Embed Size (px)
Citation preview

IAEA RTC – Hybrid Imaging: SPECT/CT, PET/CT, and Sentinel
Lymph Node Detection
Hybrid Imaging of Infection
Giuliano Mariani
Regional Center of Nuclear Medicine
University of Pisa, Pisa, Italy
Parnu (Estonia), October 6 – 10, 2014

Inflammation ….. a long story
sh me me t
Shememet = inflammation
Smith Papyrus, circa 1650 B.C.
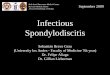
Time after single injury, days
Re
lati
ve
am
ou
nt Edema
Neutrophils
Monocytes/Macrophages
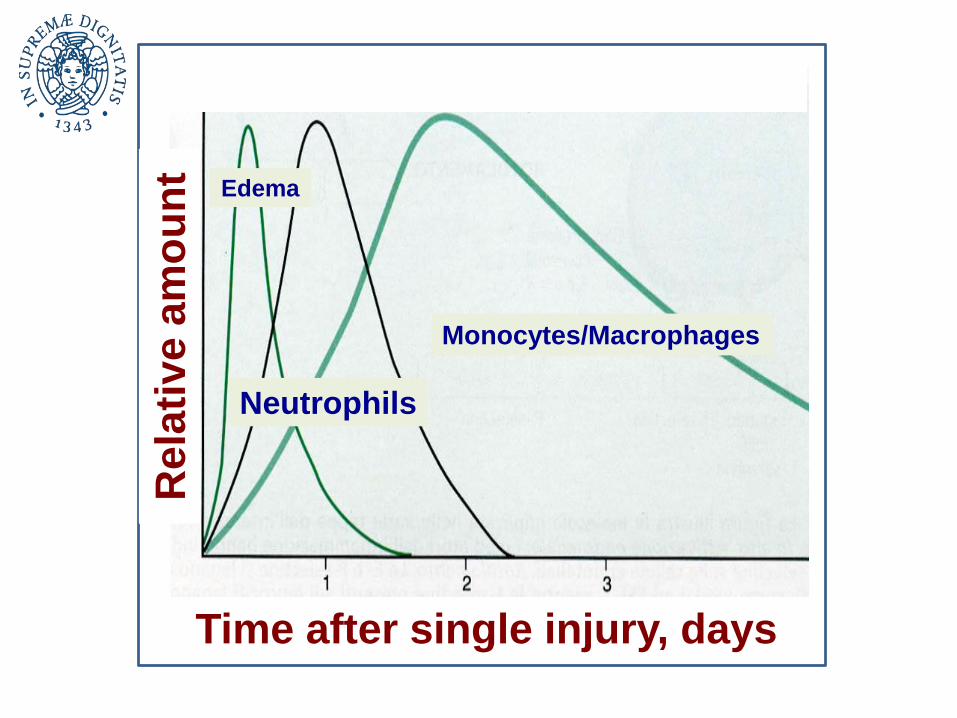
Acute Infection/Inflammation
granulocytes IgM macrophagescitokines
1 2 32

Nuclear Medicine Imaging of Acute
Infection/Inflammation
99mTc-HMPAO-WBC111In-oxine-WBC[18F]FDGAnti-granulocyte MoAb
67Ga-citrate68Ga-citrate
IL-8
18F-FDG
99mTc-Antibiotics111In-VitaminsAntimicrobial peptides

Chronic Infection/Inflammation

67Ga-citrate68Ga-citrate
Nuclear Medicine Imaging of Chronic
Infection/inflammation
[18F]FDG
Moab anti-TNF,IL-2
IL-8 (acute)
IL-1 (chronic)
IL-2 (chronic)
Moab anti-
TNF
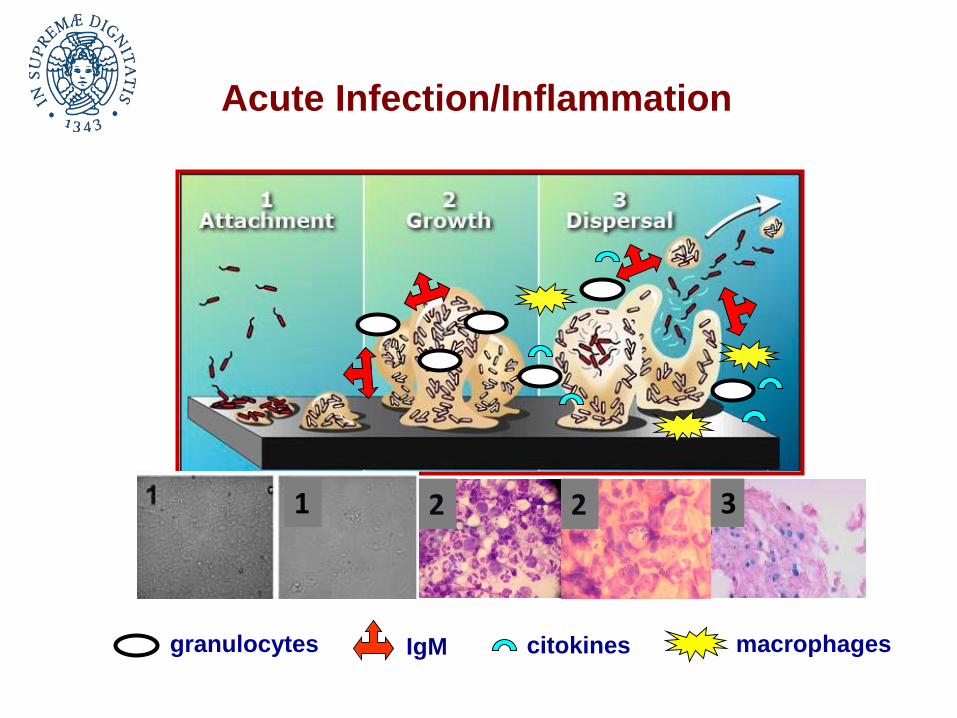
Nuclear Medicine Imaging of Infection
INDIRECT: by targeting the host immune system, proteins, cytokines and hypermetabolic activity
DIRECT: by targeting the bacteria
67Ga-citrate68Ga-citrate
Labelled
leukocytes
MoAb anti-
granulocytes
Labelled
antibioticsLabelled
antimicrobial
peptides
Labelled
vitamins
[18F]FDG
HIG

99mTc-HMPAO-leukocytes
Nuclear Medicine for Indirect Imaging of Infection
Standard Protocol of 99mTc-HMPAO-Leukocyte scintigraphy:
Labelling of leukocytes with 99mTc-HMPAO according to EANM guidelines
(www.eanm.org)
I.v. injection of 99mTc-HMPAO-Leukocytes (370-740 MBq).
Total-body and planar images at 30 min, planar and/or SPECT/CT at 4 hr
and 24 hr.
Advantages: high sensitivity and specificity (except for spine infection).
Limitations: time-consuming, need for specialized staff.
Active chemotaxis in infectious foci
Planar images (anterior and lateral) of 99mTc-
HMPAO-Leukocyte scintigraphy in patient with
vascular (aorto-bifemoral) prosthesis 30 min (left)
and 4 hr (right) p.i.

[18F]FDG Overexpression of Glut-I and Glut-III on the surface of the
inflammatory cells and activated leukocytes
K1
K2
Standard Protocol of [18F]FDG PET/CT:
I.v. injection of 3.5 MBq/kg [18F]FDG
Total-body PET/CT acquisition at 1 hr p.i.
Advantages: high sensitivity
Limitations: low specificity
Follow-up with [18F]FDG PET/CT
in patient with right hip prosthesis
implanted after surgical removal of
femoral head, site of metastasis
from breast cancer.
Nuclear Medicine for Indirect Imaging of Infection

67Ga-citrate68Ga-citrate
Standard Protocol of 68Ga-citrate PET/CT
I.v. injection of 68Ga-citrate (2-3 MBq/kg)
PET/CT acquisition at 1 hr
Advantages: total-body evaluation, short interval before acquisition
Limitations: low specificity
Presence of lactoferrin, transferrin, albumin and cells in
inflammatory tissues; presence of bacterial siderophores
Nanni et al, J Nucl Med. 2010;51:1932-6.
MRI and 68Ga-citrate PET/CT in patient
with diskitis. MRI shows abnormal signal
in L5-S1, equivocal for infective diskitis.
68Ga-citrate PET/CT shows focal area of
increased tracer uptake consistent with
inflammation (SUVmax 5.3).
Nuclear Medicine for Indirect Imaging of Infection

Labelled antimicrobial peptides:99mTc-Ubiquicidin 29-41
Radiopharmaceuticals for Direct Imaging of Infection
Criteria for interpretation: images acquired at 30, 60 (and 120) min
are considered for interpretation, since at 240 min tracer uptake is
markedly reduced.
The target is represented by bacteria

Labelled vit. H (Biotin)Locally increased capillary permeability
(edema), but also growth factor for bacteria
Soft tissue infection by Propionibacterium with minimal bone involvement
Nuclear Medicine for Direct/Indirect Imaging of Infection

So … Which Radiopharmaceutical?
[18F]FDG

The right answer depends on:
1) Region of the body to be explored
2) activity of disease (acute, chronic, subacute)
Disease Radiopharmaceutical
Acute infection Labelled leukocytes
[18F]FDG
Chronic infection 67Ga-citrate
[18F]FDG
So … Which Radiopharmaceutical?

Region of interest Agent Acquisition Imaging
Heart Labelled leukocytes (WBC)[18F]FDG
30’, 4 h, 24 h1 h
Total-body (FUO)High probability
Low probability
Labelled leukocytes[18F]FDG
30’, 4 h, 24 h1 h
Large vessel vasculitis [18F]FDG 1 h
CNS Labelled leukocytes 30’, 4 h, 24 h
Bone and Joint :Low probability
High probability Dynamic bone scanLabelled leukocytes 30’, 4 h, 24 h
Spine 67Ga-citrate (+ bone scan)[18F]FDG
6h, 24 h, 48 h1 h
Bowel Labelled leukocytes 30’ and 2 hr
Foot (diabetic foot) Labelled leukocytes 30’, 4 h, 24 h
Vascular prosthesisChest
Abdomen
Labelled leukocytesLabelled leukocytes[18F]FDG
30’, 4 h, 24 h30’, 4 h1 h
SPECT/CT is recommendedPET/CT is recommended
SPECT/CT according to ROI
PET/CT is recommended
PET/CT is recommended
Planar SPECT/CT if necessary
PlanarSPECT/CT if necessary
SPECT/CT is recommendedPET/CT is recommended
PlanarSPECT/CT if necessary
SPECT/CT is recommended
SPECT/CT is recommended
PET/CT is recommended
NM Imaging of Infection/Inflammation

Jutte P, Lazzeri E, Sconfienza LM,
Cassar-Pullicino V, Trampuz A, Petro-
sillo N, Signore A.
Diagnostic flowcharts in osteomyelitis,
spondylodiscitis and prosthetic joint
infection.
Q J Nucl Med Mol Imaging 2014;58:2-19.

Some Practical Considerations
Regarding Hybrid Imaging of Infection
Clinical problems:
1. Is infection present?
1. If YES, is exact anatomic localization
of infection likely to impact on clinical
treatment?

Definite Impact on Treatment (1)
Osteomyelitis:
Is infection limited to bone or does it involve
adjacent soft tissues?
Diabetic foot infection:
Is infection involving soft tissues only or does
it involve bone(s) as well?
Joint prosthesis:
Is infection involving the bone only, bone and
soft tissues, or soft tissues only?

Definite Impact on Treatment (2)
Spine infection (non-operated/post-surgery):
Is infection involving the vertebral body, body
and disc, or involving soft tissues as well?
Is the hardware involved, at different levels?
Cardiovascular infection:
Endocarditis on native valves?
Endocarditis on prosthetic valves
(mechanical/biological)?
Is septic embolism present?
Implanted electrical devices (surgical pocket,
intravascular leads, intracardiac leads).
Prosthetic vascular grafts.

Peripheral bone
Osteomyelits (Bone Infection)
Spine (SD)
Joint prosthesis

Planar SPECT/CT
Calcaneal bone osteomyelitis
High probability of Acute OM:99mTc-HMPAO-WBC

High probability of Acute OM:
Leukoscan®
Soft tissue infection without bone infection
Planar SPECT/CT

Bone and soft tissue infection
High probability of Acute OM:99mTc-HMPAO-WBC
Planar SPECT/CT

SPECT/CT
Hardware infection by St. Epidermidis
High probability of Acute OM:99mTc-HMPAO-WBC

30 min p.i. 4 h p.i. 24 h p.i.
Joint infection by St. Aureus
High probability of Acute Joint Infection:99mTc-HMPAO-WBC

Soft tissue infection
High probability of Acute Prosthetic Joint
Infection: 99mTc-HMPAO-WBC
Planar SPECT/CT

November 2011
July 2012
March 2012
Prosthetic Joint Infection: Evaluation of
Response with 99mTc-HMPAO-WBC

Reinartz classification
Prosthetic Joint Infection: [18F]FDG PET/CT

Pattern 1 Pattern 2 Pattern 3a
Pattern 4a Pattern 4b Pattern 5
No loosening
Loosening
Reinartz P. Q J Nucl Med Mol Imaging 2009;53:41-50
Prosthetic Joint Infection: [18F]FDG PET/CT

Bone and Joint Infection
Meta-analysis of 87 studies (1984-2004): WBC scintigraphy has
excellent diagnostic accuracy (up to 89%) with sensitivities and
specificities ranging from 83% to 89% and 84% to 90%,
respectively.
(Prandini N et al. Nucl Med Commun. 2006;27:633-44)
SPECT/CT can improve imaging with WBC in patients with
suspected osteomyelitis by providing accurate anatomic
localization and precise definition of the extent of infection.
(Filippi L et al. J Nucl Med
2006;47:1908-13)
WBC scintigraphy remains the gold standard technique for
diagnosing neutrophil-mediated processes. WBC/bone marrow
scintigraphy is currently the modality of choice for diagnosing
prosthetic joint infection. PET will receive full acceptance only
when specific [18F]FDG uptake patterns can be validated.(Gemmel F et al.
Eur J Nucl Med Mol Imaging. 2012; 39:892–909)
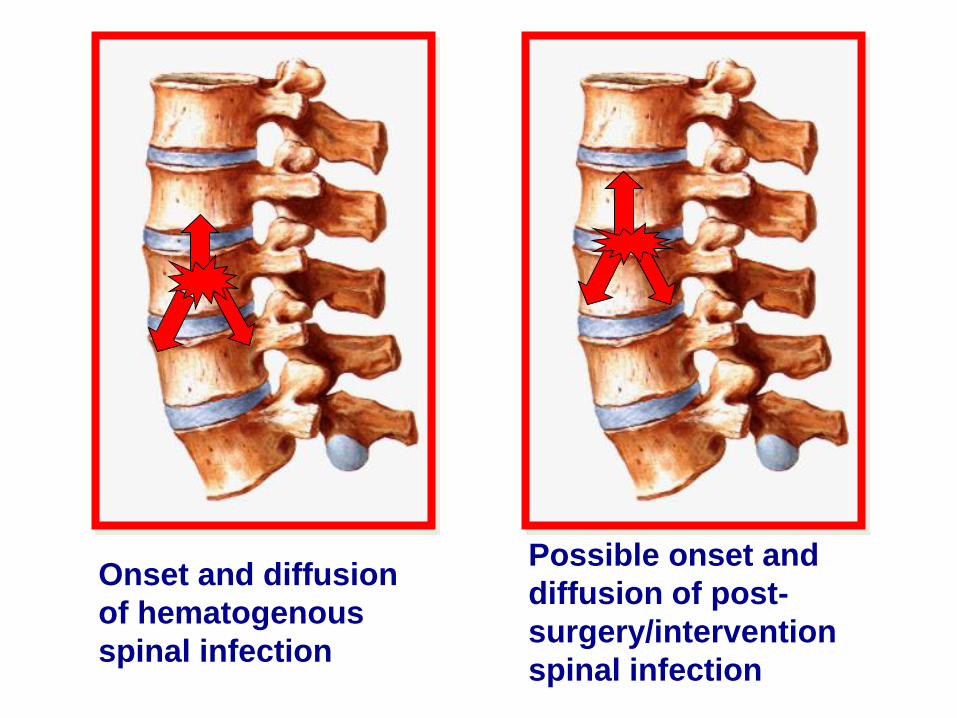
Onset and diffusion
of hematogenous
spinal infection
Possible onset and
diffusion of post-
surgery/intervention
spinal infection

Vertebral Osteomyelitis (SD)
Low probability of SD
• 99mTc-MDP Bone scan
High probability of SD
• 67Ga+99mTc-MDP
• [18F]FDG PET/CT
High probability of SD
• 67Ga-citrate + 99mTc-MDP
• [18F]FDG PET/CT

Vertebral Osteomyelitis: [18F]FDG-PET/CT
SD at L4 (Propionibacterium) and at C7 (MR St. Aureus)

MRI
Vertebral Osteomyelitis: [18F]FDG-PET/CT
bone biopsy
Bone metastasis from melanoma

111In-DTPA-Biotin[18F]FDG
Infection of the cervical spine

A systematic review of the literature (1984-2004) indicates that
the accuracy of infection tracers used for spondylodiscitis
varies from 62% to 90%.(Prandini N et al. Nucl
Med Commun. 2006;27:633-44)
“FDG-PET is a promising alternative to bone/gallium imaging.
The advantages of the procedure are obvious: the study is
sensitive, it is completed in a single session and image
resolution is superior to that obtained with single-photon-
emitting tracers. As with gallium, however, specificity remains
an issue.
While FDG uptake in uninfected fractures may normalise sooner
than gallium or diphosphonate uptake, differentiating infection
from tumour will be problematic.“(Gemmel F. Eur J Nucl Med Mol
Imaging 2006;33:1226–1237)
Vertebral Osteomyelitis (SD)

Region of interest Radiopharmaceuticals Acquisition Imaging
Peripheral bone infections
Low probability
High probability Dynamic bone scanLabelled leukocytes
3 h30’, 4 h, 24 h
Joint infection and prosthetic joint infection
Low probability
High probability Dynamic bone scanLabelled leukocytes
3 h30’, 4 h, 24 h
Spine infections
Low probability
High probability Bone scan67Ga-citrate (+ bone scan)[18F]FDG PET
3 h6 h, 24 h. 48h1 h
PlanarSPECT/CT if necessary
PlanarSPECT/CT if necessary
SPECT/CT is recommendedPET/CT is recommended
Nuclear Medicine Imaging of
Osteomyelitis

Imaging for Suspected
Postoperative Spondylodiscitis
• Radiography
• Computed Tomography
• Magnetic Resonance Imaging
• Bone scintigraphy
• SPECT, SPECT/CT
• PET, PET/CT

Sumer J et al. SPECT/CT in patients with lower back pain
after lumbar fusion surgery (LFS). Nucl Med Commun 2013
• Retrospective study in 37 patients with lower back pain
after LFS: three-phase bone scan and delayed
SPECT/CT.
• Five diagnostic categories:
1) metal loosening
2) insufficient stabilization of metal implants
3) adjacent instability for degenerative disease
4) indeterminate
5) normal
• Normal scan in 8/37 patients.
• 62 abnormal foci by planar/SPECT; 55 by SPECT/CT
• SPECT/CT reclassified 28/62 foci (45.2%): 5/12 in class 1;
16/29 in class 2; 7/20 in class 3; 1/1 in class 4.

Spinal hardware
infection
Loosening of upper
construct screws without
infection
Bagrosky et al. Pediatr Radiol 2013
[18F]FDG PET/CT in Suspected Infection of
Hardware after Spine Fusion Surgery
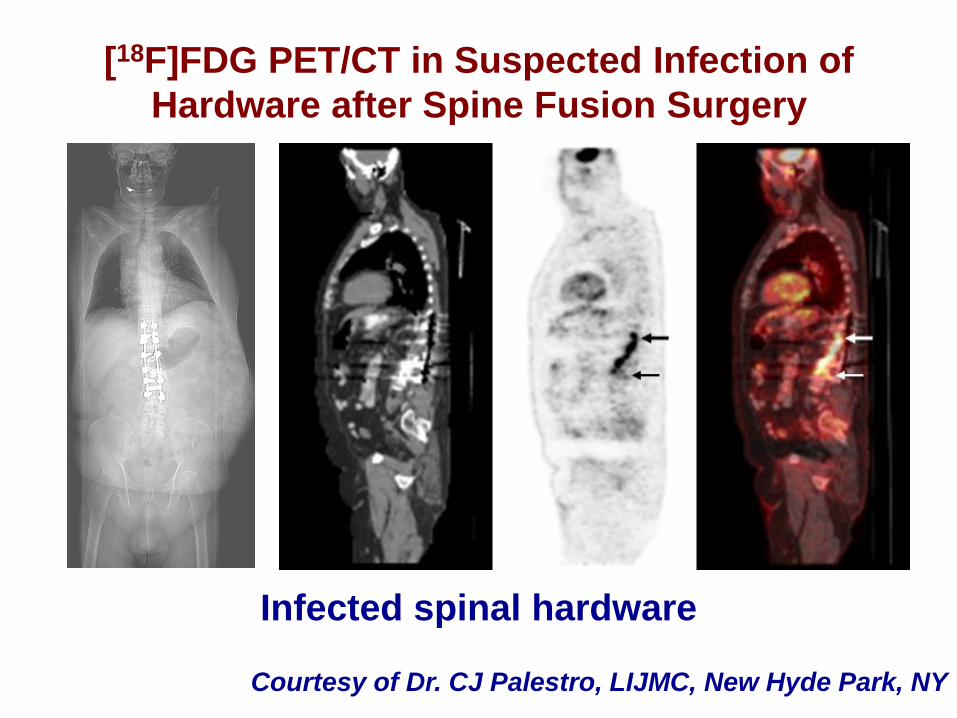
Infected spinal hardware
[18F]FDG PET/CT in Suspected Infection of
Hardware after Spine Fusion Surgery
Courtesy of Dr. CJ Palestro, LIJMC, New Hyde Park, NY

[18F]FDG PET/CT in Suspected Infection of
Hardware after Spine Fusion Surgery
Courtesy of Dr. CJ. Palestro, LIJMC, New Hyde Park, NY
Uninfected spinal hardware

Physiologic
al [18F]FDG
distribution
Slightly elevated uptake in the inter- or paraverte-bral region
Clearly elevated uptake with linear or disci-form pattern in the interverte-bral space
Clearly elevated uptake with linear or disciformpattern in the inter-vertebral space and involvement of ground or cover plate or both plates of the adjacent vertebrae
Clearly elevated uptake with linear or disciform pattern in the intervertebral space and involvement of ground or cover plate or both plates of the
adjacent vertebrae +
surrounding soft-tissue
abscess
normal disciti
s
spondylodisciti
s
[18F]FDG in Spinal Infection
Hungenback et al. Nucl Med Commun 2013

Score 2 Score 3
Score 4
[18F]FDG in Spinal Infection
Hungenback et al. Nucl Med Commun 2013

“FDG-PET is a promising alternative to HDP/gallium
imaging because:
- the study is highly sensitive
- the study has high image resolution
-the study is completed in a single session
However, specificity remains an issue because non-
specific accumulation of FDG around the fusion
material is not uncommon and differentiating infection
from tumour will be problematic”
Caveats about [18F]FDG in Spinal Infection
Gemmel et al. Eur J Nucl Med Mol Imaging 2006

At diagnosis After
antibiotic therapy
[18F]FDG PET/CT for Assessing Response to
Therapy in Spinal Infection
Possible threshold in ΔSUVmax change: around 45%

• Kim et al. Prediction of residual disease of
spine infection using F-18 FDG PET/CT.
Spine (Phila Pa 1976) 2009.
• Nanni et al. FDG PET/CT is useful for the
interim evaluation of response to therapy
in patients affected by haematogenous
spondylodiscitis. Eur J Nucl Med Mol
Imaging 2012.

Advantages
• Diagnostic accuracy better than bone/gallium.
• High sensitivity.
• Total-body imaging allows the detection of septic
embolism.
• High negative predictive value.
• Potential for monitoring the efficacy of therapy.
Limitations
• Published evidence: less than a dozen articles with
less than 200 total patients.
• Relatively poor specificity.
• False-positive results possible because of:
- degenerative diseases
- post-surgical inflammatory reaction/recent
fracture
- primary and metastatic spine tumors
Strengths/Weaknesses of [18F]FDG PET for
Spinal Infection

SPECT/CT with 99mTc-HMPAO-WBC:
the Diabetic Foot

99mTc-HMPAO-WBC SPECT/CT: focal accumulation involving both
the soft tissues and the 2rd metatarsal bone (soft tissue infection
and concomitant osteomyelitis).

99mTc-HMPAO-WBC SPECT/CT with 3D fusion Volume Rendering

Diabetes Care 2012; 35: 1826-1831
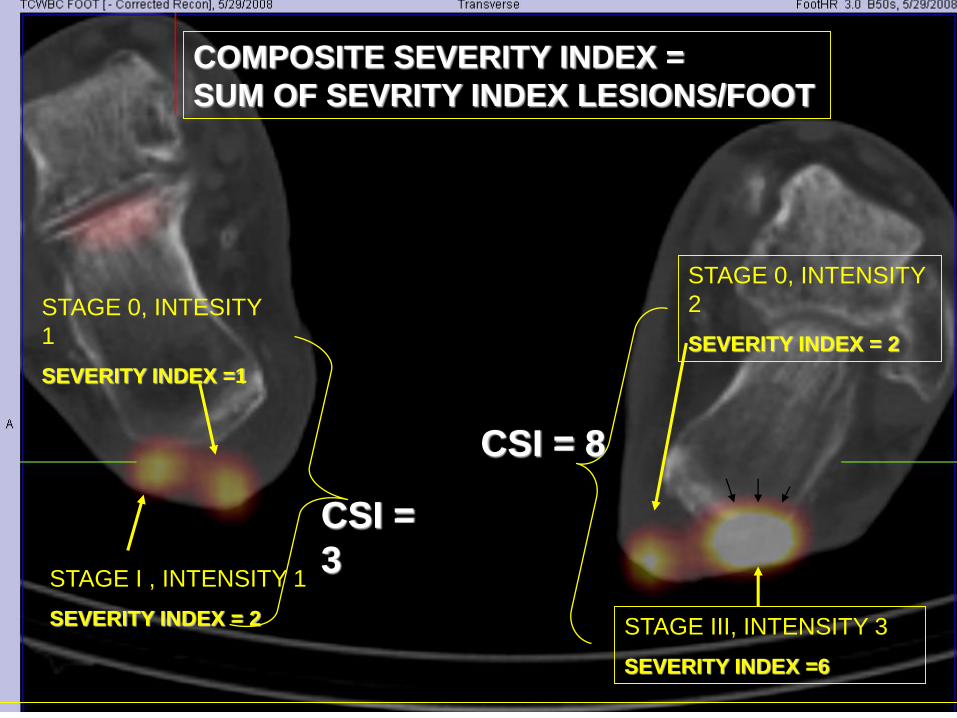
STAGE 0, INTENSITY
2
SEVERITY INDEX = 2
STAGE III, INTENSITY 3
SEVERITY INDEX =6
STAGE I , INTENSITY 1
SEVERITY INDEX = 2
STAGE 0, INTESITY
1
SEVERITY INDEX =1
COMPOSITE SEVERITY INDEX =
SUM OF SEVRITY INDEX LESIONS/FOOT
CSI =
3
CSI = 8

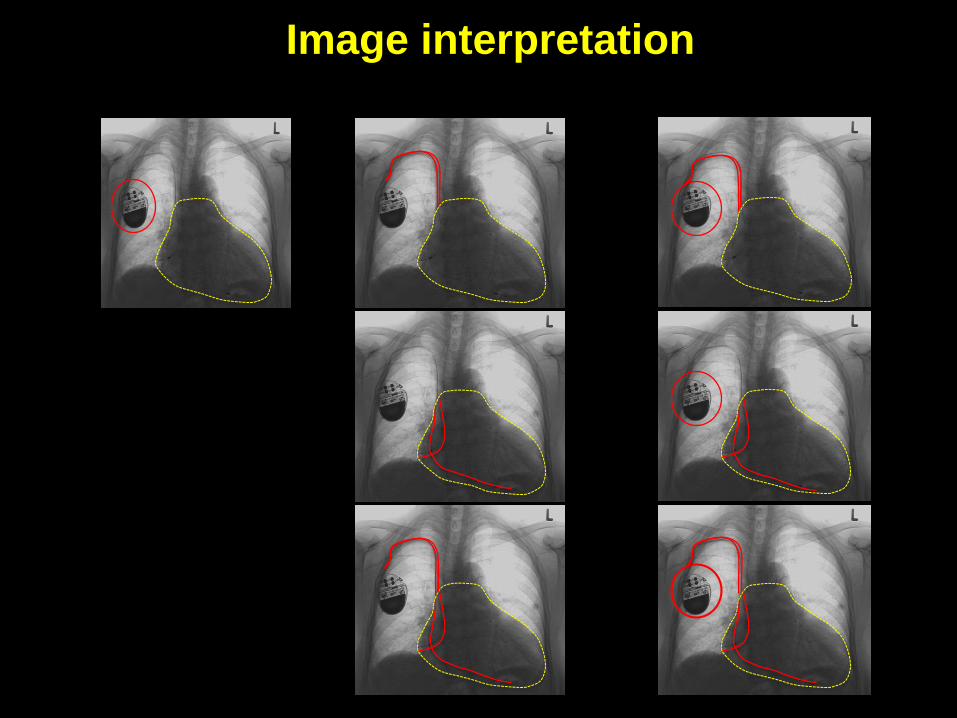
[18F]FDG PET/CT for Infective Endocarditis

Image interpretation
NEGATIVE for IE POSITIVE for IE
Negative Infection
extra-IE
IE IE+ embolism/
extra-IE
infection

99mTc-HMPAO-WBC scan in patient with “Possible” IE (mechanical
prosthesis of mitral valve). Fever and leukocytosis. Negative TTE
and TEE); blood colture positive for St. Aureus
Labelled WBC for Infective Endocarditis

99mTc-HMPAO-WBC SPECT/CT in patient with “Definite” IE
(positive blood cultures -Pseudomonas- and fever few months
after implant of mitral valve mechanical prosthesis). Clear focus
of uptake in right heart, that SPECT/CT identifies as endocarditis
of the native tricuspid valve. Endocarditis of mechanical
prosthesis, expected site of infection was thus excluded.
Labelled WBC for Infective Endocarditis

65 yr old man with previous IE after kidney
transplantation; occasional finding of vegetation at
the mitral valve. No fever, normal WBC.

Baseline
May 2007
After ABT
October 2007
Pocket EC Pocket + EC
Image interpretation
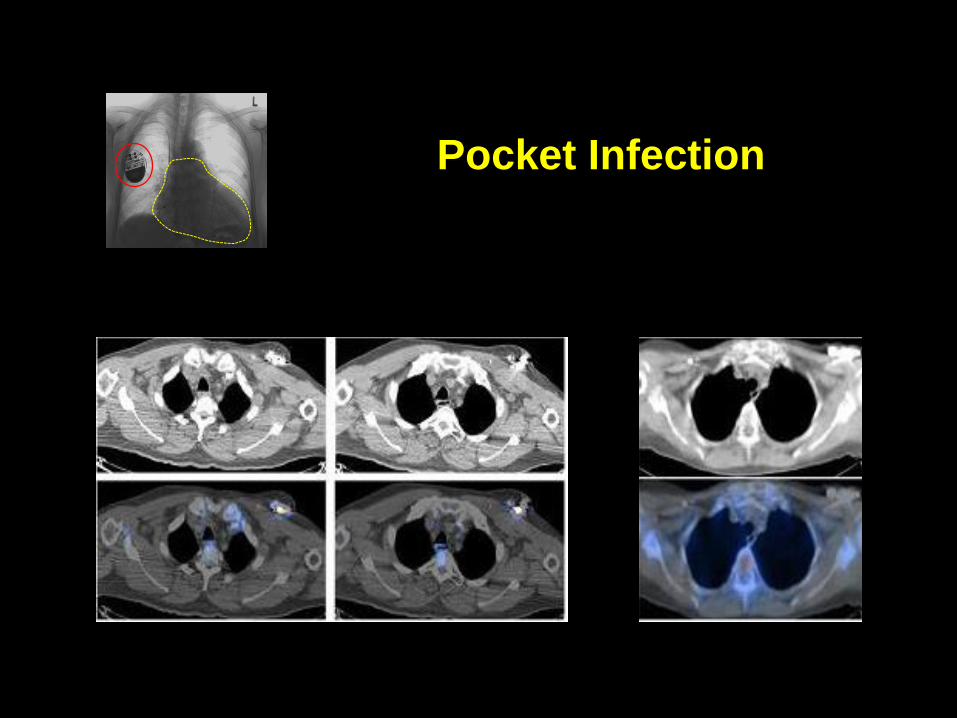
Pocket Infection
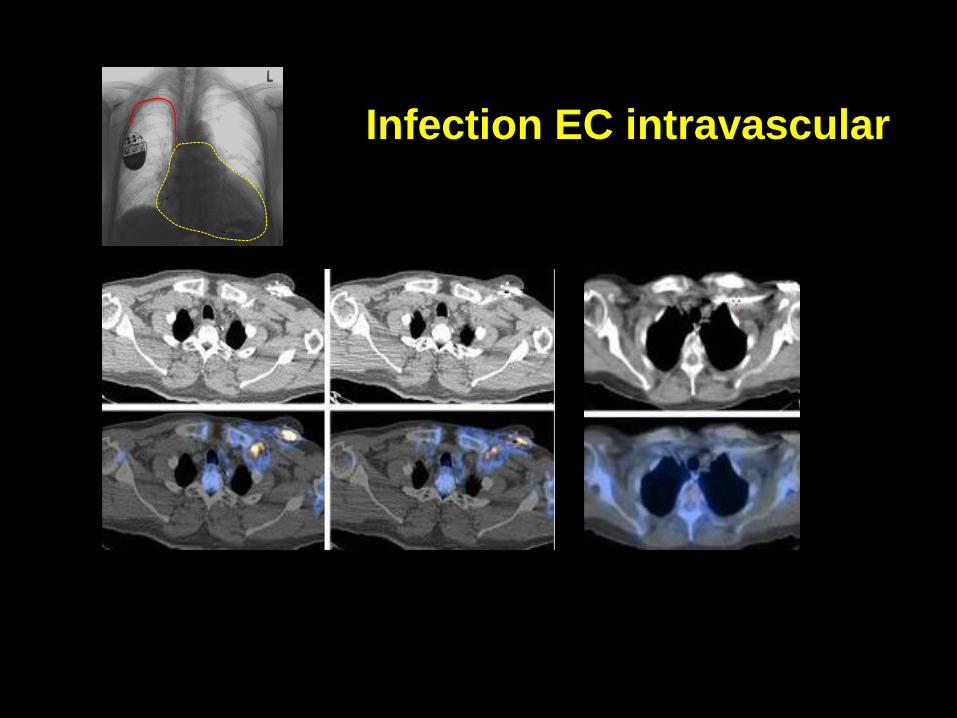
Infection EC intravascular

99mTc-HMPAO-WBC SPECT/CT
Infection of the intracardiac portion of the lead

Advantages:
• High sensitivity.
• Whole-body images allow the detection of septic embolism.
• High negative predictive value.
Limitations:
• Relatively poor specificity.
• Chance of high uptake of myocardial tissue.
• False-positive results possible because of:
- recent thrombi
- soft atherosclerotic plaques
- primary and metastatic cardiac tumors
- sarcoidosis
- post-surgical inflammatory reaction
- artifacts
Diagnostic Performance of [18F]FDG PET/CT for IE

Advantages:
• Discrimination between septic and sterile vegetations
detected at echocardiography.
• Whole-body images followed by additional planar and
SPECT/CT spot images allow the detection of distant
sites of septic embolism.
Limitations:
• False-negative results possible because of:
- small vegetations (< 5 mm)
- mycetes and infections with low leukocyte
recruitment
- long-lasting antibiotic treatment
- warning for very early post-surgical IE
Diagnostic Performance of Labelled WBC for IE

Millar BC et al, Int J Cardiol (2013)

Classification of Vascular Prosthesis
Infections (VPI)
Time from procedure to infection:
• Early (acute): < 4 months (+++ first 2 months)
• Subacute: 4-12 months
• Late (chronic): > 12 months (“biofilm”)

• Scintigraphy with radiolabelled WBC
(99mTc o 111In) is most frequently used.
• Pre-hybrid imaging meta-analysis:99mTc-HMPAO-WBC sensitivity: 82-100%
specificity 85-100%
versus 75% sensitivity 75and 56.6% specificity
for CT

SPECT/CT:
reduces FP
defines extent of disease
facilitates imaging reading even when post-surgical changes are present
high specificity even if performed early post-surgery
high sensitivity for late VPI

30 min
4 ore

[18F]FDG-PET/CT for VPI Assessment:
Sensitivity = 93% (versus 64% for CT)
Specificity = 70-91% (versus 86% for CT)
increased accuracy when the criteria of
FOCAL [18F]FDG uptake + irregular border of
the prosthesis are adopted
Diffuse uptake = inflammation, post-surgical
scar that can persist for years after surgery
(heterologous material)



Focal [18F]FDG + irregular prosthesis
border can predict the presence of VPI
with <5% diagnostic error
Spacek et al. Eur J Nucl Med Mol Imaging. 2009
• 99mTc-HMPAO WBC “gold standard” for diagnosis of VPI
• diagnostic accuracy increases by using SPECT/TC
• [18F]FDG-PET/CT with specific interpretation criteria is good option

1. High clinical suspicion and negative CT.
2. Lack of clinical response after adequate
antibiotic therapy.
3. Monitoring treatment response?
When and Why?

1. Clinical suspicion wih
unconclusive diagnostic angio-
CT
2. Lack of clinical response after
adequate ABT
3. Monitoring treatment response? [18F]FDG
Labeled
WBC
Labeled
WBC
Which Radiopharmaceutical?
[18F]FDG
High NPV