take a Valium or other palliativemedication prior to HSG testing.
8/13/2019 Hydrosalpinx
http://slidepdf.com/reader/full/hydrosalpinx 2/3
An HSG dye test, which shows blockages of thefallopian tubes and any deformation of the tube,
indicating a hydrosalpinx
3. Laparoscopic surgery provides the most definitive
diagnosis of hydrosalpinx, but it is also the most
invasive of the three procedures. After placing thepatient under general anesthesia, the surgeon
makes a small abdominal incision and inserts gas to
separate the abdominal and pelvic organs from each other. S/he will then insert a
camera into the abdominal cavity to visualize the condition of the reproductive structures
and their neighboring tissues. Since surgery and anesthesia entail greater risks to the
patient, this technique is usually reserved for diagnosis with a planned treatment.
Surgical treatment of hydrosalpinx may open a tube, but most reproductive
endocrinologists consider a tube with a hydrosalpinx to be permanently damaged,
decreasing the chance for a successful IVF and presenting an ongoing threat of ectopic
pregnancy for the mother. More and more, surgeons tend to remove any tube that has ahydrosalpinx.
4. Laparotomy is defined by an open surgery, performed under general anesthesia. In
this instance, the surgeon cuts deeply enough into the pelvic cavity to directly visualize
and treat any areas that can benefit from his/her surgical skills. The surgeon may insert
dye during laparotomy or laparoscopy, to test for tubal patency (open tube) or occlusion
(blocked tube).
Treating Hydrosalpinx SurgicallyNeosalpingostomy (surgery that incises the hydrosalpinx and leaves an opening in the
tube) is another surgical option. The tube, however, often closes again enabling the
hydrosalpinx to return. The most positive results are obtained with younger women andwomen with small hydrosalpinges. For others, the preferred treatment is usually total
removal of the tube prior to IVF.
Treating Hydrosalpinx
Non-Surgically
8/13/2019 Hydrosalpinx
http://slidepdf.com/reader/full/hydrosalpinx 3/3
Clear Passage's non-surgical infertility treatment uses pelvic physical therapy to
decrease the adhesions causing tubal damage and hydrosalpinx. Once mobility is
restored, the previously blocked tube(s) often regains normal function, creating a free
path for conception to occur. Read what treatment is like.
This therapy, called the Wurn Technique® has been shown to open tubes and return the
ability to conceive naturally for women with hydrosalpinx (left)1 and blocked fallopian
tubes (right)2 regardless of the location of the blockage. 1,2
Our initial success rates opening hydrosalpinges are very promising, and of interest to
reproductive physicians and surgeons. Recently, Clear Passage Physical Therapy was
honored by the American Society for Reproductive Medicine (ASRM) who invited us to
present abstracts of three studies to their several thousand members. One of these
study abstracts, published in Fertility and Sterility (9/06) examines our ability to open
totally blocked fallopian tubes, with subsequent natural pregnancies and births, in
women with hydrosalpinx.
While the number of participants in this initial study was small, the results were
considered pioneering, and important enough to publish in one of the most prestigiousreproductive medicine journals in the world.
The abstract examined eight women who had confirmed bilateral tubal occlusion
(diagnosed by hysterosalpingogram). Each also had the additional complication of
hydrosalpinx. The women were then treated with the Clear Passage 20-hour protocol of
pelvic physical therapy.
After therapy, 50% of the patients (4/8) had at least one tube with hydrosalpinx opened
by the therapy and half of those became pregnant naturally from the tube that had
hydrosalpinx before therapy. One of the participants has already had a second natural
pregnancy and birth; another had a successful post-therapy IVF, followed by a post-
therapy natural pregnancy and birth. We, and many physicians are very encouraged bythese findings





![Innovation in fertility treatment - fertilityvision.cz · [Murray, Fertil steril, 1998]. TAKE HOME MESSAGE •Improvement in IVF results may have reduced the negative impact of hydrosalpinx](https://img.pdfslide.us/doc/110x75/5cf7ab1f88c99346318d81a1/innovation-in-fertility-treatment-murray-fertil-steril-1998-take-home.jpg)










